Back to Journals » International Journal of Women's Health » Volume 14
Secondary Postpartum Hemorrhage Due to Retained Placenta Accreta Spectrum: A Case Report
Authors Mercier AM, Ramseyer AM, Morrison B, Pagan M, Magann EF ![]() , Phillips A
, Phillips A
Received 25 January 2022
Accepted for publication 12 April 2022
Published 22 April 2022 Volume 2022:14 Pages 593—597
DOI https://doi.org/10.2147/IJWH.S359857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ann Marie Mercier,1 Abigail M Ramseyer,2 Bethany Morrison,1 Megan Pagan,1 Everett F Magann,1 Amy Phillips1
1Department of Obstetrics and Gynecology at the University of Arkansas for Medical Sciences, Little Rock, AR, USA; 2Department of Obstetrics and Gynecology, Maternal & Fetal Medicine at Sparrow Medical Group, Lansing, MI, USA
Correspondence: Everett F Magann, Department of Obstetrics and Gynecology, University of Arkansas for Medical Sciences, 4301 W. Markham St. Slot # 518, Little Rock, AR, 72205-7199, USA, Tel +1 501-686-8345, Email [email protected]
Background: Retained products of conception and placenta accreta spectrum are causes of postpartum hemorrhage. Placenta accreta spectrum is frequently managed with cesarean hysterectomy, but conservative approaches are emerging. We present a case of delayed postpartum hemorrhage secondary to a retained placenta increta.
Case: A 29-year-old G3P2 presented with heavy vaginal bleeding 20 days postoperatively following an uncomplicated classical cesarean delivery at 27 5/7 weeks’ gestation for preterm labor in the setting of a vasa previa. On workup, imaging showed retained products of conception and concern for placenta accreta. A hypervascular area in the lower uterine segment was identified at the time of postpartum laparotomy. Total abdominal hysterectomy was performed due to postpartum hemorrhage and clinical suspicion for placenta accreta spectrum disorder. Pathology confirmed a placenta increta.
Conclusion: Diagnosis of placenta accreta spectrum in the remote postpartum period is uncommon but should be a considered etiology in delayed postpartum hemorrhage. Careful inspection and documentation of the placenta implantation site should occur in cesarean sections because placenta accreta spectrum disorders can remain unnoticed during delivery.
Keywords: delayed postpartum hemorrhage, placenta accreta, pregnancy, hysterectomy, vasa previa
Introduction
Retained products of conception (RPOC) and placenta accreta spectrum (PAS) are two known causes of postpartum hemorrhage.1 RPOC is often diagnosed in the postpartum period immediately after delivery with uterine atony or later in the postpartum course with vaginal bleeding or fever.1 RPOC is typically seen on ultrasound as a heterogeneous intrauterine mass. PAS is frequently diagnosed antenatally during the second or third trimester, and maternal outcomes have been shown to be improved with the earlier detection of PAS.2,3 An increasing number of cesarean deliveries not only increases the risk of PAS but also both maternal and perinatal morbidity and mortality.4–6 Commonly, PAS is managed by a cesarean hysterectomy following delivery of the fetus with the placenta left in-situ.4,7 A multi-disciplinary PAS team approach is emerging to optimize management and surgical expertise to improve maternal morbidity and mortality.4,5,8,9 Recent studies have shown that conservative options, such as leaving the placenta in situ, may be offered to appropriate candidates, suggesting that PAS management be individualized with patient-centered discussions.4,10 Local resection of the placenta and repair of the placental site has also been reported.11 We present a case of delayed postpartum hemorrhage due to undiagnosed, retained placenta accreta spectrum.
Based on 45 CFR 46.102(b), our university Institutional Review Board (IRB) does not consider case reports to be human subject research and does not require IRB Review or Approval. The authors have followed standard ethical guidelines in respect to patient anonymity. The patient has given permission to participate and to publish this information.
Case
A 29-year-old G3P2 was transported to the regional academic medical center at 26 weeks 3 days of gestation due to vaginal bleeding in the setting of known vasa previa with possible PAS. She had a history of one previous cesarean delivery. Prenatal ultrasound at 27 weeks' gestation reported anterior placenta with marginal cord insertion and a vasa previa without sonographic evidence of PAS. On hospital day 9, she underwent a classical cesarean delivery with bilateral tubal ligation due to active preterm labor and vaginal bleeding. The patient had requested that a bilateral tubal ligation be undertaken at the time of the cesarean delivery and signed the appropriate consent forms. After delivery of the fetus, the placenta was manually expressed without difficulty, and the uterus was exteriorized for hysterotomy closure. There were no intraoperative complications documented and no evidence of PAS at the time of cesarean delivery. Estimated blood loss from the procedure was 870cc. Her immediate postpartum course was uncomplicated, and she was discharged home on postpartum day two. The placenta pathology report confirmed an unremarkable three-vessel cord, fetal membranes with bland decidual necrosis, villous maturation accelerated for gestational age with patchy edema, and decidual vasculopathy.
On postoperative day 20, the patient presented to a local hospital with heavy vaginal bleeding. A transvaginal ultrasound showed vascularity in the lower uterine segment along with a mass which was concerning for RPOC. CT and MRI at the local hospital supported this diagnosis. The patient was transported to the regional tertiary medical center where she had previously delivered for further management. The images were reviewed by the radiologists at the tertiary medical center, and they reported the presence of a hypervascular soft tissue mass with hemorrhagic components located in the anterior lower uterine segment and invading through the myometrium, which was suggestive of a retained placenta accreta versus a uterine dehiscence with extrusion of the products of conception. The patient underwent a diagnostic laparoscopy with no evidence of hemoperitoneum or obvious uterine dehiscence. Adhesions near the bladder limited visualization of the lower uterine segment. Suction dilation and curettage was performed under ultrasound guidance without successful evacuation of the suspected products of conception. Concern for PAS was again raised due to brisk vaginal bleeding totaling 2 liters following dilation and curettage. An immediate exploratory laparotomy was undertaken. After the vesicouterine adhesions were lysed and a bladder flap was created, a 4×3 cm area of hypervascularity was noted in the lower uterine segment consistent with PAS, and a total abdominal hysterectomy was accomplished. Total estimated blood loss from the case was 3.4 liters; the patient received 3 units of packed red blood cells and 2 units of albumin intraoperatively (Figures 1 and2). The pathology report detailed retained tissue, measuring 4×3 cm, grossly adherent to the anterior endometrial surface invading into the anterior uterine wall, without penetrating the serosal surface. The depth of invasion was 2.5 cm, 0.1 cm from the serosal surface, confirming a placenta increta. The patient’s postoperative course was uncomplicated, and she was discharged home on postoperative day two.
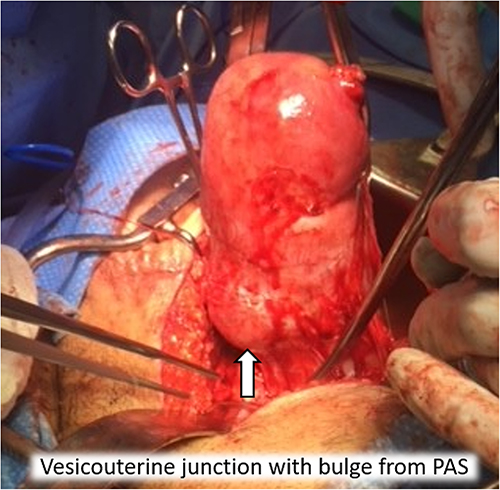 |
Figure 1 Lower uterine segment after vesicouterine peritoneum dissection at time of hysterectomy. Arrow indicates vesicouterine junction with bulge from PAS (placental accreta spectrum). |
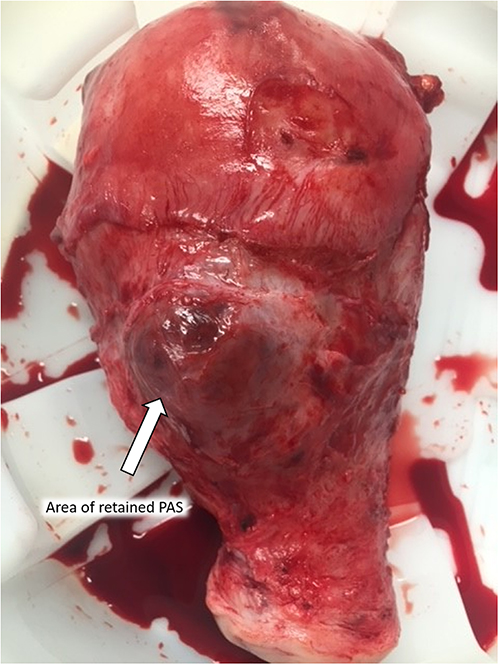 |
Figure 2 Uterus after removal demonstrating 3x4 cm bulging area of hypervascularity consistent with PAS (placental accreta spectrum). Arrow indicates area of retained PAS (placental accreta spectrum). |
Discussion
The precursor of PAS is a scar pregnancy most frequently located in a uterus with a prior cesarean scar.12 A limited number of cases of unintentional retained PAS have been reported in the literature with variations in management.13–17 Guarino et al described a successful hysteroscopic resection of RPOC three months postpartum after a vaginal delivery.18 Dasari et al described a patient with postpartum bleeding after a forceps-assisted vaginal delivery and imaging that revealed concern for RPOC and PAS. This patient was managed medically with five doses of methotrexate, and the mass was expelled on postpartum day #35 without complications.19 Intentional, delayed hysterectomy or conservative management of PAS is emerging in the obstetrics field.15,20–22 Risks of conservative management of PAS include hemorrhage requiring urgent hysterectomy.20,21 In our case, we were unable to utilize embolization or other conservative techniques due to acute operative hemorrhage requiring definitive surgical intervention.
In our case, an anterior placenta increta was ultimately found during the postpartum course and hysterectomy performed due to hemorrhage after a failed dilation and curettage. Anterior placentation in PAS and placenta previa is associated with higher rates of hemorrhage, transfusions, and hysterectomy compared with posterior placentation, which are often associated with a delayed diagnosis.22 This case also highlights the limitations of prenatal ultrasound in detecting PAS. Ultrasound is recommended as the initial imaging modality and has a high accuracy for antepartum diagnosis of placentation disorders in high‐risk patients; the addition of color Doppler use improves diagnostic accuracy.4,23,24 A 2017 meta-analysis found a 90% antenatal detection rate with ultrasound.25 Use of MRI to differentiate retained PAS from other causes of postpartum hemorrhage has been described.26 Care for the patient occurred in a medical center with an accreta center of excellence designation with an experienced dedicated placenta accreta team in place.
Delayed diagnosis of PAS in the postpartum period is rare; however, a retained PAS may lead to delayed postpartum hemorrhage. MRI was helpful in making the diagnosis of PAS in our case. Additional research is necessary to determine the optimal imaging modality for diagnosis if PAS is suspected postpartum. In this case, cesarean delivery did not aid in the diagnosis of PAS as the uterine cavity inspection at the time of delivery did not reveal the PAS. The placenta had separated easily from the uterine wall at the time of delivery, and there was no immediate or early postpartum hemorrhage. The uterine incision used was a classical incision in the contractile portion of the uterus. With the placenta having easily detached after delivery of the fetus, the lower uterine segment may not have been inspected to the degree it would have been if the incision was a low segment transverse incision. Additionally, a bladder flap was not created. The creation of a bladder flap at the time of the cesarean delivery may have enhanced visualization of the lower uterine segment and might have improved the detection of PAS.
During the hysterectomy, after the bladder flap was created and the vesicouterine space entered, the area of abnormal placentation was obvious with raised, blue, vascular tissue present just under the uterine serosa. Careful inspection and documentation of the placental implantation site at the time of cesarean section should occur in all cases as placenta accreta spectrum disorders can go unnoticed.
Acknowledgments
Thanks to Donna Eastham, BA for her help in editing and submitting this manuscript.
Funding
This project received no funding.
Disclosure
The authors have no financial disclosures to declare and no conflicts of interest to report in this work.
References
1. Sheffield JS. Williams Obstetrics.
2. Wong HS, Hutton J, Zuccollo J, Tait J, Pringle KC. The maternal outcome in placenta accreta: the significance of antenatal diagnosis and non-separation of placenta at delivery. N Z Med J. 2008;121(1277):30–38.
3. Erfani H, Fox KA, Clark SL, et al. Maternal outcomes in unexpected placenta accreta spectrum disorders: single-center experience with a multidisciplinary team. Am J Obstet Gynecol. 2019;221(4):
4. American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Obstetric care consensus no. 7: placenta accreta spectrum. Obstet Gynecol. 2018;132(6):e259–e275. doi:10.1097/aog.0000000000002983
5. American College of Obstetricians and Gynecologists. Levels of maternal care: obstetric care consensus no, 9. Obstet Gynecol. 2019;134(2):e41–e55. doi:10.1097/aog.0000000000003383
6. Silver RM, Branch DW. Placenta accreta spectrum. N Engl J Med. 2018;378(16):1529–1536. doi:10.1056/NEJMcp1709324
7. Collins SL, Alemdar B, van Beekhuizen HJ, et al. Evidence-based guidelines for the management of abnormally invasive placenta: recommendations from the International Society for Abnormally Invasive Placenta. Am J Obstet Gynecol. 2019;220(6):511–526. doi:10.1016/j.ajog.2019.02.054
8. Silver RM, Fox KA, Barton JR, et al. Center of excellence for placenta accreta. Am J Obstet Gynecol. 2015;212(5):561–568. doi:10.1016/j.ajog.2014.11.018
9. Shamshirsaz AA, Fox KA, Salmanian B, et al. Maternal morbidity in patients with morbidly adherent placenta treated with and without a standardized multidisciplinary approach. Am J Obstet Gynecol. 2015;212(2):
10. Allahdin S, Voigt S, Htwe TT. Management of placenta praevia and accreta. J Obstet Gynaecol. 2011;31(1):1–6. doi:10.3109/01443615.2010.532248
11. Karaman E, Kolusarı A, Çetin O, et al. Local resection may be a strong alternative to cesarean hysterectomy in conservative surgical management of placenta percreta: experiences from a tertiary hospital. J Matern Fetal Neonatal Med. 2017;30(8):947–952. doi:10.1080/14767058.2016.1192119
12. Timor-Tritsch IE, Monteagudo A, Calì G, D’Antonio F, Kaelin Agten A. Cesarean scar pregnancy: diagnosis and pathogenesis. Obstet Gynecol Clin North Am. 2019;46(4):797–811. doi:10.1016/j.ogc.2019.07.009
13. Cramer S, Hatem F, Heller DS. Placenta increta presenting as retained placenta: a report of 3 cases. Fetal Pediatr Pathol. 2019;38(3):215–225. doi:10.1080/15513815.2019.1582121
14. Schoolmeester JK, Bakkum-Gamez JN. Retained products of conception after cesarean section and occult placenta accreta. Mayo Clin Proc. 2020;95(11):2462–2463. doi:10.1016/j.mayocp.2020.08.046
15. Zuckerwise LC, Craig AM, Newton JM, Zhao S, Bennett KA, Crispens MA. Outcomes following a clinical algorithm allowing for delayed hysterectomy in the management of severe placenta accreta spectrum. Am J Obstet Gynecol. 2020;222(2):
16. Takeda A, Koike W. Conservative endovascular management of retained placenta accreta with marked vascularity after abortion or delivery. Arch Gynecol Obstet. 2017;296(6):1189–1198. doi:10.1007/s00404-017-4528-0
17. Katsogiannou M, Amar-Millet A, Muller C, Desbriere R. Radiofrequency ablation of retained placenta accreta after conservative management. Eur J Obstet Gynecol Reprod Biol. 2019;240:383–384. doi:10.1016/j.ejogrb.2019.07.017
18. Guarino A, Di Benedetto L, Assorgi C, Rocca A, Caserta D. Conservative and timely treatment in retained products of conception: a case report of placenta accreta ritention. Int J Clin Exp Pathol. 2015;8(10):13625–13629.
19. Dasari P, Venkatesan B, Thyagarajan C, Balan S. Expectant and medical management of placenta increta in a primiparous woman presenting with postpartum haemorrhage: the role of Imaging. J Radiol Case Rep. 2010;4(5):32–40. doi:10.3941/jrcr.v4i5.343
20. Matsuzaki S, Grubbs BH, Matsuo K. Delayed hysterectomy versus continuing conservative management for placenta percreta: which is better? Am J Obstet Gynecol. 2020;223(2):304. doi:10.1016/j.ajog.2020.03.025
21. Matsuzaki S, Yoshino K, Endo M, Kakigano A, Takiuchi T, Kimura T. Conservative management of placenta percreta. Int J Gynaecol Obstet. 2018;140(3):299–306. doi:10.1002/ijgo.12411
22. Collins SL, Sentilhes L, Chantraine F, Jauniaux E. Delayed hysterectomy: a laparotomy too far? Am J Obstet Gynecol. 2020;222(2):101–102. doi:10.1016/j.ajog.2019.09.042
23. Ayati S, Leila L, Pezeshkirad M, et al. Accuracy of color Doppler ultrasonography and magnetic resonance imaging in diagnosis of placenta accreta: a survey of 82 cases. Int J Reprod Biomed. 2017;15(4):225–230.
24. D’Antonio F, Iacovella C, Bhide A. Prenatal identification of invasive placentation using ultrasound: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2013;42(5):509–517. doi:10.1002/uog.13194
25. Jauniaux E, Bhide A. Prenatal ultrasound diagnosis and outcome of placenta previa accreta after cesarean delivery: a systematic review and meta-analysis. Am J Obstet Gynecol. 2017;217(1):27–36. doi:10.1016/j.ajog.2017.02.050
26. Tanaka YO, Shigemitsu S, Ichikawa Y, Sohda S, Yoshikawa H, Itai Y. Postpartum MR diagnosis of retained placenta accreta. Eur Radiol. 2004;14(6):945–952. doi:10.1007/s00330-004-2266-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.