Back to Journals » Infection and Drug Resistance » Volume 15
Septic Arthritis Complicating Arthroscopic Anterior Cruciate Ligament Reconstruction: An Experience from a Tertiary-Care Hospital
Authors El-Kady RAE, ElGuindy AMF
Received 3 April 2022
Accepted for publication 6 July 2022
Published 13 July 2022 Volume 2022:15 Pages 3779—3789
DOI https://doi.org/10.2147/IDR.S369240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Rania Abd El-Hamid El-Kady,1,2 Ahmed Mahmoud Fouad ElGuindy3,4
1Department of Medical Microbiology and Immunology, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 2Department of Pathological Sciences, Fakeeh College for Medical Sciences, Jeddah, Kingdom of Saudi Arabia; 3Department of Orthopedic Surgery, Faculty of Medicine, Fayoum University, Fayoum, Egypt; 4Department of Orthopedic and Spine Surgery, Dr. Soliman Fakeeh Hospital, Jeddah, Kingdom of Saudi Arabia
Correspondence: Rania Abd El-Hamid El-Kady, Department of Pathological Sciences, Fakeeh College for Medical Sciences, P.O. Box 2537, Jeddah, 21461, Kingdom of Saudi Arabia, Tel +966569849897, Email [email protected]
Background: Septic arthritis (SA) of the knee following anterior cruciate ligament reconstruction (ACLR) is considered a catastrophic complication in terms of reduced or loss function of the involved joint. The aims of this study were to gauge the incidence, risk factors, and causative organisms of SA after ACLR.
Methods: We conducted a retrospective review of 836 patients who underwent primary ACLR at our institution from October 2018 to September 2021. Patients’ demographics, onset of presentation, clinical symptoms, laboratory findings, and management details were obtained from patients’ electronic medical records.
Results: Out of the 836 primary ACLRs, 12 were complicated with SA (1.43%). Independent risk factors associated with SA included age (OR; 11.12, 95% CI; 1.3– 94.97), obesity (OR; 8.51, 95% CI; 1.02– 71.13), and diabetes mellitus (OR; 12.58, 95% CI; 2.39– 66.3). Staphylococcus aureus was the most frequent culprit organism (66.7%), followed by Streptococcus species (25%), and Pseudomonas aeruginosa (8.3%). No fungal, mycobacterial, or polymicrobial growth were recovered from synovial fluid cultures. All of the infected cases underwent arthroscopic joint lavage and debridement in the operating room followed by intravenous antibiotics. Graft removal was not done in any of the involved patients, with eradication of infection in all cases.
Conclusion: SA after ACLR is uncommon, with S. aureus identified in about two-thirds of the patients. Prompt diagnosis and treatment are crucial to avoid graft loss and arthritis-associated joint damage. Orthopedic surgeons should consider rigorous implementation of infection control strategies to minimize the incidence of this devastating morbidity.
Keywords: ACL, reconstruction, synovial fluid, sepsis, arthritis, antibiotics
Introduction
The anterior cruciate ligament (ACL) plays key roles in providing stability of the knee joint.1 It restrains excessive anterior translation of the tibia relative to the femur, thus impeding hyperextension of the knee joint.2 In addition, it has proprioceptors that detect changes in the location of the knee joint, as well as direction and speed of movement.3
Globally, tears of the ACL are one of the most frequent orthopedic injuries of the knee joint,4 with a yearly incidence exceeding 2 million cases.5 In the United States, about 200,000 ACL ruptures occur annually, with nearly half of which undergo reconstructive procedures.6 Injuries usually evolve from unexpected alteration in the direction, or sudden deceleration while running that can occur in sports involving pivoting actions like basketball, football, and gymnastics.7 Unfavorable consequences of ACL injury include knee joint instability, meniscal and chondral destruction, and higher incidence of osteoarthritis.8 To retrieve the stability of the knee joint, ACL reconstruction (ACLR) is widely accepted as the gold-standard treatment for active people.9 A growing rise in the rate of ACLR in adults and teenagers is observed worldwide secondary to increased incidence of ACL ruptures and the need to resume the active lifestyle, in addition to the current availability of innovative surgical techniques for ACLR.10
Septic arthritis (SA) is an uncommon, but potentially a disastrous sequela of ACLR. The estimated incidence ranges from 0.14% to 2.6%.11 Patients who develop this serious complication generally present with a painful knee joint associated with a restricted range of motion, prolonged joint swelling, local erythema, and fever.12 An earlier study demonstrated that diabetic patients and those who had received hamstring autografts were more likely to develop postoperative SA.13 Furthermore, smoking was identified as a risk factor in another series.14
Previous data indicate that Staphylococcus species are the most commonly encountered organisms, with coagulase-negative staphylococci (CoNS) involved in 43% of the episodes followed by Staphylococcus aureus.15 On the flip side, mycotic infections complicating ACLR are extremely rare with 14 cases had been documented so far. They are associated with worse functional outcomes in comparison to Staphylococcal arthritis.16 Recently, non-tuberculous mycobacterial (NTM) knee SA has been described in the literature.17
Although SA is relatively infrequent after ACLR, orthopedic surgeons are likely to be confronted with challenging scenarios. Thereby, timely case identification and management is crucial to prevent the incidence of further deleterious effects. The primary objectives of the present study were to determine the incidence, risk factors, and causative organisms of SA following ACLR retrospectively, during a 3-year study period, from Dr. Soliman Fakeeh Hospital (DSFH), Jeddah, Kingdom of Saudi Arabia (KSA).
Patients and Methods
Study Eligibility, Design and Setting
The design of this retrospective cohort study was granted approval by the Institutional Review Board (IRB) of DSFH (Decision No. 234/IRB/2021). During the study period, all adult patients (>18 years) who underwent primary arthroscopic ACLR at the Department of Orthopedic and Spine Surgery of DSFH between October 2018 and September 2021 were eligible for our study.
Surgical Technique of Arthroscopic ACLR and Graft Harvest
Our patients were operated upon by 5 different surgeons who followed a standardized surgical technique. All of the recruited patients received a single bolus dose (2 g) of intravenous cefazoline 30 minutes’ pre-operative. A tourniquet was placed at the base of the thigh with the lower limb held in Ç Clamp at the end of the table. The incision site was washed with betadine soap sponge, then dried with sterile sponge. Skin asepsis was done by the operating room nurse using povidone iodine followed by 70% alcohol. Draping was completed by sterile disposable drapes.
The involved limb was exsanguinated by elevation for 5 minutes after tourniquet inflation to 300 mmHg. Hamstring tendon autograft was used in all of the operated patients. To accomplish that, semitendinosus (± gracilis) tendons were harvested through an oblique incision over their insertions at the proximal medial tibia using 2 right-angle forceps and an open tendon stripper. After harvest, the grafts were pre-tensioned on a preparation tray and wrapped in square gauze, soaked in 1 ampoule of gentamicin 80 mg solution. Grafts remained wrapped for at least 15 minutes. In each case, the femoral and the tibial tunnels were drilled, while the graft was prepared.
During the arthroscopic stage of the procedure, a standard anterolateral viewing portal and an anteromedial working portal were established. Knee examination was done and associated conditions were managed according to practice guidelines. Remnants of the native ACL were preserved as much as possible. Throughout the procedure, the knee was irrigated with a sterile normal saline solution. Femoral fixation was completed with a 20 mm button (Arthrex Inc., Florida 34108–1945 USA), and the tibial side was fixed with a TightRope Attachable Button System (ABS). Wound closure was done in layers with the outer layer closed with absorbable monofilament (Monocryl; Ethicon, Bridgewater, New Jersey, USA). Surgical dressing was done using povidone iodine and sterile non-marked gauze. A sterile cotton pad was used to wrap the knee, with a knee immobilizer applied from mid-thigh to mid-leg.
Postoperative intravenous 2 g of cefazoline was administered every 8 hours (5 doses), followed by oral cefuroxime 500 mg twice/day for 7 days. The surgical dressing was replaced between the third and fifth days postoperative. Patients were followed-up on days 5, 10, and 14 postoperative, then every month thereafter. All of the operated patients were advised of a post-surgical standard rehabilitation protocol by a physical therapist.
Identification of Patients Complicated with Septic Arthritis
During the post-operative follow-up visits at the Outpatient Clinics of Orthopedic and Spine Surgery, any patient presented with symptoms suggestive of knee SA (eg, intense pain, joint swelling, discharge from the incision site, poor range of motion, chills, and fever) was subjected to the following laboratory investigations: (1) complete blood count “CBC” including total and differential white blood cell count “WBC”, (2) C-reactive protein “CRP”, (3) erythrocyte sedimentation rate “ESR”, (4) procalcitonin “PCT” concentration, and (5) synovial fluid aspiration under strict aseptic precautions, before starting antimicrobial therapy.
Synovial fluid samples were transported immediately to the Microbiology laboratory of DSFH where physical examination, cytology, Gram staining, as well as culture and sensitivity were done as per the standard protocols of the hospital laboratory. VITEK TWO (bioMérieux, Brazil) automated system was used for the identification and susceptibility testing of the recovered isolates. Antibiotic susceptibility results were interpreted according to the guidelines established by the Clinical and Laboratory Standards Institute (CLSI).18,19 Diagnostic criteria for SA amongst our cohort included cloudy appearance of the synovial fluid, negative string sign, where septic synovial fluid has low viscosity compared to normal synovial fluid,20 WBC count > 50,000 cells/μL,21 and positive Gram staining results.
Management of the Infected Cases
Identified cases with SA were scheduled for urgent arthroscopic irrigation and debridement (I&D) in the operating room, where irrigation was done under strict aseptic precautions using 8 liters of sterile normal saline followed by debridement of the infected tissues. The infected cases were then prescribed empiric intravenous cefazolin (2 g) while waiting culture and sensitivity testing results, in collaboration with recommendations from infectious disease consultants. After 72 hours, WBC count, CRP, and ESR testing were repeated. Second arthroscopic I&D were performed if the inflammatory markers were still rising. In all patients, the implanted grafts showed normal appearance and were retained.
Study Participants’ Data Extraction
During the period of interest, a total of 2000 patients who experienced ACL tears were identified by reviewing the diagnosis codes of the 10th revision of the International Classification of Diseases (ICD-10). Subsequently, the Current Procedural Terminology (CPT) codes were used to distinguish cases that underwent ACLR. Patients that underwent revision ACLR (n = 332) and those aged <18 years old (n = 32) were excluded from our cohort. As a result, overall 836 adult patients who underwent primary ACLR were eligible for the current study. For the identification of cases diagnosed with SA, we used ICD-10 codes, where mono-bacterial growth was recovered from 12 collected synovial fluid samples (one sample/patient) according to DSFH Microbiology laboratory database findings.
Patients’ medical record numbers “MRN” were then used to extract the relevant data to the study cohort, including (1) demographic data (2) body mass index “BMI”, (3) clinical evidence of SA, (4) tobacco smoking, (5) findings of the laboratory investigations, eg, fasting blood glucose “FBG”, WBC count, neutrophil count, ESR, CRP, and PCT, (6) synovial fluid analysis, as well as culture and sensitivity testing results, and (7) treatment regimen applied for each patient including I&D and the prescribed antibiotics.
Exclusion Criteria
Pediatric patients (<18 years), patients with past or family history of inflammatory arthritis, such as rheumatoid, lupus, psoriatic or gouty arthritis, patients who underwent revision ACLR, and those with suspected or confirmed preoperative sepsis either local or systemic were excluded from our cohort.
Statistical Analysis
All data were analyzed using IBM®SPSS® Statistics program version 26.0 for Windows (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as numbers and percentages. Pearsons Chi-Square (χ2) and Fischer’s exact tests were performed to define the statistical significance of the data. Continuous and normally distributed data were expressed as means ± standard deviation (SD). The Independent Samples t-tests were used to compare the means of 2 independent groups. Odds ratios (OR) with 95% confidence intervals (CI) were determined. To explore the risk factors associated with the development of SA, univariate and multivariate logistic regression analyses were done. Statistical significance was judged at P-values <0.05 (2-tailed).
Results
Demographic and Baseline Features of the Study Participants
The study cohort included 769 males (92%) and 67 females (8%) with an average age of 33.89 ± 8.25 years (range; 18–50 years) and an average BMI of 28.43 ± 5.15 kg/m2 (range; 16.1–45.96 kg/m2) at the time of surgery. About two-thirds (64.7%) of the study subjects were Saudi nationals, whereas 10.4% and 6.3% were Egyptians and Yemeni, respectively. The mean FBG was 104.89 ± 20.99 mg/dl (range; 77–267 mg/dl), with 19.1% of the total cohort diagnosed with DM. None of the operated patients endured simultaneous meniscectomy, meniscus repair, chondroplasty, or other ligament reconstruction.
The aggregate rate of postoperative SA amongst our cohort was 1.43% (12/836). A statistically significant difference was noted between infected and non-infected patients with regard to age (P < 0.0001). Male dominance was observed in both groups that reached a significant difference (P= 0.001). Patients diagnosed with SA showed a significantly higher mean BMI compared to those without infection (37.08 ± 5.89 versus 28.29 ± 5.03; P < 0.0001). About 83% of SA cohort had concomitant DM compared to 18% of non-infected patients (P < 0.0001). Characteristics of both groups are shown in Table 1.
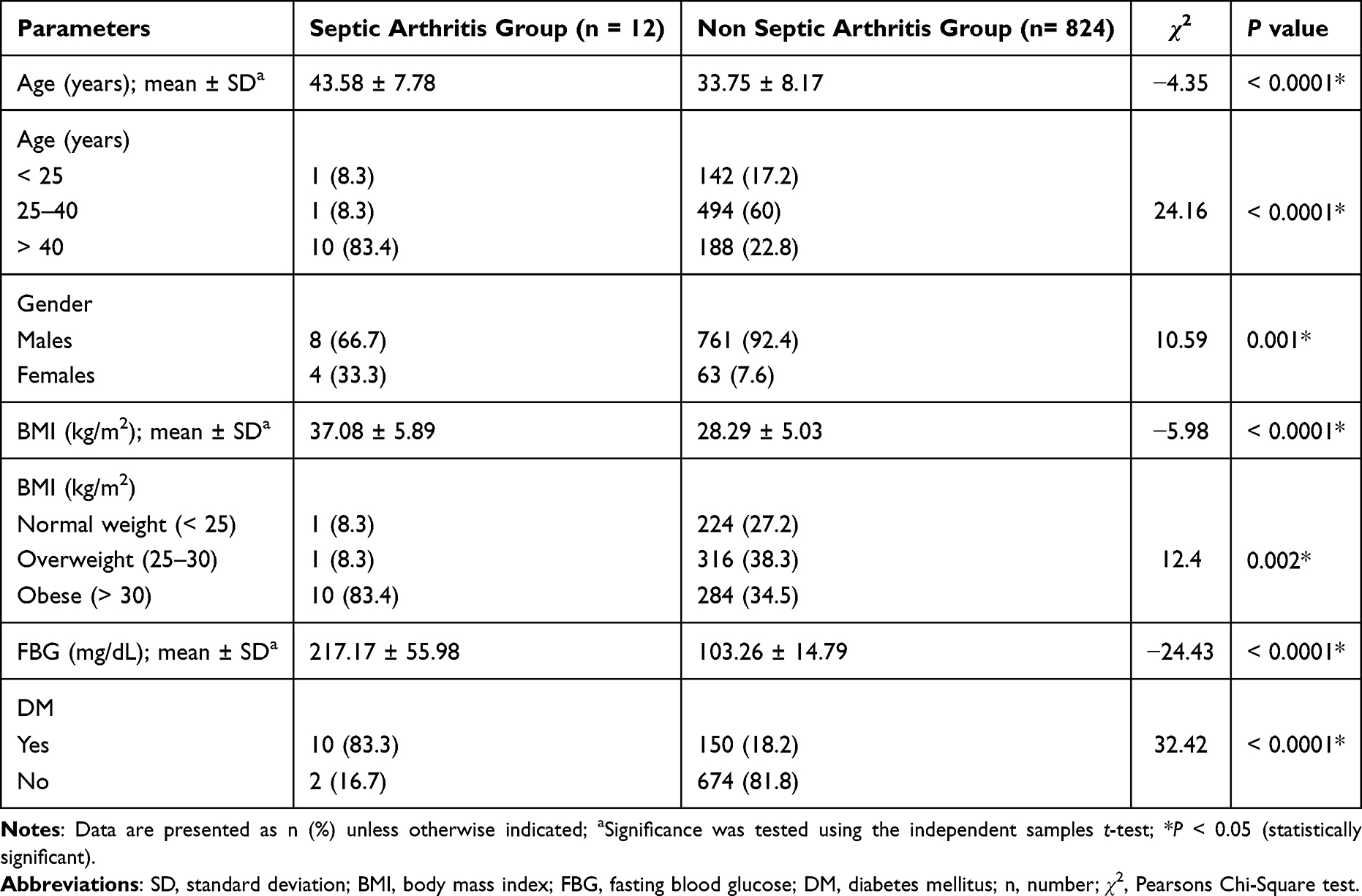 |
Table 1 Comparison Between Patients with and without Knee Septic Arthritis |
Risk Factors Associated with Septic Arthritis Amongst the Study Cohort
A multivariate logistic regression analysis model showed that independent risk factors associated with the likelihood of developing SA were age (OR; 11.12, 95% CI; 1.3–94.97), obesity (OR; 8.51, 95% CI; 1.02–71.13), and DM (OR; 12.58, 95% CI; 2.39–66.3). Data are shown in Table 2. Of note, our hospital electronic medical records showed missing data relative to the frequency of tobacco smoking amongst our cohort, so we could not shed light into this risk factor for SA. Also, data on venous thromboembolism were incomplete.
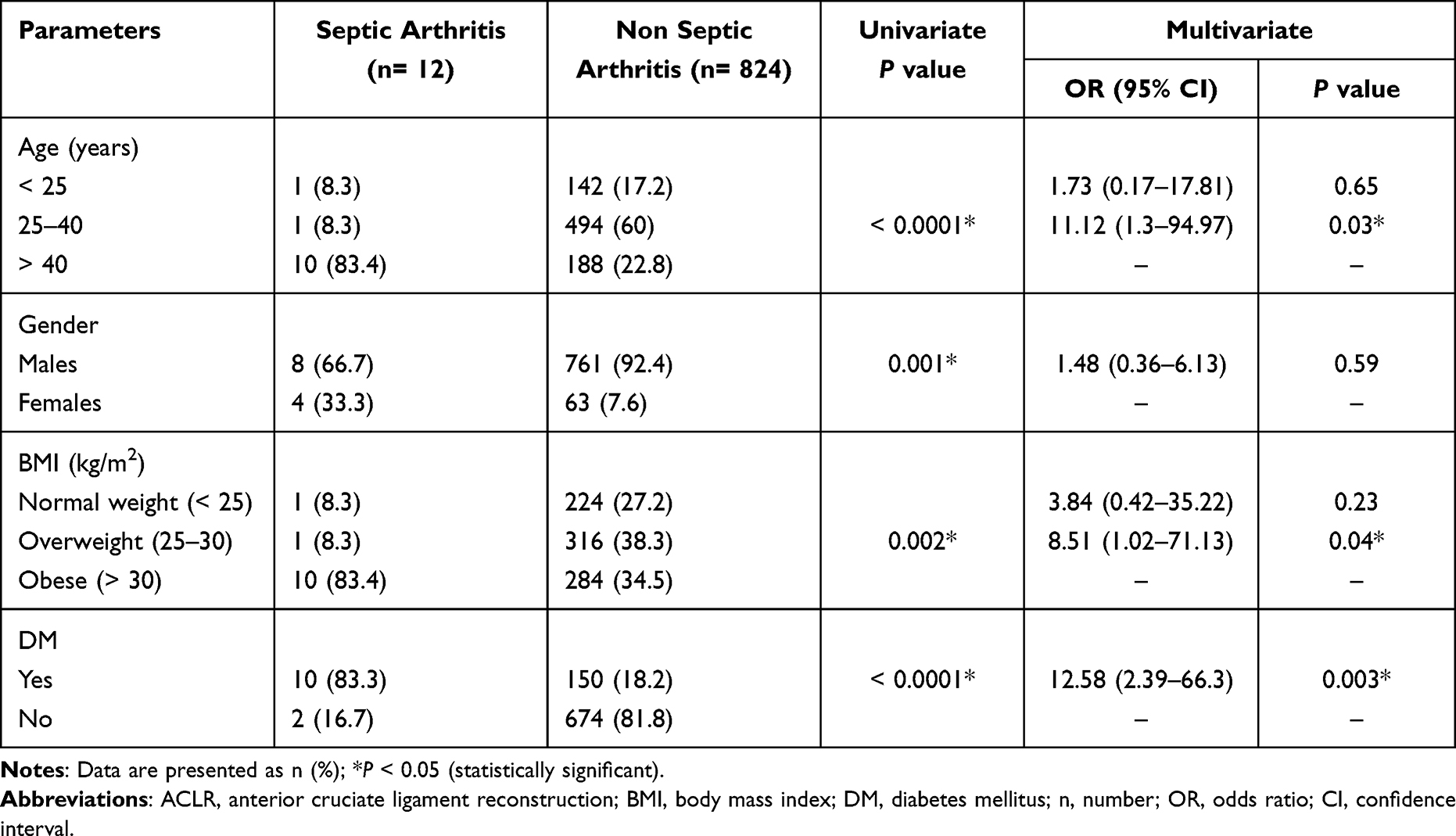 |
Table 2 Multivariate Logistic Regression Analysis of Risk Factors Associated with Septic Arthritis After Arthroscopic ACLR |
Features of Patients Diagnosed with Knee Septic Arthritis
The time from operation to presentation with sepsis at our outpatient clinics was recorded at an average of 20.17 ± 14.22 days (range; 6–47 days) post reconstruction. Out of 12 infected cases, 4 required a second debridement due to the ongoing rise of the inflammatory markers after the first procedure. All grafts were found to be intact at the time of the procedures. After debridement and intravenous antibiotics, none of the SA patients reported continuing signs of infection, so graft removal was not done in any of the involved patients (Table 3). Interestingly, normal pivot-shift testing results were detected in all of the examined cases, and no degenerative changes were shown in imaging studies.
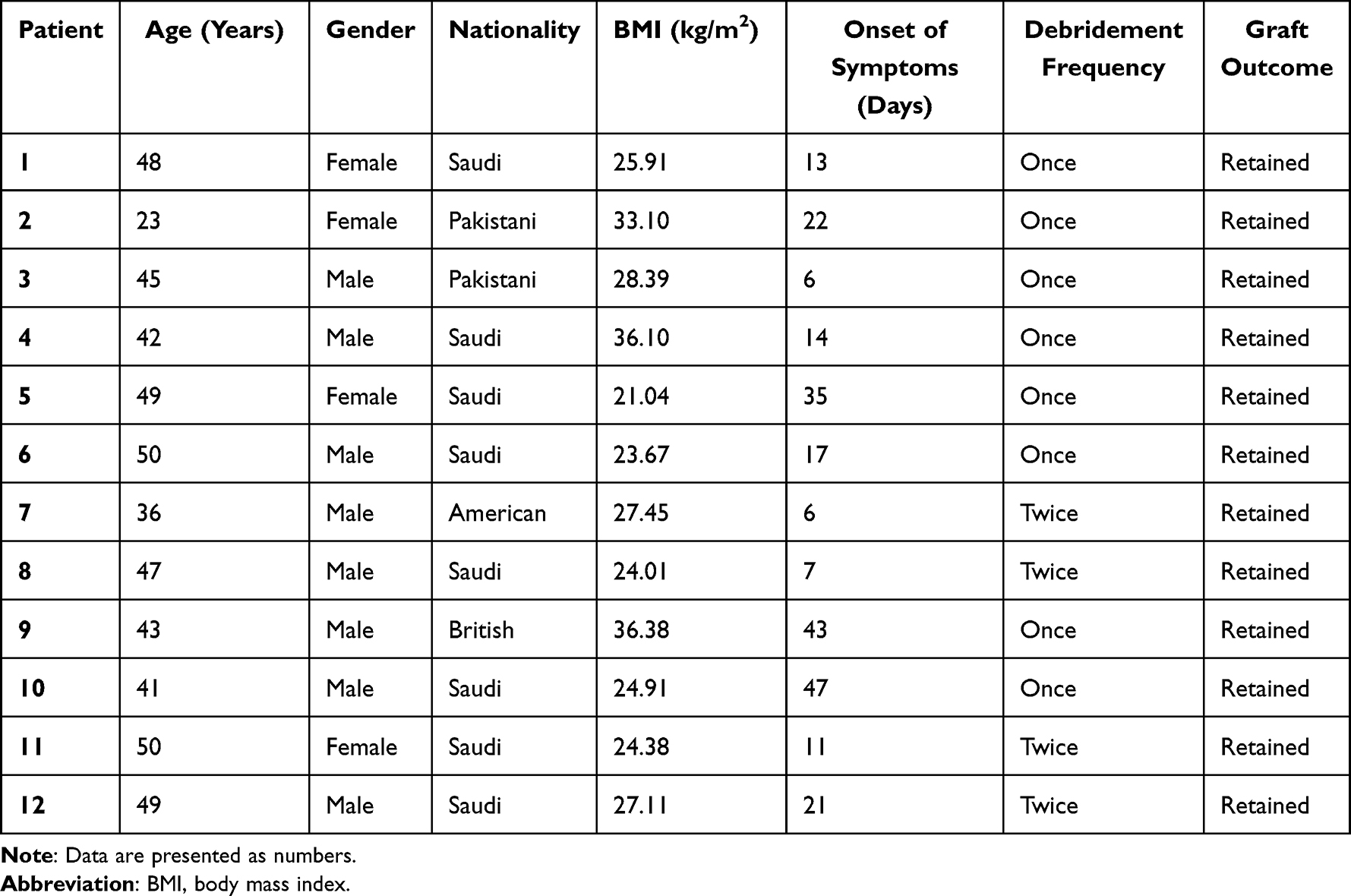 |
Table 3 Characteristics of Patients Presented with Septic Arthritis After ACLR |
Laboratory Results of Patients Identified with Septic Arthritis
Evaluation of the postoperative laboratory parameters of the infected cases, at their early follow-up visits, demonstrated an average peripheral WBC count and neutrophil % of 14.22 ± 4.17/μL (range; 8.17–21.21/μL) and 78.18 ± 12.99% (range; 59.50–96.30%), respectively. In addition, a post-surgical rise of the inflammatory markers was observed, including CRP (mean; 194.84 ± 115.18 mg/L, range; 100.49–445.00 mg/L), ESR (mean; 64.67 ± 18.08 mm/hour, range; 45–99 mm/hour), and PCT (mean; 1.77 ± 2.76 ng/mL, range; 0.05–9.66 ng/mL). The average synovial fluid WBC count was 68,609 ± 14,712/μL (range; 53,000–91,000/μL). Values per patient are depicted in Table 4.
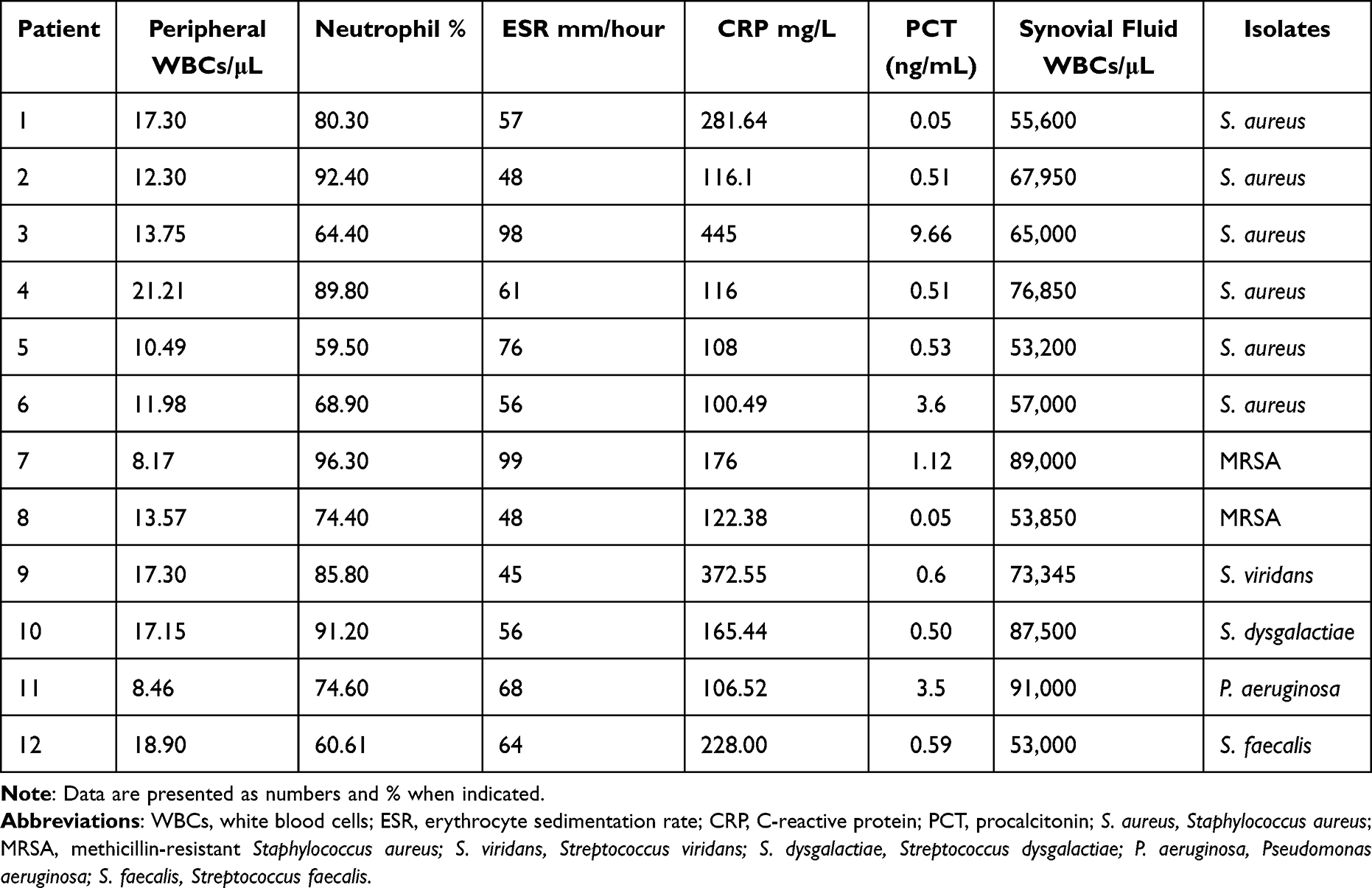 |
Table 4 Laboratory Parameters of Patients with Septic Arthritis at Their Initial Presentation |
Microbiological Findings of Septic Arthritis Cohort
Amongst our cohort, Gram-positive cocci were the most frequently isolated pathogens with S. aureus accounting for 66.7% of the total isolates (n = 8), while Streptococcus species were recovered from 3 samples (25%). On the other hand, only one sample showed a positive growth of Pseudomonas aeruginosa (8.3%). Of note, none of the collected samples yielded fungal, mycobacterial, or polymicrobial growth.
Antibiotic Susceptibility Profile of the Recovered Isolates
Overall, none of the identified Gram-positive cocci (n = 11) demonstrated resistance to levofloxacin, linezolid or vancomycin. Out of 8 S. aureus isolates, 2 were methicillin-resistant (MRSA), while all of them were resistant to penicillin. On the other hand, the obtained P. aeruginosa strain showed sensitivity to gentamicin (MIC ≤ 1 μg/mL), amikacin (≤1 μg/mL), cefepime (≤1 μg/mL), ciprofloxacin (≤0.25 μg/mL), levofloxacin (≤0.5 μg/mL), and piperacillin/tazobactam (≤8 μg/mL); meanwhile, resistance was observed for ceftazidime (≥8 μg/mL).
Discussion
Knee SA following ACLR is an orthopedic emergency that may culminate in irreversible damage to the affected joint. Despite the availability of several techniques for ACLR and the recent advent of arthroscopic reconstruction, this complication is still tackled by orthopedic surgeons. Previous studies have addressed the incidence of SA following ACLR; however, inadequate data are available regarding the risk factors as well as the causative organisms of this worrisome complication. In light of this, we designed this 3-year retrospective study.
In the present study, the cumulative incidence of SA after ACLR was 1.43%. The majority of our recruited patients reported symptoms/signs of arthritis within 6–47 days’ post-operative, which agrees with the existing literature, suggesting incidence of most of the episodes within 2 months postoperative.22 Previous literature showed that the incidence of SA following ACLR ranged from 0.14% to 2.6%.11 A systematic analysis by Makhni and associates identified 169 infections out of 31,750 patients accounting for 0.53% infection rate.23 Another extensive review by Gobbi et al, over a 20-year period, reported a total incidence of 0.37% (7 cases out 1850 ACLR).24 Recently, up to 1.1% incidence rate was described from a nationwide analysis of 26,014 ACLR performed at 52 institutions.25
On the other hand, Kim et al recognized 7 infected cases out of 98 ACLR (7.1%) during a 17-month follow-up period. They ascribed this high infection rate to several factors. One of the identified patients in their study had undergone concomitant screw fixation for a tibial fracture with undue increase in operative time as well as generation of more portals of entry for the microorganisms. They also assumed that organizing the order of ACLR settings to be the last or second to last at the end of the surgical list, participated in inadequate time for sterilization of surgical equipment. In addition, allocation of surgical instruments’ sterilization to improperly trained scrub nurse could have contributed to that high infection rate. Consequently, employing drastic action plans with strict adherence to infection control measures led to zero infection rate after ACLR at their institution.26
In our health-care facility, pre-soaking grafts in gentamicin for a minimum of 15 minutes after harvest is practiced routinely during ACLR sessions. Yazdi et al examined the impact of intra-operative gentamicin irrigation versus saline with respect to the development of SA following arthroscopic ACLR. They claimed that gentamicin had a prophylactic effect against knee infection after ACLR with a significant difference between both study groups.27 A similar study by Moriarty et al concluded that hamstring graft pre-soaking in gentamicin decreased the incidence of deep intra-articular infections as opposed to saline alone.28 Intriguingly, recent data have indicated promising outcomes of vancomycin pre-soaking of hamstring autografts in terms of reduced infection rate after ACLR. However, discrepancies among different studies as well as the dearth of prospective randomized control trials make it untimely to advise generalization of this procedure.29
Given the fact that SA following ACLR can cause a long-lasting debilitating outcome for the infected patients, it is crucial to underscore the risk factors associated with this serious morbidity. In the present study, the univariate analysis showed that increased age, male gender, higher BMI, and being diabetic were significantly associated with increased incidence of SA. In the logistic regression analysis model, increased age, increased BMI, and DM were independently associated with the likelihood of developing SA (Table 2).
Previous data addressing the risk factors for SA after ACLR are incomplete because of their sporadic incidence. Records of age and gender as significant factors are extremely lacking; however, Murphy et al observed that males and patients >20 years, included in a meta-analysis of 1397 ACLR, were at a greater risk of developing SA, which supports our findings.30 Shamrock et al observed that a higher BMI can independently forecast postoperative knee arthritis.31 It is believed that obese patients are more likely to develop sepsis due to many factors including delayed wound healing secondary to excessive subcutaneous tissue, more bacterial colonization of the skin especially of the groin, and interference with the pharmacokinetics of the preoperative cefazoline.32 On the other side, statistics from the Multicenter Orthopedic Outcomes Network (MOON) group disclosed that increased BMI did not have an impact on the rate of SA amongst their cohort. This discrepancy could be ascribed to different characteristics of the operated patients as the MOON group included rather younger (mean age; 27 ± 11 years old) and slimmer (mean BMI; 25.7 ± 4.8 kg/m2) patients compared to our cohort.13
Amongst our series, DM was diagnosed in 83.3% of the infected cases compared to 18.2% of the non-infected patients (P < 0.0001), with diabetics were 12.58 times more likely to develop SA (Table 2). Likewise, Brophy et al stated that DM was a significant risk factor for SA after ACLR with 18.8 times increased odds of infection.13 In contrast, Westermann et al proved that DM was not associated with SA. The low prevalence of DM amongst their study population, including infected (5.13%) and non-infected cases (1.71%), could contribute to this unanticipated observation.33 Recently, Kraus Schmitz and his group also found no association between DM and postoperative SA. However, they attributed this outcome to the infrequent incidence of DM amongst their cohort, leading to analysis bias.25
What is more, some investigators had established the relevance of other factors with the development of post-arthroscopic SA. A systematic review by Canal et al highlighted that the use of hamstring autografts had a 0.23 higher relative risk of infection when compared to bone-patellar tendon-bone (BTB) grafts.34 In a similar way, Kraus Schmitz et al observed that patients who received hamstring autografts were 2.23 times more likely to have SA in comparison with patellar tendon autografts due to larger surface area that facilitate the contamination of hamstring autografts during surgical manipulation.25 Importantly, all of the primary ACLR surgeries that take place in DSFH rely on hamstring autografts, so we could not test this hypothesis. On the other hand, Krutsch et al attempted to find a relationship between different types of sports and the likelihood of SA after ACLR. They conveyed that football players showed a higher incidence of infection as opposed to skiers because of distinct dressing and protective clothing at the incident of trauma.35
Among the analyzed patients, 83% showed peripheral leucocytosis with neutrophilic predominance, while 2 cases had normal WBC count despite infection (Table 4). As reported previously by other authors, peripheral WBC count is not a reliable marker for SA.36 In all of the infected patients, as shown in Table 4, levels of inflammatory parameters were elevated including CRP, ESR, and PCT. However, these raised levels may be ascribed to inflammatory response caused by surgical trauma.37 Recently, Wang et al described lower CRP values (10.9 ± 5.7 mg/dL), but consistent ESR (59.9 ± 24.1 mm/hour).38 Notably, Guillén-Astete et al concluded that at a cutoff point of 0.81 ng/dL, serum PCT demonstrates 95% specificity and 97.4% negative predictive value in diagnosing infectious arthritis. So, it can be utilized to guide clinicians in decision-making regarding perplexing cases.39
Currently, the gold standard test for the diagnosis of knee SA is joint aspirate analysis, with synovial WBC counts >50,000 μL.40 Amongst the 12 performed arthrocenteses in our study, synovial leucocytic counts (as summarized in Table 4) demonstrated marked elevation compared to previous authors.15 Notably, a previous observational study, which included 24 infected and 14 uninfected patients, underlined that at a cutoff value of 40,000 WBCs/mL; diagnosis of postoperative SA could be achieved with 100% specificity.41
In the present study, S. aureus was the most predominant inciting organism for SA (66.7%), followed by Streptococcus species (25%) as shown in Table 4. S. aureus is a resilient bacterium armed with several virulence factors contributing to the pathogenesis of SA. Capsular polysaccharides, cell wall teichoic acid and lipopolysaccharides, surface and secreted proteins, as well as multiple potent exotoxins are worth-mentioning examples.42 The likely sources of infection amongst our cohort include accidental autograft contamination during handling, contaminated inflow cannula, or use of drain. Also, contaminated surgical incision or arthroscopic portals during ACLR could predispose to infection. Of importance, 2 MRSA isolates were identified accounting for 16.7% of the total isolates, a finding comparable to those reported in previous studies.43,44 None of the recovered isolates displayed susceptibility to penicillin, reflecting the imprudent use of this antimicrobial agent in the community setting.
Erice et al demonstrated that Gram-positive cocci were the most frequently isolated organisms with CoNS, S. aureus, Streptococcus faecalis, and Streptococcus agalactiae accounting for 43%, 40%, 6.7%, and 3.3%, respectively. In addition, Gram-negative bacilli were obtained from 2 synovial fluid cultures including Serratia marcescens (3.3%), and Enterobacter cloacae (3.3%). Remarkably, MRSA strains constituted three-fourths of their S. aureus isolates.15 Then again, Pogorzelski et al mentioned that CoNS were the most frequently isolated pathogens with preponderance of S. epidermidis (71.4%), whereas S. aureus was more common in patients that underwent graft removal.45 Recently, Kamaci et al reported 2 cases of SA caused by S. lugdunensis (one of the CoNS) after ACLR. The authors ascribed these infections to the presence of multiple-ligamentous tears which imposed the operated patients on more open techniques, prolonged operative time, and extra foreign body burden.46 Though considered an opportunistic bacterium, S. lugdunensis has several virulence factors associated with arthritis as well as osteomyelitis. The organism can produce a clumping factor, two adhesions and a metalloproteinase. Furthermore, it can establish a complete biofilm within 6 hours, making bacterial eradication with antibiotics problematic.47
Strikingly, one P. aeruginosa isolate was recovered 11 days postoperative from a 50-year-old woman amongst our series of patients. A possible source of infection with this organism within a hospital setting is unsatisfactory sterilization of surgical instruments. However, no evidence of gaps in sterilization was reported within our institution during the study interval. Immunosuppression could be a predisposing factor for infection in that patient. In keeping with our finding, Parikh and his group reported a case of P. aeruginosa infection in a 15-year-old adolescent after ACLR. However, the authors believed that a patient bathing in a hot tub for 2 weeks postoperative could participate into infection by this organism.48 Fortunately, in our series, the infected patients got a satisfactory response after I&D, and infection was resolved completely in all cases with grafts retained.
Our study has few limitations that warrant mention. First, being a retrospective study, we were unable to assess some risks of infection, eg, smoking, venous thromboembolism, and the actual duration of each surgical intervention. Second, because of the overall low incidence of this morbidity, it is important to investigate a larger cohort of patients to facilitate analysis of the associated risk factors.
Conclusion
Postoperative SA after ACLR is a substantial orthopedic challenge. Patients’ age, BMI, and DM are independently associated with the risk of developing this morbidity. Timely diagnosis and treatment are essential to prevent damage to the joint of interest. In addition, orthopedic surgeons should strictly adhere to the infection control measures to circumvent the incidence of this troublesome sequela. Further studies involving the impact of vancomycin presoaking on the prepared autografts should take place in our institution to develop evidence-based guidelines.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board (IRB) of DSFH (approval no. 234/IRB/2021), and the need for informed consent was waived since all data were anonymized before analysis. Patients’ data privacy and confidentiality were considered in all stages of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raines BT, Naclerio E, Sherman SL. Management of anterior cruciate ligament injury: what’s in and what’s out? Indian J Orthop. 2017;51(5):563–575. doi:10.4103/ortho.IJOrtho_245_17
2. Marieswaran M, Jain I, Garg B, Sharma V, Kalyanasundaram D. A review on biomechanics of anterior cruciate ligament and materials for reconstruction. Appl Bionics Biomech. 2018;2018:4657824. doi:10.1155/2018/4657824
3. Büyükafşar E, Başar S, Kanatli U. Proprioception following the anterior cruciate ligament reconstruction with tibialis anterior tendon allograft. J Knee Surg. 2020;33(7):722–727. doi:10.1055/s-0039-1684010
4. Yin J, Yang K, Zheng D, Xu N. Anatomic reconstruction of the anterior cruciate ligament of the knee with or without reconstruction of the anterolateral ligament: a meta-analysis. J Orthop Surg. 2021;29(1):2309499020985195.
5. Simões OJ, Ramos A, Oliveira JP, Noronha JC, Simões JA. A review on finite element analysis of the anterior cruciate ligament reconstruction. Open J Orthop Rheumatol. 2021;6(1):001–0011. doi:10.17352/ojor.000031
6. Yao S, Fu BS, Yung PS. Graft healing after anterior cruciate ligament reconstruction (ACLR). Asia Pac J Sports Med Arthrosc Rehabil Technol. 2021;25:8–15. doi:10.1016/j.asmart.2021.03.003
7. Alsubaie SF, Abdelbasset WK, Alkathiry AA, et al. Anterior cruciate ligament injury patterns and their relationship to fatigue and physical fitness levels– a cross-sectional study. Medicine. 2021;100(1):e24171. doi:10.1097/MD.0000000000024171
8. Reijman M, Eggerding V, van Es E, et al. Early surgical reconstruction versus rehabilitation with elective delayed reconstruction for patients with anterior cruciate ligament rupture: COMPARE randomised controlled trial. BMJ. 2021;372:n375. doi:10.1136/bmj.n375
9. Paschos NK, Howell SM. Anterior cruciate ligament reconstruction: principles of treatment. EFORT Open Rev. 2017;1(11):398–408. doi:10.1302/2058-5241.1.160032
10. Longo UG, Nagai K, Salvatore G, et al. Epidemiology of Anterior Cruciate Ligament Reconstruction Surgery in Italy: a 15-Year Nationwide Registry Study. J Clin Med. 2021;10(2):223. doi:10.3390/jcm10020223
11. Meglic U, Salapura V, Zupanc O. MRI findings of early osteoarthritis in patients who sustained septic arthritis of the knee after ACL reconstruction. Orthop J Sports Med. 2021;9(11):23259671211052519. doi:10.1177/23259671211052519
12. Barbara K, Alan I, Goran V, Saša J. Knee infection following anterior cruciate ligament reconstruction: a cohort study of one thousand, eight hundred and ninety-one patients from the single-centre database. Int Orthop. 2020;44(5):869–875. doi:10.1007/s00264-020-04500-5
13. Brophy RH, Wright RW, Huston LJ, Nwosu SK, Spindler KP; MOON Knee Group, Spindler KP. Factors associated with infection following anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2015;97(6):450–454. doi:10.2106/JBJS.N.00694
14. Balato G, Di Donato SL, Ascione T, et al. Knee septic arthritis after arthroscopy: incidence, risk factors, functional outcome, and infection eradication rate. Joints. 2017;5(2):107–113. doi:10.1055/s-0037-1603901
15. Erice A, Neira MI, Vargas-Prada S, Chiaraviglio A, Gutiérrez-Guisado J, Rodríguez de Oya R. Septic arthritis following arthroscopic reconstruction of cruciate ligaments of the knee: retrospective case review. Enferm Infecc Microbiol Clin. 2018;36(6):336–341. English, Spanish. doi:10.1016/j.eimc.2017.05.002
16. Samonis G, Koutserimpas C, Vrioni G, et al. Fungal septic knee arthritis caused by aspergillus fumigatus following anterior cruciate ligament reconstruction. Diagnostics. 2021;11(11):1975. doi:10.3390/diagnostics11111975
17. Al Farsi F, Al Adawi B, Ba Tahir H, et al. Mycobacterium farcinogenes osteomyelitis of the proximal tibia: a case report. IDCases. 2021;25:e01194. doi:10.1016/j.idcr.2021.e01194
18. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
19. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
20. Mundt LA. Synovial fluid. In: Mundt LA, Shanahan K, editors. Graff’s Textbook of Urinalysis and Body Fluids.
21. Fleming C, Russcher H, Lindemans J, de Jonge R. Clinical relevance and contemporary methods for counting blood cells in body fluids suspected of inflammatory disease. Clin Chem Lab Med. 2015;53(11):1689–1706. doi:10.1515/cclm-2014-1247
22. Otchwemah R, Naendrup JH, Mattner F, Tjardes T, Bäthis H, Shafizadeh S. Effective graft preservation by following a standard protocol for the treatment of knee joint infection after anterior cruciate ligament reconstruction. J Knee Surg. 2019;32(11):1111–1120. doi:10.1055/s-0038-1675794
23. Makhni EC, Steinhaus ME, Mehran N, Schulz BS, Ahmad CS. Functional outcome and graft retention in patients with septic arthritis after anterior cruciate ligament reconstruction: a systematic review. Arthroscopy. 2015;31(7):1392–1401. doi:10.1016/j.arthro.2014.12.026
24. Gobbi A, Karnatzikos G, Chaurasia S, Abhishek M, Bulgherhoni E, Lane J. Postoperative infection after anterior cruciate ligament reconstruction. Sports Health. 2016;8(2):187–189. doi:10.1177/1941738115618638
25. Kraus Schmitz J, Lindgren V, Edman G, Janarv PM, Forssblad M, Stålman A. Risk factors for septic arthritis after anterior cruciate ligament reconstruction: a nationwide analysis of 26,014 ACL reconstructions. Am J Sports Med. 2021;49(7):1769–1776. doi:10.1177/0363546521993812
26. Kim HJ, Lee HJ, Lee JC, Min SG, Kyung HS. Evaluation of infection after anterior cruciate ligament reconstruction during a short period. Knee Surg Relat Res. 2017;29(1):45–51. doi:10.5792/ksrr.16.019
27. Yazdi H, Yousof Gomrokchi A, Nazarian A, Lechtig A, Hanna P, Ghorbanhoseini M. The effect of gentamycin in the irrigating solution to prevent joint infection after anterior cruciate ligament (ACL) reconstruction. Arch Bone Jt Surg. 2019;7(1):67–74.
28. Moriarty P, Kayani B, Wallace C, Chang J, Plastow R, Haddad FS. Gentamicin pre-soaking of hamstring autografts decreases infection rates in anterior cruciate ligament reconstruction. Bone Jt Open. 2021;2(1):66–71. doi:10.1302/2633-1462.21.BJO-2020-0181.R1
29. Figueroa F, Figueroa D, Calvo R, Vaisman A, Espregueira-Mendes J. Vancomycin presoaking of hamstring autografts to prevent infection in anterior cruciate ligament reconstruction: a narrative review. EFORT Open Rev. 2021;6(3):211–216. doi:10.1302/2058-5241.6.200059
30. Murphy MV, Du DT, Hua W, et al. Risk factors for surgical site infections following anterior cruciate ligament reconstruction. Infect Control Hosp Epidemiol. 2016;37(7):827–833. doi:10.1017/ice.2016.65
31. Shamrock A, Cates W, Cates R, et al. Graft preparation with intraoperative vancomycin decreases infection after anterior cruciate ligament reconstruction: a review of 1640 cases. Orthop J Sports Med. 2020;8(7suppl6):2325967120S00506. doi:10.1177/2325967120S00506
32. Löwik CAM, Zijlstra WP, Knobben BAS, et al. Obese patients have higher rates of polymicrobial and Gram-negative early periprosthetic joint infections of the Hip than non-obese patients. PLoS One. 2019;14(4):e0215035. doi:10.1371/journal.pone.0215035
33. Westermann R, Anthony CA, Duchman KR, et al. Infection following anterior cruciate ligament reconstruction: an analysis of 6389 cases. J Knee Surg. 2017;30(6):535–543. doi:10.1055/s-0036-1593617
34. Bansal A, Lamplot JD, VandenBerg J, Brophy RH. Meta-analysis of the risk of infections after anterior cruciate ligament reconstruction by graft type. Am J Sports Med. 2018;46(6):1500–1508. doi:10.1177/0363546517714450
35. Krutsch W, Zellner J, Zeman F, et al. Sports-specific differences in postsurgical infections after arthroscopically assisted anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3878–3883. doi:10.1007/s00167-016-4385-6
36. Borzio R, Mulchandani N, Pivec R, et al. Predictors of septic arthritis in the adult population. Orthopedics. 2016;39(4):e657–663. doi:10.3928/01477447-20160606-05
37. Long B, Koyfman A, Gottlieb M. Evaluation and management of septic arthritis and its mimics in the emergency department. West J Emerg Med. 2019;20(2):331–341. doi:10.5811/westjem.2018.10.40974
38. Wang C, Meng LY, Chen NY, Li D, Wang JQ, Ao YF. [Management algorithm for septic arthritis after anterior cruciate ligament reconstruction]. Beijing Da Xue Xue Bao Yi Xue Ban. 2021 Oct 18;53(5):850–856. Chinese. doi:10.19723/j.issn.1671-167X.2021.05.007. PMID: 34650284; PMCID: PMC8517665.
39. Guillén-Astete CA, García-García V, Vazquez-Díaz M. Procalcitonin serum level is a specific marker to distinguish septic arthritis of the knee in patients with a previous diagnosis of gout. J Clin Rheumatol. 2021;27(8):e575–e579. doi:10.1097/RHU.0000000000001215
40. Roth CA, Da Lomba T, Dadwani R, Dahm J, Strelzow J. Analysis of factors that drives arthrocentesis for suspected septic joint. Ther Adv Musculoskelet Dis. 2021;13:1759720X211002582. doi:10.1177/1759720X211002582
41. Costa GG, Grassi A, Lo Presti M, et al. White blood cell count is the most reliable test for the diagnosis of septic arthritis after anterior cruciate ligament reconstruction: an observational study of 38 patients. Arthroscopy. 2021;37(5):1522–1530.e2. doi:10.1016/j.arthro.2020.11.047
42. Jin T, Mohammad M, Pullerits R, Bacteria AA. Host interplay in Staphylococcus aureus septic arthritis and sepsis. Pathogens. 2021;10(2):158. doi:10.3390/pathogens10020158
43. Helito CP, Noffs GG, Pecora JR, et al. Epidemiology of septic arthritis of the knee at Hospital das Clínicas, Universidade de São Paulo. Braz J Infect Dis. 2014;18(1):28–33. doi:10.1016/j.bjid.2013.04.010
44. Waterman BR, Arroyo W, Cotter EJ, Zacchilli MA, Garcia EJ, Owens BD. Septic arthritis after anterior cruciate ligament reconstruction: clinical and functional outcomes based on graft retention or removal. Orthop J Sports Med. 2018;6(3):2325967118758626. doi:10.1177/2325967118758626
45. Pogorzelski J, Themessl A, Achtnich A, et al. Septic arthritis after anterior cruciate ligament reconstruction: how important is graft salvage? Am J Sports Med. 2018;46(10):2376–2383. doi:10.1177/0363546518782433
46. Kamaci S, Bedeir YH, Utz CJ, Colosimo AJ. Staphylococcus lugdunensis septic arthritis following arthroscopic anterior cruciate ligament reconstruction. Case Rep Orthop. 2020;2020:2813134. doi:10.1155/2020/2813134
47. Argemi X, Prévost G, Riegel P, et al. Kinetics of biofilm formation by Staphylococcus lugdunensis strains in bone and joint infections. Diagn Microbiol Infect Dis. 2017;88(4):298–304. doi:10.1016/j.diagmicrobio.2017.05.002
48. Parikh HB, Armento A, Mandler T, Albright J. Pseudomonas aeruginosa joint and graft infection following anterior cruciate ligament reconstruction surgery. Int J Sports Exerc Med. 2018;4:092.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.