Back to Journals » Hepatic Medicine: Evidence and Research » Volume 15
Secondary Sclerosing Cholangitis After SARS-CoV2: ICU Ketamine Use or Virus-Specific Biliary Tropism and Injury in the Context of Biliary Ischemia in Critically Ill Patients?
Authors Bartoli A ![]() , Cursaro C, Seferi H, Andreone P
, Cursaro C, Seferi H, Andreone P ![]()
Received 20 January 2023
Accepted for publication 12 July 2023
Published 1 August 2023 Volume 2023:15 Pages 93—112
DOI https://doi.org/10.2147/HMER.S384220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Alessandra Bartoli,1,2 Carmela Cursaro,1 Hajrie Seferi,1 Pietro Andreone3,4
1Division of Internal Medicine and Metabolism, Department of Internal Medicine, Ospedale Civile di Baggiovara, University of Modena and Reggio Emilia, Modena, Italy; 2Post Graduate School of Allergy and Clinical Immunology, Department of Internal Medicine, University of Modena and Reggio Emilia, Modena, Italy; 3Chief of Division of Internal Medicine and metabolism, Department of Internal Medicine, University Hospital of Modena, Modena, Italy; 4Chief of Post Graduate School of Allergy and Clinical Immunology, Department of Internal Medicine, University of Modena and Reggio Emilia, Modena, Italy
Correspondence: Alessandra Bartoli, University of Modena and Reggio Emilia, Ospedale Civile di Baggiovara, Via Pietro Giardini 1355, Baggiovara, MO, 41126, Italy, Email [email protected]
Purpose: From the beginning of the Severe Acute Respiratory Syndrome CoronaVirus-2 (SARS-CoV2) pandemic, different cases of a cholangiopathy with features of secondary sclerosing cholangitis in critically ill patients (SSC-CIP) have been reported. Patients developing it are generally recovering from severe Coronavirus disease 19 (COVID-19) and required intensive care unit (ICU) admission and mechanical ventilation. Many of them have been administered with ketamine during their ICU stay. The pathogenesis of this novel disease is still debated, and, since prognosis is poor, efforts are needed in order to better understand it.
Patients and Methods: In this review, we focused our attention on COVID-19 SSC clinical, imaging, and histology findings in order to clarify the different pathogenetic options, particularly in regard of the ischemic-direct viral damage and ketamine-related theories, beginning with a recapitulation of SSC-CIP and ketamine-induced cholangiopathy in abusers. The research has been conducted using PubMed and Google Scholar databases. Key-words were “Secondary Sclerosing Cholangiopathy”, “SSC-CIP”, “Secondary Sclerosing Cholangiopathy in critically ill patients”, “Ketamine and cholangiopathy”, “Ketamine abusers and liver disease”, “Ketamine-related cholangiopathy”, “SARS-CoV2 infection and liver disease”, “post Covid-19 secondary sclerosing cholangitis”, “Covid-19 cholangiopathy”.
Results: Many authors, based on the clinical, histological, imaging, and prognostic features of the disease, have pointed out the similarities between post COVID-19 SSC and SSC-CIP; however, peculiar features in the former were not previously observed. Therefore, a direct viral cytopathic action and SARS-CoV2-related coagulopathy are considered the most likely causes. On the other hand, ketamine, with the available data, cannot be surely linked as the main determinant cause of cholangiopathy. Moreover, ketamine-induced cholangitis (KIC) presentation is different from post COVID-19 SSC. Its role as a cofactor precipitating the disease cannot be ruled out.
Conclusion: Post COVID-19 SSC is a rare clinical entity following severe COVID-19 disease. The most accepted theory is that a sum of different insults determines the disease: biliary ischemia, direct viral damage, toxic bile, possibly worsened by ketamine and hyperinflammation due to the cytokine storm. Given the severe prognosis of the disease, with persistent cholangiopathy, organ failure, and orthotopic liver transplantation (OLT), further study on this novel clinical entity is needed.
Keywords: SARS-CoV2, cholangiopathy, secondary sclerosing cholangiopathy, ICU, SSC-CIP, ketamine, COVID-19 coagulopathy, direct viral damage
Introduction
From December 2019 a new pandemic spreading all around the world is responsible for millions of deaths and morbidity. Coronavirus disease 19 (COVID-19) is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV2), a β-coronavirus isolated for the first time in Wuhan, China. COVID-19 is typically characterized by respiratory symptoms, culminating in bilateral interstitial pneumonia followed, in the most severe cases, by an abnormal activation of the immune system. This cytokine storm, if not controlled, can determine tremendous consequences such as ARDS, heart failure, acute renal insufficiency, liver failure, and death.1
In hospitalized COVID-19 patients, a mild-moderate elevation of liver enzyme is frequent (14–58% of cases), with aspartate aminotransferase (AST) reaching higher values than alanine aminotransferase (ALT).2 Transaminase elevation is generally observed at the beginning of hospital stay, with an improvement during hospitalization.3–5 The increase of transaminases and total bilirubin is known to be a risk factor for poor outcome in severe COVID-19.6
Twelve percent of patients show an increase in cholestasis markers.2,5 The prevalence of severe cholangiopathies in COVID-19 patients varies depending on case series. In mechanically ventilated ones it can reach 4%, in other series 1%.7,8
SARS-CoV2 enters the cells through the angiotensin I converting enzyme 2 (ACE-2) receptor, and transmembrane serine protease 2 (TMPRSS2) is used for viral spike (S) protein priming. Expression of ACE-2 receptors is quite ubiquitous and can be found in tissues other than lungs and endothelium, such as gastrointestinal tract, hepatobiliary, renal, and cardiovascular systems, and pancreas. Differently from hepatocytes, cholangiocytes widely express ACE-2 receptors (2.6% vs 59.7%). For this reason, cholangiocytes may become a possible direct viral target.9–11 SARS-CoV2 virions can enter the biliary cells via blood or gut.12 Viral inclusions and SARS-CoV2 RNA have been isolated not only in hepatocytes but also in cholangiocytes in autoptic studies.12–16 Moreover, it was recently demonstrated that SARS-CoV2 can invade and replicate in organoids derived from human intrahepatic biliary epithelial cells (BECs) even if it is not known if the virus is able to replicate there in vivo.17 Infected organoids showed an augmented expression of genes associated to cell death induction and a reduction of protective mechanisms with the down-regulation of genes expressing for tight junction integrity, epithelial cell barrier, and biliary transport.18
Coagulopathy is a hallmark of severe COVID-19, and interleukin 6 (IL-6) is thought to be the key point. Therefore, a group of researchers studied its influence in COVID-19 vascular liver damage. IL-6 interacts with cells not representing its typical target through the trans-signaling pathway. Among these cells, liver sinusoidal endothelial cells (LSECs), stimulated by IL-6, determine the production of high amounts of pro-inflammatory mediators (chemokine C-X-C ligand 1–2, IL-6), procoagulant factors (factor VIII and von Willebrand factor), and adhesion molecules (P and E-selectin, intercellular adhesion molecule 1) mediating neutrophil recruitment and platelet aggregation and attachment.16
Since the pandemic beginning, several patients have developed, after severe COVID-19 disease, a cholangiopathy resemblant to secondary sclerosing cholangitis in critically ill patients (SSC-CIP), frequently requiring orthotopic liver transplantation (OLT) since no medical therapy seems to be effective.19 The pathogenesis of this so-called post COVID-19 secondary sclerosing cholangitis (SSC) is still a matter of debate. On one hand, many authors have noticed similarities between SSC-CIP and post COVID-19 SSC, suggesting a common genesis, related to biliary ischemia; on the other hand, some authors have noticed a possible association between post COVID-19 SSC and ketamine use in intensive care units (ICU).3,5,7,8,12,20–29
In this review we focused our attention on COVID-19 SSC clinical, imaging, and histological findings in order to clarify the different pathogenetic options, particularly with regard to the ischemic and direct viral damage hypothesis and ketamine-related pathogenic option, beginning with a recapitulation of SSC-CIP and ketamine-related cholangiopathy, considering literature reviews, case reports, series, and clinical studies performed on these topics.
Secondary Sclerosing Cholangitis in Critically Ill Patients (SSC-CIP)
Definition
Sclerosing cholangitides are a group of cholestatic diseases affecting intra- and extrahepatic bile ducts that can progress until liver cirrhosis. The group accounts for different clinical entities, ranging from primary sclerosing cholangitis to secondary sclerosing cholangitis (SSC). The latter can be due to different etiologies, such as infections, ischemia of the bile ducts, IgG4-related disease, drug-induced, and biliary obstruction.30 SSC-CIP is a recently identified form of SSC observed in patients with no previous liver disease, following long hospitalizations in ICU due to heterogeneous causes such as polytrauma, burn injury, cardiothoracic surgery, severe pneumonia, infections, sepsis, and bleeding after abdominal surgery. SSC-CIP rate is estimated at 1:2000 patients in the ICU; however, it is an underdiagnosed entity since half of the affected patients die during the ICU stay.31,32 It was first described in 2001 by Scheppach et al.33
Risk Factors
Patients’ common features are prolonged hospitalization in ICU, with a median need for mechanical ventilation of 30–40 days, positive end expiratory pressions (PEEP) superior to 10 cm H2O, prone positioning, and the use of vasopressors in order to sustain circulation due to a low mean blood pressure (65 mmHg) with prolonged hypotensions. The association of ventilation with high PEEP, low tidal volume, and prone positioning can lead, in critical patients, to a decrease in splanchnic blood flow with consequent biliary ischemia, which is aggravated by hypercoagulable states and blood hyperviscosity.31–34
Patients
The mean age of patients at diagnosis is 50 years with a prevalence of male sex (1.3:1 to 9:1, depending on case series).32,34 Weig et al reported a series of patients with acute respiratory distress syndrome (ARDS) due to H1N1 pneumonia and remarked that obesity, visceral fat, and prone positioning during mechanical ventilation were associated with an augmented risk of SSC-CIP.35 Kirstein et al reported that a lower C reactive protein (CRP) was associated with a prolonged OLT-free survival, whereas older age was a negative prognostic factor for OLT-free survival.32 Voigtländer et al in a multivariate analysis of a group of 54 SSC-CIP patients showed that an increased Model for Endstage Liver Disease (MELD) score and the need for renal replacement therapy represented independent risk factors for mortality in SSC-CIP patients.36
SSC-CIP has generally two different patterns of presentation: acute liver failure during ICU stay, or persistent cholestasis rapidly progressing to cirrhosis.34
Pathogenesis
The exact pathological mechanism remains unknown, but it seems that a co-participation of factors may explain disease genesis: ischemia of the bile ducts, toxic bile, and biliary infections are the main risk factors considered. These factors seem responsible for biliary cast formation, biliary obstructions, and necrosis, leading to an irreversible and progressive subversion of the biliary tree, destruction and obliteration of intrahepatic bile ducts, ending with cirrhosis.31,37–39
Hepatocytes receive blood by both hepatic arteries and portal vein; the common bile duct (CBD) is vascularized by branches of gastroduodenal and hepatic arteries, while the intrahepatic biliary tree receives its blood supply only from the peribiliary plexus, composed of branches of the hepatic arteries, so it is much more sensitive to ischemia and to the reduction of splanchnic blood pressure.40–42 The ischemic hypothesis is supported by the experience of liver transplantation (LT). A complication of LT is hepatic artery thrombosis, and when this happens bile duct necrosis can be observed.43,44 Epithelial necrosis determines bile cast formation.34 Two types of casts have been differentiated: one is mainly constituted of bilirubin (10–50%) and bile acids (10–15%) and is supposedly derived from mechanical obstruction; the other type is mainly composed of proteins (particularly collagen), which supports the hypothesis of a biliary necrosis derivation.43,44 Biliary casts in SSC-CIP are mainly composed of proteins and appear in the early weeks after cholestasis onset.38 Biliary casts are pathognomonic of SSC-CIP.31,34
The second risk factor to consider is the toxic bile. The disruption of cholangiocytes' protective mechanisms may lead to their destruction by bile acids. In normal conditions, in order to protect the lipid membrane of cholangiocytes by hydrophobic bile acids, hepatocytes secrete phospholipids via the transporter lipid export pump multidrug resistance protein 3 (MDR3)/ATP Binding Cassette Subfamily B Member 4 (ABCB4) producing mixed micelles with bile acids.45,46 Genetic defects of this transporter cause cholestatic and ductopenic liver disease.47 Also, biliary cells secrete bicarbonate via the transporter anion exchanger 2 (AE2) with the formation of an alkaline bicarbonate film to protect the apical surface of cholangiocytes.48 It has been hypothesized that patients with variants of MDR3 pump may be predisposed to develop toxic bile in presence of favorable conditions such as ischemia and inflammatory stress.45
In SSC-CIP, biliary casts cause biliary duct obstruction. Biliary obstructions predispose to infections, failing the antibacterial effect of bile flow and local immunoglobulins A (IgA) secretion.49 Biliary infections sustain local inflammation and parenchymal disruption.34 SSC-CIP patients suffer from hepato-biliary infections, and 98% of them have bile specimens positive for bacteria (enterococci in first place) and candida species.50,51
Differential diagnoses to SSC-CIP are cholestasis due to sepsis, drug-induced liver injury (DILI) with cholestatic pattern, and cholangitis due to choledocholithiasis.46,52 DILI is an interesting option since many drugs used in the ICU setting are known to be potentially hepatotoxic, and among them antibiotics and anesthetics like ketamine are debated.31,53,54
Biochemical and Histological Features
At blood tests, gamma glutamyl transferase (GGT) rises first, after a median of 7–9 days from the initial insult, rapidly followed by alkaline phosphatase (AP). Bilirubin is the last to increase. GGT reaches values 20–50 times higher than the upper limit of normal (ULN). AP reaches values 5–21 times ULN, and bilirubin 3–39 times ULN.31,55 Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are only mildly augmented.56 After some months from disease beginning, bilirubin can spontaneously decrease, while the disease keeps progressing.57 At initial phases symptoms are rare, but, with disease progression, patients may present jaundice, pruritus, upper right abdominal quadrant pain, and recurrent biliary infections. Weight loss is common.31
In SSC-CIP, cholestasis with biliary parenchyma disruption persists after the resolution of the acute phase and the discharge from ICU, and this differentiates SSC-CIP from DILI, ischemic hepatitis, and sepsis-induced cholestasis.46,58
Imaging is fundamental for the diagnosis, and endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard, but also magnetic resonance cholangiopancreatography (MRCP) can be considered, since it is non-invasive.31,37 Abdominal ultrasonography (US) has a low sensitivity (30%).59 The common initial findings at ERCP are ribbon-like intraductal filling defects, produced by biliary casts. In later stages typical findings are bile duct strictures and dilatations, bile duct walls with beaded appearance and thickening, with final architectural destruction of intrahepatic bile ducts, generally sparing the CBD. In the final stages, peripheral intrahepatic bile ducts are completely obliterated, producing an image of a pruned tree since only the central intrahepatic biliary tree can be identified.31 Notably, the distal CBD is preserved at all stages, and 20% of patients have minor extrahepatic disease. In 6% of SSC-CIP patients, the strictures are confined to the extrahepatic bile ducts.31,34
The disease progression is fast; in fact Leonhardt et al showed that 88% of patients in their series had imaging features of cirrhosis within 6 months from SSC-CIP diagnosis.31
Typical histological findings at early stages are chronic bile duct obstruction and edema of portal and periportal tracts, mild inflammatory infiltrates majorly composed of lymphocytes and minorly by neutrophils and cytological alterations in the interlobular bile ducts as cytoplasmic vacuolization. Gelban et al and Leonhardt et al noticed that at earlier stages there were features of bile duct obstruction such as periportal bile duct infarcts, perivenular bilirubinostasis with bile plugins, and dilatated canaliculi.31,38,60 After 4–12 months, biopsies showed bile duct proliferation, portal inflammatory infiltrate, and portal and periductular fibrosis.38,57,60 Only in later stages could hepatocellular rosettes and cholestatic necrosis be observed, with eventual progression to biliary fibrosis and secondary biliary cirrhosis.61
Therapy
Patients are generally treated with ursodeoxycholic acid (UDCA) without frank improvements. Broad-spectrum antibiotics are used for the infections.34,57 ERCP with cast and sludge extraction, endoscopic dilatations, sphincterotomy of Oddi sphincter, and intermittent stenting are routinely performed with temporal reduction in bilirubin and AP levels but short-term clinical improvement.38,39 These measures, combined with UDCA therapy are not resolutive and do not seem to alter the natural history of the disease.34 Patients seem to be divided into two main groups: those who do not survive the critical phase during ICU stay and those who survive it, in whom the disease tends to become chronic and to evolve towards biliary cirrhosis and to the need, in most cases, for OLT evaluation.32 Up to 75% of patients need liver transplantation (LT) evaluation during the first year from disease diagnosis.31 Mortality rate is very high; in Voigtländer study half of the 54 patients died, and six required LT.36 Kulaksiz et al reported a one-year transplantation-free survival of 55%, reduced to 14% at 6 years with liver failure as the most frequent cause of death.62 In a more recent retrospective analysis performed by Kirstein et al, the median OLT-free survival of a group of 111 patients with SSC-CIP was 16 months.32
Leonhardt et al, in their report about 16 patients with SSC-CIP, showed a one-year survival rate after LT of 85%.31 In a retrospective study by Kirchner et al, seven out of eleven patients survived after OLT. Sepsis was the main cause of death in transplanted patients. The 1, 3, and 5-year-survival rates were 64%.63 Voigtländer et al also reported the outcomes of 21 SSC-CIP patients who underwent LT. Six out of 21 died, and sepsis was the main cause of death. In this case the 1, 3, and 5-year survival rates were 100%, 86%, and 76%.64
Ketamine-Induced Cholangiopathy (KIC) in Abusers
General Features
Ketamine is an N-methyl-D-aspartate (NMDA) non-competitive receptor antagonist used as a second-line agent in anesthesia. It is also used as a recreational drug, very popular among young people all around the world, given its psychedelic effects: floating sensation, vivid dreams, and hallucinations.65 Street ketamine is composed 30–90% of ketamine, cut with other substances such as paracetamol, flour, and aspirin. It is assumed injected, snorted, or swallowed, and it takes 10 minutes to act. Its action lasts up to two hours if taken orally.66 It is metabolized by P450 hepatic cytochrome by nitrogen demethylation to norketamine, a water-insoluble metabolite with a half-life of 2.5 hours. It is excreted, once glucurono-conjugated, 90% through urine and 10% through bile.67
Symptoms
The most diffuse long-term symptoms related to its chronic abuse are urinary tract dysfunctions (frequency, urgency, dysuria, hematuria, hydronephrosis, and chronic kidney injury) and secondly abdominal pain associated or not to cholestasis enzyme elevation with cholangitis.68 Talking about cholestasis, patients are usually asymptomatic at the initial stage, and they show enzyme alterations after 1 or 2 years of abuse. Thereafter, abdominal pain may appear, especially concomitant with drug intake.69
Wong et al described symptoms of a cohort of ketamine abusers, and among 297 patients 9.8% presented liver injury.70
Ng et al reported a series of 223 ketamine-addicted patients accepted at their emergency department; 21% had abdominal pain as major disturb, and liver function alterations could be noticed in 16% of patients.71
Pathogenesis
The mechanism through which ketamine determines cholestasis and cholangitis is uncertain, but different theories have been postulated. The blockade of NMDA receptors situated in smooth muscle cells could determine biliary tract dysfunction and dilatation with bile accumulation. Also, Oddi sphincter contraction could exacerbate biliary tract dilatation, increasing flow resistance, with consequent further bile stasis. Bile stasis could determine the precipitation of norketamine, and consequently biliary obstructions and cholangitis, with a possible toxic effect on biliary epithelium.54 Some animal studies have demonstrated that the blockade of NMDA receptors in the dorsal motor nucleus of the vagal nerve induced gallbladder dyskinesia.29,54
In ketamine cholangiopathy, GGT can reach values 30 times ULN, and AP and bilirubin 10 times ULN.29,54,72
Histological, Biochemical, and Imaging Features
Yu et al studied imaging and histological typical features of a group of ketamine abusers with cholestasis and abdominal pain; 100% of the group presented a dilatation of the CBD with distal narrowing, while no one had signs of intrahepatic bile ducts involvement. Patients achieving abstinence showed a reduction in CBD diameter. Alteration of cholestasis enzymes was typical and tended to respond to the cessation of ketamine abuse.72 Seto et al described the MRCP profiles of a group of 257 ketamine abusers. The mean drug exposure duration was 10.5 years; 159/257 patients (61.9%) had biliary system alterations, while 73/159 presented a diffuse extrahepatic dilatation pattern, 64/159 had a fusiform extrahepatic dilatation pattern, and only 22/159 showed isolated intrahepatic ductal anomalies.73
Considering some single case reports, alterations in the intrahepatic bile ducts could be found, such as dilatations and strictures, always accompanied by CBD dilatations.69,74–76
At liver biopsy, biliary epithelial disarray, periductal and portal fibrosis, lymphocytic cholangitis, and mild ductular reaction with proliferation of the small portal tracts were observed.54,69,72,77 In a liver sample, copper deposits were found.69
Lo et al described a patient, pointing out how, in their experience, the dilatation of CBD accompanied by abdominal pain and cholestasis enzyme alteration was temporary and recurrent in case of ketamine intake.54
Causes Other Than Ketamine Abuse
Even if the vast majority of reports about KIC refers to chronic drug abuse, also ketamine hospital use has been linked to the development of a cholangiopathy, in a minority of cases. Talking about its therapeutic potential, ketamine has been used as treatment for complex regional pain syndrome (CRPS).78 A few reports highlighted its effects, when infused at subanesthetic dosage, on the development of a cholangiopathy characterized by the CBD dilatation, GGP, AP, and bilirubin elevation, accompanied by abdominal pain. In general, this clinical entity tended to resolve after ketamine infusion cessation and was similar to that described in drug abusers.78–80
In 2017, the French national agency for drug safety issued an alert relating to the potential toxic liver effects of ketamine, if used for prolonged periods in ICU, or in case of off-label utilization, so the drug doses were restricted.81 In 2021, de Tymowsky et al compared patients mechanically ventilated due to severe burn injury and treated with ketamine, before its dose restrictions and after. A total of 219 patients who received ketamine in the liberal period (doses 1–3 mg/kg/h) and 74 subjects treated during the restrictive period (doses 0.01–0.05 mg/kg/h) were compared regarding cholangiopathy development. Patients’ severity was the same. Cholestasis at discharge was more prevalent in the first group (33% vs 20%), and 9 patients from the first group versus 1 from the second developed SSC-CIP. In this case the studied group was composed of critically ill patients who were treated in ICU, and ketamine was considered as an adjunctive hit precipitating the development of cholangiopathy.28
Prognosis and Treatment
Prognosis mainly depends on ketamine intake interruption. Enzyme elevation usually normalizes after ketamine cessation, as do biliary alterations, even if these ones do not always regress.69 Biliary stenting and Oddi papilla sphincterotomy were effective in some cases.76 Nyirenda et al reported a case of a chronic heavy ketamine consumer for decades, who presented with liver damage so advanced that even after abuse cessation, medical therapy, and biliary stenting, liver function could not be restored. In this case LT was the only option.74
Post COVID-19 Secondary Sclerosing Cholangitis (SSC)
General Features
Disease Definition and Risk Factors
This cholangiopathy is characterized by abnormal liver tests, in particular AP, GGT, and bilirubin, and to a lesser extent AST and ALT, accompanied by jaundice, pruritus, biliary tract imaging distortions, biliary casts, bile stasis, and liver function disruption.3,5–8,12,19–23,82
Patients developing post COVID-19 SSC are generally recovering from the acute phase of severe COVID-19 bilateral interstitial pneumonia, with an average time from COVID-19 diagnosis to cholangiopathy diagnosis of 118 days in an American case series.7 These patients have been hospitalized in ICU, have had acute hypoxemic respiratory insufficiency needing mechanical ventilation with high PEEPs (>10 cm H2O), prone-positioning, and the administration of a mix of different drugs such as vasopressor agents and, in some cases, extracorporeal membrane oxygenation (ECMO) and dialysis. Patients are majorly men with a mean age of 50.5 years, no pre-existing liver disease, or, at most, liver steatosis. Main comorbidities are hypertension, obesity, and diabetes, which are also risk factors for severe forms of COVID-19 disease.3,5–8,19–29,82–84
Concerning biochemistry, AST and ALT can moderately increase early, at hospital admission, with a normalization in the course of hospitalization. In a later stage, patients tend to show an increase in AP, GGT, and total bilirubin, often associated to jaundice. GGT and AP can reach values higher than 20–30 times ULN. Other causes of hepatic and biliary diseases, such as hepatotropic viruses and liver autoimmune diseases, were discarded.3,5–8,19–23,82–84
Radiological Features
At abdominal computed tomography (CT) and magnetic resonance imaging (MRI) the most commonly depicted features are dilatations and strictures of intrahepatic bile ducts with beaded appearance, bile duct thickening, and hyperenhancement; the dilatation of the CBD, sometimes accompanied by strictures, can be observed. Biliary casts are a typical finding.3,5–8,19–29,82–84
An interesting study on radiological features of 17 post COVID-19 SSC patients found intrahepatic bile duct strictures (17/17), with (10/17) or without upstream dilatations, and intrahepatic bile duct beading (14/17). Vanishing ducts were observed in 7 patients, bilobar for the major part. None of these patients had CBD dilatation, while 1 patient presented an extrahepatic bile duct stricture without upstream dilatation. Only 2 patients had biliary casts, and 1 had biliary abscesses. Also, some morphological liver changes were noticed, such as hepatomegaly (4/17) and structural liver changes (10/17). No vascular damage was observed. Only one-third of the observed group received ketamine during ICU sedation.85
Histology
Liver biopsies generally showed cellular infiltrate of portal tracts (rarely plasma cells, in most cases lymphocytes), portal, periportal, and bridging fibrosis, cholangiocyte cytoplasm vacuolization, and cholangiocyte necrosis in marginal ductules and in terminal bile ducts accompanied by regenerative changes. In some biopsy samples, cytokeratin 7 immuno-stain positivity highlighted ductular reaction.3,5,7,8,12,20–23,25,26,82,86 Concerning large bile ducts, in some reports, acute or chronic obstructions could be noticed as well as vascular damage, in the form of hepatic vein endo-phlebitis, hepatic artery endothelial swelling, and, in one patient, a focal sinusoidal obstruction syndrome.20
Treatment and Prognosis
UDCA, cholestyramine, and obeticholic acid were not able to arrest the disease progression.3,5,7,8,12,20–23,25,26,82,86 ERCP papilla sphincterotomy, bile sludge and cast extraction, and stenting resulted in some positive effects in few reports.87 Prognosis is poor with high mortality rates. Since no medical therapy is effective, OLT represents the most important therapeutic option.3,7,12,22
Cholangioscopy was useful to diagnose COVID-19 SSC since it let strictures and epithelial anomalies be observed. Koepfi and Franzini in fact highlighted the irregular and edematous biliary mucosa as sign of ischemic cholangiopathy in post COVID-19 SSC, similar to that of patients with ischemic complications after OLT, clues that support a possible ischemic genesis of the disease.88,89
Pathogenesis
The debate on the pathogenesis of this disorder is still open. The most accredited theory is that of a multifactorial disease, primarily bound to ischemia of the biliary tract leading to cholangiocyte necrosis and cast formation. Ischemia also determines toxic bile phenomena, precipitating the disease. Biliary tract ischemia in COVID-19 patients has been mainly linked to viral coagulopathy, endotheliopathy, cytokine storm, and splanchnic hypoperfusion and hypotension consequent to SARS-CoV2 severe pneumonia, mechanical ventilation with low tidal volumes, high PEEPs, prone positioning, and the use of vasopressors.11,12,16 COVID-19 hepatic microangiopathy is characterized by a three-compartment damage: portal vein phlebitis, hepatic artery endothelial swelling, and sinusoid obstruction syndrome, which is a hallmark of COVID-19 liver vasculopathy.3,20 In an autoptic series of 40 severe COVID-19 patients, Lagana et al found sinusoidal microthrombi in 15% of the specimens.90 At the same time, some authors have postulated a role of different drugs used during the ICU stay in the development of post COVID-19 SSC, particularly ketamine, given its effects on the biliary tree.26,28
Post COVID-19 SSC and SSC-CIP Similarities
Roth et al described 3 COVID-19 patients who developed post COVID-19 SSC after recovery from ARDS. The authors highlighted some features that this cholangiopathy had in common with SSC-CIP, particularly imaging, endoscopic findings in form of intrahepatic biliary tree dilatations and strictures, and histology with cholangiocyte necrosis, biliary epithelium destruction, ductular reaction, and progressive fibrosis of portal tracts with progression to secondary biliary cirrhosis. At liver biopsy, in fact, they observed extensive degenerative cholangiocyte injury with vacuolization and necrosis of the epithelial layer in terminal bile ducts and marginal ductules. The authors also described hepatic artery endothelial swelling with luminal narrowing and portal vein endophlebitis. One patient had a sinusoidal obstructive syndrome with pericentral confluent fibrosis. Also, biliary casts, pathognomonic of SSC-CIP, were typically found in COVID-19 SSC patients. There were also some differences that made post COVID-19 SSC a quite unique entity, such as cholangiocyte cytoplasm vacuolization, regenerative changes, and the vascular damages reported. In the authors' opinion COVID-19 SSC resembles SSC-CIP, and the differences may probably be bound to a direct SARS-CoV2 effect that in this case could not be proved since immunohistochemistry and in situ hybridization were negative for SARS-CoV2; polymerase chain reaction (PCR) thus was not performed.20
Mayorquin-Aguilar et al have reported three cases of post COVID-19 SSC. One patient was treated with ketamine during ICU stay. MRI and ERCP features were consistent with previous reports with intrahepatic biliary stenosis, accompanied in one case by CBD dilatation; biliary casts were removed in all three patients without improvement. At biopsy, the main features were regenerative changes, cholangiocyte swelling, and inflammatory infiltrates in portal vein and artery with fibrosis of portal spaces. Prognosis was poor with a patient on the list for OLT, one in palliative care due to sepsis complications, and the third dead. The authors found many similarities between their patients and those reported by Roth, concluding that COVID-19 SSC may represent a confluence between SSC-CIP and direct viral damage, even if a DILI, as aggravating factor, could not be discarded.86
A German retrospective multicenter study of 127 patients with a diagnosis of SSC by ERCP/MRI aimed to better trace the differences between SSC-CIP and COVID-19 SSC. Patients showed strictures and/or dilatations of the biliary system, rarefaction of biliary tree including contrast filling defects or detection of biliary casts. A total of 77 patients had SSC-CIP, 24 had post COVID-19 SSC, and 26 patients had other types of SSC.26 Of the total number of patients, 84 received UDCA 13.6 mg/kg, 94.5% received an ECRP, and 108 a sphincterotomy. Cast extraction was possible in 53% of patients. In COVID-19 patients, cholangitis was diagnosed a median of 91 days after COVID-19 diagnosis. Comparing the two groups, age, gender, and laboratory features were similar as well as symptoms and initial clinical findings. The COVID-19 SSC group was more likely to have diabetes and less coronary and cerebrovascular disease compared to the other group. Liver cirrhosis was rarely found upon diagnosis in COVID-19 SSC. Cholangitis occurred frequently in both groups.25
The median survival of the complete cohort was 22 months; 45 patients died, and 18 received an OLT (3 of them from the COVID-SSC group). OLT was performed after a median of 93 days from SSC diagnosis. Higher bilirubin levels were associated with a higher mortality in the two groups, while the use of UDCA was associated with an increased transplantation-free survival only in the SSC-CIP group. Treatment outcome did not significantly differ in the two groups.25
Butikofer et al performed a retrospective single-center cohort study comparing 34 severe COVID-19 ICU-admitted patients with 34 severe influenza ICU-admitted patients. The COVID-19 group developed severe cholestasis (9/34 vs 2/34) and SSC (4/34 vs 0/34) significantly more often than the control group. Patients from the COVID-19 group developing moderate and severe cholestasis had been treated with ketamine during their ICU stay, while none from the influenza group had received it. Diabetes was prevalent among patients with severe cholestasis and SSC. Severe cholestatic patients had had a significantly longer and more complicated disease course than those without it. Influenza patients were more severely affected than the COVID-19 group at ICU admission, but the length of their hospital stay was significantly shorter, and they had a lower need of prone positioning during ventilation. Of the COVID-19 group, 10/34 patients died. From the autoptic study of one patient from the severe cholestasis group, at liver sections, transmural necrosis in large and medium-sized perihilar bile ducts, hepatocyte necrosis, and fresh parenchymal infarcts were observed; portal vein thrombi were noticed even without evident endothelialitis. In two patients with severe cholestasis, later developing SSC, liver biopsy was performed and showed a cholestatic pattern with perihilar bile duct obstruction, similar to SSC-CIP histology. The authors associated these cases of COVID-19 SSC to SSC-CIP, due to clinical, radiological, and histological features. To explain the vascular damage observed in the deceased patients, a direct role of SARS-CoV2 was evoked.21
Post COVID-19 SSC and Ketamine
Different authors have noticed a possible link between post COVID-19 SSC and the use of ketamine during ICU stay.26–29 Severe COVID-19 patients were in fact more difficult to treat, and, to reach a deep sedation, first-line sedative and analgesics agents were associated to second-line ones and the most used was ketamine.26 Data about its toxicity are scarce, but it is known to be hepatotoxic if used at doses higher than 1 mg/kg/h for prolonged periods.91
Mallet et al described 5 patients with post COVID-19 SSC, linking it to the use of ketamine for sedation and stating that liver injury was dose-dependent and progressive and that total ketamine exposure correlated with the outcome, including liver-related deaths. In the report by Mallet et al, MRI features were those of sclerosing cholangitis with strictures and dilatations of the intrahepatic bile ducts, peribiliary cysts, and multiple biliary casts. At biopsy, biliary obstructions, biliary plugs, and inflammatory infiltrate in portal spaces were observed, accompanied by fibrosis and cirrhosis, in the two most severe patients. The authors speculated that over-exposure to ketamine led norketamine to precipitate in the biliary tree with toxic effects. They therefore hypothesized that the pathogenic mechanism could be more complex, so that ketamine could act as an adjunctive hit on an already injured biliary tract. The disease should not entirely be linked to ischemic phenomena, but other etiologies such direct viral damage and drug toxicity should be considered.26
Other authors responded to Mallet et al’s report highlighting that histologic damage and MRI and ERCP features of his patients were more in line with an ischemic origin. In fact, biliary casts and the rarefaction of intrahepatic biliary ducts without great changes in CBD had already been observed in patients suffering from ischemic cholangiopathy following liver transplantation and in those suffering from SSC-CIP. Also, patients’ medical history was in line with that of SSC-CIP subjects.24
At the time of these reports, in 2021, 24 patients with post COVID-19 SSC had been described and 10/24 received ketamine, while for the others the sedation protocol was not specified. Mallet et al further investigated the relationship between the dose of ketamine and bilirubin maximum peak in adult patients with ARDS due to COVID-19 in Paris. A total of 2258 patients were included. Patients were divided into two groups, based on ketamine infusion dose. Patients in the lower group were older and had more comorbidities and higher initial (CRP). Mortality was similar among the two groups. Ketamine was associated with jaundice, but its contribution to organ failure was not defined.27
As cited in the ketamine-induced cholangiopathy section, after the restriction of ketamine doses was imposed by the French national agency for drug safety, due to the potential toxic liver effects of ketamine, de Tymowsky et al, in the COVID era, compared the outcomes of patients mechanically ventilated due to severe burn injury treated with ketamine, before its dose restriction and after, in order to investigate a possible role of the drug in SSC development.28,81 Patient severity did not differ in the two groups. Cholestasis at discharge was more prevalent in the first group (33% vs 20%), and 9/219 patients from the first group versus 1/74 from the second developed SSC-CIP. The authors therefore speculated that ketamine had a causative role in COVID-19 SSC, since it was administered at doses higher than recommended. The authors also stated that ketamine had to be considered as a second hit on a liver already injured by direct viral damage, inflammation, and ischemia.28
In Zurich, Wendel-Garcia et al compared ARDS SARS-CoV2 patients treated with and without ketamine. A post-hoc analysis was made to observe if ketamine could be linked to the development of post COVID-19 SSC. The ketamine group (n=170) received ketamine at a rate of 1.4 (0.9–2) mg/kg/h for 9 (4–18) days. The ketamine-free group was composed of 73 patients. Ketamine patients had a higher sequential organ failure assessment (SOFA) score at intubation and a lower arterial pressure of oxygen/inspired oxygen fraction (P/F) ratio (140 mmHg vs 168 mmHg, p<0.001). A total of 100/170 subjects out of the ketamine group presented cholestatic liver injury, 67/100 of whom moderate and 33/100 severe. From the ketamine-free group, 14/73 patients developed a cholestatic liver injury, 13/14 of whom moderate and 1/14 severe. Ketamine was not associated with an increased hospital mortality. The mixed effects model showed a positively related infusion duration effect and a dose effect correlation between ketamine administration and rising bilirubin levels, with higher hazard of developing a cholestatic disease. Because of its design, this study could not prove a direct causal effect of ketamine on the histological damage. This study presents some limitations: the design, since it is not a randomized controlled clinical trial; and, second, a possible confounding effect due to the fact that patients treated with ketamine had also a more severe COVID-19 disease. Nevertheless, the specific model used in this study corrects for confounding factors such as disease severity.29
A group of colleagues from Dallas reported a case of a woman with severe COVID-19 who needed mechanical ventilation with long ketamine infusion, and 5 days after ketamine discontinuation she showed a slow but persistent rise in AP, GGT, AST, and ALT, which gradually reduced. Due to a staphylococcal pneumonia she had to be reintubated and received an adjunctive ketamine bolus. After that, AP and GGT rose again. MRCP carried out at AP peak showed a dilatated CBD with distal narrowing and beaded appearance of intrahepatic bile ducts. At liver biopsy the main findings were ductular reaction and lobular inflammation with a small non-necrotizing granuloma without viral inclusions. The authors diagnosed a ketamine-induced cholangitis. The clinical course was characterized by an improvement in cholestasis enzymes which were, 3 months after, almost normalized; at the time of writing the paper the follow-up MRCP had not been performed to see if CBD alterations had resolved or not.92
Table 1 shows the main features of the three different types of cholangiopathies: SSC-CIP, ketamine-induced cholangiopathy, and post COVID-19 SSC.
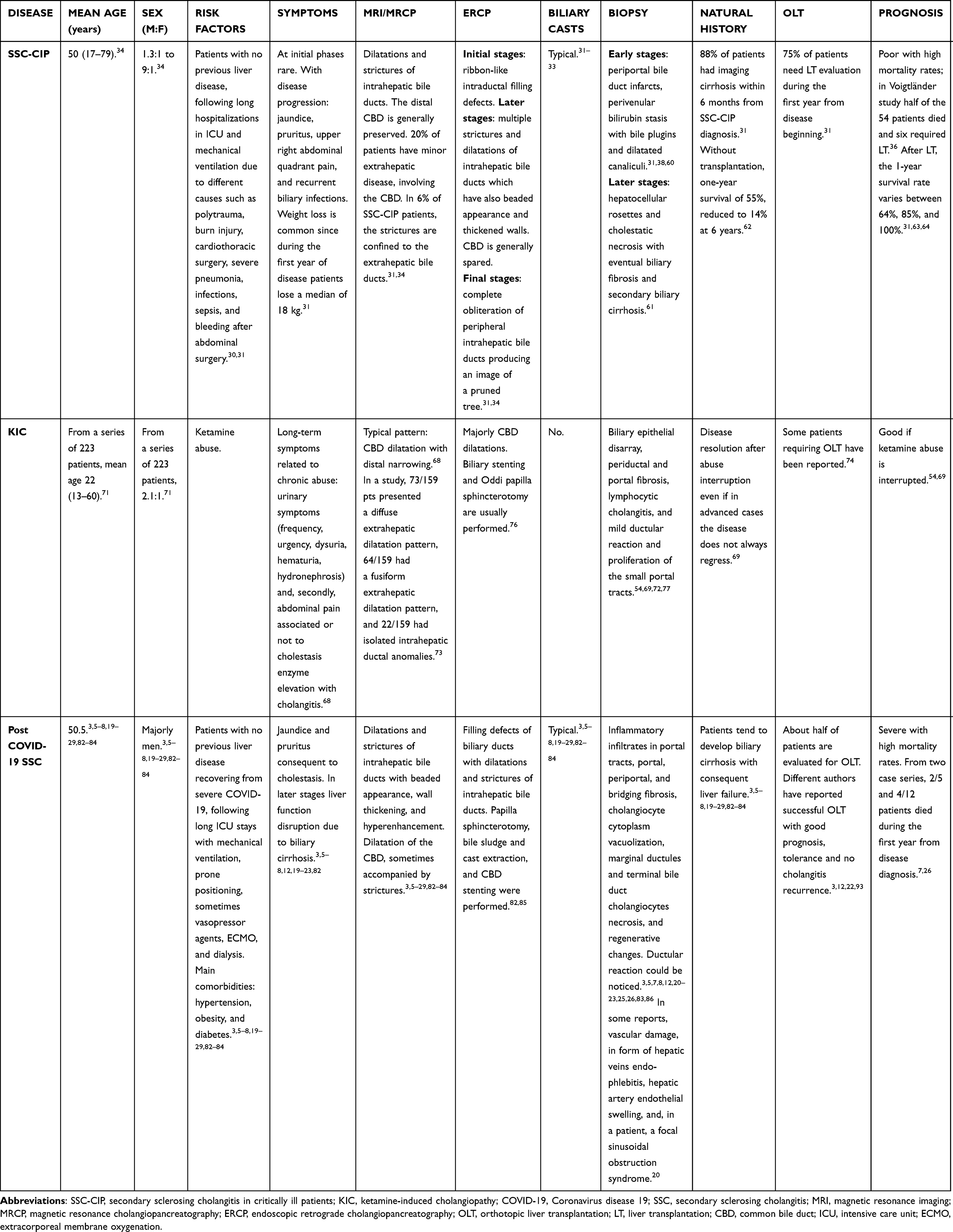 |
Table 1 Main Features Characterizing the Three Different Types of Cholangiopathy, SSC-CIP, KIC, and Post COVID-19 SSC |
Prognosis
From case reports and series, COVID-19 SSC prognosis is poor with high mortality rates. Medical therapy relies on UDCA and cholestyramine to control pruritus. Obeticholic acid has been used in some cases. These medications did not prove to be effective.3,5,6,8,19–29,82–84 Of 5 patients reported by Mallet et al, 2 died due to decompensated cirrhosis26 In Faruqui et al's experience, 4/12 patients died due to severe SSC complications, 1 patient developed decompensated liver cirrhosis and multiorgan failure, 1 received an auxiliary partial OLT (APOLT), 2 patients were evaluated for OLT, and 4 patients were not listed for transplant but did not improve with UDCA therapy.7 Also, Lee, Klindt, Durazo, and Rela and their co-authors reported successful LT (OLT and APOLT) in patients affected by COVID-19 SSC with good prognosis and tolerance and no cholangitis recurrence.3,12,22,93
Discussion
Patients with post COVID-19 SSC show, based on the different case series and reports, common clinical, imaging, and histological features, and most authors correlated this clinical entity with SSC-CIP.3,5,7,8,12,20–25,82,83,86–89,93,94 Table 2 shows the principal case series and reports about post COVID-19 SSC. In fact, in the development of a cholangiopathy following ICU admission, the use of mechanical ventilation, with high PEEPs and low tidal volume, and the use of vasopressors are common features among the two groups. At imaging, COVID-19 severe cholangiopathy is mainly expressed by strictures and dilatations of the intrahepatic bile ducts, which show a beaded appearance, and, to a somewhat lesser extent, by the involvement of the extrahepatic bile ducts, CBD, which may show dilatations and narrowing. Characteristic of both diseases are biliary casts, which are a classic feature of ischemic biliary damage, and a complication of post liver transplantation.
 |
Table 2 Case Reports and Series of Post COVID-19 SSC Patients |
Regarding biliary vascularization, the intrahepatic bile ducts receive blood only from the hepatic artery, whereas the extrahepatic bile tree is vascularized by both the hepatic and the gastroduodenal arteries, and this feature gives the latter less susceptibility to ischemia. Compared to the typical histologic features of SSC-CIP, patients with post COVID-19 SSC show peculiar damage, including cholangiocyte cytoplasm vacuolization, regenerative changes, and various aspects of vascular damage.20 For this reason, several authors such as Butikofer et al and Roth et al have surmised a possible direct viral damage.3,5,7,20–22,82,86 Many reports from autoptic, bioptic, and explant samples demonstrated the presence of SARS-CoV2 inclusions in hepatocytes and cholangiocytes.12,16 SARS-CoV2 is also known to determine a hypercoagulable state responsible for macroangiopathy and microangiopathy, proved in different autoptic, bioptic, and explant samples. Also, the cytokine storm correlated to SARS-CoV2 infection participates in hypercoagulopathy in patients with severe disease.16
The hypothesis of a toxic genesis, related to the administration of high doses of ketamine during ICU stay, is understandable given the high percentage of patients treated with this drug in the ICU.21,26,29,85,86,92 Ketamine in fact can cause a cholangiopathy, which is common among abusers.70,71 However, ketamine-induced cholangiopathy (KIC) has different features than post COVID-19 SSC. It is characterized by a preponderant involvement of the CBD, which, in most cases, is dilated with distal narrowing.72,73 In KIC, biliary casts are not found, and the disease typically regresses both in terms of cholestasis and structural anomalies after abuse cessation.69 KIC pathogenesis is unknown, but it may depend on ketamine mechanism of action and on the precipitation of the drug in the bile.54 In the case of COVID-19 patients, they were treated with high doses of ketamine for long periods and they often suffered from conditions that may alter drug metabolism, such as renal failure.26 Such factors could contribute to the precipitation of ketamine in the biliary tract or to its direct effects on the biliary tree and Oddi sphincter. In this regard, it is interesting to consider the already cited case report by Knooihuizen et al. In fact, the patient who developed the cholangiopathy during her ICU stay for COVID-19 severe pneumonia had different features than those reported in COVID-19 SSC cases. Not only did the enzyme peak gradually reduce, after ketamine cessation, but also, the imaging features, with dilated CBD, closely resembled those of patients with KIC and not those of patients with post COVID-19 SSC.92 It is difficult to understand whether ketamine may actually play a major role in the genesis of post COVID-19 SSC since it was used to sedate the most severe patients, who, therefore, had other risk factors promoting the development of SSC.
In particular, in Butikofer et al’s study, COVID-19 patients had a more severe disease than those with influenza.21 Also, in Wendel-Garcia at al’s study, the ketamine-treated group had a higher SOFA score and lower P/F ratio than the control group. In the study concerning imaging features of post COVID-19 SSC, by Ghafoor et al, only one-third of patients who developed cholangiopathy received ketamine.29
Kulkarni et al decided to study the relationship between anti SARS-CoV2 vaccination and post COVID-19 SSC risk. The authors compared SARS-CoV2 vaccinated (n=7) and unvaccinated (n=8) patients, with severe COVID-19 and cholestasis. None from the vaccinated group developed SSC, while 6/8 from the unvaccinated group did. Vaccinated patients had a less severe COVID-19 than the unvaccinated ones. This study based on a small sample seems to suggest that vaccination can alter the course of post COVID-19 SSC, protecting patients84 Vaccination, in reducing the severity of COVID-19 disease, may reduce the incidence of SSC. Even if this study has limitations bound to the sample size, comparing the incidence of post COVID-19 SSC between vaccinated and non-vaccinated people on a large scale could be interesting.
Conclusions
Post COVID-19 SSC is a rare clinical entity following severe COVID-19 disease. Clinical, radiological, and histological features, as well as prognosis and response to medical therapy, make it resemble SSC-CIP. The pathogenesis of biliary tract damage in both the diseases is not clearly understood but presumably bound to ischemic phenomena. COVID-19 cholangiopathy thus presents also peculiar features that let some authors speculate about a possible direct viral cytopathic role.
A principal role of ketamine in COVID-19 cholangiopathy cannot be proved by case series and clinical trials conducted until now, nor is it supported by radiological and histological features of post COVID-19 SSC. Nonetheless, in view of its potential toxic effect on the biliary tree, it can represent an additional precipitating factor on disease pathogenesis. In fact, the most accepted theory is that a sum of different insults determines the disease: biliary ischemia, direct viral damage, toxic bile, possibly worsened by ketamine and hyperinflammation due to the cytokine storm. Given the severe prognosis of the disease, with persistent cholangiopathy, organ failure, and OLT need, further studies on this novel clinical entity are needed.
Disclosure
The authors report no conflicts of interest in this work and received no funding.
References
1. Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status. Mil Med Res. 2020;7:11. doi:10.1186/s40779-020-00240-0
2. Cai Q, Huang D, Yu H, et al. COVID-19: abnormal liver function tests. J Hepatol. 2020;73:566–574. doi:10.1016/j.jhep.2020.04.006
3. Durazo FA, Nicholas AA, Mahaffey JJ, et al. Post-Covid-19 cholangiopathy-a new indication for liver transplantation: a case report. Transplant Proc. 2021;53:1132–1137. doi:10.1016/j.transproceed.2021.03.007
4. Fix OK, Hameed B, Fontana RJ, et al. Clinical best practice advice for hepatology and liver transplant providers during the COVID-19 pandemic: AASLD Expert Panel Consensus Statement. Hepatology. 2020;72:287–304. doi:10.1002/hep.31281
5. Tafreshi S, Whiteside I, Levine I, D’Agostino C. A case of secondary sclerosing cholangitis due to COVID-19. Clin Imaging. 2021;80:239–242. doi:10.1016/j.clinimag.2021.07.017
6. Hundt MA, Deng Y, Ciarleglio MM, et al. Abnormal liver tests in COVID-19: a retrospective observational cohort study of 1827 patients in a Major U.S. Hospit NetHepatol. 2020;72:1169–1176. doi:10.1002/hep.31487
7. Faruqui S, Okoli FC, Olsen SK, et al. Cholangiopathy after severe COVID-19: clinical features and prognostic implications. Am J Gastroenterol. 2021;116:1414–1425. doi:10.14309/ajg.0000000000001264
8. Meersseman P, Blondeel J, De Vlieger G, et al. Collaborators Leuven liver transplant program. Secondary sclerosing cholangitis: an emerging complication in critically ill COVID-19 patients. Intensive Care Med. 2021;47:1037–1040. doi:10.1007/s00134-021-06445-8
9. Moreira JLS, Barbosa SMB, Goncalves Junior J. Pathophysiology and molecular mechanisms of liver injury in severe forms of COVID-19: an integrative review. Clin Res Hepatol Gastroenterol. 2021;45:101752. doi:10.1016/j.clinre.2021.101752
10. Zhao B, Ni C, Gao R, et al. Recapitulation of SARS-CoV-2 infection and cholangiocyte damage with human liver ductal organoids. Protein Cell. 2020;11:771–775. doi:10.1007/s13238-020-00718-6
11. Alqahtani SA, Schattenberg JM. Liver injury in COVID-19: the current evidence. United Europ Gastroenterol J. 2020;8(5):509–519. doi:10.1177/2050640620924157
12. Klindt C, Jensen BE, Brandenburger T, et al. Secondary sclerosing cholangitis as a complication of severe COVID-19: a case report and review of the literature. Clin Case Rep. 2021;9(5):e04068. PMID: 34084492; PMCID: PMC8142800. doi:10.1002/ccr3.4068
13. Sonzogni A, Previtali G, Seghezzi M, et al. Liver histopathology in severe COVID 19 respiratory failure is suggestive of vascular alterations. Liver Int. 2020;40:2110–2116. doi:10.1111/liv.14601
14. Kaltschmidt B, Fitzek ADE, Schaedler J, et al. Hepatic vasculopathy and regenerative responses of the liver in fatal cases of COVID-19. Clin Gastroenterol Hepatol. 2021;19:1726.e3–1729.e3. doi:10.1016/j.cgh.2021.01.044
15. Wang Y, Liu S, Liu H, et al. SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19. J Hepatol. 2020;73:807–816. doi:10.1016/j.jhep.2020.05.002
16. McConnell MJ, Kawaguchi N, Kondo R, et al. Liver injury in COVID-19 and IL-6 trans-signaling-induced endotheliopathy. J Hepatol. 2021;75(3):647–658. doi:10.1016/j.jhep.2021.04.050
17. Lui VC, Hui KP, Babu RO, et al. Human liver organoid derived intra-hepatic bile duct cells support SARS-CoV-2 infection and replication. Sci Rep. 2022;12(1):5375. PMID: 35354880; PMCID: PMC8965546. doi:10.1038/s41598-022-09306-6
18. Yang L, Han Y, Nilsson-Payant BE, et al. A human pluripotent stem cell-based platform to study SARS-CoV-2 tropism and model virus infection in human cells and organoids. Cell Stem Cell. 2020;27(1):125–136.e7. PMID: 32579880; PMCID: PMC7303620. doi:10.1016/j.stem.2020.06.015
19. Bartoli A, Cursaro C, Andreone P. Severe acute respiratory syndrome coronavirus-2-associated cholangiopathies. Curr Opin Gastroenterol. 2022;38(2):89–97. PMID: 35098930; PMCID: PMC8815639. doi:10.1097/MOG.0000000000000808
20. Roth NC, Kim A, Vitkovski T, et al. Post-COVID-19 Cholangiopathy: a Novel Entity. Am J Gastroenterol. 2021;116(5):1077–1082. PMID: 33464757. doi:10.14309/ajg.0000000000001154
21. Bütikofer S, Lenggenhager D, Wendel Garcia PD, et al. Secondary sclerosing cholangitis as cause of persistent jaundice in patients with severe COVID-19. Liver Int. 2021;41(10):2404–2417. PMID: 34018314; PMCID: PMC8242687. doi:10.1111/liv.14971
22. Lee A, Wein AN, Doyle MBM, Chapman WC. Liver transplantation for post-COVID-19 sclerosing cholangitis. BMJ Case Rep. 2021;14(8):e244168. PMID: 34446515; PMCID: PMC8395362. doi:10.1136/bcr-2021-244168
23. Edwards K, Allison M, Ghuman S. Secondary sclerosing cholangitis in critically ill patients: a rare disease precipitated by severe SARS-CoV-2 infection. BMJ Case Rep. 2020;13(11):e237984. PMID: 33168538; PMCID: PMC7654135. doi:10.1136/bcr-2020-237984
24. Deltenre P, Moreno C, Trépo E. Progressive cholangiopathy in COVID-19 patients: other possible diagnoses than ketamine-induced cholangiopathy should be considered. J Hepatol. 2021;75(4):989–990. PMID: 33753153; PMCID: PMC7977066. doi:10.1016/j.jhep.2021.02.036
25. Hunyady P, Streller L, Rüther DF, et al. Secondary sclerosing cholangitis following COVID-19 disease: a multicenter retrospective study. Clin Infect Dis. 2022;9:ciac565. PMID: 35809032; PMCID: PMC9278244. doi:10.1093/cid/ciac565
26. Mallet V, Bock K, Mandengue PD; Keta-Cov research group. Electronic address: [email protected]; Keta-Cov research group. Intravenous ketamine and progressive cholangiopathy in COVID-19 patients. J Hepatol. 2021;74(5):1243–1244. PMID: 33617925; PMCID: PMC7893247. doi:10.1016/j.jhep.2021.02.007
27. Mallet V, Mallet V, Bock K; Keta-Cov research group. Reply to: “Progressive cholangiopathy in COVID-19 patients: other possible diagnoses than ketamine-induced cholangiopathy should be considered”. J Hepatol. 2021;75(4):990–992. PMID: 34174378; PMCID: PMC8223115. doi:10.1016/j.jhep.2021.06.024
28. de Tymowski C, Dépret F, Dudoignon E, Legrand M, Mallet V; Keta-Cov Research Group. Ketamine-induced cholangiopathy in ARDS patients. Intensive Care Med. 2021;47(10):1173–1174. PMID: 34313797; PMCID: PMC8315088. doi:10.1007/s00134-021-06482-3
29. Wendel-Garcia PD, Erlebach R, Hofmaenner DA, et al. Long-term ketamine infusion-induced cholestatic liver injury in COVID-19-associated acute respiratory distress syndrome. Crit Care. 2022;26(1):148. PMID: 35606831; PMCID: PMC9125956. doi:10.1186/s13054-022-04019-8
30. Brooling J, Leal R. Secondary Sclerosing Cholangitis: a Review of Recent Literature. Curr Gastroenterol Rep. 2017;19(9):44. PMID: 28752474. doi:10.1007/s11894-017-0583-8
31. Leonhardt S, Veltzke-Schlieker W, Adler A, et al. Secondary Sclerosing Cholangitis in Critically Ill Patients: clinical Presentation, Cholangiographic Features, Natural History, and Outcome: a Series of 16 Cases. Medicine. 2015;94(49):e2188. PMID: 26656347; PMCID: PMC5008492. doi:10.1097/MD.0000000000002188
32. Kirstein MM, Book T, Manns MP, von Hahn T, Voigtländer T. Secondary sclerosing cholangitis in critically ill patients has a poor outcome but lower tumour incidence than primary sclerosing cholangitis. United Europ Gastroenterol J. 2020;8(6):716–724. PMID: 32366182; PMCID: PMC7437091. doi:10.1177/2050640620924274
33. Scheppach W, Druge G, Wittenberg G, et al. Sclerosing cholangitis and liver cirrhosis after extrabiliary infections: report on three cases. Crit Care Med. 2001;29(2):438–441. PMID: 11246328. doi:10.1097/00003246-200102000-00042
34. Martins P, Verdelho Machado M. Secondary Sclerosing Cholangitis in Critically Ill Patients: an Underdiagnosed Entity. GE Port J Gastroenterol. 2020;27(2):103–114. PMID: 32266307; PMCID: PMC7113589. doi:10.1159/000501405
35. Weig T, Schubert MI, Gruener N, et al. Abdominal obesity and prolonged prone positioning increase risk of developing sclerosing cholangitis in critically ill patients with influenza A-associated ARDS. Eur J Med Res. 2012;17(1):30. PMID: 23259907; PMCID: PMC3543205. doi:10.1186/2047-783X-17-30
36. Voigtländer T, Negm AA, Schneider AS, et al. Secondary sclerosing cholangitis in critically ill patients: model of end-stage liver disease score and renal function predict outcome. Endoscopy. 2012;44(11):1055–1058. PMID: 23108773. doi:10.1055/s-0032-1325733
37. Leonhardt S, Veltzke-Schlieker W, Adler A, et al. Trigger mechanisms of secondary sclerosing cholangitis in critically ill patients. Crit Care. 2015;19(1):131. PMID: 25886728; PMCID: PMC4407292. doi:10.1186/s13054-015-0861-5
38. Gelbmann CM, Rümmele P, Wimmer M, et al. Ischemic-like cholangiopathy with secondary sclerosing cholangitis in critically ill patients. Am J Gastroenterol. 2007;102(6):1221–1229. PMID: 17531010. doi:10.1111/j.1572-0241.2007.01118.x
39. Engler S, Elsing C, Flechtenmacher C, Theilmann L, Stremmel W, Stiehl A. Progressive sclerosing cholangitis after septic shock: a new variant of vanishing bile duct disorders. Gut. 2003;52(5):688–693. PMID: 12692054; PMCID: PMC1773636. doi:10.1136/gut.52.5.688
40. Douglass TC, Cutter WW. Arterial blood supply of the common bile duct. Arch Surg. 1948;57(4):599–612. PMID: 18102777. doi:10.1001/archsurg.1948.01240020606015
41. Deltenre P, Valla DC. Ischemic cholangiopathy. Semin Liver Dis. 2008;28(3):235–246. PMID: 18814077. doi:10.1055/s-0028-1085092
42. Kobayashi S, Nakanuma Y, Matsui O. Intrahepatic peribiliary vascular plexus in various hepatobiliary diseases: a histological survey. Hum Pathol. 1994;25(9):940–946. PMID: 8088771. doi:10.1016/0046-8177(94)90016-7
43. Shah JN, Haigh WG, Lee SP, et al. Biliary casts after orthotopic liver transplantation: clinical factors, treatment, biochemical analysis. Am J Gastroenterol. 2003;98(8):1861–1867. PMID: 12907345. doi:10.1111/j.1572-0241.2003.07617.x
44. Gor NV, Levy RM, Ahn J, Kogan D, Dodson SF, Cohen SM. Biliary cast syndrome following liver transplantation: predictive factors and clinical outcomes. Liver Transpl. 2008;14(10):1466–1472. PMID: 18825683. doi:10.1002/lt.21492
45. Trauner M, Fickert P, Wagner M. MDR3 (ABCB4) defects: a paradigm for the genetics of adult cholestatic syndromes. Semin Liver Dis. 2007;27(1):77–98. PMID: 17295178. doi:10.1055/s-2006-960172
46. Aronsohn A, Jensen D. Hepatobiliary manifestations of critically ill and postoperative patients. Clin Liver Dis. 2011;15(1):183–197. PMID: 21112000. doi:10.1016/j.cld.2010.09.004
47. Gotthardt D, Runz H, Keitel V, et al. A mutation in the canalicular phospholipid transporter gene, ABCB4, is associated with cholestasis, ductopenia, and cirrhosis in adults. Hepatology. 2008;48(4):1157–1166. PMID: 18781607. doi:10.1002/hep.22485
48. Beuers U, Maroni L, Elferink RO. The biliary HCO(3)(-) umbrella: experimental evidence revisited. Curr Opin Gastroenterol. 2012;28(3):253–257. PMID: 22450897. doi:10.1097/MOG.0b013e328352aab2
49. Zimmer V, Lammert F. Acute Bacterial Cholangitis. Viszeralmedizin. 2015;31(3):166–172. PMID: 26468310; PMCID: PMC4569195. doi:10.1159/000430965
50. Voigtländer T, Leuchs E, Vonberg RP, et al. Microbiological analysis of bile and its impact in critically ill patients with secondary sclerosing cholangitis. J Infect. 2015;70(5):483–490. PMID: 25659761. doi:10.1016/j.jinf.2015.01.013
51. Gadour E, Hassan Z. Meta-analysis and systematic review of liver transplantation as an ultimate treatment option for secondary sclerosing cholangitis. Prz Gastroenterol. 2022;17(1):1–8. PMID: 35371357; PMCID: PMC8942010. doi:10.5114/pg.2021.110483
52. Horvatits T, Trauner M, Fuhrmann V. Hypoxic liver injury and cholestasis in critically ill patients. Curr Opin Crit Care. 2013;19(2):128–132. PMID: 23403733. doi:10.1097/MCC.0b013e32835ec9e6
53. Gudnason HO, Björnsson HK, Gardarsdottir M, et al. Secondary sclerosing cholangitis in patients with drug-induced liver injury. Dig Liver Dis. 2015;47(6):502–507. PMID: 25840876. doi:10.1016/j.dld.2015.03.002
54. Lo RS, Krishnamoorthy R, Freeman JG, Austin AS. Cholestasis and biliary dilatation associated with chronic ketamine abuse: a case series. Singapore Med J. 2011;52(3):e52–5. PMID: 21451916.
55. Laurent L, Lemaitre C, Minello A, et al. Cholangiopathy in critically ill patients surviving beyond the intensive care period: a multicentre survey in liver units. Aliment Pharmacol Ther. 2017;46(11–12):1070–1076. PMID: 29023905. doi:10.1111/apt.14367
56. Lin T, Qu K, Xu X, et al. Sclerosing cholangitis in critically ill patients: an important and easily ignored problem based on a German experience. Front Med. 2014;8(1):118–126. PMID: 24415157. doi:10.1007/s11684-014-0306-6
57. Benninger J, Grobholz R, Oeztuerk Y, et al. Sclerosing cholangitis following severe trauma: description of a remarkable disease entity with emphasis on possible pathophysiologic mechanisms. World J Gastroenterol. 2005;11(27):4199–4205. PMID: 16015689; PMCID: PMC4615442. doi:10.3748/wjg.v11.i27.4199
58. Ruemmele P, Hofstaedter F, Gelbmann CM. Secondary sclerosing cholangitis. Nat Rev Gastroenterol Hepatol. 2009;6(5):287–295. PMID: 19404269. doi:10.1038/nrgastro.2009.46
59. Molvar C, Glaenzer B. Choledocholithiasis: evaluation, Treatment, and Outcomes. Semin Intervent Radiol. 2016;33(4):268–276. PMID: 27904245; PMCID: PMC5088099. doi:10.1055/s-0036-1592329
60. Esposito I, Kubisova A, Stiehl A, Kulaksiz H, Schirmacher P. Secondary sclerosing cholangitis after intensive care unit treatment: clues to the histopathological differential diagnosis. Virchows Arch. 2008;453(4):339–345. PMID: 18769938. doi:10.1007/s00428-008-0654-1
61. Pollheimer MJ, Fickert P, Stieger B. Chronic cholestatic liver diseases: clues from histopathology for pathogenesis. Mol Aspects Med. 2014;37:35–56. PMID: 24141039. doi:10.1016/j.mam.2013.10.001
62. Kulaksiz H, Heuberger D, Engler S, Stiehl A. Poor outcome in progressive sclerosing cholangitis after septic shock. Endoscopy. 2008;40(3):214–218. PMID: 18264887. doi:10.1055/s-2007-967024
63. Kirchner GI, Scherer MN, Obed A, et al. Outcome of patients with ischemic-like cholangiopathy with secondary sclerosing cholangitis after liver transplantation. Scand J Gastroenterol. 2011;46(4):471–478. doi:10.3109/00365521.2010.537683
64. Voigtländer T, Jaeckel E, Lehner F, Manns MP, Lankisch TO. Liver transplantation for critically Ill patients with secondary sclerosing cholangitis: outcome and complications. Liver Transpl. 2015;21(10):1295–1299. PMID: 26069199. doi:10.1002/lt.24192
65. Jansen KL. A review of the nonmedical use of ketamine: use, users and consequences. J Psychoactive Drugs. 2000;32(4):419–433. PMID: 11210204. doi:10.1080/02791072.2000.10400244
66. Al-Nowfal A, Al-Abed YA. Chronic biliary colic associated with ketamine abuse. Int Med Case Rep J. 2016;9:135–137. PMID: 27330331; PMCID: PMC4898409. doi:10.2147/IMCRJ.S100648
67. Corkery JM, Hung WC, Claridge H, Goodair C, Copeland CS, Schifano F. Recreational ketamine-related deaths notified to the National Programme on Substance Abuse Deaths, England, 1997–2019. J Psychopharmacol. 2021;35(11):1324–1348. PMID: 34092131; PMCID: PMC8600594. doi:10.1177/02698811211021588
68. Wood D, Cottrell A, Baker SC, et al. Recreational ketamine: from pleasure to pain. BJU Int. 2011;107(12):1881–1884. PMID: 21314885. doi:10.1111/j.1464-410X.2010.10031.x
69. Lui KL, Lee WK, Li MK. Ketamine-induced cholangiopathy. Hong Kong Med J. 2014;20(1):78.e1–e2. PMID: 24473697. doi:10.12809/hkmj133796
70. Wong GL, Tam YH, Ng CF, et al. Liver injury is common among chronic abusers of ketamine. Clin Gastroenterol Hepatol. 2014;12(10):1759–62.e1. PMID: 24534547. doi:10.1016/j.cgh.2014.01.041
71. Ng SH, Tse ML, Ng HW, Lau FL. Emergency department presentation of ketamine abusers in Hong Kong: a review of 233 cases. Hong Kong Med J. 2010;16(1):6–11. PMID: 20124567.
72. Yu WL, Cho CC, Lung PF, et al. Ketamine-related cholangiopathy: a retrospective study on clinical and imaging findings. Abdom Imaging. 2014;39(6):1241–1246. PMID: 24934474. doi:10.1007/s00261-014-0173-2
73. Seto WK, Mak SK, Chiu K, et al. Magnetic resonance cholangiogram patterns and clinical profiles of ketamine-related cholangiopathy in drug users. J Hepatol. 2018;69(1):121–128. PMID: 29551711. doi:10.1016/j.jhep.2018.03.006
74. Nyirenda TJ, Shirazi-Nejad A, Soliman AS. Persistent Ketamine-Induced Cholangiopathy: an Approach to Management. Cureus. 2020;12(11):e11611. PMID: 33364128; PMCID: PMC7752773. doi:10.7759/cureus.11611
75. Aslam SP, Cacciottolo TM, Bowden D, Griffiths WJH, Godfrey EM. An unusual cause of cholangiopathy. Gastrointest Endosc. 2019;90(5):850–851. PMID: 31238057. doi:10.1016/j.gie.2019.06.020
76. Cheung TT, Poon RT, Chan AC, Lo CM. Education and Imaging. Hepatobiliary and pancreatic: cholangiopathy in ketamine user--an emerging new condition. J Gastroenterol Hepatol. 2014;29(9):1663. PMID: 25154444. doi:10.1111/jgh.12682
77. Turkish A, Luo JJ, Lefkowitch JH. Ketamine abuse, biliary tract disease, and secondary sclerosing cholangitis. Hepatology. 2013;58(2):825–827. PMID: 23695896. doi:10.1002/hep.26459
78. Schwartzman RJ, Alexander GM, Grothusen JR, Paylor T, Reichenberger E, Perreault M. Outpatient intravenous ketamine for the treatment of complex regional pain syndrome: a double-blind placebo controlled study. Pain. 2009;147(1–3):107–115. PMID: 19783371. doi:10.1016/j.pain.2009.08.015
79. Hewitt NA, Cox P. Recurrent Subanesthetic Ketamine Infusions for Complex Regional Pain Syndrome Leading to Biliary Dilation, Jaundice, and Cholangitis: a Case Report. A a Pract. 2018;10(7):168–170. doi:10.1213/XAA.0000000000000650
80. Cotter S, Wong J, Gada N, et al. Repeated or continuous medically supervised ketamine administration associated with hepatobiliary adverse events: a retrospective case series. Drug Saf. 2021;44(12):1365–1374. doi:10.1007/s40264-021-01120-9
81. Agence nationale de sécurité du médicament et des produits de santé (ANSM). Ketamine: risk of serious liver damage during prolonged use and/ or at high doses–Information Point. Available from: https://ansm.sante.fr/S-informer/Points-d-information-Points-d-information/Ketamine-risque-d-atteintes-hepatiques-graves-lors-d-utilisations-prolongees-et-ou-a-doses-elevees-Point-d-Information.
82. Caballero-Alvarado J, Zavaleta Corvera C, Merino Bacilio B, Ruiz Caballero C, Lozano-Peralta K. Post-COVID cholangiopathy: a narrative review. Gastroenterol Hepatol. 2022;S0210–5705(22):221–227. PMID: 36174796; PMCID: PMC9512521. doi:10.1016/j.gastrohep.2022.09.004
83. Rojas M, Rodríguez Y, Zapata E, Hernández JC, Anaya JM. Cholangiopathy as part of post-COVID syndrome. J Transl Autoimmun. 2021;4:100116. PMID: 34485887; PMCID: PMC8406516. doi:10.1016/j.jtauto.2021.100116
84. Kulkarni AV, Khelgi A, Sekaran A, et al. Post-COVID-19 cholestasis: a case series and review of literature. J Clin Exp Hepatol. 2022;12(6):1580–1590. PMID: 35719861; PMCID: PMC9187855. doi:10.1016/j.jceh.2022.06.004
85. Ghafoor S, Germann M, Jüngst C, Müllhaupt B, Reiner CS, Stocker D. Imaging features of COVID-19-associated secondary sclerosing cholangitis on magnetic resonance cholangiopancreatography: a retrospective analysis. Insights Imaging. 2022;13(1):128. PMID: 35939241; PMCID: PMC9358102. doi:10.1186/s13244-022-01266-9
86. Mayorquín-Aguilar JM, Lara-Reyes A, Revuelta-Rodríguez LA, et al. Secondary sclerosing cholangitis after critical COVID-19: three case reports. World J Hepatol. 2022;14(8):1678–1686. PMID: 36157873; PMCID: PMC9453459. doi:10.4254/wjh.v14.i8.1678
87. Soldera J, Balbinot RA, Balbinot SS. Billiary casts in post-COVID-19 cholangiopathy. Gastroenterol Hepatol. 2022;S0210–5705(22):212–216. PMID: 36116722; PMCID: PMC9476357. doi:10.1016/j.gastrohep.2022.08.008
88. Kroepfl V, Treml B, Freund MC, Profanter C. Early detection of COVID-19 cholangiopathy using cholangioscopy-a case report of two critically ill patients. Eur Surg. 2022;54(6):326–330. PMID: 36189108; PMCID: PMC9510572. doi:10.1007/s10353-022-00776-6
89. Franzini TAP, Guedes MMF, Rocha HL, Fleury CA, Bestetti AM, Moura EGH. CHOLANGIOSCOPY IN A POST-COVID-19 CHOLANGIOPATHY PATIENT. Arq Gastroenterol. 2022;59(2):321–323. PMID: 35830050. doi:10.1590/S0004-2803.202202000-58
90. Lagana SM, Kudose S, Iuga AC, et al. Hepatic pathology in patients dying of COVID-19: a series of 40 cases including clinical, histologic, and virologic data. Mod Pathol. 2020;33(11):2147–2155. PMID: 32792598; PMCID: PMC7424245. doi:10.1038/s41379-020-00649-x
91. Noppers IM, Niesters M, Aarts LP, et al. Drug-induced liver injury following a repeated course of ketamine treatment for chronic pain in CRPS type 1 patients: a report of 3 cases. Pain. 2011;152(9):2173–2178. PMID: 21546160. doi:10.1016/j.pain.2011.03.026
92. Knooihuizen SAI, Aday A, Lee WM. Ketamine-Induced Sclerosing Cholangitis (KISC) in a Critically Ill Patient With COVID-19. Hepatology. 2021;74(1):519–521. doi:10.1002/hep.31650
93. Rela M, Rajakannu M, Veerankutty FH, Vij M, Rammohan A. First report of auxiliary liver transplantation for severe cholangiopathy after SARS-CoV-2 respiratory infection. Am J Transplant. 2022;22(12):3143–3145. doi:10.1111/ajt.17165
94. Saleem N, Li BH, Vuppalanchi R, Gawrieh S, Gromski MA. Critical Illness Cholangiopathy in COVID-19 Long-haulers. Tech Innov Gastrointest Endosc. 2022;24(4):351–353. doi:10.1016/j.tige.2022.05.006
95. Weaver M, McHenry S, Das KK. COVID-19 and Jaundice. Gastroenterology. 2021;160(7):e1–e3. doi:10.1053/j.gastro.2020.10.006
96. Linneweber L, Mann AB, Denk G, Kraft E, Weber S. Cholangiopathy in early rehabilitation after intensive care treatment of patients with COVID-19. Am J Gastroenterol. 2022;117(1):197–198. doi:10.14309/ajg.0000000000001511
97. Gourjault C, Tarhini H, Rahi M, et al. Cholangitis in three critically ill patients after a severe CoVID-19 infection. IDCases. 2021;26:e01267. doi:10.1016/j.idcr.2021.e01267
98. Sanders D, Bomman S, Irani S. COVID-19-induced bile duct casts and cholangitis: a case report. Cureus. 2021;13(4):e14560. doi:10.7759/cureus.14560
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.