Back to Journals » International Journal of General Medicine » Volume 19
Serial C-Reactive Protein Measurements for Prognostication and Antimicrobial Decision-Making in ICU Sepsis Patients: A Retrospective Cohort Study
Authors Al-Dorzi HM ![]() , Aleid AM, Alqahtani AA, Alwarafi AA, Alwahbi SF
, Aleid AM, Alqahtani AA, Alwarafi AA, Alwahbi SF
Received 6 March 2026
Accepted for publication 4 June 2026
Published 15 June 2026 Volume 2026:19 606472
DOI https://doi.org/10.2147/IJGM.S606472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hasan M Al-Dorzi,1– 3 Abdullah Mohammed Aleid,1 Abdulmajid Abdullah Alqahtani,1 Abdulmajed Ali Alwarafi,1 Saleh Fahad Alwahbi1
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Intensive Care Department, King Abdulaziz Medical City, Ministry of National Guard -Health Affairs, Riyadh, Saudi Arabia
Correspondence: Hasan M Al-Dorzi, Intensive Care Department, Mail Code 1425, King Abdulaziz Medical City, Ministry of National Guard -Health Affairs, PO Box 22490, Riyadh, 11426, Saudi Arabia, Email [email protected]
Background: C-reactive protein (CRP) is a widely used biomarker for sepsis management; however, its prognostic value remains uncertain. This study evaluated whether serial CRP measurements are associated with mortality in intensive care unit (ICU) patients with sepsis.
Methods: This retrospective cohort study included adult patients admitted to a tertiary-care ICU between 2020 and 2023, who had at least three serial CRP measurements around days 1, 3, and 7 to guide sepsis management as diagnosed by the treating team. We examined the relationship between CRP levels and 90-day mortality.
Results: The study included 171 patients (median age: 67 years; 55% male). Compared to patients with lower CRP levels, those with day-1 CRP ≥ 75 mg/L (n=87, 50.9%) had similar clinical characteristics, except for a higher prevalence of malignancy. Antibiotic use and clinical outcomes were similar between the groups. Meropenem duration tended to be shorter in patients whose CRP levels decreased from days 1 to 7 than in those whose CRP levels increased (median 7 days vs. 10 days; p=0.06). 42 patients (24.6%) died within 90 days. Compared to survivors, non-survivors had slightly higher CRP levels on day 1 (91 mg/L vs. 70 mg/L, p=0.08) and similar changes in CRP over time. Receiver operating characteristic curve analysis demonstrated that both CRP levels and their temporal changes had poor prediction for 90-day mortality (area under the curve for day-1 CRP, 0.590), with day-1 procalcitonin performing slightly better (area under the curve, 0.658). In the multivariable logistic regression analysis, day-1 CRP was not associated with 90-day mortality.
Conclusion: Serial CRP measurements did not reliably predict mortality in ICU patients with sepsis but may have influenced the antibiotic duration. Routine CRP monitoring in ICU patients with sepsis may have a limited prognostic value.
Plain Language Summary: Sepsis is a serious, potentially life-threatening condition that often requires treatment in the intensive care unit (ICU). One of the blood tests commonly used in these situations is C-reactive protein (CRP) level, which increases in the presence of inflammation or infection. Although CRP is widely measured, it remains uncertain whether repeated CRP results can help to predict which ICU patients with sepsis are more likely to survive. This study examined whether CRP levels measured on days 1, 3, and 7 were associated with death within 90 days.
Our study included 171 adult ICU patients who underwent at least three CRP tests as part of their sepsis management. We compared CRP values and how they changed over time between patients who survived and those who did not. Overall, 24.6% of the patients died within 90 days. Those who died had slightly higher CRP levels on the first day, but the differences were small, and the changes in CRP levels over the week were similar between survivors and non-survivors. CRP levels and trends showed a poor ability to predict which patients would die, indicating that CRP may not be a reliable prognostic tool. Another blood marker, procalcitonin, showed moderately better results. The study also found that CRP levels may have influenced the duration for which physicians continued certain antibiotics such as meropenem.
In summary, our findings suggest that while CRP may assist physicians in some treatment decisions, serial CRP measurements may not be able to predict survival in ICU patients with sepsis.
Keywords: C-reactive protein, mortality, sepsis, biomarkers, intensive care
Introduction
Inflammatory biomarkers are frequently used in critical care settings to detect systemic inflammation, diagnose infections, evaluate disease severity, assess responses to therapy, and predict outcomes.1–6 C-reactive protein (CRP) is a biomarker produced by the liver in response to interleukin-6 following inflammation or cellular damage.1 CRP levels can increase up to 1000 times as compared with normal physiological conditions.1 CRP can activate the complement pathway by binding to ligands such as lipoproteins, and has an anti-inflammatory effect by inhibiting neutrophils and platelet-activating factors that slow the aggregation process.1
CRP is a widely used laboratory marker7 that has been studied across different patient populations, including those with cancer, heart failure, stroke, venous thromboembolism, general critical illness, and sepsis.7,8 In the intensive care unit (ICU) setting, many observational studies explored CRP utility in clinical practice using different methodologies. For example, a multicenter prospective observational study of 813 general ICU patients in China found that lower baseline CRP levels were associated with lower ICU mortality, and baseline CRP levels > 62.8 mg/L were independently associated with an almost two-fold increase in ICU mortality on multivariable logistic regression analysis.9 Similarly, a multicenter retrospective study from Sweden involving 851 patients with sepsis reported that admission CRP levels >100 mg/L were associated with increased ICU and 30-day mortality as well as prolonged stays in the ICU and hospital among survivors.10 A multicenter prospective cohort study from Portugal evaluated the daily CRP levels in 891 ICU patients with community-acquired pneumonia and found no significant differences in CRP levels between survivors and non-survivors until the third day of antibiotic treatment.2 CRP levels decreased faster in patients who responded to treatment than in those who did not.2 Despite these findings, other studies questioned the clinical value of CRP, with a systematic review)60 studies and 15681 patients) reporting that CRP did not predict 30-day mortality in critically ill patients with sepsis.11
Despite the uncertainty and challenges surrounding the application and interpretation of inflammatory biomarkers3,12 clinicians often place considerable weight on CRP levels when making management decisions, which may lead to inappropriate use.7 As the relationship between CRP levels and clinical outcomes in ICU patients remains controversial, our study aimed to evaluate whether baseline CRP levels and their serial changes influence clinical management and predict mortality in critically ill patients with sepsis.
Materials and Methods
Patients and Setting
This retrospective cohort study evaluated critically ill patients admitted to the adult Intensive Care Department of King Abdulaziz Medical City in Riyadh, Saudi Arabia. The Intensive Care department has eight different units that admit different types of critically ill patients, with six medical teams performing daily multidisciplinary rounds. Each ICU medical team consisted of one ICU consultant, one staff physician/fellow, and 2–4 residents. Patients were eligible for this study if they were adults (age ≥ 18 years), were admitted to the ICU between January 1, 2020, and December 31, 2023, had an ICU stay of at least 3 days, received antibiotics for sepsis that was clinically suspected or confirmed by the treating ICU team at the first CRP measurement; all patients were subsequently diagnosed to have sepsis and had at least three CRP measurements on different days within 8 days. In our hospital, CRP levels were measured using immunoturbidimetry (Abbott Alinity CI series; Abbott, Illinois, USA). The normal CRP level was up to 5 mg/L.
Data Collection
The collected data included demographic information, medical history (chronic cardiovascular disease, chronic respiratory disease, chronic kidney disease, stroke, cancer, diabetes, and hypertension), admission category (medical, surgical, and trauma), admission Glasgow Coma Scale score, and sepsis-related variables (confirmed vs. suspected at the time of the first CRP measurement, community-acquired vs. hospital-acquired, infection source, culture results, antibiotic therapy, and duration of meropenem therapy). We recorded the following laboratory results: white blood cell count, hemoglobin, creatinine, bilirubin, international normalized ratio, albumin, lactate levels, COVID-19 status, CRP levels on day 1, CRP on day 3–5, CRP on day 6–8, and procalcitonin levels on the same days. We also noted selected management interventions in the ICU including vasopressor use, invasive mechanical ventilation, and renal replacement therapy.
Outcome data in this study included vital status at 30-day and 90-day and hospital mortality, and length of stay (LOS) in the ICU and hospital. Because 30-day mortality was low and hospital LOS was prolonged in most patients, we considered 90-day mortality as the primary outcome.
Statistical Analysis
A modified Sequential Organ Failure Assessment (SOFA) score,13 which assess the severity of illness, was calculated using available variables (creatinine, bilirubin, Glasgow Coma Scale, vasopressor use, and mechanical ventilation status). The respiratory component was simplified by assigning 3 points for mechanical ventilation and 0 for no mechanical ventilation. The cardiovascular component was scored as 3 for any vasopressor use and 0 for no vasopressor use. The coagulation component was omitted because platelet counts were unavailable. This approach has been used in prior retrospective studies when complete SOFA data were not obtainable.14
We calculated the changes in CRP between days 3–5 and day 1 as follows: CRP on day 3 minus CRP on day 1, divided by CRP on day 1. We calculated the changes in CRP between days 6–8 and day 1 as follows: CRP on day 7 minus CRP on day 1, divided by CRP on day 1. Similarly, we calculated the changes in procalcitonin levels. We used two approaches to compare patients. First, to explore the clinical implications of initial CRP levels, we compared patients with higher and lower CRP levels on day 1. This approach aimed to identify factors associated with elevated CRP levels and their corresponding outcomes. Second, we compared patients who died within 90 days with those who survived to assess the relationship between baseline CRP levels, their temporal changes and mortality.
Continuous data are presented as medians with interquartile ranges (IQRs), and categorical variables as frequencies and percentages. Group comparisons were performed using Student’s t-test or Mann–Whitney U-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. We performed receiver operator characteristic (ROC) analysis to assess the discriminative ability of CRP levels on days 1, 3, and 7, changes in CRP and procalcitonin levels on days 1, 3, and 7, and changes in procalcitonin to predict 90-day mortality and reported their area under the curve (AUC). We also conducted stepwise multivariable logistic regression analysis, applying backward elimination based on the likelihood ratio test to determine if a CRP level > vs. < 75 mg/L on day 1 was a risk factor for 90-day mortality (binary variable). Clinically significant variables (age, sex, body mass index, chronic comorbidities [diabetes, hypertension, chronic cardiovascular disease, chronic respiratory disease, chronic kidney disease, stroke, and cancer], admission Glasgow Coma Scale score, confirmed vs. suspected sepsis at the time of the first CRP measurement, community-acquired vs. hospital-acquired sepsis, baseline laboratory tests [white blood cell count, hemoglobin, creatinine, bilirubin, international normalized ratio, albumin and lactate levels], modified SOFA score, vasopressor therapy, and mechanical ventilation) were entered into the model as independent variables. In the model, we imputed the missing values for the continuous variables by their respective medians, as most variables were non-normally distributed. The results are presented as odds ratios (OR) with 95% confidence intervals (CI). All statistical analyses were performed using the SPSS version 15. Statistical significance was defined as a two-sided p-value < 0.05.
Results
Characteristics of Patients
The study cohort consisted of 171 patients with a median age of 67 years (IQR, 56–77 years), 55% male, and a median modified SOFA score of 5 (IQR, 2–7) (Table 1). Most patients were admitted to the medical service (64.9%), followed by surgery (23.4%) and hematology/oncology (11.7%). Chronic comorbidities were also common. The median CRP level on day 1 was 76 mg/L (IQR 20, 148). 84 patients (49.1%) had the first CRP < 75 mg/L and 87 (50.9%) ≥ 75 mg/L. Compared to patients with lower CRP levels, those with CRP levels ≥ 75 mg/L had similar demographics and clinical characteristics, except for a higher prevalence of malignancy (35.6% vs. 14.3%, p=0.001) and lower albumin levels. Forty-two patients (24.6%) died within 90 days and tended to be older (median age 70.5 vs. 66 years, p=0.06), with more admissions under hematology/oncology (31% vs. 5.4%, p<0.0001) and higher median SOFA score (6 vs.s 4, p=0.01) (Table 1).
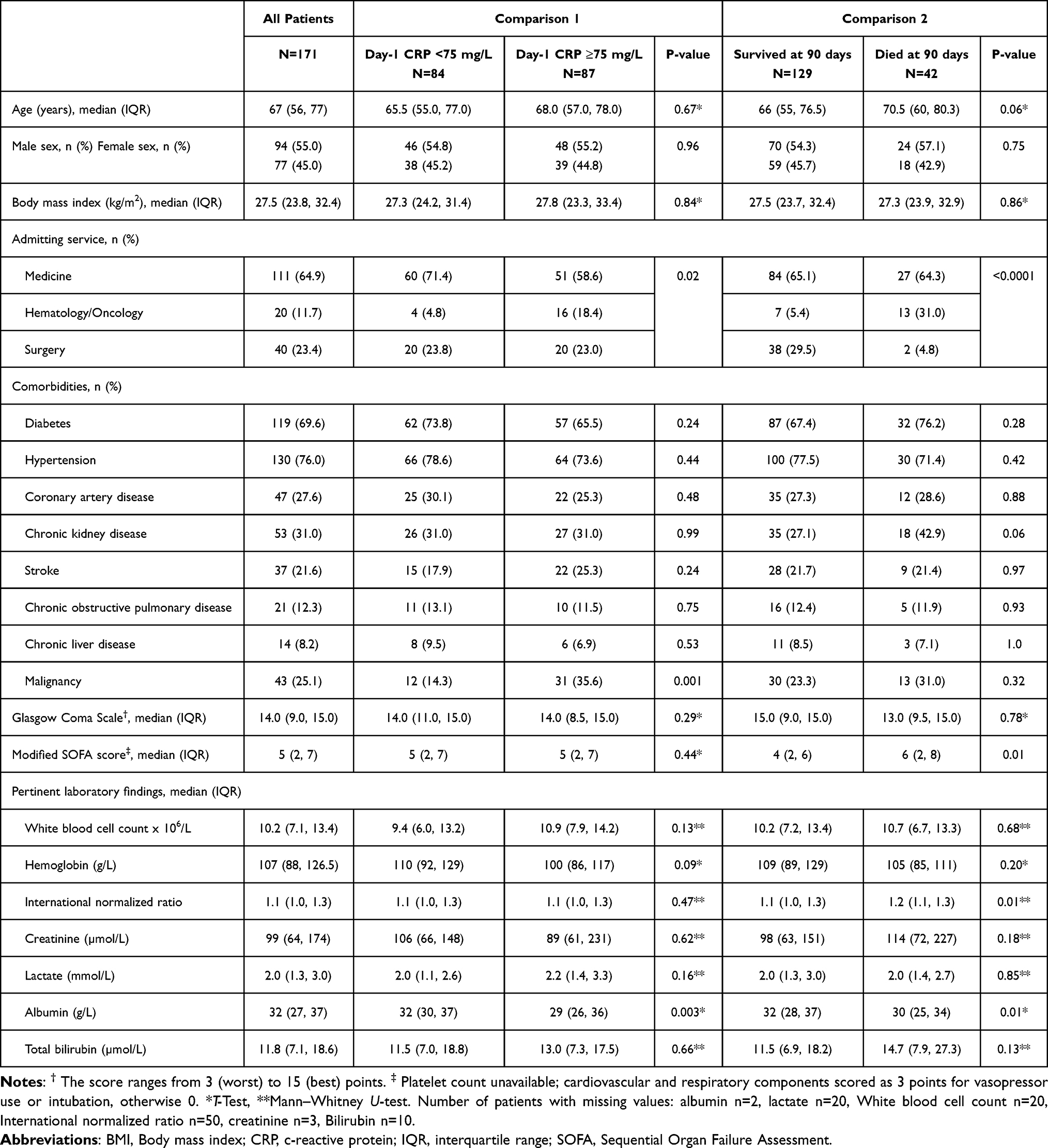 |
Table 1 Characteristics of the Study Cohort Using Two Comparison Groups: Baseline CRP <75 vs. ≥75 mg/L, and 90-Day Outcome (Survivors vs. Non-Survivors) |
Sepsis Characteristics and Diagnostic Workup, Including CRP Levels
Table 2 presents data related to sepsis. Among the 171 patients, sepsis was suspected in 64.3% and confirmed in 35.7% of patients when the first CRP level was measured. The most common source of infection was respiratory infection (36.2%). Multidrug-resistant organisms from different sources were identified in 17.5% of the patients. COVID-19 and influenza were detected in 20.8% and 3.7% of the patients, respectively. The CRP levels on days 1, 3, and 7 were 76 mg/L, 78 mg/L, and 73 mg/L, respectively. The CRP/albumin ratio on day 1 was 2.2. The proportional changes in CRP from day 1 to day 3 and from day 1 to day 7 were 0.00 and −0.08, respectively. Procalcitonin levels on days 1, 3, and 7 were 0.31, 0.43, and 0.31 ng/mL, respectively. The proportional changes in procalcitonin were 0.14 and 0.20, respectively.
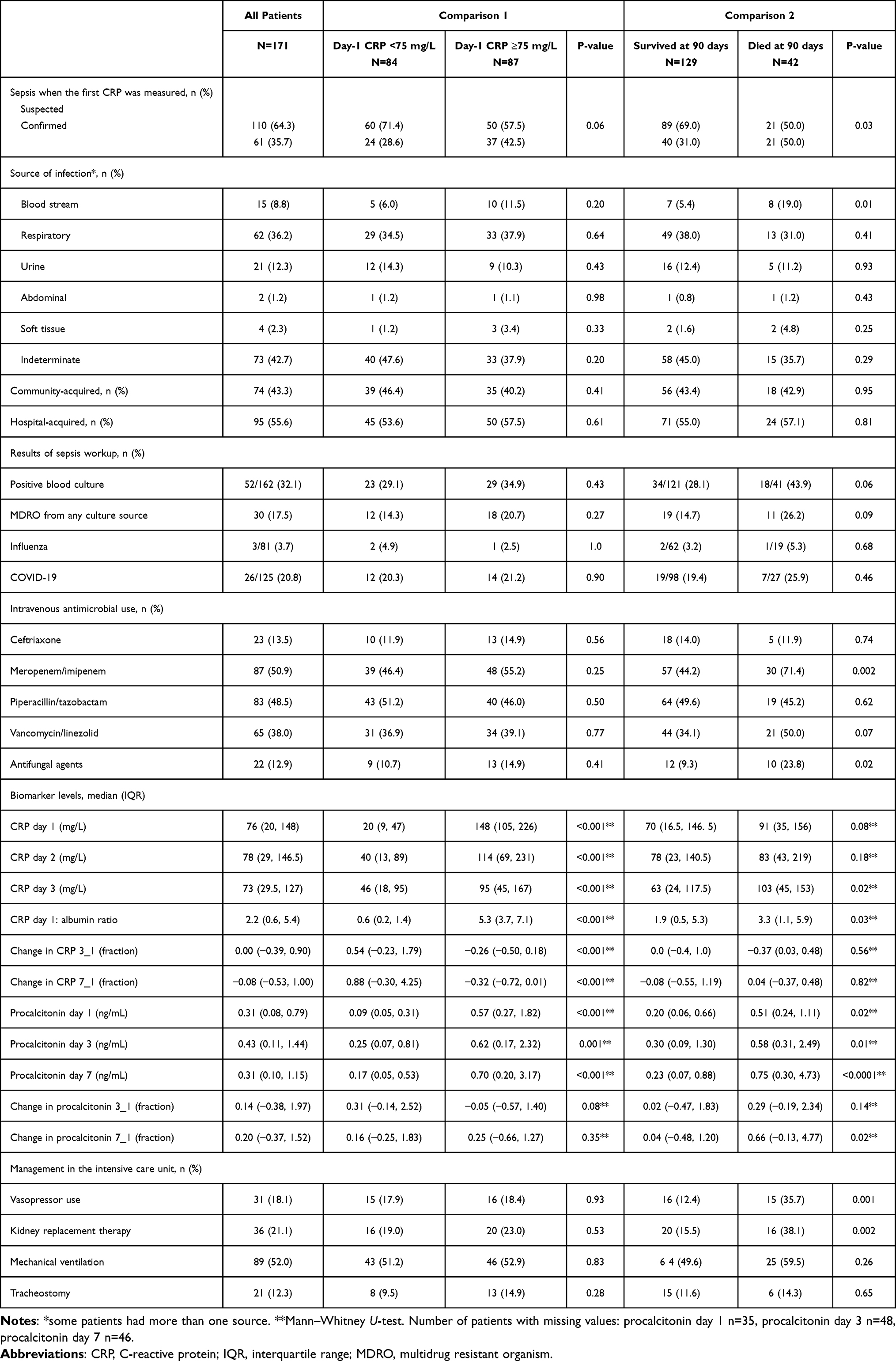 |
Table 2 Sepsis Workup Results and Key Management in the Intensive Care Unit for the Study Cohort. We Used Two Comparison Groups: Baseline CRP <75 vs. ≥75 mg/L, and 90-Day Outcome (Survivors vs. Non-Survivors) |
Compared to survivors, non-survivors had a significantly higher rate of confirmed sepsis (50.0% vs. 31.0%, p=0.03), bloodstream infections (19.0% vs. 5.4%, p=0.01), and multidrug-resistant organisms (26.2% vs. 14.7%, p=0.09). Figure 1A shows the serial CRP measurements. The CRP level on day 1 was slightly higher in the non-survivors (p=0.08). CRP/albumin on day 1 and CRP on day 7 were significantly higher in the non-survivors (p=0.020 and p=0.03, respectively). However, the proportional changes in the CRP levels over time were similar. Procalcitonin levels on days 1, 3, and 7 were significantly higher in non-survivors, especially on day 7 (p<0.0001), with a proportional change from day 1 to day 7 (p=0.02) (Figure 1B).
 |
Figure 1 Box plots for C-reactive protein (A) and procalcitonin (B) levels on days 1, 3 and 7 in patients who died and did not die at 90 days after hospital admission. Circles indicate mild outliers. Stars indicate extreme outliers. |
Sepsis Management
Meropenem/imipenem (50.9%) and piperacillin/tazobactam (48.5%) were the most commonly administered antibiotics used. Among these patients, 18.1% required vasopressors, 21.1% underwent renal replacement therapy, and 52.0% required mechanical ventilation. The median number of administered antibiotics was one in the low CRP group (IQR: 1, 2) and two in the high CRP group (IQR: 1, 3; p=0.46). Although meropenem duration was similar between the high and low CRP groups, it tended to be shorter in patients who had a decrease in CRP levels from days 1 to 7 (median 7 days [IQR: 5–10]) than in those whose CRP levels increased (median 10 days [IQR: 7–14]; p=0.06). ICU interventions did not differ significantly between the two CRP groups. Surprisingly, no association was observed between meropenem duration and PCT changes over time.
In contrast, when comparing survivors with non-survivors, antibiotic and ICU management patterns differed significantly. Non-survivors were more likely to receive broad-spectrum antibiotics such as meropenem/imipenem (71.4% vs. 44.2%, p=0.002; similar meropenem duration) and antifungal therapy (23.8% vs. 9.3%, p=0.02). They also received more intensive support including vasopressors (35.7% vs. 12.4%, p=0.001) and renal replacement therapy (38.1% vs. 15.5%, p=0.002) (Table 2).
Outcomes
In the study cohort, 30-day mortality rate were 11.7%, 90-day mortality 24.6%, and hospital mortality reached 29.8%, respectively (Table 3). Patients with lower and higher baseline CRP levels had similar outcomes, with 30-day mortality rates of 8.37% and 14.9%, respectively (p=0.18) and hospital mortality rates of 25.0% and 34.5%, respectively (p=0.18). The 90-day mortality rate in the high CRP group was 29.9% compared with 19.0% in the lower CRP group (p=0.10). ROC curve analysis revealed that CRP on day1 had poor discrimination between 90-day survivors and non-survivors (AUC 0.590, 95% CI 0.498–0.681) (Figure 2A and Table 4). Changes in CRP levels from day 1 to days 3 and 7 also did not predict mortality (AUC 0.470, 95% CI 0.377–0.562 and AUC 0.512, 95% CI 0.423–0.601, respectively). Procalcitonin levels were more accurate in predicting 90-day mortality (Figure 2B and Table 4). On multivariable logistic regression analysis, the CRP level on day 1 was not associated with 90-day mortality. The significant risk factors were age (OR per one-year increment, 1.044, 95% CI 1.010–1.079, p=0.01), hypertension (OR 0.138, 95% CI 0.041–0.462, p=0.001), chronic kidney disease (OR 2.720, 95% CI 1.039–7.121, p=0.04), and modified SOFA score (OR per unit increment 1.208, 95% CI 1.066–1.369, p=0.003).
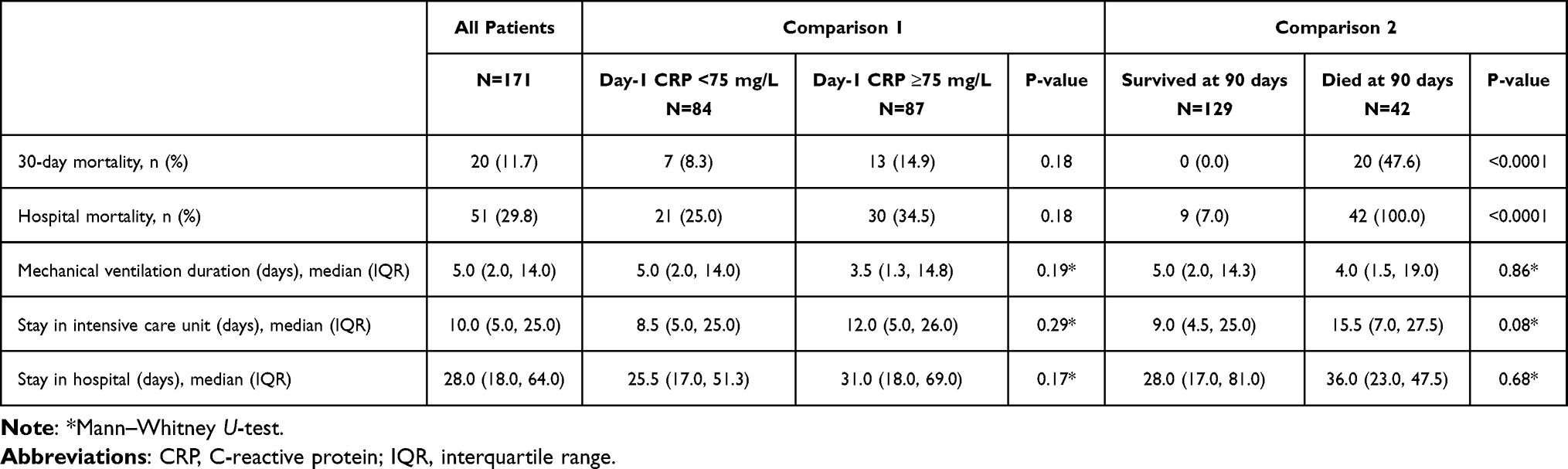 |
Table 3 Other Outcomes of the Study Cohort. We Used Two Comparison Groups: Baseline CRP <75 vs. ≥75 mg/L, and 90-Day Outcome (Survivors vs. Non-Survivors) |
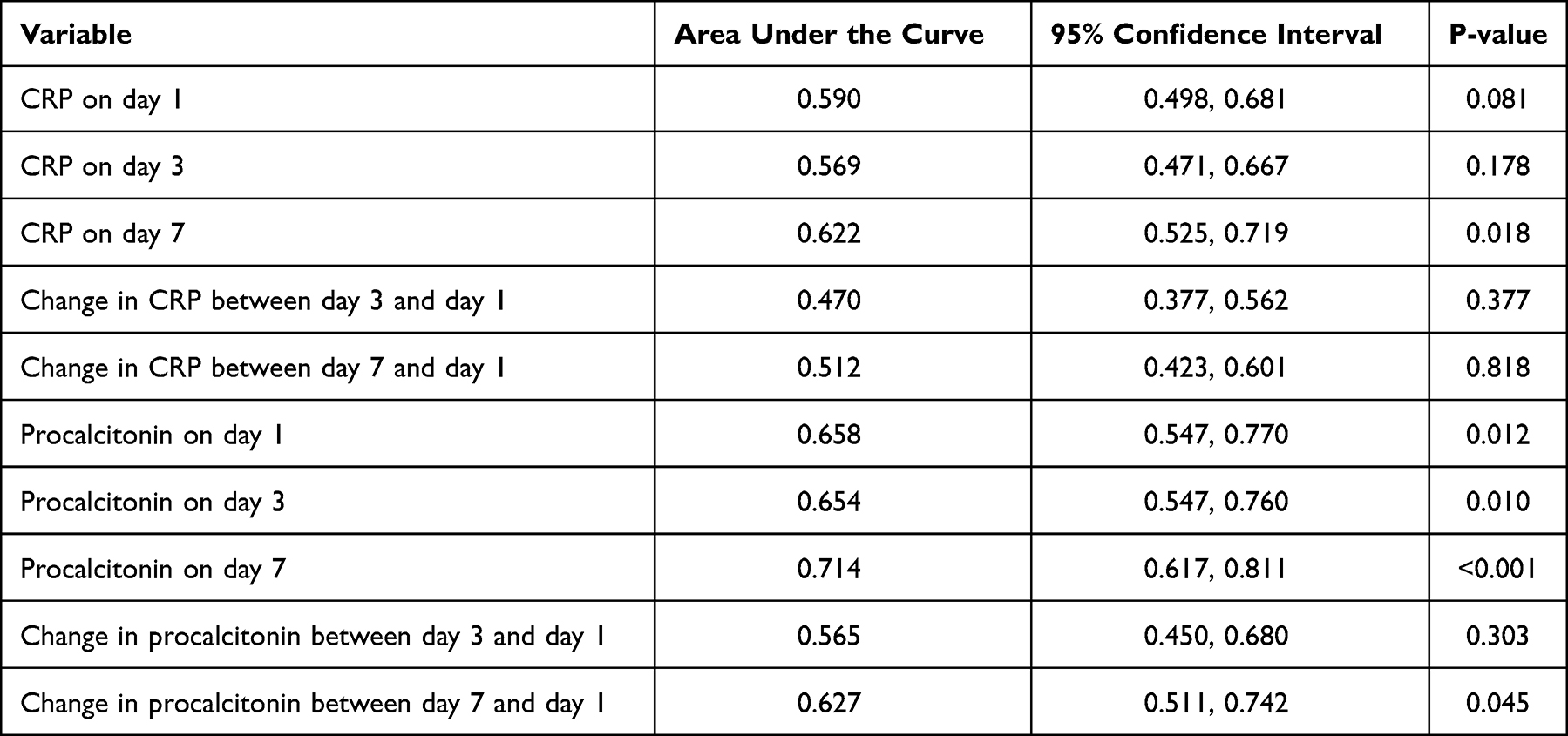 |
Table 4 Receiver Operating Characteristic Curve Analysis for Ability of C-Reactive Protein (CRP) and Procalcitonin Levels, and Their Temporal Changes, to Predict 90-Day Mortality |
 |
Figure 2 Receiver operating characteristic (ROC) curve analysis evaluating the ability of C-reactive protein (CRP) levels and their changes over time (A) and procalcitonin levels and their changes over time (B) to predict 90-day mortality. |
There were no differences in other outcomes, including duration of mechanical ventilation and length of stay in the ICU and hospital, between the lower and higher CRP groups and 90-day survivors and non-survivors, except for a slightly longer LOS in the ICU for non-survivors (15.5 vs. 9.0 days, p=0.08) (Table 3).
Discussion
Several inflammatory markers are used during critical illness for diagnostic, risk stratification, management, and prognostic purposes and may be used as part of individualized medicine.4,5 These biomarkers include white blood cell count, differential cell ratios, erythrocyte sedimentation rate, and acute phase proteins such as CRP and procalcitonin.4,5 CRP is a fast, easy-to-use, and cost-effective measurement. It has become a routinely used test in the management of hospitalized patients.7,8 In sepsis, one of the main clinical applications of CRP in sepsis is to guide antibiotic therapy. A meta-analysis of three randomized controlled trials, including 727 hospitalized patients with sepsis, found that CRP-guided management reduced the antibiotic duration by almost 2 days without a significant increase in mortality.6 A similar finding was observed in a trial involving patients with community-acquired pneumonia.15 However, a recent multicenter trial in 2760 ICU adults patients with suspected sepsis found that while a procalcitonin-guided protocol shortened antibiotic duration, a CRP-guided protocol did not provide benefits compared with standard care.16 We found a trend for a shorter meropenem duration in patients who had CRP levels decreased from days 1 to 7, suggesting that clinicians may have incorporated serial CRP measurements into antibiotic decision-making.
Our findings showed that baseline CRP level was not independently associated with 90-day mortality in ICU patients with sepsis. Multiple observational studies have demonstrated that CRP has prognostic value;9,10 however, this was not observed in other studies. Our findings align with those of a systematic review in which the baseline CRP level in critically ill patients was not associated with mortality at 28–30 days (OR 1.01, 95% CI 0.87–1.17), even after adjusting for covariates such as age and severity score.11 Other biomarkers, including baseline procalcitonin and interleukein-6, did not perform better.11 Heterogeneity across studies, including differences in patient characteristics and study methodologies, likely contributes to the variability in the reported findings. For example, one study found that CRP levels were higher in gram-negative infections than in gram-positive infections17 suggesting that the prognostic performance of a biomarker may be affected by patient characteristics, which may vary across studies.
We also found that CRP changes over time (days 3 and 7) did not have a better predictive accuracy for mortality than baseline CRP. In contrast, Povoa et al found that CRP levels decreased faster in patients with community-acquired pneumonia who responded to treatment than in non-responders.2 Another study found that changes in CRP were significantly associated with mortality in patients with sepsis but with poor discriminatory ability (AUC 0.629).18 In a large ICU cohort of 1464 patients with sepsis, four CRP trajectories were identified: persistently low, intermediate, gradually increasing, and persistently high.19 The multiple logistic regression analysis showed that patients with persistently high and unexpectedly low CRP levels had a higher risk of in-hospital mortality than those with intermediate CRP levels.19 Our findings further challenge the assumption that CRP kinetics is a reliable prognostic marker in critically ill patients with sepsis.
In the present study, procalcitonin outperformed CRP in the prediction of mortality. In contrast to CRP, procalcitonin levels were significantly higher in non-survivors at all time points and showed better discrimination of the 90-day mortality. This supports growing evidence that procalcitonin may be a more robust biomarker for risk stratification in sepsis. A systematic review of 44 studies performed between 1997 and 2024 with 10755 patients, procalcitonin exhibited a higher pooled AUC of 0.74 (95% CI 0.62–0.84) than CRP, which had an AUC of 0.67 (95% CI 0.56–0.77).20 The 2026 international guidelines for sepsis management discourage procalcitonin for antibiotic initiation but suggests its use, with clinical judgment, to guide discontinuation.21
The strengths of this study include real-world data from a high-volume tertiary ICU in Saudi Arabia, serial CRP measurements, and evaluation of the clinical significance of CRP levels using different statistical methods. However, this study has several limitations. First, the retrospective observational design is prone to confounding, and the single-center data and inclusion of patients with at least 3 different CRP measurements within 8 days may have excluded the sickest patients and early deaths, introducing selection bias and limiting generalizability of our findings. Second, the sample size (171 patients with 42 death events within 90 days) was relatively small, which may have underpowered our ability to detect significant associations. The small number of early deaths further reduced power to study the association between CRP levels and short-term outcomes. Third, we were not able to verify whether Sepsis-3 criteria or other sepsis definitions were applied by the ICU team for sepsis diagnosis. Fourth, we could not calculate the full SOFA score because of unavailable data. While modified SOFA scores are used in retrospective analysis, they may affect the accuracy of illness-severity assessment and subsequent inferential analysis. Fifth, factors such as infection source control, antibiotic appropriateness, and the timing of interventions were not evaluated and may have influenced the outcomes and the observed associations. Lastly, many patients had missing procalcitonin level data, preventing robust comparison with CRP.
Conclusions
In this study, serial CRP measurements appeared to influence antimicrobial decision-making, but did not reliably differentiate survivors from non-survivors, challenging the assumption that CRP kinetics serve as robust indicators of outcome in critically ill patients. This suggests that the prognostic utility of CRP in sepsis is limited and supports a more cautious and context-specific use of CRP in prognostication. Our study highlights the critical need for rigorous, prospective, multicenter studies to clearly define the role of inflammatory biomarkers in sepsis management.
AI Declarations
All authors declare that AI tools were not utilized in the writing of the manuscript, creation of images, or collection and analysis of the data.
Data Sharing Statement
Data supporting the findings of this study are available upon request from the corresponding author. The data were not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia (study number: NRR24/038/8; IRB approval no: 0000036924). As the study was retrospective, with no direct contact with the patients, the requirement for informed consent was waived. This study was conducted in accordance with the guidelines of the Declaration of Helsinki (2000) and Good Clinical Practice E6 (R2).
Acknowledgment
The authors acknowledge the faculty of the Research Unit of the College of Medicine, King Saud bin Abdulaziz University for Health Sciences for their support. The authors confirm that the manuscript has not been published on any website or printed journal in any language other than English.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any direct or indirect financial contributions or support from any organization or donor for the completion of this research.
Disclosure
The authors declare no competing interests in this work.
References
1. Lelubre C, Anselin S, Zouaoui Boudjeltia K, Biston P, Piagnerelli M. Interpretation of C-reactive protein concentrations in critically ill patients. Biomed Res Int. 2013;2013(1):124021. doi:10.1155/2013/124021
2. Povoa P, Teixeira-Pinto AM, Carneiro AH, Portuguese Community-Acquired Sepsis Study Group S. C-reactive protein, an early marker of community-acquired sepsis resolution: a multi-center prospective observational study. Crit Care. 2011;15(4):R169. doi:10.1186/cc10313
3. Heffernan AJ, Denny KJ. Host diagnostic biomarkers of infection in the ICU: where are we and where are we going? Curr Infect Dis Rep. 2021;23(4):4. doi:10.1007/s11908-021-00747-0
4. Heilmann E, Gregoriano C, Schuetz P. Biomarkers of infection: are they useful in the ICU? Semin Respir Crit Care Med. 2019;40(4):465–11. doi:10.1055/s-0039-1696689
5. Germolec DR, Shipkowski KA, Frawley RP, Evans E. Markers of Inflammation. Methods Mol Biol. 2018;1803:57–79.
6. Dias RF, De Paula ACRB, Hasparyk UG, et al. Use of C-reactive protein to guide the antibiotic therapy in hospitalized patients: a systematic review and meta-analysis. BMC Infect Dis. 2023;23(1):276. doi:10.1186/s12879-023-08255-3
7. Plebani M. Why C-reactive protein is one of the most requested tests in clinical laboratories? Clin Chem Lab Med. 2023;61(9):1540–1545. doi:10.1515/cclm-2023-0086
8. Singh B, Goyal A, Patel BC. C-Reactive Protein: clinical Relevance and Interpretation. In: StatPearls. Treasure Island (FL); 2025.
9. Qu R, Hu L, Ling Y, et al. C-reactive protein concentration as a risk predictor of mortality in intensive care unit: a multicenter, prospective, observational study. BMC Anesthesiol. 2020;20(1):292. doi:10.1186/s12871-020-01207-3
10. Koozi H, Lengquist M, Frigyesi A. C-reactive protein as a prognostic factor in intensive care admissions for sepsis: a Swedish multicenter study. J Crit Care. 2020;56:73–79. doi:10.1016/j.jcrc.2019.12.009
11. Molano-Franco D, Arevalo-Rodriguez I, Muriel A, et al. Basal procalcitonin, C-reactive protein, interleukin-6, and presepsin for prediction of mortality in critically ill septic patients: a systematic review and meta-analysis. Diagn Progn Res. 2023;7(1):15. doi:10.1186/s41512-023-00152-2
12. Moniz P, Coelho L, Povoa P. Antimicrobial stewardship in the intensive care unit: the role of biomarkers, pharmacokinetics, and pharmacodynamics. Adv Ther. 2021;38(1):164–179. doi:10.1007/s12325-020-01558-w
13. Vincent J-L, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine (see contributors to the project in the appendix). Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
14. Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317(3):290–300. doi:10.1001/jama.2016.20328
15. Duijkers R, Prins HJ, Kross M, et al. Biomarker guided antibiotic stewardship in community acquired pneumonia: a randomized controlled trial. PLoS One. 2024;19(8):e0307193. doi:10.1371/journal.pone.0307193
16. Dark P, Hossain A, McAuley DF, et al. Biomarker-guided antibiotic duration for hospitalized patients with suspected sepsis: the ADAPT-sepsis randomized clinical trial. JAMA. 2025;333(8):682–693. doi:10.1001/jama.2024.26458
17. Tang A, Shi Y, Dong Q, et al. Prognostic differences in sepsis caused by gram-negative bacteria and gram-positive bacteria: a systematic review and meta-analysis. Crit Care. 2023;27(1):467. doi:10.1186/s13054-023-04750-w
18. Toker AK, Çelik İ, Özdemir AT, et al. The value of C-reactive protein velocity (CRPv) on mortality in sepsis patients who are emergently hospitalized in the ICU: a retrospective single-center study. Heliyon. 2024;10(19):1.
19. Jiang X, Zhang C, Pan Y, Cheng X, Zhang W. Effects of C-reactive protein trajectories of critically ill patients with sepsis on in-hospital mortality rate. Sci Rep. 2023;13(1):15223. doi:10.1038/s41598-023-42352-2
20. Chuang C-L, Yeh H-T, Niu K-Y, Chen C-B, Seak C-J, Yen -C-C. Diagnostic performances of procalcitonin and C-reactive protein for sepsis: a systematic review and meta-analysis. Eur J Emerg Med. 2025;32(4):248–258. doi:10.1097/MEJ.0000000000001235
21. Prescott HC, Antonelli M, Alhazzanic W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2026. Intensive Care Med. 2026;52:1–74. doi:10.1007/s00134-025-08213-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.