")
Back to Journals » Open Access Emergency Medicine » Volume 11
Self-administered alcohol enema causing chemical proctocolitis
Authors Seki T, Fukushima H
Received 10 March 2019
Accepted for publication 10 May 2019
Published 11 June 2019 Volume 2019:11 Pages 129—132
DOI https://doi.org/10.2147/OAEM.S208214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Tadahiko Seki,1 Hidetada Fukushima2
1Department of Emergency and Critical Care Medicine, Nara Prefecture General Medical Center, Nara, Japan; 2Department of Emergency and Critical Care Medicine, Nara Medical University, Nara, Japan
Background: There are few reports of chemical proctocolitis induced by transanal administration of alcohol.
Case report: The patient was a 21-year-old male with no medical history. He transanally pumped 1.8 L of 35% alcohol, experienced melena and disturbance of consciousness, and was transported by ambulance to our hospital. Abdominal computed tomography and endoscopy findings indicated ischemic colitis. He was administered conservative treatment and discharged after 9 days of hospital stay.
Conclusion: Reports on alcohol-induced chemical proctocolitis are rare. None of the reported cases involved perforation or required surgery, and all were resolved with conservative therapy, as observed in the study patient.
Keywords: rectal administration, colonoscopy, ischemic colitis, conservative therapy
Introduction
Orally ingested alcohol does not cause damage to the upper gastrointestinal tract. However, in an animal experiment, mucosa of the rat colon was damaged with 10% alcohol.1 Here, we report the case of a patient who experienced extensive chemical proctocolitis by transanally administering a large quantity of 35% alcohol, with a review on the clinical course of previous reports.
Case report
A 21-year-old male with no medical history was found lying on the bathroom floor in his home by his family who called an ambulance and had him transported to our hospital. On arrival, he experienced disturbance of consciousness with Glasgow Coma Score 6 (eye, verbal, motor responses: E2V1M3), pulse 101/min, blood pressure 118/66 mmHg, respiratory rate 18 respirations/min, and 35.5°C body temperature. He was not wearing clothing on his lower body, and a small quantity of melena was found from his anus. Blood tests revealed increased levels of white blood cells (23,900/μL) and hemoglobin (Hb) (17.5 g/dL). Blood gas analysis results were as follows: pH 7.299, bicarbonate (HCO3−) 19.9 mmol/L, base excess (BE) −6.0 mmol/L, and lactate 5.4 mmol, indicating metabolic acidosis and hyperlactacidemia. Results of drug toxicity screening (Triage® DOA) were negative. Brain CT revealed no intracranial hemorrhagic lesions. Non-contrast enhanced CT of the abdomen and pelvis disclosed thickening of the wall from ascending colon to the rectum (Figure 1).
 | Figure 1 Wall thickening of the sigmoid colon and rectum. |
Development after admission: While we were preparing for further tests in the ICU to determine the cause of disturbance of consciousness (eg, acute poisoning by a substance that could not be detected with Triage® DOA or post-ictal disturbance), his level of consciousness gradually improved, and the patient declared that he used a manual siphon pump to inject 1.8 L of white distilled liquor (35% alcohol) into his anus. Thus, the cause of disturbance of consciousness was believed to be acute alcohol poisoning by anally administered alcohol. Because we were unable to measure blood alcohol levels at our hospital, we could not definitively diagnose the cause of disturbance of consciousness. A lower digestive tract endoscopy was performed to examine the edematous changes extending from the colon to the rectum on abdominal CT suspected to be caused by alcohol-induced chemical proctocolitis (Figure 2). Diffuse bleeding, mucosal edema, ulcer, and submucosal bleeding were found from the ascending colon to the rectum. There were no lesions in the mucosal surface of the ileum. Prednisolone (60 mg) was rectally administered. Although the increase in lactic acid levels was immediately improved by fluid therapy and was thought to be due to dehydration, not due to intestinal necrosis. The patient was administered conservative treatment as per the standard treatment for ischemic colitis (fluid therapy with fasting). By the second day of illness, melena disappeared. Lower digestive tract endoscopy on the seventh day of illness showed improved inflammation; hence, he was initiated on an oral diet. There was no recurrence of melena, and the patient was discharged on the ninth day. He was followed up by a nearby physician who noted no delayed onset complications such as intestinal stenosis at two months of follow up. During hospitalization, the patient was asked why he transanally administered alcohol. He responded that he was suffering from insomnia due to severe anxiety as he prepared for his university entrance examinations and learned on the internet about anally administering alcohol with a siphon pump as a method to quickly induce sleep.
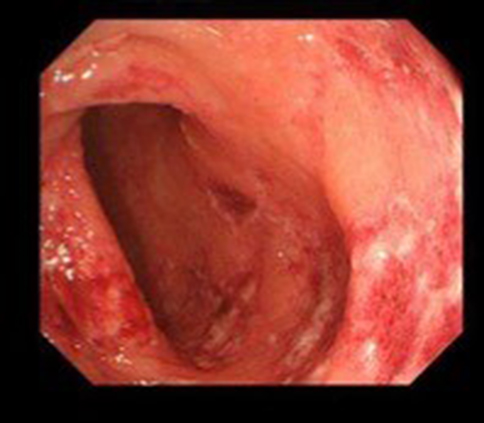 | Figure 2 Endoscopic view of transverse colon mucosa showing diffuse redness, erosion, ulcer, and hemorrhage. |
Discussion
To the best of our knowledge, there are only 13 reports, including this case, of chemical proctocolitis induced by transanally administered alcohol (Table 1).2–13 There are little is known about alcohol lesions in the colonic mucosa, compared from gastric mucosa. In a rat animal model, mucosa of the rat colon was damaged with 10% alcohol,1 and the histological appearance of acute lesions (10 mins after 30% ethanol enema) showed complete destruction of the surface epithelium. Necrosis extended throughout the depth of the mucosal layer but did not penetrate the muscularis mucosa. The mucosal injury in the colon also may be mediated by prostaglandin pathways, because intrarectal administration of prostaglandins decreases the damage.14 Previous reports listed the intention of suicide, sexual pleasure, and medical accidents as reasons for anally administering alcohol. Metabolism of ethanol begins as soon as it reaches gastric mucosa. Rectal absorption of ethanol bypasses the first pass metabolism, allowing for a higher systemic concentration of blood ethanol, greater potential for central nerve system depression. To feel alcohol effects quickly, alcohol enemas have been performed since ancient times, and pottery has been found representing that Mayan priests are injecting alcohol from the anus.15 In recent years, it has been noted as a dangerous alcohol intake method called “butt chugging” among university students in the USA.16 Clinical symptoms included melena, tenesmus, and burning sensation in the anus. Little abdominal pain has been reported, as observed in this patient who did not complain of abdominal pain. Colonoscopy findings showed diffuse redness, edema, bleeding, erosion, and ulcer of the intestinal mucosa, which were similar to the endoscopic findings of ischemic colitis.2–8 In this study case, moderate edematous changes were found in the ascending colon to the rectum, particularly in the transverse colon, as well as multiple lesions of submucosal bleeding and erosion. Histopathological findings showed sloughed epithelial cells, interstitial edema, capillary dilation, bleeding of the lamina propria and submucosa, and a nonspecific inflammatory response, which were also similar to those of ischemic colitis.5,8,11,12 In this case, since no pathological examination has been conducted, no histological evaluation could be obtained. Regarding the relationship between the concentration of alcohol in the injected fluid and the resulting damage, previous studies reported relatively good course with conservative therapy, even for a patient who injected 96% alcohol and required hospitalization for 7 days.6 Intestinal perforation and necrosis were not reported in any of the previous cases. This patient, who administered 35% alcohol, was discharged after 9 days of hospital stay with conservative therapy alone. In terms of the relationship between the volume of alcohol injected and extent of damage, 200 mL reached only the descending colon, whereas 1,000 mL caused damage in the transverse colon as well. This individual administered 1,800 mL, which was the highest quantity among the existing reports, and the damage was observed in the ascending colon. The extent of damage in alcohol-induced chemical proctocolitis depends on the quantity administered; however, clinical symptoms and course are similar to ischemic colitis and can be treated with conservative therapy.
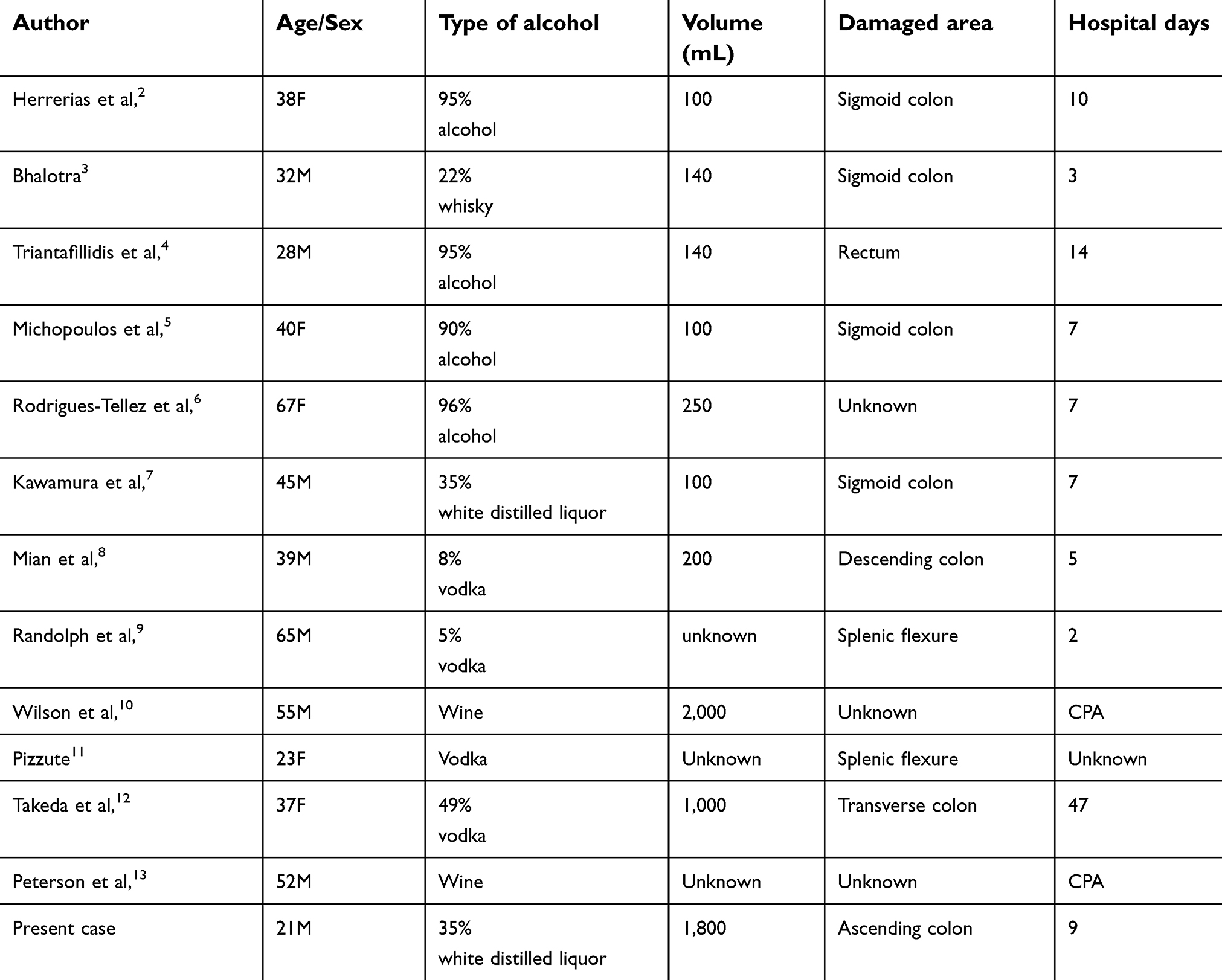 | Table 1 Clinical features of alcohol-induced proctitis |
Conclusions
We experienced a rare case of chemical proctocolitis induced by transanally administering alcohol. Clinical symptoms and course were similar to ischemic colitis.
Ethical statement
Written consent has been provided by the patient to have the case details and accompanying images published. Institutional approval was not required.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Esmaily H, Sanei Y, Asadi-Shamirzadi A, et al. Induction of inflammatory bowel disease through activation of immune system against enteric bacteria. J GHR. 2014;3:977–984.
2. Herrerias JM, Muniain MA, Sanchez S, Garrido M. Alcohol-induced colitis. Endscopy. 1983;15:121–122. doi:10.1055/s-2007-1021485
3. Bhalotra RJ. Alcohol-induced proctitis in a human. Clin Gastroenterol. 1988;10:592. doi:10.1097/00004836-198810000-00028
4. Triantafillidis JK, Vekini J, Nicolakis D, et al. Ethanol-induced proctitis: another kind of chemical proctitis. Am J Gatroenterol. 1994;89:1270–1271.
5. Michopoulos S, Bouzakis H, Sotiropoulou M, Papaspyrou I, Tsibouris P, Kralios N. Colitis due to accidental alcohol enema: clinicopathological presentation and outcome. Dig Dis Sci. 2000;45:1188–1191.
6. Rodriguez-Tellez M, Herrerias JM
7. Kawamura O, Sawada T, Hara T, et al. Chemical prctocolitis due to alcohol (Shochu) enema. Gastroenterol Endosc. 2002;4:1019–1022.
8. Mian SR, McFadden KL, Valenstein PN, Shehab TM. Self-administered alcohol(vodka) enema causing severe colitis: case report and review. Gastrointest Endosc. 2005;61:922–926.
9. Randolph M, Longacre TA, Gerson LB. Acute colitis secondary to self-administered alcohol enemas: a mimic of ischemic colitis. J Clin Gastroenterol. 2005;39:78–79.
10. Wilson CI, Ignacio SS, Wilson GA. An unusual form of fatal ethanol intoxication. J Forensic Sci. 2005;50:676–678.
11. Pizzute C. Self-administered alcohol (vodka) enema causing severe colitis: case report and review. Gastrotntest Endosc. 2006;63:1087–1088. doi:10.1016/j.gie.2006.01.019
12. Takeda M, Natori K, Moroi R, et al. Severe acute proctocolitis caused by a self-administered vodka enema. J Abdom Emerg Med. 2013;33:735–739.
13. Peterson T, Rentmeester L, Judge BS, Cohle SD, Jones JS. Self-administered ethanol enema causing accidental death. Case Rep Emerg Med. 2014;1–3. doi:10.1155/2014/191237
14. Wallace JL, Whittle BJR, Boughton-Smith NK. Prostaglandin protection of rat colonic mucosa from damage induced by ethanol. Dig Dis Sci. 1985;30:866–876. doi:10.1007/BF01309518
15. de Smet PA, Hellmuth NM. A multidisciplinary approach to ritual enema scenes on ancient Maya pottery. J Ethnopharmacol. 1986;16:213–262. doi:10.1016/0378-8741(86)90091-7
16. Johnson J Tennessee frat guys. The Washington Post. 2012 Sep 26. Available from:
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.