Back to Journals » Infection and Drug Resistance » Volume 19
Sepsis Caused by Clostridium Perfringens in an Elderly Female Patient with Breast Cancer: A Case Report
Authors Fan N, Cheng Z, Zhang X, Wang Y, Zhang A
Received 19 August 2025
Accepted for publication 25 January 2026
Published 5 February 2026 Volume 2026:19 560686
DOI https://doi.org/10.2147/IDR.S560686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hemant Joshi
Ning Fan,1 Zhuanying Cheng,2 Xinying Zhang,1 Yuanyuan Wang,1 Anrui Zhang1
1Department of Laboratory Medicine, The First People’s Hospital of Xianyang, Xianyang, People’s Republic of China; 2Department of Internal Medicine, The First People’s Hospital of Xianyang, Xianyang, People’s Republic of China
Correspondence: Zhuanying Cheng, Department of Internal Medicine, The First People’s Hospital of Xianyang, Xianyang, 712000, People’s Republic of China, Email [email protected]
Objective: To report a rare case of a breast cancer patient who developed septic shock and multiple organ injury. It analyzes the clinical characteristics, pathogenic factors, and prognosis associated with a mixed infection caused by Clostridium perfringens and Escherichia coli, aiming to provide a reference for the early identification and intervention of similar clinical cases.
Methods: A retrospective analysis was conducted on the clinical data of a 75-year-old female patient with breast cancer, who also had a history of hypertension and diabetes. The clinical manifestations, results of etiological tests, treatment regimen, and patient outcomes were summarized, along with an analysis based on existing literature.
Results: The patient was admitted due to nausea, vomiting, abdominal pain, diarrhea, fever, and loss of consciousness, accompanied by acute myocardial infarction and progressively worsening shock. A diagnosis of septic shock and multiple organ injury was established. Etiological tests confirmed an infection with Clostridium perfringens type A carrying the plc(α) toxin gene, as well as Escherichia coli. Despite receiving anti-infective treatment with meropenem, the patient succumbed to multiple organ failure, including heart failure, within less than four days. This case represents the third documented instance of breast cancer patients complicated by Clostridium perfringens bacteremia in the medical literature. Based on clinical manifestations, the source of infection was presumed to be gastrointestinal, with a potential predisposing factor related to the patient’s consumption of watermelon on that had been left unrefrigerated for over 24 hours. Although bloodstream infections caused by Clostridium perfringens are relatively rare, accounting for only about 0.017% of all bloodstream infections, the mortality rate can be as high as 70% to 100% in immunocompromised patients and those with malignant tumors.
Conclusion: When immunocompromised patients with a history of malignant tumors present with infectious symptoms such as fever, myocardial injury, and hemolysis, the potential for infection by virulent anaerobes, such as Clostridium perfringens, should be considered. Early identification and targeted intervention are crucial for improving the prognosis of these patients.
Keywords: Clostridium perfringens sepsis, malignant breast tumor, alpha toxin
Introduction
Clostridium perfringens is an anaerobic, Gram-positive bacterium that forms spores and is frequently located in the gastrointestinal tract, skin, and genitourinary system. It is associated with a variety of conditions, including gastroenteritis, myonecrosis, liver abscess, and gas gangrene.1 Immunocompromise or external factors, such as dietary changes and medications, may trigger dysbiosis, which, in severe cases, can lead to Clostridium perfringens sepsis.2 Although bloodstream infections caused by this bacterium are rare, accounting for approximately 0.017% of all such infections, they predominantly affect immunocompromised individuals, diabetics with poor glycemic control, patients with malignancies such as leukemia, and those undergoing cancer treatments like radiotherapy. The mortality rate associated with these infections can be as high as 70% to 100%.3 This article presents a case of an elderly female breast cancer patient who succumbed to multiple organ failure resulting from Clostridium perfringens sepsis.
Case Presentation
On July 5, 2024, a 75-year-old female patient was admitted to Xianyang First People’s Hospital due to confusion. The patient had a medical history of hypertension and diabetes mellitus and had undergone breast lesion resection and modified radical mastectomy for right breast invasive carcinoma on April 13, 2023, followed by chemotherapy (specific regimen unknown) at another hospital the following month. Approximately 30 hours prior to admission, the patient consumed overnight watermelon and subsequently developed nausea, abdominal pain, vomiting, fever, and sweating, which progressed to infectious myocardial injury accompanied by loss of consciousness. Upon admission, anti-infective therapy with cefoperazone-sulbactam was immediately initiated and switched to meropenem on the third day. Despite symptomatic treatment and emergency resuscitation measures, the patient ultimately succumbed on the fourth day of hospitalization due to septic shock and multiple organ failure. The final identification from the blood culture revealed the presence of Clostridium perfringens and Escherichia coli. The progression, clinical manifestations, diagnosis, and treatment details of this disease are illustrated in Figure 1, while Figure 2 displays the results of the patient’s cardiac ultrasound examination. The relevant laboratory test results are summarized in Table 1.
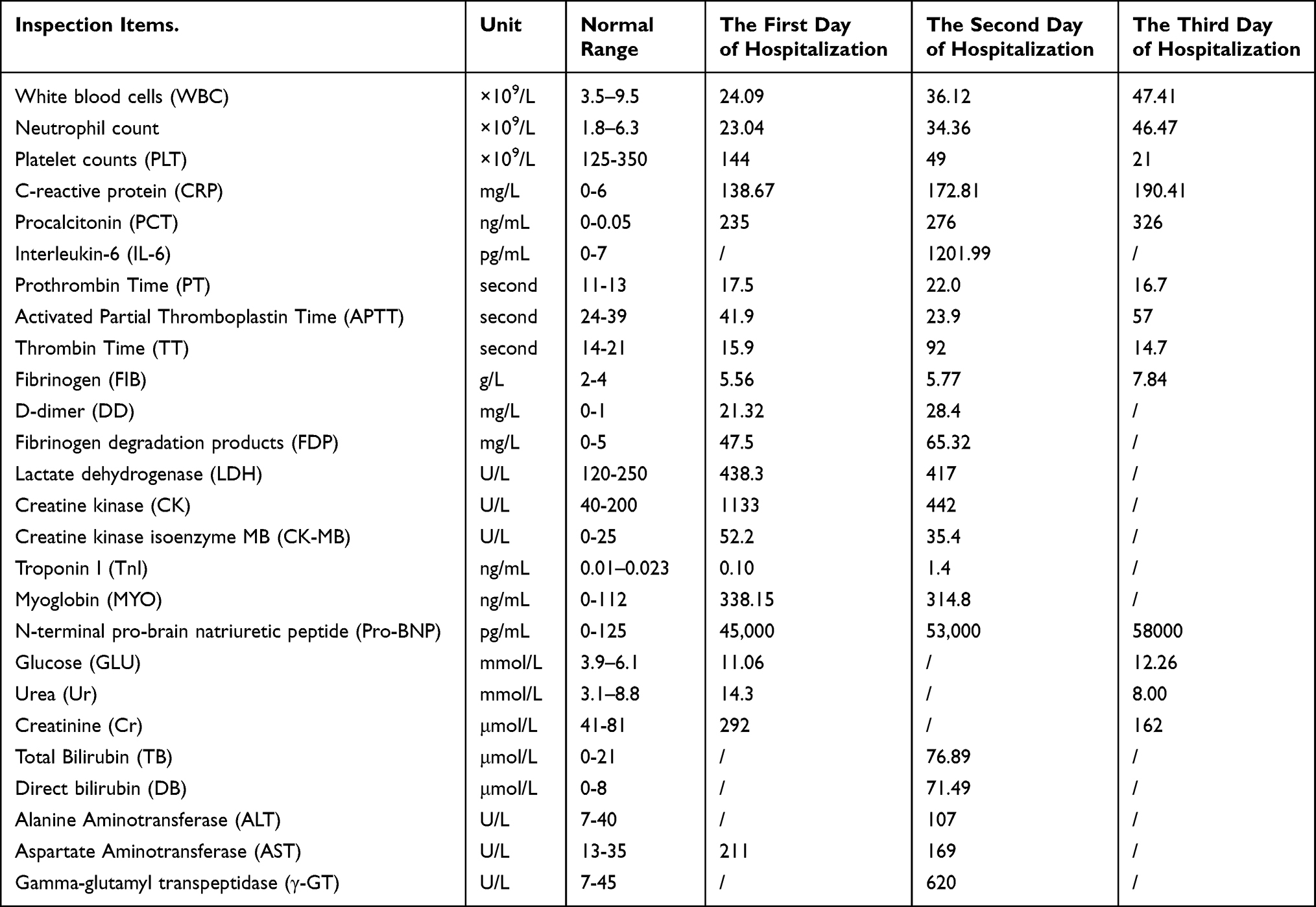 |
Table 1 The Results of Laboratory Test During Patient Hospitalization |
 |
Figure 1 Patient’s disease progression. |
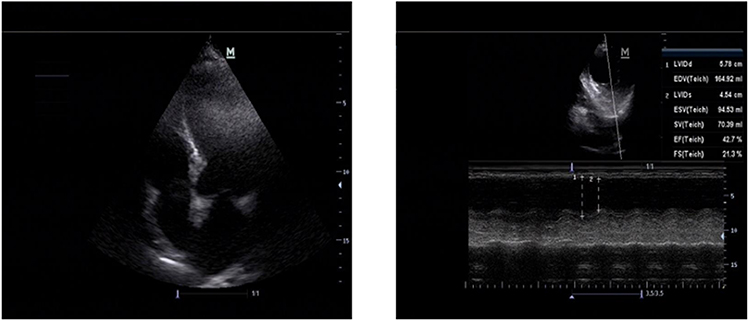 |
Figure 2 Patient’s cardiac ultrasound findings: The left ventricular apex exhibits a rounded morphology, which does not rule out the possibility of ventricular aneurysm formation. Additionally, there are observed segmental wall motion abnormalities in the left ventricle, indicative of reduced left heart function. Aortic sclerosis is present, along with a small degree of mitral and tricuspid valve regurgitation. Tachycardia is also noted. The above performance is consistent with the changes in ultrasound images of myocardial infarction. |
The patient’s two sets of anaerobic blood culture bottles yielded positive results at 0.57 days and 0.58 days, respectively. Microscopic examination of one bottle revealed Gram-positive bacilli, while the other displayed both Gram-positive and Gram-negative bacilli (see Figures 3A and B). In contrast, the aerobic bottles tested positive at 3.06 days and 3.14 days, with smears indicating Gram-negative bacilli. Identification of pure colonies via MALDI-TOF MS (VITEK MS, bioMérieux, Marcy l’Étoile, France) confirmed the presence of Clostridium perfringens and Escherichia coli in the anaerobic bottles, while pure culture identification from the aerobic bottles verified the presence of Escherichia coli, all with 99.9% confidence. Figure 3C illustrates the colony morphology of Clostridium perfringens after 24 hours of anaerobic culture on Columbia blood agar plates, while Figure 3D depicts the colony characteristics of Escherichia coli following 24 hours of conventional culture on MacConkey agar plates.
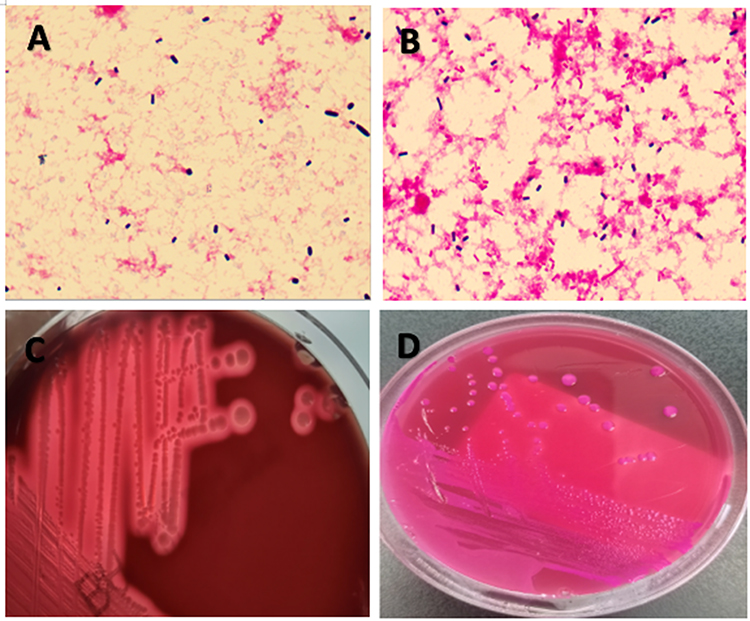 |
Figure 3 Microbiological examination images of Clostridium perfringens. (A) A direct smear of the anaerobic blood culture fluid on the right side, revealing Gram-positive bacilli (Gram stain, ×1000). (B) A direct smear of the anaerobic blood culture fluid on the left side, where both Gram-positive and Gram-negative bacilli are visible (Gram stain, ×1000). (C) The blood culture solution is transferred to a Columbia blood agar plate and cultured anaerobically for 24 hours, resulting in the formation of round, moist, smooth colonies with visible double β-hemolytic rings. (D) The aerobic bottle is transferred to a MacConkey plate and incubated aerobically for 24 hours, leading to the development of red, medium-sized, flat, moist, and smooth colonies. |
The detection of six virulence genes of Clostridium perfringens, namely plc (ɑ), cpb (β), etx (ε), iap (ι), cpe, and cpb2 (β2), was performed using the PCR method. The amplification primers and target genes are detailed in Table 2. Gene sequencing confirmed the presence of the plc (ɑ) toxin gene, which exhibited a match score of 100.0%, an E-value of 2e-153, and an accession number of KP163982.1. The remaining five toxin genes, including cpe, were not detected, thereby confirming that the strain was identified as Clostridium perfringens type A.
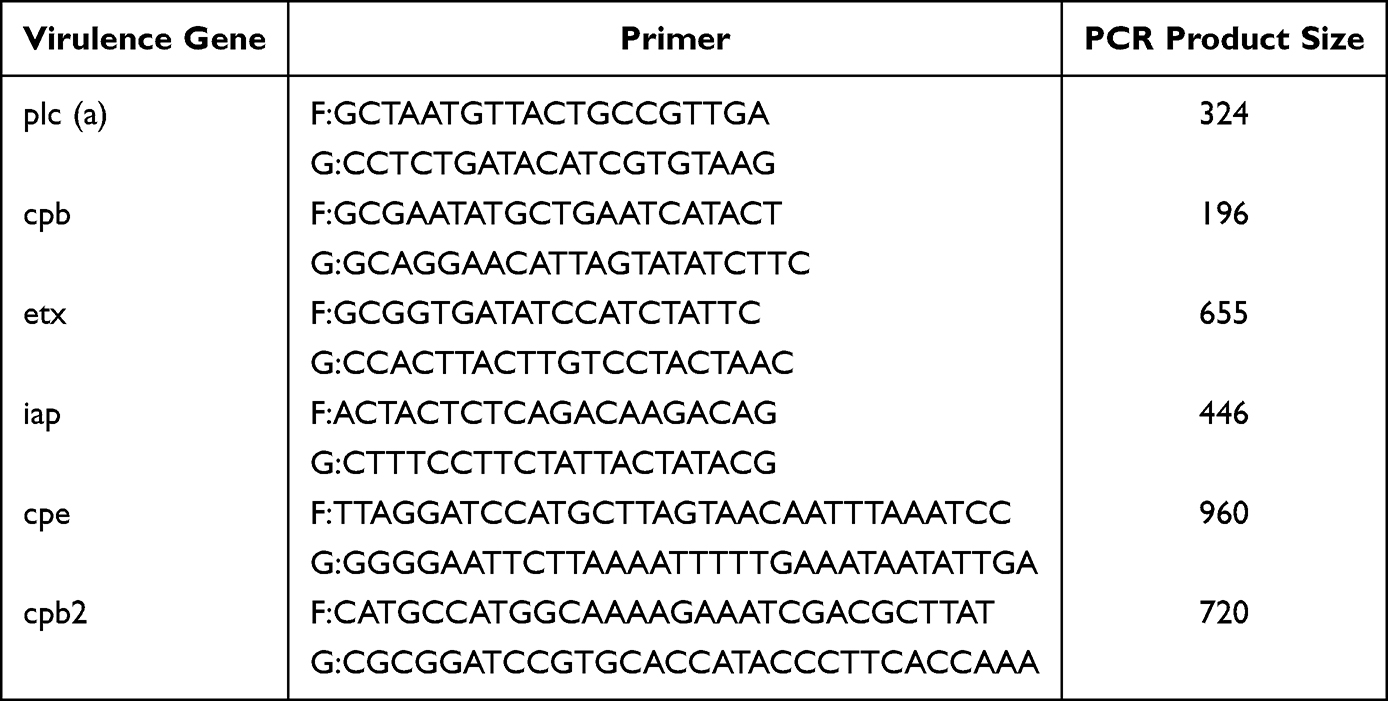 |
Table 2 Oligonucleotide Primers for Six Toxin Genes of Clostridium Perfringens |
Antimicrobial susceptibility testing of Clostridium perfringens was performed using E-test strips (Kont-Biotechnology Co., Ltd., Wenzhou, China) in accordance with the breakpoint criteria established by the Clinical and Laboratory Standards Institute (CLSI). The detailed results are presented in Table 3.
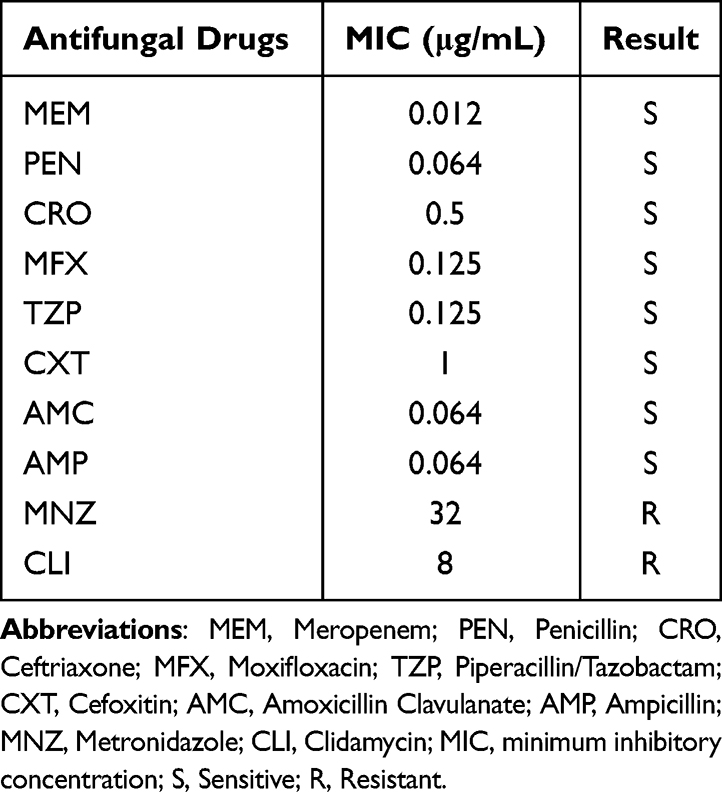 |
Table 3 Results of Antifungal Sensitivity Test of Clostridium Perfringens by E-Test Method |
Discussion
Clostridium perfringens is the most frequently isolated species within the genus Clostridium.4 In 1891, William H. Welch identified the bacterium for the first time while performing an autopsy on a 38-year-old male.5 Bacteremia caused by Clostridium perfringens is an uncommon medical issue mainly seen in senior adults, contributing to its designation as a disease linked to age. Around half of reported instances stem from infections in the abdominal region, whereas the rest are connected to infections of the respiratory tract. Additionally, this form of bacteremia can occur as a primary illness, especially in elderly patients suffering from hepatobiliary conditions, kidney impairment, or cancer, as these individuals face a heightened risk for developing Clostridium perfringens bacteremia.6
A search conducted in PubMed using the medical subject terms “malignant tumor,” “Clostridium perfringens,” and “bacteremia” yielded 29 articles documenting 32 cases of Clostridium perfringens bacteremia in patients diagnosed with malignant tumors, as of February 2025.1,2,6–32 Hematologic malignancies (28.13%) and hepatocellular carcinoma (21.88%) were the most prevalent types, while breast cancer accounted for only 2 cases.1,30 The infections primarily originated from the gastrointestinal tract (37.5%) and the liver (31.25%). The sepsis-related mortality rate reached 59.38%, with typical manifestations including fever, acute hemolysis, liver abscess, and multiple organ failure. More detailed information is presented in Table 4.
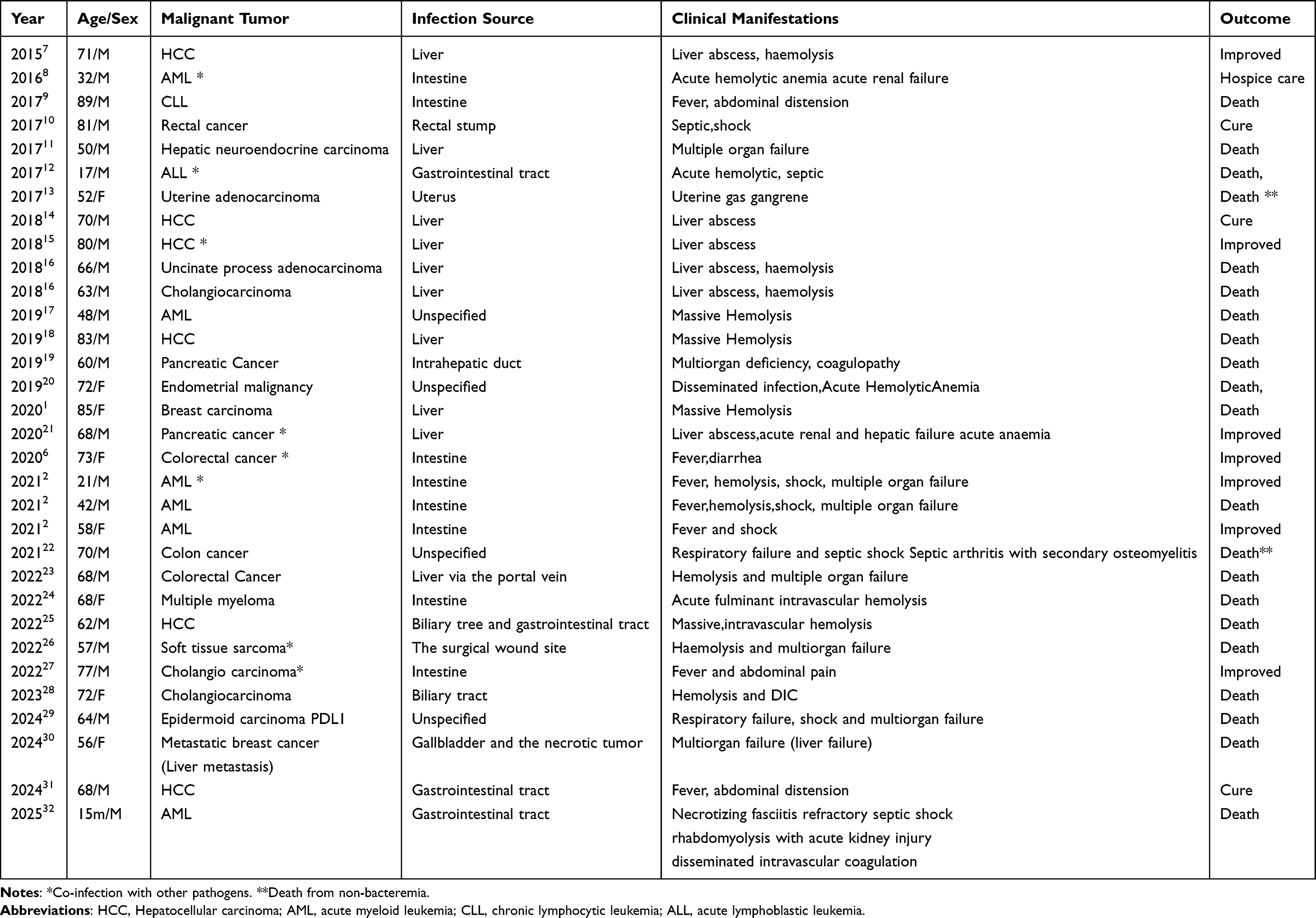 |
Table 4 Reported Cases of Sepsis Caused by Clostridium Perfringens in Patients with Malignant Tumors |
Malignant tumors can significantly compromise the mucosal barrier, thereby increasing the risk of bloodstream infections. Surgical procedures, radiotherapy, and chemotherapy all weaken the immune system and may damage the gastrointestinal mucosa. The compromised integrity of the gastrointestinal mucosa facilitates the translocation of intestinal bacteria into the bloodstream, ultimately leading to Clostridium perfringens bloodstream infections.31 The tumor microenvironment, characterized by necrosis and hypoxia, creates conditions that are conducive to the growth of Clostridium perfringens. In this context, the release and action of exotoxins can induce lethal effects within as little as 12 hours, rendering timely diagnosis and treatment exceedingly challenging.20 However, in this particular patient, a mastectomy was performed a year and a half ago, with no evidence of recurrence or metastatic disease and no corresponding tumor foci. She has a medical history of hypertension and diabetes mellitus and underwent chemotherapy following breast tumor resection, which may have contributed to her compromised immune function. Unlike the two previously reported cases of breast cancer, this case may be associated with dietary factors and involved co-infection with Escherichia coli and Clostridium perfringens, exhibiting rapid disease progression. The patient initially developed gastrointestinal symptoms after consuming watermelon that had been left unrefrigerated for a day. Based on her clinical presentation, we hypothesize that the infection likely originated from the gastrointestinal tract. The concurrent presence of Escherichia coli and Clostridium perfringens supports the hypothesis that these pathogens may have emerged from the gut microbiota. Under conditions of impaired immune function, poor dietary habits may act as potential contributing factors, leading to gut dysbiosis and damage to the intestinal mucosal barrier. This scenario facilitates the translocation of both Clostridium perfringens and Escherichia coli through shared pathways into the bloodstream, resulting in a synergistic infection.
Gastrointestinal sources of Clostridium perfringens bacteremia are primarily associated with hematologic malignancies,2,8,9,12,24,32 often related to neutropenia, with only two reported cases having a history of poor dietary habits.2 This case, based solely on clinical presentation, suggests that dietary factors may serve as potential contributing elements to infections in immunocompromised patients.
Clostridium perfringens can be classified into seven toxin types based on the various combinations of six major exotoxins it produces: Type A (α), Type B (α, β, ε), Type C (α, β), Type D (α, ε), Type E (α, ι), Type F (α, cpe), and Type G (α, β2). Among these, Type A is the primary causative agent of the majority of food poisoning cases associated with Clostridium perfringens.33 In this case, the Clostridium perfringens strain was classified as type A, possessing only the plc(α) toxin gene. The pathogenicity of Clostridium perfringens is primarily attributed to its production of alpha toxin, which is linked to the clinical manifestations and ultimate outcome observed in this patient. The alpha toxin directly inhibits myocardial contraction and adversely impacts the circulatory system.34 In this patient, alongside the initial gastrointestinal symptoms, myocardial injury and heart failure emerged as the most significant manifestations. The toxin, a phospholipase C lecithinase, degrades phospholipids in erythrocyte membranes, thereby accelerating the destruction of red blood cell membranes and causing severe hemolysis. It can also induce platelet destruction, resulting in thrombocytopenia.34 Although the patient did not display obvious clinical symptoms of hemolysis, laboratory findings such as elevated bilirubin, lactate dehydrogenase, and aspartate aminotransferase levels, along with persistently decreased red blood cell count, hemoglobin, and hematocrit, suggest the potential for concurrent hemolytic anemia. The alpha toxin can also activate signaling pathways in neutrophils, endothelial cells, and platelets, thereby enhancing the production of adhesion molecules and platelet-activating factors. This results in intravascular leukostasis and thrombosis, which promotes vascular damage and the formation of an anaerobic environment.17 Ultimately, the rapid progression of sepsis led to the patient’s death from multiple organ failure within less than four days.
In cases of Clostridium perfringens bacteremia, approximately half are classified as polymicrobial, with Escherichia coli and Klebsiella pneumoniae being the most frequently encountered concurrent bacteria.6 It is noteworthy that the presence of additional bacteria alongside Clostridium perfringens does not appear to influence the clinical progression of the infection.1 However, Escherichia coli may alter the local microenvironment through its metabolic activities, creating favorable conditions for the proliferation and virulence expression of Clostridium perfringens. Clostridium perfringens sepsis can escalate rapidly and poses a significant risk of mortality, particularly in immunosuppressed patients, the associated mortality rate is estimated to be approximately 70–80%, with a 30-day mortality rate ranging from 27% to 44%. The median time to death is reported to be around 9.7 hours.28 Therefore, anti-infective therapy targeting Clostridium perfringens, combined with symptomatic and supportive treatment, remains crucial for improving prognosis.
Currently, there are no established treatment guidelines for food poisoning or bacteremia caused by Clostridium perfringens. The Sanford Guide to Antimicrobial Therapy (53rd Edition)35 only provides the preferred regimen for gas gangrene caused by Clostridium perfringens, For infections caused by the genus Clostridium, the recommended first-line treatment is penicillin G.
The empirical treatment for Clostridium perfringens bacteremia and septic shock typically involves β-lactams, aminoglycosides, and/or glycopeptides.29 In this case, due to the rapid progression of the disease, the initial empirical regimen was modified from cefoperazone/sulbactam to meropenem. Although drug susceptibility testing indicated sensitivity to meropenem and successful treatment cases have been documented in the literature,2,6,21 the patient unfortunately succumbed three days later. This outcome underscores the individual variability in treatment response and the potentially fatal nature of this pathogen. Clinically, our current understanding of this anaerobic bacterium remains limited, which may lead to an underestimation of its toxin pathogenicity. The patient’s early critical clinical manifestations were characterized by toxin-induced cardiac injury, necessitating special clinical attention. Initial coverage for anaerobic infections, combined with appropriate symptomatic treatment and antitoxin therapy, may enhance the patient’s clinical outcomes, this situation calls for clinical reflection.
Conclusion
In summary, we present the third documented case of Clostridium perfringens sepsis in a patient with a malignant breast tumor, Notably, this is also the only case potentially associated with a history of poor dietary habits. However, the limitation lies in the absence of etiological testing and virulence gene analysis on the patient’s stool samples and the consumed watermelon, which results in a lack of conclusive evidence.This situation underscores the necessity for a comprehensive analysis of infection sources and transmission routes in similar cases, which would be advantageous for future prevention strategies.
Although Clostridium perfringens sepsis is rare, it is associated with a significantly high mortality rate, particularly among patients with malignant tumors. Due to its non-specific clinical manifestations,early diagnosis remains challenging, and there is a lack of standardized treatment protocols. Therefore, when symptoms such as fever, hemolysis, and myocardial injury which are indicative of infection arise, the possibility of virulent anaerobes such as Clostridium perfringens infection should be considered. Rapid empirical coverage is crucial, and the role of bacterial toxins in disease progression must be fully acknowledged, with appropriate symptomatic treatment measures implemented. Additionally, it is essential to assess patients’ dietary habits, emphasizing the importance of dietary health management for immunocompromised populations, such as cancer patients.
This study has certain limitations, primarily due to its single-case design, which restricts the ability to generalize the findings to a broader population. Individual differences among patients could significantly influence the outcomes observed in this research, making it challenging to apply these conclusions universally. Recognizing these limitations, further accumulation of similar cases and summarizing clinical experiences to enhance the early diagnosis and treatment of Clostridium perfringens sepsis, thereby improving clinical cure rates.
Data Sharing Statement
The article contains the original contributions outlined in the study. Any further inquiries can be directed to the authors designated for correspondence.
Ethics Approval and Informed Consent
Approval for the research involving human participants was granted by the Ethics Review Committee at The First People’s Hospital of Xianyang. Written informed consent for participation in this study was provided by the patient’s family members.Case details are publishable without requiring further institutional approval.
Consent for Publication
The family of the patient has given their written permission for the publication of this case report.
Funding
The authors state no funding is involved.
Disclosure
The authors indicate that the research was conducted free from any commercial or financial connections that could be perceived as a potential conflict of interest.
References
1. Olds KL, Gilbert JD, Byard RW. Unexpected death associated with clostridial sepsis. Am J Forensic Med Pathol. 2021;42(3):289–9. doi:10.1097/PAF.0000000000000640
2. Liu F, Xue S, Zhang Y, et al. Clostridium perfringens sepsis in three patients with acute leukemia and review of the literature. Int J Hematol. 2021;113(4):508–517. doi:10.1007/s12185-020-03060-z
3. Chen DD. Cao JR, Wang Y, et al. Clinical and etiological analysis of a case of bloodstream infection caused by Clostridium perfringens. Lab Med Clin. 2018;15(18):2836–2837. doi:10.3969/j.issn.1672-9455.2018.18.048
4. Yamamoto Y, Itoh N, Sugiyama T, et al. Clinical features of Clostridium bacteremia in cancer patients: a case series review. J Infect Chemother. 2020;26(1):92–94. doi:10.1016/j.jiac.2019.07.019
5. Welch WH. A gas-producing bacillus capable of rapid development in the blood vessels after death. Bull Johns Hopkins Hosp. 1892;1892(3):81.
6. Huang CY, Wang MC. Clostridium perfringens bacteremia associated with colorectal cancer in an elderly woman. Turk J Gastroenterol. 2020;31(12):960–961. doi:10.5152/tjg.2020.19987
7. Li JH, Yao RR, Shen HJ, et al. Clostridium perfringens infection after transarterial chemoembolization for large hepatocellular carcinoma. World J Gastroenterol. 2015;21(14):4397–4401. doi:10.3748/wjg.v21.i14.4397
8. Medrano-Juarez RM, Sotello D, Orellana-Barrios MA, et al. Acute hemolysis with renal failure due to clostridium bacteremia in a patient with AML. Case Rep Infect Dis. 2016;2016:6549268. doi:10.1155/2016/6549268
9. Melnick S, Nazir S, Chwiecko B, et al. There may be more than meets the eye with Clostridium perfringens bacteremia. J Commun Hosp Intern Med Perspect. 2017;7(2):134–135. doi:10.1080/20009666.2017.1327793
10. Bath M, McKelvie M, Canna K. Rare postoperative complication:Clostridium perfringens septic shock following elective abdominal surgery. BMJ Case Rep. 2017;2017:bcr2017221980. doi:10.1136/bcr-2017-221980
11. Landi G, Gualtieri G. Bello IS, et al. A case of fatal Clostridium perfringens bacteremia and sepsis following CT-guided liver biopsy of a rare neuroendocrine hepatic tumor. Forensic Sci Med Pathol. 2017;13(1):78–81. doi:10.1007/s12024-016-9823-8
12. Kukul MG, Ciki K, Karadag-Oncel E, et al. A fatal Clostridium perfringens infection with hemolysis after chemotherapy in an adolescent. Arch Argent Pediatr. 2017;115(2):e92–e95. doi:10.5546/aap.2017.eng.e92
13. Kremer KM, McDonald ME, Goodheart MJ. Uterine Clostridium perfringens infection related to gynecologic malignancy. Gynecol Oncol Rep. 2017;22:55–57. doi:10.1016/j.gore.2017.09.006
14. Yoshikawa T, Ohana M, Fukuda A. High fever after radiofrequency ablation of hepatocellular carcinoma. Gastroenterology. 2018;155(2):e3–e4. doi:10.1053/j.gastro.2017.12.037
15. Takemura K, Sekoguchi S, Yamane S, et al. A case of a gas-forming liver abscess caused by Clostridium perfringens after transcatheter arterial chemoembolization. Nihon Shokakibyo Gakkai Zasshi. 2018;115(6):554–562. doi:10.11405/nisshoshi.115.554
16. Martí Gelonch L, Jiménez Agüero R, Rodríguez Canas N, et al. Massive haemolysis due to sepsis caused by Clostridium perfringens secondary to liver abscess. presentation of two cases with a similar history. Gastroenterol Hepatol. 2018;41(9):562–563. doi:10.1016/j.gastrohep.2017.11.012 English, Spanish.
17. Jakharia N, Hossain A, Luethy P, et al. 48-Year-Old male with febrile neutropenia and massive hemolysis. Clin Infect Dis. 2019;69(12):2193–2194. doi:10.1093/cid/ciz042
18. Uojima H, Onoue M, Hidaka H, et al. A suspected case of Clostridium perfringens sepsis with intravascular hemolysis after transhepatic arterial chemoembolization: a case report. J Med Case Rep. 2019;13(1):125. doi:10.1186/s13256-019-2023-x
19. Xu J, Wang Y, Cui H, et al. Fatal liver infection caused by Clostridium perfringens after common bile duct stenting due to pancreatic cancer: a case report. Infect Drug Resist. 2019;12:3343–3347. doi:10.2147/IDR.S219472
20. Cypher LR, Sullivan C, Jones R, et al. Clostridium Perfringens bacteremia with acute hemolytic anemia in the setting of endometrial malignancy. Acad Forens Pathol. 2019;9(1–2):127–133. doi:10.1177/1925362119851240
21. Dahl SS, Thorsteinsson M, Lambine TL, et al. Severe sepsis caused by a gas-forming Clostridium perfringens and Klebsiella variicola liver abscess following total pancreatectomy. BMJ Case Rep. 2020;13(10):e238896. doi:10.1136/bcr-2020-238896
22. Mohamed AI, Elgasim MEM, Markey G. Clostridium Perfringens septic arthritis of the sternoclavicular joint. J Emerg Med. 2021;61(2):169–171. doi:10.1016/j.jemermed.2021.03.001
23. Kohya R, Murai T, Taguchi Y, et al. An autopsy case of rapidly aggravated Clostridium perfringens septicemia with colorectal cancer. Case Rep Infect Dis. 2022;2022:1071582. doi:10.1155/2022/1071582
24. Yamamoto H, Mizutani Y, Iriyama C, et al. Acute fulminant intravascular hemolysis induced by Clostridium perfringens in a symptomatic multiple myeloma patient under immuno-chemotherapy. Ann Hematol. 2022;101(12):2813–2815. doi:10.1007/s00277-022-05010-7
25. Guo J, Li C, Gao X. Liver abscess after microwave ablation of hepatocellular carcinoma caused by Clostridium perfringens. J Infect Dev Ctries. 2022;16(1):222–225. doi:10.3855/jidc.13756
26. Sogorski A, Bernstorff M, Lehnhardt M, et al. Letaler verlauf einer fulminanten nekrotisierenden fasziitis und Clostridium-perfringens-Infektion nach resektion eines Weichteil-Sarkoms [Fatal necrotizing fasciitis with clostridium perfringens infection following resection of soft tissue sarcoma of the thigh]. Handchir Mikrochir Plast Chir. 2022;54(2):155–159. doi:10.1055/a-1712-4166
27. Itoh N, Akazawa N, Yanaidani T, et al. Clinical and microbiological features of intratumor abscess with bloodstream infection caused by Plesiomonas shigelloides, Citrobacter freundii, Streptococcus mitis/oralis, Clostridium perfringens, and Candida albicans in a patient with cholangiocarcinoma: a case report. J Infect Chemother. 2022;28(12):1677–1681. doi:10.1016/j.jiac.2022.08.024
28. Tohmatsu Y, Yamada M, Otsuka S, et al. Liver abscess caused by Clostridium perfringens after left hepatic trisectionectomy for perihilar cholangiocarcinoma: a case report. Surg Case Rep. 2023;9(1):111. doi:10.1186/s40792-023-01687-8
29. Ben Saïd L, Diancourt L, Rabeau A, et al. Binary enterotoxin producing Clostridium perfringens isolated in blood cultures: case report and review of the literature. Microorganisms. 2024;12(6):1095. doi:10.3390/microorganisms12061095
30. Alrajhi S, Kou XS, Wiseman JS. “Yellow Death.”. McGill University; 2024.
31. Zhang Y, Zhu Y, Han Y, et al. Clostridium perfringens sepsis after comprehensive multicourse treatment of hepatocellular carcinoma: a case report and review. Heliyon. 2024;10(12):e33279. doi:10.1016/j.heliyon.2024.e33279
32. Alsowailmi B, Alshaalan M, Johani SA, et al. Fulminant non-traumatic Clostridium perfringens necrotizing fasciitis and myonecrosis in a child with acute myeloid leukemia. J Infect Public Health. 2025;18(3):102635. doi:10.1016/j.jiph.2024.102635
33. Yu SK, Cui ZY, Liu L, et al. Pathogenic analysis of suspected food poisoning by Clostridium perfringens based on whole genome sequencing. J Chin J Zoonoses. 2025;41(01):61–66.
34. Hifumi T. Spontaneous non-traumatic Clostridium perfringens sepsis. Jpn J Infect Dis. 2020;73(3):177–180. doi:10.7883/yoken.JJID.2019.382
35. Gilbert DN, Chambers HF, Saag MS, et al. The Sanford Guide to Antimicrobial Therapy 2023 (Chinese Edition) Fan HW, Trans. Li TS, Rev. 53rd Ed. Vol. 50. Beijing: Peking Union Medical College Press; 2023:80.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.