Back to Journals » OncoTargets and Therapy » Volume 18
Serum Response Factor Expression, Microvascular Density, and Postoperative Recurrence in Glioblastoma
Authors Tan B ![]() , He S, Chen T, Song P, Huang Y, Yin X
, He S, Chen T, Song P, Huang Y, Yin X
Received 10 June 2025
Accepted for publication 12 September 2025
Published 19 September 2025 Volume 2025:18 Pages 1043—1052
DOI https://doi.org/10.2147/OTT.S546017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr John Riches
Bo Tan, Shuangyin He, Tao Chen, Peng Song, Yaohui Huang, Xiaohong Yin
Neurosurgery of Guangyuan Central Hospital, Guangyaun, Sichuan, 628000, People’s Republic of China
Correspondence: Xiaohong Yin; Bo Tan, Email [email protected]; [email protected]
Objective: To investigate the association between serum response factor (SRF) expression, tumour microvascular density (MVD), and postoperative recurrence in glioblastoma.
Methods: This retrospective study analysed 92 patients with histologically confirmed glioblastoma treated between July 2021 and July 2023. Tumour and adjacent normal brain tissues were collected during surgery for immunohistochemical detection of SRF and CD105. MVD was determined by counting CD105-positive microvessels in the most vascularised tumour regions. Spearman correlation assessed the association between SRF and MVD. All patients underwent maximal surgical resection and were followed for 1 year. Recurrence was defined by MRI. Multivariate logistic regression identified independent predictors of recurrence.
Results: SRF-positive tumours were significantly more frequent than in adjacent normal brain tissue (56.5% vs 2.2%, P< 0.001) and had higher MVD (86.79 ± 14.12 vs 70.58 ± 8.77 vessels/field, P< 0.05). SRF expression correlated positively with MVD (r = 0.749, P< 0.05). At 1 year, 24 patients (26.1%) recurred. Compared with non-recurrent cases, the recurrence group had higher rates of SRF positivity, tumour size ≥ 5 cm, poor differentiation, high grade, and incomplete resection (all P< 0.05). Multivariate analysis identified SRF positivity, tumour size ≥ 5 cm, poor differentiation, high grade, and incomplete resection as independent recurrence predictors.
Conclusion: SRF overexpression in glioblastoma is associated with increased angiogenesis and higher recurrence risk. SRF may promote tumour proliferation, differentiation, and migration, and serve as a prognostic biomarker and potential therapeutic target.
Keywords: glioblastoma, serum response factor, immunohistochemistry, microvascular density, recurrence
Introduction
Glioblastoma (GBM), the most prevalent and most aggressive primary malignancy of the brain, comprises more than half of intracranial malignant tumors.1–3 It is marked by rapid cellular proliferation, widespread infiltration into adjacent brain tissue, and pronounced resistance to available therapies.4 Collectively, these features result in an extremely poor prognosis. Patients with GBM typically present with signs of elevated intracranial pressure (such as headaches, nausea, and vomiting) along with focal neurological deficits, for example, seizures and disturbances of vision.5–7 Even with aggressive standard therapy that combines maximal surgical resection with postoperative radiotherapy as well as chemotherapy, achieving complete tumor elimination is rare.8 Postoperative recurrence is common. As a result, the median survival time for patients with GBM is only around 12 to 15 months, and the five-year survival rate remains under 5%s;9 these grim outcomes underscore the urgent need to identify reliable biomarkers that reflect tumor progression and inform therapeutic decision-making.
One potential biomarker is the serum response factor (SRF), a MADS-box transcription factor encoded at the 6p21.1 locus that regulates a wide range of genes involved in cytoskeletal organization, cellular motility, and cell growth. SRF is a key regulator of fundamental cellular processes such as proliferation, migration, and differentiation.10,11 It also influences angiogenesis by modulating vascular remodeling and the migration of endothelial cells. Aberrant SRF expression occurs in multiple other cancers (eg, esophageal, gastric, and hepatocellular carcinomas). This dysregulation is often accompanied by heightened invasive and metastatic behavior.10–12 Initial evidence suggests that SRF is upregulated in GBM, implying a potential prognostic role in this disease.8 At a mechanistic level, SRF can drive neovascularization and tumor invasiveness through upregulation of various matrix-remodeling and pro-angiogenic factors, including vascular endothelial growth factor (VEGF), matrix metalloproteinase-9 (MMP-9), and the chemokine CXCL12.2,13 Moreover, extensive tumor angiogenesis is a hallmark of GBM. One measure of tumor angiogenesis is microvessel density (MVD), typically measured by immunostaining for an endothelial marker (eg, CD105). This parameter reflects the extent of neovascularization within the tumor. A higher MVD generally indicates a more aggressive tumor.13–15
Because SRF appears to promote tumor progression, and angiogenesis is a central feature of GBM, we hypothesized that elevated SRF expression might contribute to tumor angiogenesis and in turn increase the likelihood of recurrence. To test this hypothesis, we performed a retrospective analysis of 92 GBM patients, examining whether SRF expression levels were correlated with tumor MVD and tumor recurrence following surgery. Additionally, we evaluated various clinical factors linked to recurrence and examined the prognostic significance of SRF expression.
Materials and Methods
General Information
We retrospectively reviewed 92 patients with pathologically confirmed gliomas who underwent surgery at Guangyuan Central Hospital between July 2021 and July 2023. The study population comprised 50 men and 42 women, with ages ranging from 35 to 70 years (mean ± SD: 52.68 ± 6.55 years). The mean body mass index (BMI) was 22.14 ± 2.12 kg/m² (range: 18.63–26.98 kg/m²). The average Karnofsky Performance Status (KPS) score was 85.78 ± 3.75. Tumor sites included the frontal lobe (n = 46), temporal lobe (n = 25), parietal lobe (n = 17), and other brain regions (n = 4). Based on preoperative MRI, 51 tumors measured <5 cm, while 41 were ≥5 cm. The 5 cm threshold was selected because it is widely used in neuro-oncology for prognostic stratification and treatment planning, and it also approximated the median tumor size in this cohort. Tumor differentiation and histological grade were determined according to the 2021 WHO Classification of Central Nervous System Tumors.15 In total, 37 tumors were categorized as low-grade and 55 as high-grade. Histological grading included Grade I (11 cases), Grade II (29 cases), Grade III (30 cases), and Grade IV (22 cases). Among the low-grade cases (40 tumors), there were 11 pilocytic astrocytomas and 29 oligodendrogliomas; among the high-grade group (52 tumors), 14 were anaplastic astrocytomas, 16 anaplastic oligodendrogliomas, and 22 glioblastomas. The study protocol was reviewed and approved by the Ethics Committee of Guangyuan Central Hospital (Approval No. GYZX220627), and written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Patient Selection
Inclusion Criteria
- Histological diagnosis of glioma according to the 2018 “Guidelines for Diagnosis and Treatment of Brain Gliomas”.13
- Underwent surgical resection with curative intent, based on imaging and clinical criteria.
- Adequate cognition and communication, KPS >70, and agreement to participate in follow-up.
- No prior chemo-, radio-, or immunotherapy before surgery.
- Availability of complete clinical, pathological, and follow-up data.
Exclusion Criteria
- Presence of other intracranial disorders (eg, mass lesions, trauma, stroke, vascular malformations).
- Previous intracranial surgery, radiotherapy, chemotherapy, or recurrent glioma.
- Other active malignancies, systemic infection, hematologic or immune disorders, organ dysfunction, or psychiatric illness.
- Pregnant or lactating women.
- Estimated life expectancy <1 year.
Tumor Tissue Acquisition and Immunohistochemistry
Tissue Collection
Preoperative MRI was used to determine tumor size, location, and extent. After routine preparation and general anesthesia, patients received 2–3 mg/kg of 1% sodium fluorescein intravenously to enhance intraoperative visualization. Tumor resection was performed under microscopic guidance, and a sample of normal brain tissue (>5 cm from the lesion) was also obtained as a control. All specimens were preserved in liquid nitrogen.
Immunohistochemistry (IHC)
Collected specimens were fixed in 10% neutral-buffered formalin and embedded in paraffin. Sections of 4 μm thickness were cut, deparaffinized, and rehydrated. Antigen retrieval was performed using citrate buffer (pH 6.0), and endogenous peroxidase activity was quenched with 3% hydrogen peroxide. Slides were blocked with 10% goat serum, then incubated overnight at 4°C with primary antibodies against SRF and CD105 (dilution 1:100). Following washing, appropriate HRP-conjugated secondary antibodies were applied for 30 minutes at 37°C. Staining was developed using DAB and counterstained with hematoxylin. Positive and negative tissue controls were included to verify staining specificity. Two certified pathologists independently evaluated all slides under a light microscope (Olympus CX21), blinded to clinical information. Cohen’s kappa coefficient was used to assess inter-rater reliability.
Evaluation Criteria
SRF Expression
Scored using a semiquantitative immunoreactive score (IRS), combining staining intensity (0–3) and percentage of positive cells (0–4). IRS >4 indicated positive expression.14
Microvascular Density (MVD)
Assessed by CD105 staining. The five most vascularized regions (“hot spots”) per section were identified at low power (×100). Microvessels were counted in five high-power fields (×400), and the average was taken as MVD.15
All patients were monitored for 12 months with MRI every 3 months and/or clinical examination. Recurrence was defined according to RANO criteria as new enhancing lesions on T1-weighted MRI or progression of existing lesions. Images were reviewed independently by two experienced neuroradiologists blinded to clinical data, and patients were categorized into recurrence and non-recurrence groups.
Statistical Analysis
Analyses were performed with SPSS 26.0. Continuous variables were expressed as mean ± SD and compared using t-tests; categorical variables as frequencies and percentages, compared with chi-square or Fisher’s exact test. Correlations between SRF expression (binary) and MVD were assessed by Spearman’s test. Significant univariate predictors of recurrence were entered into multivariate logistic regression to identify independent risk factors, reported as odds ratios (OR) with 95% confidence intervals (CI). A P-value <0.05 was considered statistically significant. In addition, Kaplan–Meier curves and Log rank tests were used to analyze recurrence-free survival (RFS), and Cox regression was applied for multivariate survival analysis. Assumptions of proportional hazards were checked using Schoenfeld residuals. As this was an exploratory, single-center retrospective study, no formal sample size calculation was performed, and results should be interpreted with caution.
Results
SRF Expression and Microvascular Density in Tumor and Adjacent Brain Tissue
Of the 92 glioblastoma specimens analyzed, SRF positivity was observed in 52 cases (56.5%), whereas only 2 out of 92 samples (2.2%) from adjacent non-tumorous brain tissue showed immunoreactivity (χ² = 65.53, P < 0.001). The average MVD in glioblastoma tissue reached 78.59 ± 10.36 vessels per field, which was markedly greater than that in normal brain tissue (9.68 ± 1.85; t = 62.806, P < 0.001). These findings highlight the upregulation of SRF and enhanced angiogenesis in GBM (Table 1). Furthermore, recurrent tumors were significantly more likely to be SRF-positive, and SRF-positive samples showed higher MVD levels compared with SRF-negative ones (Figure 1).
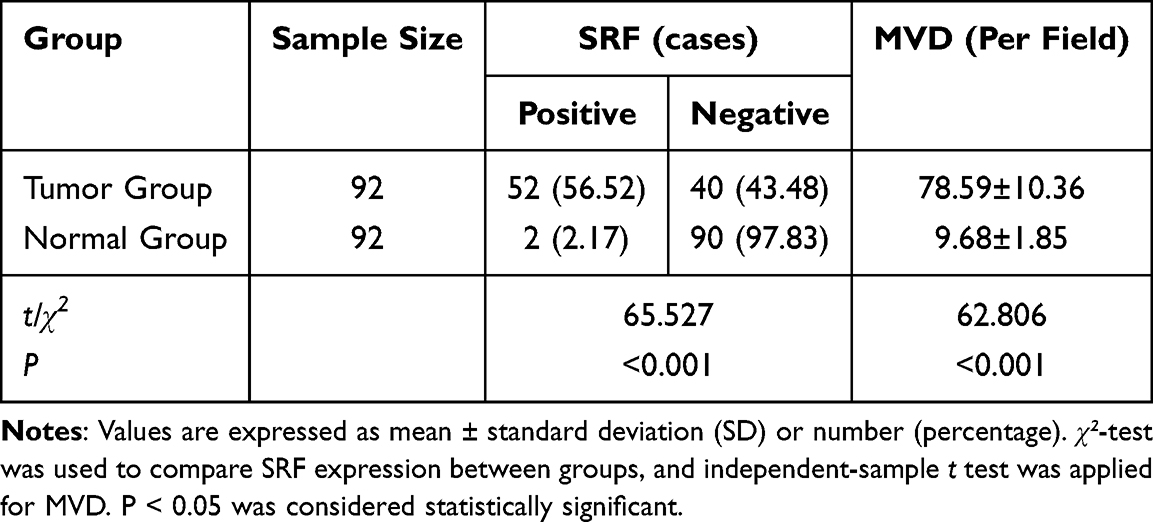 |
Table 1 SRF Immunoreactivity and MVD in Glioblastoma Versus Normal Brain [Mean ± SD, n (%)] |
 |
Figure 1 SRF expression and MVD in glioma: tumor vs normal and recurrence vs non-recurrence. Notes: Left Panel: Stacked bar plot illustrating the percentage of SRF-positive and SRF-negative cases in tumor and normal tissues, with a dot plot overlaid to show mean MVD (microvessel density) per field ± standard deviation (Tumor: 78.6 ± 10.4, Normal: 9.7 ± 1.9). Both SRF expression and MVD show significant differences (P<0.001). Right Panel: Line plot comparing the percentage distribution of significant clinical features (SRF expression, tumor diameter, differentiation, histological grade, and resection status) between recurrence and non-recurrence groups. Significant differences (P<0.001) are annotated above the corresponding indicators. |
Association Between SRF Expression and MVD
In the studied cohort, glioblastomas with SRF expression displayed substantially elevated MVD values (86.79 ± 14.12 vessels/field) compared with those lacking SRF expression (70.58 ± 8.77; P < 0.05). Spearman’s rank correlation confirmed a strong positive relationship between SRF positivity and MVD (r = 0.749, P < 0.05), supporting the notion that SRF upregulation contributes to increased vascular density.
SRF Expression in Relation to Clinical Features and Recurrence
Within the 12-month follow-up period, 24 patients (26.1%) developed tumor recurrence. Comparative analysis of clinical and pathological characteristics (Table 2) revealed no significant group differences in age, sex, BMI, KPS score, or tumor location (all P > 0.05). However, recurrence was strongly associated with unfavorable features: all recurrent cases were SRF-positive (100% vs 41.2% in non-recurrent, P < 0.001). Additionally, larger tumor size (≥5 cm: 87.5% vs 29.4%, P < 0.001), poor differentiation (91.7% vs 22.1%, P < 0.001), high histological grade (95.8% vs 25.0%, P < 0.001), and incomplete resection (100% vs 54.4%, P < 0.001) were more frequent in the recurrence group. These results suggest that SRF expression, along with aggressive pathological features, is enriched in patients prone to recurrence.
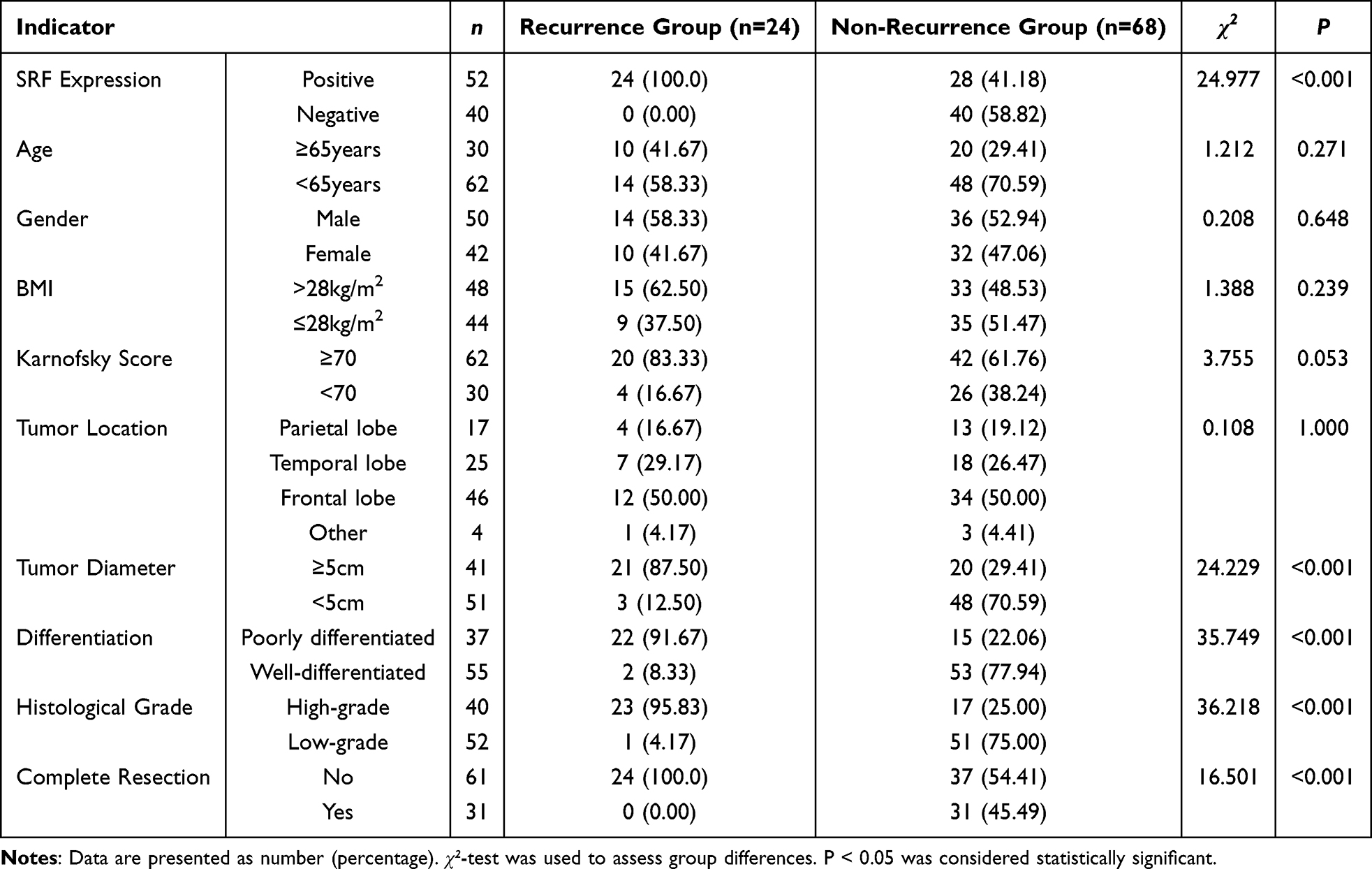 |
Table 2 Association of SRF Expression with Clinical and Pathological Features in Recurrent Versus Non-Recurrent Glioma Patients [n (%)] |
Independent Predictors of Postoperative Recurrence
Multivariate logistic regression, incorporating all significant univariate variables, identified several independent risk factors for recurrence (Table 3). These included SRF positivity (OR = 2.358, 95% CI: 1.395–3.988, P = 0.001), tumor diameter ≥5 cm (OR = 2.591, 95% CI: 1.500–4.476, P = 0.001), poor differentiation (OR = 2.545, 95% CI: 1.343–4.821, P = 0.004), high histological grade (OR = 2.489, 95% CI: 1.455–4.259, P = 0.001), and incomplete surgical removal (OR = 3.077, 95% CI: 1.528–6.219, P = 0.002). Each of these parameters significantly increased the likelihood of recurrence (Figure 2).
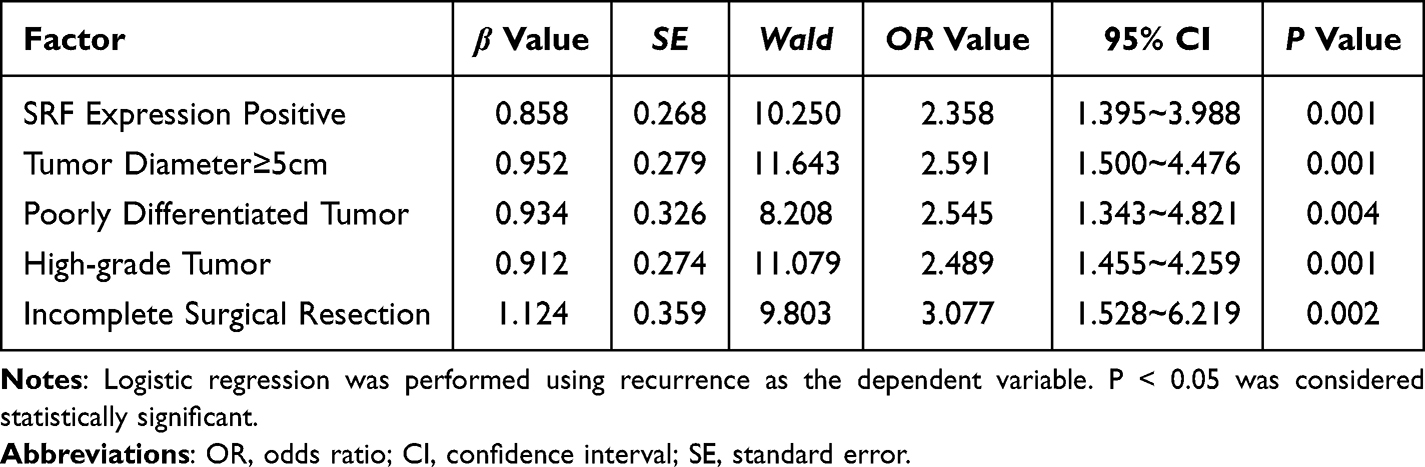 |
Table 3 Multivariate Logistic Regression Analysis of Factors Associated with Postoperative Recurrence in Glioma Patients (n) |
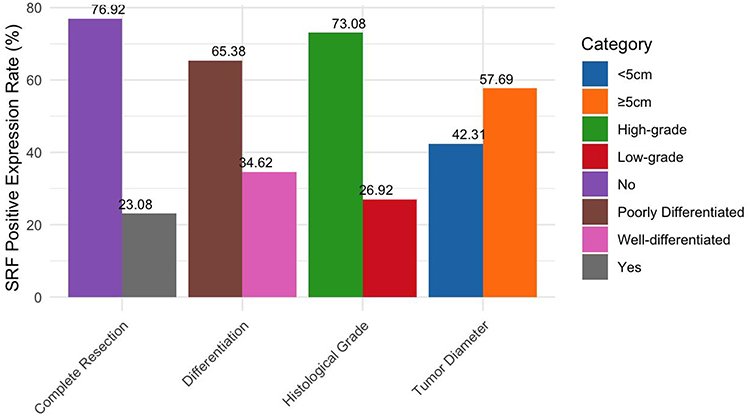 |
Figure 2 Distribution of SRF Positivity Across Pathological Characteristics in Glioma Patients. Notes: This grouped bar plot illustrates the SRF positive expression rates (%) for different pathological features in glioma patients, including Tumor Diameter (≥5cm vs <5cm), Differentiation (Poorly vs Well-differentiated), Histological Grade (High-grade vs Low-grade), and Complete Resection (No vs Yes). Each bar represents the percentage of SRF positive expression within the respective category, with statistical significance indicated by p-values (Tumor Diameter: p=0.004, Differentiation: p<0.001, Histological Grade: p=0.003, Complete Resection: p=0.014). Data is derived from a cohort of 92 patients. |
In addition, SRF expression showed clear correlations with aggressive tumor behavior (Table 4). Tumors expressing SRF were more frequently larger in size (≥5 cm: 57.7% vs 42.3%, P = 0.004), poorly differentiated (65.4% vs 34.6%, P < 0.001), of higher grade (73.1% vs 26.9%, P = 0.003), and incompletely resected (76.9% vs 23.1%, P = 0.014). These associations underscore SRF’s link to glioblastoma malignancy and are further illustrated in Figure 3.
 |
Table 4 Association of SRF Expression with Clinicopathological Characteristics in Glioma Patients [n (%)] |
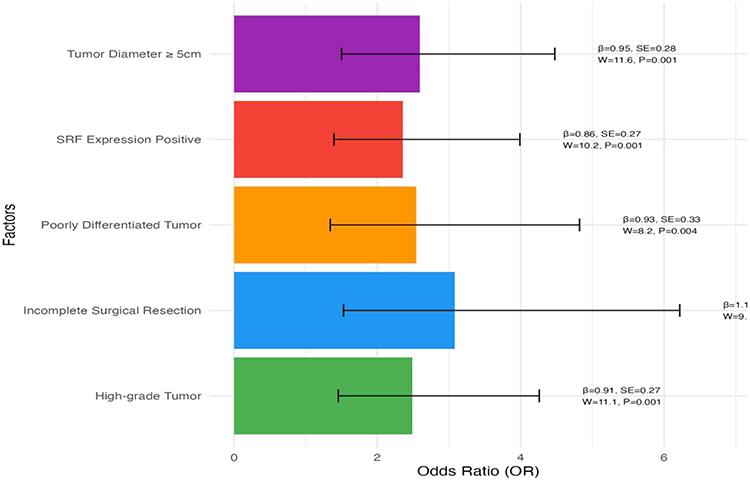 |
Figure 3 Forest plot of odds ratios for predictors of postoperative recurrence in glioma patients. Notes: Bar plot illustrating the Odds Ratios (OR) with 95% Confidence Intervals (CI) for factors associated with postoperative recurrence in glioma patients. Each bar represents a factor, with annotations indicating the regression coefficient (β), standard error (SE), Wald statistic (W), and P-value. Data derived from a multivariate analysis of glioma patient outcomes (n=not specified). The plot uses a white background for clarity, with distinct colors for each factor to enhance visual differentiation. |
Discussion
Glioblastoma remains a highly lethal malignancy, largely due to its infiltrative growth pattern and high propensity for recurrence. In our cohort, SRF expression was markedly elevated in glioblastoma tissues compared with adjacent non-tumorous brain. Moreover, SRF-positive tumors displayed significantly greater microvascular density, and statistical analysis confirmed a strong positive correlation between SRF expression and MVD.16,17 These observations suggest that SRF may contribute to tumor angiogenesis in GBM. Previous studies provide biological support for this role: SRF in mural cells has been shown to regulate vascular organization and hemodynamics.18–21 By activating downstream genes that modulate endothelial activity and vascular proliferation, SRF may enhance angiogenic potential, thereby driving tumor expansion and invasiveness.22,23
After one year of follow-up, 26.1% of patients experienced recurrence. Consistent with its role in progression, SRF positivity was universal in recurrent tumors, while only 41.2% of non-recurrent tumors expressed SRF (P < 0.001). Logistic regression further established SRF positivity as an independent predictor of recurrence. Other significant predictors included tumor diameter ≥5 cm, poor cellular differentiation, advanced histological grade, and incomplete resection. Although the 5 cm cutoff might appear somewhat arbitrary, it is widely recognized in neuro-oncology for its prognostic implications and practical surgical relevance. Notably, this threshold was also close to the median size of tumors in our cohort, making it both clinically and statistically reasonable. Nonetheless, larger multicenter studies may consider alternative stratification cutoffs. These clinical risk factors collectively represent tumor aggressiveness: larger and poorly differentiated lesions carry higher malignant potential, and residual tumor cells left after incomplete resection readily promote regrowth.10,23–26 The close association between SRF expression and these adverse features underscores its potential role as a driver of aggressive tumor biology.
From a mechanistic standpoint, SRF likely influences glioblastoma progression through several biological processes. One key pathway is epithelial–mesenchymal transition (EMT), in which SRF regulates cytoskeletal and adhesion molecules.27–30 For example, SRF activation promotes β-catenin translocation into the nucleus and upregulates cyclin D1, while repressing E-cadherin, thereby enhancing motility and proliferation.6,17,31–33 In gliomas, SRF-driven EMT and angiogenic programs may allow residual cells to migrate and stimulate neovascularization, fostering recurrence. The observed association between SRF overexpression and increased angiogenesis supports this hypothesis, as SRF may upregulate angiogenic mediators such as VEGF or matrix metalloproteinases, reshaping the microenvironment in favor of tumor growth.34–38
Emerging data also link SRF to mesenchymal transition and therapeutic resistance. For instance, SRF promotes EMT by modulating microRNA expression and cytoskeletal remodeling in other solid tumors, accelerating metastatic spread.39,40 Single-cell transcriptomic studies of recurrent glioblastoma have revealed mesenchymal-like subpopulations enriched in EMT-related genes (eg, EGR1, SERPINE1), which correlate with poor survival outcomes. Taken together, these findings imply that SRF not only promotes angiogenesis but also facilitates mesenchymal phenotypic transition, highlighting its multifaceted role in glioblastoma biology.
From a clinical perspective, these data suggest that SRF expression could serve as a prognostic marker. Patients with elevated SRF may have an increased likelihood of early recurrence and thus could benefit from intensified adjuvant therapies or closer clinical monitoring.36 Furthermore, SRF itself represents a potential therapeutic target; blocking SRF signaling may reduce angiogenesis and invasiveness, although no SRF-targeted agents are currently approved for GBM. Our findings provide a rationale for further translational research in this direction.
In addition to angiogenesis, systemic inflammation has been recognized as a major contributor to glioblastoma recurrence and progression. Recent studies41 reported that systemic inflammatory indices, such as neutrophil-to-lymphocyte ratio and systemic immune-inflammation index, correlate with tumor size and recurrence risk in high-grade gliomas. This raises the possibility that SRF-driven angiogenesis may act synergistically with systemic inflammatory pathways to create a permissive microenvironment for relapse. Although our study did not include inflammatory parameters, future work integrating SRF expression with systemic immune markers may yield more robust prognostic models.
Our study has several limitations. It was retrospective, single-center, and based on a relatively modest sample size. Follow-up was limited to one year, which restricts conclusions about long-term outcomes. Moreover, we did not explore the detailed signaling pathways by which SRF contributes to angiogenesis and recurrence. Importantly, molecular markers such as IDH mutation, MGMT promoter methylation, and ATRX status were not available, which prevented integration of SRF into the current WHO molecular classification system. This absence of molecular stratification may partly influence the interpretation of SRF’s prognostic role. Future multicenter studies with larger cohorts and molecular profiling are necessary to validate these findings and dissect the underlying mechanisms.
Conclusion
In conclusion, SRF expression was significantly upregulated in glioblastoma tissues compared to adjacent brain, and its expression was positively correlated with increased microvascular density. Elevated SRF expression was also linked with a higher risk of postoperative recurrence. These results suggest that SRF contributes to glioblastoma progression by promoting angiogenesis and aggressive tumor phenotypes. While SRF shows promise as a prognostic biomarker, these results are preliminary and based on a single-center retrospective analysis. Larger prospective studies incorporating molecular classification are needed to confirm its prognostic significance and clarify its biological role in glioblastoma recurrence and vascular remodeling.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Guangyuan Central Hospital.
Written informed consent was obtained from all participants before their involvement in the study.
Consent for Publication
All authors have read and approved the final manuscript and consent to the publication of the data in this study.
Acknowledgments
We would like to thank the Health Commission of Sichuan Province Medical Science and Technology Program and the Wu Jieping Medical Foundation for their financial support, and we appreciate the contributions of all authors. Their support and contributions were invaluable in completing this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Bo Tan and Shuangyin He contributed equally to this work and are co-first authors.
Funding
Health Commission of Sichuan Province Medical Science and Technology Program. (No.24WSXT042); Wu Jieping Medical Foundation. (No.320.6750.2024-6-113); Sichuan Provincial Clinical Key Specialty Construction project. (No.2024HSWKP001).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Chen X, Zheng Y, Zhang Q, et al. Dual-targeted delivery of temozolomide by multi-responsive nanoplatform via tumor microenvironment modulation for overcoming drug resistance to treat glioblastoma. J Nanobiotechnol. 2024;22(1):264. doi:10.1186/s12951-024-02531-3
2. Ramachandran M, Vaccaro A, van de Walle T, et al. Tailoring vascular phenotype through AAV therapy promotes anti-tumor immunity in glioma. Cancer Cell. 2023;41(6):1134–1151. doi:10.1016/j.ccell.2023.04.010
3. Wang J, Tang W, Yang M, et al. Inflammatory tumor microenvironment responsive neutrophil exosomes-based drug delivery system for targeted glioma therapy. Biomaterials. 2021;73(1):120784–120797. doi:10.1016/j.biomaterials.2021.120784
4. Bruno F, Pellerino A, Pronello E, et al. Elderly gliobastoma patients: the impact of surgery and adjuvant treatments on survival: a single institution experience. Brain Sci. 2022;12(5):632. doi:10.3390/brainsci12050632
5. Varela ML, Comba A, Faisal SM, et al. Gene therapy for high grade glioma: the clinical experience. Expert Opin Biol Ther. 2023;23(2):145–161. doi:10.1080/14712598.2022.2157718
6. Luo J, Pan M, Mo K, et al. Emerging role of artificial intelligence in diagnosis, classification and clinical management of glioma. Semin Cancer Biol. 2023;91:110–123. doi:10.1016/j.semcancer.2023.03.006
7. Romo CG, Piotrowski AF, Campian JL, et al. Clinical, histological, and molecular features of gliomas in adults with neurofibromatosis type 1. Neuro Oncol. 2023;25(8):1474–1486. doi:10.1093/neuonc/noad033
8. Matsumae M, Nishiyama J, Kuroda K. Intraoperative MR imaging during glioma resection. Magn Reson Med Sci. 2022;21(1):148–167. doi:10.2463/mrms.rev.2021-0116
9. Schaff LR, Mellinghoff IK. Glioblastoma and other primary brain malignancies in adults: a review. JAMA. 2023;329(7):574–587. doi:10.1001/jama.2023.0023
10. Elmarsafi T, Anghel EL, Sinkin J, et al. Risk factors associated with major lower extremity amputation after osseous diabetic charcot reconstruction. J Foot Ankle Surg. 2019;58(2):295–300. doi:10.1053/j.jfas.2018.08.059
11. Bending D, Pesenacker AM, Ursu S, et al. Hypomethylation at the regulatory T cell-specific demethylated region in CD25hi T cells is decoupled from FOXP3 expression at the inflamed site in childhood arthritis. J Immunol. 2014;193(6):2699–2708. doi:10.4049/jimmunol.1400599
12. Azam H, Pierro L, Reina M, et al. Emerging role for the serum response factor (SRF) as a potential therapeutic target in cancer. Expert Opin Ther Targets. 2022;26(2):155–169. doi:10.1080/14728222.2022.2032652
13. Onuh JO, Qiu H. Serum response factor-cofactor interactions and their implications in disease. FEBS J. 2021;288(10):3120–3134. doi:10.1111/febs.15544
14. Saffar H, Mirzaii M, Mirzaian E, et al. Assessment of micro-vessel density in brain glioma by CD105 expression. Iran J Pathol. 2018;13(2):205–211.
15. Villa C, Miquel C, Mosses D, et al. The 2016 world health organization classification of tumours of the central nervous system. Presse Med. 2018;47(11–12 Pt 2):e187–e200. doi:10.1016/j.lpm.2018.04.015
16. National Health Commission of the People’s Republic of China. Diagnostic and therapeutic guidelines for glioma (2018 edition). Chin J Neurol Surg. 2019;35(3):217–239.
17. Prencipe M, Fabre A, Murphy TB, et al. Role of serum response factor expression in prostate cancer biochemical recurrence. Prostate. 2018;78(10):724–730. doi:10.1002/pros.23516
18. Eichten A, Adler AP, Cooper B, et al. Rapid decrease in tumor perfusion following VEGF blockade predicts long-term tumor growth inhibition in preclinical tumor models. Angiogenesis. 2013;16(2):429–441. doi:10.1007/s10456-012-9328-3
19. Li T, Li J, Chen Z, et al. Glioma diagnosis and therapy: current challenges and nanomaterial-based solutions. J Control Release. 2022;352:338–370. doi:10.1016/j.jconrel.2022.09.065
20. Samuel N, Harmsen IE, Ding MYR, et al. Investigation of neurophysiologic and functional connectivity changes following glioma resection using magnetoencephalography. Neurooncol Adv. 2023;5(1):vdad091. doi:10.1093/noajnl/vdad091
21. Wang GM, Cioffi G, Patil N, et al. Importance of the intersection of age and sex to understand variation in incidence and survival for primary malignant gliomas. Neuro Oncol. 2022;24(2):302–310. doi:10.1093/neuonc/noab199
22. Zhang S, Cheng L, Su Y, et al. AGBL4 promotes malignant progression of glioblastoma via modulation of MMP-1 and inflammatory pathways. Front Immunol. 2024;15:1420182. doi:10.3389/fimmu.2024.1420182
23. Nie D, Ling Y, Lv W, et al. In situ attached photothermal immunomodulation-enhanced nanozyme for the inhibition of postoperative malignant glioma recurrence. ACS Nano. 2023;17(14):13885–13902. doi:10.1021/acsnano.3c03696
24. Chen CF, Chen B, Yang SJ, et al. MRI-based perfusion imaging histogram features for predicting recurrence of high-grade gliomas. Chin J Pract Neurol Dis. 2024;27(6):668–673.
25. Setlai BP, Hull R, Reis RM, et al. MicroRNA interrelated epithelial-mesenchymal transition (EMT) in glioblastoma. Genes. 2022;13(2):244. doi:10.3390/genes13020244
26. Wang J, Zhong Q, Zhang H, et al. Nogo-B promotes invasion and metastasis of nasopharyngeal carcinoma via RhoA-SRF-MRTFA pathway. Cell Death Dis. 2022;13(1):76. doi:10.1038/s41419-022-04518-0
27. Kuchler O, Gerlach J, Vomhof T, et al. Single-molecule tracking (SMT) and localization of SRF and MRTF transcription factors during neuronal stimulation and differentiation. Open Biol. 2022;12(5):210383. doi:10.1098/rsob.210383
28. Dinsmore CJ, Soriano P. Differential regulation of cranial and cardiac neural crest by serum response factor and its cofactors. Elife. 2022;11:e75106. doi:10.7554/eLife.75106
29. Xu M, Zhu F, Yin Q, et al. Serum response factor-regulated IDO1/Kyn-Ahr pathway promotes tumorigenesis of oral squamous cell carcinoma. Cancers. 2023;15(4):1319. doi:10.3390/cancers15041319
30. Yin J, Lv X, Hu S, et al. Overexpression of serum response factor is correlated with poor prognosis in patients with gastric cancer. Hum Pathol. 2019;85:10–17. doi:10.1016/j.humpath.2018.10.018
31. Jaiswal R, Goel MM, Mishra A. Microvessel density (cluster of differentiation-34 & vascular endothelial growth factor) in nasopharyngeal angiofibroma: clinical correlation. Int J Pediatr Otorhinolaryngol. 2023;174:111746. doi:10.1016/j.ijporl.2023.111746
32. Orlich MM, Diéguez-Hurtado R, Muehlfriedel R, et al. Mural cell SRF controls pericyte migration, vessel patterning, and blood flow. Circ Res. 2022;131(4):308–327. doi:10.1161/CIRCRESAHA.122.321109
33. Song T, Wang D, Zhang Y, et al. Effects of glutamine synthetase on neovascularization in glioma: in vivo mr vessel size imaging and histology. Curr Med Imaging. 2024;20(1):e15734056287859. doi:10.2174/0115734056287859240319062720
34. Liu D, Liu W. Diagnostic effect of MRI diffusion-weighted imaging apparent diffusion coefficient value on postoperative recurrence of brain glioma. Altern Ther Health Med. 2023;27:AT9342.
35. Qiang M, Zhen Y, Hao C, et al. Correlation between serum miR-27b-3p levels and postoperative recurrence in brain glioma patients. Chin J Pract Neurol Dis. 2023;26(11):1321–1325.
36. Eng C, Zhu Y, Li Y, et al. Recurrence-and malignant progression-associated biomarkers in low-grade gliomas and their roles in immunotherapy. Front Immunol. 2022;13:899710. doi:10.3389/fimmu.2022.899710
37. Qiao W, Wang Y, Luo C, et al. Development of preoperative and postoperative models to predict recurrence in postoperative glioma patients: a longitudinal cohort study. BMC Cancer. 2024;24(1):274. doi:10.1186/s12885-024-11996-2
38. Haixia H, Yubao D, Xiaohua W, et al. Expression of snail and SRF in human malignant glioma and their relationship with microvessel density. Chin J Lab Diagn. 2014;18(7):1092–1093.
39. Tian Y, Li J, Cai X, et al. Molecular drivers of epithelial-mesenchymal transition (EMT) in glioblastoma and impact on therapy resistance. Pathol Res Pract. 2025;272:156111. PMID: 40651122. doi:10.1016/j.prp.2025.156111
40. Li J, Long S, Zhang Y, et al. Single-cell transcriptome sequencing reveals new epithelial-stromal associated mesenchymal-like subsets in recurrent gliomas. Acta Neuropathol Commun. 2025;13(1):127. doi:10.1186/s40478-025-02036-6
41. Satragno C, Schiavetti I, Cella E, et al. Systemic inflammatory markers and volume of enhancing tissue on post-contrast T1w MRI images in differentiating true tumor progression from pseudoprogression in high-grade glioma. Clin Transl Radiat Oncol. 2024;49:100849. doi:10.1016/j.ctro.2024.100849
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.