Back to Journals » Journal of Healthcare Leadership » Volume 17
Second Victim Syndrome Among Healthcare Professionals: A Systematic Review of Interventions and Outcomes
Authors Ong TSK, Goh CN, Tan EKYE, Sivanathan KA, Tang ASP, Tan HK, Ng QX ![]()
Received 6 March 2025
Accepted for publication 27 May 2025
Published 3 June 2025 Volume 2025:17 Pages 225—239
DOI https://doi.org/10.2147/JHL.S526565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Pavani Rangachari
Timothy Sheng Khai Ong,1,* Celeste Natasha Goh,1,* Erel Kane Yun En Tan,1,* Kavin Abimanyu Sivanathan,2 Ansel Shao Pin Tang,1 Hiang Khoon Tan,3– 5 Qin Xiang Ng4,6
1NUS Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore; 2Wallace Wurth, University of New South Wales, New South Wales, Australia; 3Division of Surgery and Surgical Oncology, Singapore General Hospital and National Cancer Centre Singapore, Singapore, Singapore; 4SingHealth Duke-NUS Global Health Institute, Singapore, Singapore; 5Duke Global Health Institute, Duke University, Durham, NC, USA; 6Saw Swee Hock School of Public Health, National University of Singapore and National University Health System, Singapore
*These authors contributed equally to this work
Correspondence: Qin Xiang Ng, Saw Swee Hock School of Public Health, National University of Singapore and National University Health System, Singapore, Email [email protected]
Background: Second Victim Syndrome (SVS) refers to the significant emotional and psychological distress experienced by healthcare professionals following adverse patient events. While numerous interventions have been developed to support second victims, their effectiveness remains poorly understood. This systematic review aimed to synthesize the evidence on the outcomes of available interventions targeting SVS.
Methods: We systematically searched MEDLINE, Embase, and the Cochrane Library databases, covering all records up to July 7, 2024. We included studies that evaluated the impact of SVS interventions on psychological, professional, and institutional outcomes. We assessed the quality of the included studies using the Joanna Briggs Institute (JBI) critical appraisal tool and evaluated the certainty of evidence using the GRADE framework. Due to heterogeneity in study designs and outcome measures, we opted for a narrative synthesis.
Results: Fifteen studies were included, predominantly of moderate quality. Peer support programs were the most commonly implemented interventions, often structured around the Scott Three-Tiered Model. These programs demonstrated consistent short-term benefits, such as reduced emotional distress and perceived isolation. However, evidence for long-term outcomes—including professional resilience, burnout reduction, and retention—was mixed and generally of low certainty. Structured psychological interventions, including cognitive behavioral therapy (CBT) and mindfulness-based programs, showed more promising long-term results but remain underexplored. Standardized outcome measures, such as the Second Victim Experience and Support Tool (SVEST), were infrequently used, limiting comparability across studies.
Conclusion: SVS interventions, particularly peer support, offer short-term relief but limited long-term impact. There is a critical need for longitudinal research using standardized outcome measures to better evaluate effectiveness. This review highlights the need for system-wide, evidence-based interventions and standardized evaluation metrics to support healthcare professionals effectively.
Plain Language Summary: Healthcare professionals involved in medical errors or adverse events often experience emotional distress, a phenomenon known as Second Victim Syndrome (SVS). This review examined existing programs designed to support these individuals and assessed their effectiveness. We reviewed 15 studies that evaluated interventions such as peer support, counseling, and mindfulness programs. Peer support programs were widely implemented and helped reduce feelings of isolation and distress in the short term. However, their long-term impact on mental health and professional well-being was unclear. More structured psychological interventions, like cognitive behavioral therapy (CBT) and mindfulness, showed promise but were underexplored. A key challenge was the lack of standardized outcome measures, making it difficult to compare program effectiveness. Future research should focus on integrating professional psychological support, improving intervention accessibility, and using validated tools to assess outcomes. Addressing SVS requires a system-wide commitment to fostering a supportive healthcare culture.
Keywords: second victim syndrome, SVS, medical errors, healthcare, healthcare professionals
Introduction
Healthcare professionals (HCPs) work in high-stakes environments where adverse events and medical errors are an unfortunate reality.1 While the immediate focus is often on patients and institutional accountability, the emotional and psychological toll on healthcare providers involved in such incidents is increasingly recognized as a critical issue.1,2 This phenomenon, termed Second Victim Syndrome (SVS) by Wu in 2000, refers to the emotional distress, self-doubt, and psychological sequelae experienced by HCPs following adverse patient outcomes, unanticipated events, or clinical errors.2 ‘Second Victims’ may be directly or indirectly involved in the unanticipated adverse patient event, and SVS can manifest as guilt, anxiety, sleep disturbances, and diminished professional confidence, with potential long-term repercussions on well-being and career trajectory.3–5SVS is highly prevalent. Global estimates suggest that almost 50% of healthcare providers experience SVS at least once in their career, and the prevalence ranges from 10.4% to 43.3%.3 The consequences extend beyond individual suffering, with exacerbated risks of increased burnout, absenteeism, staff turnover, and even compromised patient safety and quality of care.1,5
Recognizing the detrimental impact of Second Victim Syndrome (SVS), healthcare institutions have developed various interventions to support affected professionals. Notable programs such as the Resilience in Stressful Events (RISE) initiative at Johns Hopkins Hospital6 and the ForYOU program at the University of Missouri Health Care7 emphasize peer support, individual counseling, and structured debriefing. Scott’s Three-Tiered Model of Support, which includes immediate emotional first aid, peer support, and access to professional counseling services, has emerged as a widely adopted framework.8 However, the effectiveness of such interventions remains poorly understood, as most studies focus on subjective experiences rather than standardized outcome measures.
There is limited consensus on which interventions are most effective, especially in the long term. Prior reviews, including those by Coughlan et al (2017) and Nydoo et al (2020), have synthesized available programs but primarily focused on describing the types of support offered rather than evaluating outcomes.9,10 More recent reviews often emphasize the availability of resources or theoretical models without critically appraising the effectiveness of interventions or using standardized outcome measures.1,9 Besides many studies relying on anecdotal feedback or non-validated tools, significant variability exists in intervention outcome measurement, including differences in tools used, study design, targeted populations, and types of interventions,11–13 which inevitably hinders cross-study comparison, comparability and generalizability. Only recently has an international consensus been reached on key indicators for evaluating SVS programs;14 inadequate evaluation of such programs limits understanding of program effectiveness, which, in turn, impedes institutional adoption.
This systematic review therefore aims to identify the interventions supporting Second Victims in literature and examine their effectiveness, so as to inform healthcare institutions on best practices for mitigating SVS and inspire further investigation in this important area of research. These findings aim to bridge the methodological limitations of past reviews, as well as the gap between research on SVS and their practical applications in healthcare institutions.
Methods
Study Design
This current systematic review adhered to the latest Preferred Reporting Items for Systematic Reviews and Meta Analysis (PRISMA) statement,15 with search terms including but not limited to: “Intervention”, “Second Victim Syndrome”, “Medical Errors” and “Healthcare Personnel”. We searched MEDLINE, Embase and Cochrane library databases, covering all records up to July 7, 2024. The full search strategy is available in Table S1. The study protocol was prospectively registered in PROSPERO (registration number CRD42024562333). In addition to peer-reviewed databases, we reviewed reference lists of included studies and relevant grey literature sources (eg, institutional reports and program evaluations) to ensure a comprehensive search. However, we did not include unpublished conference proceedings.
Eligibility and Selection Criteria
All search results were imported into Covidence (Melbourne, Victoria, Australia), a systematic review management software platform, used to facilitate duplicate removal and study screening. Each title and abstract were independently screened by two pre-assigned reviewers (TOSK, CNG, EKYET or KAS) working separately to ensure unbiased assessment. Reviewers were assigned in rotating pairs to evenly distribute the workload across the team. Any discrepancies were resolved through discussion, and, if necessary, with input from a third reviewer (ASPT, HKT or QXN). The term “independent” refers to the independent conduct of initial screening by reviewers within the study team, not to external or unaffiliated reviewers. Full-text articles were similarly assessed in duplicate using the same process. We did not formally calculate inter-rater reliability (eg, kappa), but discrepancies were minimal and resolved through consensus with a senior author (ASPT, HKT or QXN).
Studies selected for inclusion had to: (1) be original randomized controlled trials, observational studies, pilot studies and quasi-experimental studies; (2) investigate the Second Victim phenomenon and interventions, programs, or strategies to improve outcomes of Second Victims; (3) report the efficacy of these interventions regarding personal, physical, mental health or workplace outcomes; (4) be available in English or have a professionally translated English manuscript. Second Victims were defined as HCPs involved in an unanticipated adverse patient event, in a medical error and/or a patient-related injury and become victimized in the sense that they are traumatized by the event. Second Victim syndrome was defined as the continuum of symptoms and emotions experienced by Second Victims. Systematic reviews, editorials, opinion pieces, case reports and conference abstracts; studies investigating non-healthcare worker populations; and studies not available in the English language were excluded.
Data Extraction and Outcomes
We developed and piloted a standardized data extraction form on a small subset of studies to ensure clarity and consistency. Two pairs of authors (TSKO, CNG, EKYET or KAS) independently extracted data including: (1) study characteristics (author, publication year), (2) patient demographics (number, age, gender), (3) baseline status, (4) treatment characteristics and (5) treatment outcomes. Any discrepancies were resolved in consultation with a senior author (ASPT or QXN). Given the anticipated heterogeneity of outcomes, narrative synthesis was utilized to examine the impact of different methods employed for SVS in literature. The primary outcomes of interest were the improvements in psychological and physical well-being of Second Victims. For the purposes of this review, immediate outcomes were defined as those pertaining to emotional and psychological well-being shortly after implementation of the intervention, for example, individual emotions and satisfaction. Long term outcomes were defined twofold. Firstly, as those pertaining to helping individuals deal with future adverse events, such as department culture, resilience and perceived institutional support and secondly, as longer-term impacts on individual well-being, such as burnout and depression.
Quality Assessment
The Joanna Briggs Institute (JBI) critical appraisal tool16 was used for quality assessment for the studies included in this review. We chose this tool as all the studies included in this review were quasi-experimental in nature. The JBI checklist for quasi-experimental studies contains 9 items that evaluate the internal validity and risk of bias across various domains such as the bias related to temporal precedence, selection and allocation, confounding factors, administration of intervention and measurement of outcomes. An overall appraisal rating is synthesized to determine the quality of the paper. The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework was also used to evaluate the certainty of evidence for outcomes.17 The GRADE framework assesses five domains including: Risk of bias, inconsistency, indirectness, imprecision and publication bias. The GRADE assessments were conducted with input from the senior authors (ASPT and QXN) and presented in a structured and transparent approach to guide the interpretation of the findings.
Results
Study Selection and Characteristics
A comprehensive search across Embase, MEDLINE, and Cochrane Library databases identified 10,322 studies. After removing 2615 duplicates, 7647 studies were excluded during title and abstract screening for not meeting inclusion criteria. Following full-text review of 58 studies and additional grey literature search, 15 studies published between 2015 and 2024 were included.6,12,13,18–29 The selection process was summarized and is available in Figure 1 (further details of excluded studies are available in Table S2). Characteristics of the included studies are summarized in Table 1.
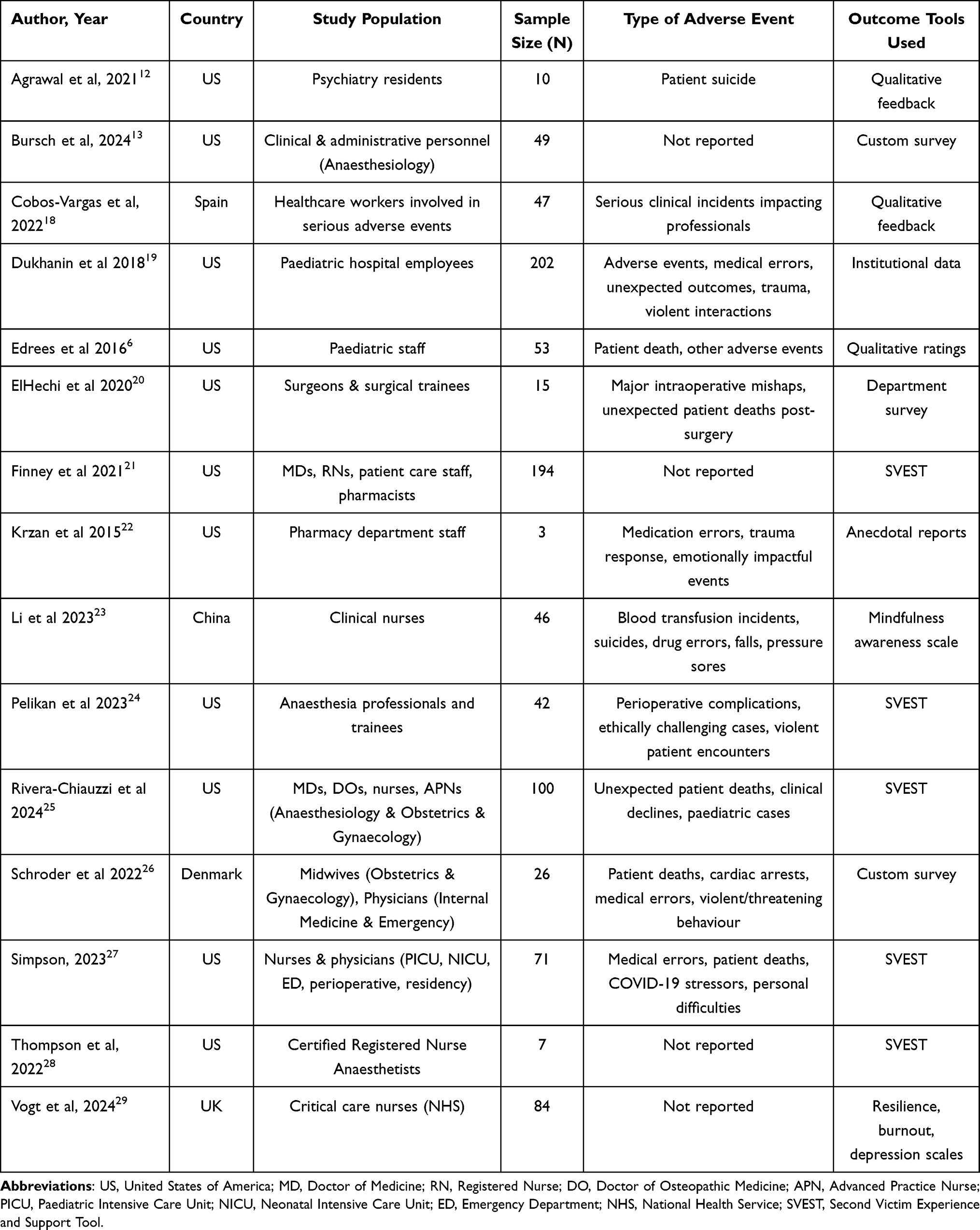 |
Table 1 Summary of Included Studies |
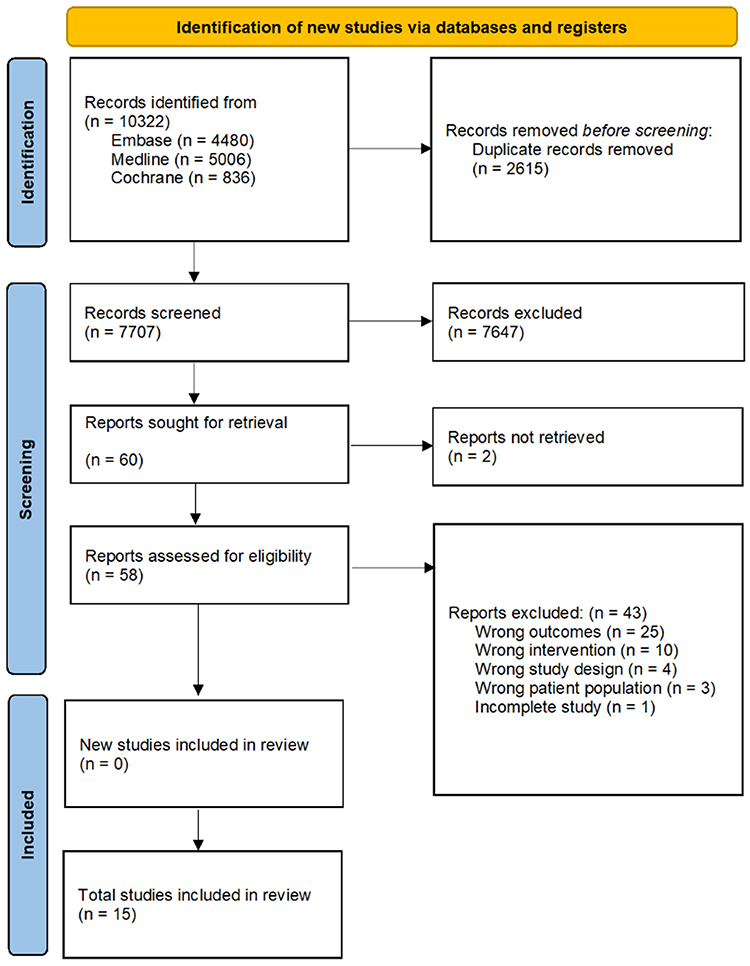 |
Figure 1 PRISMA flowchart showing study selection process. |
As shown in Table 1, a total of 11 studies were conducted in the United States (US),6,12,13,19–22,24,25,27,28 with the remaining 4 studies conducted in Spain,18 China,23 Denmark26 and the United Kingdom (UK),29 respectively. Participants were predominantly female and included HCPs across roles such as medical doctors, nurses, pharmacists, and administrative personnel. Three studies focused on paediatric departments. Definitions of SVS were roughly consistent across most studies, typically describing HCPs who after being involved in unanticipated adverse patient events, medical errors, or patient-related injuries, suffer physical or psychological sequelae. The programs differed slightly in terms of the adverse events studied, ranging from stressful circumstances,27 new or ethically challenging cases and unfamiliar work environments,24 to incidents in patient care such as medication errors, patient harm, decline or death6,18–20,22–27 and even patient suicide.15,23 Notably, four studies did not explicitly define the nature of adverse events studied.13,21,28,29
Across the included studies, several demographic trends were observed. Participants were predominantly female HCPs, reflecting broader workforce demographics in nursing and certain medical specialties. Many studies focused on staff from anesthesia and pediatric departments, which may be due to the high acuity and emotional demands associated with these specialties. A wide range of professional roles were represented, including nurses, physicians, residents, pharmacists, and allied health staff, indicating the cross-cutting occurrence of SVS across clinical hierarchies and disciplines. However, few studies disaggregated findings by profession or gender, limiting more nuanced analysis.
Quality Assessment
Quality of the included studies was assessed using the JBI checklist for quasi-experimental studies. Of the included studies, one (6.7%) was rated high quality,23 14 (93.3%) moderate quality,6,12,13,18–22,24–29 and none of low quality. Most studies defined their study variables, defined the outcome measurement, and employed appropriate statistical analyses. Common flaws included lack of control groups, insufficient justification for exclusions, and incomplete follow-up descriptions. Table S3 provides the detailed quality assessment findings.
Types of Interventions
Details of Second Victim Interventions and their key intervention characteristics and outcomes are summarised in Table 2. Majority of the studies involved peer support programs.6,12,13,18–22,24–29 Implemented in 13 studies, peer support programs were largely modelled after early initiatives such as forYOU, RISE, and HELP. These programs provided emotional and psychological first aid to Second Victims, either individually or in groups, with timing ranging from immediate outreach to multi-week follow-ups. Two studies used online formats,13,29 while others were in-person.6,12,18–28 Programs emphasized non-judgmental support, often employing Scott’s Three-Tiered Model of intervention.8
 |
Table 2 Summary of SVS Intervention Details and Outcomes |
Additionally, two studies evaluated specific psychological therapies; Vogt et al studied cognitive behavioural therapy (CBT) in individual and group settings,29 while Li et al implemented mindfulness and meditation techniques.23
Effectiveness of Interventions
To further elaborate on the outcomes achieved, for peer support programs, most studies reported positive short-term outcomes, including reduced loneliness, isolation, and emotional fatigue. For example, Simpson et al found significant reductions in perceived judgment and disengagement (p<0.01).27 However, in terms of long-term outcomes, these programs generally increased awareness of available resources and willingness to seek support,13,19,25 but there were mixed results for sustained improvements in professional efficacy and reduced turnover intentions.12,18
With regard to psychological therapies, Vogt et al reported significant reductions in burnout and depression (p<0.001) and improved resilience (p<0.001).29 Li et al demonstrated increased mindfulness and physical/mental coping skills (p<0.01).23
Few studies used standardized tools to evaluate interventions. Four studies assessed intervention effectiveness using the Second Victim Experience and Support Tool (SVEST),21,23,24,28 which reported mixed results across various dimensions. Psychological distress showed slight reductions post-intervention in some studies, but the improvements were statistically insignificant in most cases (p-values ranging from 0.04 to 0.61).21,24,28 Physical distress demonstrated minor declines post-intervention, though these changes were also not statistically significant (p-values ranging from 0.24 to 0.28).21,24,28 Colleague and supervisor support showed inconsistent trends. While one study (Li et al) reported a significant decline in perceived colleague and supervisor support following intervention (p<0.01),23 other studies found no meaningful changes (p-values ranging from 0.06 to 0.95).21,24,28 Institutional support, however, consistently improved across studies (p-values ranging from <0.01 to <0.001),21,23,24,28 indicating that interventions, particularly structured peer support programs, contributed to greater awareness and perceived organizational backing. Conversely, non-work-related support and professional self-efficacy did not show meaningful changes, with all studies reporting non-significant p-values (p = 0.13 to 0.78).21,23,24,28 Turnover intentions and absenteeism remained largely unchanged post-intervention, with negligible effect sizes (p-values ranging from 0.09 to 0.99).21,24,28 Overall, while peer support interventions and institutional support programs were associated with short-term improvements in perceived institutional backing, their impact on long-term psychological well-being, professional self-efficacy, and retention outcomes remain unclear.
GRADE Assessment of Certainty of Evidence
Using the GRADE framework, the overall certainty of evidence for short-term improvements in emotional well-being after peer support was rated as ‘Low’, primarily due to serious risk of bias (lack of control groups, small sample sizes) and imprecision. Evidence for long-term mental health outcomes (eg, reductions in burnout or depression) was ‘Very Low’, reflecting inconsistency among studies, lack of standardized measures, limited follow-up and the overall sparse number of studies. While individual studies of formal counseling or mindfulness reported promising results, the confidence in these findings remains ‘Low’. These data are likewise limited by small sample sizes and lack of control groups, resulting in an overall ‘Low’ certainty. The results for the GRADE methodology can be found in Table 3.
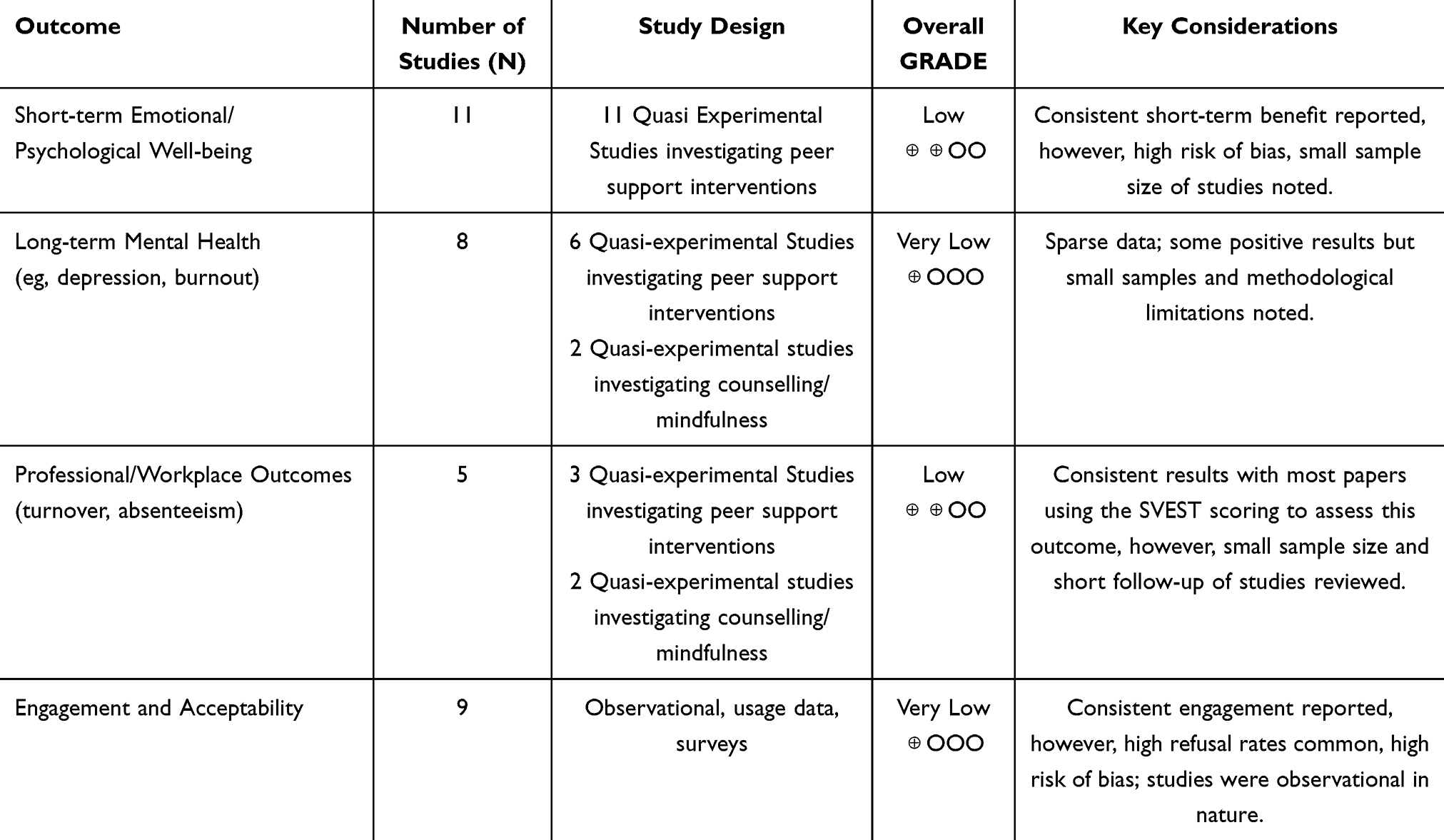 |
Table 3 GRADE Appraisal for Certainty of Intervention Outcomes |
Discussion
Based on the findings of our review, there are a number of interventions studied for tackling the issue of SVS. Peer support is the most widely studied intervention likely due to its simplicity, accessibility and adaptability to various healthcare settings.30 The immediate benefits of peer support include reduced feelings of loneliness, isolation, and emotional distress, with many participants reporting positive subjective experiences. However, peer support programs, albeit widely implemented and generally perceived as beneficial for immediate emotional support, may lack long-term efficacy for improving mental health and professional outcomes based on the overall body of evidence.6,12,13,18–22,24–29 Programs such as HELP,21 RISE,6 and forYOU7 aim to provide structured, tiered support, fostering a culture of institutional backing. However, the effectiveness of these interventions in terms of long-term psychological well-being and professional resilience remains unknown. To be effective, these programs also require some degree of customisation, co-production and tailoring to setting-specific implementation.30 The inherently transient nature of peer support encounters may limit their ability to address deeper psychological and emotional impacts.
Moreover, despite the availability of these programs and that participants generally reported satisfaction with peer support, only a subset of Second Victims engaged with the programs, with reported refusal rates of 40% to 65%. Several key barriers have been often cited. In one study, among 234 second Victims offered peer support, 58.1% declined, citing self-sufficiency, unfamiliarity with the program, or discomfort with peer supporters as primary reasons.27 Fear of judgment and lack of anonymity were minor concerns.27 Affected individuals may not recognize their own suffering as well as the importance of addressing the psychological impacts of adverse events.1,10,11 Although engagement and perceived acceptability of interventions in the studies reviewed appears high, this is likely skewed by those already willing to partake in these programs. There is a need for greater research into targeted strategies to increase the uptake by other Second Victims. Alternative programs should also be explored amongst those who find peer support less desirable.
While peer support can serve as a stepping stone, it is insufficient as a standalone solution, as highlighted by prior reviews.1,10,11 To enhance the effectiveness of peer support programs, structured training for peer supporters and tiered support models that provide escalation pathways are recommended. Trusted peer supporters—rather than anonymous individuals—may also enhance program acceptance and confidentiality. A multi-faceted strategy to support Second Victims, blending peer-based and professional interventions should be the focus of future research. Moreover, compared to peer support, structured psychological interventions, including mindfulness and CBT-based programs, demonstrated promising results, albeit only two studies assessed psychological interventions, making it difficult to draw firm conclusions.23,29 Vogt et al showed significant reductions in burnout and depression scores (p<0.001) following structured CBT sessions.29 Li et al reported increased mindfulness and improved emotional regulation (p<0.01) following a guided meditation and mindfulness-based intervention.23 These findings mirror broader literature on stress reduction interventions in HCPs, which suggests that counselling and mindfulness-based strategies may be more effective in fostering long-term resilience.31
In a recent meta-analysis, Ong et al reported that mindfulness-based interventions such as stress reduction programmes and meditation had significant emotional and psychological benefits to HCPs in general, although long-term outcomes were variable and not consistently sustained.31 The structured nature of these programs ensures that participants receive targeted coping strategies, unlike peer support models, which generally rely more on informal emotional validation. Hence, peer support programs should be viewed as an entry point for comprehensive SVS care, with mechanisms to escalate to other support and professional interventions as required. Integrating mindfulness and counselling into institutional frameworks may provide a more holistic approach, and a multi-faceted strategy blending peer-based and professional interventions should be the focus of future research.
Theoretical Implications
The findings of this review highlight important theoretical considerations for understanding SVS interventions. Peer support programs, while valuable for immediate relief, may not sufficiently address the extant psychological impact of adverse events. This aligns with stress-coping models and theories of trauma recovery, which emphasize the need for structured, guided processing to achieve long-term resilience.32 The review also underscores the importance of institutional culture as a mediating factor—HCPs’ perception of organizational support may influence not only engagement with interventions but also the trajectory of recovery. Furthermore, SVS can be framed within occupational stress and burnout frameworks, reinforcing the idea that post-event distress is not an isolated psychological issue but part of a broader ecosystem involving workload, team dynamics, and leadership behaviors. The paucity of reports of peer support improving long-term outcomes may point to the need for more integrated, system-level interventions that go beyond interpersonal coping to address structural contributors to distress.
Practical Implications
Although interventions to tackle SVS have been increasingly documented over recent years, to the best of our knowledge, this is the first paper attempting to systematically review the outcomes arising from such interventions. Existing reviews are sparse and focus mainly on reporting the availability of Second Victim support resources. A 2021 systematic review primarily investigated peer support interventions, with outcomes mainly related to descriptive statistics and self-reported benefits of the intervention itself.33 Similarly, a 2020 literature review by Stone provided a brief summary of SVS programs implemented,34 and a more recent scoping review by Wade et al focused only on mapping the available support at an institutional level.11 The aforementioned studies were also conducted some years ago between 2020 and 2021. Our review thus represents a significant advancement by synthesizing newer evidence on intervention outcomes, identifying key limitations, and providing direction for future research.
In terms of the areas for future research, there is a need for greater research into targeted strategies to increase coverage and engagement of potential Second Victims. It is well documented that stigma is a significant barrier to healthcare workers receiving mental health support in any form.35,36 It is therefore imperative that institutions and healthcare leaders continue raising awareness of support available while normalizing responses to adverse events, without stigmatising Second Victims who require support. Similar to the findings of a focus group conducted by the European Researchers’ Network Working on Second Victims (ERNST),37 the importance of a comprehensive occupational health approach, strong organisational safety culture, allocating adequate resources for ongoing support, securing leadership commitment, and tailoring interventions to the unique sociocultural and legal contexts of each institution and country cannot be overemphasized. Programs are more likely to be accepted and sustained when leadership visibly endorses them, when psychological safety is prioritized, and when organizational norms encourage open discussions about emotional well-being. Leadership training, trauma-informed supervision, and policies that normalize help-seeking behavior are thus crucial. Finally, the metric of outcome measurement was poorly standardized across papers. Given the equivocal nature of many of the subjective results from various studies, formal indicators of Second Victim outcomes and tools such as the SVEST38 to assess Second Victim interventions need to be used by future studies. Assessment of psychological symptoms should ideally use established questionnaires, for example, the Patient Health Questionnaire-9 (PHQ-9) for depression. We urge future studies to adopt appropriate survey and statistical techniques to assess significance and provide numerical outcomes where necessary, rather than generic survey questionnaires.
To situate SVS interventions within the broader healthcare resilience landscape, it is helpful to compare them to other established programs. For instance, Schwartz Rounds foster emotional reflection and team cohesion through narrative exchange,39 while Mindfulness-Based Stress Reduction (MBSR) and resilience training programs have shown sustained benefits on stress, empathy, and well-being in healthcare settings.31 Unlike SVS interventions, which often focus on reactive support after adverse events, these broader approaches tend to emphasize preventive resilience and are often more embedded into institutional routines. This suggests that combining the strengths of both models—reactive and preventive—could provide a more comprehensive support system for HCPs.
Limitations and Future Research
Nevertheless, several limitations of the review should be acknowledged. First, a major limitation in the current literature is the lack of standardized outcome metrics, as aforementioned. Many studies rely on subjective evaluations or non-validated tools, leading to equivocal findings. As previously mentioned, validated instruments such as the SVEST should be more widely adopted to enable robust comparisons across studies. Second, most of the included studies were short-term and most interventional studies to date focus more on process measures related to the delivery and perceived utility of the intervention, instead of analyzing outcomes related to the actual benefit to Second Victims, attrition data and follow-up on their status. Finally, the heterogeneous nature of the studies reviewed and their varied outcome measures precluded the possibility of conducting a meta-analysis.
Conclusion
In summary, this systematic review identified 15 studies analyzing Second Victim interventions and their outcomes. Peer support interventions were the most studied intervention and appeared feasible and appropriate as initial support methods, but their overall benefit tended to be equivocal. Structured psychological interventions, such as CBT and mindfulness programs, show promise but remain underexplored. Given the high prevalence of SVS and its implications for both HCPs and patient safety, future strategies should focus on integrated, multi-tiered models that combine peer support with access to professional mental health services. To advance the field, there is a pressing need for standardized outcome measures and longitudinal research to assess lasting impact and implementation effectiveness. More broadly, addressing SVS demands a shift from reactive, optional support to a proactive, institutionalized culture of psychological safety. Professional bodies such as the World Health Organisation (WHO), the American Medical Association (AMA), and their national counterparts should develop formal SVS response frameworks that provide institutions with guidance on best practices, implementation strategies, and evaluation metrics. Furthermore, we advocate for the integration of SVS awareness and support training into healthcare professional education, as well as continuing professional development, to ensure that HCPs are equipped to recognize and respond to emotional and psychological distress resulting from adverse events.
Data Sharing Statement
All articles in this manuscript are available from publicly available databases: Ovid/Medline, Embase and Cochrane.
Ethical Statements
The study was conducted in accordance with the Declaration of Helsinki. The study was exempt from IRB review as no original data was generated and no human participants were directly involved.
Acknowledgments
Timothy Sheng Khai Ong, Celeste Natasha Goh and Erel Kane Yun En Tan are co-first authors for this study. We thank Dr Kevin Xiang Zhou for reading an earlier version of the manuscript and providing useful comments and feedback. No part of this manuscript or its contents have been presented in any capacity outside of this manuscript as of the time of submission. This systematic review protocol was registered with PROSPERO (registration number CRD42024562333).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The manuscript has not received any funding in its synthesis.
Disclosure
All authors of the manuscript do not have a conflict of interest to declare.
References
1. Chong RIH, Yaow CYL, Chong NZ, et al. Scoping review of the second victim syndrome among surgeons: understanding the impact, responses, and support systems. Am J Surg. 2024;229:5–14.PMID: 37838505. doi:10.1016/j.amjsurg.2023.09.045
2. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320(7237):726–727. PMID: 10720336. doi:10.1136/bmj.320.7237.726
3. Seys D, Wu AW, Van Gerven E, et al. Health care professionals as second victims after adverse events: a systematic review. Eval Health Prof. 2013;36(2):135–162. PMID: 22976126. doi:10.1177/0163278712458918
4. Vanhaecht K, Seys D, Russotto S, et al. An evidence and consensus-based definition of second victim: a strategic topic in healthcare quality, patient safety, person-centeredness and human resource management. Int J Environ Res Public Health. 2022;19(24):16869.PMID: 36554750. doi:10.3390/ijerph192416869
5. Waterman AD, Garbutt J, Hazel E, et al. The emotional impact of medical errors on practicing physicians in the United States and Canada. Joint Commission J Quality Patient Safety. 2007;33(8):467–476. doi:10.1016/S1553-7250(07)33050-X
6. Edrees H, Connors C, Paine L, Norvell M, Taylor H, Wu AW. Implementing the RISE second victim support programme at the Johns Hopkins Hospital: a case study. BMJ Open. 2016;6(9):e011708. PMID: 27694486. doi:10.1136/bmjopen-2016-011708
7. Merandi J, Liao N, Lewe D, et al. Deployment of a second victim peer support program: a replication study. Pediatr Qual Saf. 2017;2(4):e031. doi:10.1097/pq9.0000000000000031
8. Scott SD, Hirschinger LE, Cox KR, et al. Caring for our own: deploying a systemwide second victim rapid response team. Jt Comm J Qual Patient Saf. 2010;36(5):233–240. PMID: 20480757. doi:10.1016/s1553-7250(10)36038-7
9. Coughlan B, Powell D, Higgins MF. The second victim: a review. Eur J Obstet Gynecol Reprod Biol. 2017;213:11–16.PMID: 28526169. doi:10.1016/j.ejogrb.2017.04.002
10. Nydoo P, Pillay BJ, Naicker T, Moodley J. The second victim phenomenon in health care: a literature review. Scand J Public Health. 2020;48(6):629–637. PMID: 31405351. doi:10.1177/1403494819855506
11. Wade L, Fitzpatrick E, Williams N, Parker R, Hurley KF. Organizational interventions to support second victims in acute care settings: a scoping study. J Patient Saf. 2022;18(1):e61–e72. PMID: 32404849. doi:10.1097/pts.0000000000000704
12. Agrawal A, Gitlin M, Melancon SNT, Booth BI, Ghandhi J, DeBonis K. Responding to a tragedy: evaluation of a postvention protocol among adult psychiatry residents. Acad Psychiatry. 2021;45(3):262–271. PMID: 33686537. doi:10.1007/s40596-021-01418-x
13. Bursch B, Ziv K, Marchese S, Aralis H, Bufford T, Lester P. Department of anesthesiology skilled peer support program outcomes: second victim perceptions. Jt Comm J Qual Patient Saf. 2024;50(6):442–448. PMID: 38556442. doi:10.1016/j.jcjq.2024.03.006
14. Guerra-Paiva S, Carrillo I, Mira J, et al. Developing core indicators for evaluating second victim programs: an international consensus approach. Int J Public Health. 2024;69:1607428.PMID: 39280904. doi:10.3389/ijph.2024.1607428
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PMID: 33782057. doi:10.1136/bmj.n71
16. Barker TH, Habibi N, Aromataris E, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evid Synth. 2024;22(3):378–388. PMID: 38287725. doi:10.11124/jbies-23-00268
17. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD.
18. Cobos-Vargas A, Perez-Perez P, Nunez-Nunez M, Casado-Fernandez E, Bueno-Cavanillas A. Second victim support at the core of severe adverse event investigation. Int J Environ Res Public Health. 2022;19(24):16850. PMID: 36554728. doi:10.3390/ijerph192416850
19. Dukhanin V, Edrees HH, Connors CA, Kang E, Norvell M, Wu AW. Case: a second victim support program in pediatrics: successes and challenges to implementation. J Pediatr Nurs. 2018;41:54–59.PMID: 29395793. doi:10.1016/j.pedn.2018.01.011
20. El Hechi MW, Bohnen JD, Westfal M, et al. Design and impact of a novel surgery-specific second victim peer support program. J Am Coll Surg. 2020;230(6):926–933. PMID: 31857209. doi:10.1016/j.jamcollsurg.2019.10.015
21. Finney RE, Czinski S, Fjerstad K, et al. Evaluation of a second victim peer support program on perceptions of second victim experiences and supportive resources in pediatric clinical specialties using the second victim experience and support tool (SVEST). J Pediatr Nurs. 2021;61:312–317. PMID: 34500175. doi:10.1016/j.pedn.2021.08.023
22. Krzan KD, Merandi J, Morvay S, Mirtallo J. Implementation of a “second victim” program in a pediatric hospital. Am J Health Syst Pharm. 2015;72(7):563–567. PMID: 25788510. doi:10.2146/ajhp140650
23. Li J, Yan X, Chen G, Sun H. Mindfulness meditation intervention improves the mindfulness awareness level of nurses’ second victims to enhance their psychological support. SAGE Open Nurs. 2023;9:23779608231178136.PMID: 37273551. doi:10.1177/23779608231178136
24. Pelikan M, Finney RE, Jacob A. Use of the second victim experience and support tool (SVEST) to assess the impact of a departmental peer support program on anesthesia professionals’ second victim experiences (SVEs) and perceptions of support two years after implementation. AANA J. 2023;91(5):371–379. PMID: 37788179.
25. Rivera-Chiauzzi EY, Huang L, Osborne AK, et al. Rapid expansion of the healing emotional lives of peers program during COVID-19: a second victim peer support program for healthcare professionals. J Patient Saf. 2024;20(1):28–37. PMID: 37966348. doi:10.1097/pts.0000000000001179
26. Schroder K, Bovil T, Jorgensen JS, Abrahamsen C. Evaluation of’the Buddy Study’, a peer support program for second victims in healthcare: a survey in two Danish hospital departments. BMC Health Serv Res. 2022;22(1):566. PMID: 35477365. doi:10.1186/s12913-022-07973-9
27. Simpson SL, Khan S, Schiferl LM, et al. Implementation of a peer-to-peer support program in a quaternary pediatric medical center. Acad Pediatr. 2023;23(8):1481–1488. PMID: 37482296. doi:10.1016/j.acap.2023.07.004
28. Thompson M, Hunnicutt R, Broadhead M, Vining B, Aroke EN. Implementation of a certified registered nurse anesthetist second victim peer support program. J Perianesth Nurs. 2022;37(2):167–73e1. PMID: 34980539. doi:10.1016/j.jopan.2021.05.005
29. Vogt KS, Johnson J, Coleman R, et al. Can the Reboot coaching programme support critical care nurses in coping with stressful clinical events? A mixed-methods evaluation assessing resilience, burnout, depression and turnover intentions. BMC Health Serv Res. 2024;24(1):343. PMID: 38491374. doi:10.1186/s12913-023-10468-w
30. Cooper RE, Saunders KRK, Greenburgh A, et al. The effectiveness, implementation, and experiences of peer support approaches for mental health: a systematic umbrella review. BMC Med. 2024;22(1):72. PMID: 38418998. doi:10.1186/s12916-024-03260-y
31. Ong NY, Teo FJJ, Ee JZY, et al. Effectiveness of mindfulness-based interventions on the well-being of healthcare workers: a systematic review and meta-analysis. Gen Psychiatr. 2024;37(3):e101115. PMID: 38737894. doi:10.1136/gpsych-2023-101115
32. Calhoun CD, Stone KJ, Cobb AR, Patterson MW, Danielson CK, Bendezú JJ. The role of social support in coping with psychological trauma: an integrated biopsychosocial model for posttraumatic stress recovery. Psychiatr Q. 2022;93(4):949–970. PMID: 36199000. doi:10.1007/s11126-022-10003-w
33. Busch IM, Moretti F, Campagna I, et al. Promoting the psychological well-being of healthcare providers facing the burden of adverse events: a systematic review of second victim support resources. Int J Environ Res Public Health. 2021;18(10):5080. PMID: 34064913. doi:10.3390/ijerph18105080
34. Stone M. Second victim support programs for healthcare organizations. Nurs Manage. 2020;51(6):38–45. PMID: 32472858. doi:10.1097/01.NUMA.0000662664.90688.1d
35. Sedile R, Zizza A, Bastiani L, et al. Understanding the second victim phenomenon among healthcare workers in an Italian hospital. Eur J Investig Health Psychol Educ. 2024;14(12):3073–3086. PMID: 39727509. doi:10.3390/ejihpe14120201
36. Yaow CYL, Ng QX, Chong RIH, et al. Intraoperative adverse events among surgeons in Singapore: a multicentre cross-sectional study on impact and support. BMC Health Serv Res. 2024;24(1):512. PMID: 38659030. doi:10.1186/s12913-024-10998-x
37. Mira JJ, Carrillo I, Gil-Hernández E, et al. Key elements for designing effective second victim support interventions: a focus group study in European clinical settings. BMJ Open. 2025;15(1):e089923. PMID: 39762106. doi:10.1136/bmjopen-2024-089923
38. Yj DMY, Ng QX, Teoh SE, Loh CYL, Xin X, Thumboo J. Validation and use of the second victim experience and support tool questionnaire: a scoping review. Public Health. 2023;223:183–192.PMID: 37672831. doi:10.1016/j.puhe.2023.08.003
39. Maben J, Taylor C, Reynolds E, McCarthy I, Leamy M. Realist evaluation of Schwartz rounds® for enhancing the delivery of compassionate healthcare: understanding how they work, for whom, and in what contexts. BMC Health Serv Res. 2021;21(1):709. PMID: 34275468. doi:10.1186/s12913-021-06483-4
40. Bamdad MC, Vitous CA, Rivard SJ, et al. The best gift you could give a resident: a qualitative study of well-being resources and use following unwanted outcomes. Annals Surgery Open. 2022;3(2):e139. doi:10.1097/AS9.0000000000000139
41. Bredenkamp K, Raschka MJ, Holmes A. A review of medication errors and the second victim in pediatric pharmacy. J Pediatr Pharmacol Ther. 2024;29(2):100–106. doi:10.5863/1551-6776-29.2.100
42. Burlison JD, Scott SD, Browne EK, Thompson SG, Hoffman JM. The second victim experience and support tool: validation of an organizational resource for assessing second victim effects and the quality of support resources. J Patient Safety. 2017;13(2):93–102. doi:10.1097/PTS.0000000000000129
43. Chen J, Ghardallou W, Comite U, et al. Managing hospital employees’ burnout through transformational leadership: the role of resilience, role clarity, and intrinsic motivation. Int J Environ Res Public Health. 2022;19(17). doi:10.3390/ijerph191710941
44. Shuang S, Shi X. Balint Group’s intervention effect on the psychological resilience of the second victim of nurses. ChiCtr. 2024;PubMed PMID: CN-02690666.
45. Copley DJ, Burchill CN, Lindell D, Dolansky MA. Second victim phenomenon educational program evaluation. J Nurses Prof Dev. 2024;40(1):10–15. doi:10.1097/NND.0000000000000978
46. Eidt JF, Mannoia K. A toolkit for individualizing interventions to mitigate second-victim syndrome in a diverse surgery community. J Vasc Surg Venous Lymph Disord. 2024;12(2):101680. doi:10.1016/j.jvsv.2023.08.019
47. Fall F, Hu YY, Walker S, et al. Peer support to promote surgeon well-being: the APSA program experience. J Pediatric Surg. 2024;59(jmj, 0052631):1665–1671. doi:10.1016/j.jpedsurg.2023.12.022
48. Fatima S, Soria S, Esteban-Cruciani N. Medical errors during training: how do residents cope?: a descriptive study. Bmc Med Educ. 2021;21(1):408. doi:10.1186/s12909-021-02850-1
49. Fendel JC, Aeschbach VM, Schmidt S, Goritz AS. The impact of a tailored mindfulness-based program for resident physicians on distress and the quality of care: a randomised controlled trial. J Internal Med. 2021;290(6):1233–1248. doi:10.1111/joim.13374
50. Ferrus L, Silvestre C, Olivera G, Mira JJ. Qualitative study about the experiences of colleagues of health professionals involved in an adverse event. J Patient Safety. 2021;17(1):36–43. doi:10.1097/PTS.0000000000000309
51. Govindan M, Keefer P, Sturza J, Stephens MR, Malas N. Empowering residents to process distressing events: a debriefing workshop. MedEdPORTAL. 2019;15(101714390):10809. doi:10.15766/mep_2374-8265.10809
52. Gupta K, Rivadeneira NA, Lisker S, Chahal K, Gross N, Sarkar U. Multispecialty physician online survey reveals that burnout related to adverse event involvement may be mitigated by peer support. J Patient Safety. 2022;18(6):531–538. doi:10.1097/PTS.0000000000001008
53. Harrison R, Lawton R, Perlo J, Gardner P, Armitage G, Shapiro J. Emotion and coping in the aftermath of medical error: a cross-country exploration. J Patient Safety. 2015;11(1):28–35. doi:10.1097/PTS.0b013e3182979b6f
54. Harrison R, Wu A. Critical incident stress debriefing after adverse patient safety events. Am J Manag Care. 2017;23(5):310–312.
55. Hess A, Flicek T, Watral AT, et al. BONE break: a hot debrief tool to reduce second victim syndrome for nurses. Jt Comm J Qual Patient Saf. 2024;50(101238023):673–677. doi:10.1016/j.jcjq.2024.05.005
56. Kappes M, Romero-Garcia M, Sanchez M, Delgado-Hito P. Coping trajectories of intensive care nurses as second victims: a grounded theory. Austr Crit Care. 2024;37(4):606–613. doi:10.1016/j.aucc.2024.01.001
57. Kershaw K. Adverse clinical incidents: support for midwives. RCM Midwives. 2007;10(10):462–465.
58. Khajouei R, Afzali F, Bagheri F, Jahanbakhsh F. The effect of electronic error-reporting forms on nurse’s stress and the rate of error-reporting. Health Info J. 2023;29(4):14604582231212518. doi:10.1177/14604582231212518
59. Khansa I, Pearson GD. Coping and recovery in surgical residents after adverse events: the second victim phenomenon. Plastic Reconst Surg Global Open. 2022;10(3):e4203. doi:10.1097/GOX.0000000000004203
60. Lane MA, Newman BM, Taylor MZ, et al. Supporting clinicians after adverse events: development of a clinician peer support program. J Patient Safety. 2018;14(3):e56–e60. doi:10.1097/PTS.0000000000000508
61. Lewis EJ, Baernholdt MB, Yan G, Guterbock TG. Relationship of adverse events and support to RN burnout. J Nurs Care Quality. 2015;30(2):144–152. doi:10.1097/NCQ.0000000000000084
62. Li X, Che CC, Li Y, Wang L, Chong MC. The mediating role of coping styles in the relationship between second victim experience and professional quality of life among nurses: a cross-sectional study. BMC Nurs. 2023;22(1):312. doi:10.1186/s12912-023-01473-9
63. Marmon LM, Heiss K. Improving surgeon wellness: the second victim syndrome and quality of care. Seminars Pediatric Surg. 2015;24(6):315–318. doi:10.1053/j.sempedsurg.2015.08.011
64. Marr R, Goyal A, Quinn M, Chopra V. Support opportunities for second victims lessons learned: a qualitative study of the top 20 US News and World Report Honor Roll Hospitals. BMC Health Serv Res. 2021;21(1):1330. doi:10.1186/s12913-021-07315-1
65. Mira JJ, Carrillo I, Guilabert M, et al. The second victim phenomenon after a clinical error: the design and evaluation of a website to reduce caregivers’ emotional responses after a clinical error. J Med Internet Res. 2017;19(6):e203. doi:10.2196/jmir.7840
66. Mira JJ, Lorenzo S, Carrillo I, et al. Interventions in health organisations to reduce the impact of adverse events in second and third victims. BMC Health Serv Res. 2015;15:341. Epub 20150822. PubMed PMID: 26297015; PubMed Central PMCID: PMC4546284. doi:10.1186/s12913-015-0994-x
67. Mohd Kamaruzaman AZ, Ibrahim MI, Mokhtar AM, Mohd Zain M, Satiman SN, Yaacob NM. The effect of second-victim-related distress and support on work-related outcomes in Tertiary Care Hospitals in Kelantan, Malaysia. Int J Environ Res Public Health. 2022;19(11):6454. doi:10.3390/ijerph19116454
68. Mok WQ, Chin GF, Yap SF, Wang W. A cross-sectional survey on nurses’ second victim experience and quality of support resources in Singapore. J Nurs Manag. 2020;28(2):286–293. doi:10.1111/jonm.12920
69. Reiser Crelier F, Schwappach D, Schwendimann R. Supporting health professionals after an adverse event in Swiss hospitals: a cross-sectional study. Swiss Med Weekly. 2020;150(d10, 100970884):w20278. doi:10.4414/smw.2020.20278
70. Schiechtl B, Hunger MS, Schwappach DL, Schmidt CE, Padosch SA. Second victim: critical incident stress management in clinical medicine. Der Anaesthesist. 2013;62(9):734–741. doi:10.1007/s00101-013-2215-5
71. Scrimgeour G, Turner K. Hospital and departmental level strategies for managing the impact of adverse events on surgeons. Urol Oncol. 2024;42(9805460):310–314. doi:10.1016/j.urolonc.2024.03.002
72. Seitz KP, Baclig NV, Stiller R, Chen A. Implementation of a near-peer support program to improve trainee well-being after patient safety events. ATS Scholar. 2023;4(4):423–430. doi:10.34197/ats-scholar.2023-0011PS
73. Shapiro J, Galowitz P. Peer support for clinicians: a programmatic approach. Acad med. 2016;91(9):1200–1204. doi:10.1097/ACM.0000000000001297
74. Tamburri LM. Creating healthy work environments for second victims of adverse events. AACN Advanced Critical Care. 2017;28(4):366–374. doi:10.4037/aacnacc2017996
75. Trent M, Waldo K, Wehbe-Janek H, Williams D, Hegefeld W, Havens L. Impact of health care adversity on providers: lessons learned from a staff support program. J Healthcare Risk Manag. 2016;36(2):27–34. doi:10.1002/jhrm.21239
76. van Pelt F. Peer support: healthcare professionals supporting each other after adverse medical events. Qual Saf Health Care. 2008;17(4):249–252. doi:10.1136/qshc.2007.025536
77. White AA, Brock DM, McCotter PI, et al. Risk managers’ descriptions of programs to support second victims after adverse events. J Healthcare Risk Manag. 2015;34(4):30–40. doi:10.1002/jhrm.21169
78. Winning AM, Merandi JM, Lewe D, et al. The emotional impact of errors or adverse events on healthcare providers in the NICU: the protective role of coworker support. J Adv Nurs. 2018;74(1):172–180. doi:10.1111/jan.13403
79. Zhang X, Li Q, Guo Y, Lee S-Y. From organisational support to second victim-related distress: role of patient safety culture. J nurs manag. 2019;27(8):1818–1825. doi:10.1111/jonm.12881
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.