Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Sedentary Behavior Interventions in COPD: A Scoping Review of Strategies, Behavior Change Techniques, and Device-Measured Outcomes
Authors Fang P, Mu W, Song M, Wang H, Lyu F, Zhao R, Li M, Cao J, Li Y, Lou L, Qian F
Received 10 September 2025
Accepted for publication 3 March 2026
Published 13 March 2026 Volume 2026:21 566739
DOI https://doi.org/10.2147/COPD.S566739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Ping Fang,1 Weilan Mu,1 Meiying Song,1 Haitao Wang,2 Fangfei Lyu,1 Ruifeng Zhao,1 Manna Li,1 Jintao Cao,3 Yunchuan Li,1 Lanhua Lou,1 Feng’e Qian1
1School of Nursing, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 2Department of Orthopedics, The First Affiliated Hospital of Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 3Nursing Department, Huize County People’s Hospital, Qujing, Yunnan, People’s Republic of China
Correspondence: Feng’e Qian, School of Nursing, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China, Email [email protected]
Background: Sedentary behavior is an independent risk factor for disease progression and mortality in COPD patients. However, there is a lack of systematic research on its intervention strategies in China. We provide, in a domestic context, a scoping synthesis of this field that underscores the necessity for more robust and localized research.
Purpose: This scoping review aims to clarify the characteristics, effectiveness, and BCTs of sedentary behavior interventions for COPD patients.
Methods: Following the scoping review method proposed by Arksey. A comprehensive search was conducted across eight electronic databases, including PubMed, Embase, the Cochrane Library, Web of Science, CNKI, WanFang Data, CBM, and VIP. The search time frame encompassed records from the inception of each respective database up to August 20, 2025. The study selection, data extraction, and coding of the BCTs were all performed independently by two researchers.
Results: The 6 included studies (comprising 4 RCTs, one quasi-experimental, and one case-control study) were primarily conducted in China and Europe, with sample sizes ranging from 30 to 327 and intervention durations of 6 to 24 weeks. Four studies reported reduced sedentary time, while two found no statistically significant difference. Guided by the BCW, the interventions in four studies included components such as knowledge education, use of wearable devices, and Nordic walking. Applied BCTs (Goals and Planning, Feedback and Monitoring, etc) primarily targeted the COM-B components of Psychological Capability and Reflective Motivation.
Conclusion: The combined evidence suggests that most interventions reduce both total daily sedentary time and prolonged sitting bouts. However, the evidence base remains limited by regional concentration, short follow-ups, and heterogeneity.
Keywords: chronic obstructive pulmonary disease, sedentary behavior, intervention strategies, behavior change techniques, behavior change wheel, accelerometry
Introduction
Sedentary behavior was defined as any waking behavior characterized by an energy expenditure of ≤1.5 metabolic equivalents (METs) while in a sitting, reclining, or lying posture, not only increases the risk of overweight and obesity when practiced long-term but is also significantly associated with various chronic disease risks.1 Physical inactivity is defined as insufficient amounts of moderate-to-vigorous physical activity (ie, not meeting specified physical activity guidelines)2 Sedentary behavior not only has a high incidence in patients with chronic obstructive pulmonary disease (COPD), but also has been identified as an independent risk factor for the development of COPD. Related study showed that patients with COPD spend approximately 62.6% of the day in sedentary activities, which can significantly increase the risk of hospital readmission, acute exacerbation, and mortality among COPD patients, and can also be linked to a diminished quality of life.3 For COPD patients, some individual studies have reported large association estimates such as a 42% higher mortality risk per hour of increased sedentary time, but results vary across studies.4 The results of a systematic review showed that the sedentary time of COPD patients is about 447 minutes per day, which is far beyond the safe threshold and may exacerbate disease progression and increase the risk of complications.5 At present, foreign studies mainly focus on the relationship between sedentary behavior and chronic diseases such as cardiovascular disease and stroke, as well as aging-related biomarkers and mental health.6–8 In contrast, sedentary behavior, especially in the specific population of COPD patients, has been understudied. Guidelines suggest that replacing sedentary behavior with low-intensity or moderate-to-vigorous intensity physical activity reduces the risk of all-cause death.9 Given that the origin of this causal pathway lies in the behavior itself, effective interventions require precise targeting of its actionable levers. For example, “Breaking Persistent Sitting” can reverse metabolic inhibition through behavior shaping and cueing techniques; “Wearable device feedback” relies on self-monitoring technology to visualize abstract sedentary behavior to improve behavioral awareness; Motivational interviewing (MI) was used to maintain long-term change by resolving ambivalence and strengthening self-regulation. It can be seen that the above intervention strategies essentially rely on the identification, guidance and consolidation of individual behavior patterns, which is the core category of Behavior Change Techniques (BCTs). However, intervention studies in this field have small sample sizes, short follow-up periods, heterogeneity of intervention components, inconsistent reporting, and lack of standardized coding and theoretical correlates of BCTs. Because SB is usually not a planned activity but occurs in daily life, recalling daily amounts of sedentary time is difficult, and self-reported measures are often biased. Devices such as accelerometers and inclinometers have high accuracy, which can be used to objectively measure SB and are more accurate than self-report.10 Device data provide objective, continuous, and high-resolution behavioral records, which are particularly suited for quantifying key dimensions such as total sedentary time, prolonged sitting bouts, and breaks in sitting.
Based on the current evidence, the sedentary behavior of COPD patients can be viewed as a behavior pattern driven by a vicious cycle of “symptom-avoidance”: the core symptoms of the disease (such as dyspnea and physical decline) encourage patients to adopt activity avoidance strategies to avoid discomfort, which is directly manifested as prolonged sedentary time. In turn, prolonged sitting can exacerbate physical decline and dyspnea, creating a self-reinforcing loop. In addition, factors such as severity of illness, frequency of acute exacerbations, burden of comorbidities, and seasonal variation act as important moderators, which further modulate the strength of this cycle and the manifestation of sedentary behavior by influencing symptom burden and environmental conditions.11,12 In addition, there is a lack of description of the characteristics, effectiveness, and BCTs of the existing intervention strategies to reduce sedentary behavior in COPD patients. Therefore, this review uses behavior change as the core framework to explain the intervention strategies corresponding to sedentary time in COPD patients. The COM-B model believes that behavior change is the result of the interaction of Capability, Opportunity and Motivation, that is, the intervention for reducing sedentary behavior in COPD patients can be carried out from the above three aspects. Specifically, Physical and Psychological Capability, such as disease knowledge and self-monitoring skills; Physical and Social Opportunity, such as vibratory prompts from wearable devices and social support; and Reflective and Automatic Motivation, such as awareness of health consequences and the disruption of sedentary habits. Corresponding intervention functions include education, enablement, environmental restructuring, and training. Unlike previous intervention strategies that mainly focused on the number of steps or moderate-to-vigorous intensity physical activity (MVPA), the objective of this review is to systematically evaluate intervention strategies that affect sedentary behavior in patients with COPD and analyze their effects on sedentary time. Specifically, we will explore intervention types, BCTs, devices and metrics, and direction and consistency of effects. These interventions have clinically important implications for improving physical health and quality of life in patients with COPD by reducing prolonged sitting and increasing activity breaks.
Methods
This study follows the scope review method framework proposed by Arksey,13 and the specific implementation steps are as follows: (i)Clarify the research questions; (ii)Search relevant literature; (iii)Identification of included literatures; (iv)Data extraction; (v)Organize and analyze the data and report.
The specific research questions covered the following three aspects: (i)What are the specific intervention strategies for sedentary behavior in COPD patients, and what are their general characteristics? (ii)What are the main components of these intervention strategies? What BCTs do they employ? (iii)What are the actual effects of these intervention strategies?
Search Strategy
A comprehensive search was conducted in PubMed, Embase, Cochrane Library, Web of Science, CNKI, WanFang Data, CBM, and VIP databases. The search formula was constructed using subject headings plus free words and Boolean logic connectives. A citation tracing strategy was implemented to ensure the comprehensiveness of the search, and the search time spanned all relevant literature data up to August 20, 2025.See Table 1 for PubMed search strategy as an example.
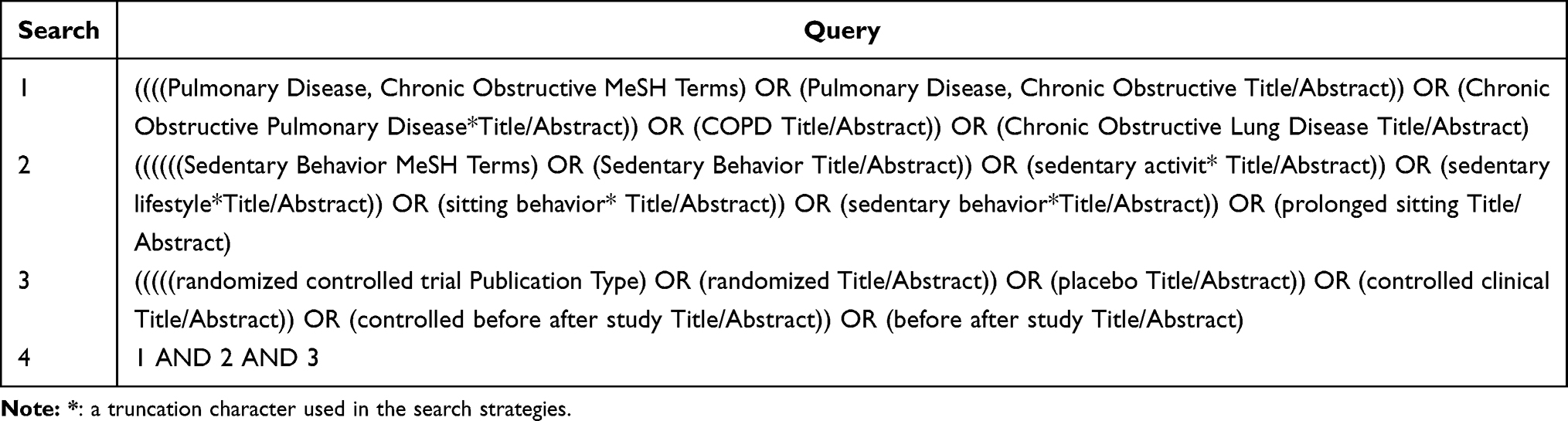 |
Table 1 Search Strategies of PubMed |
Eligibility Criteria
The inclusion criteria were (i) population:Patients who met the international diagnostic criteria for COPD, aged ≥18 years old. (ii) Intervention strategy: Any strategy to reduce or interrupt the occurrence of sedentary behavior in different Settings. (iii) Control: no limit. (iv) Outcome measures: included but were not limited to sedentary time, 6-minute walk distance, number of steps per day, exercise capacity, and walking time. (v) Study type: Intervention study (randomized controlled, before-after control).
The exclusion criteria were (i) No full-text literature was available in Non-Chinese or English or duplicate literature. (ii) Literature of the study protocol only. (iii) Meeting abstracts and reports that could not be extracted or had incomplete data.
Study Selection
Two independent researchers strictly used Endnote 21 software to screen the literature according to the established inclusion and exclusion criteria. By reading the title and abstract of the literature, after excluding the literature that obviously did not conform to the theme, the remaining literature was read in full for further screening. In case of disagreement during the screening process, consensus was reached through discussion or consultation with third-party experts to ensure the accuracy and consistency of the screening results.
Data Extraction and Charting
Data extraction was performed independently by two investigators, and in case of disagreement, a third investigator was consulted to reach consensus. Two coders independently extracted the text content describing the core components of the intervention from the full-text reports of all included studies, and coded the BCTs strictly according to BCTv1.We clarify that this study did not employ a statistical measure, such as Cohens kappa, to quantify inter-coder agreement. Furthermore, we have indicated that intervention components were systematically categorized by mapping them to the COM-B model. The extracted contents included: general information (such as author, publication time, country, etc), basic characteristics of the sample (such as sample size), intervention in the control group, description of intervention strategies in the intervention group (such as general characteristics of intervention strategies, specific content and BCTs used, etc), and outcome information (such as type of outcome and measurement time point). Descriptive analysis was used to analyze the extracted data in this study.
Results
Results of the Search
A total of 485 literatures were collected by preliminary searching database and citation tracing. After removing duplicate literatures, 317 literatures were left, and 314 literatures were left after further excluding literatures that could not obtain full text. By carefully reading the title, abstract, and full text of the remaining literature, 6 literatures were finally selected for inclusion,14–19 of which 4 English and 2 Chinese studies. The literature screening process is shown in Figure 1.
 |
Figure 1 PRISMA flow diagram of literature selection. |
Summarise and Report the Results
A total of 6 articles were included in this study, and the studies were conducted in 4 countries, including China, Germany, Austria, and Australia, showing the global attention and research on sedentary behavior intervention strategies. Most of them were randomized controlled trials (n=4), and the included studies were published from 2010 to 2024, and most of them were conducted after 2020 (n=5). The sample size ranged from 30 to 327. The basic characteristics of each literature are detailed in Table 2. Patterns for the intervention are presented in Table 3 and the device. Outcome measurements are presented in Table 4 and BCTs applied in the included 6 studies are presented in Table 5.
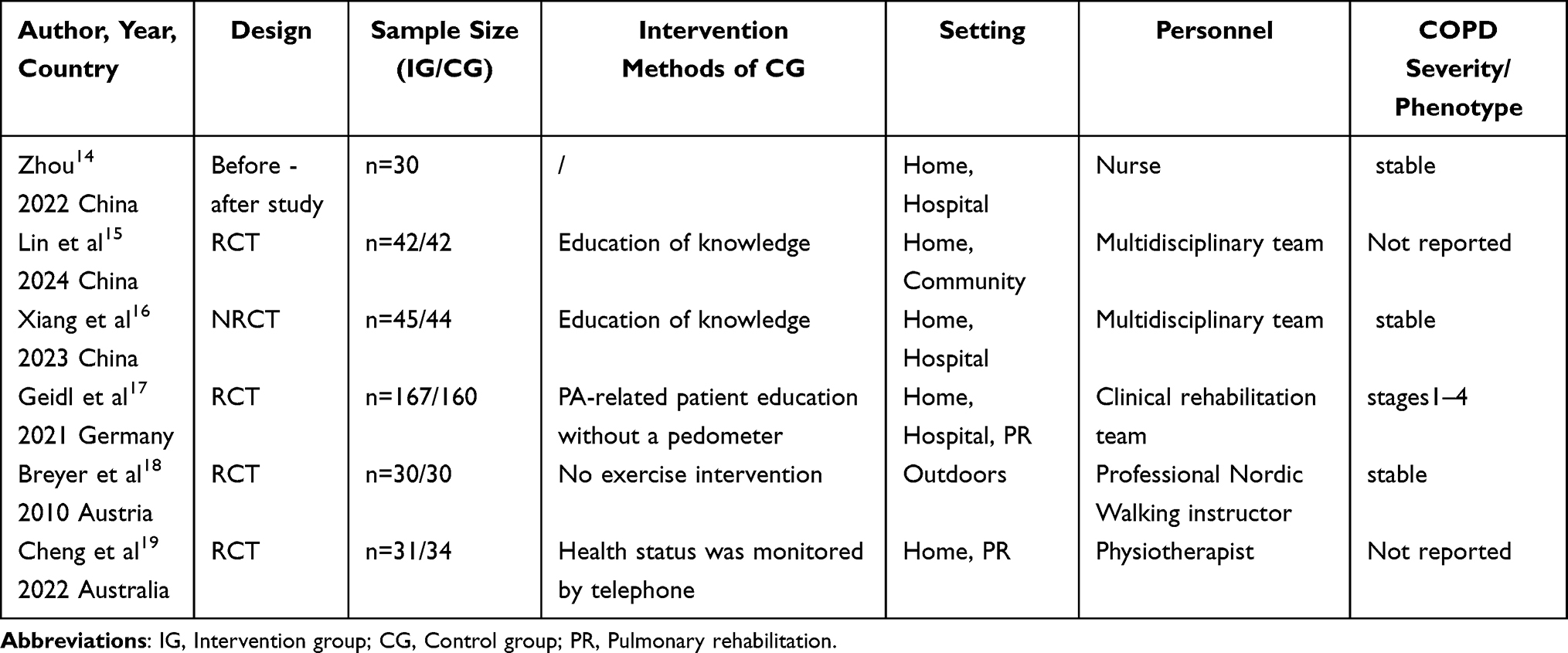 |
Table 2 Summary of Study Characteristics |
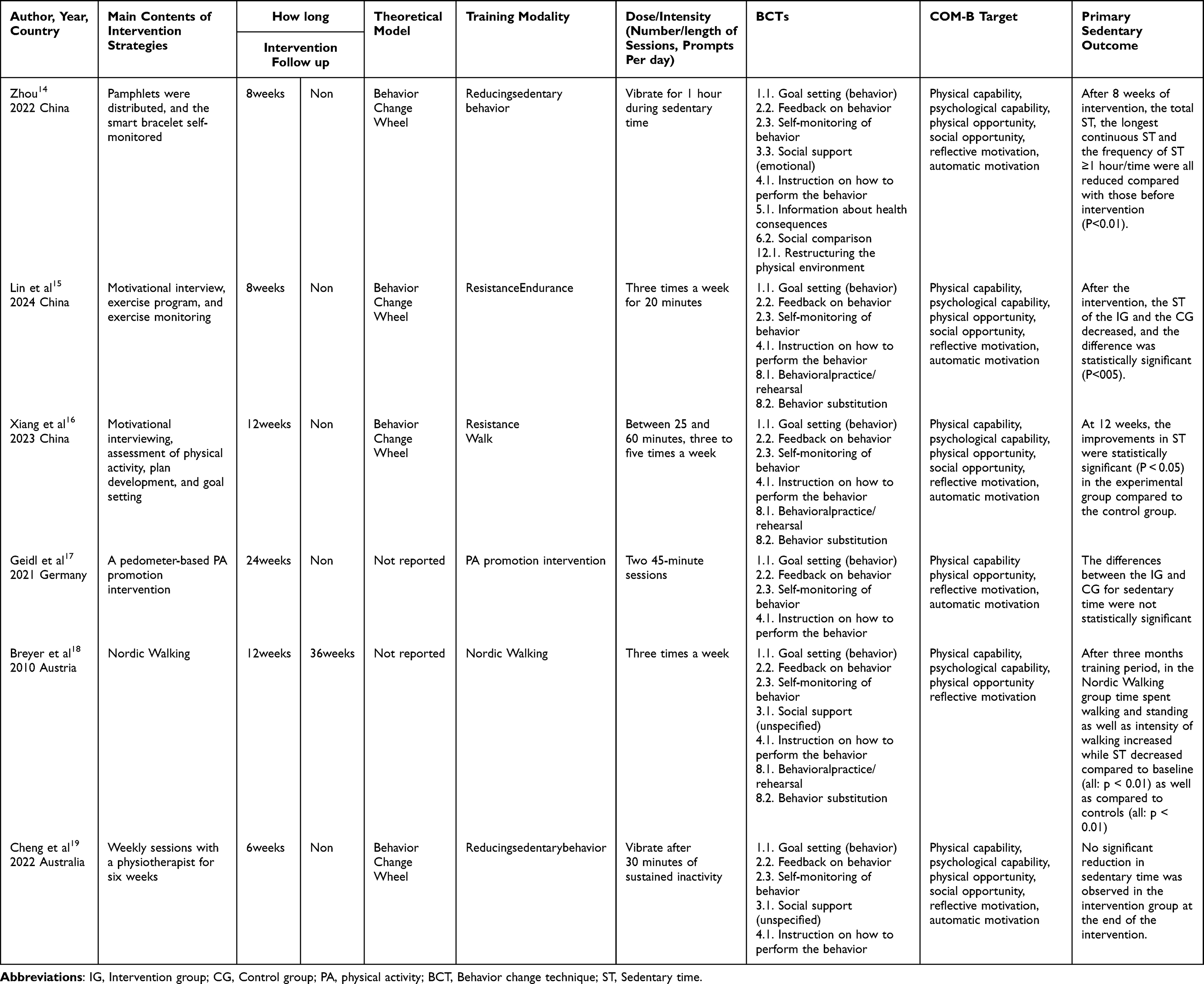 |
Table 3 Patterns for the Intervention |
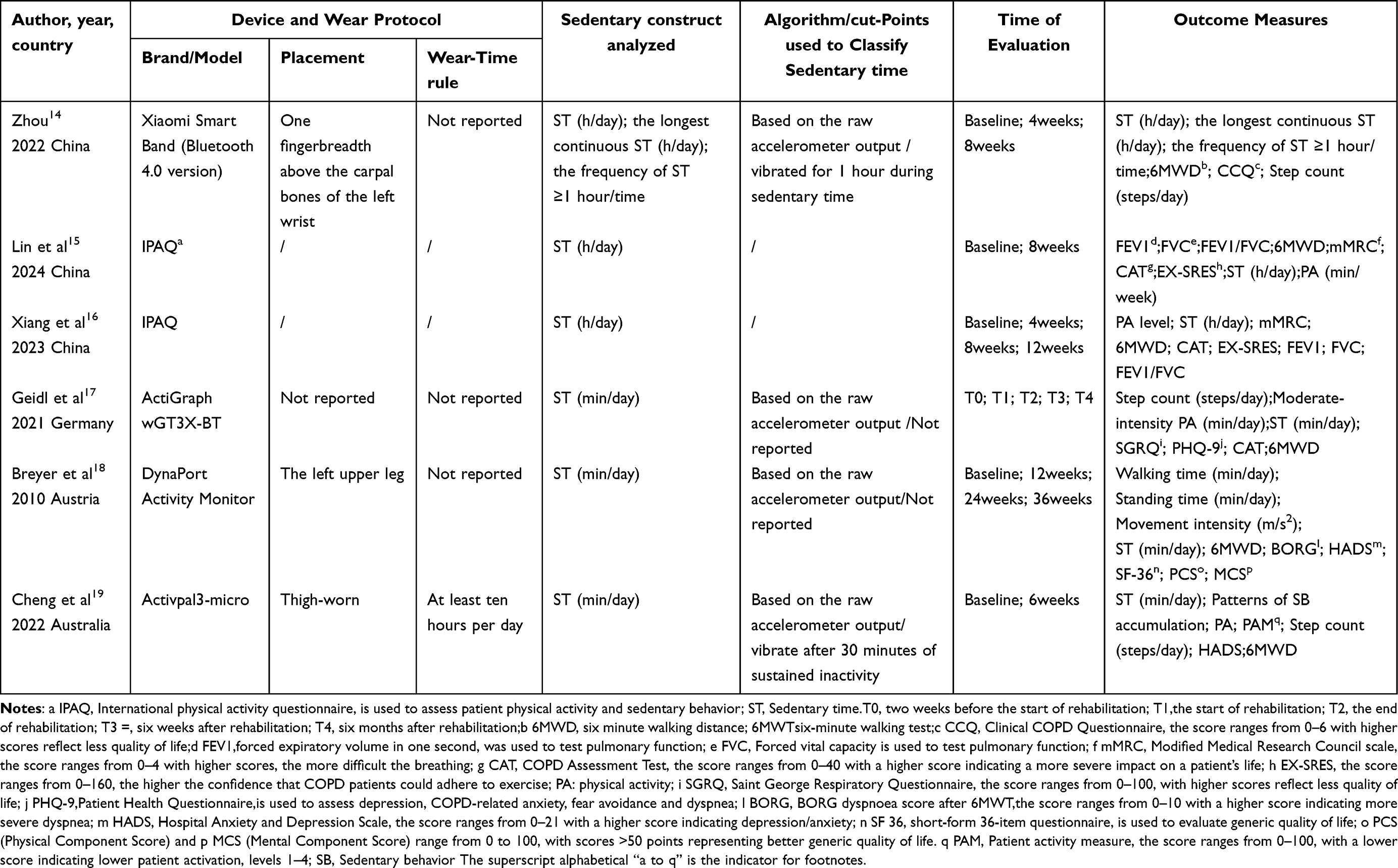 |
Table 4 Device and Outcome Measurements |
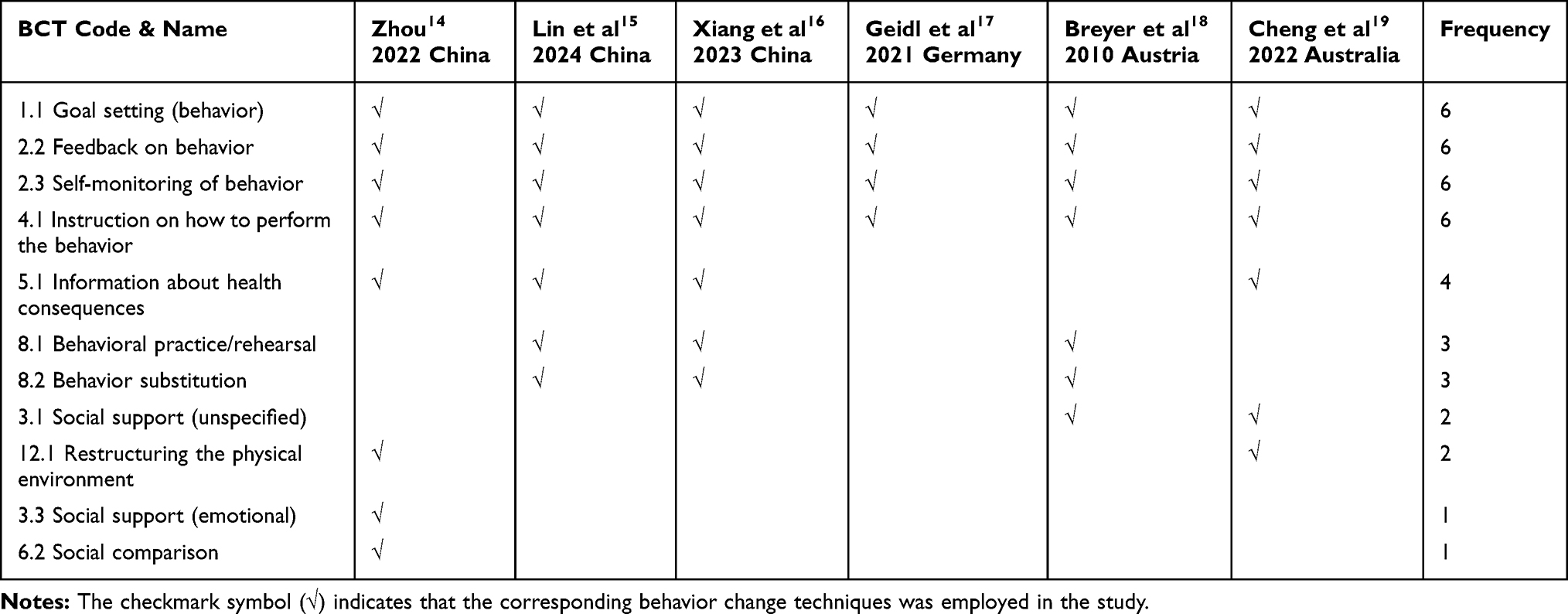 |
Table 5 Behavior Change Techniques Applied in the Included 6 Studies |
Characteristics and Contents of Intervention Strategies for Sedentary Behavior
This study showed that 4 studies14–16,19 clearly explained the theoretical names used in the sedentary behavior intervention strategies, and all of them were the Behavior Change Wheel (BCW) theory, which ensured the scientific nature and effectiveness of the intervention strategies. The duration of the intervention varied between studies and ranged from 6 weeks to 24 weeks. The interventions were mainly delivered by multidisciplinary teams (n = 2), physiotherapists (n = 1), nurses (n = 1), professional Nordic Walking instructor (n =1), clinical rehabilitation team (n =1). The interventions were primarily delivered as home-based (n=5). The sedentary behavior metrics analyzed were primarily assessed using accelerometers (n=3) and questionnaires (n=2). The evaluation outcome indicators of the articles were diverse, and the evaluation indicators of each study included sedentary time, and the evaluation time was diverse, including 2 to 4 time points. In the study of Breyer et al, although the intervention time was three months, the evaluation time included 6 months and 9 months, aiming to evaluate the long-term effect of Nordic walking exercise on improving sedentary behavior of patients with chronic obstructive pulmonary disease18 The intervention contents were diversified, including the construction of intervention program based on the ability, opportunity, and motivation of BCW theory, the use of wearable devices, and Nordic walking exercise.
Behavior Change Techniques Used in Sedentary Behavior Intervention Strategies
Sedentary behavior interventions incorporated a variety of BCTs. Within the established taxonomy of 93 potential BCTs,20 the following were most commonly applied across the included studies: Goal setting (behavior)(1.1), Feedback on behavior (2.2) Self-monitoring of behavior (2.3) and instruction on how to perform the behavior (4.1) were each utilized in all six studies.14–19 Information about health consequences (5.1) was also frequently included, appearing in four studies.14–16,19 The techniques of Repetition and substitution (8.1/8.2) were employed in three studies.15,16,18 Social support (unspecified) (3.1)18,19 and Restructuring the physical environment (12.1)14,19 were each used twice, while Social support (emotional) (3.3)14 and Social comparison (6.2)14 were applied only once. Notably, Goal setting (behavior)(1.1), Feedback on behavior (2.2) Self-monitoring of behavior (2.3) and instruction on how to perform the behavior (4.1) were consistently implemented together, forming a core combination of BCTs that appeared in all the included studies.14–19 This pattern suggests that an integrated approach combining education, self-regulation, and feedback is considered foundational in designing interventions aimed at reducing sedentary behavior in this population.
Effects of Intervention Strategies for Sedentary Behavior
The six articles included in this study all reported that the sedentary time of patients decreased after the intervention compared with that before the intervention. Although the 6-week study by Cheng et al did not show a significant difference in sedentary time between groups, the intervention group demonstrated an increase of 2,037 steps and more time in moderate-to-vigorous physical activity (MVPA) compared to the control group after the intervention19 This suggests that the behavior change strategies may have been more effective in replacing sedentary behavior with stepping rather than simply increasing standing time or breaking up prolonged sitting. Similarly, adding a brief behavioral intervention with a pedometer to the German standard three-week inpatient pulmonary rehabilitation did not result in significant additional gains in sedentary time at 6 weeks or 6 months after rehabilitation.17 One study reported a 47.4 min reduction in the longest continuous sedentary time compared with the pre-intervention period, and the reduction in sedentary time was statistically different at 8 weeks of intervention compared with 4 weeks of intervention.11 In the study by Xiang et al, a comprehensive intervention based on the BCW theory significantly reduced sedentary time from a baseline of 724 hours to 6.19 hours at week 12 compared to usual care.16 In the 3-month Nordic walking intervention by Breyer et al, objective data showed that compared to baseline, the intervention group increased walking time by an average of 149 minutes/day and standing time by 129 minutes/day, while reducing sitting time by 128 minutes/day.18 The reduction in sedentary time was maintained up to the ninth month, indicating the long-term efficacy of Nordic walking in decreasing sedentary time among patients with COPD.
Since the included studies were conducted in different countries, variations in healthcare systems, cultural contexts, and patient beliefs compared to other regions may exist. Therefore, the feasibility and effectiveness of the interventions require validation within broader cultural settings.
Discussion
The Content of Intervention Strategies for Sedentary Behavior in Patients with Chronic Obstructive Pulmonary Disease Is Diversified
The Behavior Change Wheel (BCW) theory aims to assist intervention personnel to focus on the behavior itself, analyze the factors hindering the behavior change in depth, and formulate effective intervention measures accordingly.21 Michie et al constructed BCW based on the framework of 19 behavioral intervention theories for the development of effective intervention measures22 In its three-layer circular structure, its core layer focused on ability, opportunity and motivation-behavior model. Among the literatures included in this study, 4 literatures were guided by the core layer of BCW and conducted motivational interviews with patients to understand the current stage of behavior change of patients, stimulate intrinsic motivation, and then improve the ability of patients, such as knowledge education, setting goals and plans, and finally remind patients to change the environment of sedentary behavior through monitoring and feedback. However, in the report of Zhou Dandan, motivational interviewing was not conducted on patients, which may be due to the fact that motivational interviewing requires interviewers to have certain qualifications, takes a long time and has high uncertainty of effect.14 In addition, although the other 2 studies conducted one-on-one interviews, the qualifications of the interviewers were not specified. Therefore, future studies need to further improve the qualifications of the interviewers and ensure the reliability and accuracy of the research results. BCW theory is widely regarded as a comprehensive and influential theoretical framework in health behavior research, covering almost all behavioral determinants. In the studies on sedentary behavior in patients with diabetes, researchers have used BCW theory as a framework to identify the key determinants of sedentary behavior in patients with type 2 diabetes, which lays a theoretical foundation for the development of targeted interventions in the future.23 In addition, the BCW theory was used as a framework to develop home-based exercise programs for overweight and obese adults, and 24 behavior-change techniques were identified to improve the success of exercise programs for overweight and obese adults.24 Wearable devices can monitor patients’ sedentary time in real time and record their daily steps, providing intuitive feedback data to help patients recognize their own problems and reminding patients to change their sedentary lifestyle through vibration. In the study of Cheng et al, it was also pointed out that the number of steps has high accuracy and sensitivity in identifying sedentary lifestyles25 Breyer et al showed that Nordic walking exercise has a significant effect on reducing sedentary time, and it is a simple and effective way of physical exercise18 The study by Della Guardia et al found that Nordic walking exercise not only reduced fasting blood glucose but also improved quality of life in sedentary type 2 diabetic patients.26
Effectiveness of Intervention Strategies for Sedentary Behavior in Patients with Chronic Obstructive Pulmonary Disease
The results of this study show that intervention strategies for sedentary behavior in COPD patients are feasible in reducing sedentary time, with 4 studies reporting an improvement in sedentary time in COPD patients compared with before intervention. However, due to the lack of relevant studies on sedentary behavior intervention strategies for COPD patients, only 6 studies were included in this study, which were from 4 countries such as China and Germany, and there may be differences between different countries. In addition, except for the Nordic walking exercise, which had better long-term effects, other studies did not continue to track the long-term effects. However, in contrast, Cheng et al’s19 study did not observe a reduction in sedentary time but an increase in moderate-to-vigorous intensity physical activity, possibly because the 6-week intervention period may be short compared with the 10-week period needed to develop new, solid “sedentary reduction” habits Furthermore, the mean rate of goal attainment of 64% suggests that an “effective dose” of the intervention may not be sufficient to induce behavioral change. A study with up to 9 years of follow-up found that adequate physical activity and reduced sedentary time reduced the risk of death, and there was no significant association between the degree of physical activity and the risk of death.27 The results of Tofoli et al showed that light physical activity is the main determinant of sedentary behavior in COPD, and focusing on increasing the time of light physical activity level has a promoting effect on patient health outcomes.28 The intervention strategy in this study was effective, so corresponding measures can be actively taken to reduce sedentary time in COPD patients and reduce the risk of death.
Despite multiple studies having assessed the effects of sedentary behavior interventions on patients with COPD, the outcomes have shown heterogeneity. By synthesizing these conflicting results, we have identified several potential underlying patterns and moderating factors that may explain the variations, such as intervention durations that may be too short, high baseline physical activity levels, an insufficient dose of intervention, and worsening COPD symptoms during the intervention period.
The studies included in this review present certain limitations in their implementation context, which may affect the broad applicability of the conclusions. Geographically, the evidence originates from several countries including China, Germany, Austria, and Australia. The interventions were primarily delivered by multidisciplinary teams and professional Nordic walking instructors in home-based settings, utilizing specialized devices such as accelerometers for the analysis of sedentary behavior metrics. Collectively, these factors suggest that the transferability of the current evidence across different healthcare systems, resource availability (eg, access to specialized coaches or equipment), and cultural contexts requires careful evaluation.
Behavior Change Techniques of Intervention Strategies for Sedentary Behavior in Patients with COPD Can Be Used Synergistically
The results of this study showed that the BCTs used in the sedentary behavior intervention strategies for COPD patients were diverse, and more than four BCTs were used in the included studies, and there may be synergistic effects between various techniques. Goal setting (1.1), Feedback on behavior (2.2), Self-monitoring of behavior (2.3), and Instruction on how to perform the behavior (4.1) form the cornerstone of all interventions. This combination systematically enhances patients’ self-management capability and reflective motivation, creating a complete support loop of “set goals - learn skills - monitor progress - receive feedback. Information about health consequences (5.1) was used in 4 studies. This indicates that beyond core self-regulation support, educational strategies to alter cognitions and enhance perceived benefits/risks of behavior change are widely adopted. Behavioral practice/rehearsal (8.1) and Behavior substitution (8.2) were each applied in 3 studies. These techniques directly target automatic motivation, aiming to substitute sedentary behavior with physical activity. However, environmental restructuring (12.1) was only applied in two studies, and its effectiveness in altering sedentary behavior requires further investigation. Social support (3.3) can provide emotional support and help, so that patients feel cared for and encouraged by others, so as to more firmly change their sedentary behavior. In the future, research can combine a variety of BCTs to construct a variety of intervention strategies for sedentary behavior in COPD, so as to reduce the sedentary time of patients.
Conclusion
This paper summarizes the current intervention strategies for sedentary behavior in COPD patients through a scoping review, and preliminary summarizes the core characteristics, clinical effectiveness, and BCTs of these strategies. Existing evidence indicates that interventions grounded in behavior change show signals of reducing device-measured daily total sedentary time and shortening prolonged sitting bouts in patients with COPD; however, the durability of these effects varies across studies. At the end of the intervention period, effective interventions could reduce patients’ daily total sedentary time by 60–128 minutes per day. These changes imply a decrease in prolonged, unbroken sitting periods, which carries potential clinical benefits for alleviating symptoms such as dyspnea and fatigue, as well as improving circulatory function. Nevertheless, it should be transparently noted that the current evidence base is limited by small sample sizes and high heterogeneity, with a lack of standardized measurement devices and core outcome indicators. Only one study included a follow-up assessment extending to 36 weeks, demonstrating the maintenance of reduced sedentary time, while two studies reported no significant change in total daily sedentary time despite observed increases in physical activity. Therefore, future research for practice, prioritize strategies that build capability, opportunity, and motivation to prompt breaks in sitting and light-intensity accrual using wearables or simple cues, for research, standardize device metrics and bout/break definitions, standardize definitions and outcome measures, report minimal clinically important changes when available, plan maintenance beyond 3–6 months including real-world implementation assessments, power trials for sedentary outcomes rather than steps alone, strengthen the standardized coding and reporting of BCTs to improve the transparency and repeatability of the research process.
Funding
This study was supported by [the Joint Special Project between Yunnan Federation of Social Sciences and Yunnan University of Chinese Medicine] (Grant number LHZX202419) and [Yunnan Provincial Annual Planning Project for Philosophy and Social Sciences] (Grant number QN202525).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020;54(24):1451–12. doi:10.1136/bjsports-2020-102955
2. Leão OAA, Knuth AG, Meucci RD. Sedentary behavior in elderly residents from the rural area in Southern Brazil. Rev Bras Epidemiol. 2020;23:e200008. PMID: 32130397. doi:10.1590/1980-549720200008
3. Katzmarzyk PT, Powell KE, Jakicic JM, Troiano RP, Piercy K, Tennant B. Sedentary behavior and health: update from the 2018 physical activity guidelines advisory committee. Med Sci Sports Exerc. 2019;51(6):1227–1241. doi:10.1249/MSS.0000000000001935
4. Furlanetto KC, Donária L, Schneider LP. Sedentary behavior is an independent predictor of mortality in subjects with COPDJ. Respiratory Care. 2017;62(5):579–587. doi:10.4187/respcare.05306
5. Hunt T, Madigan S, T WM, et al. Use of time in people with chronic obstructive pulmonary disease – a systematic review. Int J Chronic Obstr. 2014;9:1377–1388. doi:10.2147/COPD.S74298
6. You Y, Chen Y, Wang X, Wei M, Zhang Q, Cao Q. Accelerometer-measured physical activity patterns are associated with phenotypic age: isotemporal substitution effects. Heliyon. 2023;9(9):e19158. doi:10.1016/j.heliyon.2023.e19158
7. de Moura SS, de Menezes LAA, Carraro JCC, Machado-Coelho GLL, Meireles AL. Combinations of physical activity, sedentary behavior and sleep and their associations with cardiovascular risk. BMC Public Health. 2025;25(1):1024. doi:10.1186/s12889-024-20829-7
8. You Y, Chen Y, Fang W, et al. The association between sedentary behavior, exercise, and sleep disturbance: a mediation analysis of inflammatory biomarkers. Front Immunol. 2023;13:1080782. doi:10.3389/fimmu.2022.1080782
9. Schneider LP, Furlanetto KC, Rodrigues A, Lopes JR, Hernandes NA, Pitta F. Sedentary behaviour and physical inactivity in patients with chronic obstructive pulmonary disease: two sides of the same coin? COPD. 2018;15(5):432–438. doi:10.1080/15412555.2018.1548587
10. Gennuso KP, Matthews CE, Colbert LH. Reliability and validity of 2 self-report measures to assess sedentary behavior in older adults. J Phys Act Health. 2015;12(5):727–732. doi:10.1123/jpah.2013-0546
11. Cavalheri V, Straker L, Gucciardi DF, Gardiner PA, Hill K. Changing physical activity and sedentary behavior in people with COPD. Respirology. 2016;21(3):419–426. doi:10.1111/resp.12680
12. Esteban C, Antón-Ladislao A, Aramburu A, et al. ReEPOC-REDISSEC group. Physical activity and sedentary behaviour in patients admitted with COPD: associated factors. Respir Med Res. 2023;84:101052. doi:10.1016/j.resmer.2023.101052
13. Serrat R, Scharf T, Villar F, et al. Fifty-five years of research into older people’s civic participation: recent trends. Future DirectionsJ the Gerontologist. 2020;60(1):e38–e51. doi:10.1093/geront/gnz021
14. Zhou DD. Study on Influencing Factors and Intervention of Sedentary Behavior in Patients with Stable Chronic Obstructive Pulmonary Disease Based on Behavior Change Wheel Theory D. Soochow University; 2024.
15. Effects of respiratory rehabilitation nursing based on behavior change wheel model on physical activity and sedentary behavior of patients with chronic obstructive pulmonary disease J. J Jilin Univ Med. 1–5.
16. Xiang X, Han M, Luo X, et al. Development of a behavior change intervention to improve physical activity in patients with COPD using the behavior change wheel: a non-randomized trial. Sci Rep. 2023;13(1):22929. doi:10.1038/s41598-023-50099-z
17. Geidl W, Carl J, Schuler M, et al. Long-Term Benefits of Adding a Pedometer to Pulmonary Rehabilitation for COPD: the Randomized Controlled STAR Trial. Int J Chronic Obstr. 2021;16:1977–1988. doi:10.2147/COPD.S304976
18. Breyer MK, Breyer-Kohansal R, Funk GC, et al. Nordic Walking improves daily physical activities in COPD: a randomised controlled trialJ. Respir Res. 2010;11(1):112. doi:10.1186/1465-9921-11-112
19. Cheng SWM, Alison J, Stamatakis E. Six-week behaviour change intervention to reduce sedentary behaviour in people with chronic obstructive pulmonary disease: a randomised controlled trial. Thorax. 2022;77(3):231–238. doi:10.1136/thoraxjnl-2020-214885
20. Michie S, Richardson M, Johnston M, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behavioral Medi. 2013;46(1):81–95. doi:10.1007/s12160-013-9486-6
21. Fuxia L. Application Effect of Health Education Model Based on BCW Theory in Patients with Cancer Pain D. Shandong University; 2018.
22. Michie S, van Stralen M M, West R, van Stralen MM. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
23. Zhang X, Yang D, Luo J, et al. Determinants of sedentary behavior in community-dwelling older adults with type 2 diabetes based on the behavioral change wheel: a path analysis. BMC Geriatr. 2024;24(1):502. doi:10.1186/s12877-024-05076-0
24. Power S, Broom D, Duncan M, et al. Using the behavior change wheel to design a novel home-based exercise program for adults living with overweight and obesity: comprehensive reporting of intervention development. Obesity Science & Practice. 2024;10(3):e774. doi:10.1002/osp4.774
25. Cheng SWM, Alison JA, Stamatakis E, Dennis SM, McKeough ZJ. Validity and accuracy of step count as an indicator of a sedentary lifestyle in people with chronic obstructive pulmonary disease. J Arch Phys Med Rehabil. 2023;104(8):1243–1252. doi:10.1016/j.apmr.2023.01.020
26. Della Guardia L, Carnevale Pellino V, Filipas L, et al. Nordic walking improves cardiometabolic parameters, fitness performance, and quality of life in older adults with type 2 diabetes. Endocr Pract off J Am Coll Endocrinol Am Assoc Clin Endocrinologists. 2023;29(2):135–140. doi:10.1016/j.eprac.2022.11.007
27. Yuan L, Zhang L, Wang Y, et al. Impact of leisure-time physical activity and sedentary behavior on mortality in patients with chronic obstructive pulmonary disease. Am. J. Phys. Med. Rehabil. 2025;104(4):e49–e57. doi:10.1097/PHM.0000000000002612
28. Tofoli TM, Santin L, Medeiros L. Determinant factors of sedentary time in individuals with COPD. Respir Med. 2024;234:107839. doi:10.1016/j.rmed.2024.107839
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.