Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Self-reported efficacy of neurofeedback treatment in a clinical randomized controlled study of ADHD children and adolescents
Authors Duric NS, Aßmus J ![]() , Elgen I
, Elgen I
Received 18 April 2014
Accepted for publication 22 May 2014
Published 2 September 2014 Volume 2014:10 Pages 1645—1654
DOI https://doi.org/10.2147/NDT.S66466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Nezla S Duric,1–3 Jörg Aßmus,4 Irene B Elgen1,5
1Department of Clinical Medicine, University of Bergen, Bergen, Norway; 2Center for Child and Adolescent Mental Health, University of Bergen, Bergen, Norway; 3Department of Child and Adolescent Psychiatry, Helse Fonna Haugesund Hospital, Haugesund, Norway; 4Center for Clinical Research, Haukeland University Hospital, Bergen, Norway; 5Department of Child and Adolescent Psychiatry, Haukeland University Hospital, Bergen, Norway
Background: Many non-pharmacological treatments for children and adolescents with attention-deficit/hyperactivity disorder (ADHD) have been attempted, but reports indicate that most are ineffective. Although neurofeedback (NF) is a treatment approach for children with ADHD that remains promising, a variety of appropriate measures have been used in reporting and evaluating its effect.
Objective: To report the self-evaluations of NF treatment by children and adolescents with ADHD.
Methods: Randomized controlled trial in 91 children and adolescents with ADHD, aged less than 18 years (mean, 11.2 years) participated in a 30-session program of intensive NF treatment. Participants were randomized and allocated by sequentially numbered sealed envelopes into three groups: methylphenidate (MPH) as an active control group, and two trial groups NF with MPH, and NF alone. ADHD core symptoms and school performance were given on a scale of 1 to 10 using a self-reporting questionnaire, and the changes in these scores after treatment were used as the self-reported evaluation. Basic statistical methods (descriptive, analyses of variance, exact χ2 test, and paired t-test) were used to investigate the baseline data. Changes in ADHD core symptoms and treatment effects were investigated using a general linear model for repeated measures.
Results: Eighty participants completed the treatment study and 73 (91%) responded sufficiently on the self-reporting questionnaires. The treatment groups were comparable in age, sex, and cognition as well as in the baseline levels of core ADHD symptoms. All treatments resulted in significant improvements regarding attention and hyperactivity (P<0.001), and did not differ from each other in effectiveness. However, a significant treatment effect in school performance was observed (P=0.042), in which only the NF group showed a significant improvement.
Conclusion: The self-reported improvements in ADHD core symptoms and school performance shortly after treatment indicate NF treatment being promising in comparison with medication, suggesting NF as an alternative treatment for children and adolescents who do not respond to MPH, or who suffer side effects. Further long-term follow-up is needed.
Keywords: attention deficit/hyperactivity disorder (ADHD), neurofeedback (NF), self-report, randomized controlled trial (RCT)
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a serious health problem, and adequate multimodal treatment is necessary to avoid development of behavior problems, academic impairment, social dysfunction, and poor self-esteem.1 Almost one in four children do not respond sufficiently to central stimulation treatment,2 and ADHD symptoms can continue after psychopharmacological treatment has been withdrawn.3 Alternative treatments are therefore continuously being sought.
Recently, neurofeedback (NF) has been proposed as a treatment for ADHD that improves attention and decreases hyperactivity symptoms.4–8 NF is an electroencephalographic (EEG) operant-conditioning training technique that helps individuals to alter their brain activity.9 It is a kind of behavioral therapy aimed at developing skills for self-regulation of cortical activity.10,11 This method uses real-time EEG displays to develop skills which regulate brain activity.11–13 NF is aiming to normalize the EEG by improving cortical functioning.14 The patient learns to enhance the EEG desired frequencies and suppress the undesired ones in the form of a rewards system.15 This may affect for example attention, or other neurocognitive processes.16
In mostly uncontrolled and non-randomized studies NF has been shown to provide therapeutic benefits to patients with ADHD.7,8,17 A meta-analysis by Arns et al and Lofthouse et al reviewed randomized and non-randomized, published and unpublished trials and illustrated that some studies are limited by incomplete randomization (even randomized trials), small sample size, semi-active control groups, and no placebo and that more randomized, placebo control studies are needed.18,19 Lately, randomized studies from Duric et al and Meisel et al found promising evidence of ADHD symptom improvements in treatment with NF.20,21 Significant improvements of ADHD symptoms over time after NF treatment were found in a double-blind placebo feedback-controlled design by Lansbergen et al.22 Recently, Sonuga-Barke et al suggested in a review of randomized controlled trials, alternative treatment of ADHD including NF and suggested that better evidence for efficacy of NF is required with blinded assessments.23
While NF has been reported to improve core ADHD symptoms, increase self-esteem,3,4,8 and improve learning,9 the mechanism of action still remains unknown. However, it is important to explore the effect by self-reporting as well. For adults few self-report studies have indicated that NF is comparable to treatment with stimulant medication.24–26
Using self-report in studies of children and adolescents with ADHD has been poor, with inconsistent and divisive results.25,27 The validity of health-quality reports is much greater when individuals report their own perceptions.28 The reliability of self-reports and the ability of teachers, parents, and key workers to assess ADHD symptoms have been questioned.26 Although parent reports differ from those of children, the child has valuable awareness of own experiences, especially for medical history, behavior, and health care.26,29 While some studies of children with ADHD suggest that despite functional problems in areas such as academics and development, self-reports tend to under-report the presence of symptoms,30,31 other studies indicate that they describe their difficulties adequately.30,31 Among self-report studies, those that have used NF are virtually nonexistent, although reports from parents and teachers do exist.32
One of the most basic reasons for investing resources in child self-report health data is that parents appear as proxy respondents and their reports correlate poorly with those of their children, which is a reason often cited for not assessing children directly. Despite the increasing acceptance of adolescents’ self-reports, their concordance with reports from their parents is not any better than that of parents and children.33,34 In the present study we wanted to explore self-reported efficacy of NF treatment in a clinical, randomized, and controlled study of ADHD children and adolescents.
Methods
Randomized controlled trial NCT01252446
Subjects and randomization
Children and adolescents with ADHD (aged under 18 years) who were diagnosed with ADHD according to the International Statistical Classification of Diseases and Related Health Problems Tenth Revision (ICD-10) at the Child and Adolescent Mental Health Clinic, Fonna Trust, Haugesund, Norway, from 2007 to 2009, were invited to participate in the study.32,35,36 One hundred and thirty participants with ADHD were randomly assigned to one of three groups: 1) a group treated only with methylphenidate (MPH) defined as active control group, and two experimental groups; 2) a group treated with NF and MPH (NF/MPH group), and 3) a group treated with NF (NF group). Randomization was performed using a random list with arbitrary numbers (0-1-2) in order to make three groups. No stratification regarding age, sex, or IQ was done.
Cognitive performance was assessed before starting treatment using the Wechsler Intelligence Scale for Children Revised edition (WISC-R).37 Subjects in the MPH and NF/MPH groups were administered MPH twice per day, at the recommended dose of 1 mg/kg, with total daily dosages ranging from 20 to 60 mg.
The Regional Ethics Committee on Medical Research approved the project protocol, and written consent was obtained from all of the children or parents.
ADHD
The population of Norwegian children who were referred for ADHD treatment during the 3 year period has been described in earlier publications.35,36 The children underwent diagnostic assessment to confirm the diagnosis of ADHD. In short, assessment included a clinical psychiatric interview and observations to assess ADHD and other appropriate diagnoses. Questionnaires regarding ADHD were filled out by the children, parents, and teachers of the children. A medical examination was done to exclude somatic conditions causing ADHD symptoms. A child psychiatrist evaluated the assessments and categorized the children as having ADHD or a non-ADHD condition according to ICD-10 diagnostic criteria.38
Treatment groups
The 130 participants with confirmed consent were randomly allocated by a coordinator into three groups: 1) the MED group, those treated with psychostimulant medication (MPH), 2) the NF + MED group, those treated with both NF and medication (MPH), and 3) the NF group, those only treated with NF.
Neurofeedback
Each participant was provided with 30 NF treatments for the duration of the study. Three sessions per week were conducted. The duration of each session was 45 minutes where each session started with 5 minutes of relaxation using alpha enhancement feedback, followed by two training sessions of twenty minutes each.
The system used for the recording was a Procomp Infinity from Thought Technology Ltd. (Montreal, QC, Canada) running Biograph Infinity software. This system is an eight channel, multi-modality encoder that is flexible, and designed for both clinical and research settings. The first two sensor channels provide ultimate signal fidelity (2,048 samples/s) for viewing raw EEG, electromyography (EMG), and electrocardiography (EKG) signals, and the remaining six channels (256 samples/s) can be used in combination with a variety of sensors such as EEG, EKG, EMG, skin conductance, heart rate, blood volume, pulse, and respiration. The system has an application suite which is a grouping of screens, computations, and protocols to be custom tailored to a user’s particular needs.
The NF training was based on the standard theta/beta protocol in Cz for ADHD treatments from Lubar (Association for Applied Psychophysiology and Biofeedback).39,40 In this protocol beta activity (16–20 Hz) is enhanced and theta (4–7 Hz) is suppressed.
In order to attach the electrodes to the scalp and ensure minimum impedance skin preparation was done with conductive Nuprep EEG skin gel (Weaver and Company, Aurora, CO, USA).41 The electrode placement was at Cz (based on the 10–20 system of electrode placement) for all patients referenced to an ear (unipolar derivation). During the NF session, brain activity was shown to the participant using visual and auditory feedback.
For the training theta activity was defined as 4–7 Hz, beta activity as 15–20 Hz. EMG activity, defined as 80–150 Hz, was also monitored. The goal was to decrease theta activity by inhibiting high amplitude theta activity and by simultaneously rewarding high amplitude beta activity. Successful treatment was defined as a significant increase in beta activity, and a decrease in theta and EMG activities. Rewards were given if participants could keep theta levels below threshold 70% of the treatment time and keep beta levels above threshold 20% of the time. Depending on the participant’s performance these reward thresholds were manually adjusted by the therapist. In addition, the therapist verbally reinforced the participant’s performance and helped with progress.
After each session, the therapist and participant discussed the session in order to enhance motivation and engagement for further treatment.
Self-reporting questionnaire (SRQ)
Due to the nature of ADHD, the number of questions in an SRQ was limited to ensure that each child would be able to complete the questionnaire. So for this study we developed an SRQ, with questions derived from other questionnaires, including the Self-rating Scale of Self-regulatory Function27 and the Piers-Harris Children’s Self-Concept Scale.42 The SRQ consisted of five single items, two concerning ADHD core symptoms (inattention, hyperactivity) and three regarding school performance (mathematics, reading, and writing skills); school performance was defined as the sum of the three items (Supplementary materials).
The children were asked how they would rate themselves on a scale of 1–10 with regard to inattention, hyperactivity, and school performance. The SRQ was assessed at different time points (T1, T2). The pre-treatment (T1) SRQ was assessed just before beginning the NF therapy, and the post-treatment (T2) SRQ was completed approximately 1 week after completing the therapy. The self-reported evaluation of treatment was thus calculated as the change in score from period T1 to T2 (T2–T1).
Statistical analyses
Basic statistical methods (descriptive, analyses of variance [ANOVA], exact χ2 test, paired t-test) were used to investigate the baseline data.
The pre–post changes as well as the treatment effects were investigated using a general linear model (GLM) for repeated measures, which was implemented for each subscale (inattention, hyperactivity, and school performance). The model included the raw scores at both time points as dependent variables and the treatment groups as independent factors. In the GLM, we tested both pre–post changes in the ratings as well as treatment effects (differences between the treatments). Significance of differences between the treatments was further examined using post hoc tests. Additionally, we estimated the standardized effect size ES δRM according to Morris and DeShon for each treatment change.43
The general significance level was set to 0.05. For the baseline investigation, we had to take into account the effects of multiple comparisons. However, we decided to set the significance level to 0.01, as a compromise between a Bonferroni correction and not accounting for multiple comparisons. In the GLM, we investigated only highly correlated variables, thereby reducing the number of comparisons. Therefore, we did not adjust the significance level. A correlation between self-report and parents’ report was performed. All computations were done using SPSS 21 (IBM Corporation, Armonk, NY, USA).
Results
Subjects
Of 130 randomized participants 91 completed the treatment, but only 80 participants agreed to fill out the SRQ (Table 1). However, three did not answer the SRQ for attention and hyperactivity (questions 1 and 2), and a further four participants did not complete the SRQ for school performance (question 3 to 5). The mean age for the 80 participants was 11.2±2.8 years, and the majority of participants were boys (81%).
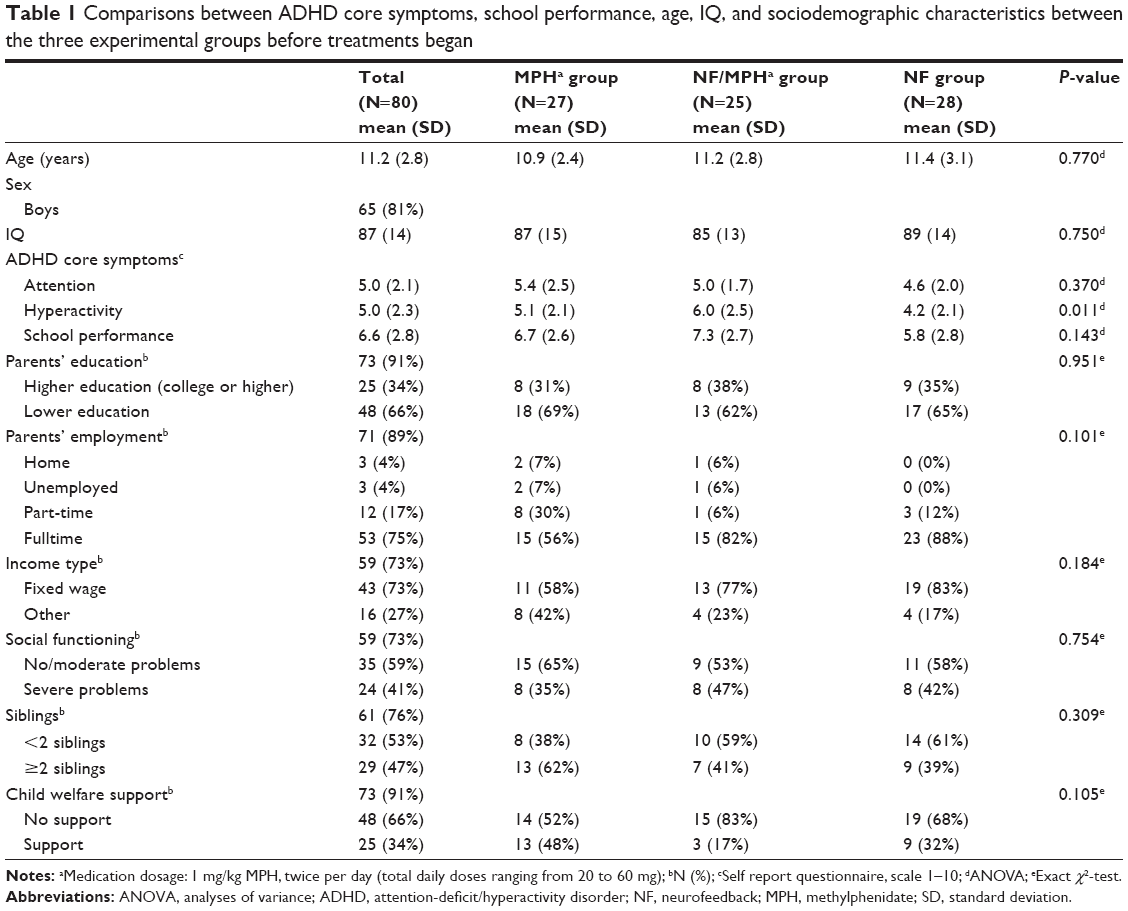 | Table 1 Comparisons between ADHD core symptoms, school performance, age, IQ, and sociodemographic characteristics between the three experimental groups before treatments began |
Dropouts
After randomization of 130 participants, a total of 39 children (30%) “dropped out” before or during the treatment.20 Before treatment started 29 participants (ten, eleven, and eight patients from groups 1–3, respectively) “dropped out” due to parental lack of interest, loss of child/adolescent motivation, or other practical reasons such as difficulties and costs of transportation, family situation. During treatment, a further ten participants (three, three, and four patients from groups 1–3, respectively) “dropped out” with no reason given. For the 91 participants completing treatment, eleven participants did not complete the SRQ (four, four, and three from groups 1–3, respectively). Of these 80 participants who completed SRQ, three of them missed the question concerning ADHD core symptoms (77) and additionally four participants did not answer on school performance (73). However, post-randomization analyses found the balance for variables age, sex, IQ, comorbidity, and socio-demography between the “dropouts” and treatment groups.
Treatment groups
Baseline properties of the study sample are given in Table 1. None of the characteristics (age, sex, IQ, and ADHD symptoms) was significantly different between the treatment groups (P>0.01), although differences in hyperactivity baseline scores almost reached significance (P=0.011). The three groups were comparable with regard to sociodemographic characteristics, including family constellation, siblings, parent education, economic factors, and other means of support such as child welfare and special school support.
Evaluation of pre–post changes
Pre–post changes and results of the GLM estimation are given in Table 2. We found a significant improvement in SRQ score for both attention (P<0.001) and hyperactivity (P=0.001) without adjustments. The effect sizes for all groups were positive. The significant pre–post changes disappeared after adjustment for age and sex.
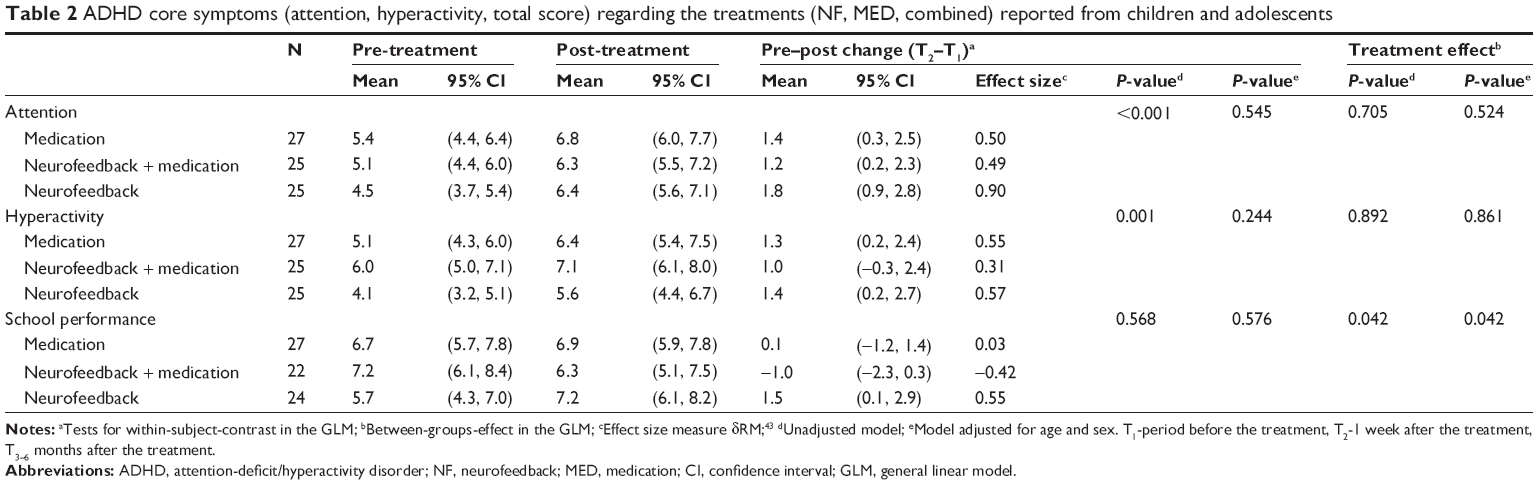 | Table 2 ADHD core symptoms (attention, hyperactivity, total score) regarding the treatments (NF, MED, combined) reported from children and adolescents |
For school achievement, the GLM analysis did not reveal any significant change in SRQ score after treatment (P=0.568, unadjusted). Note however, that school performance in the NF group did show a significant improvement (mean difference 1.5; 95% confidence interval [CI] 0.1 to 0.29).
Evaluation of treatment effect
Treatment effect was defined as the score difference between the treatment groups. We observed a significant effect of treatment on school performance (P=0.04), but not for hyperactivity (P=0.9) or attention (P=0.7) using the unadjusted model (Table 3). Similar results were obtained from the adjusted model. As seen in the results of the pre–post analysis, the NF group reported significant improvement in school performance (CI: NF, 0.1 to 2.9); the other groups did not (CI: MPH, −1.2 to 1.4; NF/MPH, −2.3 to 0.3).
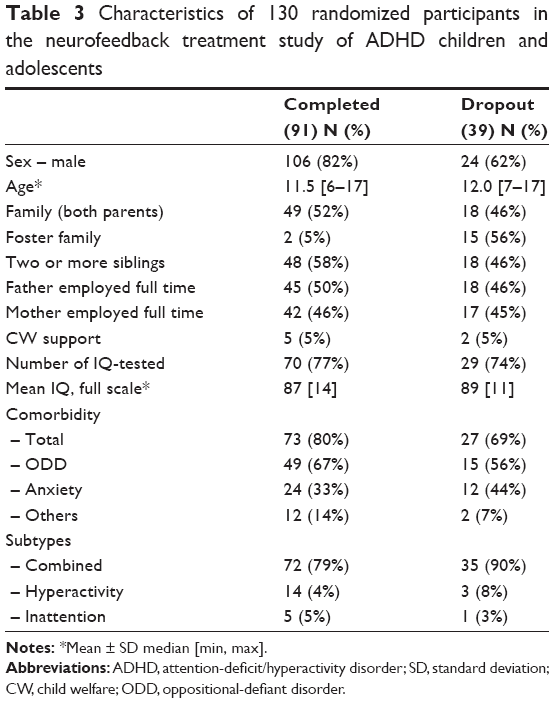 | Table 3 Characteristics of 130 randomized participants in the neurofeedback treatment study of ADHD children and adolescentsNotes: *Mean ± SD median [min, max]. |
School performance, tested by one-sample t-test (if the change score equals 0), increased for the NF group significantly regarding writing (P=0.04) and calculation (P=0.05). The MED group reported a significantly increased performance in calculation (P=0.03).
Correlation between the participants and parents
The two core symptoms of ADHD reported by parents were addressed in an earlier study.32 We did not find significant correlations between the reports from children and parents for any domain at a 5% level. The same pattern of correlation was found for both time points (T1 and T2).
Discussion
The present study randomly assigned ADHD children and adolescents to active control and two experimental groups evaluating NF with self-reports. Shortly after treatment participants in all three groups reported improvement in ADHD core symptoms, with no significant differences in ADHD symptoms between the groups.
Previous studies have seldom discussed self-reports in conjunction with NF treatment in young people with ADHD. While most studies have confirmed the difficulties in self-report design studies, they also express the importance of self-reporting in ADHD children and adolescents.27,44–46 In addition, considerable variation has been observed depending on the type of questions used for assessment.47 In the present study we wanted to explore the changes from one time to another using the same questions for the same participant and therefore we found it reasonable to compose a short form to make sure that as many participants as possible were able to complete the SRQ. This was accomplished in the present study for more than four in five participants.32,48
Children reported similar effects in all three measured factors across the three treatment groups. Other studies have also reported that clinical improvements in core ADHD symptoms after NF and stimulant medication were on par with each other.8,49,50 Indeed, NF and MPH were correspondingly effective in treating core ADHD symptoms in two separate groups.7 However, no significant pre–post changes in any groups after adjusting for age and sex have been found. The lack of a significant difference after adjusting for confounding factors was probably due to the small sample size, and a lack of power in the study with additional variables. Further, it is important to emphasize that the changes reported here were evident only 1 week after treatment completion which can be a bias, thus, longer follow-up is needed.
NF effect in randomized studies demonstrated a lower effect size (ES) for hyperactivity, suggesting that hyperactivity is probably most sensitive to non-specific treatment factors (eg, time spent with a therapist), which is not in accordance with non-randomized studies.16,18,39,40,51–53 Moriyama et al concluded in a review that non-randomized controlled trials found medium-to-large ESs, while the evidence for an NF effect in randomized controlled studies was considered more resilient.12 Still, there is no available data on optimal treatment protocols or to guide clinicians on predictors of NF response.
The impact of non-specific factors, such as parental support and/or cognitive training during NF treatment has been evaluated.18,54 Those studies concluded that the patient-therapist interaction and the time spent with the therapist in a structured learning environment may contribute to a positive behavioral effect reported in NF treatment.54 NF sessions are thought to be a form of “cognitive training”, as the therapist and patient interact, meet regularly, and spend time together. Evaluation of cognitive training activities may have positive implications on NF treatment results, as they may support the learning process, augmenting results. Arns et al has suggested that hyperactivity could be more easily influenced by non-specific effects than inattention and impulsivity.18 Moreover, parental support, including simply transporting participants to and from the place of treatment, is also of importance when evaluating the NF effect.
Reported levels of school performance were higher in the NF group, which seems to be in accordance with results reported by Gaddes and Edgell.55 They reported improvements in academic performance in 80% of ADHD children who were treated with NF.55 Cognitive improvements in children with ADHD have been reported after NF treatment from Leins et al.57 Fernandez et al also found increased cognitive and academic/school performance in children with learning disabilities after the NF treatment and explained it as a consequence of changes in brain activity during the treatment.56 The effect of self-regulation on cognitive and academic performance has also been described by Strehl et al after NF treatment with SCP.48
It is interesting that NF alone, but not in combination with medication, influences school performance. The simple explanation may be personal and subjective perception of the effectiveness by making improvements in you alone and with own means and effort. Or, one can guess whether improved cognitive functions or the transferring of learning process which the child is exposed to during the treatment, may influence or improve school performance. NF is a learning process to regulate one’s own brain activity.48 Also, because it is a learning process, it has to be repeated in order to enhance the skills. School performance will improve once this has been achieved, and will most often be maintained.
However, influence of change in parental style throughout the NF treatment as well as parents’ expectations and satisfaction with the treatment, such as reported by Leins et al might have affected the behavior and school performance and therefore confounded outcome variables.57
The strengths of the present study are the randomized design, use of ICD-10 diagnostics with a multi-domain diagnostic assessment, and a follow-up rate that is reasonable for ADHD studies. Previous studies have seldom included a control randomization, and therefore evidence of NF effect has been interpreted with precaution.8,19,22,47,48,58–60 As the randomization process is often demanding in order to fulfill all requirements, it often extends the study period.
A control group with stimulant medication was assigned in accordance with earlier studies.7,8,16 We also tried to establish a placebo control group using “sham” treatment. During the pilot period, the NF sham placebo was found unfeasible due to difficulties for the therapist to adjust feedback parameters and placebo conditions. In addition, this placebo treatment was not ethically approved in the present thesis, which Logemann et al has also addressed.61
There is no well-established standard NF treatment protocol, which presented a challenge to this study. In Lofthouse et al’s62 review they found that two in three studies have used unipolar electrodes with a Cz placement equivalent to the present study.12,19 They found a variety of session numbers (20–40), and a variety of treatment durations (30–60 min), frequency (1–5 times/week), and course durations (2–20 weeks) for NF treatment in different studies.8,16,62 To our knowledge, there is no existing consensus on standard methods regarding recommended number and frequency of sessions and standard placement of NF screening.19,62 Summarizing previous literature, 30 sessions, three times per week for 11–13 weeks using Cz unipolar placement was regarded as a “recommended” protocol, and therefore used in the present study. Furthermore, it remains unclear whether the theta/beta protocol represents an “optimal” training protocol for ADHD patients or whether other NF protocols may prove more effective.
Conclusion
The present study indicated that children and adolescents with ADHD experienced effects of NF, reported after 1 week. NF seemed to be promising as an alternative treatment given that almost a third of all children diagnosed with ADHD have complications or side effects from medication. Furthermore, while many parents oppose stimulant-based treatments on principle, they are likely to approve of NF. Long-term studies are needed to confirm these results.
Acknowledgments
We would like to thank all of the children and adolescents who participated in this study. This work was supported by the Department for Research, Helse Fonna Hospital, Norway under Grant 40411. We are grateful to Dr Doris Gundersen and Edanz Editing group for support in proofreading of the manuscript. We are grateful for valuable support and contributions regarding NF to Dr Tanju Surmeli, BCIA-C, board member of EEG and Clinical Neuroscience Society. The project was further supported by the National Competence Center for AD/HD, Tourette syndrome and Narcolepsy, Norway. We also thank the staff at the Child and Adolescent Mental Health Clinic, Helse Fonna Hospital for their support completing this study and collecting the data.
Disclosure
The authors hereby declare that there are no financial or non-financial competing interests (political, personal, religious, ideological, academic, intellectual, commercial or any other) in relation to this manuscript.
References
Daley KC. Update on attention-deficit/hyperactivity disorder. Curr Opin Pediatr. 2004;16(2):217–226. | ||
Swanson JM, Sergeant JA, Taylor E, Sonuga-Barke EJ, Jensen PS, Cantwell DP. Attention-deficit hyperactivity disorder and hyperkinetic disorder. Lancet. 1998;351(9100):429–433. | ||
Barkley RA. Attention-deficit hyperactivity disorder: A handbood for diagnosis and treatment. 2nd ed. New York: Guilford Press; 1998. | ||
Thompson L, Thompson M. Neurofeedback Intervention for Adults with ADHD. Journal of Adult Development. 2005;12(2–3):123–130. | ||
Gruzelier J, Egner T. Critical validation studies of neurofeedback. Child Adolesc Psychiatr Clin N Am. 2005;14(1):83–104. | ||
Lubar JF. Neocortical dynamics: implications for understanding the role of neurofeedback and related techniques for the enhancement of attention. Appl Psychophysiol Biofeedback. 1997;22(2):111–126. | ||
Fuchs T, Birbaumer N, Lutzenberger W, Gruzelier JH, Kaiser J. Neurofeedback treatment for attention-deficit/hyperactivity disorder in children: a comparison with methylphenidate. Appl Psychophysiol Biofeedback. 2003;28(1):1–12. | ||
Rossiter T. The effectiveness of neurofeedback and stimulant drugs in treating AD/HD: part II. Replication. Appl Psychophysiol Biofeedback. 2004;29(4):233–243. | ||
Sherlin L, Arns M, Lubar J, Sokhadze E. A position paper on neurofeedback for the Treatment of ADHD. J Neurother. 2010;14(2):66–78. | ||
Arns M, Heinrich H, Strehl U. Evaluation of neurofeedback in ADHD: The long and winding road. Biol Psychol. 2014;95:108–115. | ||
Heinrich H, Gevensleben H, Strehl U. Annotation: neurofeedback – train your brain to train behaviour. J Child Psychol Psychiatry. 2007; 48(1):3–16. | ||
Moriyama TS, Polanczyk G, Caye A, Banaschewski T, Brandeis D, Rohde LA. Evidence-based information on the clinical use of neurofeedback for ADHD. Neurotherapeutics. 2012;9(3):588–598. | ||
Gevensleben H, Rothenberger A, Moll GH, Heinrich H. Neurofeedback in children with ADHD: validation and challenges. Expert Rev Neurother. 2012;12(4):447–460. | ||
Butnik SM. Neurofeedback in adolescents and adults with attention deficit hyperactivity disorder. J Clin Psychol. 2005;61(5):621–625. | ||
Friel PN. EEG Biofeedback in the Treatment of Attention Deficit/Hyperactivity. Altern Med Rev. 2007;12(2):146–151. | ||
Monastra VJ, Monastra DM, George S. The effects of stimulant therapy, EEG biofeedback, and parenting style on the primary symptoms of attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback. 2002;27(4):231–249. | ||
Monastra VJ, Lubar JF, Linden M. The development of a quantitative electroencephalographic scanning process for attention deficit-hyperactivity disorder: reliability and validity studies. Neuropsychology. 2001;15(1):136–144. | ||
Arns M, de Ridder S, Strehl U, Breteler M, Coenen A. Efficacy of neurofeedback treatment in ADHD: the effects on inattention, impulsivity and hyperactivity: a meta-analysis. Clin EEG Neurosci. 2009; 40(3):180–189. | ||
Lofthouse N, Arnold LE, Hersch S, Hurt E, DeBeus R. A review of neurofeedback treatment for pediatric ADHD. J Atten Disord. 2012; 16(5):351–372. | ||
Duric NS, Assmus J, Gundersen D, Elgen IB. Neurofeedback for the treatment of children and adolescents with ADHD: a randomized and controlled clinical trial using parental reports. BMC Psychiatry. 2012; 12:107. | ||
Meisel V, Servera M, Garcia-Banda G, Cardo E, Moreno I. Neurofeedback and standard pharmacological intervention in ADHD: A randomized controlled trial with six-month follow-up. Biol Psychol. 2013;94(1):12–21. | ||
Lansbergen MM, van Dongen-Boomsma M, Buitelaar JK, Slaats-Willemse D. ADHD and EEG-neurofeedback: a double-blind randomized placebo-controlled feasibility study. J Neural Transm. 2011;118(2):275–284. | ||
Sonuga-Barke EJ, Brandeis D, Cortese S, et al. Nonpharmacological interventions for ADHD: systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am J Psychiatry. 2013;170(3):275–289. | ||
Laub M, van Leeuwen SPG, Logemann-Molnár Z. The effect of Neurofeedback training on healthy individuals as measured by objective and self report measures of attention and impulsivity, when compared to a sham control condition [master’s thesis]. Universitet Utrecht; 2008. | ||
Young S, Gudjonsson G, Misch P, et al. Prevalence of ADHD symptoms among youth in a secure facility: the consistency and accuracy of self- and informant-report ratings. The Journal of Forensic Psychiatry and Psychology. 2010;21(2):238–246. | ||
Riley AW. Evidence that school-age children can self-report on their health. Ambul Pediatr. 2004;4(4 Suppl):371–376. | ||
Rizzo P, Steinhausen HC, Drechsler R. Self-perception of self-regulatory skills in children with attention-deficit/hyperactivity disorder aged 8–10 years. Atten Defic Hyperact Disord. 2010;2(4):171–183. | ||
Bell L, Kellison I, Garvan CW, Bussing R. Relationships between child-reported activity level and task orientation and parental attention-deficit/hyperactivity disorder symptom ratings. J Dev Behav Pediatr. 2010; 31(3):233–237. | ||
Jensen PS, Rubio-Stipec M, Canino G, et al. Parent and child contributions to diagnosis of mental disorder: are both informants always necessary? J Am Acad Child Adolesc Psychiatry. 1999;38(12):1569–1579. | ||
Hoza B, Gerdes AC, Hinshaw SP, et al. Self-perceptions of competence in children with ADHD and comparison children. J Consult Clin Psychol. 2004;72(3):382–391. | ||
Evangelista NM, Owens JS, Golden CM, Pelham WE Jr. The positive illusory bias: do inflated self-perceptions in children with ADHD generalize to perceptions of others? J Abnorm Child Psychol. 2008; 36(5):779–791. | ||
Owens JS, Goldfine ME, Evangelista NM, Hoza B, Kaiser NM. A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clin Child Fam Psychol Rev. 2007;10(4):335–351. | ||
Eiser C, Morse R. The measurement of quality of life in children: past and future perspectives. J Dev Behav Pediatr. 2001;22(4):248–256. | ||
Waters E, Stewart-Brown S, Fitzpatrick R. Agreement between adolescent self-report and parent reports of health and well-being: results of an epidemiological study. Child Care Health Dev. 2003;29(6):501–509. | ||
Duric NS, Elgen I. Characteristics of Norwegian children suffering from ADHD symptoms: ADHD and primary health care. Psychiatry Res. 2011;188(3):402–405. | ||
Duric NS, Elgen I. Norwegian Children and Adolescents with ADHD – A Retrospective Clinical Study: Subtypes and Comorbid Conditions and Aspects of Cognitive Performance and Social Skills. Adolescent Psychiatry. 2011;1(4):349–354. | ||
Wechsler D. Manual for the Wechsler Intelligence Scale for Children. New York: Psychological Corporation; 1949. | ||
World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. World Health Organization; 1992. | ||
Lubar JF, Lubar JO. Neurofeedback Assessment and Treatment for Attention Deficit/Hyperactivity Disorders. In: Introduction to Quantitative EEG and Neurofeedback. New York: Academic Press; 1999. | ||
Lubar JF, Swartwood MO, Swartwood JN, O’Donnell PH. Evaluation of the effectiveness of EEG neurofeedback training for ADHD in a clinical setting as measured by changes in T.O.V.A. scores, behavioral ratings, and WISC-R performance. Biofeedback Self-Regul. 1995; 20(1):83–99. | ||
Miller HA, Harrison DC. Biomedical Electrode Technology. New York: Academic Press; 1974. | ||
Piers EV, Harris DB, Herzberg DS. Piers-Harris Children’s Self-Concept Scale, Second Edition (Piers-Harris 2). Los Angeles: Western Psychological Services; 2001. | ||
Morris SB, DeShon RP. Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol Methods. 2002;7(1):105–125. | ||
Curko Kera EA, Marks DJ, Berwid OG, Santra A, Halperin JM. Self-report and objective measures of ADHD-related behaviors in parents of preschool children at risk for ADHD. CNS Spectr. 2004;9(9): 639–647. | ||
Houck G, Kendall J, Miller A, Morrell P, Wiebe G. Self-concept in children and adolescents with attention deficit hyperactivity disorder. J Pediatr Nurs. 2011;26(3):239–247. | ||
Nash JK. Treatment of attention deficit hyperactivity disorder with neurotherapy. Clin Electroencephalogr. 2000;31(1):30–37. | ||
Pop-Jordanova N, Markovska-Simoska S, Zorcec T. Neurofeedback treatment of children with attention deficit hyperactivity disorder. Prilozi. 2005;26(1):71–80. | ||
Strehl U, Leins U, Goth G, Klinger C, Hinterberger T, Birbaumer N. Self-regulation of slow cortical potentials: a new treatment for children with attention-deficit/hyperactivity disorder. Pediatrics. 2006;118(5): e1530–e1540. | ||
Rossiter TR, LaVaque TJ. A Comparison of EEG biofeedback and psychostimulants in treating attention deficit/hyperactivity disorders. Journal of Neurotherapy. 1995;1:48–59. | ||
Linden M, Habib T, Radojevic V. A controlled study of the effects of EEG biofeedback on cognition and behavior of children with attention deficit disorder and learning disabilities. Biofeedback Self Regul. 1996; 21(1):35–49. | ||
Bakhshayesh AR. Die Wirksamkeit von Neurofeedback im Vergleich zum EMG Biofeedbackbei der Behandlung von ADHS-Kindern. [The effectiveness of neurofeedback in comparison to EMG Biofeedback in the treatment of ADHD children]. [PhD thesis]. Universität Potsdam, Germany; 2007. | ||
Gevensleben H, Holl B, Albrecht B, et al. Is neurofeedback an efficacious treatment for ADHD? A randomised controlled clinical trial. J Child Psychol Psychiatry. 2009;50(7):780–789. | ||
Thompson L, Thompson M. Neurofeedback combined with training in metacognitive strategies: effectiveness in students with ADD. Appl Psychophysiol Biofeedback. 1998;23(4):243–263. | ||
Bakhshayesh AR, Hansch S, Wyschkon A, Rezai MJ, Esser G. Neurofeedback in ADHD: a single-blind randomized controlled trial. Eur Child Adolesc Psychiatry. 2011;20(9):481–491. | ||
Gaddes WH, Edgell D. Learning Difficulties and Brain Functions. New York: Springer-Verlag; 1994. | ||
Fernández T, Herrera W, Harmony T, et al. EEG and behavioral changes following neurofeedback treatment in learning disabled children. Clin Electroencephalogr. 2003;34(3):145–152. | ||
Leins U, Goth G, Hinterberger T, Klinger C, Rumpf N, Strehl U. Neurofeedback for children with ADHD: a comparison of SCP and Theta/Beta protocols. Appl Psychophysiol Biofeedback. 2007;32(2):73–88. | ||
Monastra VJ, Lynn S, Linden M, Lubar JF, Gruzelier J, LaVaque TJ. Electroencephalographic biofeedback in the treatment of attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback. 2005; 30(2):95–114. | ||
Gevensleben H, Holl B, Albrecht B, et al. Neurofeedback training in children with ADHD: 6-month follow-up of a randomised controlled trial. Eur Child Adolesc Psychiatry. 2010;19(9):715–724. | ||
Stjernholm O. [Neurofeedback as ADDH therapy]. Ugeskr Laeger. 2010;172(33):2221–2225. Danish. | ||
Logemann HN, Lansbergen MM, Van Os TW, Bocker KB, Kenemans JL. The effectiveness of EEG-feedback on attention, impulsivity and EEG: a sham feedback controlled study. Neurosci Lett. 2010;479(1):49–53. | ||
Lofthouse N, Arnold LE, Hurt E. Current status of neurofeedback for attention-deficit/hyperactivity disorder. Curr Psychiatry Rep. 2012; 14(5):536–542. |
Supplementary material
Self-report questionnaire (SRQ)
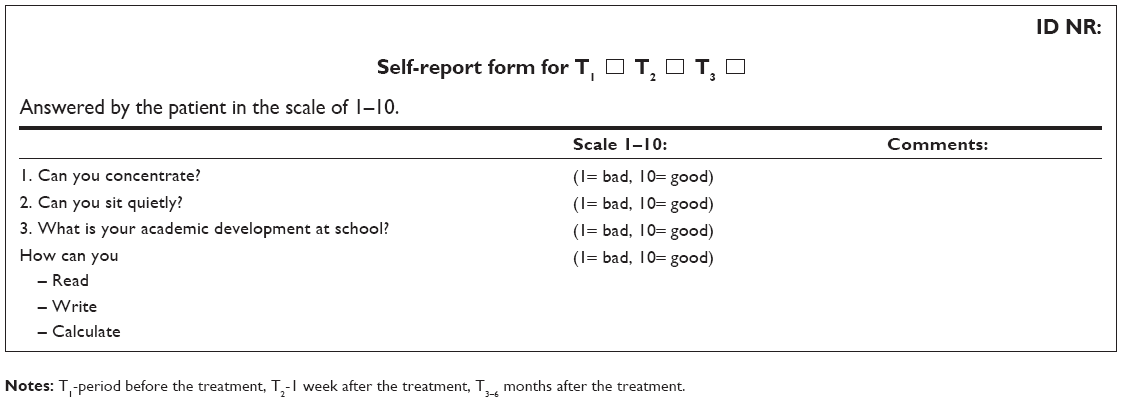 | Notes: T1-period before the treatment, T2-1 week after the treatment, T3–6 months after the treatment. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.