Back to Journals » Substance Abuse and Rehabilitation » Volume 15
Self-Forgiveness and Self-Condemnation in the Context of Addictive Behavior and Suicidal Behavior
Received 5 December 2023
Accepted for publication 10 March 2024
Published 20 March 2024 Volume 2024:15 Pages 21—30
DOI https://doi.org/10.2147/SAR.S396964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rajendra Badgaiyan
Jon R Webb, Comfort M Boye
Department of Community, Family, and Addiction Sciences; Texas Tech University, Lubbock, TX, USA
Correspondence: Jon R Webb, Texas Tech University, Department of Community, Family, and Addiction Sciences, 1301 Akron Avenue, Room 271, Lubbock, TX, 79409, USA, Tel +1 806 834 2265, Fax +1 806 742 0053, Email [email protected]
Abstract: Addictive behavior and suicidal behavior are serious individual- and public-level health concerns. For those struggling with either or both, self-condemnation is a common experience, especially with respect to shame, guilt, and self-stigma. Self-forgiveness, a construct common to both religiousness/spirituality and positive psychology, may be an effective tool in addressing the self-condemnation inherent to those struggling with addictive behavior and suicidal behavior. In this review paper, we discuss (1) the nature and definition of forgiveness, (2) theoretical modeling developed regarding the general association of forgiveness with health, (3) theoretical modeling developed regarding the specific association of forgiveness with better outcomes related to addictive and/or suicidal behavior, (4) the relevance of shame, guilt, and self-stigma to the development and maintenance of addictive and suicidal behavior, and (5) the role of self-forgiveness in addressing self-condemnation, especially shame, guilt, and self-stigma. Little work explicitly focused on the association of self-forgiveness with shame, guilt, and/or self-stigma has been done. However, empirical evidence is accumulating in support of other associations proposed in the Forgiveness-Addiction-Recovery Association (FARA) Model described herein. As such, it is likely that similar support will be found when the focus is deliberately turned to shame, guilt, and self-stigma.
Keywords: positive psychology, shame, guilt, self-stigma, twelve-step model
Introduction
Addictive behavior (whether related to substance use or gambling) and suicidal behavior (whether ideation, related behaviors, attempt, or death) are each serious health concerns, not only for the individual struggling with either or both, but also in terms of the health and welfare of society at large. Worldwide, each year, over 305,000 individuals die and more than 40,345,000 disability-adjusted life years are lost (DALYs; ie, time lost because of poor health and early death) due to a substance use disorder.1–3 Considering the mere consumption of alcohol (ie, regardless of one’s level of use or problems, etc.), worldwide, each year, about 3,000,000 individuals die and about 133,000,000 DALYs are lost.1,4 Regarding suicide and suicidal behavior, worldwide, each year, between 775,000 and over 1,000,000 people die by suicide, with up to 20 times as many suicide attempts, and more than 37,500,000 DALYs being lost due to suicidal behavior.1–3,5,6
Importantly, addictive behavior and suicidal behavior are highly comorbid; such that, if a person is struggling with one, they are likely to be struggling with the other.7–10 That is, if a person is struggling with addictive behavior, they are likely also struggling with suicidal behavior. And, conversely, if a person is struggling with suicidal behavior, they are likely also struggling with addictive behavior. Related to this, when discussing the issue of suicidal behavior, it is important to note that suicidal behavior is related not only to addictive behavior, but can also be observed in other mental disorders including bipolar, depressive, and Cluster B personality disorders.11 Also, both addictive behavior and suicidal behavior can be clinical (ie, meeting diagnostic criteria) or sub-clinical (ie, problematic, but not meeting diagnostic criteria). The DSM-5-TR (see also, the ICD-11) includes diagnostic criteria for many Substance Use Disorders and Gambling Disorder, and also includes Suicidal Behavior Disorder and Nonsuicidal Self-Injury Disorder as Conditions for Further Study.11,12 In this paper we mostly use the terms addictive behavior and suicidal behavior given their broad descriptive utility regarding the inclusion of both clinical and sub-clinical sequelae.
Many individuals struggling with addictive behavior and/or suicidal behavior are experiencing a variety of negative emotions,13,14 including self-condemnation,15,16 which can manifest as shame, guilt, and self-stigma. Theoretical modeling and empirical evidence support forgiveness, a construct common to both religiousness/spirituality and positive psychology,1 as playing an important role in attenuating the negative emotions associated with addictive and suicidal behavior,1,17 including shame, guilt, and self-stigma.18–20 The aim of this paper is to provide a brief overview of a model of the Forgiveness–Addiction–Recovery Association (FARA; see Figure 1)1 and to culminate with a more deliberate focus on the effect of self-forgiveness on shame, guilt, and self-stigma (within the FARA Model), which effect is likely to lead to better addiction recovery outcomes.
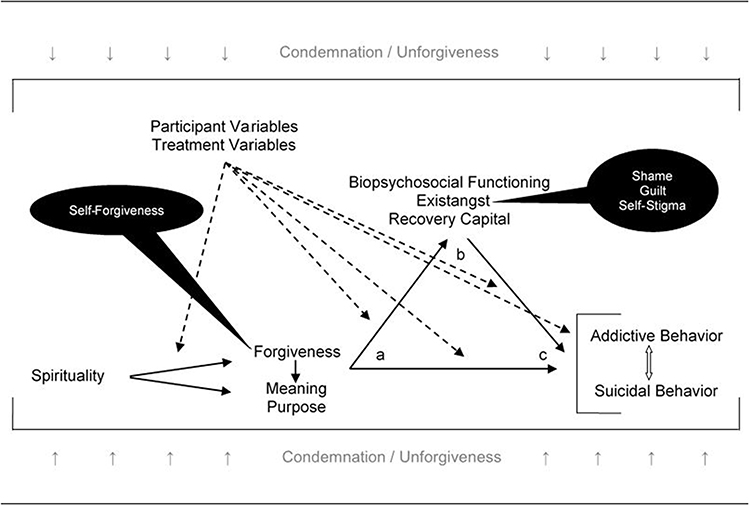 |
Figure 1 The Forgiveness–Addiction–Recovery Association: A Conceptual Model. Notes: a→c = Direct Effect of Forgiveness on Dependent Variable(s) a→b = Direct Effect of Forgiveness on Mediator Variable(s) b→c = Direct Effect of Mediator Variable(s) on Dependent Variable(s) a→b→c = Indirect Effect of Forgiveness on Dependent Variable(s) through Mediator Variable(s) dotted→ = Moderation Effect ↕ = potential for a Concomitant, Bidirectional Effect faded↓↑ = Condemnation and unforgiveness providing the context for forgiveness to become an option in the struggle of addiction recovery Adapted from Webb JR. Understanding forgiveness and addiction: Theory, research, and clinical application. Routledge; 2021, permission conveyed through Copyright Clearance Center, Inc.1 |
The Nature and Definition of Forgiveness
Forgiveness is a multidimensional construct. It can be sought, offered, and felt in the context of self, others, deity, and uncontrollable situations.21,22 Each dimension can be considered as a trait and/or a state variable; for example, although individuals may (or may not) have a tendency to forgive (ie, as a trait variable), said individuals may not (or may) forgive in a particular instance or set of circumstances (ie, as a state variable).22
Although the psychology of forgiveness, including its relationship to health and well-being, is currently receiving considerable attention in the scientific literature,23,24 a generally agreed upon definition has been difficult to come by. In an effort to bring consensus to the field, Webb et al 25 reviewed the extant literature regarding definitional issues and distilled the consistent, basic components of the general definition of forgiveness; such that it “occurs over time and is a deliberate, volitional process involving a fundamental shift in affect, cognition, and/or behavior in response to negative feelings regarding an acknowledged offensive experience, without condoning, excusing, or denying the transgression(s) – at a minimum, an absence of ill will toward an offender”.
Importantly, this general definition serves as a base upon which each dimension of forgiveness can build when incorporating its particular target (eg, self, others) or method (eg, offering, seeking). However, given particular nuance in the context of self-forgiveness (eg, the inability to avoid the self, and the need to reconcile with the self),26,27 Webb et al25 also discussed the definitional distinction of self-forgiveness; such that it also is “initiated in response to one’s own negative feelings in the context of a personally acknowledged self-instigated wrong, that results in ready accountability for said wrong and a fundamental, constructive shift in one’s relationship to, reconciliation with, and acceptance of the self through human-connectedness and commitment to change”.
Of note, although forgiveness and unforgiveness are related, they are not conceptual or empirical opposites.28 Unforgiveness is a confluence of negative emotions experienced following a transgression; for example, hatred, anger, hostility, resentment, bitterness, and fear.29 Forgiveness is considered but one option in response to the process of unforgiveness; other options include justice, avoidance, revenge, retaliation, and denial.28 In this regard, unforgiveness provides an underlying context for forgiveness, should forgiveness be the chosen response.30
Forgiveness and Health
The association of forgiveness with health and well-being is thought largely to be a function of trait or dispositional (as opposed to state or circumstantial) forgiveness and to operate through direct and indirect mechanisms.29,31 The ostensibly direct effect of forgiveness on health and well-being is thought to operate through an inextricably intertwined association with stress (ie, in terms of one’s lived, perceptual experience); such that, a forgiving person is not otherwise affected by the stress, or allostatic load,32 associated with ruminating about an offensive experience.22 Indeed, scholars explicate the general principles underlying the forgiveness-health association in the context of stress-and-coping theory.33 The indirect effect of forgiveness on health is thought to operate through explicit and distinct mediators, such as health behavior, social support, and interpersonal functioning.29,31 For example, in the context of health behavior, scholars have proposed the (un)forgiveness-energy hypothesis.29,34–36 That is, forgiveness allows one to free up the energy consumed by preoccupation with and rumination about an offensive experience and to redirect it toward other more health promoting behaviors.
Forgiveness, Addictive Behavior, and Suicidal Behavior
Worthington et al’s basic modeling regarding the general association of forgiveness with health29,31 serves as the foundation for Webb et al’s modeling regarding the association of forgiveness with the specific aspects of health related to addictive behavior and suicidal behavior (see Figure 1).1,15–17 In addition to underscoring the need for forgiveness in the context of addictive behavior and suicidal behavior arising from condemnation (whether directed toward the self or others) of those perpetrating offense, Webb et al have expanded on Worthington’s modeling in two main ways. First, in Webb et al’s modeling, the direct effect widens the scope of the intertwined relationship between forgiveness and general ruminative stress (see above) to include the specific ruminative stress of resentment. That is, forgiveness is considered a natural antidote to the fundamental interface between resentment and (1) addictive behavior and (2) suicidal behavior as described in the Twelve-Step Model (TSM) of addiction and recovery.37–40 In this regard, the importance of resentment in the relationship between forgiveness and better addiction recovery has been discussed in theoretical terms,41,42 with initial empirical evidence in support thereof.43,44
Second, in Webb et al’s modeling, additional distinct mediators have been identified and all identified mediators have been categorized. Worthington et al’s original mediators are included as examples of biopsychosocial functioning, and two additional categories of mediators have been created: existangst and recovery capital. Existangst is a term coined by Webb et al 17 to describe negative emotions which have developed into philosophical-level psychological distress; that is, existential, teleological, and angst driven emotional distress. Recovery capital refers to accessible individual characteristics (inherent or learned) and/or proximal environmental resources that facilitate initial and enduring addiction recovery.45 Examples include physical/financial capital, human capital, health capital, growth capital, social capital, family/social recovery capital, cultural capital, and community recovery capital.46
Of note, suicidal behavior also is included as an outcome variable in Webb et al’s modeling of the Forgiveness-Addiction-Recovery Association (FARA).1 When mentioning forgiveness as an antidote to the fundamental issue of resentment in the TSM (see above), four representative manifestations of the TSM were referenced, including Suicide Anonymous.40 Not only is suicidal behavior viewed as consistent with addictive behavior by adherents to the TSM, scholars also have developed theoretical modeling regarding suicidal behavior as addictive behavior and gathered empirical evidence in support thereof.47–51 Indeed, addiction has been described as a microsuicidal behavior, and similarities in the self-condemning cognitive processes of suicidal behavior and addictive behavior have been identified.52–54 Importantly, as mentioned at the outset of this paper, addictive behavior and suicidal behavior are comorbid and likely bidirectional in their relationship with one another.7–10
Existangst
Webb et al have described several negative emotional phenomena consistent with the notion of existangst.1,17 For example, symptoms of depression, anxiety, hopelessness, anger, loneliness, and temptation; that is, when such are imbued with the additional, overarching experience of “emotionally struggling with affirming one’s meaningful existence”.17, The exemplifying hallmark of existangst is psychache. Edwin Shneidman,55 considered the father of modern suicidology,56 coined the term psychache in reference to “the hurt, anguish, soreness, aching, psychological pain in the psyche, the mind. … the pain of excessively felt shame, guilt, humiliation, loneliness, fear, angst, or dread”.
Shneidman55 considered the intense, unrelenting, unremitting psychological pain of psychache – sometimes described as an aching soul57 – as the proximal cause of suicide. Although the original conceptualization of psychache occurred in the context of suicidal behavior, given the comorbidity between suicidal behavior and addictive behavior,7–10 and the torment and anguish associated with realizing one’s own self-centeredness as conceptualized in the TSM of addiction and recovery,42 Webb1 has argued for the critical relevance of psychache to addiction and recovery therefrom, whether related to substances, compulsive behaviors, or suicidal behavior.
Shame, Guilt, and Self-Stigma
As indicated above, the FARA Model operates in the context of condemnation and unforgiveness arising from intra- and/or inter-personal transgression (see Figure 1), and existangst has been discussed as a key mediator of the association of forgiveness with better outcomes related to addictive behavior and suicidal behavior. That is, higher levels of forgiveness are expected to be associated with lower levels of existangst, which in turn are expected to be associated with lower levels of addictive and/or suicidal behavior. In addition to psychache as the exemplar, the additional negative emotional phenomena of depression, anxiety, hopelessness, anger, loneliness, and temptation – when reaching philosophical-level depth and intensity – have also been identified as manifestations of existangst.1,17 Additional examples of existangst herein explicated for the first time as integral to the FARA Model are shame, guilt, and self-stigma; each of which are particularly relevant in the context of self-condemnation and self-forgiveness.
Shame and Guilt
Shame and guilt are commonly considered to be related to each other, if not essentially the same self-oriented, often negative, emotional response to problematic experiences and circumstances. Although scholars do acknowledge similarities, critical distinctive differences are emphasized as important to recognize and consider when seeking to understand and address the negative implications and consequences of each. In this regard, we draw upon the seminal work of Tangney and Dearing58 and Kurtz.59 Both authored books entitled Shame and Guilt; the former in a general, wide-ranging context, and the latter in the specific context of addictive behavior.
In terms of the similarities between shame and guilt, Tangney and Dearing58 describe both shame and guilt as emotions related to both intra- and inter-personal dynamics; both are self-conscious emotions as they involve self-evaluation and both are moral emotions as they shape ethical, socially oriented behavior (ie right versus wrong). However, while shame and guilt can arise from the same experience(s) or set of circumstances,59 there can be a stark contrast in the potential impact of each on subsequent self-perceptions and behavior, and social relations.58
Increasingly, a scholarly distinction is made between shame and guilt in terms of shame having a focus on the self, with existential-level implications for one’s self-worth, and guilt having a focus on one’s behavior, with practical implications for increasing motivation for change.58,59 Tangney and Dearing58 describe shame as “an extremely painful and ugly feeling” which can lead to an increased likelihood to blame both self and others, an increased likelihood to experience “a seething, bitter, resentful kind of anger and hostility” and a decreased likelihood to be empathic toward others. Kurtz59 describes the typical, profoundly negative experience of shame as visceral-level “narrowing, choking, [and] tightening [feelings]. … [T]he clutching feeling of dread that arises from the recognition that one is out of control”. And, that shame is reflective of “not just any lack or failure, but of the deficiency of the self as self, as human being. Shame testifies not to wrong-doing [ie, guilt] but to flawed be-ing”. Regarding guilt, Tangney58 observed that “moderately painful feelings of guilt about specific behaviors motivate people to behave in a moral, caring, socially responsible manner”. Kurtz59 describes the process of resolving guilt as painful, but not difficult and focuses on the interplay between powerlessness, unmanageability, and personal accountability facilitated by the TSM of addiction and recovery.
Arguably, when contrasted against one another, guilt is more likely to be adaptive and shame is more likely to be maladaptive; however, the reverse can occur as well. A common maxim is that guilt is good as long as it motivates one to change. The implication here is that guilt can get out of control. Indeed, Tangney and Dearing58 discuss gnawing, repetitive, and ruminative guilt arising from a lack of positive change and inaccurate attribution of responsibility for negative events to the self. Kurtz59 discusses how a person struggling with addiction may prefer to experience feelings of guilt for their poor behavior as it can help them maintain their denial of shame, rather than confronting their feelings of shame concerning their inescapable fallibility, which he argues to be the core benefit of the TSM (ie, confronting (rather than avoiding) shame through acceptance, surrender, accountability, and lifestyle change). Regarding possible positive qualities of shame, Tangney and Dearing58 argue that “the acute pain of shame may in some cases motivate productive soul-searching and revisions to one’s priorities and values. … [However,] such a positive function of shame might ensue from private, self-generated experiences of shame as opposed to public, other-generated shame episodes”.
Kurtz59 describes the paradox of the experience of shame such that it actually implies goodness; that is, when one is characterized as shameless, the insult specifies condemnation and disgrace. The implication being that one should otherwise welcome shame – within reason, of course. Of note, when scholars discuss shame and guilt and focus on the differences between the two, eg, 58,59 it is not uncommon for the lion’s share of the discussion to be focused on shame, given the assumption that shame is largely maladaptive and intra- and inter-personally destructive, whereas guilt is largely adaptive and constructive – at least when comparing and contrasting the two against each other.
Self-Stigma
Stigma is a pervasive social phenomenon that (1) influences how one is perceived, judged, and treated, (2) is based on certain characteristics or attributes determined to be negative, and (3) can lead to the devaluation of those individuals that diverge from societal norms.60 This labeling and devaluing of individuals is rooted in stereotypes, prejudice, and discrimination. Various manifestations of stigma can occur including public, perceived, enacted, and self-oriented stigma.61–63
Self-stigma, shame, and guilt are similar in that all three are psychological constructs involving negative emotions and self-evaluations. However, self-stigma differs such that it is the internalization of negative stereotypes and beliefs about oneself due to belonging to a stigmatized group.64 Also known as self-concept stigma, this form of stigma refers to the process by which individuals with stigmatized conditions or identities adopt the negative beliefs, expectations, stereotypes, attitudes, and prejudices that society holds against them, all of which can have detrimental effects on one’s mental health and help-seeking behaviors.65–68 Indeed, this can lead to feelings of shame, lowered self-esteem, reduced self-efficacy, and a sense of identity distortion.65,68
Corrigan et al 67 developed the progressive model of self-stigma, which is a theoretical framework that aims to explain the process by which individuals internalize and experience self-stigma, and includes four stages: (1) Awareness, (2) Agreement, (3) Application, and (4) Action. The first stage involves becoming aware of the negative stereotypes and societal attitudes associated with stigmatized identity(s), which, in the context of this paper, refers to addictive behavior and suicidal behavior. This awareness can occur through direct experiences of bias, discrimination, media exposure, or interaction(s) with others who hold stigma-oriented beliefs. The second stage, involves beginning to accept and internalize, or agree with the negative stereotypes and beliefs of others about one’s stigmatized identity. The stereotypes are not only adopted, but believed to be a true reflection of one’s own abilities, worth, or potential. The third stage involves the application of said stigmatizing beliefs and stereotypes to oneself. Negative views are incorporated into the self-concept, such that self-perception is considered through the lens of societal prejudice. This aspect of internalization can lead to diminished self-esteem, reduced self-efficacy, and a sense of hopelessness. The final stage of progression is action which encompasses the likely behavioral consequences of self-stigma. For example, individuals may avoid seeking help or support due to mistrust, or for fear of confirming negative stereotypes or experiencing further discrimination. Also, individuals may withdraw from social interactions or engage in self-sabotaging behaviors, thereby further perpetuating the cycle of self-stigma.
Self-Condemnation and Self-Forgiveness
Although there are particular types of associations and mechanisms within both the general forgiveness-health association29,31 and the more specific Forgiveness-Addiction-Recovery Association (FARA; see Figure 1),1 as mentioned above, the explication of the underlying nature of the association of forgiveness with health and well-being is in the broad context of stress-and-coping theory. This holds whether in the context of (1) forgiveness in general and health and well-being in general,33 (2) self-forgiveness in particular and health and well-being in general,69 or (3) self-forgiveness in particular and addictive behavior or suicidal behavior in particular.16 Moreover, the presence of condemnation (whether self-oriented or other-oriented) resulting from transgression (whether intra- or inter-personal) is a critical contributor to whether forgiveness in its various targets (self, others, etc.) and methods (offering, feeling, etc.) becomes a relevant tool for addressing health and well-being. Our focus here is addressing self-condemnation, which can manifest as shame, guilt, and self-stigma, through the process of self-forgiveness.
Self-forgiveness can be very pertinent when addressing the self-condemnation inherent to addictive and suicidal behavior, especially when conceptualized through the Twelve-Step Model (TSM) of addiction and recovery,42 which will be the main focus of the remaining discussion. Similarly though, the process of self-forgiveness also is consistent with various models of counseling, psychotherapy, and behavior change, including motivational interviewing, stages of change, second-wave (eg, Rational Emotive Behavior Therapy) and third-wave (eg, Acceptance and Commitment Therapy) cognitive-behaviorism, and thus, potentially a very relevant and important contributor to better addiction recovery outcomes beyond TSM conceptualization.1,17 Of note, forgiveness is not a panacea, whether for health and well-being in general or addiction recovery in particular. Even still, when intra- and inter-personal tension and conflict are present and a barrier to health and well-being, forgiveness can be an important catalyst for better outcomes, including with respect to addiction recovery.1,70,71
Self-condemnation – especially shame, guilt, and self-stigma – from a TSM point of view, plays a critical role in instigating and maintaining addictive and suicidal behavior, and preventing recovery therefrom, whether in the context of problems related to substances, compulsive behavioral sets (eg, gambling), or suicidal behavior. The following discussion will draw from material considered to be the basic/fundamental literature of Alcoholics Anonymous (AA),37 Narcotics Anonymous (NA),39 Gamblers Anonymous (GA),38 and Suicide Anonymous (SA),40 including accounts of the personal struggle with addictive and/or suicidal behavior. Each of these primary texts not only discusses the core principles of the TSM of addiction and recovery as applied to their particular area of focus, but also deliberately provides illustrative examples of the lived experience of addictive and/or suicidal behavior – whether in the narrative of the discussion of the core principles or the explicit presentation of personal stories. Of note, much of the following discussion will rely on quotes, as paraphrasing often does not adequately portray the lived experience of addiction and recovery.
Regarding shame, many experiences are described in the so-called Big Book of AA,37 including “heartsickness, shame, and fear bordering on panic, and no complete escape any longer except in oblivion;” indeed, “the shame was too great, and I would drive it back down with bottles of vodka and cases of beer”. Another person described feeling “full of shame, guilt, and remorse; … I wanted to die”. And, still another described feeling “ashamed and destroyed … my shame and humiliation were beyond words … and I entertained the idea of suicide. … I was hurting more than I ever knew a human could hurt, and I just wanted the pain to end”. Similarly, in the so-called Basic Text of NA,39 a person discussed how “the shame, fear, inferiority, despair, and loneliness only got bigger and bigger”. Another person discussed how the “alienation, legal problems, shame, guilt, loneliness, degradation, and despair reached such frenzied cycle that eventually suicide seemed like the only option”. And, still another stated “I was sick of myself and felt nothing but anger, disgust, and shame”. In Gamblers Anonymous: A New Beginning,38 we learn of “the tears, the guilt, the shame, the unworthiness” and of “feeling alone, frightened, helpless, desperate, and ashamed”. Lastly, in Suicide Anonymous: The Little Book40 there are reports of keeping “the thoughts to ourselves – often in shame, since suicide is a disgrace” and of going “back to shame and worthlessness, and the suicide cycle started again” and “my shame, despair, and self-loathing were so great” all of which support the notion that “nothing is more shameful than suicide”.
Regarding guilt, again, many experiences are described in the Big Book of AA,37 including “bearing the burden of guilt” and “I couldn’t get sober, and I couldn’t get drunk. I was feeling scared, remorseful, guilty”. And, “we rid ourselves of guilt and remorse as we ‘clean out the garbage’ from our minds”. Similarly, in the Basic Text of NA,39 “I felt shame and guilt and would regularly judge and punish myself” and “our addiction enslaved us. We were prisoners of our own mind and were condemned by our own guilt” and “getting off drugs was not easy, but it was the easier part. My pain, shame, guilt, and complete confusion were all too much to take”. In A New Beginning,38 “dormant, accumulating guilt has long been our enemy … Each of us has our own collection of guilt which must be unearthed. After discovering and digging up this guilt, one will find it necessary to rid oneself of it;” indeed, “the agonizing guilt”. Lastly, in The Little Book,40 “I approached social activities, friendships and decisions based on guilt and inferiority, the never-satisfied need to be accepted” and “things were too bad; the pain was too great. … I couldn’t face the guilt” and “many of us made an attempt or attempts to end our life, only to awaken sickened by the realization that our best efforts had failed. This increased our guilt, self-hatred, remorse, emptiness, and pain”.
Regarding self-stigma, in the Big Book of AA,37 “during all this time we became more or less ostracized by our friends” and “shunned as a pariah”. However, with the program of AA “emphasizing alcoholism as an illness, the social stigma associated with this condition is being blotted out;” indeed, individuals learn that “[they are not] mad or vicious [but,] a sick person … suffering from an actual disease … and a disease [is] respectable [and] not a moral stigma”. In the Basic Text of NA,39 the feeling of “being ostracized from [one’s] job and family” is described. Fortunately, a strength of the recovery program is the development of good will, which “is best exemplified in service [and] proper service is ‘doing the right thing for the right reason.’ When good will supports and motivates both the individual and the Fellowship, we are fully whole and wholly free. [However,] probably the last to be lost to [this newfound] freedom will be the stigma of being an addict”. Similarly, A New Beginning,38 in describing the utility of GA, describes how “anonymity also has great value in attracting new members who initially feel there is a stigma attached to the problem”. Lastly, The Little Book,40 addresses the importance of meetings such that they “help us overcome our sense of shame and stigma, the forces that could drive us deeper into secrecy, denial and relapse”.
The relevance of self-forgiveness in addressing the self-condemnation of addictive and/or suicidal behavior – whether in the context of shame, guilt, self-stigma, or otherwise – can also be recognized in more broad notions of addiction and recovery in the TSM. The TSM37 holds that “self-centeredness … is the root of [one’s] troubles. Driven by a hundred forms of fear, self-delusion, self-seeking, and self-pity … Above everything, we … must be rid of this selfishness. We must or it kills us”. Importantly, the TSM does not attribute the problem of addictive behavior entirely to self-centeredness. For example, the Fourth and Fifth Steps are designed to identify grudges and make amends when possible – with respect to “people, institutions, or principles with whom we [are] angry”. Clearly, Steps Four and Five can include self, others, and myriad entities or things. Also, there is no doubt that addiction often arises from trauma; that is, as an attempt to cope with the consequences and negative emotions associated with traumatic experiences. Arguably, a meaningful proportion of the self-centeredness described by the TSM is in the context of survival and self-preservation in response to traumatic experiences, but which ultimately proves to be self-defeating – given the many pitfalls of self-centeredness (see above). As Viktor Frankl,72 a psychiatrist and Holocaust survivor, stressed, “everything can be taken from [us] but one thing: the last of the human freedoms – to choose one’s attitude in any given set of circumstances, to choose one’s own way”. In this regard, self-centeredness may lead us to choose self-defeating responses. Moreover, as Webb and Toussaint42 discuss, the self-centered processes described by the TSM “will inevitably result in self-directed resentments and self-loathing. [And,] with continued and repeated failure to overcome addictive behavior (ie, relapse), overwhelming guilt and shame [and self-stigma], or excruciating self-condemnation are sure to follow”.
Lay persons (ie, the TSM; see above) and scholars59,73–75 agree that shame, guilt, and self-stigma are important to the development, maintenance, and resolution of addictive and suicidal behavior. Likewise, lay persons (ie, the TSM) and scholars1,76 agree that (un)forgiveness is very relevant to addiction and recovery. However, little empirical work has examined the association of forgiveness with shame, guilt, and self-stigma in the context of addictive behavior and/or suicidal behavior.1,19,20,77–79
Conclusion
The very nature of each of shame, guilt, and self-stigma – especially shame and self-stigma, but also guilt when it is out of control – is imbued with existangst. That is, each of these negative affective phenomena can easily rise to a philosophical-level, “[emotional struggle] with affirming one’s meaningful existence”.17, Self-forgiveness is very relevant to the process of addressing self-condemnation, including with respect to shame, guilt, and self-stigma, given the fundamental component of negative self-evaluation being inherent to each. However, although comprehensive theoretical modeling has been developed (see Figure 1), little work explicitly examining the association of self-forgiveness (indeed, all dimensions of forgiveness) with shame, guilt, and/or self-stigma in the context of addictive behavior and/or suicidal behavior has been done. Importantly, related empirical work examining (and affirming) additional potential associations of forgiveness with better outcomes related to addictive and suicidal behavior is accumulating; thereby, suggesting the same will likely be observed when the focus is deliberately turned to shame, guilt, and self-stigma. Indeed, empirical evidence suggests that many dimensions of forgiveness are associated with better addiction recovery outcomes, and that self-forgiveness may be the most important dimension thereof; that is, when forgiveness is relevant to the process of addiction recovery.1
Acknowledgement
Please contact the first and correspondence author for the page numbers associated with the quoted materials.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Webb JR. Understanding Forgiveness and Addiction: Theory, Research, and Clinical Application. Routledge; 2021.
2. World Health Organization. Health statistics and information systems: disease burden and mortality estimates: cause-specific mortality, 2000–2016. Geneva; 2016. Available from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/.
3. World Health Organization. Health statistics and information systems: disease burden and mortality estimates: disease burden, 2000–2016. Geneva: author; 2016. Available from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html.
4. World Health Organization. Global Status Report on Alcohol and Health (2018). Executive Summary. Geneva: Author; 2018.
5. Värnik P. Suicide in the world. Int J Environ Res Public Health. 2012;9(3):760–771. doi:10.3390/ijerph9030760
6. World Health Organization. LIVE LIFE: preventing suicide. Geneva: author; 2018. Available from https://www.who.int/publications-detail/live-life-preventing-suicide.
7. Amiri S, Behnezhad S. Alcohol use and risk of suicide: a systematic review and meta-analysis. J Addict Dis. 2020;38(2):200–213. doi:10.1080/10550887.2020.1736757
8. Bagge CL, Conner KR, Reed L, Dawkins M, Murray K. Alcohol use to facilitate a suicide attempt: an event-based examination. J Stud Alcohol Drugs. 2015;76(3):474–481. doi:10.15288/jsad.2015.76.474
9. Dvorak RD, Lamis DA, Malone PS. Alcohol use, depressive symptoms, and impulsivity as risk factors for suicide proneness among college students. J Affect Disord. 2013;149(1–3):326–334. doi:10.1016/j.jad.2013.01.046
10. Yuodelis‐Flores C, Ries RK. Addiction and suicide: a review. Am J Addict. 2015;24(2):98–104. doi:10.1111/ajad.12185
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
12. World Health Organization. International classification of diseases, 11th revision (ICD-11). Geneva: author; 2022. Available from https://www.who.int/classifications/classification-of-diseases.
13. Coppersmith DDL, Millgram Y, Kleiman EM, et al. Suicidal thinking as affect regulation. J Psychopathol Clin Sci. 2023;132(4):385–395. doi:10.1037/abn0000828
14. Hogarth L. Addiction is driven by excessive goal-directed drug choice under negative affect: translational critique of habit and compulsion theory. Neuropsychopharmacology. 2020;45(5):720–735. doi:10.1038/s41386-020-0600-8
15. Hirsch JK, Webb JR, Toussaint LL. Self-forgiveness, self-harm, and suicidal behavior: understanding the role of forgiving the self in the act of hurting one’s self. In: Woodyatt L, Worthington EL, Wenzel M, Griffin BJ, editors. Handbook of the Psychology of Self-Forgiveness. Springer; 2017:249–264.
16. Webb JR, Toussaint LL, Hirsch JK. Self-forgiveness, addiction, and recovery. In: Woodyatt L, Worthington EL, Wenzel M, Griffin BJ, editors. Handbook of the Psychology of Self-Forgiveness. Springer; 2017:265–277.
17. Webb JR, Hirsch JK, Toussaint LL; Suicide and Spirituality in the Military. Forgiveness as a positive psychotherapy for addiction and suicide: theory, research, and practice. Spiritual Clin Pract. 2015;2(1):48–60. doi:10.1037/scp0000054
18. Leach CW. Understanding shame and guilt. In: Woodyat L, Worthington EL, Wenzel M, Griffin BJ, editors. Handbook of the Psychology of Self-Forgiveness. Springer International Publishing/Springer Nature; 2017:17–28.
19. Verona MP, Branthoover H. The effect of a self-forgiveness model on self-stigma in individuals diagnosed with substance use disorders. Couns Values. 2022;67(2):203–224. doi:10.1163/2161007x-67020004
20. Ianni PA, Hart KE, Hibbard S, Carroll M. The association between self-forgiveness and alcohol misuse depends on the severity of drinker’s shame: toward a buffering model. Addict Disord Their Treat. 2010;9(3):106–111. doi:10.1097/ADT.0b013e3181f158cd
21. Thompson LY, Snyder CR, Hoffman L, et al. Dispositional forgiveness of self, others, and situations. J Pers. 2005;73(2):313–359. doi:10.1111/j.1467-6494.2005.00311.x
22. Toussaint LL, Webb JR. Theoretical and empirical connections between forgiveness, mental health, and well-being. In: Worthington EL, editor. Handbook of Forgiveness. Routledge; 2005:349–362.
23. Toussaint LL, Worthington EL, Williams DR, eds.. Forgiveness and Health: Scientific Evidence and Theories Relating Forgiveness to Better Health. Springer; 2015.
24. Worthington EL, Wade NG, eds.. Handbook of Forgiveness.
25. Webb JR, Bumgarner DJ, Conway-Williams E, Dangel T, Hall BB. A consensus definition of self-forgiveness: implications for assessment and treatment. Spiritual Clin Pract. 2017;4(3):216–227. doi:10.1037/scp0000138
26. Enright RD; The Human Development Study Group. Counseling within the forgiveness triad: on forgiving, receiving forgiveness, and self-forgiveness. Couns Values. 1996;40(2):107–126. doi:10.1002/j.2161-007X.1996.tb00844.x
27. Tangney JP, Boone AL, Dearing R. Forgiving the self: conceptual issues and empirical findings. In: Worthington EL, editor. Handbook of Forgiveness. Routledge; 2005:143–158.
28. Wade NG, Worthington EL. Overcoming interpersonal offenses: is forgiveness the only way to deal with unforgiveness? J Couns Dev. 2003;81(3):343–353. doi:10.1002/j.1556-6678.2003.tb00261.x
29. Worthington EL Jr, Berry JW, Parrott L. Unforgiveness, forgiveness, religion, and health. In: Plante TG, Sherman AC, editors. Faith and Health: Psychological Perspectives. Guilford Press; 2001:107–138.
30. Enright RD. Forgiveness is a Choice: A Step-by-Step Process for Resolving Anger and Restoring Hope. American Psychological Association; 2001.
31. Lavelock CR, Snipes DJ, Griffin BJ, et al. Forgiveness and health: scientific evidence and theories relating forgiveness to better health. In: Toussaint LL, Worthington EL, Williams DR, editors. A Conceptual Model of Forgiveness and Health. Springer; 2015:3.
32. McEwen BS. Stressed or stressed out: what is the difference? J Psychiatry Neurosci. 2005;30(5):315–318.
33. Strelan P. The stress-and-coping model of forgiveness: theory, research, and the potential of dyadic coping. In: Worthington EL, Wade NG, editors. Handbook of Forgiveness. Routledge; 2020:63–73:chap 7.
34. Svalina SS, Webb JR. Forgiveness and health among people in outpatient physical therapy. Disabil Rehabil. 2012;34(5):383–392. doi:10.3109/09638288.2011.607216
35. Temoshok LR, Chandra PS. The meaning of forgiveness in a specific situational and cultural context: persons living with HIV/AIDS in India. In: McCullough ME, Pargament KI, Thoresen CE, editors. Forgiveness: Theory, Research, and Practice. Guilford Press; 2000:41–64.
36. Temoshok LR, Wald RL. Forgiveness and health in persons living with HIV/AIDS. In: Handbook of Forgiveness. Brunner-Routledge; 2005:335–348.
37. Anonymous A. Alcoholics Anonymous: The Story of How Many Thousands of Men and Women Have Recovered from Alcoholism.
38. Anonymous G. A New Beginning. Author; 1989.
39. Narcotics Anonymous. Narcotics Anonymous.
40. Suicide Anonymous. Suicide anonymous, the little book (Revised edition) Memphis, TN: author; 2015. Available from https://suicideanonymous.net/readings-and-downloads.
41. Lyons GCB, Deane FP, Kelly PJ. Forgiveness and purpose in life as spiritual mechanisms of recovery from substance use disorders. Addict Res Theory. 2010;18(5):528–543. doi:10.3109/16066351003660619
42. Webb JR, Toussaint LL. Self-forgiveness as a critical factor in addiction and recovery: a 12-step model perspective. Alcohol Treat Q. 2018;36(1):15–31. doi:10.1080/07347324.2017.1391057
43. Lyons GCB, Deane FP, Caputi P, Kelly PJ. Spirituality and the treatment of substance use disorders: an exploration of forgiveness, resentment and purpose in life. Addict Res Theory. 2011;19(5):459–469. doi:10.3109/16066359.2011.555022
44. Webb JR, Boye CM, Maxton AS, Mills ME, Murphy DP, Brewer KG. Forgiveness, resentment, well-being, and college student substance use in southern Appalachia and west Texas. Alcohol Treat Q. 2024;1–19. doi:10.1080/07347324.2024.2322117
45. Granfield R, Cloud W. Coming Clean: Overcoming Addiction Without Treatment. New York University Press; 1999.
46. Hennessy EA. Recovery capital: a systematic review of the literature. Addict Res Theory. 2017;25(5):349–360. doi:10.1080/16066359.2017.1297990
47. Blasco-Fontecilla H. The addiction to suicidal behavior. In: Courtet P, editor. Understanding Suicide: From Diagnosis to Personalized Treatment. Springer International Publishing; 2016:53–61.
48. Blasco-Fontecilla H, Artieda-Urrutia P, Berenguer-Elias N, et al. Are major repeater patients addicted to suicidal behavior? Adicciones. 2014;26(4):321–333. doi:10.20882/adicciones.38
49. Blasco-Fontecilla H, Fernández-Fernández R, Colino L, Fajardo L, Perteguer-Barrio R, de Leon J. The addictive model of self-harming (non-suicidal and suicidal) behavior. Front Psychiatry. 2016;7:doi:10.3389/fpsyt.2016.00008
50. Hatteschweiler C, Graziani P, Bon M, Charbonnier E. Addiction et passage à l’acte suicidaire: des processus cognitifs similaires? = Addiction and passage to the suicidal act: similar cognitive processes? Revue Francop de Clinique Comport Cog. 2015;20(3):35–44.
51. Tullis K. A theory of suicide addiction. Sex Addict Compuls. 1998;5(4):311–324. doi:10.1080/10720169808402339
52. Firestone L; Suicide and the Inner Voice. Ellis TE, editor. Cognition and suicide: theory, research, and therapy. In: American Psychological Association. 2006:119–147.
53. Firestone RW. The ‘inner voice’ and suicide. Psychotherapy. 1986;23(3):439–447. doi:10.1037/h0085636
54. Firestone RW, Seiden RH. Microsuicide and suicidal threats of everyday life. Psychotherapy. 1987;24(1):31–39. doi:10.1037/h0085688
55. Shneidman E. Suicide as Psychache: A Clinical Approach to Self-Destructive Behavior. Jason Aronson, Inc.; 1993.
56. Jobes DA, Nelson KN; Shneidman’s contributions to the understanding of suicidal thinking. Ellis TE, editor. Cognition and suicide: theory, research, and therapy. In: American Psychological Association. 2006:29–49.
57. Holden RR, Mehta K, Cunningham EJ, McLeod LD. Development and preliminary validation of a scale of psychache. Can J Behav Sci. 2001;33(4):224–232. doi:10.1037/h0087144
58. Tangney JP, Dearing RL. Shame and Guilt. The Guilford Press; 2002.
59. Kurtz E. Shame & Guilt.
60. Goffman E. Stigma: Notes on the Management of Spoiled Identity. Simon & Schuster; 2009.
61. Corrigan PW, Powell KJ, Rüsch N. How does stigma affect work in people with serious mental illnesses? Psychiatr Rehabil J. 2012;35(5):381–384. doi:10.1037/h0094497
62. Fox AB, Earnshaw VA, Taverna EC, Vogt D. Conceptualizing and measuring mental illness stigma: the mental illness stigma framework and critical review of measures. Stigma Health. 2018;3(4):348–376. doi:10.1037/sah0000104
63. Pattyn E, Verhaeghe M, Sercu C, Bracke P. Public stigma and self-stigma: differential association with attitudes toward formal and informal help seeking. Psychiatr Serv. 2014;65(2):232–238. doi:10.1176/appi.ps.201200561
64. Vogel DL, Wade NG, Hackler AH. Perceived public stigma and the willingness to seek counseling: the mediating roles of self-stigma and attitudes toward counseling. J Couns Psychol. 2007;54(1):40–50. doi:10.1037/0022-0167.54.1.40
65. Corrigan PW, Kuwabara SA, O’Shaughnessy J. The public stigma of mental illness and drug addiction: findings from a stratified random sample. J Soc Work. 2009;9(2):139–147. doi:10.1177/1468017308101818
66. Corrigan PW, Watson AC. The paradox of self-stigma and mental illness. Clin Psychol. 2002;9(1):35–53. doi:10.1093/clipsy.9.1.35
67. Corrigan PW, Watson AC, Barr L. The self-stigma of mental illness: implications for self-esteem and self-efficacy. J Soc Clin Psychol. 2006;25(8):875–884. doi:10.1521/jscp.2006.25.8.875
68. Luoma JB, Ak O, Kohlenberg BS, Hayes SC, Fletcher L. The development and psychometric properties of a new measure of perceived stigma toward substance users. Subst Use Misuse. 2010;45(1–2):47–57. doi:10.3109/10826080902864712
69. Toussaint LL, Webb JR, Hirsch JK. Self-forgiveness and health: a stress-and-coping model. In: Woodyatt L, Worthington EL, Wenzel M, Griffin BJ, editors. Handbook of the Psychology of Self-Forgiveness. Springer; 2017:87–99.
70. Toussaint LL, Worthington EL Jr, Williams DR, Webb JR. Forgiveness and physical health. In: Worthington EL, Wade NG, editors. Handbook of Forgiveness.
71. Webb JR, Toussaint LL. Forgiveness, well-being, and mental health. In: Worthington EL, Wade NG, editors. Handbook for Forgiveness.
72. Frankl VE. Man’s Search for Meaning: An Introduction to Logotherapy. Lasch I.
73. Luoma JB, Kulesza M, Hayes SC, Kohlenberg B, Larimer M. Stigma predicts residential treatment length for substance use disorder. Am J Drug Alcohol Abuse. 2014;40(3):206–212. doi:10.3109/00952990.2014.901337
74. Snoek A, McGeer V, Brandenburg D, Kennett J. Managing shame and guilt in addiction: a pathway to recovery. Addict Behav. 2021;120:106954. doi:10.1016/j.addbeh.2021.106954
75. Batchelder AW, Glynn TR, Moskowitz JT, et al. The shame spiral of addiction: negative self-conscious emotion and substance use. PLoS One. 2022;17(3):e0265480. doi:10.1371/journal.pone.0265480
76. Calhoun FJ. Developmental research on alcohol and spirituality: what we know and what we don’t know. South Med J. 2007;100(4):427–429. doi:10.1097/SMJ.0b013e3180315de4
77. Babić N. Ruminacije o pijenju alkohola kao prediktor depresivnosti i alkoholne žudnje kod osoba na bolničkom liječenju od ovisnosti o alkoholu = Rumination about drinking as a predictor of depression and alcohol craving among inpatients in treatment of alcohol use disorder. Psihologijske Teme. 2019;28(3):645–660. doi:10.31820/pt.28.3.10
78. Carlier J. Penal substitutionary atonement and the problem of shame in addiction. Pastoral Psychol. 2023;72(5):659–673. doi:10.1007/s11089-023-01089-5
79. Mosher DK, Hook JN, Grubbs JB. Self-forgiveness and hypersexual behavior. In: Woodyatt L, Worthington EL, Wenzel M, Griffin BJ, editors. Handbook of the Psychology of Self-Forgiveness. Springer International Publishing/Springer Nature; 2017:279–291.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.