Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Serum Apolipoprotein B Levels and Apolipoprotein B/Apolipoprotein A1 Ratio as Predictors of Dyslipidemia Risk in Patients Treated with Second-Generation Antipsychotics: A Retrospective Cohort Study
Authors Zhang JX ![]() , Huang ZQ
, Huang ZQ ![]() , Yang JM, Wang WY, Li WN
, Yang JM, Wang WY, Li WN ![]()
Received 2 September 2025
Accepted for publication 21 November 2025
Published 8 December 2025 Volume 2025:21 Pages 2795—2804
DOI https://doi.org/10.2147/NDT.S564450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Jia-Xuan Zhang,1 Zhi-Qiang Huang,1 Jian-Ming Yang,2 Wen-Yong Wang,3 Wei-Na Li2
1Clinical Lab, Zhongshan Third People’s Hospital, Zhongshan, Guangdong, People’s Republic of China; 2Nanlang Outpatient Department, Zhongshan Third People’s Hospital, Zhongshan, Guangdong, People’s Republic of China; 3Department of Geriatric Mental Disorders, Zhongshan Third People’s Hospital, Zhongshan, Guangdong, People’s Republic of China
Correspondence: Wei-Na Li, Nanlang Outpatient Department, Zhongshan Third People’s Hospital, 80 Tianbian Main Street, Nanlang Subdistrict, Zhongshan, Guangdong, 528451, People’s Republic of China, Email [email protected]
Purpose: To assess the predictive ability of baseline serum apolipoprotein B (ApoB) and the ratio of ApoB to apolipoprotein A1 (ApoB/ApoA1 ratio) for dyslipidemia risk in patients receiving second-generation antipsychotics (SGAs).
Patients and Methods: Medical records of patients hospitalized between March 2019 and March 2025 were retrospectively reviewed. The optimal cut-off points for baseline serum ApoB levels and the ApoB/ApoA1 ratio were identified using a maximally selected log-rank statistic analysis. Multivariable Cox proportional hazards models estimated hazard ratios (HRs) with 95% confidence intervals (95% CIs). The Kaplan-Meier method with Log rank testing was used to compare the cumulative incidence of dyslipidemia between groups defined by these cut-off points.
Results: Of 311 enrolled patients, 33 (10.6%) lacking baseline ApoA1 measurements were excluded from ApoB/ApoA1 ratio analyses. The optimal cut-off points were 0.70 g/L for baseline ApoB and 0.45 for the ApoB/ApoA1 ratio. Multivariable Cox proportional hazards models, fully adjusted for covariates, demonstrated significantly elevated dyslipidemia risk for patients exceeding these thresholds vs low-risk groups: adjusted HR 2.98 (95% CI: 2.05– 4.32, p < 0.001) for high ApoB and 3.17 (95% CI: 1.62– 6.22, p = 0.001) for high ApoB/ApoA1 ratio. Continuous analysis showed each 0.1 g/L ApoB increase conferred a 34% higher risk (adjusted HR 1.34, 95% CI: 1.21– 1.48, p < 0.001), while each 0.1-unit ApoB/ApoA1 ratio increase conferred a 20% higher risk (adjusted HR 1.20, 95% CI: 1.10– 1.30, p < 0.001). Kaplan-Meier curves confirmed significantly higher cumulative dyslipidemia incidence in high vs low groups for both markers (Log rank test, both p < 0.001).
Conclusion: Baseline serum ApoB levels and the ApoB/ApoA1 ratio are valuable risk markers for dyslipidemia in patients treated with SGAs.
Keywords: ApoB, ApoB/ApoA1, metabolic risk, second-generation antipsychotics, biomarker, maximally selected log-rank
Introduction
Second-generation antipsychotics (SGAs), also known as atypical antipsychotics, are a class of medications, such as olanzapine, clozapine, risperidone, aripiprazole, and amisulpride. Compared with first-generation antipsychotics (FGAs), SGAs demonstrate superior efficacy, greater improvements in quality of life, and a reduced incidence of extrapyramidal side effects, making them the first-line treatments for various psychiatric disorders.1–3 However, treatment with SGAs is associated with the development of metabolic syndrome (MetS).4 The prevalence of MetS among patients treated with SGAs is 47.4%, which is significantly higher than that in first-episode patients and antipsychotic-naïve patients (both approximately 10%).5,6
Patients with MetS face double the cardiovascular disease (CVD) risk and a more than fivefold increased risk of diabetes within 5–10 years.7 In contrast, those with schizophrenia experience a 16- to 19-year reduction in life expectancy compared with the general population, with CVD being the leading cause of death.8,9 The pathogenesis of MetS is multifactorial, with dyslipidemia contributing to its development. Validated early-stage biomarkers for risk stratification of future dyslipidemia among patients receiving SGAs would allow pre-symptomatic intervention, thereby preventing the development of MetS. Nevertheless, such biomarkers are currently unavailable.
Apolipoproteins serve crucial regulatory roles in maintaining lipid metabolic homeostasis.10 Apolipoprotein A1 (ApoA1) is the main apolipoprotein component of high-density lipoprotein (HDL), which can promote the reverse transport of peripheral cholesterol to the liver, thereby exerting an anti-atherosclerotic effect.10 In contrast, apolipoprotein B (ApoB) is responsible for transporting cholesterol to peripheral tissues, which may enhance the formation of atherosclerotic thrombosis.11 The ratio of ApoB to ApoA1 (ApoB/ApoA1 ratio) can reflect the balance between pro-atherosclerotic factors and anti-atherosclerotic factors in plasma. Several studies have found that serum ApoB levels and the ApoB/ApoA1 ratio can predict the risk of developing metabolic diseases, even outperforming traditional biomarkers.12–15 However, to the best of our knowledge, no study has reported the predictive value of baseline serum ApoB levels and the ApoB/ApoA1 ratio for dyslipidemia risk associated with SGAs.
This study aimed to investigate the predictive value of baseline serum ApoB levels and the ApoB/ApoA1 ratio for the development of dyslipidemia within 4 months in patients initiating SGAs.
Materials and Methods
Study Population
This single-center retrospective cohort study was conducted at Zhongshan Third People’s Hospital in China, using medical records of patients hospitalized between March 2019 and March 2025. This study was approved by the Ethics Committee of the Zhongshan Third People’s Hospital (Ethics Approval No. SSYLL-KY-20231103). As a retrospective observational study with anonymized data, the ethics committee formally waived the requirement for informed consent in this study.
Inclusion criteria: (1) inpatients aged ≥18 years, (2) no antipsychotic treatment for at least 3 months prior to enrollment, (3) absence of dyslipidemia or hyperglycemia at admission.
Exclusion criteria: (1) endocrine disorders, severe hepatic/renal/cardiac/pulmonary dysfunction, autoimmune diseases, malignancies, allergies, or active infections, (2) use of glucocorticoids or medications for diabetes/dyslipidemia in the preceding 3 months, (3) pregnancy or lactation.
Variables
Data Collection
Demographic and clinical data were extracted from medical records, including: sex, age at admission, baseline weight, smoking status, psychiatric diagnosis (classified according to ICD-10 criteria), total cumulative dose and duration of SGA treatment, concomitant medications, baseline serum levels of ApoB and ApoA1, and serial serum lipid levels measured at baseline and monthly intervals for approximately four months post-admission. The follow-up period spanned from admission until the earliest occurrence of any of the following events: dyslipidemia diagnosis, hospital discharge, or the 4-month endpoint.
Laboratory Measurements
Overnight (≥ 8 hours) fasting venous blood samples were collected from participants. Serum glucose and apolipoprotein levels, along with lipid profiles (including the levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), HDL cholesterol (HDL-C), and triglycerides (TG)), were subsequently analyzed using a Beckman Coulter AU680 automated analytical system (Beckman Coulter, Inc., Fullerton, CA, USA). The instrument was used in strict accordance with protocols following daily quality control inspections.
Diagnostic Criteria
According to the Chinese guidelines for the prevention and treatment of dyslipidemia in adults (2016 revision),16 dyslipidemia was defined as meeting any of the following criteria: (1) TC ≥ 5.2 mmol/L, (2) LDL-C ≥ 3.4 mmol/L, (3) HDL-C < 1.0 mmol/L, or (4) TG ≥ 1.7 mmol/L; hyperglycemia was defined as fasting blood glucose (FBG) > 6.1 mmol/L.
SGA Metabolic Risk
SGAs were stratified into three metabolic risk categories:17 (1) high risk: olanzapine, clozapine; (2) intermediate risk: risperidone, paliperidone, quetiapine; (3) low risk: amisulpride, aripiprazole, ziprasidone, lurasidone. Consistent use of a single SGA was defined as SGA monotherapy, while SGA polytherapy referred to either a combination of multiple SGAs or a switch between SGAs. Patients receiving SGA polytherapy spanning multiple metabolic risk categories were classified into the highest corresponding metabolic risk tier covered by their regimen.
SGA Dosage Standardization
Individual SGA dosages were standardized into olanzapine-equivalent units using the World Health Organization’s Defined Daily Dose (DDD) methodology,18 with the following conversion ratios: 1 mg olanzapine = 30 mg clozapine = 0.5 mg risperidone = 0.6 mg paliperidone = 40 mg quetiapine = 40 mg amisulpride = 1.5 mg aripiprazole = 8 mg ziprasidone = 6 mg lurasidone. The average daily dose of SGA was derived from the total dose divided by the total days of treatment.
Concomitant Medication Classification
Concomitant medications were categorized into five pharmacological categories: anxiolytics, mood stabilizers, hypnotics, antidepressants, and FGAs. No data were collected for medications used for ≤ 7 days or those not expected to impact serum lipid levels.
Statistical Analysis
Continuous variables were expressed as median (interquartile range [IQR]) and compared using the Mann–Whitney U-test. Categorical variables were expressed as numbers (%), and compared using Pearson chi-square or Fisher’s exact test, as appropriate.
To comprehensively evaluate the predictive value of baseline serum ApoB levels and the ApoB/ApoA1 ratio, we employed a multi-faceted analytical strategy designed to yield complementary insight: (1) Identification of Clinically Actionable Thresholds: A maximally selected log-rank statistic analysis was applied to identify the optimal cut-off points for baseline serum ApoB levels and the ApoB/ApoA1 ratio to predict dyslipidemia within 4 months of initiating treatment with SGAs. (2) Risk Assessment Using Dichotomized Variables: Multivariable Cox proportional hazards models were used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs) for the risk of dyslipidemia, comparing patients above versus below the identified cut-off points. (3) Risk Assessment Using Continuous Variables: To assess the dose-response relationship without relying on arbitrary thresholds, we also analyzed baseline serum ApoB levels and the ApoB/ApoA1 ratio as continuous variables in separated multivariable Cox models. To account for potential confounding, models incorporated clinically relevant covariates: age, sex, baseline weight, smoking status, antipsychotic-naïve status, SGA monotherapy, SGA metabolic risk category, and concomitant medication use. The Kaplan-Meier method with Log rank testing was used to compare the cumulative incidence of dyslipidemia across groups defined by the optimal cut-off points for baseline ApoB levels and the ApoB/ApoA1 ratio.
All p values were two-tailed, with statistical significance defined as p < 0.05. Statistical analyses were performed using IBM SPSS (version 25.0) and R software (version 4.3.0).
Results
Baseline Characteristics of Subjects
Baseline characteristics of patients are summarized in Table 1. A total of 311 patients were enrolled in this study. Among them, thirty-three patients (10.6%) with missing baseline ApoA1 measurements were excluded from the ApoB/ApoA1 ratio analyses. Based on a maximally selected log-rank statistic analysis (Figure 1), the optimal cut-off points for stratifying patients into two distinct groups were determined to be 0.70 g/L for baseline serum ApoB levels and 0.45 for the ApoB/ApoA1 ratio. Compared with the high ApoB group (> 0.70 g/L), patients in the low ApoB group (≤ 0.70 g/L) were younger, had a lower proportion of smokers, and exhibited lower baseline levels of TC, LDL-C, and TG but higher HDL-C. Separately, when stratified by the ApoB/ApoA1 ratio, the low ratio group (≤ 0.45) exhibited lower baseline weight and levels of TC and LDL-C but higher levels of HDL-C and FBG than the high ratio group (> 0.45).
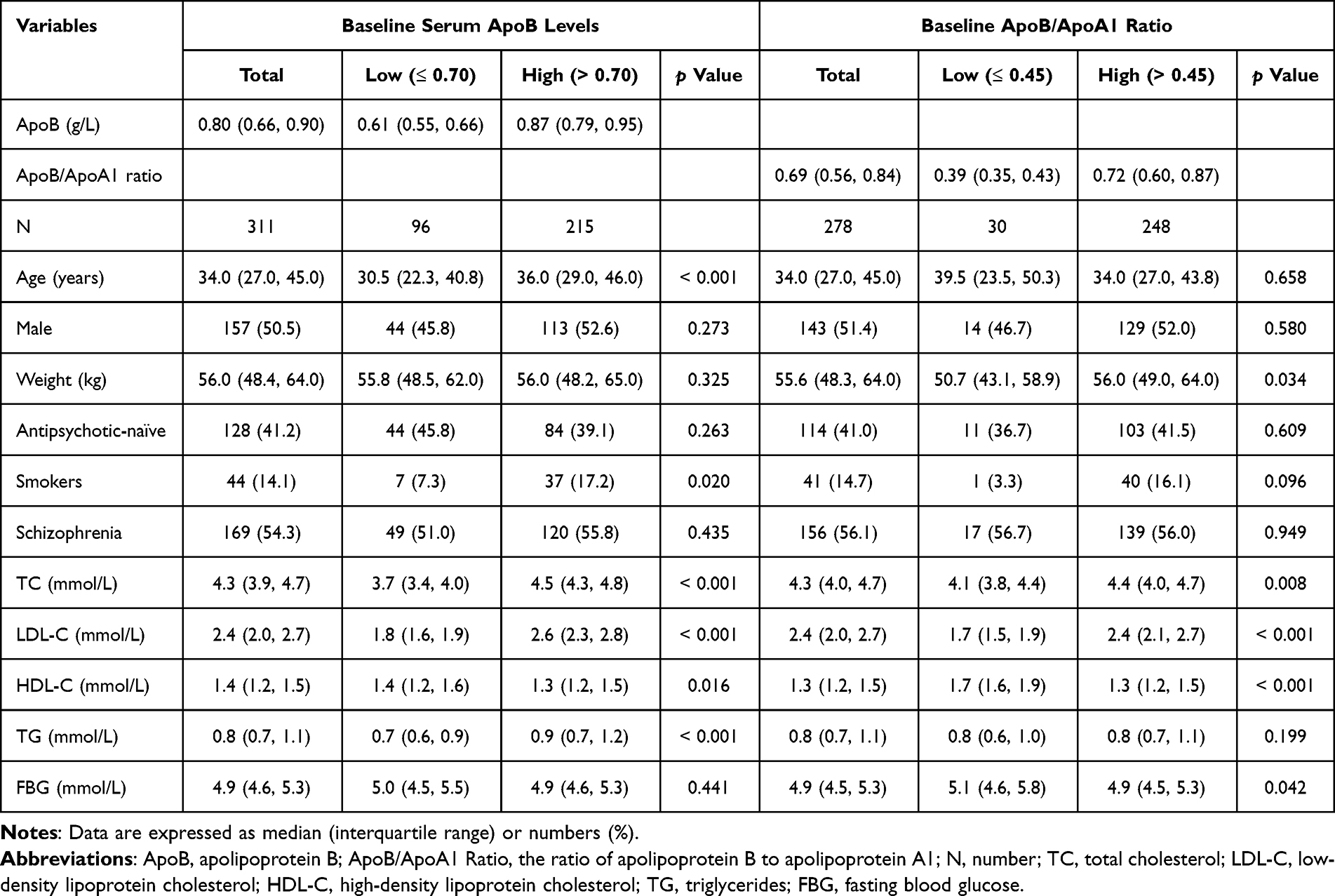 |
Table 1 Baseline Characteristics of Patients Grouped by the Optimal Cut-off Points for Baseline ApoB Levels and the ApoB/ApoA1 Ratio |
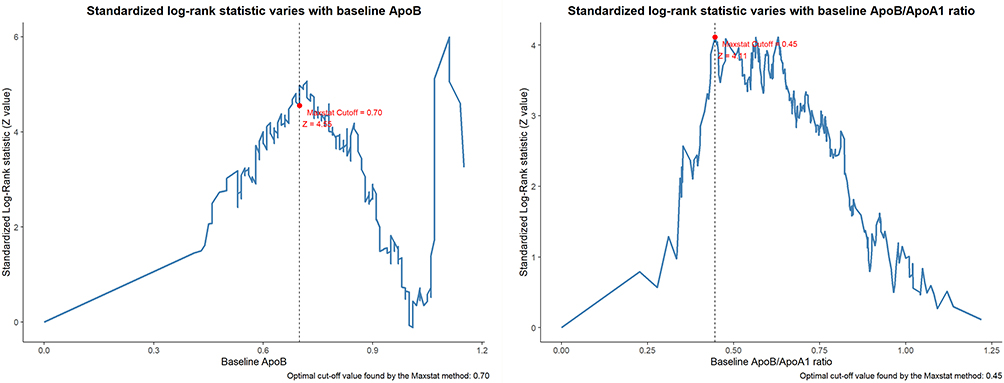 |
Figure 1 Determination of the optimal cut-off values of 0.70 g/L for baseline serum apolipoprotein B (ApoB) levels and 0.45 for the ratio of apolipoprotein B to apolipoprotein A1 (ApoB/ApoA1 ratio) using a maximally selected log-rank statistic analysis. |
SGA Treatment of Subjects
SGA treatment and concomitant medications of patients are presented in Table 2. The most commonly prescribed SGAs were olanzapine (182, 58.5%), risperidone (119, 38.3%), quetiapine (49, 15.8%), aripiprazole (30, 9.6%), paliperidone (14, 4.5%), clozapine (12, 3.9%), amisulpride (12, 3.9%), ziprasidone (2, 0.6%), and lurasidone (1, 0.3%). Except for a significantly higher proportion of antidepressant use in the high ApoB/ApoA1 ratio group, no significant differences were observed in other medication usage (including SGA treatment and concomitant medications) between groups stratified by ApoB levels or the ApoB/ApoA1 ratio.
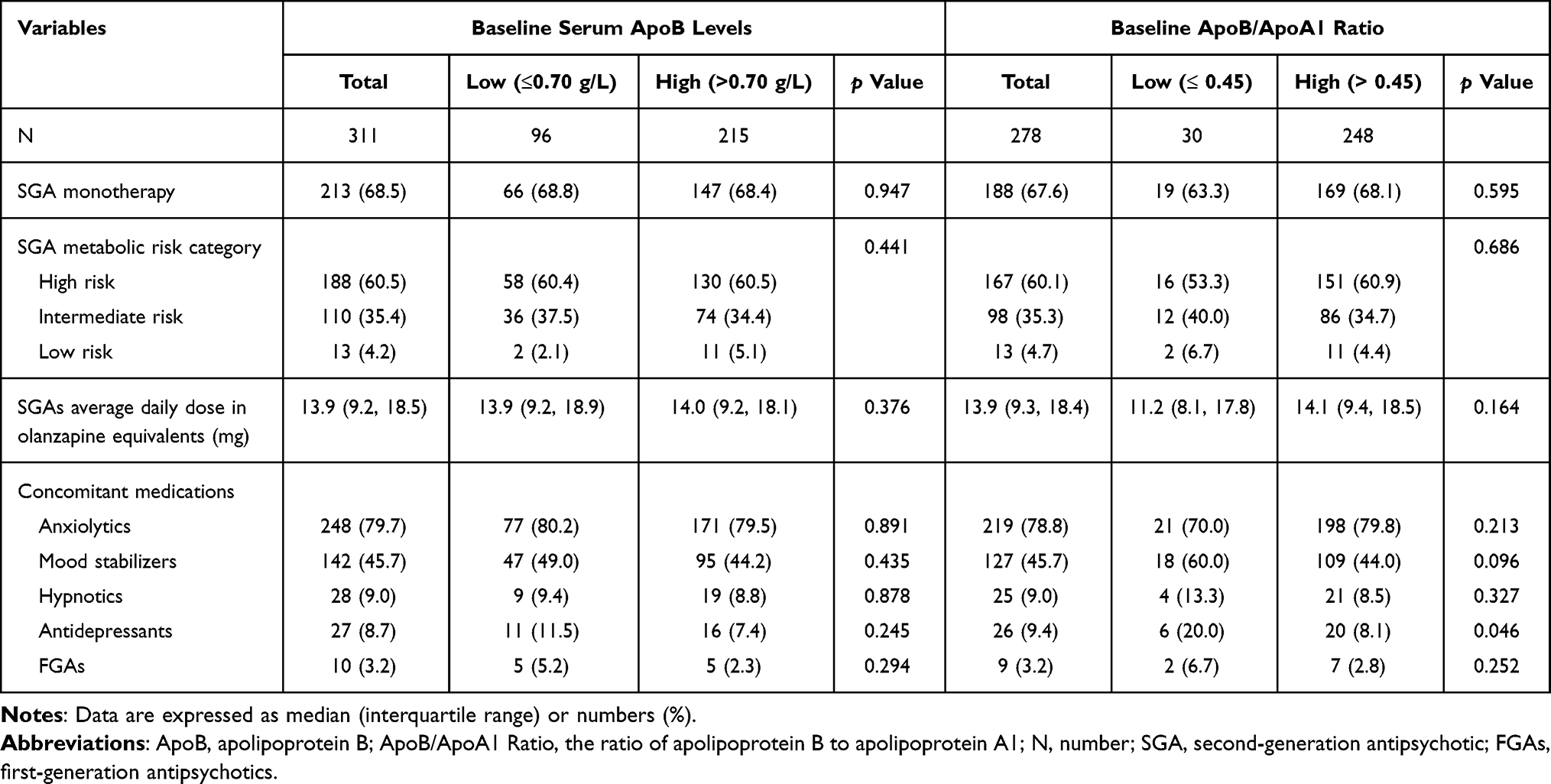 |
Table 2 SGA Treatment and Concomitant Medications of Patients Grouped by the Optimal Cut-off Values for Baseline ApoB Levels and the ApoB/ApoA1 Ratio |
Baseline Serum ApoB Levels and the ApoB/ApoA1 Ratio in Relation to Dyslipidemia Risk
In the overall cohort, the proportion of patients with new-onset dyslipidemia at months 1, 2, 3, and 4 was 28.0% (87/311), 25.7% (80/311), 7.7% (24/311), and 1.6% (6/311), respectively. Corresponding proportions in the ApoB/ApoA1 ratio subgroup were 28.4% (79/278), 25.5% (71/278), 7.6% (21/278), and 2.2% (6/278).
Table 3 presents the association of baseline serum ApoB levels and the ApoB/ApoA1 ratio with incident dyslipidemia, analyzed as continuous variables. Elevated baseline serum ApoB levels and a higher ApoB/ApoA1 ratio were associated with an increased risk of dyslipidemia. For every 0.1 g/L increase in baseline serum ApoB levels, the risk of incident dyslipidemia increased by 34% (adjusted HR 1.34, 95% CI: 1.21–1.48, p < 0.001). Similarly, for every 0.1 unit increase in the baseline ApoB/ApoA1 ratio, the risk of dyslipidemia increased by 20% (adjusted HR 1.20, 95% CI: 1.10–1.30, p < 0.001).
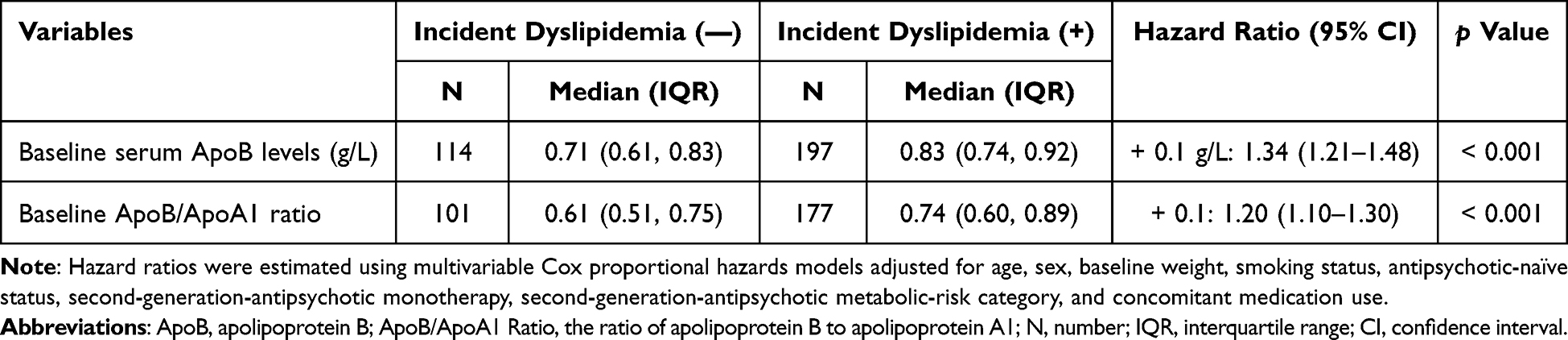 |
Table 3 Association of Baseline Serum ApoB Levels and the ApoB/ApoA1 Ratio with Incident Dyslipidemia |
Table 4 presents the risk of dyslipidemia stratified by the optimal cut-off points for baseline serum ApoB levels and the ApoB/ApoA1 ratio. According to multivariate Cox proportional hazards model 1 (adjusted for age and sex), compared with their respective low groups, the high ApoB group exhibited a significantly elevated risk (HR = 2.48, 95% CI: 1.74–3.54, p < 0.001), while the high ApoB/ApoA1 ratio group showed an even greater risk (HR = 3.29, 95% CI: 1.73–6.23, p < 0.001). These significant associations persisted in the fully adjusted model 2 (ApoB: HR = 2.98, 95% CI: 2.05–4.32, p < 0.001; ApoB/ApoA1 ratio: HR = 3.17, 95% CI: 1.62–6.22, p = 0.001).
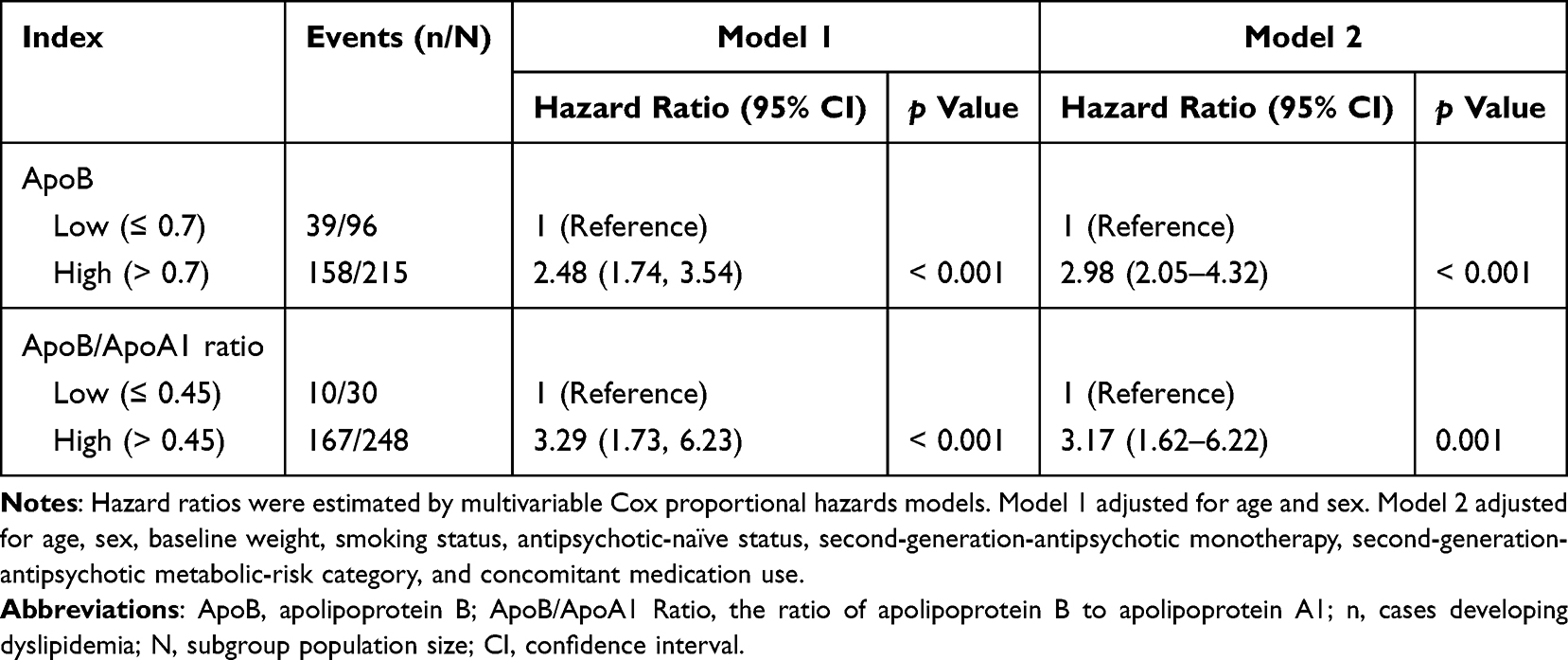 |
Table 4 Risk of Dyslipidemia Stratified by the Optimal Cut-off Values for Baseline Serum ApoB Levels and the ApoB/ApoA1 Ratio |
Figure 2 shows Kaplan-Meier curves indicating a significantly higher cumulative incidence of dyslipidemia among participants in the high ApoB group and those in the high ApoB/ApoA1 ratio group compared with their respective low-level counterparts (Log rank test, both p < 0.001).
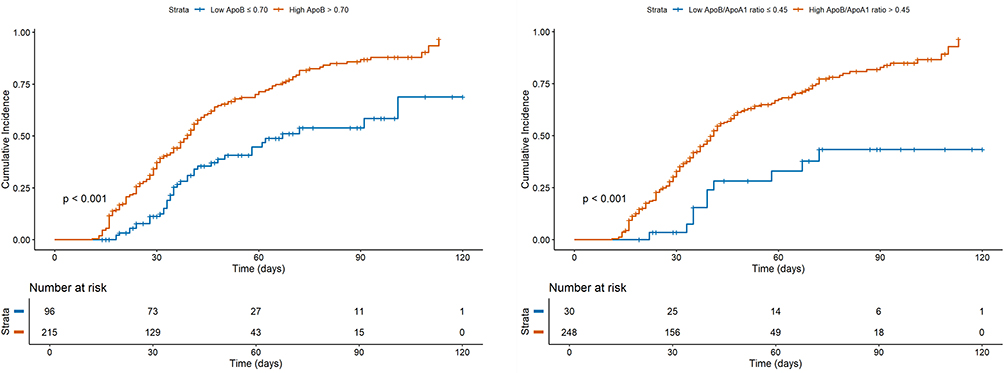 |
Figure 2 Kaplan-Meier cumulative incidence curves for dyslipidemia incidence, stratified by the optimal cut-off points for baseline apolipoprotein B (ApoB) levels and the ratio of apolipoprotein B to apolipoprotein A1 (ApoB/ApoA1 ratio). |
Discussion
SGAs are widely and effectively used to treat mental disorders, including schizophrenia, bipolar mania, depression, anxiety, sleep disorder, obsessive-compulsive disorder, autistic disorder, Tourette’s disorder, posttraumatic stress disorder, and delirium.1 However, their clinical utility is frequently accompanied by metabolic adverse effects, such as dyslipidemia and subsequent MetS.4 As demonstrated in our study, over 50% of patients developed dyslipidemia within two months of initiating SGAs. In addition to elevating CVD and diabetes risk, these metabolic side effects have also been associated with poorer performance on specific cognitive domains in patients with schizophrenia and comorbid MetS, compared with those without MetS.7,19 As patients with mental disorders typically require long-term antipsychotic treatment, it is critical to balance efficacy and safety. Long-term antipsychotic use demonstrates no elevated hospitalization risk from severe physical morbidity while correlating with significantly reduced mortality.20 Conversely, antipsychotic tapering or discontinuation over several months elevated relapse risk versus maintenance treatment, without improving social functioning or altering clinical/social outcomes at two-year follow-up.21 These collective findings pose a major therapeutic challenge, as effective pharmacotherapy must achieve dual objectives: controlling psychiatric symptoms while simultaneously preventing dyslipidemia and subsequent MetS.
SGAs exerted significantly differential effects on serum levels of TC, LDL-C, HDL-C, and TG, manifested as three distinct metabolic risk profiles: (1) clozapine and olanzapine had the highest metabolic risk; (2) risperidone, paliperidone, and quetiapine showed intermediate metabolic risk; (3) amisulpride, aripiprazole, brexpiprazole, cariprazine, lurasidone, and ziprasidone had the lowest metabolic risk.17,22 The identification of biomarkers capable of predicting antipsychotic-induced dyslipidemia risk would allow optimizing SGA selection, balancing symptom control with prevention of lipid abnormalities and subsequent MetS, thereby advancing personalized antipsychotic therapy. However, as far as we know, no study has reported such candidate biomarkers. The absence of validated biomarkers complicates SGA selection in mental disorders.
In this retrospective study, baseline serum ApoB levels and the ApoB/ApoA1 ratio demonstrated strong and consistent predictive value for dyslipidemia risk. Using a maximally selected log-rank statistic analysis, we identified the optimal cut-off values of 0.70 g/L for serum ApoB levels and 0.45 for the ApoB/ApoA1 ratio to stratify patients into distinct risk groups. Kaplan-Meier curves confirmed a significantly higher cumulative incidence of dyslipidemia in both the high ApoB and the high ApoB/ApoA1 ratio groups compared to their low-level counterparts (Log rank test, both p < 0.001). Accordingly, patients exceeding these thresholds showed substantially elevated risks: the high ApoB group exhibited a 2.98-fold higher risk (95% CI: 2.05–4.32, p < 0.001), and the high ApoB/ApoA1 ratio group had a 3.17-fold higher risk (95% CI: 1.62–6.22, p = 0.001) compared with their low-risk counterparts, according to multivariate Cox proportional hazards models. Moreover, when analyzed as continuous measures, each 0.1 g/L increase in baseline serum ApoB levels was associated with a 34% (adjusted HR 1.34, 95% CI: 1.21–1.48, p < 0.001) increased risk of incident dyslipidemia, and each 0.1 unit increase in the baseline ApoB/ApoA1 ratio conferred a 20% (adjusted HR 1.20, 95% CI: 1.10–1.30, p < 0.001) increased risk.
The predictive value of ApoB and the ApoB/ApoA1 ratio for dyslipidemia in patients treated with SGAs aligns with the central roles these apolipoproteins play in lipid metabolism, which are pathways that are directly disrupted by SGAs. ApoB serves as the core structural protein of pro‑atherogenic lipoproteins, including LDL and very low-density lipoproteins (VLDL), which deliver cholesterol to peripheral tissues, whereas ApoA1 is the principal component of anti‑atherogenic HDL particles that mediate reverse cholesterol transport.10,11 SGAs perturb intracellular cholesterol homeostasis through multiple interconnected mechanisms.23 First, they impair the trafficking of LDL‑derived cholesterol out of endolysosomal compartments, resulting in intracellular accumulation and compensatory upregulation of LDL receptor‑mediated uptake. Second, SGAs influence the secretion and metabolism of ApoB‑containing VLDL and ApoA1‑containing HDL particles, which promotes ApoB secretion and VLDL production while often reducing plasma HDL levels. Collectively, these disruptions shift lipid metabolism toward a pro‑atherogenic state, characterized by elevated ApoB and an increased ApoB/ApoA1 ratio. Therefore, elevated baseline levels of these biomarkers likely identify individuals with pre‑existing susceptibility in lipid regulatory pathways, which becomes markedly exacerbated upon SGA treatment. This is supported by our data: compared with the low-level group, both the high ApoB group and the high ApoB/ApoA1 group showed significantly higher baseline levels of TC and LDL-C, as well as significantly lower HDL-C. The high ApoB group also demonstrated significantly higher TG levels. Although the high ApoB/ApoA1 group showed a non-significant increase in TG (IQR: 0.7–1.1 vs 0.6–1.0, p = 0.199), the overall profile aligns with a trend toward dyslipidemia.16 This mechanistic understanding further reinforces the utility of these metrics in clinical practice. Notably, ApoA1 and ApoB levels can be reliably measured under non-fasting conditions, as their concentrations remain unaffected by elevated TG levels.24 This property, combined with their strong pathophysiological basis, makes ApoB levels and the ApoB/ApoA1 ratio more reliable predictors of dyslipidemia risk in patients treated with SGAs. These findings are consistent with previous research which has identified ApoB levels and the ApoB/ApoA1 ratio as independent and powerful predictors of MetS.14,25,26 Therefore, ApoB and the ApoB/ApoA1 ratio serve as practical tools to facilitate individualized antipsychotic therapy selection guided by clinical presentation, patient tolerance, and metabolic risk profiles.
This study observed that the low-risk group stratified by the ApoB/ApoA1 ratio had a significantly smaller sample size (n = 30) than the group stratified by ApoB levels alone (n = 96), reflecting the inherent biological properties of this composite metric. Achieving an ApoB/ApoA1 ratio ≤ 0.45, which requires both low ApoB levels and high ApoA1 levels, is challenging given the significantly lower serum ApoA1 levels observed in patients with schizophrenia compared with healthy controls.27 Consequently, a low ApoB/ApoA1 ratio represents a stricter criterion for metabolic health than isolated low ApoB levels. Consistent with these findings, a systematic review and meta-analysis reported that children and adolescents with MetS showed elevated ApoB levels, an increased ApoB/ApoA1 ratio, and reduced ApoA1 levels.28 Multivariable Cox proportional hazards models further demonstrated that, compared with their respective low-risk groups, the high ApoB/ApoA1 ratio group had a significantly higher hazard ratio for dyslipidemia than the high ApoB group. This pattern was consistent in both the age-sex-adjusted model (High ApoB/ApoA1 ratio: HR = 3.29, 95% CI: 1.73–6.23, p < 0.001; High ApoB: HR = 2.48, 95% CI: 1.74–3.54, p < 0.001) and the fully adjusted model (High ApoB/ApoA1 ratio: HR = 3.17, 95% CI: 1.62–6.22, p = 0.001; High ApoB: HR = 2.98, 95% CI: 2.05–4.32, p < 0.001). The threshold of ApoB/ApoA1 ratio ≤ 0.45 highlights the clinical value of this ratio: it may identify a truly low-risk, rare subgroup that can safely tolerate high metabolic-risk SGAs, such as olanzapine. Conversely, patients with baseline serum ApoB levels > 0.70 g/L and an ApoB/ApoA1 ratio > 0.45 should be administered high metabolic-risk SGAs with caution and receive intensified metabolic monitoring.
To our knowledge, this is the first study evaluating the predictive value of baseline serum ApoB levels and the ApoB/ApoA1 ratio for dyslipidemia risk in psychiatric patients treated with SGAs. Notably, previous research indicated that patients with normal baseline metabolic parameters experienced greater adverse changes in all metabolic indices compared with those with baseline abnormalities.29 This finding underscored the clinical significance of our study, which specifically enrolled patients without dyslipidemia or hyperglycemia at admission.
This study has several limitations. First, as a retrospective study, it was susceptible to selection bias and incomplete data. To minimize residual confounding, we performed covariate adjustments in our analytical models. Consequently, our findings reflect real-world associations of baseline serum ApoB levels and the ApoB/ApoA1 ratio with the risk of dyslipidemia following SGA initiation, providing clinically relevant insights. Second, the strict inclusion and exclusion criteria limited the sample size. Therefore, while the study enabled group-level comparisons of metabolic risk across SGA classes, it precluded both agent-specific analysis and an investigation into formulation differences (oral vs long-acting injectable (LAI)). Given the differing pharmacodynamic profiles of SGAs, as well as emerging evidence30,31 that LAI formulations may have distinct efficacy and adverse effects, dyslipidemia risk is likely to vary across specific agents and formulations. Thus, caution is warranted in applying the cut-off value to individual SGAs or specific formulations, especially those with high metabolic risk. Future studies should therefore investigate whether the predictive power of ApoB and the ApoB/ApoA1 ratio for dyslipidemia risk differs across specific agents and formulations. Such research could further refine personalized treatment strategies. Third, as our findings were derived exclusively from a Chinese population, extrapolation to other populations should be made with caution. Finally, key lifestyle determinants of metabolic health (eg, dietary patterns and physical activity) were not systematically assessed or included in the analytical models, which could introduce unmeasured confounding. However, as participants were inpatients, their diet and physical activity were uniformly regulated by the hospital, likely minimizing variability in these factors in our study.
Conclusion
This study demonstrates that baseline serum ApoB levels and the ApoB/ApoA1 ratio are valuable risk markers for dyslipidemia in patients treated with SGAs. However, given the retrospective design and inherent heterogeneity of the cohort, further validation through large prospective studies combined with molecular investigations is warranted. Such research should confirm the predictive utility of these biomarkers, establish optimal cut-off values for clinical implementation, and investigate whether combining these markers with traditional lipid profiles or other alternative laboratory parameters can improve the accuracy of predictive models for dyslipidemia risk in patients treated with SGAs.
Data Sharing Statement
Access to the raw data underlying this study is restricted under hospital medical regulations, which prohibit unauthorized data sharing.
Ethics Approval
This study was approved by the Ethics Committees of Zhongshan Third People’s Hospital (Ethics Approval No. SSYLL-KY-20231103). All procedures complied with the ethical standards of the responsible institutional and national committees on human experimentation and the Helsinki Declaration of 1975, as revised in 2008 (5).
Consent to Participate
Because this was a retrospective, non-interventional study using anonymized data, the Ethics Committee of Zhongshan Third People’s Hospital formally waived the requirement to obtain informed consent.
Acknowledgments
The authors gratefully acknowledge the staff at the Clinical Lab of Zhongshan Third People’s Hospital.
Funding
This study was funded by the Guangdong Provincial Medical Science and Technology Research Fund (Grant No. A2024535).
Disclosure
No conflict of interest was declared.
References
1. Feng XZ, Li Z, Li ZY. et al. Effectiveness and safety of second-generation antipsychotics for psychiatric disorders apart from schizophrenia: a systematic review and meta-analysis. Psychiatry Res. 2024;332:115637. doi:10.1016/j.psychres.2023.115637
2. Gründer G, Heinze M, Cordes J, et al. Effects of first-generation antipsychotics versus second-generation antipsychotics on quality of life in schizophrenia: a double-blind, randomised study. Lancet Psychiatry. 2016;3(8):717–729. doi:10.1016/S2215-0366(16)00085-7
3. Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31–41. doi:10.1016/S0140-6736(08)61764-X
4. Akinola PS, Tardif I, Leclerc J. Antipsychotic-Induced Metabolic Syndrome: a Review. Metab Syndr Relat Disord. 2023;21(6):294–305. doi:10.1089/met.2023.0003
5. Trigueiro AJP, Ramirez J, Hennessey E, Beqiri M. Metabolic Syndrome Identification in Patients Treated With Second-Generation Antipsychotic Medications. J Psychosoc Nurs Ment Health Serv. 2022;60(8):11–18. doi:10.3928/02793695-20220314-01
6. Mitchell AJ, Vancampfort D, De Herdt A, Yu W, De Hert M. Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta-analysis of first episode, untreated and treated patients. Schizophr Bull. 2013;39(2):295–305. doi:10.1093/schbul/sbs082
7. Samson SL, Garber AJ. Metabolic syndrome. Endocrinol Metab Clin North Am. 2014;43(1):1–23. doi:10.1016/j.ecl.2013.09.009
8. Laursen TM. Life expectancy among persons with schizophrenia or bipolar affective disorder. Schizophr Res. 2011;131(1–3):101–104. doi:10.1016/j.schres.2011.06.008
9. Azad MC, Shoesmith WD, Al Mamun M, et al. Cardiovascular diseases among patients with schizophrenia. Asian J Psychiatr. 2016;19:28–36. doi:10.1016/j.ajp.2015.11.012
10. Su X, Peng D. The exchangeable apolipoproteins in lipid metabolism and obesity. Clin Chim Acta. 2020;503:128–135. doi:10.1016/j.cca.2020.01.015
11. Morita S. Metabolism and Modification of Apolipoprotein B-Containing Lipoproteins Involved in Dyslipidemia and Atherosclerosis. Biol Pharm Bull. 2016;39(1):1–24. doi:10.1248/bpb.b15-00716
12. Singh K, Prabhakaran D. Apolipoprotein B - An ideal biomarker for atherosclerosis? Indian Heart J. 2024;76(Suppl 1):S121–S129. doi:10.1016/j.ihj.2023.12.001
13. Ojanen X, Cheng R, Törmäkangas T, et al. Towards early risk biomarkers: serum metabolic signature in childhood predicts cardio-metabolic risk in adulthood. EBioMedicine. 2021;72:103611. doi:10.1016/j.ebiom.2021.103611
14. Chou YC, Kuan JC, Bai CH, et al. Predictive value of serum apolipoprotein B/apolipoprotein A-I ratio in metabolic syndrome risk: a Chinese cohort study. Endocrine. 2015;49(2):404–414. doi:10.1007/s12020-014-0447-z
15. Park KJ. Associations between apolipoprotein B/A1 ratio, lipoprotein(a), and the risk of metabolic-associated fatty liver diseases in a Korean population. Lab Med. 2023;54(6):633–637. doi:10.1093/labmed/lmad021
16. Zhu JR, Gao RL, Zhao SP, Lu GP, Zhao D, Li JJ. Chinese guidelines for the prevention and treatment of dyslipidemia in adults (2016 revision). Chin Circul J. 2016;31(10):937–953. doi:10.3969/j.issn.1000-3614.2016.10.001
17. Yu X, Si TM, Shi C, et al. Chinese expert consensus on the management of metabolic syndrome in patients with schizophrenia. Chin J Psychiat. 2020;53(01):3–10. doi:10.3760/cma.j.issn.1006-7884.2020.01.002
18. World Health Organization Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index. Available from: http://www.whocc.no/atcddd/.
19. Zheng W, Jiang WL, Zhang X, et al. Use of the RBANS to Evaluate Cognition in Patients with Schizophrenia and Metabolic Syndrome: a Meta-Analysis of Case-Control Studies. Psychiatr Q. 2022;93(1):137–149. doi:10.1007/s11126-021-09889-9
20. Taipale H, Tanskanen A, Mehtälä J, Vattulainen P, Correll CU, Tiihonen J. 20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20). World Psychiatry. 2020;19(1):61–68. doi:10.1002/wps.20699
21. Moncrieff J, Crellin N, Stansfeld J, et al. Antipsychotic dose reduction and discontinuation versus maintenance treatment in people with schizophrenia and other recurrent psychotic disorders in England (the RADAR trial): an open, parallel-group, randomised controlled trial. Lancet Psychiatry. 2023;10(11):848–859. doi:10.1016/S2215-0366(23)00258-4
22. Pillinger T, McCutcheon RA, Vano L, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(1):64–77. doi:10.1016/S2215-0366(19)30416-X
23. Vantaggiato C, Panzeri E, Citterio A, Orso G, Pozzi M. Antipsychotics Promote Metabolic Disorders Disrupting Cellular Lipid Metabolism and Trafficking. Trends Endocrinol Metab. 2019;30(3):189–210. doi:10.1016/j.tem.2019.01.003
24. Marcovina S, Packard CJ. Measurement and meaning of apolipoprotein AI and apolipoprotein B plasma levels. J Intern Med. 2006;259(5):437–446. doi:10.1111/j.1365-2796.2006.01648.x
25. Du R, Wu X, Peng K, et al. Serum apolipoprotein B is associated with increased risk of metabolic syndrome among middle-aged and elderly Chinese: a cross-sectional and prospective cohort study. J Diabetes. 2019;11(9):752–760. doi:10.1111/1753-0407.12904
26. Jing F, Mao Y, Guo J, et al. The value of Apolipoprotein B/Apolipoprotein A1 ratio for metabolic syndrome diagnosis in a Chinese population: a cross-sectional study. Lipids Health Dis. 2014;13:81. doi:10.1186/1476-511X-13-81
27. Boiko AS, Mednova IA, Kornetova EG, et al. Apolipoprotein serum levels related to metabolic syndrome in patients with schizophrenia. Heliyon. 2019;5(7):e02033. doi:10.1016/j.heliyon.2019.e02033
28. Dinpanah K, Kazemi T, Shetty S, Bizhaem SK, Fanoodi A, Riahi SM. The association of the apolipoprotein B/A1 ratio and the metabolic syndrome in children and adolescents: a systematic review and meta-analysis. J Diabetes Metab Disord. 2023;23(1):1–10. doi:10.1007/s40200-023-01235-z
29. Zhang Y, Wang Q, Reynolds GP, et al. Metabolic Effects of 7 Antipsychotics on Patients With Schizophrenia: a Short-Term, Randomized, Open-Label, Multicenter, Pharmacologic Trial. J Clin Psychiatry. 2020;81(3):19m12785. doi:10.4088/JCP.19m12785
30. Kishimoto T, Hagi K, Kurokawa S, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre-post studies. Lancet Psychiatry. 2021;8(5):387–404. doi:10.1016/S2215-0366(21)00039-0
31. Wang D, Schneider-Thoma J, Siafis S, et al. Long-Acting Injectable Second-Generation Antipsychotics vs Placebo and Their Oral Formulations in Acute Schizophrenia: a Systematic Review and Meta-Analysis of Randomized-Controlled-Trials. Schizophr Bull. 2023;50(1):132–144. doi:10.1093/schbul/sbad089
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.