")
Back to Journals » Patient Preference and Adherence » Volume 17
Secukinumab for the Treatment of Psoriasis in Pediatrics: Patient Selection and Acceptability
Authors Narbutt J, Niedźwiedź M , Lesiak A, Ceryn J, Skibińska M
Received 10 January 2023
Accepted for publication 11 February 2023
Published 16 February 2023 Volume 2023:17 Pages 421—431
DOI https://doi.org/10.2147/PPA.S350753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Joanna Narbutt,1 Michał Niedźwiedź,1 Aleksandra Lesiak,1 Justyna Ceryn,1,2 Małgorzata Skibińska1
1Department of Dermatology, Pediatric Dermatology and Dermatological Oncology, Medical University of Lodz, Lodz, Poland; 2International Doctoral School of the Medical University of Lodz, Lodz, Poland
Correspondence: Michał Niedźwiedź, Department of Dermatology, Pediatric Dermatology and Oncology, Medical University of Lodz, gen. Karola Kniaziewicza 1/5, Lodz, 91-347, Poland, Tel +48 690 529 430, Email [email protected]
Abstract: Psoriasis (PsO) is a chronic, systemic, immune-mediated inflammatory skin disease affecting 1% to 5% population worldwide. In one-third of patients, the first symptoms of PsO manifest in childhood, with a mean age of nine years. Psoriasis in children under 16 years of age constitutes 4% of dermatological problems in this age group. Chronic inflammation of the skin observed in PsO is associated with a development of potentially serious comorbidities, including psoriatic arthritis, hypertension, metabolic syndrome, cardiovascular diseases, inflammatory bowel disease, depression and anxiety. It is reported that among children with psoriasis between 5 and 16 years of age health-related quality of life is reduced by 30.5%. Early diagnosis and effective treatment are crucial in pediatric psoriatic patients to avoid future complications and stigmatization. Treatment for psoriasis consists of a range of topical medications, phototherapy and non-biologic and biologic systemic therapies. Approved biologics for PsO in pediatric patients include etanercept, adalimumab, ustekinumab, ixekizumab and secukinumab. Secukinumab, a recombinant, fully human monoclonal antibody targeting IL-17A, was approved by the EMA (2020) and FDA (2021) in pediatric patients above 6 years of age for the treatment of moderate to severe plaque psoriasis who are candidates for systemic therapy. This review discusses the selection and acceptability of secukinumab in children with psoriasis.
Keywords: pediatric psoriasis, psoriasis vulgaris, secukinumab, acceptability
Psoriasis and Pediatric Psoriasis - Introduction
Psoriasis (PsO) is a chronic, systemic, immune-mediated inflammatory skin disease affecting 1% to 5% population worldwide.1–3 It is characterized by increased proliferation of keratinocytes caused by an induced activity of T-cells with an important role of genetic and epigenetic factors.4,5 The most common variant of psoriasis, plaque psoriasis is characterized by red plaques covered with silver or white scales localized mainly around elbows, knees, scalp and trunk.6 Psoriasis may also affect nails and scalp. In one-third of patients, the first symptoms of PsO manifest in childhood, with a mean age of nine years.7 Psoriasis in children under 16 years of age constitutes 4% of dermatological problems in this age group.7
Chronic inflammation of the skin observed in PsO is associated with a development of potentially serious comorbidities, such as obesity, type 2 diabetes, dyslipidemia, hypertension, metabolic syndrome, cardiovascular diseases (CVD), arthritis (including psoriatic arthritis – PsA), inflammatory bowel diseases (IBD), non-alcoholic fatty liver disease, multiple sclerosis, depression and anxiety.8–12 Triggering factors in children psoriasis slightly differ from adults and include trauma, stress and bacterial infections.6
Because of skin lesions, children with PsO often face stigmatization which dramatically decreases their quality of life, causing social isolation and difficulties in learning. This may affect not only childhood, but also influence their future life, including choosing an occupation and whether to start a family.13–16 It is reported that among children with psoriasis between 5 and 16 years of age health-related quality of life is reduced by 30.5%.16 Interestingly, the impairment of quality of life in children with psoriasis seems to be greater than atopic dermatitis, alopecia and acne.16 The psychological impact of the unpredictability of the course of skin disease leads to frustration and lack of satisfaction from treatment.16 Parents or caregivers of children with PsO often also suffer from anxiety, guilt and depression that decreases their quality of life and affects family interrelationships.17 Early diagnosis and effective treatment seem to be crucial in pediatric psoriatic patients to avoid future complications and stigmatization.
Measurement of Psoriasis Severity
Assessing the intensity and severity of psoriasis in children, as well as in adults, guides the doctors to choose the right treatment for the patients. The severity of psoriasis in children can be measured by a number of methods including assessment of the Body Surface Area (BSA) covered with psoriatic lesions, the Psoriasis Area and Severity Index (PASI) Investigator’s Global Assessment (IGA) and the Children’s Dermatology Life Quality Index (CDLQI), with a separate version for infants called the Infants’ Dermatology Life Quality Index (IDLQI).18–22 Body surface area describes the percentage of involved skin with psoriatic lesions. A standard way to measure BSA in children is the rule of nines, the same as used in burns assessment, with adjustment to the age of the child. Commonly, psoriasis with BSA of less than 3% of involved skin is considered as mild, from 3 up to 10% to be moderate, and equal and above 10% is considered as severe disease. PASI score assesses not only the involved skin area, but also psoriasis intensity (redness, scaling and plaque thickness). The PASI score ranges from 0 to 72, in which the score between 0 and 5 describe none to mild psoriasis, 6 to 10 moderate, and 10 and above severe PsO. PASI scores are also used for monitoring the clinical response to the treatment. For example, if the patient achieves PASI 50 it means the reduction of PASI score by 50%, or PASI 75 means reduction of PASI by 75% from the baseline. The CDLQI is a 10 question survey which includes questions about the severity of pruritis, impact of skin lesions on self-esteem, relationships, clothing, physical activities and hobbies, education, stigmatization and quality of sleep.18,23 Maximum score of CDLQI is 30 and the results between 7 and 12 show moderate impact and results above 12 show a very large effect of the disease on the quality of patients’ life. The survey for patients from 4 to 16 years of age is also available in cartoon format, which may appeal more to younger children.18 For children aged from 0 to 4 years old there is a separate questionnaire called the Infants’ Dermatitis Quality of Life Index based on the same principle.24 Additionally, the Investigator’s Global Assessment (IGA) scale may be used by the clinicians for grading the severity of the disease.25 IGA scale is a simple instrument providing a clinician’s subjective evaluation of psoriasis severity with scores of 0 (clear skin), 1 (almost clear), 2 (mild), 3 (moderate) or 4 (severe).
In clinical trials, recommendations for treatment and every day assessments, simplified versions of BSA, PASI, CDLQI and IGA scores for severity of the disease are used (Table 1).
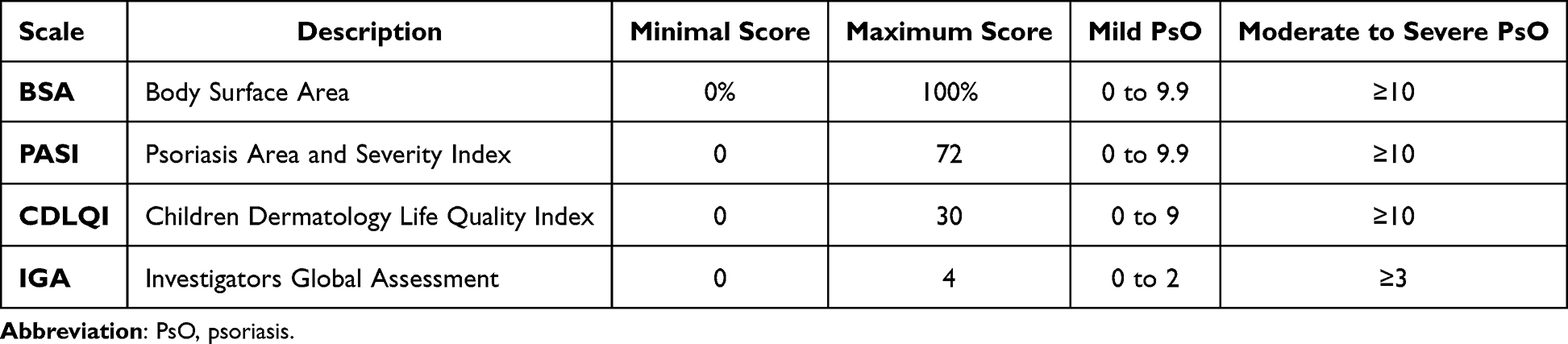 |
Table 1 Four Most Common Scales Used in the Assessment of Psoriasis in Children |
Topical and Conventional Treatment for Pediatric Psoriasis
Diagnosing psoriasis in children has its challenges, especially in very young patients, however it should not be a problem for majority of physicians. Therapy, mainly due to the necessity of treating children off-label, may be more challenging.6,26 Treatment for psoriasis consists of a range of topical medications, phototherapy, non-biologic and biologic systemic therapies. Topical treatment of PsO is mostly based on corticosteroids, calcineurin inhibitors, and vitamin D3 analogues. Combination of topical medications, including also topical tazarotene, anthralin and coal tar, which are still available in some countries, may be also an option.6,19 Another treatment used in pediatric psoriasis is narrow band-UVB therapy (NB-UVB). The course of NB-UVB includes around 30 short sessions of exposure to the UV wavelength of 311–313 nm and is considered safe and effective.27 Data on efficacy and safety of oral psoralens with UVA (PUVA) therapy in children with PsO are limited, however due to the side effects of the treatment it should not be used in children younger than 12 years old and currently is used less often in adults.28 Phototherapy requires regular visits to the treatment center over a period of time, which may be troublesome for parents and caregivers. There are several nonbiologic agents used in the treatment of moderate to severe psoriasis in children. Methotrexate (MTX), acitretin and cyclosporin A (CsA) are the most frequently used, but none of them is registered for pediatric psoriasis treatment.19,29,30 The main objective in the treatment of PsO in children is to control and maintain remission of skin lesions.
Biological Treatments for Pediatric Psoriasis
Depending on the country, there may be different approvals for biological treatment in children, however it is the first group of medications with clinical trials and registrations in this group of patients.6,31 The availability of biological treatment in many countries may still be limited to referential medical facilities which in consequence reduces its accessibility for pediatric patients. Approved biologics for PsO in pediatric patients (depending on the country and medical agency) are etanercept, adalimumab, ustekinumab, ixekizumab and secukinumab (Table 2). Biologics are more likely to be prescribed in patients with moderate-to-severe PsO, overweight and with concomitant psoriatic arthritis.32 Approximately 25% of pediatric patients with psoriasis are treated with biologics at some point in their life, and one-third of them will also simultaneously receive topical and/or conventional treatment.32 The real-life study conducted among psoriatic patients by Marques et al33 which included also children revealed superior effectiveness of biological medications when compared to topical and non-biological therapies, but higher rate of side effects including mild infections, which are consistent with other studies.34 European recommendations emphasize that choosing biologics for patients should be influenced by specific circumstances, such as presence of comorbidities, pregnancy or chronic infections.35 However, due to lack of long-term results of head-to-head studies, it is still unknown which biologic treatment should be primarily used in treatment for pediatric patients with PsO.36
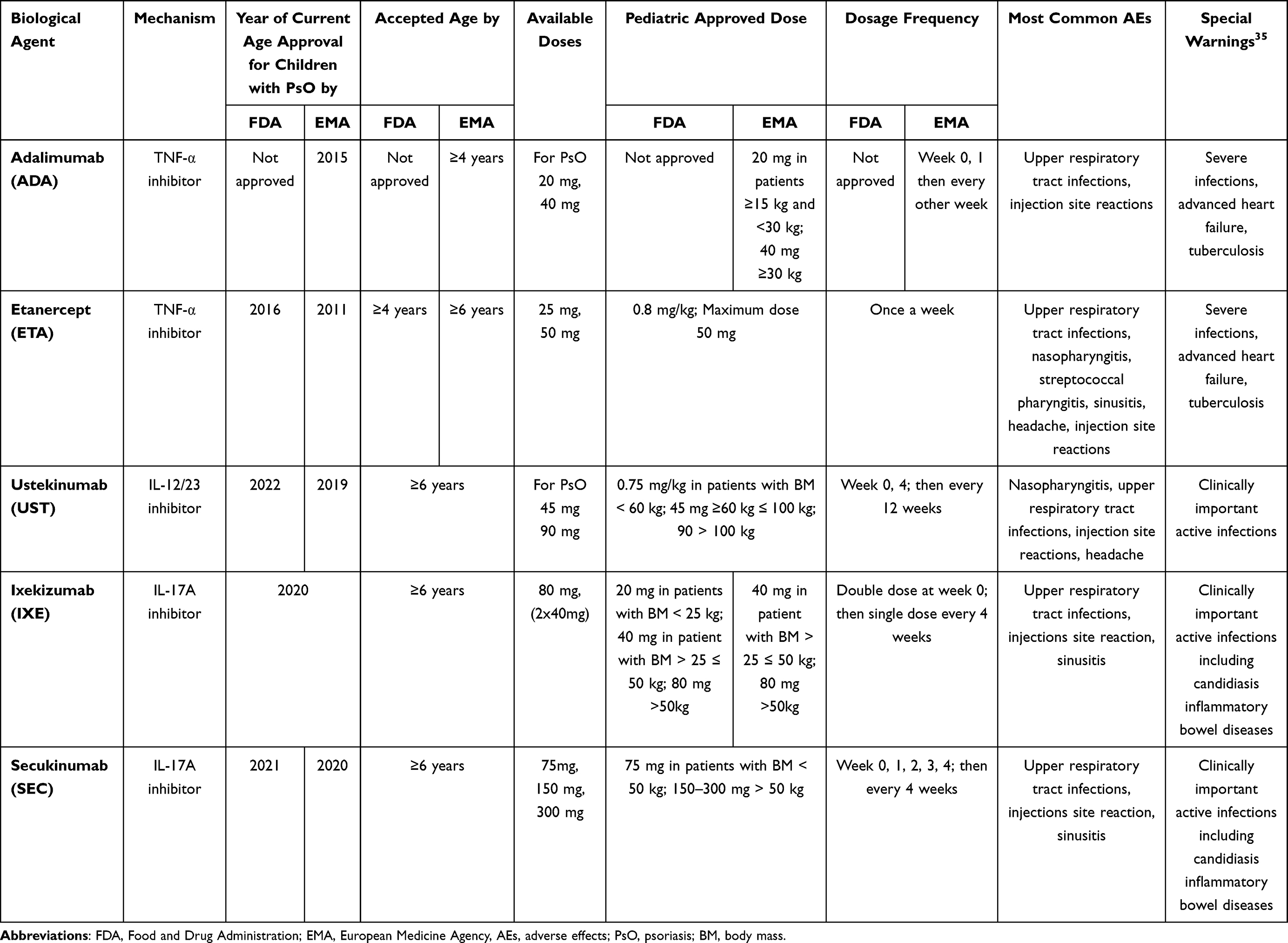 |
Table 2 Biological Agents Registered by FDA and EMA for Pediatric Plaque Psoriasis Treatment |
Role of IL-17 in Inflammatory Reactions and Psoriasis
It has been known for a long time that several cytokines are taking part in the development of psoriasis.37 Beyond TNF-α, IL-12, IL-23 and IFN-γ, IL-17 seems to play a key role in the immunopathogenesis of psoriasis.2,37,38 Many types of immune cells, including dendritic, natural killer, macrophages, and T-cells are producing the IL-17 family cytokines.39 IL-17 drives the inflammations by stimulating production of antimicrobial peptide LL37, IL-6, and 8, granulocyte colony-stimulating factor, chemokine ligand 20, and granulocyte-macrophage-colony stimulating factor.40 Genomic sequencing has led to the identifications of six IL-17 subtypes, IL-17A, B, C, D, E (also known as IL-25), and IL-17F, of which both IL-17A and IL-17F are most homologous (55%) and seem to be most important in psoriatic pathological pathways.38,41,42 Physiologically, IL-17A takes part in many phenomena, such as antimicrobial defense (against bacteria and fungi), the metabolic function of adipocytes, keratinocyte differentiation, thermoregulation, bone growth and regeneration, and wound healing.40 Elevated levels of this interleukin were observed in autoimmune diseases and cancer progression. Involvement of IL-17A has been described in plaque psoriasis (PsO), psoriasis arthritis (PsA), ankylosing spondylitis, hidradenitis suppurativa (HS), pityriasis rubra pilaris (PRP), and Behçet’s disease. Increased levels of IL-17 induce the inflammatory reaction with hyperproliferation of keratocytes causing psoriatic plaque. It is also hypothesized that blocking the hyperactivity of Th17 lymphocytes may even reduce the risk of atherosclerotic plaque development.10,35,43
Secukinumab
Through understanding that IL-17 plays a crucial role in the pathogenesis of psoriasis, developing the treatment blocking the pathway of this interleukin seemed to be an obvious choice. There are two ways to inhibit the IL-17 pathway: blocking the receptors or/and directly blocking the molecule. Secukinumab, a recombinant, fully human monoclonal antibody targeting IL-17A, is approved by European Medicine Agency (EMA) and by the Food and Drug Agency (FDA) in the USA for the treatment of moderate to severe plaque psoriasis in pediatric patients above 6 years of age who are candidates for systemic therapy (EMA) or phototherapy (FDA).
Secukinumab in Pediatric Patients
The data on treatment with secukinumab in pediatric patients with PsO is still limited as it was registered in children in 2020–21. However, the results of clinical trials and real-life experience do exist for adults.44
Three clinical trials on secukinumab in children with psoriasis have been published so far (December 2022). The first double-blind randomized, controlled trial compared the efficacy and safety of low and high dose of secukinumab when compared to placebo and etanercept (TNF-α inhibitor) in pediatric patients with psoriasis. One hundred and sixty-two children and adolescents from 6 to 18 years of age with severe chronic plaque-type PsO were enrolled.45 PASI score ≥20, Investigator’s Global Assessment (IGA) of 4, and BSA ≥ 10% were among the inclusion criteria for the study. All patients had a history of psoriasis ≥3 months and were assessed as candidates for systemic therapy. Patients with active inflammatory diseases and other types of psoriasis were excluded from the study. Patients were randomized to four arms: receiving low-dose (LD, n = 40) secukinumab of 75 mg per injection in patients with weight <50 kg, and 150 mg in patients with weight ≥50 kg, receiving high-dose (HD; n = 40) secukinumab of 150 mg in patients with weight <25 kg, 150 mg in patients weighing >25 and <50 kg, and 300 mg in patients with a weight ≥50 kg; receiving etanercept (n = 41) with a dose of 0.8 mg per kilogram of body mass (up to 50 kg), or receiving placebo (n = 41). Patients received secukinumab and placebo injections at weeks 0, 1, 2, 3, and 4 and then every 4 weeks, and patients who were administered etanercept received injections every week. At twelve weeks of the trial, the mean PASI scores improved from baseline by 82.9% in the LD SEC group, and by 79.9% in the SEC HD group in comparison to 29.3% in the placebo group and 74.2% in the etanercept group. Both secukinumab doses (LD and HD SEC) demonstrated greater clinical improvement compared to etanercept throughout the study up to week 52. The mean PASI scores improved by 92.6% in the LD SEC group, 91.8% in the HD SEC and 77.7% in the etanercept group. This effect was even more pronounced at week 52, with the improvement by 92.6% (LD SEC) and 91.8% (HD SEC) with etanercept group showing reduction of the PASI score by 77.7% in comparison. The authors of the paper emphasize that patients ≥50 kg should be considered for the higher dose of secukinumab if a low dose provides insufficient efficacy. The quality of life among treated patients also improved in both LD and HD SEC groups when compared to placebo and etanercept groups. Scores of 0 or 1 in CDLQI were achieved by 44.7% (LD SEC group), 50.0% (HD SEC group), 15% (placebo group), and 36.6% (etanercept group) at week 12 and in 60.6% in LD SEC group, 66.7% in HD group and 44.4% in etanercept group at week 52. Secukinumab was also well tolerated in both LD and HD SEC groups. Reported adverse effects (AE) were consistent with the data from clinical trials in adult PsO patients. The most frequent AEs were mild infections, injection site reactions, headaches, and neutropenia. Only in three patients (out of 114) treated with secukinumab, the treatment was discontinued due to the AEs. No cases of inflammatory bowel disease were reported over 52 weeks observation period.
Another trial was an open-label, randomized, Phase 3, two-arm, multicenter study in pediatric patients aged 6 to <18 years with moderate to severe chronic plaque psoriasis. This was published first with the results from week 24 and then with observation up to 52 weeks of treatment.46,47 Inclusion criteria included PASI score ≥12, IGA (modification 2011) score ≥3, and BSA ≥ 10% at randomization. All patients had a history of psoriasis ≥3 months and were assessed as candidates for systemic therapy. Patients with other subtypes of psoriasis and active inflammatory diseases were excluded. Eighty-four patients were divided into two arms: low-dose SEC (n = 42), and high-dose SEC (n = 42). Early improvements were seen with a reduction of PASI score by 75% (PASI 75) responses in 61.9% (LD) and 71.4% (HD) patients at week 4. PASI 75 and IGA 0/1 score responses increased in week 24 (LD: 95.2%/88.1% and HD: 96.9%/93.3% respectively) and sustained up to week 52 (LD: 92.8%/88.9% and HD: 93.3%/84.7% respectively). By week 52 the reduction of PASI score by 90% and 100% were obtained in 78.7% and 53.5% patients, respectively, in the LD group and 84.7% and 70.0% in the HD group. CDLQI scores 0/1 were achieved in 50.0% and 61.9% of patients in week 12, which increased to 70.7% and 70.3% in week 52, respectively, in the LD and HD groups. Statistical analysis revealed consistent secukinumab efficacy across all subgroups (separated by age, body, weight, disease severity scores, and drug dose). Treatment emergent adverse events were reported by 65.5% of patients with no difference in frequency between LD and HD groups. The most common AEs were infections and infestations, such as nasopharyngitis, diarrhea, and vomiting. Mild severity Candida infections were reported in 3 patients, with no need for dose adjustment or stopping the medication. Acne was reported in 6 patients with no link to the study medication or its dose. Six patients discontinued the study due to: alanine aminotransferase and aspartate aminotransferase serum level elevation (n = 1 HD), hemorrhagic diarrhea (n = 1 HD), lack of efficacy (n = 2, 1 LD and 1 HD) and subject/guardian decision (n = 2 LD). The case of hemorrhagic diarrhea led to an investigation into possibility of inflammatory bowel disease diagnosis, which was not confirmed.
The results of presented clinical trials are similar to those conducted in adult patients.44 Meta-analysis using SUCRA (surface under cumulative ranking curve) performed by Huang et al48 showed that among all available clinical trials with biologics in pediatric population (etanercept, adalimumab, ustekinumab, ixekizumab and secukinumab), low dose secukinumab showed the best PASI 90 response (84.7%), followed by ixekizumab (70.8%) at weeks 12–16. Similar analysis was provided by Gohlen at al.49 confirming efficacy of biologics in both pediatric and adult populations. Another analysis by Lernia et al50 also showed superiority of anti-IL-17 and anti-IL12/23 agents when compared to anti-TNF-α therapies. Specifically, they reported that treatment with anti-IL-12/23 and anti-IL-17 showed a better number needed to treat for achieving PASI 75 and treatment with anti-IL-17 for PASI 90.
Overall infections (the most common side effect of biologics treatment) were more frequent with TNFα inhibitors than other groups of biologics. As IL-17 is involved in neutrophil recruitment, production of antimicrobial peptides and maintaining the skin/mucous membranes barrier, using anti-IL17 biologics may be connected to higher levels of Candida infections, which were reported in 0.0–1.8% pediatric patients in the clinical trials.40,49 Candida infections connected with secukinumab use were all mild to moderate in severity. Anti-IL17 medications may worsen the course of inflammatory bowel disease (IBD).51 In the pediatric clinical studies for secukinumab and ixekizumab IBD was reported in 0–1.5% patients. As in adults, this group of biologics should not be prescribed for patients with diagnosed inflammatory bowel disease and the patients’ history should be screened for the symptoms.31,51,52
Selection of Pediatric Patients for Secukinumab
Secukinumab is indicated for the treatment of moderate to severe plaque psoriasis in children from the age of 6 years who are candidates for systemic therapy. Both clinical trials on the efficacy of secukinumab in pediatric patients with PsO revealed efficacy and safety in children and adolescents with moderate-to-severe chronic psoriasis, however patients with other active inflammatory conditions were excluded. Unfortunately, there are no clear dermatological guidelines for the specific indication for each biologic (including secukinumab) in pediatric patients. Clinical guidelines and recommendations are based on available scientific data; however, it does not mean that those medications can be freely prescribed for the patients. National Institute of Clinical Excellence (NICE) in the UK recommends secukinumab in children with PASI score >10 but only if the disease did not respond to other systemic treatments including ciclosporin, methotrexate and phototherapy, or these options are contraindicated or not tolerated. There is also a commercial agreement with the National Health Service regarding funding of the treatment and recommending to the doctors to choose the least expensive medications from the range of suitable treatments for the particular patients.53 If the patients do not achieve PASI 75 at 12 weeks the treatment must be stopped. NICE puts secukinumab effectiveness above etanercept and on similar level to ustekinumab, however there are no direct head-to-head studies. Adalimumab effectiveness when compared with secukinumab is uncertain. Recommendations for pediatric psoriasis patients developed by Peris et al54 suggest that early treatment with biologics in pediatric patients with moderate to severe psoriasis may positively modify the disease course. At the same time, they agreed that choosing the right systemic therapy must be based on the child’s age, psoriasis severity, comorbidities, no response to topical treatments and phototherapy and the psychological and social state of the patients, including the impact of the disease on the quality of life. Overall, in their algorithm for pediatric psoriasis treatment, they do recommend biologics (as the first line of systemic therapies equally to narrow-band UVB) in children with PASI >10 or BSA >10 and CDLQI >10. Joint American Academy of Dermatology and National Psoriasis Foundation guidelines of care for the management and treatment of psoriasis in pediatric patients published in 2019, before the registration for secukinumab was obtained in this age group, recommend etanercept and ustekinumab and to a lesser extent adalimumab and infliximab.19 Recommendations of the Polish Dermatological Society for pediatric psoriasis treatment suggest to consider systemic treatment, preferably biologics in all children with PASI ≥ 10 and/or BSA ≥ 10% and/or CDLQI ≥ 10.52,55
There are no published clinical trials on the efficacy of secukinumab in other types of psoriasis; however, few case studies indicate that the medication may be used successfully in psoriatic disorders. Children with generalized pustular psoriasis (GPP) due to a deficiency of IL-36 receptor antagonist (DITRA) successfully treated with secukinumab were reported.56–58 Albela et al59 described case series of four pediatric patients with acute GPP who were treated with off-label use of secukinumab, with a dose of 150 mg per injection in patients under 30 kg, and with an initial dosage of 300 mg following 150 mg per injection in a patient with body mass over 40 kg. Patients with an insufficient outcome with conventional treatment (oral acitretin, cyclosporin) received secukinumab injections with clearance of skin lesions in up to 50% of baseline findings within 48 hours. In January 2023 Ruan et al60 published a retrospective analysis of 18 children with general pustular psoriasis treated with secukinumab with a 48 weeks observation period. Secukinumab was used at a dose of 75 mg at weeks 0, 1, 2, 4 and every 4 weeks thereafter. Significant improvement was observed as early as after 3 days from injection with disappearance of pustules and gradual reduction of erythema and scaling over the next 2 weeks. At 48-weeks 88.9% of patients were free of lesions. No serious adverse reactions were observed, with eczema-like reactions, nasopharyngitis, headaches, injection site reactions and diarrhea presented in single patients. Assessments of quality of life were performed with CDLQI and Pediatric Quality of Life Inventory scale. Both showed a significant negative impact of the disease on the patients’ physical and psychosocial status and the treatment with secukinumab remarkably improved those scores.
In 2018, Craiglow et al61 proposed a new dermatological condition, CARD14 - Associated Papulosquamous Eruption (CAPE) describing the spectrum of skin disorders with clinical features of psoriasis, pityriasis rubra pilaris, ichthyosis and/or atopic dermatitis. The authors suggest that after the confirmation of CARD14 mutations, physicians should consider treatment with secukinumab in this group of patients. Secukinumab treatment was also used in different types of ichthyoses with mixed results.62,63
Currently, results of phase 3 clinical trials with secukinumab in the juvenile idiopathic arthritis including juvenile psoriatic arthritis patients were published, showing significantly longer time to disease flare when compared with placebo-treated patients.64 Majority of the site effects were similar to those observed in adult patients treatment, with nasopharyngitis, nausea, upper respiratory tract infections, oropharyngeal pain, headache, fever and diarrhea being the most common ones. In one patient Crohn’s disease was diagnosed during the study. In all 86 treated patients discontinuation of the treatment due to AE happened in 8 (9.3%), but 5 of them were in the placebo group. The FDA approved secukinumab for children aged 2 years or older (EMA for ≥6 years of age) with active juvenile psoriatic arthritis in 2022.
Secukinumab Acceptability for Pediatric Patients
The acceptability of health-care medication reflects the appropriation of the treatment based on anticipated or experienced responses to the intervention.65 It consists of factors such as burden (which may be reason of treatment discontinuation), side effects, experience and satisfaction of the patients but also physicians, and cost of the therapy. Patients and their parents/caregivers expect full clearance of skin lesions and pruritis, long-term remission and using safe and effective treatment.66 As one may expect children put preference for non sticky medications, giving quick results and no or fewer blood samples needed.66 From the clinicians’ point of view, the aim of treating children with psoriasis is to stop the inflammation and achieve clinical remission.55
In all pediatric clinical trials of secukinumab, no deaths were reported, and severe AEs were rare. The most commonly reported AEs in all studies were mild infections.45–47 A few case reports of more severe infections were described, including a case of staphylococcal toxic shock syndrome associated with secukinumab treatment in a 6-year-old girl with psoriasis and necrotizing fasciitis in a patient with severe combined immunodeficiency.67,68 Those cases emphasize the role of IL-17 in the antimicrobial response and the need for screening patients for wounds and skin infections, including candidiasis, during secukinumab treatment.67,68 Injection site reactions with secukinumab (6%) were mild and mostly did not require any treatment. Hypersensitivity reactions need to be immediately assessed and treated, and the treatment should be discontinued.51 It is important to remember that it is not recommended to use secukinumab in patients with IBD. So far, secukinumab safety profile in children has not showed significant differences when compared to adults. However, there are no head-to-head studies comparing secukinumab and other biologics (excluding etanercept) and systemic medications in the pediatric population regarding efficacy, safety and acceptability. Meta analysis with such a small number of studies may be underpowered, therefore more published clinical and real-world studies, which are ongoing, would be beneficial for further assessment of secukinumab position in psoriasis treatment in children.48,50
Secukinumab is available in three doses: 75 mg (in pre-filled syringe), 150 and 300 mg in pre-filled syringe and recently pre-filled pen, all administered subcutaneously (Figure 1). One of the main disadvantages of secukinumab for children is the route of admission. Subcutaneous injections can be not well tolerated due to needle phobia which is common in pediatric population. However, it is possible to use various techniques that reduce discomfort and anxiety during the injection, such as diverting the child’s attention or application of cold compresses.31,69 Recently available pre-filled pens may reduce this disadvantage significantly.
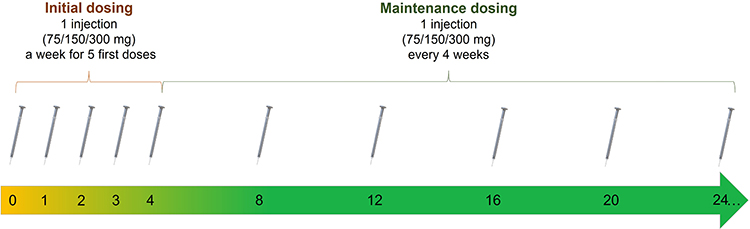 |
Figure 1 Administration of secukinumab algorithm. |
As mentioned before, major factors in the acceptability of medications are their price, availability, and route of administration. Secukinumab is not reimbursed in many countries and facilities that provide this medication are limited. In the USA, requirement for administration of biologics by payers is insufficient response to the conventional treatment despite lack of on-label indications, limited efficacy and safety data.70 Sometimes, the insurance cover of newer biologics is denied, even with registration for pediatric patients.71 In Poland, secukinumab for children with psoriasis can be provided free of charge only through an emergency access to medications pathway where acceptance criteria are very strict, and require fulfillment of several conditions.
Conclusion
Considering possible complications of chronic inflammation and comorbidities of PsO, it is crucial to start an effective treatment as soon as it is possible. Secukinumab was proved to be safe and effective medication in pediatric patients with psoriasis. Clinical trials and case studies show that it is a highly effective drug with a rapid and sustained clinical response. Also, relatively infrequent administration of the drug may increase acceptability for children. However, it is worth remembering that patients can develop infections and other side effects that rarely, but potentially can have profound consequences. Individualized and holistic medical care ongoing with close monitoring, as well as good contact between doctors and parents or legal guardians of patients, can help in safe treatment with secukinumab.
Funding
This research was funded by statutory activity no. 503/5-064-04/503-01 (Medical University of Lodz).
Disclosure
Joanna Narbutt is a speaker and/or advisor for: AbbVie, Almirall, Bausch Health, Bayer, Eli Lilly, Janssen, Mylan, Novartis, Polpharma, Pfizer, Sandoz, Sanofi and UCB. Michał Niedźwiedź declares that he has no competing interests. Aleksandra Lesiak is a speaker and/or advisor for: AbbVie, Almirall, Bausch Health, Bayer, Eli Lilly, Janssen, Mylan, Novartis, Polpharma, Pfizer, Sandoz, Sanofi and UCB. Justyna Ceryn declares that she has no competing interests. Małgorzata Skibińska is a speaker and/or advisor for: AbbVie, Eli Lilly, Mylan, Novartis, Polpharma and Sanofi.
References
1. Blair HA. Secukinumab: a review in moderate to severe pediatric plaque psoriasis. Pediatric Drugs. 2021;23(6):601–608. doi:10.1007/s40272-021-00476-w
2. Elder JT, Bruce AT, Gudjonsson JE, et al. Molecular dissection of psoriasis: integrating genetics and biology. J Invest Dermatol. 2010;130(5):1213–1226. doi:10.1038/jid.2009.319
3. Lebwohl MG, Kavanaugh A, Armstrong AW, van Voorhees AS. US perspectives in the management of psoriasis and psoriatic arthritis: patient and physician results from the population-based multinational assessment of psoriasis and psoriatic arthritis (MAPP) survey. Am J Clin Dermatol. 2016;17(1):87–97. doi:10.1007/s40257-015-0169-x
4. Diotallevi F, Campanati A, Martina E, et al. The role of nutrition in immune-mediated, inflammatory skin disease: a narrative review. Nutrients. 2022;14:3. doi:10.3390/nu14030591
5. Atak MF, Kundakci N, Farabi B. Link between childhood tobacco exposure and childhood psoriasis: a case-control study. Pediatr Dermatol. 2022;39(1):49–54. doi:10.1111/pde.14896
6. Diotallevi F, Simonetti O, Rizzetto G, Molinelli E, Radi G, Offidani A. Biological treatments for pediatric psoriasis: state of the art and future perspectives. Int J Mol Sci. 2022;23:19. doi:10.3390/ijms231911128
7. Kaushik SB, Lebwohl MG. Psoriasis: which therapy for which patient: focus on special populations and chronic infections. J Am Acad Dermatol. 2019;80(1):43–53. doi:10.1016/j.jaad.2018.06.056
8. Brembilla NC, Senra L, Boehncke WH. The IL-17 family of cytokines in psoriasis: IL-17A and beyond. Front Immunol. 2018;9(AUG). doi:10.3389/fimmu.2018.01682
9. Gałecka M, Bliźniewska-Kowalska K, Orzechowska A, et al. Inflammatory versus anti-inflammatory profiles in major depressive disorders—the role of il-17, il-21, il-23, il-35 and foxp3. J Pers Med. 2021;11(2):1–14. doi:10.3390/jpm11020066
10. Wierzbowska‐drabik K, Lesiak A, Skibińska M, Niedźwiedź M, Kasprzak JD, Narbutt J. Psoriasis and atherosclerosis—skin, joints and cardiovascular story of two plaques in relation to the treatment with biologics. Int J Mol Sci. 2021;22:19. doi:10.3390/ijms221910402
11. M Griffiths CE, Armstrong AW, Gudjonsson JE, Barker JN. Psoriasis; 2021. Available from: www.thelancet.com.
12. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
13. Kara T, Topkarcı Z, Yılmaz S, Akaltun İ, Erdoğan B. Pediatric patients with psoriasis and psychiatric disorders: premorbidity and comorbidity in a case-control study. J Dermatol Treat. 2019;30(2):129–134. doi:10.1080/09546634.2018.1476653
14. Dalgard FJ, Gieler U, Tomas-Aragones L, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European Countries. J Invest Dermatol. 2015;135(4):984–991. doi:10.1038/jid.2014.530
15. Cheng BT, Silverberg JI. Association of pediatric atopic dermatitis and psoriasis with school absenteeism and parental work absenteeism: a cross-sectional United States population-based study. J Am Acad Dermatol. 2021;85(4):885–892. doi:10.1016/j.jaad.2021.02.069
16. Kelly KA, Balogh EA, Kaplan SG, Feldman SR. Skin disease in children: effects on quality of life, stigmatization, bullying, and suicide risk in pediatric acne, atopic dermatitis, and psoriasis patients. Children. 2021;8:11. doi:10.3390/children8111057
17. Datta D, Sarkar R, Podder I. Parental stress and quality of life in chronic childhood dermatoses: a review. J Clin Aesthet Dermatol. 2021;14(9Suppl 1):S19.
18. Salek MS, Jung S, Brincat-Ruffini LA, et al. Clinical experience and psychometric properties of the children’s dermatology life quality index (CDLQI), 1995–2012. Br J Dermatol. 2013;169(4):734–759. doi:10.1111/BJD.12437
19. Menter A, Cordoro KM, Davis DMR, et al. Joint American Academy of Dermatology–National Psoriasis Foundation guidelines of care for the management and treatment of psoriasis in pediatric patients. J Am Acad Dermatol. 2020;82(1):161–201. doi:10.1016/j.jaad.2019.08.049
20. Lavaud J, Mahé E. Severity scores for childhood psoriasis: a systematic literature review. Ann Dermatol Venereol. 2019;146(12):771–782. doi:10.1016/j.annder.2019.03.007
21. Burden-Teh E, Murphy R, Gran S, et al. Identifying the best predictive diagnostic criteria for psoriasis in children (< 18 years): a UK multicentre case–control diagnostic accuracy study (DIPSOC study)*. Br J Dermatol. 2022;186(2):341–351. doi:10.1111/bjd.20689
22. Nourmohammadpour P, Ehsani AH, Hatami P, et al. Do clinical severity scores correlate with the quality of life in children with psoriasis? A cross-sectional study of Iranian pediatric patients. Pediatr Dermatol. 2022;39(2):211–214. doi:10.1111/pde.14891
23. Bruins FM, Bronckers IMGJ, Groenewoud HMM, van de Kerkhof PCM, de Jong EM, Seyger MMB. Association between quality of life and improvement in psoriasis severity and extent in pediatric patients. JAMA Dermatol. 2020;156(1):72–78. doi:10.1001/jamadermatol.2019.3717
24. Basra MKA, Gada V, Ungaro S, Finlay AY, Salek SM. Infants’ dermatitis quality of life index: a decade of experience of validation and clinical application. Br J Dermatol. 2013;169(4):760–768. doi:10.1111/BJD.12563
25. Langley RGB, Feldman SR, Nyirady J, van de Kerkhof P, Papavassilis C. The 5-point Investigator’s Global Assessment (IGA) scale: a modified tool for evaluating plaque psoriasis severity in clinical trials. J Dermatolog Treat. 2015;26(1):23–31. doi:10.3109/09546634.2013.865009
26. Seyger MMB, Augustin M, Sticherling M, et al. Physician-reported clinical unmet needs, burden and treatment patterns of paediatric psoriasis patients: a US and EU real-world evidence study. Acta Derm Venereol. 2022;102:adv00660. doi:10.2340/actadv.v101.981
27. Zamberk P, Velázquez D, Campos M, Hernanz JM, Lázaro P. Paediatric psoriasis - Narrowband UVB treatment. J Eur Acad Dermatol Venereol. 2010;24(4):415–419. doi:10.1111/j.1468-3083.2009.03425.x
28. Veith WB, Deleo VA, Silverberg NB. Medical phototherapy in childhood skin diseases. Minerva Pediatr. 2011;63(4):327–333.
29. Sadowska M, Narbutt J, Skibińska M, Lesiak A. Pros and cons of using systemic Acitretin in the paediatric population. Postepy Dermatol Alergol. 2022;39(1):34–38. doi:10.5114/ADA.2020.98558
30. Sahin G, Aydin F, Yuksel EP. Systemic treatments in pediatric psoriasis: a retrospective single-center study. Arch Iran Med. 2021;24(12):903–909. doi:10.34172/aim.2021.135
31. Hebert AA, Browning J, Kwong PC, Duarte AM, Price HN, Siegfried E. Managing pediatric psoriasis: update on treatments and challenges—a review. J Dermatol Treat. 2022;33(5):2433–2442. doi:10.1080/09546634.2022.2059051
32. Sticherling M, McPherson T, de Lucas Laguna R, et al. Patient characteristics and treatment patterns in European pediatric patients with psoriasis: a real-world, cross-sectional study. Dermatol Ther (Heidelb). 2022;12(8):1793–1808. doi:10.1007/s13555-022-00761-7
33. Marques E, Paluch Z, Boháč P, Slanař O, Běláček J, Hercogová J. The safety profile of biologic agents in comparison with non-biologic systemic agents, and topical compounds in the management of psoriasis—a 30-month prospective, observational cohort study. Int J Clin Pract. 2021;75:12. doi:10.1111/ijcp.14915
34. Sun HY, Phan K, Paller AS, Sebaratnam DF. Biologics for pediatric psoriasis: a systematic review and meta-analysis. Pediatr Dermatol. 2022;39(1):42–48. doi:10.1111/pde.14870
35. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris – part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317. doi:10.1111/jdv.16926
36. Cai XC, Ru Y, Liu L, et al. Efficacy and safety of biological agents for the treatment of pediatric patients with psoriasis: a Bayesian analysis of six high-quality randomized controlled trials. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.896550
37. Arican O, Aral M, Sasmaz S, Ciragil P. Serum levels of TNF-α, IFN-γ, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients with active psoriasis and correlation with disease severity. Mediators Inflamm. 2005;2005(5):273–279. doi:10.1155/MI.2005.273
38. Meehan EV, Wang K. Interleukin-17 family cytokines in metabolic disorders and cancer. Genes. 2022;13:9. doi:10.3390/genes13091643
39. Blauvelt A, Chiricozzi A. The immunologic role of IL-17 in psoriasis and psoriatic arthritis pathogenesis. Clin Rev Allergy Immunol. 2018;55(3):379–390. doi:10.1007/s12016-018-8702-3
40. Eshwar V, Kamath A, Shastry R, Shenoy AK, Kamath P. A review of the safety of interleukin-17A inhibitor secukinumab. Pharmaceuticals. 2022;15(11):1365. doi:10.3390/ph15111365
41. Akimzhanov AM, Yang XO, Dong C. Chromatin remodeling of interleukin-17 (IL-17)-IL-17F cytokine gene locus during inflammatory helper T cell differentiation. J Biol Chem. 2007;282(9):5969–5972. doi:10.1074/jbc.C600322200
42. Gaffen SL. Structure and signalling in the IL-17 receptor family. Nat Rev Immunol. 2009;9(8):556–567. doi:10.1038/nri2586
43. von Stebut E, Reich K, Thaçi D, et al. Impact of secukinumab on endothelial dysfunction and other cardiovascular disease parameters in psoriasis patients over 52 weeks. J Invest Dermatol. 2019;139(5):1054–1062. doi:10.1016/j.jid.2018.10.042
44. Gottlieb AB, Deodhar A, McInnes IB, et al. Long-term safety of secukinumab over five years in patients with moderate-to-severe plaque psoriasis, psoriatic arthritis and ankylosing spondylitis: update on integrated pooled clinical trial and post-marketing surveillance data. Acta Derm Venereol. 2022;102:adv00698. doi:10.2340/actadv.v102.563
45. Bodemer C, Kaszuba A, Kingo K, et al. Secukinumab demonstrates high efficacy and a favourable safety profile in paediatric patients with severe chronic plaque psoriasis: 52-week results from a Phase 3 double-blind randomized, controlled trial. J Eur Acad Dermatol Venereol. 2021;35(4):938–947. doi:10.1111/jdv.17002
46. Magnolo N, Kingo K, Laquer V, et al. Efficacy of secukinumab across subgroups and overall safety in pediatric patients with moderate to severe plaque psoriasis: week 52 results from a phase iii randomized study. Pediatric Drugs. 2022;24(4):377–387. doi:10.1007/s40272-022-00507-0
47. Magnolo N, Kingo K, Laquer V, et al. A phase 3 open-label, randomized multicenter study to evaluate efficacy and safety of secukinumab in pediatric patients with moderate to severe plaque psoriasis: 24-week results. J Am Acad Dermatol. 2022;86(1):122–130. doi:10.1016/j.jaad.2021.08.066
48. Huang IH, Yu CL, Tai CC, Tu YK, Chi CC. Biologics for pediatric moderate-to-severe plaque psoriasis: a systematic review and network meta-analysis. JDDG. 2022;20(9):1201–1209. doi:10.1111/ddg.14832
49. Golhen K, Winskill C, Theiler M, et al. Understanding efficacy-safety balance of biologics in moderate-to-severe pediatric psoriasis. Front Med. 2022;9. doi:10.3389/fmed.2022.944208
50. Di Lernia V, Macca L, Peterle L, Ingrasciotta Y, Trifirò G, Guarneri C. Efficacy of systemic biologic drugs in pediatric psoriasis: evidence from five selected randomized clinical trials. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.847308
51. Bardowska K, Krajewski PK, Tyczyńska K, Szepietowski JC. Safety evaluation of secukinumab in pediatric patients with plaque psoriasis. Expert Opin Drug Saf. 2022;21(7):867–872. doi:10.1080/14740338.2022.2073349
52. Narbutt J, Reich A, Adamski Z, et al. Psoriasis in children. Diagnostic and therapeutic recommendations of the polish dermatological society. Part 2. Przegl Dermatol. 2021;108(5):335–353. doi:10.5114/DR.2021.111962
53. NICE. Secukinumab for treating moderate to severe plaque psoriasis in children and young people. Guidance NICE. Available from: https://www.nice.org.uk/guidance/ta734.
54. Peris K, Fortina AB, Bianchi L, et al. Update on the management of pediatric psoriasis: an Italian consensus. Dermatol Ther (Heidelb). 2022;12(8):1753–1775. doi:10.1007/s13555-022-00758-2
55. Narbutt J, Reich A, Adamski Z, et al. Psoriasis in children. Diagnostic and therapeutic recommendations of the polish dermatological society. Part 1. Przegl Dermatol. 2021;108(4):239–257. doi:10.5114/DR.2021.110913
56. Nishida M, Takeichi T, Kono M, et al. Successful secukinumab treatment of recalcitrant juvenile generalized pustular psoriasis. J Dermatol. 2020;47(3):e77–e78. doi:10.1111/1346-8138.15228
57. Köstner K, Prelog M, Almanzar G, Fesq H, Haas JP, Hügle B. Successful use of secukinumab in a 4-year-old patient with deficiency of interleukin-36 antagonist. Rheumatology. 2018;57(5):936–938. doi:10.1093/RHEUMATOLOGY/KEX510
58. Hou RH, Wen XT, Wang Q, Wang L. Using secukinumab in a patient with endplate inflammation complicated by hepatitis B virus infection. Chin Med J. 2021;134(21):2644–2646. doi:10.1097/CM9.0000000000001801
59. Albela H, Begum S, Leong KF. Successful treatment of paediatric generalized pustular psoriasis with secukinumab: a case series. J Dermatolog Treat. 2022;33(3):1769–1773. doi:10.1080/09546634.2021.1899111
60. Ruan SF, Zhang LL, Liu Z, et al. Real-world data on the clinical use of secukinumab in pediatric generalized pustular psoriasis: a 48-week retrospective study. J Am Acad Dermatol. 2023;88:1. doi:10.1016/J.JAAD.2022.04.064
61. Craiglow BG, Boyden LM, Hu R, et al. CARD14 – associated Papulosquamous Eruption (CAPE): a spectrum including features of psoriasis and pityriasis Rubra pilaris. J Am Acad Dermatol. 2018;79(3):487. doi:10.1016/J.JAAD.2018.02.034
62. Subramani D, Sardana G, Kothari R, Gupta A. Secukinumab significantly reduces inflammation but only mildly improves scaling in four cases of autosomal recessive congenital ichthyosis. Clin Exp Dermatol. 2022;47:12. doi:10.1111/CED.15373
63. Lefferdink R, Rangel SM, Chima M, et al. Secukinumab responses vary across the spectrum of congenital ichthyosis in adults. Arch Dermatol Res. 2022. doi:10.1007/S00403-022-02325-3
64. Brunner HI, Foeldvari I, Alexeeva E, et al. Secukinumab in enthesitis-related arthritis and juvenile psoriatic arthritis: a randomised, double-blind, placebo-controlled, treatment withdrawal, phase 3 trial. Ann Rheum Dis. 2023;82:1. doi:10.1136/ARD-2022-222849
65. Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17:1. doi:10.1186/s12913-017-2031-8
66. Schaap MJ, Broekhuis SCE, Spillekom-van Koulil S, Groenewoud HMM, de Jong EMGJ, Seyger MMB. Treatment goals and preferences of pediatric psoriasis patients, young adults, and parents. J Dermatol Treat. 2022;33(5):2527–2533. doi:10.1080/09546634.2021.1985058
67. Fisher S, Ziv M. Skin and soft tissue infections in biological therapy for psoriasis-A case report and systematic review of the literature. Int J Dermatol. 2021;60(11):1429–1434. doi:10.1111/IJD.15679
68. Sánchez Martín M, Amores Hernández I, Argumánez García D, et al. Staphylococcal toxic shock syndrome in a child with interleukin-17 inhibitor treatment for psoriasis. Pediatr Dermatol. 2020;37(5):952–954. doi:10.1111/PDE.14228
69. Shah V, Taddio A, McMurtry CM, et al. Pharmacological and combined interventions to reduce vaccine injection pain in children and adults: systematic review and meta-analysis. Clin J Pain. 2015;31(10 Suppl):S38–S63. doi:10.1097/AJP.0000000000000281
70. Eichenfield LF, Ahluwalia J, Waldman A, Borok J, Udkoff J, Boguniewicz M. Current guidelines for the evaluation and management of atopic dermatitis: a comparison of the Joint Task Force practice parameter and American Academy of Dermatology guidelines. J Allergy Clin Immunol. 2017;139(4):S49–S57. doi:10.1016/j.jaci.2017.01.009
71. Schneeweiss MC, Huang JT, Wyss R, Schneeweiss S, Merola JF. Serious infection risk in children with psoriasis on systemic treatment: a propensity score-matched population-based study. J Am Acad Dermatol. 2020;82(6):1337–1345. doi:10.1016/j.jaad.2020.02.065
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.