Back to Journals » Infection and Drug Resistance » Volume 19
Sentinel Surveillance-Based Epidemiological Analysis of Foodborne Diseases in Shengsi County, China, 2019–2024
Authors Chen J, Liu X, Wang H, Su Y, Bao R, Ma L, Zhang H
Received 20 January 2026
Accepted for publication 12 May 2026
Published 28 May 2026 Volume 2026:19 594651
DOI https://doi.org/10.2147/IDR.S594651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Oliver Planz
Jiayi Chen,1,* Xinyu Liu,2,* Hongtao Wang,1,* Ying Su,3 Ruijing Bao,4 Lanxin Ma,4 Hangjie Zhang5,6
1Department of Prevention and Control of Infectious Disease, Shengsi County Center for Disease Control and Prevention, Zhoushan, Zhejiang, People’s Republic of China; 2School of Public Health, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 3Center for General Practice Medicine, Department of Research Administration, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 4School of Life Science and Agriculture Forestry, Qiqihar University, Qiqihar, Heilongjiang, People’s Republic of China; 5Department of Prevention and Control of Infectious Disease, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China; 6Key Laboratory of Vaccine, Prevention and Control of Infectious Disease of Zhejiang Province, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hangjie Zhang, Department of Prevention and Control of Infectious Disease, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Globally, foodborne diseases (FBDs) pose a significant public health burden, particularly in coastal regions where seafood consumption is high. Therefore, continuous surveillance is essential to detect shifts in pathogen profiles.
Purpose: We analyzed the epidemiological characteristics and temporal dynamics of pathogen profiles in patients with FBD in Shengsi County, Zhoushan City, Zhejiang Province, China.
Patients and Methods: A descriptive epidemiological analysis was conducted on FBD cases that occurred between 2019 and 2024 and were reported by sentinel surveillance hospitals in Shengsi County through the China Foodborne Disease Surveillance and Reporting System.
Results: A total of 2173 cases were analyzed, with an average of 362 cases occurring per year. Cases were primarily in adults aged ≥ 19 years (68.20%), with peak incidence occurring in the summer (38.93%). Marine animals and their products were the main suspected food category (34.74%), and the primary food consumption setting was the household (76.44%). Vibrio parahaemolyticus was the predominant pathogen observed throughout the study period, with annual positivity rates ranging from 5.93% to 13.48%. Notably, Salmonella cases surged to 9.32% in 2024, compared to 0– 1.09% between 2019 and 2023. The proportion of febrile cases also increased in 2024 (34.10%), coinciding with the rise in Salmonella infections.
Conclusion: FBDs in Shengsi County exhibited distinct seasonal and household-related patterns. While V. parahaemolyticus remains endemic, the sharp increase of Salmonella cases in 2024 warrants heightened vigilance. Future efforts should focus on the safety of marine food products and household kitchen hygiene, alongside sustained surveillance to detect dynamic pathogen shifts.
Keywords: foodborne diseases, epidemiology, pathogen surveillance, Vibrio parahaemolyticus, Salmonella
A Letter to the Editor has been published for this article.
Introduction
Foodborne diseases (FBDs) present a significant global public health challenge. The World Health Organization estimates that FBDs account for approximately 600 million illnesses and 420,000 deaths annually worldwide.1,2 In China, the spatial distribution of FBDs is markedly uneven. Cases are disproportionately concentrated in the southern and coastal regions, a pattern that has expanded significantly over the past five years. Coastal provinces have reported substantially higher proportions of FBD events than inland areas due to high seafood consumption, intensive cold-chain logistics, and a vibrant catering industry.3 Moreover, the disease burden in these regions is considerable. For example, surveillance in Zhejiang Province between 2015 and 2020 documented 962 outbreaks, which affected 8324 individuals and resulted in 1028 hospitalizations and 20 deaths.4 Similarly, in Taiwan Province between 2012 and 2015, an estimated 3,895,914 annual FBD cases led to 1,445,384 physician visits, 50 deaths, and a loss of 4974 disability-adjusted life years.5
The causative agents of FBDs are diverse; they encompass bacteria (eg, Salmonella spp., Vibrio parahaemolyticus, Listeria monocytogenes, and Staphylococcus aureus), viruses (eg, Norovirus and Hepatitis A), parasites, fungal toxins, chemical contaminants, and various environmental and behavioral factors.6 In coastal China, V. parahaemolyticus is the most prominent foodborne pathogen. A national sentinel-surveillance-based study examining the years 2013 to 2022 identified it as the leading cause of sporadic FBDs, with cases concentrated in coastal provinces.7 In addition to V. parahaemolyticus, Salmonella spp. is a common pathogen in coastal areas and nationwide. Nontyphoidal Salmonella spp. is a frequent cause of foodborne gastrointestinal infections in China, consistently ranking among the top three pathogens responsible for bacterial FBD outbreaks.8
Zhejiang Province has maintained a provincial-level FBD sentinel surveillance system since 2010. These hospitals follow standardized protocols for case definition, specimen collection, and data reporting. Data from this system have provided detailed evidence of the local FBD burden. From 2010 to 2022, V. parahaemolyticus was the dominant foodborne pathogen in Zhejiang, with outbreaks peaking in summer and exhibiting significant associations with air temperature and sea surface temperature.9 Salmonella also exhibited a clear seasonal pattern, with infections peaking in the summer.10
This study focused on Shengsi County, an archipelago in Zhoushan City, Zhejiang Province, which serves as an ideal natural laboratory for studying FBDs. Shengsi is China’s easternmost island county and a core part of the Zhoushan Fishing Ground. Marine fisheries are its traditional industry, and the local diet is heavily based on seafood, often consumed raw, lightly cooked, or fermented (eg, drunken crab and raw, marinated shellfish), leading to a high risk for V. parahaemolyticus infection. In addition, Shengsi is a popular tourist destination that experiences considerable seasonal population influxes, which strains local food safety oversight. Despite the endemicity of V. parahaemolyticus in coastal Zhejiang, it remains unclear whether the pathogen profile has changed in recent years. In particular, healthcare-seeking behavior for mild gastrointestinal symptoms may have decreased during the COVID-19 pandemic (2020–2022) due to lockdowns and a fear of visiting hospitals. Food exposure patterns may have also shifted from communal dining toward home-based or solitary eating, as tourism-related activities declined during the pandemic.11
Therefore, this study analyzed the 2019–2024 surveillance data from Shengsi County to describe the epidemiological characteristics of local FBDs, identify high-risk populations and exposure settings, and track changes in pathogen profiles. The findings should provide evidence-based support for local food safety risk communication, targeted health education, and the optimization of surveillance strategies.
Materials and Methods
Data Source
Data were extracted from the Foodborne Disease Case Surveillance System within the China Information System for Disease Control and Prevention after approval by the Shengsi County Center for Disease Control and Prevention (CDC). The dataset included all FBD events and case information reported between January 1, 2019 and December 31, 2024 for individuals whose registered residence was in Shengsi County. The collected information encompassed four dimensions: clinical manifestations, epidemiological investigation, food hygiene investigation, and laboratory testing. Specifically, data for each case included basic demographic information, recorded signs and symptoms, dietary exposure history, clinical laboratory results, and the clinical diagnosis. The surveillance system requires complete reporting of these key variables. A small number of incomplete cases were excluded from the final analysis. Shengsi County People’s Hospital served as the primary sentinel surveillance site and was responsible for the active monitoring of suspected FBD cases, specimen collection, and subsequent shipment of samples to the local CDC for testing.
Case Definition
An FBD case was defined according to the Foodborne Disease Surveillance and Reporting Regulations issued by the National Health Commission.12 This definition encompasses infectious and toxic diseases, including food poisoning, caused by pathogens entering the body via food. A reportable case was defined as an individual presenting primarily with diarrhea (defined as ≥3 bowel movements per day with abnormal stool consistency) that was confirmed or suspected to be caused by food consumption. Cases presenting with vomiting without meeting the diarrhea definition were excluded from the analysis.
Laboratory Methods
Specimen Collection and Transport
Fecal specimens or rectal swabs were collected by attending physicians at Shengsi County People’s Hospital from patients meeting the case definition. Collection occurred preferably before antibiotic administration. Specimens were transported to the laboratory of the Shengsi County CDC for analysis.
Bacterial Culture
Routine testing was performed for three major bacterial pathogens: V. parahaemolyticus, Salmonella spp., and Shigella spp., following the standard culture-based protocols of the National Manual for Foodborne Disease Surveillance. Serological confirmation was further performed by slide agglutination assay with type-specific and group-specific antisera to validate strain serotype and ensure accurate species identification.
Molecular Detection
All presumptive V. parahaemolyticus isolates were subjected to nucleic acid extraction using a commercial kit (TIANGEN Biotech, Beijing, China). Subsequently, real-time polymerase chain reaction (qPCR) was carried out with a commercial PCR detection kit (Beijing Baiao Leibo Technology Co., Ltd., Beijing, China) to detect key virulence genes encoding thermostable direct hemolysin and thermostable-direct-hemolysin-related hemolysin. A cycle threshold (Ct) value ≤35 was defined as a positive result.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.2.2). Categorical data are presented as numbers and percentages (n, %). Group comparisons were performed using Pearson’s chi-square test to examine differences in the distribution of baseline characteristics across different years. The significance level was set at α = 0.05, and a two-sided P-value <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 2173 FBD cases were reported in Shengsi County between 2019 and 2024, with an annual average of 362 cases. The annual case numbers remained relatively stable: 337 cases in 2019, 341 in 2020, 439 in 2021, 322 in 2022, 385 in 2023, and 349 in 2024. In total, 51.73% of the cases were in male patients and 48.27% were in female patients. Adults aged ≥19 years accounted for 68.20% of all cases, with 29.13% aged between 19 and 40 years and 39.07% were ≥41 years. The most frequently represented occupational categories were office workers (21.95%), children in childcare (19.33%), and homemakers/unemployed individuals (17.44%).
Summer was the peak season for disease outbreaks (38.93% of all incident cases occurred during the summer), followed by spring (22.32%), autumn (20.57%), and winter (18.18%). Marine animals and their products were the most frequently implicated food category (34.74%), followed by other or unknown foods (25.03%), and plant-based foods (19.10%) (P < 0.001). Households were the primary setting for food consumption (76.44%), and meals were most commonly shared in small groups of one to three persons (83.34%). Most cases (97.28%) did not require hospitalization. Co-diners also developed symptoms in 10.03% of cases, and 7.87% of cases had used antibiotics within 12 hours prior to seeking medical care.
Chi-square tests revealed significant differences in the distribution of most baseline characteristics across the six-year study period (age group, occupation, season, food category, consumption setting, number of people sharing a meal, co-diners with symptoms, and antibiotic use prior to seeking medical care; all P < 0.01), except for gender (P = 0.28). The annual distributions are shown in Table 1.
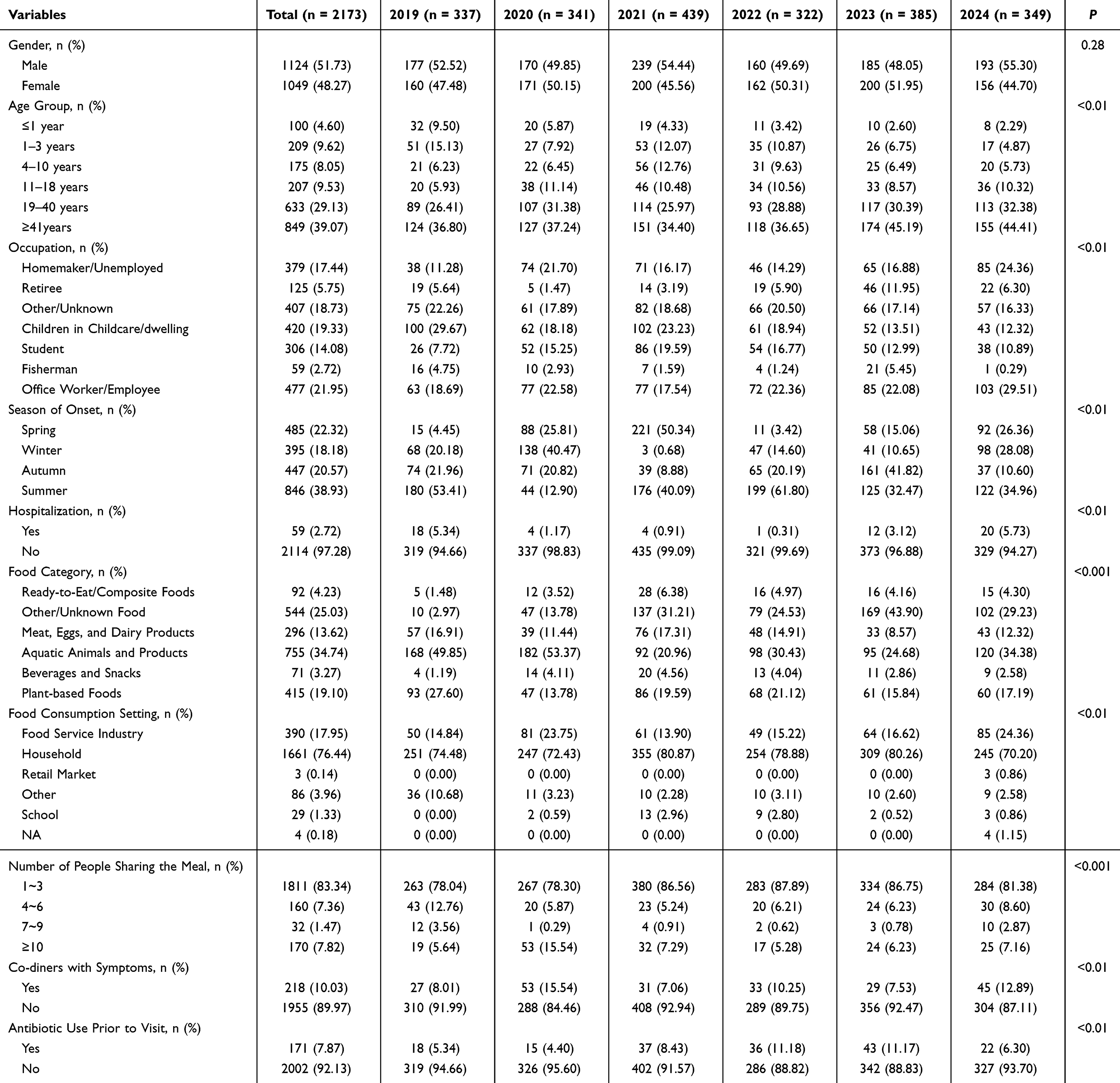 |
Table 1 Baseline Characteristics of Foodborne Disease Cases by Year, 2019–2024 |
Clinical Symptoms
Diarrhea was the most prevalent symptom, which was present in 98.94% of cases. Vomiting was reported in 31.98% of cases. Notably, the proportion of cases presenting with fever fluctuated significantly over the years, peaking at 34.10% in 2024. Other symptoms such as fatigue, headache, and decreased urine output were less frequent but also varied significantly by year, as shown in Figure 1.
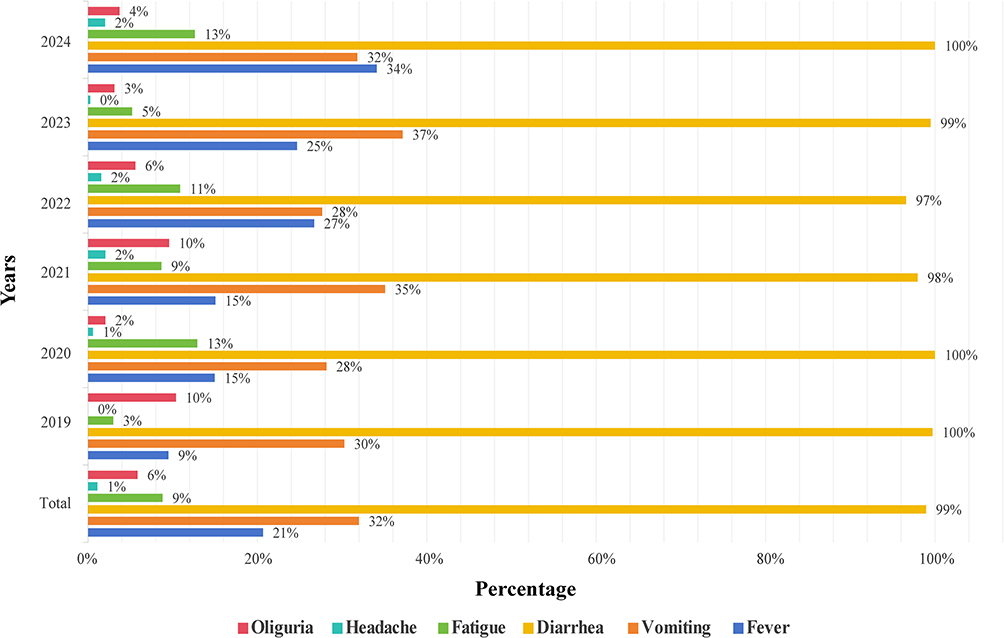 |
Figure 1 Annual distribution of clinical symptoms, 2019–2024. The bar chart shows the annual percentage of cases presenting with each symptom: diarrhea, vomiting, fever, fatigue, headache, and oliguria. Diarrhea was the most prevalent symptom across all years (98–100%), while the proportion of febrile cases peaked in 2024 (34%). Data labels indicate the exact percentage for each symptom by year. |
Pathogen Detection Trends
A total of 634 cases were tested for Salmonella spp. and V. parahaemolyticus, and 604 for Shigella spp. From 2019 to 2024, V. parahaemolyticus consistently had the highest detection rate, with annual positivity rates ranging from 5.93% (2021) to 13.48% (2022). In contrast, Salmonella spp. positivity was minimal between 2019 and 2023, ranging from 0% to 1.09%. However, in 2024, the Salmonella spp. positivity rate surged to 9.32%, the highest recorded during the six-year period. No Shigella spp. were detected throughout the entire surveillance period. The annual positivity rate trends of the three pathogens are presented in Figure 2.
 |
Figure 2 Annual positivity rates of major bacterial pathogens, 2019–2024. The line chart shows the annual positivity rates of three bacterial pathogens: Vibrio parahaemolyticus, Salmonella spp., and Shigella spp. V. parahaemolyticus consistently exhibited the highest detection rate (5.93–13.48%). Salmonella spp. positivity remained low (0–1.09%) from 2019 to 2023 but surged to 9.32% in 2024. No Shigella spp. were detected during the surveillance period. |
Discussion
This study analyzed 2173 FBD cases reported in Shengsi County between 2019 and 2024. Our results show a distinct seasonal pattern (with cases peaking in summer), a predominance of adult cases, and a primary exposure link to marine products consumed in household settings. V. parahaemolyticus remained the dominant pathogen throughout the study period, but Salmonella spp. positivity increased sharply in 2024.
The age distribution analysis showed that adults aged ≥19 years accounted for 68.20% of all cases. This likely reflects a higher exposure frequency, as this demographic is more engaged in social and economic activities, including dining out and home cooking. In terms of occupational distribution, office workers may have been exposed through the workplace or commercial dining, students via school meals, and homemakers or unemployed individuals primarily through household food handling. However, despite these differences, households remained the common exposure setting across all groups.13,14
Summer was the peak season for FBD incidence, which is consistent with other national and international studies.10,15 Zhejiang Province has a subtropical monsoon climate, characterized by high temperature and humidity in the summer. During this period, coastal water temperatures enter the optimal range for bacterial proliferation, creating ideal conditions for the contamination of seafood, particularly filter-feeding or benthic species such as shellfish, shrimp, and crabs.16 Moreover, in coastal regions such as Shengsi, local dietary habits shift during the summer toward increased consumption of raw or lightly cooked seafood, which further heightens exposure risk.17 Summer is also the peak tourist season. National surveillance data have identified multiple FBD outbreaks associated with tourism, primarily caused by V. parahaemolyticus and Salmonella spp., with cases mainly occurring in tourist area catering services.18
Household outbreaks have consistently been a major component of FBD incidents in China,19,20 where household meals are typically shared between one to three persons and are prepared by household members. The handling of marine products during home cooking may also increase the risk of foodborne illnesses. A study in Wenzhou (another coastal city in Zhejiang Province) reported that households accounted for 30.8% of foodborne outbreaks, with marine products being the primary source of contamination.14 A national investigation of V. parahaemolyticus outbreaks in China further identified the main contamination links as incomplete cooking of marine food products and cross-contamination between raw and ready-to-eat meat and vegetable products.17
Among the three pathogens tested for in this study, V. parahaemolyticus consistently exhibited the highest detection rate. This confirms its status as the dominant, endemic pathogen in this coastal region, which is consistent with its role as the leading cause of bacterial FBD in coastal Zhejiang Province.4,7,9 The most striking pathogen profile change was the sharp surge in the positivity rate of Salmonella infections in 2024 (rising from 0 to 1.09% in previous years to 9.32%). This marked shift within a short period suggests potential changes in local contamination sources or transmission routes. Salmonella is commonly associated with raw or undercooked eggs, poultry, and meat, as well as cross-contamination during food preparation, such as using the same cutting board for raw meat and ready-to-eat foods such as salads.21 In Zhejiang Province, contaminated fruit and fruit products have been reported as the leading cause of Salmonella infections.10 Unsafe food preparation practices and contaminated food items may be more common in household kitchens, potentially contributing to the rise in Salmonella cases observed in 2024. This study also included the COVID-19 pandemic period. We found that the positivity rate of V. parahaemolyticus in 2021 was the lowest observed throughout the six-year period. This pattern is consistent with findings from Jiangsu Province, where the detection rate of V. parahaemolyticus decreased significantly during the pandemic, likely due to restaurant closures and reduced tourism.22 Changes in healthcare-seeking behavior and reduced testing during the pandemic may have also contributed to the decline in reported cases. After the pandemic, the resumption of tourism activities may have introduced new strains or increased exposure opportunities for Salmonella spp.23
Our analysis points to several practical considerations. First, the consistent summer peaks in FBD outbreaks support the allocation of enhanced surveillance resources during this season, combined with public messaging on the risks of consuming raw or undercooked seafood during warm months. Second, given that households accounted for over three-quarters of the exposure settings, future health education initiatives should target household food handlers with practical guidance on the proper storage of marine products, the importance of separating raw and cooked foods, and the need for thorough cooking. Given that households were a common exposure setting across all demographic groups, community-based interventions may be more effective than general messaging. Also, given the persistently high prevalence of V. parahaemolyticus, targeted interventions should cover the entire “catch to consumption” chain of marine products. Finally, the sharp increase in Salmonella spp. positivity in 2024 calls for targeted investigations into local food supply chains, particularly poultry, egg, meat, and fruit products, along with enhanced supervision and sampling of poultry and livestock products.
This study has several limitations. First, the design is descriptive. Therefore, no multivariable regressions or causal inferences were conducted. Hence, all interpretations should be considered speculative rather than conclusive. Second, the data were derived from hospital-based sentinel surveillance, which may not have captured mild cases that did not seek medical care. Furthermore, pathogen testing was systematic but not universal; thus, some cases may have been missed. Third, data on pregnancy status was not collected, which may be relevant given the potential susceptibility of pregnant women to certain foodborne pathogens. Finally, the COVID-19 pandemic may have influenced healthcare-seeking behavior and exposure patterns. Future research incorporating molecular subtyping techniques (eg, whole genome sequencing) is needed to trace infection sources and better understand the transmission dynamics of the emerging Salmonella spp. strains in Shengsi County.
Conclusion
Based on six-year sentinel surveillance data from Shengsi County, we found that local FBDs exhibited distinct epidemiological profiles characterized by a summer peak, a predominance of adult cases, and household exposure to marine food products as the primary setting for infections. Throughout the study period, V. parahaemolyticus maintained its role as the dominant, endemic pathogen. Notably, Salmonella spp. positivity increased sharply in 2024, with 11 positive cases out of 118 tested (9.32%), compared to only 3 positive cases in total during the 2019–2023 period (annual positivity rate 0–1.09%). Future efforts should focus on strengthening the safety of marine products and household kitchen hygiene, maintaining continuous pathogen surveillance, and optimizing the regulation of local food supply chains.
Abbreviations
FBD, Foodborne disease; CDC, Center for Disease Control and Prevention.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval Statement
This study was approved by the Ethics Committee of Shengsi County Center for Disease Control and Prevention (Approval No. SSCDC-IEC-2025-004) along with a waiver of informed consent. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. All data were deidentified after collection and analyzed anonymously.
Acknowledgments
The authors sincerely thank the staff from the Centers for Disease Control and Prevention and the sentinel hospitals for their invaluable support and contributions to this study.
Author Contributions
All authors made a significant contribution to the work reported here, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the key grants of Department of Science and Technology of Zhejiang Province (2024C03216, 2025C02186); the Key Program of Health Commission of Zhejiang Province/Science Foundation of National Health Commission (WKJ-ZJ-2523); the National Key Research and Development Project by the Ministry of Science and the Technology of China (2023YFC2308705); the Zhejiang Provincial Medical and Health Science and Technology Plan (2023RC143); and the Zhejiang Provincial Disease Prevention and Control Science and Technology Plan (2025JK014); the Disease Prevention and Control Innovation Team of Zhejiang Province (2026JKC-04); the Young Talent Support Program of Zhejiang Provincial Association for Science and Technology; the Young Emerging Talents in Medicine of Zhejiang Province.
Disclosure
The authors declare that they have no competing interests.
References
1. Faour-Klingbeil D, CD Todd E. Prevention and control of foodborne diseases in Middle-East North African countries: review of national control systems. Int J Environ Res Public Health. 2019;17(1):70. doi:10.3390/ijerph17010070
2. Torgerson PR, Devleesschauwer B, Praet N, et al. World Health Organization estimates of the global and regional disease burden of 11 foodborne parasitic diseases, 2010: a data synthesis. PLoS Med. 2015;12(12):e1001920. doi:10.1371/journal.pmed.1001920
3. Ruoyu W, Baishi H, Zhuolin P, Ye L. Analysis of the geographic distribution and influencing factors of foodborne diseases among Chinese residents. World Reg Stud. 2020;29(01):168–10.
4. Chen L, Sun L, Zhang R, Liao N, Qi X, Chen J. Surveillance for foodborne disease outbreaks in Zhejiang Province, China, 2015–2020. BMC Public Health. 2022;22(1):135. doi:10.1186/s12889-022-12568-4
5. Lai YH, Chung YA, Wu YC, Fang CT, Chen PJ. Disease burden from foodborne illnesses in Taiwan, 2012–2015. J Formos Med Assoc. 2020;119(9):1372–1381. doi:10.1016/j.jfma.2020.03.013
6. Paudyal N, Pan H, Liao X, et al. A meta-analysis of major foodborne pathogens in Chinese food commodities between 2006 and 2016. Foodborne Pathog Dis. 2018;15(4):187–197. doi:10.1089/fpd.2017.2417
7. Jiang D, Han H, Guo Y, et al. Epidemiological characteristics of sporadic foodborne diseases caused by vibrio parahaemolyticus — China, 2013–2022. China CDC Weekly. 2024;6(51):1354–1359. doi:10.46234/ccdcw2024.269
8. Wang T, Li W, Zhang R, et al. Epidemiological features of nontyphoidal Salmonella infections reported to foodborne disease surveillance system in China, 2013–2022. BMC Public Health. 2025;25(1):2258. doi:10.1186/s12889-025-23439-z
9. Chen L, Wang J, Chen J, et al. Epidemiological characteristics of Vibrio parahaemolyticus outbreaks, Zhejiang, China, 2010–2022. Front Microbiol. 2023;14:1171350. doi:10.3389/fmicb.2023.1171350
10. He Y, Wang J, Zhang R, et al. Epidemiology of foodborne diseases caused by Salmonella in Zhejiang Province, China, between 2010 and 2021. Front Public Health. 2023;11:1127925. doi:10.3389/fpubh.2023.1127925
11. Zhu Q, Zong W, Wu Y, Fu P, Dai Y. Foodborne disease outbreaks before and during the COVID-19 pandemic in Jiangsu Province, China. One Health. 2025;21:101154. doi:10.1016/j.onehlt.2025.101154
12. China NHCotPsRo. Foodborne disease surveillance and reporting regulations (Trial). 2019 [cited October 17, 2019]. Available from: https://www.gov.cn/zhengce/zhengceku/2019-11/13/content_5451649.htm.
13. Chen L, Chen J, Wang J, et al. Surveillance of chemical foodborne disease outbreaks in Zhejiang Province, China, 2011–2023. Foods. 2025;14(6):936. doi:10.3390/foods14060936
14. Gao S, Chen Q, Chen L, et al. Analysis of foodborne outbreaks in Wenzhou City, China, 2012–2022. Epidemiol Infect. 2024;152:e175. doi:10.1017/S0950268824001626
15. Wang Y, Ni Q. Analysis of active surveillance results of foodborne diseases in a sentinel hospital in Tianjin from 2019 to 2023. J Appl Prev Med. 2025;31(04):406–409.
16. Zhang W, Chen K, Zhang L, et al. The impact of global warming on the signature virulence gene, thermolabile hemolysin, of Vibrio parahaemolyticus. Microbiol Spectr. 2023;11(6):e0150223. doi:10.1128/spectrum.01502-23
17. Wu P, Liu J, Dai Y, et al. Investigation of foodborne disease outbreaks caused by vibrio parahaemolyticus in China’s Mainland from 2010 to 2020. Chin J Food Hyg. 2024;36(1):73–78. doi:10.13590/j.cjfh.2024.01.012
18. Center NFSRA. Do not take foodborne disease prevention and control lightly during the tourism season. China Food Safety News; 2024. Available from: http://paper.cfsn.cn/content/2024-08/06/node_3.htm.
19. Hongqiu L, Yunchang G, Zhitao L, et al. Analysis of foodborne disease outbreaks in Chinese mainland in 2022. Chin J Food Hyg. 2023. doi:10.13590/j.cjfh.2024.08.011
20. Chen J, Liu Q, Luo S, et al. Epidemiological characteristics of foodborne disease outbreaks in Chongqing from 2003 to 2023. PLoS One. 2026;21(3):e0342130. doi:10.1371/journal.pone.0342130
21. Health N. Salmonellosis - prevention guidelines. Available from: https://www.health.nsw.gov.au/Infectious/factsheets/Pages/salmonella-translations/chinese-simplified.aspx.
22. Shuangshuang H, Kai M, Yijing Z, Xiang H. Analysis of the epidemiological characteristics of foodborne diseases caused by Vibrio parahaemolyticus from 2018 to 2022. Chin J Food Hyg. 2025;37(08):778–785. doi:10.13590/j.cjfh.2025.08.013
23. Love NK, Jenkins C, McCarthy N, Baker KS, Manley P, Wilson D. International travel as a risk factor for gastrointestinal infections in residents of North East England. Epidemiol Infect. 2024;152:e97. doi:10.1017/S0950268824000827
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.