Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Self-medication practices among Vietnamese residents in highland provinces
Authors Ha TV, Nguyen AMT ![]() , Nguyen HST
, Nguyen HST
Received 7 April 2019
Accepted for publication 16 May 2019
Published 2 July 2019 Volume 2019:12 Pages 493—502
DOI https://doi.org/10.2147/JMDH.S211420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thuy Van Ha,1 An Mai Thi Nguyen,2 Ha Song Thi Nguyen3
1Department of Health Insurance, Ministry of Health of Vietnam, Hanoi 100000, Vietnam; 2Department of Planning and Financing, Ministry of Health of Vietnam, Hanoi 100000, Vietnam; 3Department of Pharmacoeconomics and Management, Hanoi University of Pharmacy, Hanoi 100000, Vietnam
Background: Monitoring self-medication practice, which refers to individuals using medicine without instructions of physicians, is critical to control its harmful effects. However, in Vietnam, evidence about self-medication among individuals in highland areas is constrained. This study examined self-medication practice among residents living in highland areas in Vietnam and determined associated factors.
Materials and methods: A cross-sectional study was performed in five highland provinces with 1000 individuals. Information about individual and household’s socioeconomic status and self-medication practice in the last 12 months was surveyed. Multivariate logistic and Poisson regressions were used to identify associated factors with self-medication.
Results: 83.3% reported self-medication in the last 12 months, with the mean times of self-medication being 4.5 times (SD=4.1). Female (OR=0.62, p<0.01), ethnic minorities, higher number of members having health insurance in family (OR=0.82, p<0.01) and higher annual household income (OR=0.78, p<0.05) were associated with the lower likelihood of “Only buy medicines at pharmacy stores when having illness in the last 12 month”. Moreover, people who were females (OR=0.59, p<0.05), white-collar worker (OR=0.25, p<0.01) and had higher number of children in the family (OR=0.68, p<0.05) were less likely to practice self-medication. People who were ethnic minorities, white-collar worker (Coef.=−0.32, p<0.01) and higher number of members having health insurance in family had lower times of self-medication in the last 12 months compared to other groups. Meanwhile, individuals having higher number of members in the family (Coef.=0.07, p<0.01) and higher annual household income (Coef.=0.08, p<0.01) had highertimes of self-medication in the last 12 months.
Conclusion: Residents in highland areas in Vietnam had a considerably high 12-month prevalence of self-medication. Medical products quality management and self-medication guideline are potential to maximize the effects of self-medication. Moreover, promoting the use of health insurance should also be concerned as a solution to address this issue.
Keywords: self-medication, factors, residents, highland, Vietnam
Introduction
Self-medication refers that people choose to treat their illnesses or symptoms by using any medical products without a prescription or following unprofessional recommendations.1,2 Responsible self-medication is the use of medicines which are officially approved and allowed to use without prescriptions.3 Otherwise, nonresponsible self-medication is when people use drugs which are not allowed to use without a prescription.4 Self-medication is beneficial to individuals because this approach is affordable and convenient, particularly when people have mild diseases or symptoms.5 It has a crucial role in the health care system in reducing the needs to see the physicians and alleviating medical resources spending especially in settings with resources constrained.5 However, self-medication practice possibly raises some health-related complications, namely, incorrect drug selection, drug resistance, uncontrolled adverse effects or drug reactions or interactions,6,7 misdiagnosis and delay in medical care.5,8,9
Self-medication has been well-documented as a pervasive phenomenon in both developed and developing countries. The prevalence of self-medication varies from 12.7% to 18% in Spain,10,11 32–45.4% in China,12,13 53% in Mexico14 and 75% in the United Kingdom and Chile.15,16 Previous experiences, advice from friends/relatives and the high cost of medical services are primary reasons for self-medication.12,17 Moreover, literature underline the roles of socioeconomic (eg, gender, education, occupation and location), clinical (eg, severity of diseases and symptoms, and history of treatment) and health system (eg, lack of service, high cost or ease in purchasing medicines) factors in facilitating self-medication behavior.2,16–21
Self-medication has been recognized as a common issue in Vietnam. The self-medication rate in the general population has ranged from 40% to 60% in rural areas22 to 76% in urban areas.23 However, none of the evidence was found among individuals in highland areas of Vietnam. People in this setting are believed to have different sociocultural-economic characteristics compared to those living in rural and urban areas. Monitoring the self-medication patterns and their determinants among people in highland areas is therefore particularly important. This study aims to describe the prevalence of self-medication among residents living in highland areas of Vietnam as well as determine factors that might be related to this behavior.
Materials and methods
Cross-sectional data were collected in five highland provinces of Vietnam comprising Kon Tum, Gia Lai, Dak Lak, Dak Nong and Lam Dong. This study was conducted from July to November 2018. In this study, we applied a multistage sampling technique to enroll participants. Initially, in each province, we developed a list with 62 districts and 721 communes in five provinces as a sampling frame. Next, we randomly chose two districts per province and two communes per district by using a computer software. A total of 20 communes in 10 districts of 5 provinces were selected. Finally, in each commune, 5 villages per commune and 10 households per village were randomly selected. We applied a door-to-door recruitment technique to recruit residents into the study. The recruitment process finished when we had a sufficient sample size.
In this study, we used the formula for estimating a population proportion with specificied absolute precision to compute the necessary sample size. With P=0.5 (50% as expected 12-month prevalence of self-medication), an absolute precision =0.07 and a confident level =95%, the sample size was 196 households per provinces. Five percent of the sample size was also added to compensate the individuals who refused to participate or had incomplete data. There were 1029 households listed in the sampling frame. In each household, we randomly selected and invited one person who had following characteristics: 1) aged from 18 years and above; 2) did not have a psychological and physical impairment that influences their ability to answer interview and 3) accepted to participate and gave written informed consents. Finally, after excluding people declining to participate due to several reasons such as “busy work” or “privacy”, information of 1000 individuals was used for data analysis (response rate 97.2%).
Data collection and measurements
Each participant had face-to-face interviews for 15–20 mins by sung a structured questionnaire. This questionnaire was built and piloted with 10 residents in Dak Lak province. We did not include these data into the final dataset. Feedbacks from the pilot study were used to revise with respect to content, language and logical perspectives. We also revised the text of each item to ensure cultural appropriateness. The questionnaire was finalized and approved by the research team and local authorities. To ensure the quality of the data collection process, we conducted a two-day intensive training session with instructors including principal investigators and team members who had experiences in pharmacy and community health. We recruited local health workers to become interviewers. They were provided the study aims, questionnaire’s contents and interview skills in order to collect high-quality data.
The questionnaire had three parts: 1) socio-demographic status of respondents (age, gender, ethnic, education, marital status and occupation); 2) socio-demographic status of households (number of family members, number of children in family, number of people having health insurance in family, annual household income and household economic based on the government’s classification) and 3) self-medication practice. For ethnicity, because “Kinh” is the predominant ethnic in Vietnam, we categorized those belonging to other ethnic groups into “ethnic minorities”.
Self-medication
n this study, self-medication was defined as a person-utilized medicines without the instructions of physicians.24 This behavior includes the use of over-the-counter medications and prescription-only medications,25 reutilization of prior prescriptions, consuming medicines based on recommendations from relatives or other unqualified people (eg, friends, drug sellers, etc.) or using leftover drugs at home.26 This term also consists of the use of any herbal products, vitamins or supplements that are not prescribed by the physicians.27,28
First, we explained clearly about the definition of self-medication and gave the respondents examples to ensure that they could recall their self-medication practice accurately. Respondents were asked to recall places where they bought medicines if having any illnesses in the last 12 months. If they only bought medicines at the pharmacy store when having any illnesses, we asked them to report the reasons for such behavior. We also asked them to recall the frequency of self-medication (Usually (>50% number of times sick)/sometimes (>0–50% number of times sick)/Never (0% number of times sick)) and times of self-medication in the last 12 months. Those reporting “Usually” and “Sometimes” were categorized “Self-medication” while people reporting “Never” were classified “No self-medication”. The times of self-medication were defined as “the number of exposures to self-medication”. The details of the questionnaire are in the Supplementaary materials.
Statistical analysis
A p-value less than 0.05 was treated as statistical significance. Data were analyzed using Stata version 14.0. Skewness–Kurtosis test was used to test the normality of the continuous variables. Descriptive analysis including mean, standard deviation, frequency, and percentage was performed to describe the variables. Chi-squared test was used to examine the variability of self-medication among different socioeconomic groups. Mann–Whitney test (for non-normal distribution data) was applied to test the difference in age, number of members in the family, number of children in the family, number of members having health insurance in family and annual household income (million VND) between people with and without self-medication.
Multivariate logistic regression was used to identify the factors associated with two binary outcomes including “Only buy medicines at pharmacy stores when having any illnesses” (Yes/No) and “Self-medication” (Yes/No), and one continuous outcome, namely, “Times of self-medication in the last 12 months”. The first variable refers to the behavior that they went to the pharmacy store and purchase the medicines by themselves without the instruction of physicians or other qualified health professionals, which can be treated as an indicator for self-treatment. In addition, multivariate Poisson regression was employed to determine factors associated with “Times of self-medication in the last 12 months” because this variable was a count variable with Poisson distribution. Independent variables included prior socioeconomic characteristics of respondents and households. Data on the annual household income was transformed to log form due to non-normal distribution.
Ethical consideration
The study protocol was approved by the Institutional Review Board of the Vietnam Ministry of Health (Code: 114/QD-YTTN2). Participants had the right to stop the interview or withdraw to the study at any time without any barriers. They were obtained written informed consents if they agreed to participate in the study.
Results
Of 1000 participants, the mean age was 36.7 (SD=12.7) years. Most of the participants were female (57.9%), working in agriculture/fishery/forestry sector (76.4%) and having lower high school education (71.7%). “Kinh” was the dominant ethnic with 45.0%. The majority of households had one child (56.0%) and were classified as nonpoor household according to the government’s standard. The mean annual household income was 79.0 (SD=102.1) million VND (Table 1).
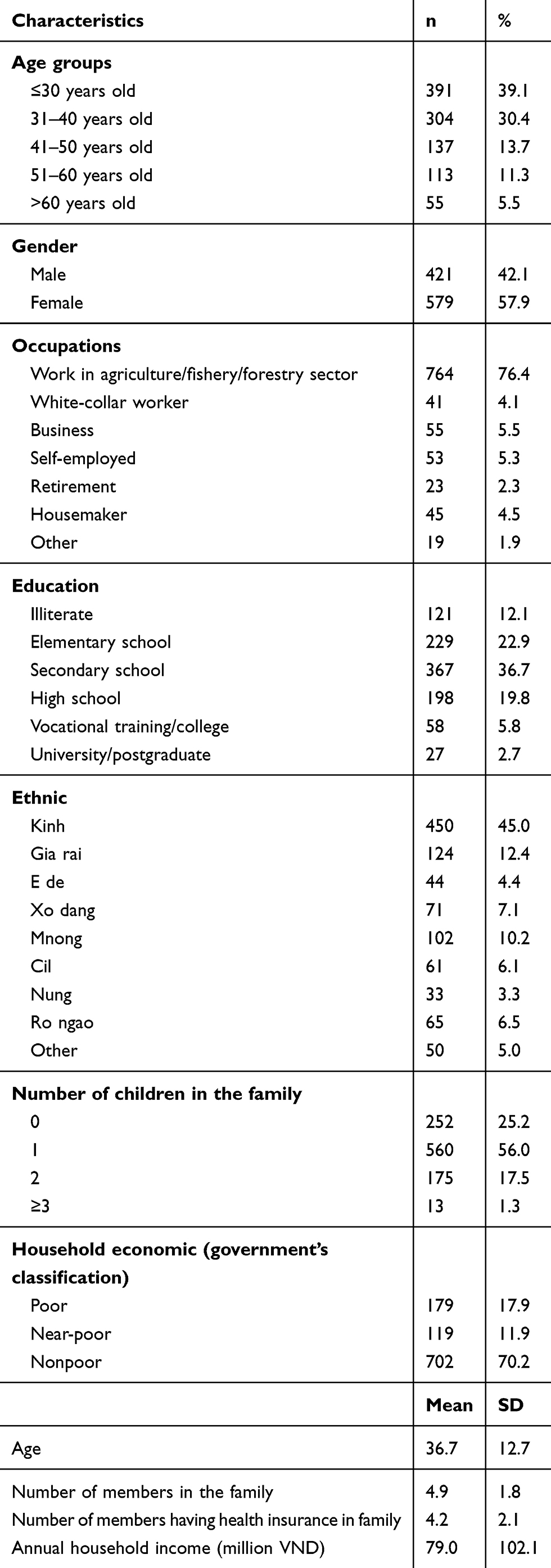 |
Table 1 Demographic characteristics of respondents (n=1000) |
Table 2 depicts that when having any illnesses, approximately one-fifth of the sample (20.8%) only bought medicines at pharmacy stores if having any illnesses, with the most common reasons consisting of “Near home” (57.7%), “Believe in the expertise of drug sellers” (27.9%) and “Availability of many types of drugs” (15.9%). In the last 12 months, most of the participants reported they sometimes and always bought medicines without prescription (64.7%and 18.7%, respectively) and the mean times of self-medication was 4.5 (SD=4.1). Totally, 83.3% reported self-medication in the last 12 months.
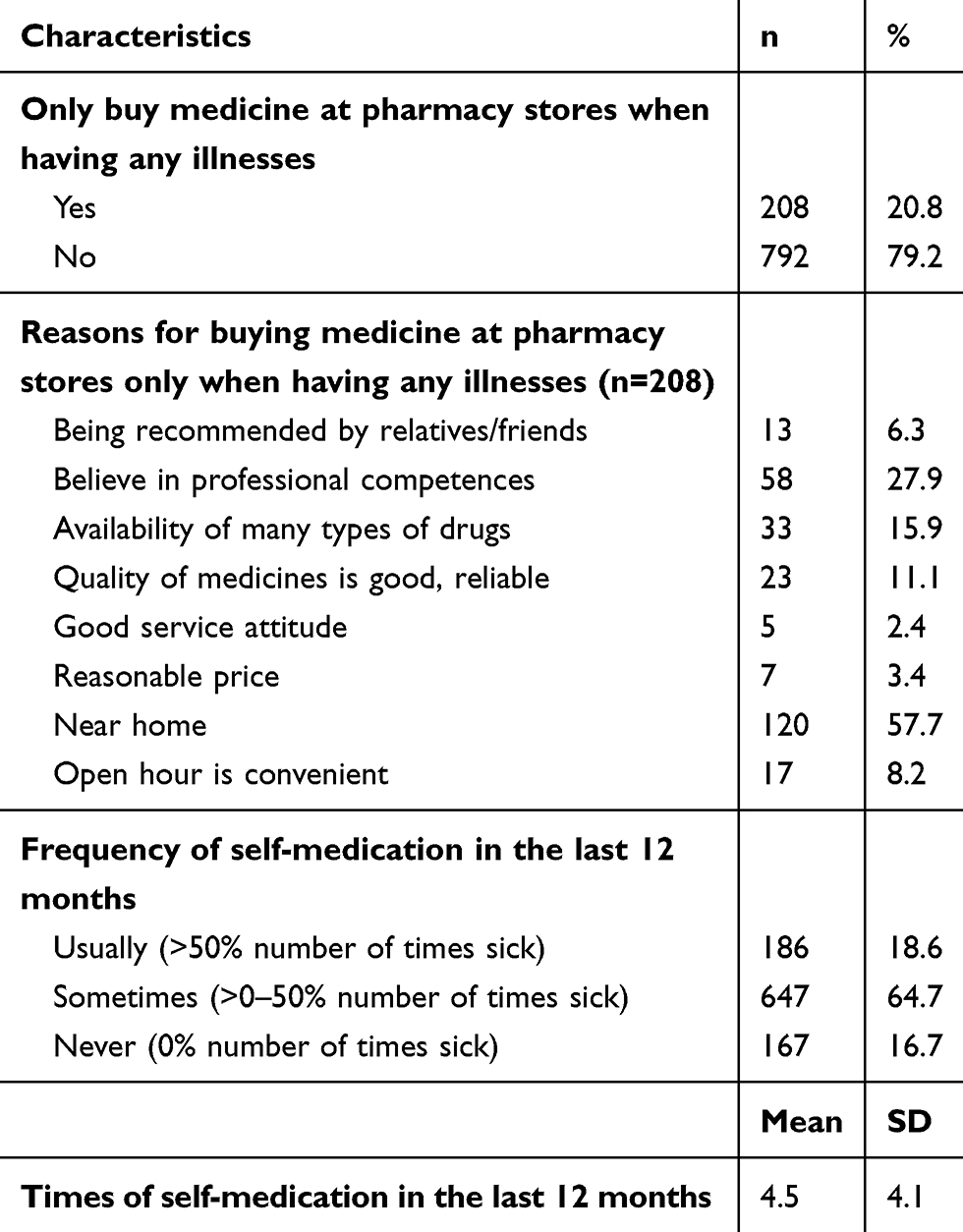 |
Table 2 Self-medication practices (n=1000) |
Table 3 shows that male respondents had a significantly higher rate of self-medication (87.4%) than that in females (80.3%) (p<0.01). Regarding occupations, white-collar workers reported the lowest rate of self-medication (63.4%) compared to other groups (p<0.01). Regarding ethnicity, “E de” people had the lowest prevalence of self-medication (70.5%), while “Nung”, “Cil” and “Kinh” residents had the highest rates at 90.9%, 90.2% and 86.4%, respectively. The differences among ethnic groups were significant (p<0.01). People in self-medication group had significantly higher annual household income compared to those in not self-medication group (p<0.01). No significant difference was found in self-medication regarding education, household economic classification, age, number of members in the family, number of children in the family and number of members having health insurance in the family (p>0.05).
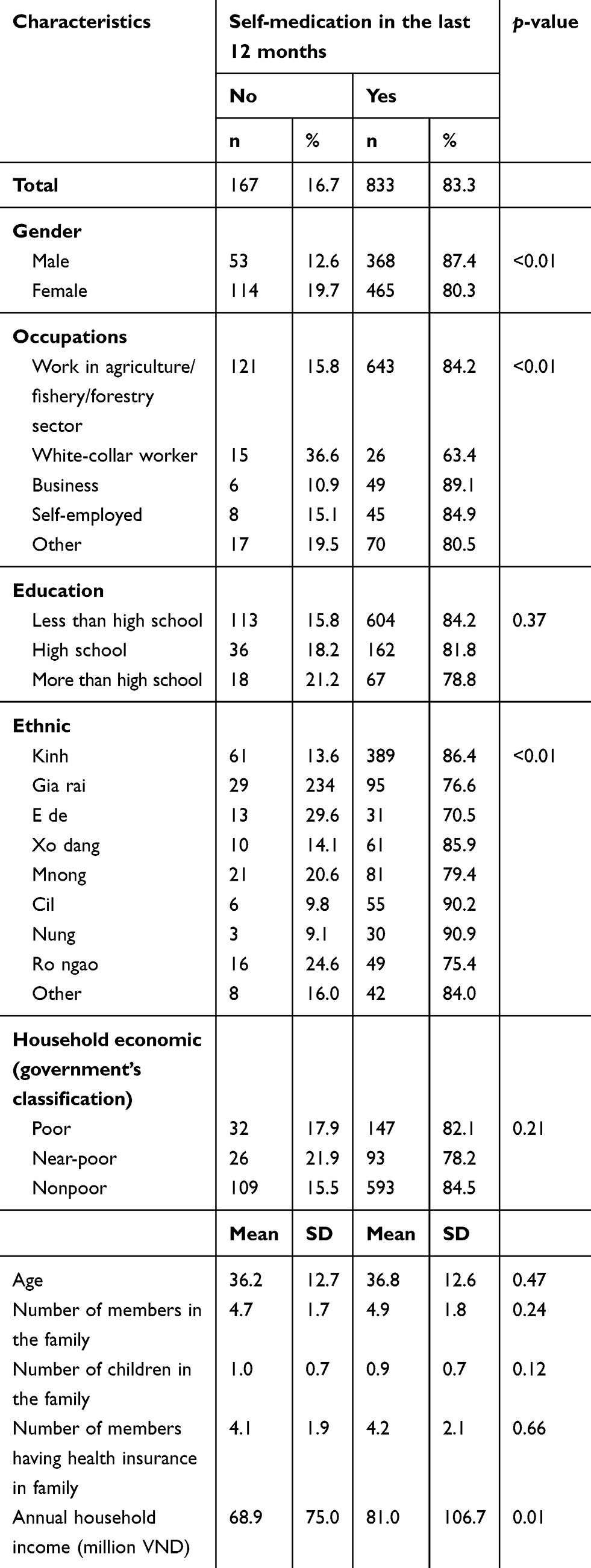 |
Table 3 Self-medication according to different characteristics (n=1000) |
Multivariate regressions in Table 4 indicate that female (OR=0.62, p<0.01), ethnic minorities, high number of members having health insurance in family (OR=0.82, p<0.01) and high annual household income (OR=0.78, p<0.05) were negatively associated with “Only buy medicines at pharmacy stores when having illness in the last 12 month”. Moreover, females (OR=0.59, p<0.05), white-collar worker (OR=0.25, p<0.01), and high number of children in the family (OR=0.68, p<0.05) were negatively related to self-medication.
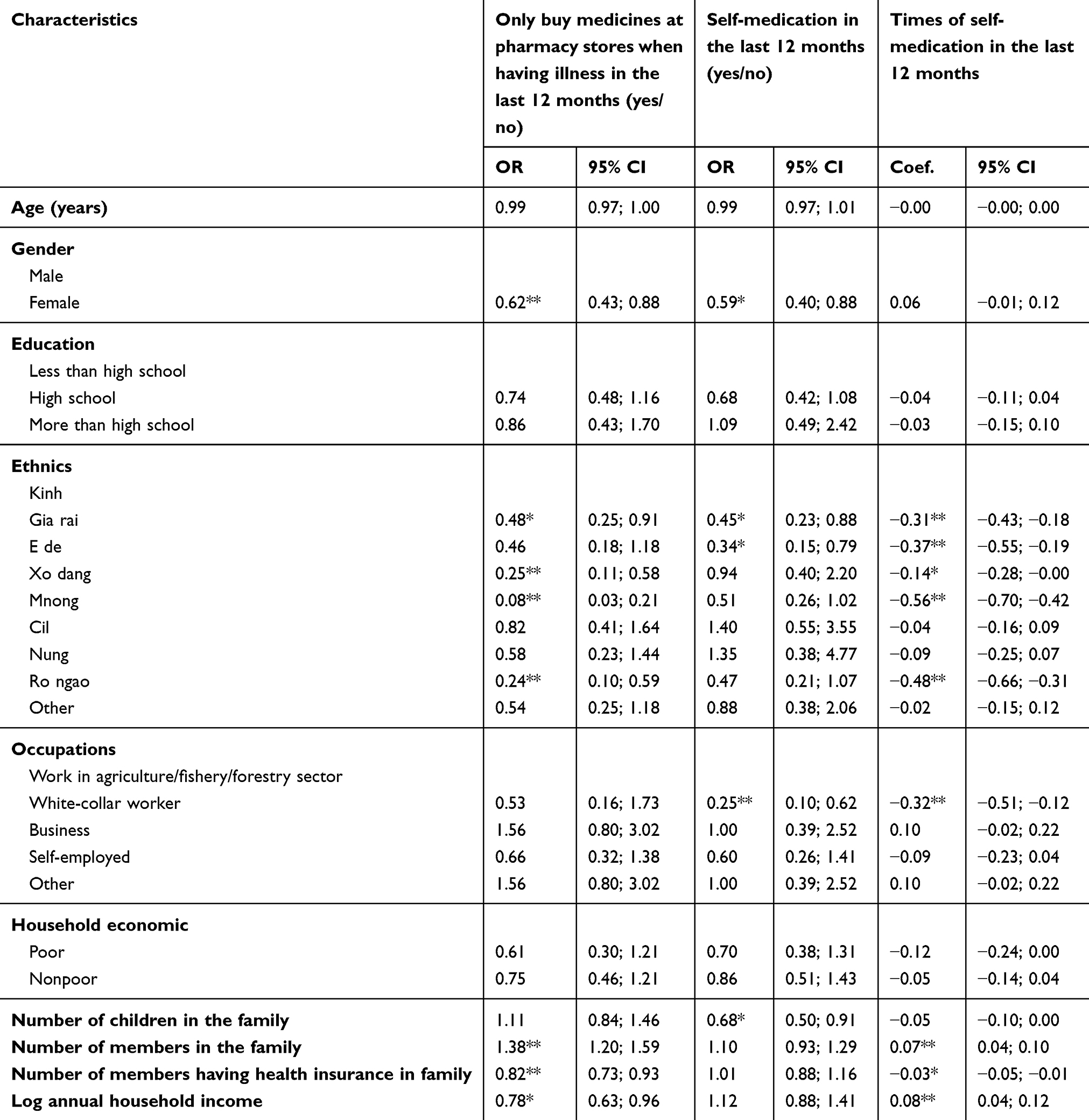 |
Table 4 Associated factors with self-treatment practices |
People who were ethnic minorities, white-collar worker (Coef.=−0.32, p<0.01) and high number of members having health insurance in the family were negatively correlated with times of self-medication in the last 12 months. Higher number of members in the family were positively correlated to times of self-medication in the last 12 months. Meanwhile, high number of members in the family (Coef.=0.07, p<0.01) and high annual household income (Coef.=0.08, p<0.01) were positively related to times of self-medication in the last 12 months.
Discussion
This study provides that self-medication was a common practice among highland residents in Vietnam. The 12-month prevalence of self-medication in our study was 83.3%, which was much higher than this rate in other settings in the world such as Spain (12.7–18%),10,11 China (32–45.4%),12,13 Mexico (53%),14 the United Kingdom and Chile (75%).15,16 This result was also higher than a prior study in rural Vietnam (40–60%)22 and approximately equaled to that in urban areas (76.0%).23 The differences might be explained by the variations of recall time period, socio-cultural-economic as well as health care accessibility among different settings. In Vietnam, previous studies indicated poor living conditions, health status and health care access among people in highland and mountainous areas compared to residents in urban and rural settings.29–31 Therefore, when having any illnesses, they chose to visit private pharmacy stores near their home and get advice from pharmacists, whom participants believed in their competences. In literature, pharmacists are argued to be a primary source to facilitate self-medication decision-making.32 In our study, these two reasons were also the most common reasons for purchasing medicine in the pharmacy store only rather than going to the health facilities.
In this study, our findings indicate a significant role of socioeconomic as well as family factors that were associated with the likelihood of self-medication. Males are more involved in this practice than females, which was in line with previous findings in India and Nepal.33–35 However, it was different from a study in Vietnamese urban area, which revealed that no association between self-medication and gender.23 This difference might be due to the role of each gender in different settings. Selvaraj et al argued that males were more likely to ignore to go to clinics because of mild symptoms and loss of income.33 In Vietnamese highland areas, males were responsible for earning income for the family; hence, hospitalization could reduce their working time and then decrease the wages. Meanwhile, in an urban setting, this role was shared between males and females, facilitating similar patterns of self-medication between two genders.
We also observed that residents working in agriculture/fishery/forestry sectors were also more likely to practice self-medication compared to those with other jobs. Working in these sectors required spending an enormous amount of time daily; thus, going to the hospital would diminish this time, which led to the reduction of income. Nonetheless, our study did not find any association between education and self-medication in the last 12 months. Globally, the association between education and self-medication has been in debate. Several studies found that self-medication was more likely to occur in illiterate people or those are having lower education level,21,36 while other studies in Europe and Vietnam indicated that higher education could project a higher chance of self-medication.23,37 This finding indicated that self-medication was common in highland settings in Vietnam regardless of the level of education; thus, interventions to improve the self-medication practice should not differentiate targeted populations based on the education.
Surprisingly, we found that people in the ethnic minorities were less likely to self-medication as well as had lower times of self-medication compared to Kinh people (ie the ethnic majority). In literature, limited health care access was a facilitator of self-medication.2,16–21 Ngo et al found a lower level of health care utilization among ethnic minorities than that of the ethnic majority in mountainous settings in Vietnam.38 However, Tran et al in their study in another mountainous province in Vietnam revealed that ethnic minorities were more easy to access commune health centers than Kinh people.39 In our study, the residents in ethnic minority groups mentioned that there was a lack of pharmacy stores near their homes; therefore, they went to the commune health centers for health check-up and buying medicine also. Meanwhile, Kinh people could access pharmacy stores easily, which encouraged them to self-medication.
Health insurance in this study was also an important associated factor of self-medication. Specifically, a higher number of members in the family having health insurance was correlated to a lower likelihood of self-medication. This result was in line with previous findings in China and Vietnam.23,40 Indeed, health insurance system in Vietnam has covered medicines for most of the common diseases in the community. With health insurance, people could visit hospitals for treatment with affordable prices compared to purchase drugs alone in the pharmacy store without professional medical advice and financial support of health insurance.
Several implications can be drawn from the findings of this study. First, since the self-medication rate is significantly high among highland residents, strategies to manage drug and medical products quality should be ensured to reduce the potential adverse effects of self-medication. Moreover, a guideline for self-medication should be developed for the general population to optimize the positive effects of self-medication. Second, educational interventions should be performed to promote the use of health insurance in people living in highland areas, which could alleviate the self-medication behavior. Third, further interventions to control self-medication in this setting should concern socio-cultural-economic sensitives to assure the effectiveness of these interventions.
Our study has a strength in a large sample size (1000 residents) in a wide setting (five provinces). Nonetheless, this study has several methodological issues that should be acknowledged. First, the causal relationships between self-medication practice and its associated factors could not be established due to the nature of study design. We did not measure the characteristics of people declining to participate in the study, whose self-medication behaviors might be critical. Second, the self-reported approach might result in information bias, recall bias and social desirability bias. We have trained the data collection team carefully, develop the data collect guideline as well as explained clearly the purpose of the study to the respondents in order to reduce the bias. Third, several critical information was not included in the study, for example, participants’ behaviors, impacts of family and social relationships or health service quality, number and names of medical products used for self-medication. Thus, our findings should be used in caution. Further studies should be warranted to fill the knowledge gap in the self-medication among highland residents.
Conclusion
This study highlights a considerably high 12-month prevalence of self-medication among people residing in highland areas in Vietnam. Gender, ethnicity, employment, household income and number of people/children in the family are important factors that might influence the self-medication practice. Medical products quality management and assurance strategies and self-medication guideline are potential to maximize the effects of self-medication. Moreover, promoting the use of health insurance in residents should also be concerned as a solution to address this issue.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Hernandez-Juyol M, Job-Quesada JR. Dentistry and self-medication: a current challenge. Med Oral. 2002;7(5):344–347.
2. Shaghaghi A, Asadi M, Allahverdipour H. Predictors of self-medication behavior: a systematic review. Iran J Public Health. 2014;43(2):136–146.
3. Association WM. WMA Statement on Self-Medication; Re-Afffirmed by the 191st WMA Council Session. Prague, Czech Republic: World Medical Association; 2012.
4. Galato D, Galafassi L, Alano GM, Trauthman SC. Responsible self-medication: review of the process of pharmaceutical attendance. Braz J Pharm Sci. 2009;45:625–633. doi:10.1590/S1984-82502009000400004
5. Bennadi D. Self-medication: A current challenge. J Basic Clin Pharm. 2013;5(1):19–23. doi:10.4103/0976-0105.128253
6. Panda A, Pradhan S, Mohapatra G, Mohapatra J. Drug-related problems associated with self-medication and medication guided by prescription: A pharmacy-based survey. Indian J Pharmacol. 2016;48(5):515–521. doi:10.4103/0253-7613.190728
7. Ruiz ME. Risks of self-medication practices. Curr Drug Saf. 2010;5(4):315–323.
8. Hughes CM, McElnay JC, Fleming GF. Benefits and risks of self medication. Drug Safety. 2001;24(14):1027–1037. doi:10.2165/00002018-200124140-00002
9. Patil AD. Self medication: a potentially avoidable cause of antibiotic misuse and resistance. Int J Basic Clin Pharmacol. 2017;2(4):2.
10. Figueiras A, Caamano F, Gestal-Otero JJ. Sociodemographic factors related to self-medication in Spain. Eur J Epidemiol. 2000;16(1):19–26.
11. Carrasco-Garrido P, Jimenez-Garcia R, Barrera VH, Gil de Miguel A. Predictive factors of self-medicated drug use among the Spanish adult population. Pharmacoepidemiol Drug Saf. 2008;17(2):193–199. doi:10.1002/pds.1455
12. Lei X, Jiang H, Liu C, Ferrier A, Mugavin J. Self-medication practice and associated factors among residents in Wuhan, China. Int J Environ Res Public Health. 2018;15(1). doi:10.3390/ijerph15061188
13. Lam CL, Catarivas MG, Munro C, Lauder IJ. Self-medication among Hong Kong Chinese. Soc Sci Med. 1994;39(12):1641–1647. doi:10.1016/0277-9536(94)90078-7
14. Balbuena FR, Aranda AB, Figueras A. Self-medication in older urban mexicans: an observational, descriptive, cross-sectional study. Drugs Aging. 2009;26(1):51–60. doi:10.2165/0002512-200926010-00004
15. James DH, French DP. The development of the Self-Medicating Scale (SMS): a scale to measure people’s beliefs about self-medication. Pharm World Sci. 2008;30(6):794–800. doi:10.1007/s11096-008-9227-2
16. Fuentes Albarran K, Villa Zapata L. Analysis and quantification of self-medication patterns of customers in community pharmacies in southern Chile. Pharm World Sci. 2008;30(6):863–868. doi:10.1007/s11096-008-9241-4
17. Jalilian F, Hazavehei SM, Vahidinia AA, Jalilian M, Moghimbeigi A. Prevalence and related factors for choosing self-medication among pharmacies visitors based on health belief model in Hamadan Province, west of Iran. J Res Health Sci. 2013;13(1):81–85.
18. Loyola Filho AI, Lima-Costa MF, Uchoa E. Bambui project: a qualitative approach to self-medication. Cad Saude Publica. 2004;20(6):1661–1669. doi:10.1590/S0102-311X2004000600025
19. Omolase CO, Adeleke OE, Afolabi AO, Afolabi OT. Self medication amongst general outpatients in a nigerian community hospital. Ann Ib Postgrad Med. 2007;5(2):64–67.
20. Yousef AM, Al-Bakri AG, Bustanji Y, Wazaify M. Self-medication patterns in Amman, Jordan. Pharm World Sci. 2008;30(1):24–30. doi:10.1007/s11096-007-9135-x
21. Sedighi B, Ghaderi-Sohi S, Emami S. Evaluation of self-medication prevalence, diagnosis and prescription in migraine in Kerman, Iran. Saudi Med J. 2006;27(3):377–380.
22. Okumura J, Wakai S, Umenai T. Drug utilisation and self-medication in rural communities in Vietnam. Soc Sci Med. 2002;54(12):1875–1886. doi:10.1016/S0277-9536(01)00155-1
23. Hoai NT, Dang T. The determinants of self-medication: evidence from urban Vietnam. Soc Work Health Care. 2017;56(4):260–282. doi:10.1080/00981389.2016.1265632
24. Montastruc JL, Bagheri H, Geraud T, Lapeyre-Mestre M. [Pharmacovigilance of self-medication]. Therapie. 1997;52(2):105–110.
25. Pereira FS, Bucaretchi F, Stephan C, Cordeiro R. Self-medication in children and adolescents. J Pediatr (Rio J). 2007;83(5):453–458. doi:10.2223/JPED.1703
26. Zafar SN, Syed R, Waqar S, et al. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58(4):214–217.
27. Haenen GR, Bast A. The use of vitamin supplements in self-medication. Therapie. 2002;57(2):119–122.
28. Eichhorn T, Greten HJ, Efferth T. Self-medication with nutritional supplements and herbal over-thecounter products. Nat Prod Bioprospect. 2011;1(2):62–70. doi:10.1007/s13659-011-0029-1
29. Hoi le V, Thang P, Lindholm L. Elderly care in daily living in rural Vietnam: need and its socioeconomic determinants. BMC Geriatr. 2011;11:81. doi:10.1186/1471-2318-11-81
30. Gt L, Wd P. The Elderly Population in Vietnam during Economic Transformation: An Overview. Hanoi: Vietnam Development Forum; 2007.
31. Knodel J, Anh TS. Viet Nam’s older population: the view from the census. Asia Pac Popul J. 2002;17(3):5–22. doi:10.18356/2702b8d0-en
32. Rutter P. Role of community pharmacists in patients’ self-care and self-medication. Integr Pharm Res Pract. 2015;4:57–65. doi:10.2147/IPRP.S70403
33. Selvaraj K, Kumar SG, Ramalingam A. Prevalence of self-medication practices and its associated factors in Urban Puducherry, India. Perspect Clin Res. 2014;5(1):32–36. doi:10.4103/2229-3485.124569
34. Deshpande SG, Tiwari R. Self medication–a growing concern. Indian J Med Sci. 1997;51(3):93–96.
35. Shankar PR, Partha P, Shenoy N. Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: a questionnaire-based study. BMC Fam Pract. 2002;3:17. doi:10.1186/1471-2296-3-17
36. Bilal M, Haseeb A, Khan MH, et al. Self-medication with antibiotics among people dwelling in rural areas of Sindh. J Clin Diagn Res. 2016;10(5):Oc08–13. doi:10.7860/JCDR/2016/18294.7730
37. Grigoryan L, Haaijer-Ruskamp FM, Burgerhof JG, et al. Self-medication with antimicrobial drugs in Europe. Emerg Infect Dis. 2006;12(3):452–459. doi:10.3201/eid1205.050992
38. Toan NV, Trong LN, Hojer B, Persson LA. Public health services use in a mountainous area, Vietnam: implications for health for policy. Scand J Public Health. 2002;30(2):86–93. doi:10.1080/14034940210133780
39. Tran BX, Nguyen LH, Nong VM, Nguyen CT. Health status and health service utilization in remote and mountainous areas in Vietnam. Health Qual Life Outcomes. 2016;14(1):85. doi:10.1186/s12955-016-0426-6
40. Yuefeng L, Keqin R, Xiaowei R. Use of and factors associated with self-treatment in China. BMC Public Health. 2012;12:995. doi:10.1186/1471-2458-12-995
Supplementary materials
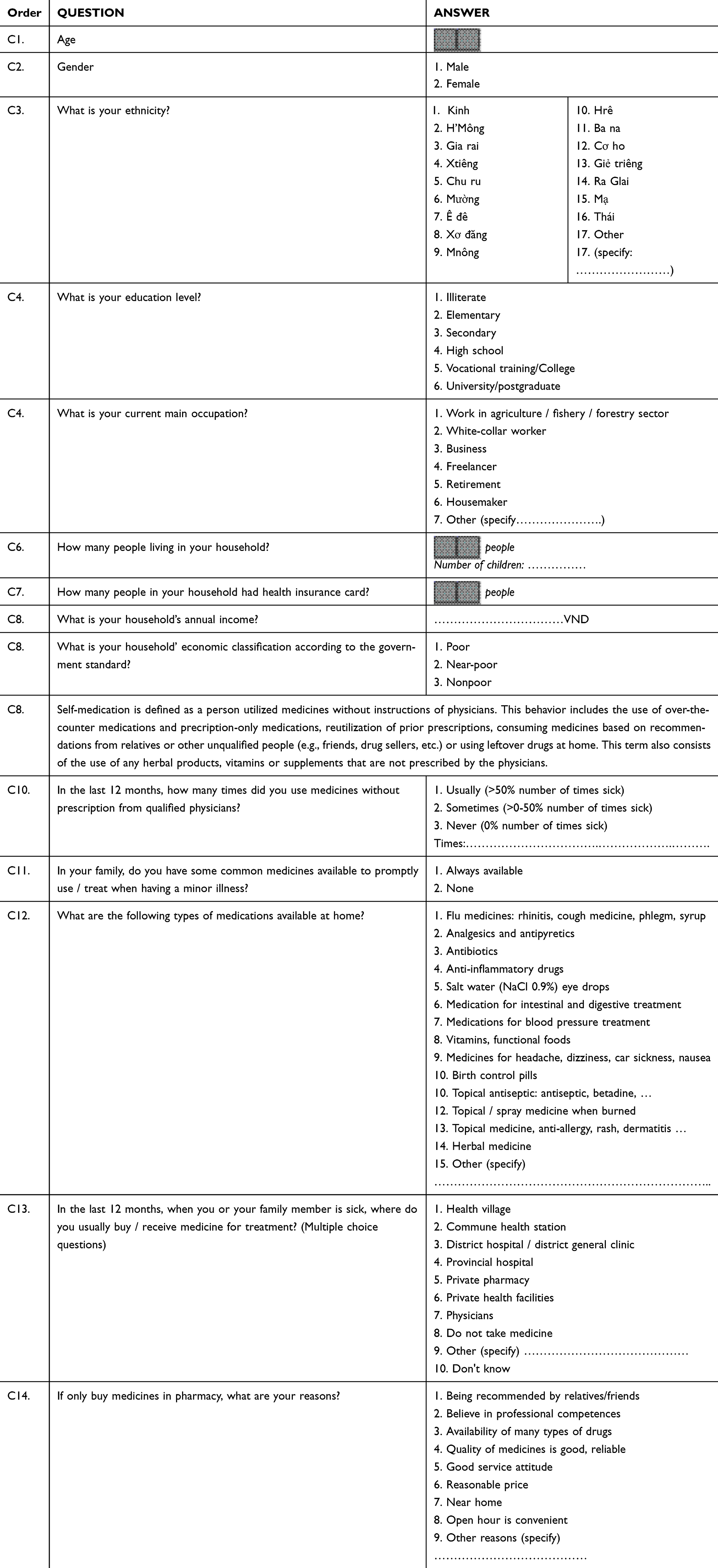 |
Table S1 Questionnaire |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.