Back to Archived Journals » Clinical Audit » Volume 16
Seniors Improved the Documentation of Junior Physicians’ Medical Records in a Teaching Hospital in Ethiopia
Authors Arega B ![]() , Minda A, Admasu A, Teshome A, Tewabe E
, Minda A, Admasu A, Teshome A, Tewabe E ![]() , Kibret A, Mamo D, Agunie A
, Kibret A, Mamo D, Agunie A
Received 20 September 2023
Accepted for publication 15 March 2024
Published 19 March 2024 Volume 2024:16 Pages 19—27
DOI https://doi.org/10.2147/CA.S441196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zoka Milan
Balew Arega,1 Abraham Minda,2 Andualem Admasu,2 Ayele Teshome,3 Elias Tewabe,1 Alemu Kibret,4 Dawit Mamo,1 Asnake Agunie2
1Department of Internal Medicine, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia; 2Department of Health Care Quality, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia; 3Department of Health System Capacity Building, Ministry of Health, Addis Ababa, Ethiopia; 4Deparment of Public Health, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Correspondence: Balew Arega, Yekatit 12 Hospital Medical College, Sidst Kilo Square, P.O.Box: 257, Addis Ababa, Ethiopia, Email [email protected]
Background: Complete medical documentation is an integral part of health system quality and safe patient care. However, this is compromised during duty hours while the physician is tired, high patient-to-physician ratio, and a lack of senior physician guidance from junior doctors. This quality improvement project aimed to improve medical documentation duty hours for admitted patients through the senior physician’s audit feedback strategies.
Methods: This quality improvement project was undertaken to improve the medical documentation of junior physicians for patients admitted during duty hours. We did it through the senior physician-led audit feedback system and by integrating the project tasks into senior physicians’ workflow. A collective group of project members teams, duty-assigned senior physicians, internal medicine residents, medical interns, nursing team, internal medicine, quality personnel, internal medicine department heads, and clinical vice provost. Quality improvement methods were used to test the role of the senior physician in improving the medical records documentation and maintaining the improvements obtained.
Results: The medical record documentation improved from 73% to 96.4% before and after implementing the improvement interventions, respectively. It was effectively maintained for six months (97.2%). The senior physician-led audited feedback strategies increased the clinical audit score by 24%.
Conclusion: The senior physician found to improve the junior physician’s medical record documentation of hospitalized patients during duty hours. The project also showed successful integration of the intervention into the routine clinical workflow.
Keywords: medical record, senior physicians, Ethiopia
Background
Clinical documentation is an integral part of every doctor’s job. Good record-keeping is essential for patient care, research, audit, and quality improvement purposes, accurate recording of consultations, and effective communication within the multidisciplinary team. Documentation is a legal requirement and is a fundamental factor if a medico-legal issue were to be raised whereby the healthcare professional and the hospital trust could be held accountable.1 However, for a variety of reasons, healthcare providers are continuously challenged to maintain proper medical documentation. These might be related to physician burnout, ambiguity about the precise definition of a diagnosis, the presence of multiple diagnostic criteria, a lack of good historians, an absence of attendants for critical patients, and a lack of training for junior doctors.2 Poor medical documentation mainly occurs during duty hours, an out-of-balance patient-to-physician ratio, and tired clinical providers all contribute to the problem’s escalation.3
Improving the quality of medical record documentation is becoming an increasingly important part of health system patient care and one of the key indicators of healthcare delivery service quality.4 Previous research showed that audit and feedback, through a systematic assessment of care against specified standards/ criteria and the implementation of change, significantly increase the quality of medical record documentation and outcomes.5,6
Senior physicians’ participation may enhance the quality of medical documentation done by the junior physician (general, specialty students, or interns) using the principle of the audit feedback cycle.7 The audit feedback cycle to improve medical documentation can be done by using robust methodologies that integrate it into the current workflow, practical guidance for junior physicians by senior physicians, ensuring adherence to the set protocol, and continuous monitoring of the improvement initiative by the institution manager.8
In teaching hospitals, the junior physician including specialty students (residents) and interns performs the initial patient evaluations and maintains medical records of newly admitted patients. The senior physicians are verbally consulted by juniors as necessary. A previous study in an Ethiopian teaching hospital found that nearly two-thirds (59%) of medical records were incomplete, and the problem is expected to worsen when the patient is admitted during duty hours.9
A monthly clinical report by the study hospital quality team that the medical documentation of patients hospitalized during duty hours had incomplete medical records. In this project, we conducted a quality improvement project to answer the following questions. First, is the engagement of senior physicians improving the quality/ completeness/ medical record documentation done by junior physicians for patients admitted during duty through an audit feedback system? Secondly, how well-integrated and sustainably implemented is this intervention within the institution’s clinical workflow?
Materials and Methods
Project Design, Setting, and Period
This is a quality improvement project that included structured auditing of junior physician clinical documentation of patients admitted during duty periods. The project was completed within a twelve-month quality project including a six-month implementation and another six months to ensure the sustainability of the project. Based on the preintervention baseline finding, relatively long intervention, and sustainability periods, we target to make the medical records documentation completeness 95% and above.
We conducted the project at Yekatit 12 Hospital Medical College, a teaching hospital, in Addis Ababa, Ethiopia. The hospital has about 500 beds and 21 departments. In 2020, the hospital fully implemented electronic medical records (EMR) system in all departments, including the pharmacy and laboratory, and every patient’s evaluation is documented on the EMR. The hospital receives patients referred by health facilities within its coverage area in Addis Ababa as well as from other health facilities throughout the country. There are many different types of professionals working at the college, including doctors (junior and senior doctors), nurses, midwives, health officers, non-clinical academic staff, and non-clinical supportive staff. Those with specialty education in clinical science are considered senior physicians, while general practitioners, last year’s medical students (interns), or specialty students (residents) are considered junior physicians.
The scope of physicians who initially evaluate, document, and treat patients in the hospital differs by service area. In terms of outpatient care, general practitioners evaluate and treat patients who visit general medical clinics, whereas senior physicians evaluate and treat patients who visit referral clinics. For inpatient care, either during working hours or duty hours the initial evaluation, medical record documentation recording, and treatment planning are done by the medical interns and internal medicine residents. The duty hours are 16 hours (5:30 pm to 2:00 a.m. including 1 hour at lunchtime) during the working days, and 24 hrs during the weekends and holidays. The vital sign recording, medication administration, and nursing care are done by the respective ward’s nurse.
This project was carried out specifically in the internal medicine department wards. The department has 75 operational beds and five wards. Each ward is staffed during working hours by three to four interns, two internal residents, two senior physicians, and approximately 12 nurses. However, the number of treating teams during duty hours decreased by more than half in each ward compared to the respective working hours. The emergency department admitted the vast majority of patients admitted to inpatient care. Admission to inpatient care is commonly done late in the afternoon and during duty hours. This is because the bed became available in the afternoon after patients were discharged from wards. The admission decision from emergency departments is also made by the emergency senior physicians after a round and evaluation until lunchtime. It frequently results in a disproportional physician-to-patient ratio during duty hours, which has an impact on the quality of care and medical record documentation. The project team comprised junior physicians, nursing staff, senior physicians, internal medicine heads, the quality team, and senior managers of the hospital. All the team members were from our hospital, making interventions easier to carry out. The major responsibility of each team in the project is presented in Table 1.
 |
Table 1 The Project Team Members and the Responsibilities |
Project Strategy
We use the plan, do, study, and act (PDSA) approach to improve medical documentation, primarily through the audit feedback cycle, which is also used in similar previous studies.9,10 We derived several change ideas and chose some of them to test in the PDSA cycles. We conducted two PDSA cycles (PDSA 1 and 2) of interventions for six months (3 months each), and another six months of maintenance (PDSA 3) phase (Supplement 1 - PDSAs).
PDSA cycle 1: During this cycle, we formed the improvement team and made the task division specified in Table 1. We gave training about the aim of the project, data collection procedure, data measurement, monitoring, and subsequent plans. The duration of this cycle of the project was from September to November 2021 for 12 weeks. Using the control chart, we found areas of improvement, and the overall medical record completeness plan which was 95% above was achieved. The improvement team decided to proceed to PDSA2 by adding some improvement points and tools. These include 1) Creating a department webpage (telegram) for posting the audit result early morning, and 2) the patient’s medical record completeness issue incorporated as one agenda in the college’s weekly clinical form.
PDSA Cycle 2: We hypothesized by incorporating additional interventions listed, telegram page, and weekly form, in PDA cycle I, we became more successful in completing the medical records of duty hours admitted patients. Other interventions applied during PDSA cycle 1 were continued in this cycle. We believe that failure to integrate and test these tools would prevent the improvement from being maintained. Based on the outcome, the sign of improvement found in cycle I was further improved and the improvement team decided to implement the change intervention and monitoring for the following six months. This cycle was run from December 2021 to February 2022.
Maintenance phase: We thought it crucial to assess the sustainability of quality improvement interventions found in the PDSA cycles for an extended period of six months. We incorporate all the change interventions and tools in this cycle. The control chart is used to analyze the results. This phase was run from March to August 2022.
Intervention Tools and Process
We utilized basic and frequently used clinical criteria adopted from the national clinical audit guidelines for our data collection.11 The standardized definition of the components of the intervention is presented in Table 2. We developed a data auditing tool based on the national clinical audit standards.11 The following questions were developed to audit the appropriate documentation of junior physicians. 1) Were patients timely evaluated? 2) Was appropriate history documented? 3) Were appropriate physical examinations documented? 4) Were appropriate investigations documented? 5) Were appropriate diagnoses documented? 6) Were management plans documented? 7) Were medication sheets documented? 8) Were order sheets documented? And 9) Were vital signs documented? The data extraction sheet is presented in Supplement 2.
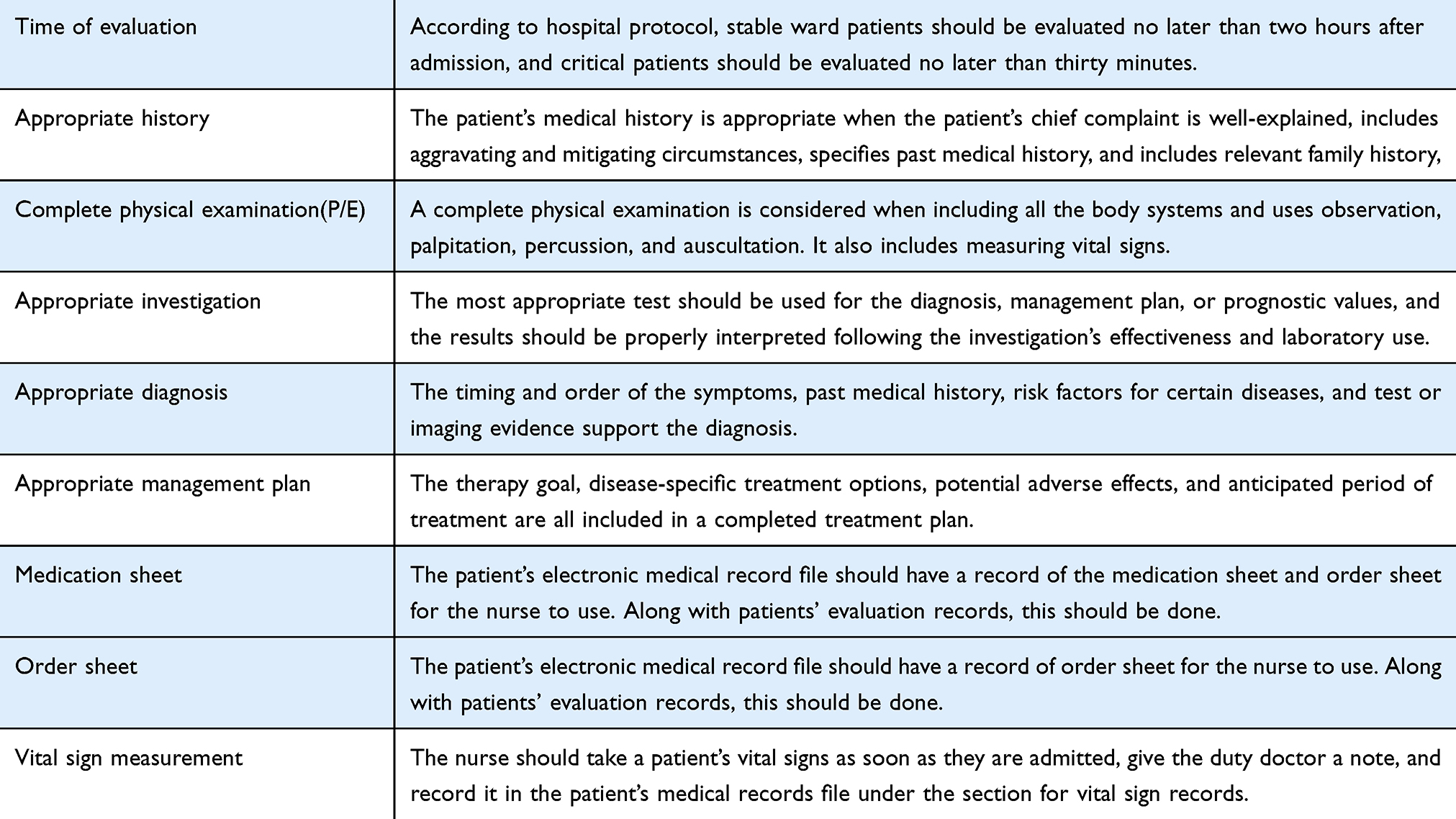 |
Table 2 The Standard Auditing Tool Adopted from the National Guideline |
The intervention process is conducted as follows. First, after the patient is admitted to the ward, the duty junior physician evaluates the patient and documents his/her clinical assessment on the electronic medical record. Second, the senior physician evaluated the junior physician’s clinical documentation using the prepared tool (Supplement 2). Third, the senior physician evaluates the newly admitted patients along with the junior physician. Fourth, the senior physician gave feedback and recommendations (if any) to the junior physician based on his audit findings and what the patients had. Finally, the senior physician re-audits the junior’s assessment and submits the audit result to the department. The process is presented in Supplement 3.
Workflow and Baseline Study Data
Before the start of the current project, the workflow and clinical practice of study wards during duty hours were as follows: −1) The senior physicians did not stay the entire night in the hospital, participated in patient evaluations in person, and did not review the medical records, documentation, and treatment plan of the junior physicians on duty. The duty-assigned senior physician consulted the junior doctor’s members through the so-called on-call duty over the phone. 2) The junior doctors assessed newly admitted patients and recorded medical information on the electronic medical record. 3) the nursing duty team takes the patient’s vital signs, administers medication, and provides nursing care. 4) The medical records of the junior physician’s evaluation and nursing documentation were independently reviewed by the college quality and clinical audit team. Their audit on medical records documentation (completeness), management plan, justified investigation, nursing care, and vital sign monitoring of admitted patients. The team extracted three months (June to August 2021) of data from the EMR of each patient’s file. They found a significant gap in the completion of medical records documentation for patients admitted during duty hours. We used this finding as baseline data. Based on this, we planned to improve the overall level of medical documentation completion of all newly admitted patients in internal medicine wards during duty time.
Measures and Analysis
The project outcome measure was the medical record completeness of duty hours admitted patients. The evaluation tool contains nine core measuring variables used to audit the medical documentation of the junior physician evaluation. The overall medical completeness in each PDSA cycle is calculated. We use a run chart to detect signal improvement during PDSA cycle I and II. An improvement is considered when five or more consecutive points all increase over 3 months (12 weeks). During the maintenance phase (PDSA III cycle), we use (specifically, a u-chart) control chart to determine that a process/ change made/ is controlled with only common cause variation.12
Results
Our main outcome measure was overall medical record completeness with the core elements that should be included in every patient’s medical record documentation. Throughout the project, weekly data collection allowed us to rapidly assess changes in our data and determine their relation to individual PDSA cycles. We have seen data improvement with all of our PDSA cycles, which was sustained following our third PDSA cycle for six months.
Data were obtained from 343 patients hospitalized during duty hours for our preintervention baseline study, and the total clinical documentation completeness score was 73% (Figure 1).
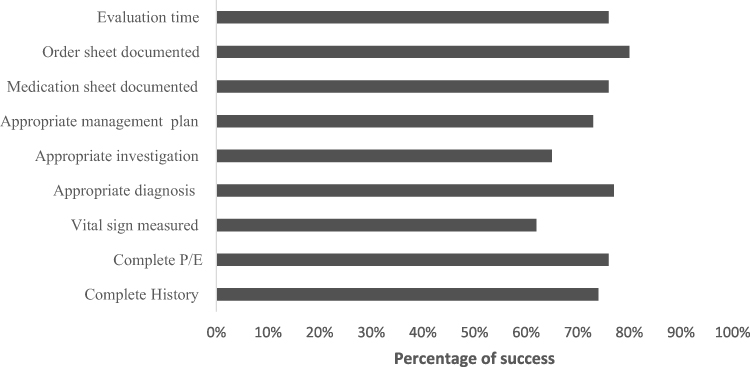 |
Figure 1 Baseline study results of newly admitted patients’ medical record documentation during duty hours. |
During the intervention periods, 1420 patients were admitted and audited, including 382 during the PDSA 1 cycle, 413 during the PDSA 2 cycle, and 605 during the maintenance phases. On the PDSA 1 cycle, we reached 95.88% medical record completeness in November 2021, a 22.9% improvement over the baseline data (Figure 2A). After the telegram page and weekly form were added to the intervention, this improvement was further increased over the following 3 months and reached 96.14% which was 23.14% higher than the baseline during PDSAII (Figure 2B). The score of each study variable during the intervention phase (PDSA1 and PDSA1 cycle) is presented in Figure 2C.
 |
Figure 2 (A–C) Intervention periods study results of newly admitted patients’ medical record documentation during duty hours. Abbreviations: CL, confidence limit, LCL, lower confidence limit, UCL, upper confidence limit. |
The result of the improvement made throughout the PDSA cycles is maintained over the following six months (97.2%) (Figure 3A) and showed a 24.2% improvement from the baseline data. The score of each study variable during the maintenance phase is presented in Figure 3B.
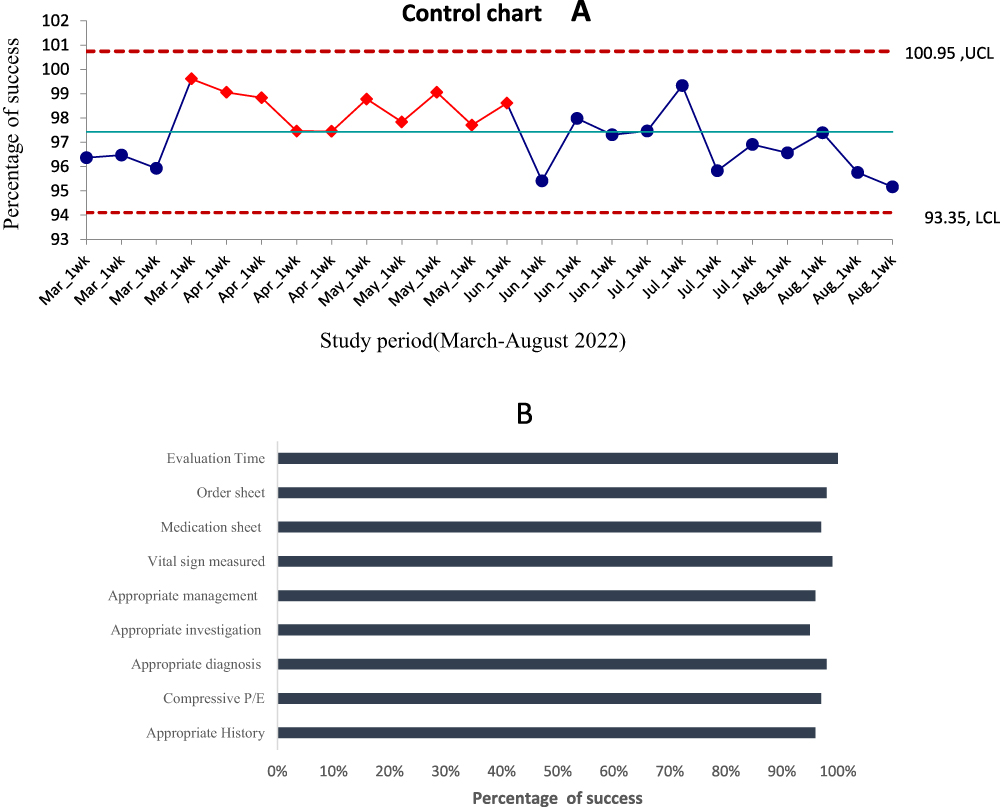 |
Figure 3 (A and B) Maintenance period medical record documentation among newly admitted patients during duty hours. |
The overall average medical record completeness over the entire project period is 96.4% with a net 23.4% improvement from the pre-intervention periods.
Discussion
Lesson Learned
Our project demonstrated an improvement in record completeness and was effectively carried out over an extended period to ensure the program’s sustainability. The finding revealed that senior physician-led audit feedback is found to improve the medical records completeness of the junior physicians for patients admitted during duty hours when problems are anticipated to get worse. The subsequent intervention cycles implemented resulted in a significant effect on medical records completeness scores during the period from September 2021 to August 2022.
The previously conducted studies in the country assessed the completeness of medical records documentation among hospitalized patients13,14 or evaluated the effect of short-term training on medical record documentation15 but no published quality improvement project evaluated the effect of well-trained physicians on medical record documentation. This might be ignored due to the following reasons. First, despite increasing over the last 5–10 years, the number of senior physicians was few at the national level. Second, the medical documentation was peppered based in almost all governmental hospitals which is cumbersome to trace and monitor patients’ medical documentation. Third, at the national level, the concept of patient-quality care was ignored and the health sectors mainly focused on expanding the healthcare facilities at the national level.
In our quality improvement project, we designed a phased improvement project that spanned two cycles of testing the intervention and one cycle of maintaining the change. Each of the interventions was designed with a slightly different change to the existing practice at that time to address the identified problems. We believe that this was successful since the change idea aimed to integrate into the doctor’s workflow, using this as a place for prompts and more effective than the introduction of a new workflow and the requirement for additional labor.
Improvement huddles, such as quick staff meetings regularly to discuss performance, standard work, and regular program monitoring, have been shown in earlier research to be crucial tools to sustain the improvement of a facility.16,17 The weekly audit submission review meeting including the hospital managers, the department coordinator’s reminders of the duty of senior physicians, and the regular monitoring actions of the quality team and telegram page all contribute to the sustainability of our project in this case.
This pragmatic approach to facility-based improvement projects can be adapted and scalable the similar institutions for improving medical record documentation. However, context factors in the local setting relevant to implementation success should be validated.18,19 This finding also served as an important learning experience for designing another quality improvement for another problem, such as improving patient outcomes, reducing hospital stays, preventing in-hospital complications such as hospital-acquired infection, and others.
Limitations
Although our findings showed an improvement in the medical record documentation completeness among duty hours admitted patients, we did not see a corresponding improvement in terms of overall increased incidence of patient discharge rate, clinical improvement, and reduced mortality among the patients on the ward (outcome measure). In addition, higher scores on the medical documentation completeness and order sheet did not ensure the actual delivery of the service to the patients. We felt that the next quality improvement project will evaluate the senior physicians’ impact on actual patient care quality improvement.
Conclusion
We demonstrated a significant improvement in medical record documentation completeness of admitted patients during duty hours when the senior physician-led audit feedback was introduced in internal medicine during the two intervention phases. When this was enrolled for the subsequent six months to ensure sustainability, there was still further improvement. With a standardized platform now established, another department in the hospital adopted the intervention and monitored it by the college quality team. After a context assessment of an institution, this project easily adapted to other similar health systems in the country.
Ethical Approval
This project was designed to improve the service for patients. It was undertaken using improvement science methodology and was not deemed to require ethics approval. Yekatit 12 Hospital Medical College’s ethical approval committee exempts the ethical approval. The interventions made were designed to improve the quality of medical documentation and optimize routine accepted good practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Koh J, Ahmed M. Improving clinical documentation: introduction of electronic health records in pediatrics. BMJ Open Qual. 2021;3:10.
2. Lorenzetti DL, Quan H, Lucyk K, et al. Strategies for improving physician documentation in the emergency department: a systematic review. BMC Emerg Med. 2018;18(1):36. doi:10.1186/s12873-018-0188-z
3. Malley KJ, Cook KF, Price MD, et al. Measuring diagnoses: ICD code accuracy. Health Serv Res. 2005;40(5p2):1620–1639. doi:10.1111/j.1475-6773.2005.00444.x
4. Beracochea E, Dickson R, Freemand P, Thomason J. Case management quality assessment in rural areas of Papua New Guinea. Trop doctor. 1995;25(2):69–74. doi:10.1177/004947559502500207
5. Ivers N, Jamtvedt G, Flottorp S, et al. Audit and feedback effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2012;6(6):CD000259.
6. Rosenbaum BP, Lorenz RR, Luther RB, et al. Improving and measuring inpatient documentation of medical care within the MS-DRG system: education, monitoring, and normalized case mix index. Perspect Health Inf Manag. 2014;2:11.
7. National Institute for Clinical Excellence. Principles for Best Practice in Clinical Audit. Abingdon: Radcliffe Medical Press; 2002.
8. Services CFMM. ICD- 10- CM official guidelines for coding and reporting FY2020; 2020.
9. Glen P, Earl N, Gooding F, Lucas E, Sangha N, Ramcharitar S. Simple interventions can greatly improve clinical documentation: a quality improvement project of record keeping on the surgical wards at a district general hospital. BMJ Qual Improv Rep. 2015;4(1):1. doi:10.1136/bmjquality.u208191.w3260
10. Zucco L, Webb C. Improving the documentation of the daily review of patients in general intensive care. BMJ Qual Improv Rep. 2014;3(1):1. doi:10.1136/bmjquality.u539.w496
11. Ethiopia Ministry of Health. This national clinical audit implementation guide is designed to support the effective implementation of the Health Service Transformation in Quality (HSTQ) guide in all public health facilities; 2019.
12. Gupta M, Kaplan HC. Measurement for quality improvement: using data to drive change. J Perinatol. 2020;40(6):962–971. doi:10.1038/s41372-019-0572-x
13. Endriyas M, Kawza A, Alano A, Lemango F. Quality of medical records in public health facilities: a case of Southern Ethiopia, resource-limited setting. Health Informa J. 2022;28(3):14. PMID: 35793497. doi:10.1177/14604582221112853
14. Sahile AT, Teka MW, Teshome MA, Jata TD. Medical record documentation system in Ethiopia; 2020.
15. Tola K, Abebe H, Gebremariam Y, Jikamo B. Improving completeness of inpatient medical records in Menelik II referral hospital, Addis Ababa, Ethiopia. Adv Public Health. 2017;2017:8389414. doi:10.1155/2017/8389414
16. Silver SA, McQuillan R, Harel Z, et al. How to sustain change and support continuous quality improvement. Clin J Am Soc Nephrol. 2016;11(5):916–924. doi:10.2215/CJN.11501015
17. Kaplan HC, Brady PW, Dritz MC, et al. The influence of context on quality improvement success in health care: a systematic review of the literature. Milbank Q. 2010;88(4):500–559. doi:10.1111/j.1468-0009.2010.00611.x
18. Beer M, Nohria N. Cracking the code of change. Harvard Business Review. 2000;78(3):133–141.
19. Jacob A, Raj R, Alagusundaramoorthy S, Wei J, Wu J, Eng M. Impact of patient load on the quality of electronic medical record documentation. J Med Educ Curric Dev. 2021;8:238. doi:10.1177/2382120520988597
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.