Back to Journals » Journal of Pain Research » Volume 14
Serratus Anterior Block for Long-Term Post-Thoracoscopy Pain Management
Authors Semyonov M, Fedorina E, Shalman A ![]() , Dubilet M
, Dubilet M ![]() , Refaely Y, Ruderman L, Frank D, Gruenbaum BF, Koyfman L, Friger M, Zlotnik A, Klein M, Brotfain E
, Refaely Y, Ruderman L, Frank D, Gruenbaum BF, Koyfman L, Friger M, Zlotnik A, Klein M, Brotfain E
Received 1 December 2020
Accepted for publication 18 January 2021
Published 15 December 2021 Volume 2021:14 Pages 3849—3854
DOI https://doi.org/10.2147/JPR.S295019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Michael Semyonov,1,* Ekaterina Fedorina,1,* Anna Shalman,1 Michael Dubilet,1 Yael Refaely,2 Leonid Ruderman,2 Dmitry Frank,1 Benjamin F Gruenbaum,3 Leonid Koyfman,1 Michael Friger,4 Alexander Zlotnik,1 Moti Klein,1 Evgeni Brotfain1
1Department of Anesthesiology and Critical Care, General Intensive Care Unit, Soroka Medical Center, Faculty of Health Science, Ben-Gurion University of the Negev, Beer Sheva, Israel; 2Department of Cardiothoracic Surgery, Soroka Medical Center, Faculty of Health Science, Ben-Gurion University of the Negev, Beer Sheva, Israel; 3Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Jacksonville, FL, USA; 4Department of Public Health, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel
*These authors contributed equally to this work
Correspondence: Evgeni Brotfain
Department of Anesthesiology and Critical Care, Soroka Medical Center, Ben Gurion University of the Negev, Beer Sheva, 84101, Israel
Tel +972 54-621-8106
Email [email protected]
Purpose: Neuropathic, chronic pain is a common and severe complication following thoracic surgery, known as post-thoracotomy pain syndrome (PTPS). Here we evaluated the efficacy of an ultrasound-guided serratus anterior plane block (SAPB) on pain control compared to traditional pain management with intravenous opioids and nonsteroidal anti-inflammatory drugs (NSAIDs) six months after thoracic surgery.
Patients and Methods: In this retrospective observational study, we analyzed data from a questionnaire survey. We interviewed all patients who underwent elective video-assisted thoracoscopy surgery (VATS) at Soroka University Medical Center between December 2016 and January 2018. The responses of ninety-one patients were included.
Results: Participants reported PTPS in both groups, 43% of patients in the SAPB group and 57% of patients in the standard group, which failed to reach significance. However, we demonstrated that the percentage of pain occurrence trended lower in the SAPB group. There was significantly less burning/stitching or shooting, shocking, pressure-like, and aching pain in SAPB patients compared to the standard protocol group. Patients in the SAPB group had significantly less pain located in the upper and lower posterior thorax anatomical regions compared to the standard protocol group. Moreover, we found a significant difference in occurrence of PTPS depending on the type of thoracic surgery. From both study groups, 69% of patients who underwent lobectomy reported pain, compared with 41.9% of those in the segmental (wedge resection) procedure, and 42.1% of patients in other procedures.
Conclusion: While the present study did not demonstrate a statistically significant reduction of PTPS after SAPB concerning postoperative pain control, there was a trend of a decrease. We also found significance in the type of pain and location of pain after thoracic surgery between the two groups, as well as a significant difference between pain occurrence in types of thoracic surgeries from both groups.
Keywords: chronic pain, post-thoracotomy pain syndrome, PTPS, regional anesthesia block, serratus anterior, thoracic surgery
Introduction
Chronic pain, or pain lasting for at least 12 weeks,1,2 is the highest contributor to long-term disabilities and the third most problematic issue facing global health in recent years.1 It has been estimated that one out of every ten people is diagnosed with chronic pain each year.2 Many surgeries are associated with severe chronic post-surgical pain originating from several factors. These factors can include peripheral sensitization via inflammation and/or nerve injury; maladaptive central neural plasticity at spinal and higher levels (central sensitization), caused by opioids (particularly when given preoperatively), stress, or other variables; pathological descending nociceptive facilitation; or cognitive factors such as anxiety or stress.3 Chronic pain can cause insomnia and loss of appetite and may incapacitate patients, making daily activities difficult or impossible.4
Chronic, neuropathic pain is particularly common following thoracic surgery, known as post-thoracotomy pain syndrome (PTPS). The incidence of PTPS has been estimated to be as high as 57% and 47% at 3 and 6 months post-surgery, respectively.1–3 This severe complication can last for months or years, and is associated with symptoms such as burning pain or shooting, shocking, pressure-like, and aching pain.5,6 Although there are several mechanisms that contribute to the development of PTPS, intercostal nerve damage and subsequent dysfunction have been well established.6 Risk factors for the development of chronic pain after thoracic surgery are multifactorial, but can include inadequate postoperative pain control.6 Furthermore, Homma et al5 found that preoperative use of hypnotic medication, the type of thoracotomy approach, and a surgery lasting more than 2.5 hours are associated with increased risk of PTPS. A complete video-assisted thoracoscopy surgery (VATS) may decrease the incidence of postoperative neuropathic pain, regardless of the duration of surgery. However, chronic pain after VATS has still been observed in 20–25% of patients.4
Providing analgesia for thoracic surgery is challenging for a variety of reasons. Narcotic-based patient-controlled analgesia (PCA) may not provide adequate pain relief, and the side effects of respiratory depression and impaired mental status can outweigh its benefits. Thoracic epidural analgesia is associated with serious risks due to its significant resultant hemodynamic instability.7 Thus, many new methods of regional anesthesia techniques, such as paravertebral blocks, intercostal nerve blocks, interscalene blocks, erector spinal blocks and pectoralis and serratus anterior plane blocks for postoperative pain management have been tested after thoracic surgery.8 Semyonov et al9 have validated ultrasound-guided serratus anterior plane block (SAPB) as an effective and safe technique for postoperative pain relief after different types of thoracic surgery.10–12
In this retrospective observational study, we evaluated the efficacy of an ultrasound-guided SAPB on pain control compared to traditional pain management with intravenous opioids and nonsteroidal anti-inflammatory drugs (NSAIDs) six months after thoracic surgery. Ultimately, we hope this study assists in better understanding the utilization of SAPB as an alternative treatment modality for post-thoracotomy pain control.
Patients and Methods
The study was conducted according to the recommendations of the Declaration of Helsinki and was approved by the Human Research and Ethics Committee at Soroka Medical Center (RN-0345-16.SOR). The formal informed consent for the survey was obtained from each patient who was recruited in a previous prospective study.9 In this study, we interviewed all the patients who underwent elective VATS at Soroka University Medical Center, a 1000-bed tertiary-care, Trauma Level I university teaching hospital located in Beer Sheva, Israel, between December 2016 until January 2018. Responses from ninety-one patients were included.
Inclusion Criteria
All patients over the age of 18 who underwent elective VATS at Soroka University Medical Center between December 2016 until January 2018 and received SAPB or standard pain control for postoperative pain management were included.
Exclusion Criteria
Patients were excluded if they refused to participate in the survey or did not respond to several phone calls, or if they died within six months of the VATS procedure.
Data Survey
Each patient was interviewed via a phone call by a staff anesthesia physician six months after surgery. We administered a questionnaire form to each participant (Appendix A) that included a modified version of the McGill Pain Questionnaire administered in Hebrew.13 Data ascertained by the survey included characteristics of pain, intensity, anatomic localization and also pain management for six months post-procedure. Chronic pain was defined as pain that persisted for more than three months after surgery.
Variables and Measurements
In addition to the survey, we collected data from electronic records from the hospital and intensive care unit including demographics of gender, age, weight, ethnicity, area of residence; American Society of Anesthesiologists physical status classification (ASA class) from I–III; duration of the surgery; type of surgery; and duration of hospital stay.
Postoperative Pain Management Protocols and Surgical Approach9
All patients underwent thoracoscopy for anatomic or non-anatomic lung resection performed under general anesthesia. The standard thoracoscopy approach in our institution includes the three holes technique. This consists of two incisions of 1 cm each and one utility incision of 4 cm. In the case of a technical impossibility of tumor extraction or bleeding, thoracotomy is performed. The standard thoracotomy is posterior-lateral thoracotomy which divides the latissimus dorsi muscle but spares the serratus anterior muscle.
The patients interviewed for this study were previously divided into two different protocols for postoperative pain management.9 Group 1 (“standard group”) patients received standard pain control that included treatment by opioids, NSAIDs and acetaminophen (paracetamol). Patients in Group 2 received ultrasound-guided SAPB immediately after induction and positioning for surgery (0.25% bupivacaine hydrochloride in a dose of 2 mg/kg in addition to a standard pain control protocol).
Statistical Analysis
In order to meet the main objective of the study, we calculated sample based on means comparison with WINPEPI 11.65 software.14 Sample size was calculated for a significance level of 0.05 and power level of 90%, and a standard deviation of 2.2 for the standard group and 3.6 for the SAPB group, based on data from previous research.9 A difference of 1.5 between mean VAS was considered clinically significant. The sample size that matches such data is 168 patients (84 in each group). Data summaries will be performed using SPSS (version 16.01 or higher). Data collected in this study were summarized using frequency tables, summary statistics, confidence intervals, and p-values as appropriate. Continuous variables were compared by t-tests. For continuous variables with non- normal distribution, comparisons were evaluated for significance with the use of the Wilcoxon rank-sum test. For continuous variables, the 95% confidence interval were calculated using means and standard errors from Student’s t-test statistics. Variable selection in multivariable modeling was based on clinical and statistical significance. Laboratory test values at admission were included.
Results
Ninety-one patients who underwent elective thoracic surgery from December 2016 to January 2018 were included in this survey. The patients consisted of 38 men and 53 women. The demographic data (age, gender, weight, Jewish or Arab ethnicity, urban or village region, ASA classification, and length of hospital stay) are summarized in Table 1. There were no significant differences found between any of these measured data.
 |
Table 1 Demographic Data, ASA Classification and Length of Hospital Stay |
Table 2 demonstrates the type of thoracic surgery and duration of the procedure. The duration of the procedure (including anesthetic preparation) was significantly longer in the SAPB group with a mean procedure time of 142.67 minutes compared to the standard group with a mean procedure time of 111.54 minutes (p<0.05). No differences in the type of thoracic surgery were found.
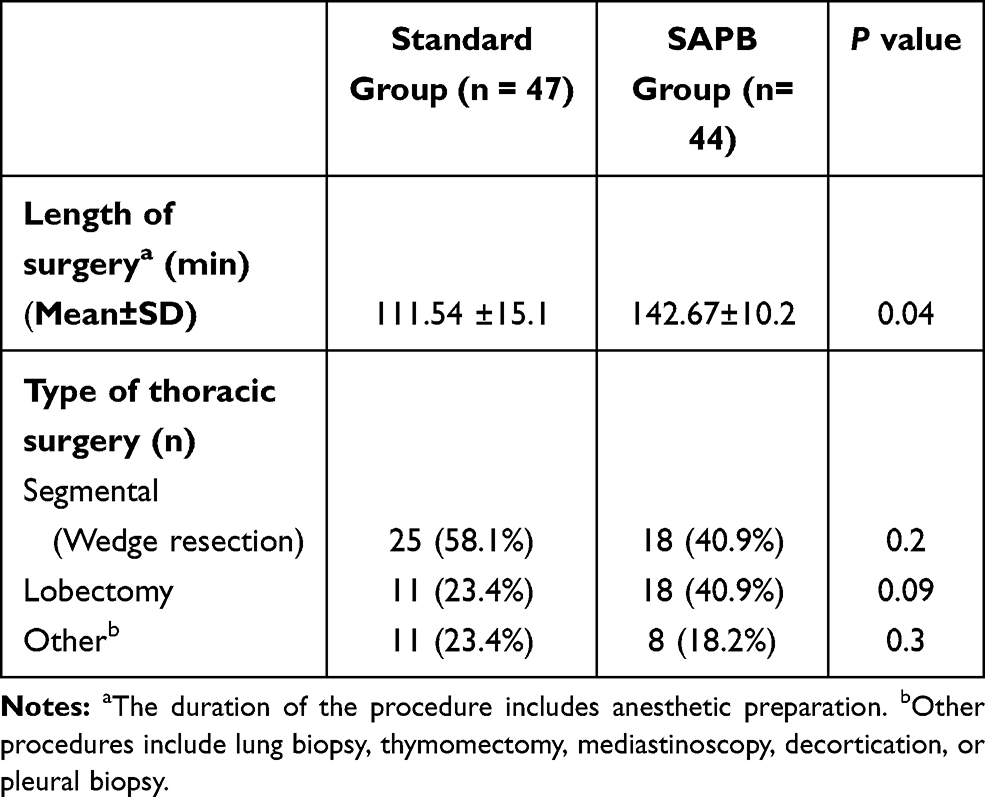 |
Table 2 Type of Thoracic Surgery and Duration of Procedure |
Table 3 shows data of occurrence of PTPS as well as different types of pain. The overall occurrence of PTPS was not statistically significant between the study groups (57.4% in the SAPB group and 43.2% in the standard protocol group). However, this data reflects a trend of a decreased percentage of pain syndrome occurrence in the SAPB group.
 |
Table 3 Characteristics of Post-Thoracoscopy Chronic Pain Syndrome (PTPS) |
The types of pain observed between the two group were significant. The data demonstrated a significantly lower percentage of burning/stitching and other pain (shooting, shocking, pressure-like, and aching) in the SAPB group patients, at 45% and 7%, respectively, compared to standard pain control protocol group at 57% and 15% (p<0.05, see Table 3). Patients in the SAPB group had a significantly less percentage of pain syndrome localized in upper and lower posterior thorax anatomical regions (11%) compared to the standard protocol group (28%, with a p value<0.05).
Moreover, we found a significant difference in occurrence of pain syndrome dependent on the type of thoracic surgery. From both study groups, 20 patients (69%) who underwent lobectomy, 18 patients (41.9%) who underwent a segmental procedure (wedge resection), and 8 patients (42.1%) who underwent other types of thoracic surgeries suffered from PTPS. There were no differences in intensity of pain between both study groups. There were no patients who described their chronic pain as “insufferable”.
There was no difference in therapeutic management of PTPS between both study groups for occurrence of any drug treatment (43.2% for SAPB and 57.4% for the standard group) or type of medication prescribed (Table 4).
 |
Table 4 Therapeutical Management of Post-Thoracoscopy Chronic Pain Syndrome |
Table 5 shows the results of multivariate logistic regression analysis of chronic post-thoracoscopy pain syndrome. Male gender, Jewish ethnicity and lobectomy as a type of thoracic surgery were found to be independent risk factors for development of chronic pain syndrome. All patients were able to return to their typical lifestyle within one month of the procedure.
 |
Table 5 Multivariate Logistic Regression Analysis for Risk Factors of Chronic Post-Thoracoscopy Pain Syndrome Development for Both Study Groups |
Discussion
PTPS is a serious complication of thoracic surgery, lasting months or years, and is accompanied by a range of painful sensations.5,6 This chronic pain can lead to disruption of daily life and long-term disability.1,4 Bayman et al4 found that the chronic pain related to thoracic surgery was associated with more severity of average acute pain during the first 3 days after surgery. Furthermore, a meta-analysis of randomized, controlled trials by Weinstein et al,15 revealed that the intraoperative use of regional anesthesia in addition to general anesthesia reduced the risk of PTPS. Univariate statistical analysis showed the overall percent of PTPS occurred in 43% of SAPB patients and 57% of patients undergoing standard protocol. Bayman et al4 yielded similar incidence of 44% of patients suffering chronic pain at 3 months after surgery. They also did not reach significance when comparing the percent of PTPS after either type of thoracic surgery.4 Our study, however, did demonstrate a significantly increased incidence of PTPS after lobectomy (69% of patients) compared to other types of thoracic procedures.
Furthermore, we found a significantly low percentage of burning/stitching or shooting, shocking, pressure-like, and aching pain in the SAPB group patients compared to the patients in the standard pain control group. Surprisingly, our data revealed a lower incidence of the sensation of pain specifically located in the upper and lower posterior thorax anatomical regions among participants from the SAPB group compared to the standard protocol group. Those findings may result from the benefits of patient placement on the operating table when administered the SAPB.
The incidence of chronic pain after surgery varies markedly between different studies and between individual procedures, from 5% to 65% for patients after thoracotomy or/thoracoscopy.16–19 A single operation may lead to a number of different pain conditions. Thoracotomy is associated with post-operative pain potentially arising from the musculoskeletal system from rib retraction, neuropathic pain from trauma to intercostal nerves, damage to internal organs producing visceral pain and pain due to the placement of chest drains.20
Moreover, we showed that only male gender, Jewish ethnicity and lobectomy as a type of thoracic surgery were found to be independent predictors of development of chronic pain syndrome after thoracic surgery. In contrast to our findings, McHugh et al21 demonstrated pre-treatment differences in opioid dependence severity: women reported significantly greater functional and psychiatric impairment and a higher likelihood of using opioids to cope with negative side effects and pain than men did. However, the same authors21 showed that once the study treatment was initiated, women and men exhibited similar opioid use outcomes. Similarly, Manubay et al22 did not find differences between males and females in age, race, education, marital status or employment status regarding the prescription of opioids for chronic pain. Huang,23 and Wyatt,24 demonstrated a significant gap between the evaluation and treatment of pain in white people and its evaluation and treatment in Black Americans and Hispanics. Hispanics and Black Americans are more likely to report any pain and severe pain, respectively, than white Americans.23–25 Women have been shown to treat pain more often than men, but are less likely to be taken seriously about their pain.26
Our study has a number of limitations. As a retrospective, observational questionnaire design, this study utilized a phone call survey only for collecting relevant data, but answers were based on the subjective experience of the participant and the clinician. No clinical or imaging assessment was able to be provided. We did not perform an additional SAPB or other regional anesthesia procedures during the postoperative period for patients after thoracic surgery. Thus, it may be that the clinical and pharmacological effects of SAPB are limited to the early postoperative time. Future studies could examine SAPB pain control earlier than six months after the procedure.
Conclusion
While the present study did not demonstrate a statistically significant reduction of PTPS after a SAPB for postoperative pain control, there was a trend that the incidence of PTPS decreased compared to the standard group. We also observed a significant difference in the type of pain and anatomical location of pain after the surgery between the two groups. While this method holds many promising aspects for the future of pain management, especially for PTPS, we feel that further studies are needed to better understand the clinical significance of SAPB approach for postoperative pain control after thoracic surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Majedi H, Amini MH, Yousefshahi F, et al. Predicting factors of pain duration in patients with chronic pain: a large population-based study. Anesth Pain Med. 2020;10(1):e95776. doi:10.5812/aapm.95776
2. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. doi:10.1186/1471-2458-11-770
3. Geil D, Thomas C, Zimmer A, Meissner W. Chronified pain following operative procedures: the place of locoregional and systemic local anesthetics. Deutsches Ärzteblatt Int. 2019;116(15):261. doi:10.3238/arztebl.2019.0261
4. Bayman EO, Parekh KR, Keech J, Selte A, Brennan TJ. A prospective study of chronic pain after thoracic surgery. Anesthesiology. 2017;126(5):938–951. doi:10.1097/ALN.0000000000001576
5. Homma T, Doki Y, Yamamoto Y, et al. Risk factors of neuropathic pain after thoracic surgery. J Thorac Dis. 2018;10(5):2898. doi:10.21037/jtd.2018.05.25
6. Mesbah A, Yeung J, Gao F. Pain after thoracotomy. BJA Educ. 2016;16(1):1–7. doi:10.1093/bjaceaccp/mkv005
7. Brodsky J. Anaesthesia, pain, intensive care & emergency APICE. Springer Milan. 2008;29:305–312.
8. Kelsheimer B, Williams C, Kelsheimer C. New emerging modalities to treat post-thoracotomy pain syndrome: a review. Mo Med. 2019;116(1):41.
9. Semyonov M, Fedorina E, Grinshpun J, et al. Ultrasound-guided serratus anterior plane block for analgesia after thoracic surgery. J Pain Res. 2019;12:953. doi:10.2147/JPR.S191263
10. Anaesthesiology SG, Gautam SK, Gautam SK, Agarwal A, Agarwal A. Serratus anterior plane block: a new analgesic technique for post-thoracotomy pain. Pain Physician. 2015;18:E421–E424.
11. Okmen K, Okmen BM, Uysal S. Serratus anterior plane (SAP) block used for thoracotomy analgesia: a case report. Korean J Pain. 2016;29(3):189. doi:10.3344/kjp.2016.29.3.189
12. Khalil AE, Abdallah NM, Bashandy GM, Kaddah TA-H. Ultrasound-guided serratus anterior plane block versus thoracic epidural analgesia for thoracotomy pain. J Cardiothorac Vasc Anesth. 2017;31(1):152–158. doi:10.1053/j.jvca.2016.08.023
13. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
14. Abramson JH. WINPEPI updated: computer programs for epidemiologists, and their teaching potential. Epidemiol Perspect Innov. 2011;8(1):1. doi:10.1186/1742-5573-8-1
15. Weinstein EJ, Levene JL, Cohen MS, et al. Local anaesthetics and regional anaesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children. Cochrane Database Syst Rev. 2018;6.
16. Bayman EO, Brennan TJ. Incidence and severity of chronic pain at 3 and 6 months after thoracotomy: meta-analysis. J Pain. 2014;15(9):887–897. doi:10.1016/j.jpain.2014.06.005
17. Pluijms W, Steegers M, Verhagen A, Scheffer G, Wilder‐Smith O. Chronic post‐thoracotomy pain: a retrospective study. Acta Anaesthesiol Scand. 2006;50(7):804–808. doi:10.1111/j.1399-6576.2006.01065.x
18. Mongardon N, Pinton-Gonnet C, Szekely B, Michel-Cherqui M, Dreyfus J-F, Fischler M. Assessment of chronic pain after thoracotomy: a 1-year prevalence study. Clin J Pain. 2011;27(8):677–681. doi:10.1097/AJP.0b013e31821981a3
19. Hetmann F, Kongsgaard UE, Sandvik L, Schou‐Bredal I. Prevalence and predictors of persistent post‐surgical pain 12 months after thoracotomy. Acta Anaesthesiol Scand. 2015;59(6):740–748. doi:10.1111/aas.12532
20. Neil MJ, Macrae WA. Post surgical pain-the transition from acute to chronic pain. Rev Pain. 2009;3(2):6–9. doi:10.1177/204946370900300203
21. McHugh RK, DeVito EE, Dodd D, et al. Gender differences in a clinical trial for prescription opioid dependence. J Subst Abuse Treat. 2013;45(1):38–43. doi:10.1016/j.jsat.2012.12.007
22. Manubay J, Davidson J, Vosburg S, Jones J, Comer S, Sullivan M. Sex differences among opioid-abusing chronic pain patients in a clinical trial. J Addict Med. 2015;9(1):46. doi:10.1097/ADM.0000000000000086
23. Huang CJ. On being the “right” kind of chronic pain patient. Narrative Inquirybioethics. 2018;8(3):239. doi:10.1353/nib.2018.0073
24. Wyatt R. Pain and ethnicity. AMA J Ethics. 2013;15(5):449–454.
25. Zhao S, Chen F, Feng A, Han W, Zhang Y. Risk factors and prevention strategies for postoperative opioid abuse. Pain Res Manage. 2019;2019:2019. doi:10.1155/2019/7490801
26. Grol-Prokopczyk H. Sociodemographic disparities in chronic pain, based on 12-year longitudinal data. Pain. 2017;158(2):313–322. doi:10.1097/j.pain.0000000000000762
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.