Back to Journals » Patient Preference and Adherence » Volume 19
Self-Care Activities and Self-Efficacy Among Jordanian Patients with Hypertension: A Cross-Sectional Study
Authors Ayasrah S ![]() , Hamdan Y, Mazahreh SA
, Hamdan Y, Mazahreh SA ![]() , Alsadaan N, Basheti IA
, Alsadaan N, Basheti IA
Received 21 July 2025
Accepted for publication 12 November 2025
Published 20 November 2025 Volume 2025:19 Pages 3701—3715
DOI https://doi.org/10.2147/PPA.S555129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Qizhi (Cathy) Yao
Shahnaz Ayasrah,1 Yaman Hamdan,2 Suliman A Mazahreh,3 Nourah Alsadaan,4 Iman A Basheti5
1Applied Science Department, Al-Balqa Applied University, Al-Salt, Jordan; 2Urology Surgical Department, Islamic Hospital, Amman, Jordan; 3Department of Surgery, King Hussein Cancer Center, Amman, Jordan; 4Department of Nursing Administration and Education- College of Nursing, Jouf University, Sakaka, 72388, Saudi Arabia; 5Pharmaceutical Sciences Department - Faculty of Pharmacy, Jadara University, Irbid, Jordan
Correspondence: Shahnaz Ayasrah, Al-Balqa Applied University, Al-Salt, Jordan, Email [email protected]
Purpose: This study aimed to evaluate self-care activities (SCAs) and self-efficacy, and to determine their correlates and predictors among Jordanian patients with hypertension.
Patients and Methods: A descriptive, cross-sectional correlational design study was used among 231 patients. Data was collected using structured interviews guided with a questionnaire that included demographic and clinical data, the Arabic version of the Hypertension Self-care Activity Level Effects (H-SCALE), and the Perceived Self-Efficacy Scale.
Results: The mean age was 49.2 years (SD = 13.4); 55.4% were males and 72.7% were married. Among them, comorbidities were prevalent (68%), with 42% of participants reporting diabetes. More than half were smokers (56.3%). The mean BMI was 28.3 (SD = 4.5), indicating overweight status. The mean H-SCALE score was 40.7 (SD = 9.1, range 17.82– 62.8), indicating low adherence to recommended self-care activities to manage hypertension. Female patients and those with chronic hypertension had significantly higher H-SCALE scores (p < 0.001). Significant predictors of H-SCALE included gender (B = 2.91, p =0.027), marital status (B = − 4.52, p =0.01), time since diagnosis (B = 4.2, p =0.001), and self-efficacy (B =0.18, p =0.001), explaining 28% of the variance (R2 =0.277, F(10, 220) = 4.81, p < 0.001). The mean self-efficacy score was 16.6 (SD = 12.2, range 0– 45), indicating low self-efficacy. Female patients and those with chronic hypertension also had higher self-efficacy (p < 0.001). Predictors included age (B = − 0.288, p < 0.001), time since diagnosis (B = 7.84, p < 0.001), and H-SCALE score (B =0.290, p =0.001), accounting for 35% of the variance (R2 =0.354, F(10, 220) = 7.55, p < 0.001).
Conclusion: Low levels of self-care activities and self-efficacy increase the risk of hypertension-related complications. Targeted interventions, such as patient education, lifestyle modification, routine follow-up, self-monitoring, and integrating digital health tools, are needed to improve patient outcomes.
Keywords: hypertension, self-care activities, self-efficacy, adherence, Jordan
Introduction
Hypertension is a serious medical illness and a major global risk factor, affecting around 1.28 billion individuals aged 30–79 worldwide and contributing significantly to premature mortality. Among them, over 588 million (46%) are thought to be unaware of their condition, as hypertension is often symptomless.1 Due to its high prevalence, association with cardiac and renal diseases, and its role as a preventable risk factor for early death and disability, hypertension is a major global health concern.2,3 Patients from both developed and developing countries are affected, adding to the global disease burden due to its correlation with morbidity and mortality.4–7
Despite increasing awareness and treatment rates over the past decade, less than half of hypertensive patients have their blood pressure under control, regardless of ethnicity or sex.7 Across all countries, aging populations and rising obesity rates drive the high prevalence of hypertension. Additional contributors include also high dietary salt intake.8 Notably, two-thirds of the world’s hypertensive population lives in low- and middle-income countries.1 Unlike industrialized nations, developing countries face rising hypertension rates without matching increases in awareness or control.4 Contributing behavioral and social factors include but not limited to poor diet, urbanization, stress, obesity, and physical inactivity.4,5
Antihypertensive medications are often the first line of treatment; however, blood pressure does not always reduce adequately due to poor adherence.8 Patients often dislike medication or experience unpleasant side effects. Trials on antihypertensive drug efficacy reveal a high rate of study withdrawal due to adverse effects, while non-adherence can increase hospitalizations and emergency visits.9 Therapeutic lifestyle changes are recommended along with drug therapy for hypertensive patients and considered as the first-line treatment for those with pre-hypertension. Despite improvements in healthy behaviors like smoking cessation, diet, and exercise, many individuals still do not meet ideal standards. Even for people who take their prescriptions as directed, maintaining these behaviors over the long term can be difficult. Thus, it is essential to assess medication adherence as well as other self-care practices.9,10
The global number of hypertensive adults is increasing, especially in low- and middle-income countries, driven by a rise in hypertension risk factors in these populations.1 More epidemiological data are needed to assess prevalence, awareness, treatment, and control trends, as well as the factors contributing to poor management.11,12 National interventions tailored to local culture, economy, and demographics are necessary.8,10 Evaluating new hypertension management strategies in developing countries is also essential.5
Nearly one-third of Jordanian adults have high blood pressure,11 and by 2030, its prevalence is projected to rise by 7.2%.13 Jordan ranks seventh globally for hypertension-related mortality, with the condition being the sixth leading cause of death. The first and second-most common causes of death are coronary artery disease and stroke respectively, both of which are associated with hypertension.14 The gaps in the management of hypertension can be seen in that, only one-third of the Jordanians patients who treated with antihypertensive drugs have regulated their blood pressure levels.11 Suboptimal control of hypertension is related to a lack of proper implementation of evidence-based practices, lack of adherence, and inadequate public awareness. The awareness of hypertension is necessary to encourage prevention and treatment through behavioral change. In Jordan, however, patient knowledge of symptoms, risks, and treatment is still low, with a great need of public health education interventions to enhance awareness of hypertension.15 Jordan is going through a dietary transition reflected in an increase in overweight and obesity, mostly among women aged 15–49, leading to the high prevalence of noncommunicable diseases, including hypertension.16 However, men over the age of 25 face a higher risk of premature death from these conditions.17 In particular, hypertension, a major risk factor for ischemic heart disease, was identified as a high research priority in Jordan.18 Despite its importance, knowledge about self-care activities and self-efficacy among Jordanian patients with hypertension is limited. This study aimed to assess the prevalence of self-care behaviors and levels of self-efficacy, and to identify the associated factors and predictors, which play a critical role in hypertension management. The findings may inform strategies to promote self-care and support primary care physicians in helping patients achieve blood pressure control. Specifically, the study investigated the following research questions among Jordanian patients with hypertension:
- What is the prevalence of self-care behaviors recommended for optimal BP control in this population ?
- What is the level of self-efficacy?
- Which factors are associated with performing self-care activities and self-efficacy ?
- Which factors are significant predictors of self-care activities and self-efficacy ?
Materials and Methods
The study utilized a descriptive cross-sectional, correlational design among Jordanian patients with hypertension.
Setting
Patients recruited from the waiting rooms of the outpatient medical clinics at AL-Hussein / Salt Hospital a governmental hospital with 350 beds located in Al-Salt city in Jordan. Al-Hussein Hospital is centrally located in Jordan and provides services to patients from diverse rural and urban areas as well as from different health insurance sectors.
Sample and Sampling
Patients were included in the study if they were aged 18 years or older; diagnosed with essential hypertension for at least 3 months; treated with at least one antihypertensive medication based on the patient’s medical chart; had no serious complications of hypertension. Patients were excluded from the study if they have communication or comprehension impairment (e.g. aphasia (incapable to express and/or comprehend Arabic); were pregnant women; were treated for a life-threatening condition or major illness such as kidney failure or cancer, due to their special conditions. Patients suffering from diseases associated with hypertension, which may affect their physical activity, such as stroke, were also excluded.
An independent samples t-test with a statistical power of 0.80, a significant level of = 0.05, a two-tailed test of significance, and a medium effect size of 0.40 was used to compute the sample size. For a statistical power of 0.80 with a medium effect size, using G-power, a total sample of 200 hypertensive patients is required. An additional 30 patients were included to account for potential attrition. The SPSS 21.0 software was used to examine all the data.19
Data Collection
With the assistance of the clinic’s chief nurse, patient records were reviewed to confirm eligibility. Eligible patients were provided with full information about the purpose of the study, and a consent form was signed by those who consented to participate in the study. Once the consent was obtained, the researchers used the electronic medical records of the patients to obtain the required clinical information. The researchers evaluated the patients by measuring their blood pressure and implementing face-to-face interviews as the patients awaited their follow-up visits. There were no monetary rewards. Interviews were conducted using a structured questionnaire that took between 15 and 30 minutes, depending on the cooperation levels of the patient. In order to make the interview process understandable and consistent, a pilot study was carried out using 15 patients with similar characteristics to the study sample. The pilot study confirmed that the questionnaire and interview procedure were comprehensible and did not require any adjustments.
Instruments
A structured three-part questionnaire guided the interviews that used to collect data. Part one included questions related to sociodemographic factors (eg, age and sex) and clinical variables (eg, past medical history and body mass index). Patients were also asked whether they had ever received recommendations regarding self-care activities and health behaviors for managing hypertension. Part II included a translated Arabic version of the Hypertension-Self-care Activity Level Effects (H-SCALE) developed by Warren-Findlow and Seymour (2011).20
The H-SCALE is a self-report tool designed to assess adherence to recommended self-care activities and examine the relationship between adherence levels and blood pressure control.20 It consists of 30 items across six subscales: medication adherence, dietary practices, physical activity, smoking, weight management, and alcohol consumption. Each subscale contains a different number of items and is scored based on how many days in the past week the participant engaged in the respective behavior—except for weight management, which assesses agreement with weight-related behaviors over the past 30 days using a 5-point Likert scale, with scores converted for analysis. To reflect local context, culturally appropriate response options were added to the alcohol consumption and low-salt subscales; Appendix 1 contains the complete set of adapted items. The total H-SCALE score obtained by summing the scores across all subscales, with higher scores indicating healthier behaviors. An expert panel reviewed the validity of the instrument, and reliability (Cronbach’s alpha) was satisfactory across all domains: medication usage (a =0.93), physical activity (a =. 82), low-salt diet (a =0.71), and weight management (a =0.90).20,21
Part III covered an Arabic translation of the Perceived Self-Efficacy Scale developed by Warren-Findlow et al (2012) and used to measure the confidence of the participants in terms of their ability to control high blood pressure.22 The scale measures self-efficacy in respect of regular BP management, seeking healthcare when BP varies, participating in appropriate activities, alleviating emotional distress, and doing more than that of taking medications. Minor wording adjustment was done using the term high blood pressure instead of the word disease. Responses were evaluated with a scale ranging between 0 (not at all confident) and 10 (totally confident) and the higher total score suggests a higher perceived self-efficacy level. The scale has acceptable internal consistency among hypertensive population (Cronbach’s a =0.81).22
Results
The study involved 234 patients. Three patients were excluded because of missing data, leaving 231 participants in the final sample. The average age of the participants was 49.2 years (SD = 13.4) with a range of 30 to 89 years. Of them 55.4% were male, and 72.7% were married. Two-thirds were living in cities (64.1) and with their own families (95.2%). Approximately 44% had a bachelor’s degree, 10% had higher degrees and almost 65% were working. The mean gross monthly income (GMI) reported was 485 JD (SD = 230), with range 150 to 1200 JD, but only 19.5% respondents stated that their gross monthly income was adequate. Over two out of three respondents had chronic hypertension (more than six months), but only 32% of them reported having their blood pressure checked recently. In total, 68% of the participants had comorbid conditions, of them 42% had diabetes mellitus. Additionally, 56.3% were smokers. Body mass index (BMI) was a mean 28.3 (SD = 4.5), which shows that the participants were overweight. Almost 41% reported a history of surgery. The sociodemographic and clinical characteristics of the participants are presented in Table 1.
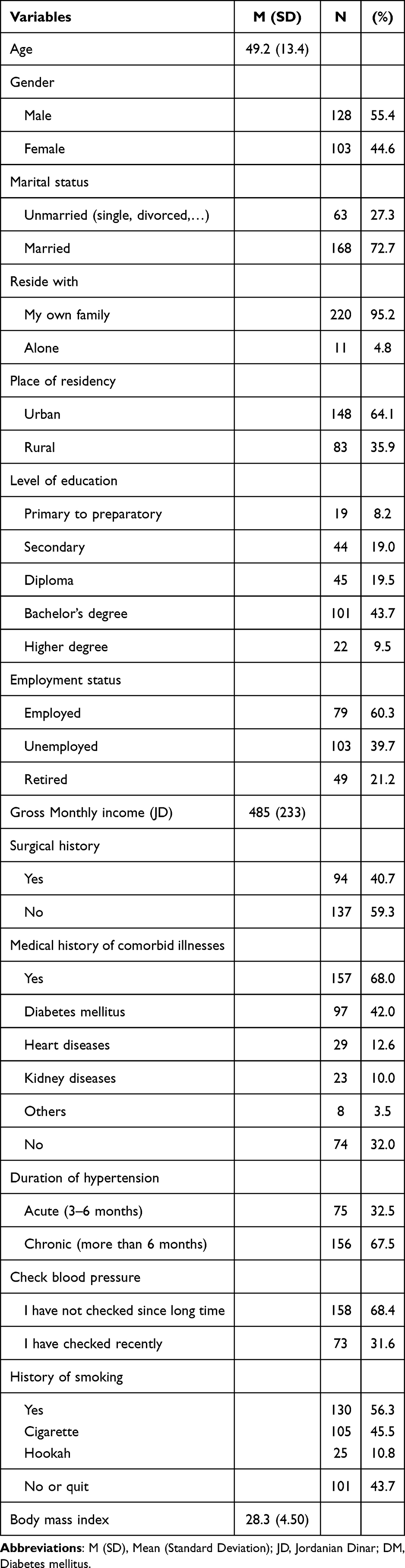 |
Table 1 Characteristics of the Study Participants (N= 209) |
Prevalence of Recommended Self-Care Behaviors
The Hypertension Self-Care Activity Level Effects (H-SCALE) summary score (30 items) had a mean of 40.7 (SD = 9.1; range: 17.82–62.8), indicating a low level of recommended healthy behaviors for controlling hypertension. Significant differences in the overall H-SCALE summary score were found based on gender, with female participants demonstrating significantly higher scores than males (t(229) = −4.28, p <0.001). Figure 1 illustrates these gender-based differences in the overall H-SCALE summary scores.
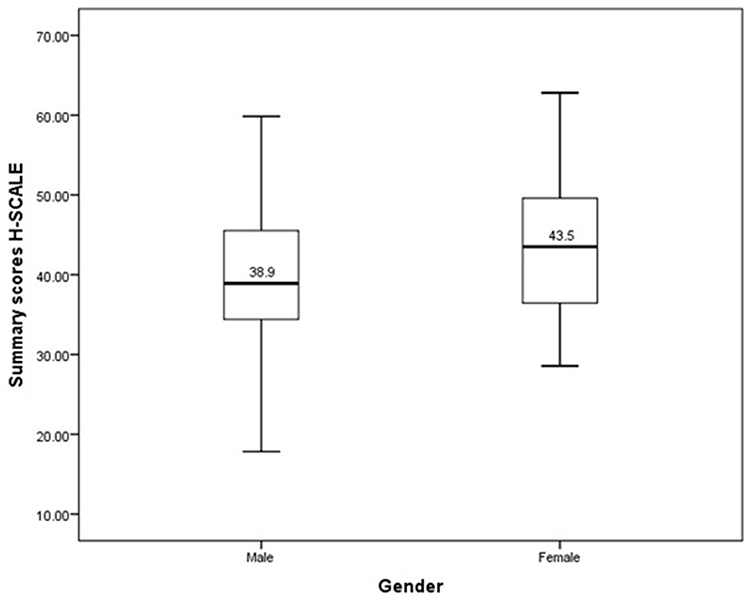 |
Figure 1 The overall H-SCALE summary scores based on gender. |
Regardless of gender, participants also showed significant differences in H-SCALE scores based on the duration since hypertension diagnosis. Those diagnosed more than six months ago exhibited significantly higher levels of recommended self-care behaviors (t(229) = −4.13, p <0.001; χ2(222) = 286, p =0.003). A one-way ANOVA also revealed statistically significant differences in mean H-SCALE scores among the five educational level groups (F(4, 226) = 2.48, p =0.045). However, Scheffé post-hoc tests showed no significant differences in the mean scores between any specific educational groups.
Table 2 presents the overall H-SCALE summary score along with mean scores for each of its six subscales. Across all six subscales, low levels of recommended healthy behaviors were observed, regardless of gender. Four subscales showed significant gender differences, and female participants generally scoring higher in recommended behaviors, except for the smoking subscale, where males scored higher.
 |
Table 2 Overall Summary Score for the H-SCALE and the 6 Subscales Scores with Comparison Based on Gender |
Levels of Self-Efficacy
The total self-efficacy scale score (based on five items) had a mean of 16.6 (SD = 12.2; range: 0.0–45), indicating a low level of self-efficacy among the study participants. A significant difference in mean self-efficacy scores was found based on gender (t(229) = −5.23, p <0.001), with female patients reporting significantly higher self-efficacy (M = 21.0, SD = 12.8) compared to male participants (M = 13.1, SD = 10.4). Additionally, significant differences were observed based on the duration since hypertension diagnosis (t(229) = −5.29, p <0.001), with patients who had chronic hypertension demonstrating higher self-efficacy (M = 19.4, SD = 11.9) than those recently diagnosed (M = 10.8, SD = 10.7). Figure 2 illustrates the overall mean self-efficacy scores by gender and duration since diagnosis.
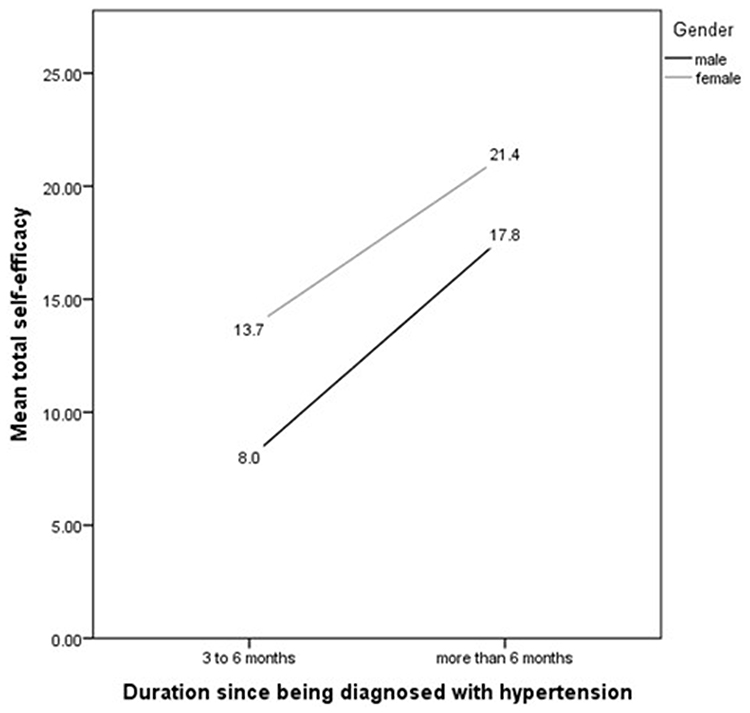 |
Figure 2 Self-efficacy scores by gender and hypertension duration (values shown as data labels). |
Correlates and Predictors of Self-Care Behaviors and Self-Efficacy
Table 3 presents the results of bivariate correlation analyses examining associations between H-SCALE, Self-Efficacy Scale scores, and participants’ demographics and clinical characteristics. Both scales were significantly correlated with age (H-SCALE: r = –0.15, p =0.030; Self-Efficacy: r = –0.34, p <0.001), gender (r = –0.24, p <0.001; r = –0.31, p <0.001), employment status (r = –0.19, p =0.003; r = –0.21, p =0.001), and duration since hypertension diagnosis (r = –0.21, p =0.001; r = –0.37, p <0.001). Marital status was significantly correlated only with H-SCALE (r =0.21, p =0.001). Married participants reported higher levels of recommended healthy behaviors (H-SCALE) compared to unmarried participants. Higher levels of recommended healthy behaviors and self-efficacy were also reported by female participants, those who were younger, employed, and had chronic hypertension. H-SCALE and self-efficacy scores were positively correlated (r =0.386, p <0.001).
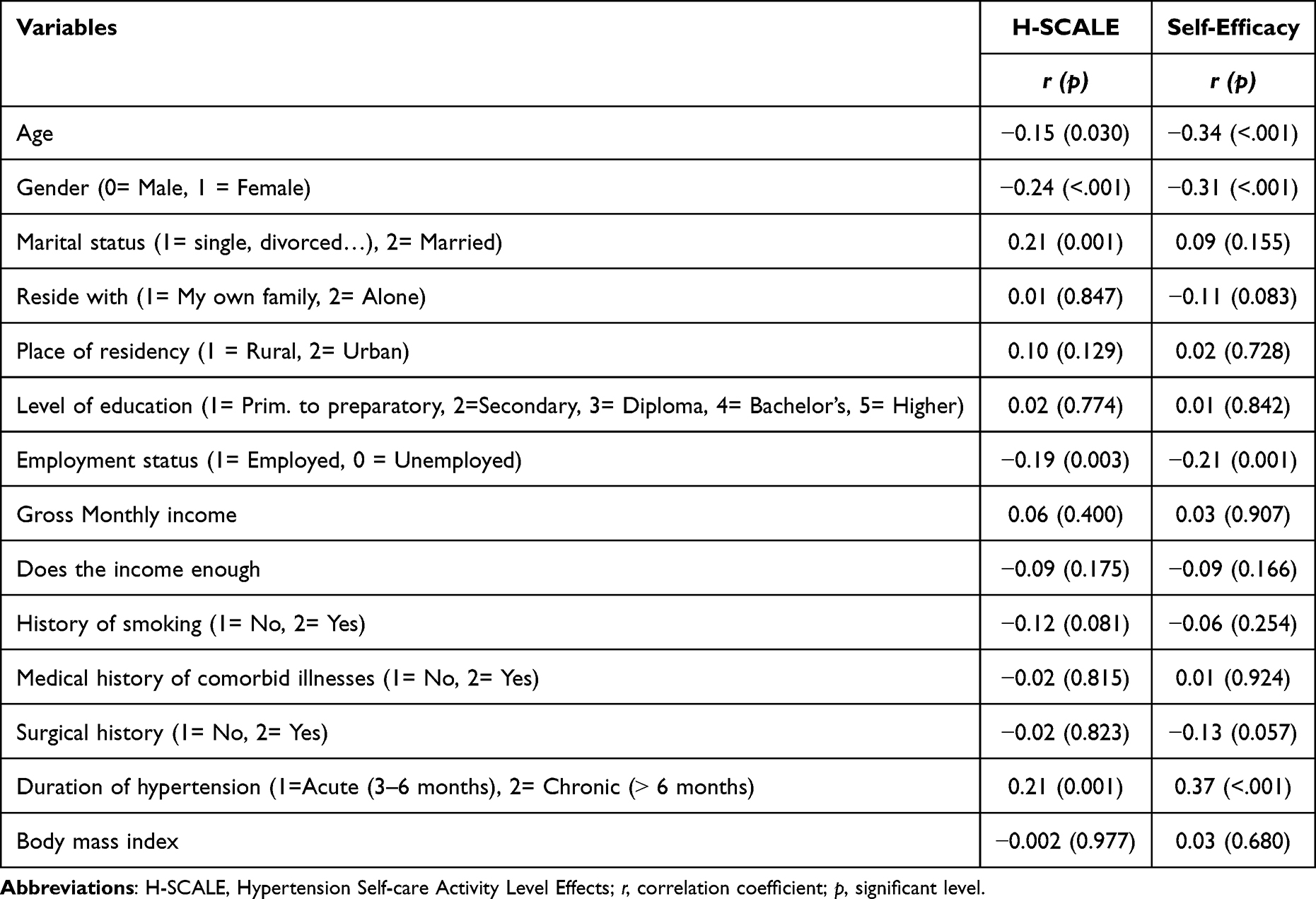 |
Table 3 The Correlation Between the Overall H-SCALE, Self-Efficacy Summary Scores and Participants’ Demographics and Clinical Characteristics (N= 231) |
Two-step hierarchical regression analyses were conducted to predict recommended healthy behaviors and self-efficacy based on demographic and clinical characteristics. Predictors included gender, age, education, marital status, residence, living arrangement, smoking history, employment, income, income adequacy, and clinical factors such as duration of hypertension, history of comorbidities, and medication adherence. Distributions were approximately normal with no extreme outliers. Regression assumptions were met, including tests for linearity, homoscedasticity, multicollinearity, and residual normality. All 231 participants were included in the analysis. Predictors included gender, age, education, marital status, residence, living arrangement, smoking history, employment, income, income adequacy, and clinical factors such as duration of hypertension, history of comorbidities, and medication adherence. Relevant categorical variables were dummy-coded by the researcher prior to the analysis.
The set of demographic characteristics was included as control variables in Block I, based on guidance from the available literature. This order of entry was chosen to account for factors not directly related to the disease process of hypertension. After adjusting for the effects of sociodemographic characteristics, clinical variables were entered next into each model. In addition to the default statistics, partial correlations for each predictor variable were requested. Table 4 summarizes the regression results for H-SCALE, while Table 5 presents the results for self-efficacy.
 |
Table 4 Multiple Hierarchal Regression of H-SCALE Levels on Demographics, and Clinical Characteristics |
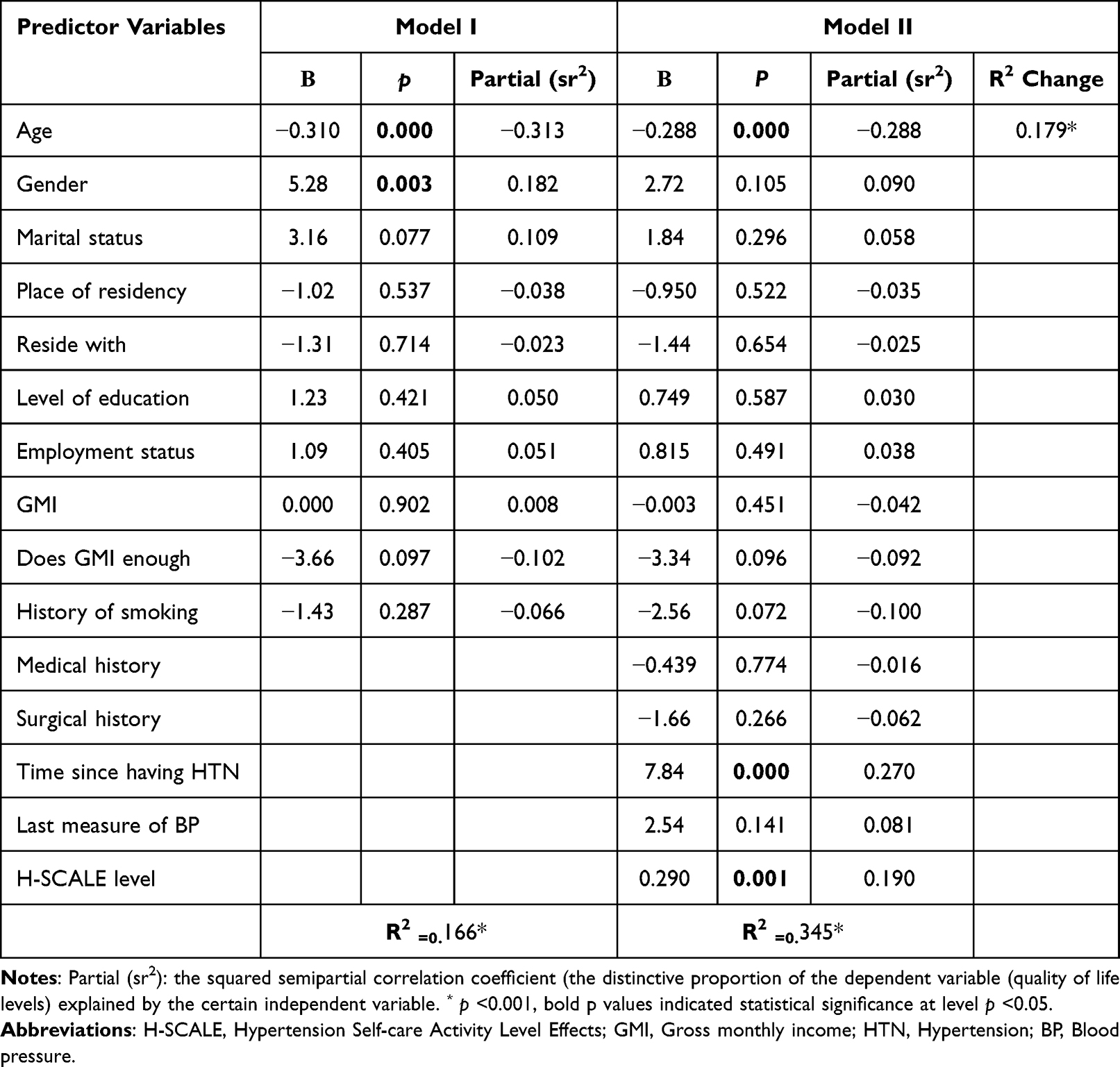 |
Table 5 Multiple Hierarchal Regression of Self-Efficacy Levels on Demographics, and Clinical Characteristics |
In the regression predicting H-SCALE scores, the model including all 10 demographic predictors was statistically significant. Demographic characteristics alone explained 14.4% of the variance in levels of recommended healthy behaviors as measured by the H-SCALE (R =0.379, R2 =0.144, adjusted R2 =0.105, F(10, 220) = 3.69, p <0.001). H-SCALE levels were significantly predicted by gender (β = 4.57, p =0.001) and marital status (β = 3.04, p =0.025). The positive slope for gender indicates that being female was associated with higher H-SCALE scores. Conversely, the negative slope for marital status suggests that being married was associated with lower H-SCALE scores.
To assess the contribution of individual predictors, the t-ratios for the regression coefficients were examined at the step each variable entered the analysis. In Step 1, gender was statistically significant (t(220) = 3.36, p =0.001; sr2 =0.21), uniquely explaining about 21% of the variance in H-SCALE scores. Thus, in this sample and within this set of predictors, gender emerged as the strongest individual predictor of H-SCALE levels.
After adjusting for the effects of sociodemographic characteristics, clinical variables were entered into the model, leading to an increase in the variance explained. For the H-SCALE, the explained variance increased from 14.4% in Model I to 27.7% in Model II (R =0.527, R2 =0.277, adjusted R2 =0.277, F(10, 220) = 4.81, p <0.001). The change in R2 from Model I to Model II was statistically significant (ΔR2 =0.107, F(15, 215) = 5.50, p <0.001).
In Model II, gender and marital status remained significant among the demographic predictors. Two clinical variables—time since being diagnosed with hypertension and self-efficacy levels—also emerged as significant predictors of H-SCALE scores. A positive slope for time since diagnosis indicated that having hypertension for more than six months was associated with higher H-SCALE scores, as was having a higher level of self-efficacy.
Other variables were not significantly related to H-SCALE levels, and when statistically controlled, their partial slopes were non-significant. Overall, H-SCALE levels were predictable from this set of predictors, with the strongest unique contributions coming from time since diagnosis (t(220) = 3.23, p <0.001; sr2 =0.187) and marital status (t(220) = −3.35, p =0.001; sr2 =0.194). Together, these two sets of variables uniquely explained about 38% of the variance in H-SCALE scores. Table 4 presents the standardized regression coefficients and squared semi-partial correlations (sr2) for each predictor in the model.
In the regression predicting self-efficacy, the model including all 10 demographic predictors was statistically significant. Demographic characteristics explained 16.6% of the variance in self-efficacy levels (R =0.408, R2 =0.166, adjusted R2 =0.128, F(10, 220) = 4.39, p <0.001). Self-efficacy levels were significantly predicted by gender (β = 5.28, p =0.003), marital status (β = 3.16, p =0.001), and age (β = −0.310, p <0.001). The positive slopes for gender and marital status indicate that being female and married were associated with higher self-efficacy scores. Conversely, the negative slope for age suggests that older age was associated with lower self-efficacy levels. To assess the contribution of individual predictors, the t-ratios for the regression coefficients were examined when each variable first entered the analysis. In Step 1, age was statistically significant (t(220) = −5.09, p <0.001; sr2 =0.313), uniquely explaining approximately 31% of the variance in self-efficacy. Thus, in this sample and within this set of predictors, age emerged as the strongest predictor of self-efficacy levels.
After adjusting for the effects of sociodemographic characteristics, clinical variables were entered into the model, resulting in an increase in explained variance. The variance explained increased from 16.6% in Model I to 35.4% in Model II (R =0.587, R2 =0.354, adjusted R2 =0.299, F(10, 220) = 7.55, p <0.001). The R2 change from Model I to Model II was statistically significant (ΔR2 =0.179, F(15, 215) = 11.37, p <0.001). In Model II, among the demographic variables, only age remained a significant predictor. Two clinical variables, namely, since being diagnosed with hypertension and H-SCALE levels, also emerged as significant predictors of self-efficacy. A positive slope for time since diagnosis indicates that having hypertension for more than six months, along with higher H-SCALE scores, was associated with higher self-efficacy.
Other variables were not significantly related to self-efficacy, and their partial slopes were not significant when controlling for other predictors. Overall, self-efficacy was predictable from this set of variables, with the strongest unique contributions coming from time since diagnosis (t(220) = 4.88, p <0.001; sr2 =0.27) and age (t(220) = −5.21, p <0.001; sr2 =0.29). Together, these two variables uniquely explained about 56% of the variance in self-efficacy levels. Thus, in this sample and within this set of predictors, age and time since being diagnosed with hypertension were the strongest predictors of self-efficacy. Table 5 presents the standardized regression coefficients and squared semi-partial correlations (sr2) for each predictor in the two models.
Discussion
This cross-sectional study aimed to assess hypertension self-care activities and self-efficacy among predominantly middle-aged Jordanian patients, while also identifying their correlates and predictor variables. More than two-thirds of the participants had comorbidities such as diabetes mellitus and heart disease. The findings revealed that participants demonstrated low levels of recommended self-care activities for managing hypertension, along with low self-efficacy, as measured by all six subscales of the H-SCALE and self-efficacy tools. Notably, over half of the participants held a bachelor’s degree or higher.
Our findings are consistent with previous studies that assessed adherence to healthy lifestyle behaviors among Jordanian patients with hypertension.23,24 Such studies reported low level of adherence to recommended behaviors needed to control hypertension. Alefan and colleagues evaluated 1,000 adult Jordanian patients with hypertension, aged 18 years and above; results indicated that 23% were fully adherent to healthy lifestyle activities.23 Results also showed that 35% of participants were either illiterate or had completed primary school at most, while 34% had completed tertiary education. In our study, over half of the participants completed a bachelor’s degree or post studies. Yet, the level of education however showed no significant correlation with adherence to recommended self-care behaviors and did not emerge as a significant predictor. In addition, results of this study support previous studies that evaluated hypertension self-care activities among diverse populations, including patients from western, African, Asian, and north American cultures, using various measurement tools. Results of such studies indicated that, regardless of gender or ethnic group, patients showed low level of self-care activities when managing their hypertension disease.25–28
Risk factors for hypertension-related complications are serious and can be prevented. In the current study, the majority of participants reported to have had hypertension for more than six months. However, adherence to blood pressure measurement was low, even with comorbidities such as diabetes mellitus. Moreover, over half of the participants were smokers and were overweight based on their body mass index. These findings reinforce previous outcomes that identified hypertension as a major contributor to the global disease burden, given its high prevalence and strong association with morbidity and mortality in both developed and developing countries, including Jordan.6,23,29–31
Self-care activities are vital and play a key role in reducing the risk of hypertension-related complications.12 The level of self-care activities for managing hypertension was found to be associated with various sociodemographic and clinical characteristics, where higher levels were found among females, married individuals, younger participants, employed participants, and individuals with chronic hypertension. Gender differences with regards to self-care are consistent with previous research,23,32 which identified female gender as a significant predictor of greater engagement in healthy self-care behavior. Higher health-related concern by females may have contributed to this association. Other studies found no significant association between gender and adherence to hypertension management,33 possibly reflecting cultural differences between the studied populations. In the present study, younger patients exhibit higher levels of engagement in self-care activities, possibly due to higher level of health awareness and lower level of physical limitations. These findings are consistent with previous studies conducted among Saudi patients with hypertension, reporting that individuals under the age of 65 were more likely to adhere to a healthy diet compared to older adults.25,34 However, in contrast to our findings, Hu and colleagues conducted a study in 2013 and found that older patients demonstrated greater self-care practices.35
Married individuals and those who were employed showed higher level of self-care activities for managing hypertension. This may be related to increased social support, financial stability, better access to healthcare services, and enhanced ability to manage stress; such factors promote adherence to healthy self-care behaviors. These findings align with previous studies.23,25 However, the study conducted in Jordan by Alefan et al (2019) reported no association between marital status and gross monthly income with adherence to healthy self-care activities.23 Our study also found no statistically significant correlation between gross monthly income and self-care activities.
Patients with long-standing chronic hypertension are more likely to engage in recommended self-care activities, a finding that is also confirmed by this study. This may be due to several factors. Their accumulated experience and awareness enhanced their understanding of self-care importance. Routine practices enhance compliance with drugs, dietary, physical activities as well as coping with stress. Engagement in self-care behaviors was further reinforced by the desire to prevent complications and continuous assistance of healthcare providers. Here our findings are in line with earlier research.25,26
The positive relationship between self-efficacy and self-care of hypertension that was observed in our study reinforces the growing body of literature that has highlighted the significance of self-efficacy as a determinant of health behavior. Individuals with high self-efficacy scores were more involved in self-care practices which means that the belief in self-efficacy in managing their health can result in desirable behavioral outcomes such as adhering to medication, healthy diet, physical activity, and stress management. The result is consistent with the existing literature that self-efficacy is a major predictor of health-promoting behaviors.22,36 It is worth noting that Findlow et al (2012) found a significant association between improved self-efficacy and adherence to various self-care behaviors except for limiting alcohol intake,22 which can indicate that self-efficacy does not affect all domains similarly. Moreover, Tan et al (2021) conducted a systematic review and reported that 21 of 22 studies had a positive correlation between self-efficacy and self-care engagement in hypertensive patients.37 The consistency of the previous studies as well as the current study underscores the primary role of self-efficacy in promoting self-management and emphasizes the need to combine strategies to improve self-efficacy in the interventions to manage hypertension.
Higher self-efficacy was predicted not only among females and those more engaged in hypertension self-care, but also in younger individuals and those with chronic hypertension. This suggests that younger individuals are more confident in managing their condition. Younger participants demonstrate greater adaptability and confidence in managing their health. Chronic hypertension patients also have a higher chance of developing coping skills and knowledge over time and enhancing self-efficacy. Increased participation in self-management practices, including medication compliance, diet change, engaging in exercise, stress management was also associated with increased self-efficacy, as it was indicated through H-SCALE. Self-care behavior among hypertensive patients can be influenced by other factors including social expectations, family involvement in health decision making and the accessibility of healthcare services.
Social and healthcare factors play a major role in determining self-care practices of hypertension patients; and it applies in the Jordanian context. Jordan has social factors, such as, but not limited to the social acceptance of smoking, a sedentary lifestyle, and a high-fat, high-salt diet, which all have adverse outcomes. Other challenges in the healthcare system that may impede the development of self-efficacy may include the discontinuity of care in primary health centers and inconsistency of patient education.15 It is possible to increase consistent healthcare education through the national level by implementing digital health tools and promotion of education on the community level. They can be behavioral interventions, motivational interviewing, and mobile health applications.38–40It is equally important to strengthen the primary care services. In Jordan, the provision of these areas could contribute greatly to better hypertension control and patient outcomes. Physician-led interventions have been recommended to enhance patient-physician communication that has been reported to positively influence adherence to healthy diets and medication regimens.41,42 Hence, healthcare providers must consider and apply engaging strategies to encourage self-care behaviors and self-efficacy in patients with hypertension to improve outcomes and overall health.
Limitations
This study can only be characterized by its cross-sectional nature and the self-report questionnaire that was used to collect data during interviews, which hindered it in measuring any possible change over time and instead might have biased the results due to possible social desirability bias since patients would have given socially desirable responses. Though, the study introduced a variable in the evaluation of the frequency of monitoring blood pressure to partly overcome this shortcoming and provide some context on patient compliance. Such bias could be reduced in longitudinal studies in the future where other objective measures such as actual BP monitoring and records on medication refills are included. This research was also conducted in one governmental hospital in Jordan and does not include patients with communication problems and patients with severe comorbidities associated with hypertension. This can limit the generalizability of the findings to the whole Jordanian population (eg patients from the private hospitals, patients with serious hypertension-related complications). Lastly, the research evaluated various demographic and clinical factors that could influence self-care behaviors and self-efficacy. Nevertheless, additional pertinent variables, including psychological distress, health literacy, and access to care were not measured, and future research is needed. In spite of the limitations, the research finds a considerably low level of self-care and self-efficacy among the hypertensive patients in Jordan and also offers valuable information on the factors and predictors associated with them.
Conclusion
Jordanian patients who experienced hypertension had poor adherence to scheduled self-care activities to manage hypertension and low self-efficacy levels, which predisposes them to complications associated with hypertension, thus burdening the healthcare systems in Jordan. It is significant to improve self-efficacy and encourage recommended self-care practices, particularly in high-risk populations, such as males, single people, older adults, and patients with acute hypertension. Timely assessment, patient education, lifestyle counseling, and psychological support can also help to enhance the outcome and decrease healthcare costs. To measure the effectiveness of the following strategies and promote evidence-based practice, future longitudinal and intervention studies are necessary.
Abbreviations
SCAs, Self-care Activities; H-SCALE, Hypertension Self-care Activity Level Effects; SD, Standard Deviation; JD, Jordanian Dinar; DM, Diabetes Mellitus; GMI, Gross Monthly Income; HTN, Hypertension; BP, Blood Pressure; B, unstandardized regression coefficients; Sr2, squared semipartial correlation “unique” effect of independent variable.
Data Sharing Statement
Due to ethical restrictions, the data that related to the study findings are available only from the corresponding author upon reasonable request.
Informed Consent and Ethics Approval
The Institutional Review Board (IRB) in Al-Hussein / Salt Hospital and the Review Board in the Faculty of Medicine at Al Balqa Applied University approved this study. Before providing written informed consent, all the participants were thoroughly informed about the objectives of the study. They were told that their involvement was voluntary and that the information they give would help in enhancing their care and it will not have any effects on their care. It was also explained to the participants that they had the option of skipping any question or dropping out of the study at will. The responses would be confidential and only accessible to the researchers. To ensure the confidentiality, it was necessary to assign each patient a code number. All data was safely kept and used only during research. The study complies with the principles of the Declaration of Helsinki.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest associated with this publication.
References
1. World Health Organization. Hypertension. Geneva: WHO; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension.
2. Forouzanfar MH, Afshin A, Alexander L, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1659–1724.
3. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–450. doi:10.1161/CIRCULATIONAHA.115.018912
4. Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360(9343):1347–1360. doi:10.1016/S0140-6736(02)11403-6
5. Ibrahim MM. Hypertension in developing countries: a major challenge for the future. Curr Hypertens Rep. 2018;20(5):38. doi:10.1007/s11906-018-0839-1
6. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
7. Whelton PK, Carey RM, Aronow WS, et al. ACC/AHA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. Hypertension. 2018;71(6):e13–e115. doi:10.1161/HYP.0000000000000065
8. Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community. J Clin Hypertens. 2014;16(1):14–26. doi:10.1111/jch.12237
9. Dickinson HO, Mason JM, Nicolson DJ, et al. Lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials. J Hypertens. 2006;24(2):215–233. doi:10.1097/01.hjh.0000199800.72563.26
10. Weir MR, Dzau VJ, Gavras I, Bresnahan M, Gavras H. The role of the kidney in hypertension: a 1997 update. J Hypertens. 1997;15(6):545–559. doi:10.1097/00004872-199715050-00011
11. Khader YS, Batieha A, Jaddou H, El-Khateeb M, Ajlouni K. Hypertension in Jordan: prevalence, awareness, control, and its associated factors. Int J Hypertens. 2019;2019:3210617. doi:10.1155/2019/3210617
12. Sari EA, Mirwanti R, Herliani YK, Pratiwi SH. Self-care behavior based on knowledge of patients with hypertension: a cross-sectional study. Vasc Health Risk Manag. 2025;21:17–24. doi:10.2147/VHRM.S489688
13. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American heart association. Circulation. 2015;131(4):e29–e322. doi:10.1161/CIR.0000000000000152
14. World Health Organization. Noncommunicable Diseases Country Profiles 2018. Geneva: WHO; 2018.
15. Almomani BA, Al-Sheyab NA, Alomari MA, Al-Smadi AM, Alzoubi KH. Hypertension knowledge, awareness, and control among hypertensive patients in Jordan. Int J Hypertens. 2022;2022:1234567.
16. World Health Organization. Jordan: hypertension. Geneva: WHO; 2018. Available from: https://www.worldlifeexpectancy.com/jordan-hypertension.
17. World Health Organization (WHO). Noncommunicable Diseases. Available from: https://www.euro.who.int/__data/assets/pdf_file/0007/350278/Fact-sheet-SDG-NCD-FINAL-25-10-17.pdf.
18. Higher Council for Science & Technology. Defining scientific research priorities in jordan for the years 2011-2020. 2010. Available from: http://www.hcst.gov.jo/sites/default/files/defining_scientific_research_priorities_in.pdf.
19. IBM Corp. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp; 2012.
20. Warren-Findlow J, Seymour RB. Prevalence rates of hypertension self-care activities among African Americans. J Nat Med Assoc. 2011;103(6):503–512. [(0027-9684 (Print))]. doi:10.1016/S0027-9684(15)30365-5
21. Warren-Findlow J, Basalik DW, Dulin M, Tapp H, Kuhn L. Preliminary validation of the hypertension self-care activity level effects (H-SCALE) and clinical blood pressure among patients with hypertension. J Clin Hypertens. 2013;15(9):637–643. doi:10.1111/jch.12157
22. Warren-Findlow J, Seymour Rb Fau - brunner huber LR, Brunner Huber LR. The Association Between Self-Efficacy and Hypertension Self-Care Activities Among African American Adults. J Commun Health. 2012;37(1):15–24.
23. Alefan Q, Huwari D, Alshogran OY, Jarrah MI. Factors affecting hypertensive patients’ compliance with healthy lifestyle. Patient Prefer Adherence. 2019;13:577–585. doi:10.2147/ppa.s198446
24. Alhalaiqa F, Al-Nawafleh A, Batiha AM, Masa’deh R, Abd Al-Razek A. A descriptive study of adherence to lifestyle modification factors among hypertensive patients. Turk J Med Sci. 2017;47(1):273–281. doi:10.3906/sag-1508-18
25. Guo YJ, Hu XY, Ji HJ, et al. The status and predictors of self-care among older adults with hypertension in China using the Chinese version of self-care of hypertension inventory - A cross-sectional study. Nurs Open. 2022;9(2):1241–1261. doi:10.1002/nop2.1165
26. Hu H, Li G, Arao T. Prevalence rates of self-care behaviours and related factors in a rural hypertension population: a questionnaire survey. Int J Hypertens. 2013;2013:526949. doi:10.1155/2013/526949
27. Niriayo YL, Ibrahim S, Kassa TD, et al. Practice and predictors of self-care behaviours among ambulatory patients with hypertension in Ethiopia. PLoS One. 2019;14(6):e0218947. doi:10.1371/journal.pone.0218947
28. Whelton PK, Carey RM, Aronow WS, et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018;71(6):1269–1324. doi:10.1161/hyp.0000000000000.
29. Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360(9343):1347–1360. doi:10.1016/S0140-6736(02)11403-6
30. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control. Circulation. 2016;134(6):441–450. doi:10.1161/CIRCULATIONAHA.115.018912
31. Mohsen Ibrahim M. Hypertension in developing countries: a major challenge for the future. Curr Hypertens Rep. 2018;20(5):38. doi:10.1007/s11906-018-0839-1
32. Kim Y, Kong KA. Do hypertensive individuals who are aware of their disease follow lifestyle recommendations better than those who are not aware? PLoS One. 2015;10(8):1368–1378.
33. Uzun S, Kara B, Yokuşoğlu M, Arslan F, Yılmaz MB, Karaeren H. The assessment of adherence of hypertensive individuals to treatment and lifestyle change recommendations. Anadolu Kardiyol Derg. 2009;9(2):102–109.
34. Elbur AI. Level of adherence to lifestyle changes and medications among male hypertensive patients in two hospitals in Taif; Kingdom of Saudi Arabia. Int J Pharm Pharm Sci. 2015;7(4):168–172.
35. Hu H, Li G, Arao T. Prevalence rates of self-care behaviours and related factors in a rural hypertension population: a questionnaire survey. Int J Hypertens. 2013;2013:526949. doi:10.1155/2013/526949
36. Du S, Yuan C. Evaluation of patient self-management outcomes in health care: a systematic review. Inter Nurs Rev. 2010;57(2):159–167. [1466-7657 (Electronic)]. doi:10.1111/j.1466-7657.2009.00794.x
37. Tan FCJH, Oka P, Dambha-Miller H, Tan NC. The association between self-efficacy and self-care in essential hypertension: a systematic review. BMC Fam Pract. 2021;22(1):44. doi:10.1186/s12875-021-01391-2
38. Zullig LL, Bosworth HB. Behavioral interventions to improve hypertension control in the Veterans Affairs healthcare system. J Clin Hypertens. 2014;16(11):827–837. doi:10.1111/jch.12423
39. Bischof G, Bischof A, Rumpf HJ. Motivational interviewing: an evidence-based approach for use in medical practice. Dtsch Arztebl Int. 2021;118(7):109–115. doi:10.3238/arztebl.m2021.0014
40. Morawski K, Ghazinouri R, Krumme A, et al. Association of a smartphone application with medication adherence and blood pressure control: the MedISAFE-BP randomized clinical trial. JAMA Intern Med. 2018;178(6):802–809. doi:10.1001/jamainternmed.2018.0447
41. Khairy S, Aslan A, Samara AM, et al. Factors associated with self-efficacy in patients with hypertension: a cross-sectional study from palestine. J Health Popul Nutr. 2021;40(1). doi:10.1186/s41043-021-00225-2
42. Ozoemena EL, Iweama CN, Agbaje OS, et al. Effects of a health education intervention on hypertension-related knowledge, prevention and self-care practices in Nigerian retirees: a quasi-experimental study. Arch Public Health. 2019;77(1):1–16. doi:10.1186/s13690-019-0349-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.