Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Serum IL-33/ST2 Axis Expression in Acute Exacerbations of COPD: Correlation with Pulmonary Function
Authors Wei Y, Ling L, Zhu H, Huang Q
Received 24 December 2024
Accepted for publication 8 April 2025
Published 23 July 2025 Volume 2025:20 Pages 2581—2587
DOI https://doi.org/10.2147/COPD.S514152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Yan Wei,1 Liu Ling,1 Hongping Zhu,2 Qinrong Huang1
1Department of Respiratory and Critical Care Medicine, Guangyuan First People’s Hospital, Guangyuan, Sichuan, 628000, People’s Republic of China; 2Department of Cardiovascular, Guangyuan First People’s Hospital, Guangyuan, Sichuan, 628000, People’s Republic of China
Correspondence: Qinrong Huang, Department of respiratory and critical care medicine, Guangyuan First People’s Hospital, Guangyuan, Sichuan, 628000, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) exacerbations significantly contribute to morbidity and mortality. Identifying biomarkers linked to disease severity can enhance COPD management. This study investigates the relationship between serum IL-33 and ST2 levels and reduced pulmonary function during acute exacerbations of COPD (AECOPD).
Methods: We conducted a cross-sectional analysis of 194 AECOPD patients assessing IL-33 and ST2 serum levels and their associations with pulmonary function parameters. Patients were stratified into subgroups by age, gender, and the presence of pulmonary hypertension (PH) to explore differential biomarker impacts.
Results: IL-33 and ST2 levels demonstrated significant inverse correlations with FEV1% predicted (IL-33: r = − 0.561, ST2: r = − 0.545, p < 0.001) and the FEV1/FVC ratio. Logistic regression confirmed IL-33 (OR = 1.32, p < 0.001) and ST2 (OR = 1.29, p < 0.001) was associated with reduced pulmonary function. Subgroup analysis revealed more pronounced associations in older patients (≥ 67 years), males, and those with PH.
Conclusion: IL-33 and ST2 are promising biomarkers for identifying individuals at higher risk of reduced pulmonary function during AECOPD. Their utility is particularly significant in specific demographics, emphasizing the need for integrated biomarker-guided COPD management strategies.
Keywords: AECOPD, IL-33, ST2, pulmonary function
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent and progressive respiratory disorder, imposing a significant global health burden. Characterized by airflow limitation and chronic inflammation, COPD is exacerbated by exposure to noxious particles or gases, notably tobacco smoke. It affects over 250 million individuals worldwide and is predicted to become the third leading cause of death by 2030.1 Acute exacerbations of COPD (AECOPD) significantly contribute to disease progression, morbidity, and mortality, worsening symptoms and leading to frequent hospitalizations.2
AECOPD triggers complex inflammatory responses, including immune cell activation and pro-inflammatory cytokine release. In animal experiments, the IL-33/ST2 axis, a key immune response component, has been implicated in COPD exacerbations.3 IL-33, a cytokine expressed in barrier tissues like the lungs, activates the ST2 receptor on immune cells, inducing inflammation and tissue remodeling, which was assessed in vitro epithelial damage assays and three-dimensional, air-liquid interface cell culture models.4 This interaction is implicated in various diseases, including COPD. The ST2 receptor exists in membrane-bound (ST2L) and soluble (sST2) forms, with sST2 potentially modulating inflammation by inhibiting IL-33 signaling.5 Elevated IL-33 and ST2 levels have been associated with COPD pathogenesis, particularly during exacerbations.6
Despite the growing recognition of IL-33 and ST2 in COPD, their exact role in AECOPD remains unclear. Studies suggest that the IL-33/ST2 axis influences immune cell recruitment and cytokine production, potentially exacerbating airway inflammation and lung function decline.7 The soluble form of ST2 (sST2) may serve as a biomarker for predicting exacerbations, correlating with disease severity and pulmonary function decline.8 However, the relationship between serum IL-33/ST2 expression and pulmonary function impairment in AECOPD requires further clarification.
This study aims to investigate the serum expression levels of IL-33 and ST2 in AECOPD patients and their correlation with pulmonary function parameters. We hypothesize that elevated serum IL-33 and ST2 levels will correlate with worsened lung function in AECOPD patients. By assessing these biomarkers, we aim to enhance our understanding of the IL-33/ST2 axis’s role in AECOPD and explore its potential as a clinical biomarker for exacerbation severity.
Methods
Study Design and Participants
This was a cross-sectional observational study conducted at our hospital between January 2022 and January 2024. The primary objective of this study was to evaluate the serum expression levels of IL-33 and ST2 in patients experiencing AECOPD, and to investigate their correlation with pulmonary function.
Patients were recruited from the respiratory medicine outpatient and inpatient departments. Inclusion criteria were: (1) COPD diagnosis and severity staging were based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2022 guidelines,9 (2) age ≥40 years, (3) a smoking history of at least 10 pack-years, (4) presence of an AECOPD, defined by the presence of increased dyspnea, cough, or sputum production, and (5) informed consent to participate.
Exclusion criteria included: (1) concomitant pulmonary diseases such as asthma, bronchiectasis, or interstitial lung disease, (2) active cancer or other life-threatening comorbidities, (3) immunosuppressive therapy, and (4) participation in other clinical trials.
Data Collection
Baseline demographic and clinical data were collected, including age, gender, smoking history, COPD exacerbation history, and comorbid conditions. Disease severity was assessed using the GOLD staging system, and patients were classified into GOLD stages I–IV based on their post-bronchodilator forced expiratory volume in 1 second (FEV1) as a percentage of predicted values.
Predicted FEV1 values were calculated using the Global Lung Function Initiative (GLI) 2012 reference equations, which account for age, sex, height, and ethnicity. To align with our study population (Chinese adults), a correction factor of 0.88 was applied to the GLI reference values, as recommended for East Asian populations.10 Patients were classified into GOLD stages I–IV using post-bronchodilator spirometry: GOLD I (Mild): FEV1 ≥80% predicted. GOLD II (Moderate): 50% ≤ FEV1 <80% predicted. GOLD III (Severe): 30% ≤ FEV1 <50% predicted. GOLD IV (Very Severe): FEV1 <30% predicted.9
Pulmonary function was assessed using spirometry, and the following parameters were recorded: FEV1, forced vital capacity (FVC), and the FEV1/FVC ratio.
Blood Sample Collection and Biomarker Measurement
Peripheral venous blood samples were obtained from each participant at the time of hospital admission during an AECOPD episode. Blood samples were processed within 30 minutes of collection. Serum was separated by centrifugation at 3000 rpm for 10 minutes and stored at −80°C until further analysis.
The levels of IL-33 and ST2 in the plasma samples were determined using enzyme-linked immunosorbent assay (ELISA) kits. The Human IL-33 ELISA Kit and Human ST2/IL-33 R ELISA Kit were utilized for the quantitative detection of IL-33 and ST2, respectively. The assays were performed according to the manufacturer’s instructions.
Statistical Analysis
The normality of continuous variables (eg, IL-33, ST2, FEV1% predicted) was formally assessed using the Shapiro–Wilk test (α = 0.05). Variables with a Shapiro–Wilk p-value > 0.05 were considered normally distributed. Descriptive statistics were used to summarize patient characteristics, including means ± standard deviation for continuous variables and percentages for categorical variables. Comparisons between groups were made using the independent t-test.
Pearson’s correlation coefficient was used to assess the linear relationships between serum IL-33/ST2 levels and pulmonary function parameters (eg, FEV1% predicted, FEV1/FVC ratio). A p-value <0.05 was considered statistically significant. Patients were divided into two groups based on the median FEV1% predicted value of our study population. Multiple logistic regression analysis was performed to evaluate the potential impact of IL-33 and ST2 on pulmonary function (FEV1% predicted), adjusting for potential confounders including age, sex, smoking history, and GOLD stage. To explore the nuanced relationships between IL-33/ST2 levels and pulmonary function, we divided patients into subgroups based on age (grouped by median), gender, and the presence of pulmonary hypertension.
All analyses were performed using SPSS software version 25.0 (IBM Corporation, Armonk, NY, USA).
Results
Clinical Characteristics
The study included 194 patients experiencing AECOPD. The mean age was 67.2 ± 8.5 years, with 156 males (80.4%). All participants smoked with a mean smoking index of 44.3 ± 12.1 pack-years. Baseline disease severity was evaluated using the GOLD criteria: 50 (25.8%) were in stage II (Moderate), 88 (45.4%) in stage III (Severe), and 56 (28.9%) in stage IV (Very Severe). Common comorbidities included hypertension in 84 patients (43.3%), diabetes in 52 (26.8%), and pulmonary hypertension in 45 (23.2%). The mean C-reactive protein (CRP) level was 28.7 ± 7.9 mg/L, and white blood cell (WBC) count was 9.7 ± 2.8 × 10^9/L. Detailed baseline characteristics are presented in Table 1.
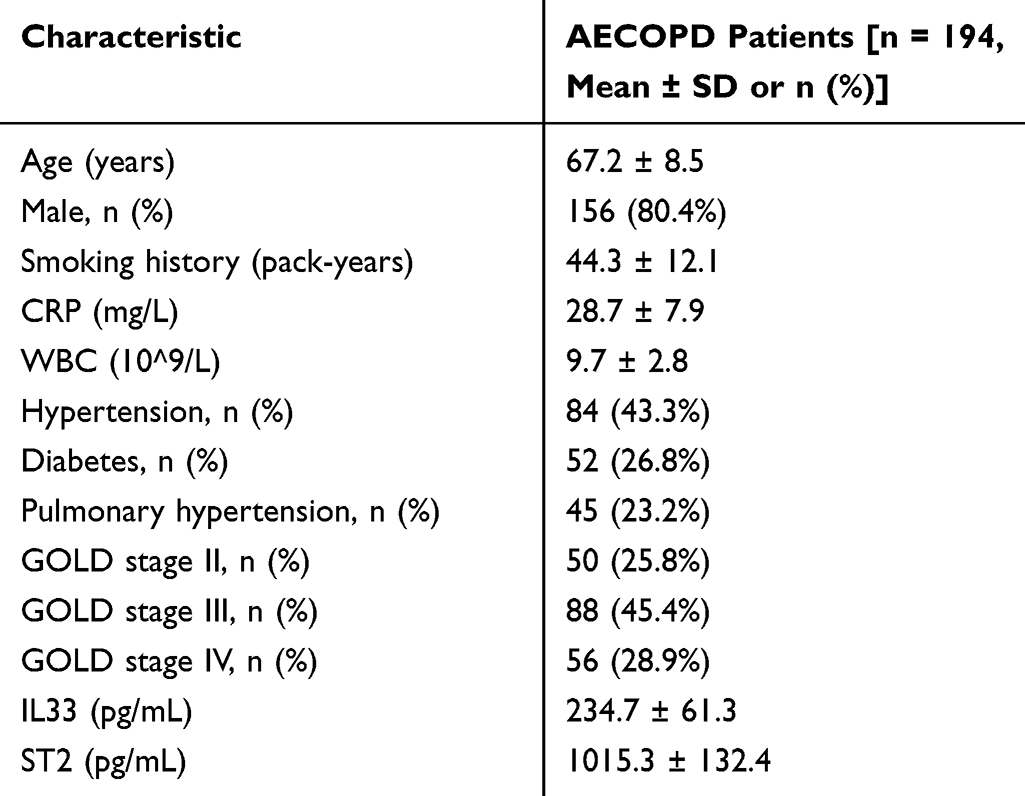 |
Table 1 Clinical Characteristics of the Study Population |
Correlation Between IL-33, ST2 Levels and Pulmonary Function
IL-33 and ST2 levels exhibited significant inverse correlations with pulmonary function parameters. Specifically, IL-33 correlated negatively with FEV1% predicted (r = −0.561, p < 0.001) and FEV1/FVC ratio (r = −0.525, p < 0.001). Similarly, ST2 showed negative correlations with FEV1% predicted (r = −0.545, p < 0.001) and FEV1/FVC ratio (r = −0.498, p < 0.001).
Comparison by Lung Function Using Median Split
Based on the cohort’s median FEV1% predicted (41%), patients were stratified into “low FEV1” (≤41%, n=97) and “high FEV1” (>41%, n=97) groups. Compared to the higher FEV1 group, the lower FEV1 group had significantly higher levels of serum IL-33 (256.1 ± 63.4 pg/mL vs 213.3 ± 55.7 pg/mL, p < 0.001) and ST2 (1087.4 ± 137.9 pg/mL vs 943.6 ± 126.5 pg/mL, p < 0.001). Moreover, the lower FEV1 group exhibited higher CRP levels and a greater prevalence of pulmonary hypertension (p < 0.05). Baseline characteristic comparisons are detailed in Table 2.
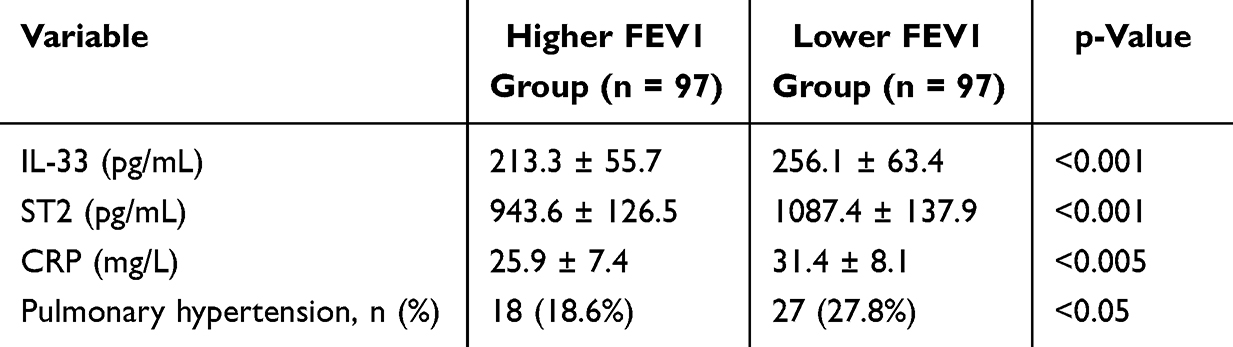 |
Table 2 Comparison of Baseline Characteristics and Biomarkers by FEV1% Predicted Group |
Association Between IL-33/ST2 Levels and Reduced Lung Function
After adjusting for age, sex, smoking status, CRP, and comorbidities, both IL-33 (odds ratio [OR] = 1.32, 95% CI: 1.15–1.51, p < 0.001) and ST2 levels (OR = 1.29, 95% CI: 1.12–1.48, p < 0.001) were significantly associated with a lower FEV1 group.
Association in Patients with Pulmonary Hypertension, Male and Older Ages
In the elderly subgroup (≥67 years), elevated IL-33 and ST2 levels were significantly associated with reduced FEV1% predicted, serving as robust predictors of impaired pulmonary function (IL-33: OR=1.38, 95% CI: 1.22–1.55, p<0.001; ST2: OR=1.31, 95% CI: 1.16–1.47, p<0.001). No statistically significant association was observed in the younger subgroup (IL-33: OR=1.25, p=0.21; ST2: OR=1.19, p=0.11).
Among male patients, IL-33 and ST2 levels correlated significantly with decreased lung function (IL-33: OR=1.32, 95% CI: 1.18–1.49, p<0.001; ST2: OR=1.27, 95% CI: 1.13–1.43, p<0.001). Female patients showed no statistically significant correlation (IL-33: OR=1.15, p=0.06; ST2: OR=1.11, p=0.55), indicating gender-based differences in biomarker relevance.
In patients with pulmonary hypertension, IL-33 and ST2 were markedly associated with reduced FEV1% predicted (IL-33: OR=1.50, 95% CI: 1.30–1.72, p<0.001; ST2: OR=1.45, 95% CI: 1.26–1.67, p<0.001). Conversely, in patients without PH, neither IL-33 (OR=1.10, p=0.12) nor ST2 (OR=1.08, p=0.15) showed significant predictive value.
Subgroup analyses highlight IL-33 (Table 3) and ST2 (Table 4) as compelling biomarkers for predicting lung function decline, particularly in older, male patients, and those with pulmonary hypertension.
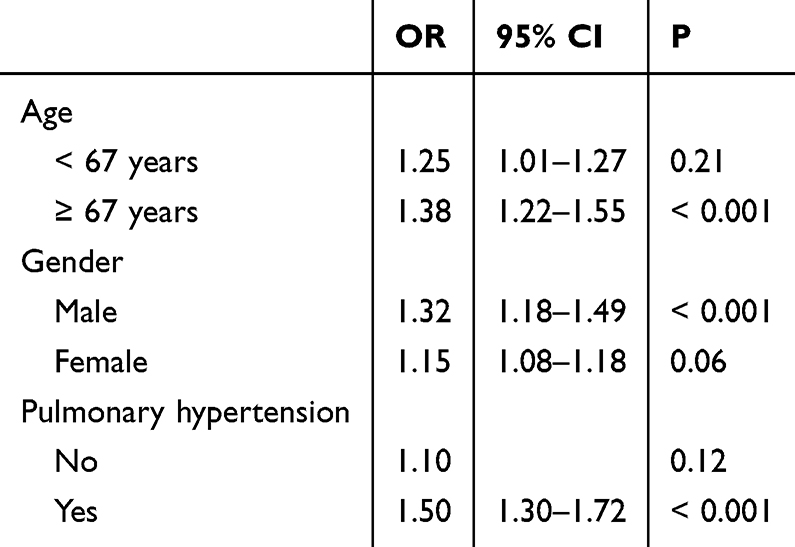 |
Table 3 Association Between IL 33 and Reduced Lung Function in Subgroups |
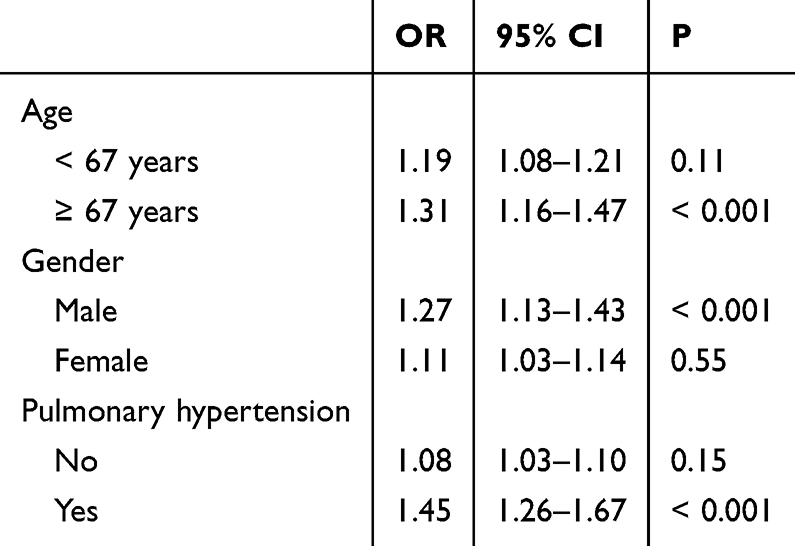 |
Table 4 Association Between ST 2 and Reduced Lung Function in Subgroups |
Discussion
This study investigated the significance of IL-33 and ST2 levels in patients experiencing AECOPD. Our findings suggest that elevated serum levels of IL-33 and ST2 are associated with reduced lung function in patients experiencing AECOPD, particularly among older patients, males, and those with concurrent pulmonary hypertension. These observations highlight IL-33 and ST2’s potential as critical indicators in managing COPD exacerbations.
Our results align with prior studies implicating the IL-33/ST2 axis in COPD pathogenesis. For example, Tworek et al reported IL-33 was involved in the development of eosinophilic airway inflammation in non-atopic COPD patients,11 and Byers. (2013) reported long-term IL-33 production by epithelial progenitor cells in chronic obstructive pulmonary disease.12 The high expression of IL-33 in the lung tissue of COPD patients was strongly correlated with the severity of the disease.13,14 We observed that IL-33 and ST2 levels correlated inversely with pulmonary function markers such as FEV1% predicted and the FEV1/FVC ratio. This inverse relationship suggests that IL-33 and ST2 could act as inflammatory mediators exacerbating lung function deterioration during acute exacerbations of COPD. The subgroup analyses further demonstrated that specific populations, namely older adults, males, and individuals with pulmonary hypertension (PH), show stronger associations between these biomarkers and lung function decline. Our results align with previous studies emphasizing the role of IL-33 in chronic inflammatory conditions, including asthma and COPD.15 IL-33’s ability to enhance immune responses by interacting with the ST2 receptor has been documented, supporting its role as a marker of inflammation.16 The current study builds on this by highlighting ST2’s specific involvement in COPD and suggesting additional application areas, particularly in AECOPD.17 Moreover, studies on PH have hinted at inflammatory pathways that might relate IL-33 and ST2 to vascular dysregulation, potentially explaining our findings regarding PH.18,19
The mechanistic pathways involved likely include IL-33’s activation of innate lymphoid cells, which can amplify Type 2 immune responses and exacerbate airway inflammation.20 This pathway not only worsens respiratory symptoms but may also lead to structural alterations in the lung parenchyma and vasculature, particularly in severe COPD cases and those complicated by PH.21–23 The lack of statistically significant associations in female patients may reflect hormonal influences or differing environmental exposures, such as smoking.24,25
The subgroup analysis underscored the pronounced impact of IL-33 and ST2 in older, male patients, and those with pulmonary hypertension, likely due to cumulative inflammatory insults and compromised vasculature.26 The more substantial association in males might reflect traditional risk factor exposure patterns, as occupational and smoking histories are significant contributors to COPD progression in this group.27,28 From a clinical standpoint, these results suggest that monitoring IL-33 and ST2 levels in these high-risk populations could provide valuable insights into disease trajectory and treatment responsiveness.
The strong association between IL-33/ST2 and reduced FEV1 during AECOPD suggests these biomarkers could aid in risk stratification. For instance, elevated IL-33/ST2 levels may identify patients at higher risk of rapid functional decline, enabling targeted interventions such as earlier escalation of anti-inflammatory therapies (eg, corticosteroids or IL-33 inhibitors under investigation). This aligns with Sanofi (2023), who proposed IL-33/ST2 as therapeutic targets in COPD.29 Furthermore, integrating these biomarkers into existing prognostic tools (eg, BODE index) may enhance personalized management strategies.
Despite these strengths, several limitations must be acknowledged. The study’s cross-sectional nature restricts our ability to infer causal relationships. Additionally, the sample was derived from a single center, which may limit generalizability. Moreover, biomarker levels were only assessed during exacerbations, precluding comparative analyses with stable disease states. Longitudinal studies are essential to determine whether these biomarkers can predict future exacerbations or track disease progression.
Future research should include diverse, multicenter cohorts to validate these findings across different populations. Investigating the potential role of IL-33/ST2 in mediating specific therapeutic responses could further enhance clinical application. Additionally, exploring personalized treatment strategies based on biomarker levels might improve management outcomes, particularly in addressing microvascular complications seen in comorbid conditions like PH.
Conclusion
In conclusion, IL-33 and ST2 may serve as potential biomarkers associated with reduced lung function in AECOPD, especially among older, male, and PH-afflicted individuals. Their role in inflammatory pathways pertinent to COPD suggests potential utility in clinical practice for identifying patients at high risk of exacerbations. By integrating these insights into patient care, healthcare providers can better tailor interventions to mitigate exacerbation impacts and optimize disease management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
This retrospective study was reviewed and granted exemption from formal ethical approval by the Institutional Review Board (IRB) of Guangyuan First People’s Hospital (Approval ID: GYFPH-IRB-2022-014). Patient consent for medical record review was waived by the IRB due to the anonymized and observational nature of the study, which posed no additional risk to participants. All data were handled in strict compliance with the Declaration of Helsinki, ensuring patient confidentiality through de-identification and secure storage protocols.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2017 report. Am J Respir Crit Care Med. 2017;195(5):557–563. doi:10.1164/rccm.201701-0218PP
2. Luo Z, Zhang W, Chen L, et al. Prognostic value of neutrophil: lymphocyte and platelet: lymphocyte ratios for 28-day mortality of patients with AECOPD. Int J Gen Med. 2021;14:2839–2848. doi:10.2147/IJGM.S312045
3. Gimenes JA, Srivastava V, ReddyVari H, et al. Rhinovirus-induces progression of lung disease in a mouse model of COPD via IL-33/ST2 signaling axis. Clin Sci. 2019;133(8):983–996. doi:10.1042/CS20181088
4. Strickson S, Houslay KF, Negri VA, et al. Oxidised IL-33 drives COPD epithelial pathogenesis via ST2-independent RAGE/EGFR signalling complex. Eur Respir J. 2023:62. doi:10.1183/13993003.02210-2022
5. Zhou Y, Xu Z, Liu Z. Role of IL-33-ST2 pathway in regulating inflammation: current evidence and future perspectives. J Transl Med. 2023;21. doi:10.1186/s12967-023-04782-4
6. Riera-Martínez L, Cànaves-Gómez L, Iglesias A, et al. The role of IL-33/ST2 in COPD and its future as an antibody therapy. Int J Mol Sci. 2023;24(10):8702. doi:10.3390/ijms24108702
7. Ma Q, Qian Y, Jiang J, et al. IL-33/ST2 axis deficiency exacerbates neutrophil-dominant allergic airway inflammation. Clin Transl Immunol. 2021;10. doi:10.1002/cti2.1300
8. Azazi E, Elshora A, Tantawy E, et al. Serum levels of Interleukin-33 and its soluble receptor ST2 in asthmatic patients. Egypt J Chest Dis Tu. 2024;63. doi:10.1016/j.ejcdt.2013.11.005
9. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2022 report. Available from: https://goldcopd.org/2022-gold-reports/.
10. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-year age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
11. Tworek D, Majewski S, Szewczyk K, et al. The association between airway eosinophilic inflammation and IL-33 in stable non-atopic COPD. Respir Res. 2018;19(108). doi:10.1186/s12931-018-0807-y
12. Byers DE, Alexander-Brett J, Patel AC, et al. Long term IL-33-producing epithelial progenitor cells in chronic obstructive lung disease. J Clin Investig. 2013;123:3967–3982. doi:10.1172/JCI65570
13. Kearley J, Silver JS, Sanden C, et al. Cigarette smoke silences innate lymphoid cell function and facilitates an exacerbated type I interleukin-33-dependent response to infection. Immunity. 2015;42:566–579. doi:10.1016/j.immuni.2015.02.011
14. Joo H, Park SJ, Min KH, et al. Association between plasma interleukin-33 level and acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm Med. 2021;21:86. doi:10.1186/s12890-021-01423-8
15. Xia J, Zhao J, Shang J, et al. Increased IL-33 expression in chronic obstructive pulmonary disease. Am J Physiol. 308;2015. doi:10.1152/ajplung.00305.2014
16. Shakerian L, Kolahdooz H, Garousi M, et al. IL-33/ST2 axis in autoimmune disease. Cytokine. 2022:158. doi:10.1016/j.cyto.2022.156015
17. Urban MH, Stojkovic S, Demyanets S, et al. Soluble ST2 and all-cause mortality in patients with chronic obstructive pulmonary disease-A 10-year cohort study. J Clin Med. 2021;11. doi:10.3390/jcm11010056
18. Geenen LW, Baggen VJM, Kauling RM, et al. The prognostic value of soluble ST2 in adults with pulmonary hypertension. J Clin Med. 2019;8:1517. doi:10.3390/jcm8101517
19. Indralingam CS, Gutierrez-Gonzalez AK, Johns SC, et al. IL-33/ST2 receptor-dependent signaling in the development of pulmonary hypertension in Sugen/hypoxia mice. Physiol Rep. 2022;10. doi:10.14814/phy2.15185
20. Barlow JL, Peel S, Fox J, et al. IL-33 is more potent than IL-25 in provoking IL-13-producing nuocytes (type 2 innate lymphoid cells) and airway contraction. J Allergy Clin Immun. 2013;132(4):933–941. doi:10.1016/j.jaci.2013.05.012
21. Li D, Guabiraba R, Besnard AG, et al. IL-33 promotes ST2-dependent lung fibrosis by the induction of alternatively activated macrophages and innate lymphoid cells in mice. J Allergy Clin Immun. 2014;134(6):1422–1432.e11. doi:10.1016/j.jaci.2014.05.011
22. Marashian SM, Mortaz E, Jamaati HR, et al. Role of innate lymphoid cells in lung disease. Iran J Allergy Asthm. 2015;14:346–60.PMID: 26547702.
23. Calderon AA, Dimond C, Choy DF, et al. Targeting interleukin-33 and thymic stromal lymphopoietin pathways for novel pulmonary therapeutics in asthma and COPD. Eur Respir Rev. 2023;32(167):220144. doi:10.1183/16000617.0144-2022
24. Draijer C, Hylkema MN, Boorsma CE, et al. Sexual maturation protects against development of lung inflammation through estrogen. Am J physiol. 2016;310;L166–74. doi:10.1152/ajplung.00119.2015
25. Grabicki M, Kuźnar-Kamińska B, Rubinsztajn R, et al. COPD course and comorbidities: are there gender differences? Adv Exp Med Biol. 2019:1113. doi:10.1007/5584_2018_160
26. Stone RA, Lowe D, Potter JM, et al. Managing patients with COPD exacerbation: does age matter? Age Ageing. 2012;41(4):461–468. doi:10.1093/ageing/afs039
27. Pallasaho P, Kainu A, Sovijärvi A, et al. Combined effect of smoking and occupational exposure to dusts, gases or fumes on the incidence of COPD. COPD. 2014;11(1):88–95. doi:10.3109/15412555.2013.830095
28. Fishwick D, Darby A, Hnizdo E, et al. COPD causation and workplace exposures: an assessment of agreement among expert clinical raters. COPD. 2013;10(2):172–179. doi:10.3109/15412555.2012.737072
29. Sanofi. A Phase 2a, Open-Label, Two-Part Study to Evaluate the Mechanism of Action of Itepekimab (Anti-IL-33 MAb) on Airway Inflammation in Patients with Chronic Obstructive Pulmonary Disease (COPD). Paris, France: Sanofi; 2023.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.