Back to Journals » Journal of Asthma and Allergy » Volume 14
Second-Hand Smoke Exposure Associated with Risk of Respiratory Symptoms, Asthma, and COPD in 20,421 Adults from the General Population
Authors Korsbæk N ![]() , Landt EM, Dahl M
, Landt EM, Dahl M ![]()
Received 3 August 2021
Accepted for publication 13 October 2021
Published 28 October 2021 Volume 2021:14 Pages 1277—1284
DOI https://doi.org/10.2147/JAA.S328748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Nanna Korsbæk,1,2 Eskild M Landt,1 Morten Dahl1,2
1Department of Clinical Biochemistry, Zealand University Hospital, Køge, Denmark; 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Morten Dahl
Department of Clinical Biochemistry, Zealand University Hospital, Lykkebækvej 1, Køge, DK-4600, Denmark
Tel +4547325545
Email [email protected]
Rationale: Individuals exposed to second-hand smoking may be more susceptible to asthma and chronic obstructive pulmonary disease (COPD). We investigated the risk of respiratory symptoms, asthma, and COPD in adults exposed to second-hand smoking at different stages of life in the general population.
Methods: We identified individuals who had been exposed to second-hand smoking in childhood only, adulthood only, or lifelong in a cohort of 20,421 adults from the Danish General Suburban Population Study and recorded respiratory symptoms, lung function, asthma, and COPD as outcomes.
Results: Among 20,421 adults from the general population, 2,551 (12%) had been lifelong exposed to second-hand smoking, 459 (2%) had been exposed in adulthood only, and 13,998 (69%) had been exposed in childhood only; the mean ages of the three groups were 54 years, 55 years, and 57 years, respectably, compared with 56 years in non-exposed individuals (P< 0.001). Equivalent values for the prevalence of current smoking were 25%, 20%, and 18% versus 12% (P< 0.001). After adjustment for age, smoking, and sex, the odds ratios for wheezing, severe dyspnoea, cough on exertion, and asthma increased as a function of second-hand smoke exposure (Ps≤ 0.004); individuals who had been exposed to second-hand smoking lifelong, in adulthood only, or in childhood only versus non-exposed had increased odds ratios for wheezing of 1.62 (95% CI=1.41– 1.87), 1.50 (1.15– 1.94), and 1.16 (1.04– 1.30). Corresponding values were 2.08 (1.52– 2.85), 2.05 (1.22-3-44), and 1.23 (0.95– 1.59) for severe dyspnoea, 1.56 (1.33– 1.83), 1.53 (1.15– 2.02), and 1.19 (1.05– 1.35) for cough on exertion, 1.36 (1.14– 1.63), 1.49 (1.09– 2.05), and 1.13 (0.99– 1.30) for asthma, and 1.24 (1.03– 1.48), 1.25 (0.90– 1.74), and 1.09 (0.96– 1.24) for COPD. The population attributable fractions of asthma and COPD due to lifelong second-hand smoke exposure were 4.3% and 2.9%.
Conclusion: Individuals exposed to lifelong second-hand smoking have increased risks of respiratory symptoms, asthma, and COPD, and may account for 4.3% and 2.9% of people with asthma and COPD in the general population.
Keywords: atopy, chronic obstructive pulmonary disease, passive smoking, pulmonary function, wheezing
Introduction
Exposure to second-hand smoking leads to more than 880,000 deaths annually according to the World Health Organization.1–3 Exposure to second-hand smoke for 1 hour has been shown to reduce lung function for the following hour, and prolonged second-hand smoke exposure has been shown to increase wheezing and other respiratory symptoms, and perhaps the susceptibility to asthma and chronic obstructive pulmonary disease (COPD).4–7
Passive smoking has been extensively studied in children, and it has been found that maternal smoking during pregnancy and childhood reduces lung function, and increases the risks of asthma and wheezing in offspring.5,6,8,9 It has been suggested that the lungs are vulnerable during pregestation and childhood, and that second-hand smoke exposure during these stages may be particularly damaging to the lungs.6,8,10 Studies have also suggested that second-hand smoke exposure in adult life leads to reduced lung function, and maybe increased risk of asthma and COPD, as well as respiratory symptoms such as breathlessness and coughing.11–13 However, studies of risk of asthma and COPD in adults according to second-hand smoke exposure in childhood only, adulthood only, or lifelong are limited.
We hypothesized that individuals exposed to second-hand smoking in childhood, adulthood, and/or lifelong compared to non-exposed are at higher risk for respiratory symptoms, asthma, and COPD in the general population. To test this, we identified second-hand smoke exposure at different stages of life in a cohort of 20,421 individuals from the Danish General Suburban Population Study and recorded respiratory symptoms, lung function, asthma, and COPD as outcomes.
Materials and Methods
Study Design and Participants
The Danish General Suburban Population Study is a cross-sectional study performed from 2010–2013 in the Danish municipality of Næstved.14 All individuals in Denmark are assigned a unique identification number at birth/immigration and recorded in the national Danish Civil Registration System. By using this unique number, individuals aged 20+ were randomly selected and invited from the National Danish Civil Registration System to reflect the adult Danish Population. A total of 21,205 individuals completed a comprehensive questionnaire and underwent a physical health examination.14 The study was approved by the institutional review board at Zealand University Hospital (Dept of Production, Forskning og Innovation, REG-077-2018) and the local ethical committee of Region Zealand (SJ-113, SJ-114) and was conducted according to the Declaration of Helsinki. All participants provided written informed consent.
Study Outcomes and Spirometry
Dyspnoea was graded according to a slightly modified version of the British Medical Research Council questionnaire’s breathlessness scale grade II and IV as previously described:15 Light dyspnoea was an affirmative response to the question “Do you get shortness of breath when you walk at an ordinary pace alongside someone your own age?” and severe dyspnoea was an affirmative response to the question “Do you get shortness of breath during morning toilette or when you get dressed?”. Wheezing was defined as whistling or wheezing while breathing. Cough on exertion was defined by coughing during physical activity. Smoking status was defined as never, former, or current smoking. Physician-diagnosed asthma was defined as an affirmative response to the question “Has a physician ever told you that you have/have had asthma?”. Lung function was measured by a hand-held Spirometer (MicroLoop, Micro Medical Ltd, Kent, UK) as described.14 Predicted values of FEV1% and FVC% were calculated based on international derived reference values.16 COPD was defined as prebronchodilator FEV1/FVC<0.7 excluding asthmatics.
Definition of Study Population
Exposure to second-hand smoke in childhood was self-reported maternal smoking during pregnancy and/or parental smoking in the childhood home. Exposure to second-hand smoking in adulthood was self-reported >1 hour/day exposure to passive smoking (ie, tobacco smoke) in adults aged 20 years and above. Lifelong second-hand smoke exposure was defined as self-reported exposure to second-hand smoking during childhood and adulthood.
Statistical Analyses
We used STATA 12.1 for the statistical analyses (StataCorp, College Station, TX). A two-tailed P-value<0.05 was considered significant. Categorical variables were analysed using Pearson’s χ2-test, and continuous variables were analysed using the Student’s t-test. Logistic regression models were adjusted for age, sex, and smoking status as appropriate. Population attributable fractions were calculated to estimate the fraction of asthma and COPD cases attributable to lifelong second-hand smoking exposure in the study sample: PAF = f(OR−1))/(1+f(OR−1), where f is the prevalence of second-hand smoking in the study sample.
Results
Socio-Demographics
Among the 20,421 adults in the Danish General Suburban Population Study, 13,998 (69%) had been exposed to second-hand smoking during childhood only, 459 (2%) had been exposed to second-hand smoke during adulthood only, and 2,551 (12%) had been exposed to lifelong second-hand smoke exposure (Table 1). Individuals exposed to lifelong second-hand smoking were more likely younger (54.1 years), males (52%), and current smokers (25%) compared to non-exposed individuals (Table 1). Individuals exposed to second-hand smoke during adulthood only versus non-exposed were more likely males (51%) and current smokers (20%), while those individuals who were exposed to second-hand smoke in childhood only were more likely older (56.6 years) and current smokers (18%).
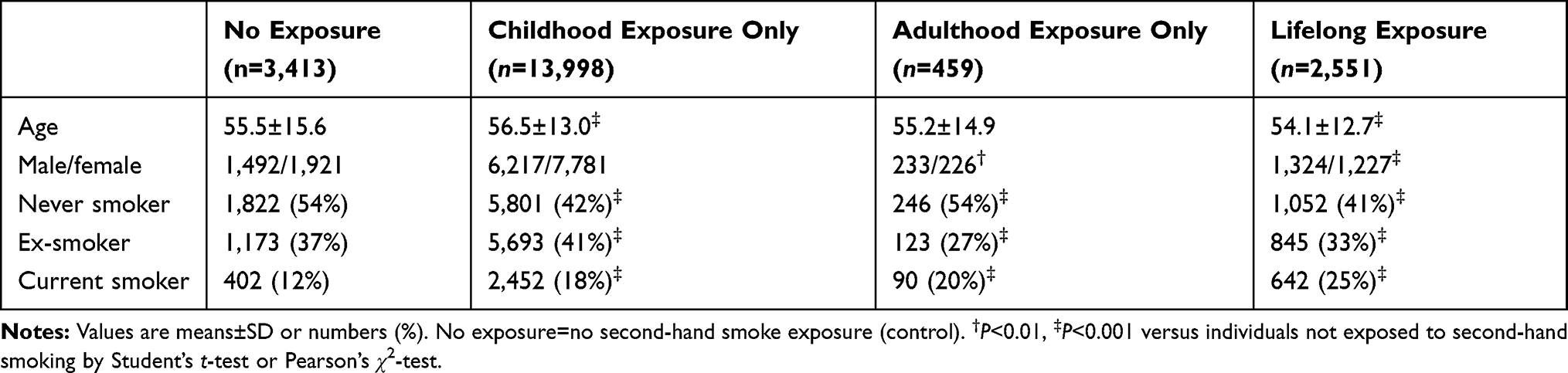 |
Table 1 Characteristics of Individuals Exposed to Second-Hand Smoking in the General Population |
Respiratory Symptoms
The multiple adjusted odds ratios for light dyspnea, severe dyspnea, wheezing, and cough on exertion increased as a function of second-hand smoke exposure in the general population (Ps<0.001; Figure 1). Individuals who had been exposed to second-hand smoking lifelong, in adulthood only, or in childhood only had increased odds ratios for light dyspnea of 1.76 (95% CI=1.47–2.11), 1.43 (1.02–2.00), and 1.14 (0.99–1.31), respectively, compared with non-exposed individuals. Corresponding values for severe dyspnea were 2.08 (1.52–2.85), 2.05 (1.22-3-44), and 1.23 (0.95–1.59), for wheezing 1.62 (1.41–1.87), 1.50 (1.15–1.94), and 1.16 (1.04–1.30), and for cough on exertion 1.56 (1.33–1.83), 1.53 (1.15–2.02), and 1.19 (1.05–1.35).
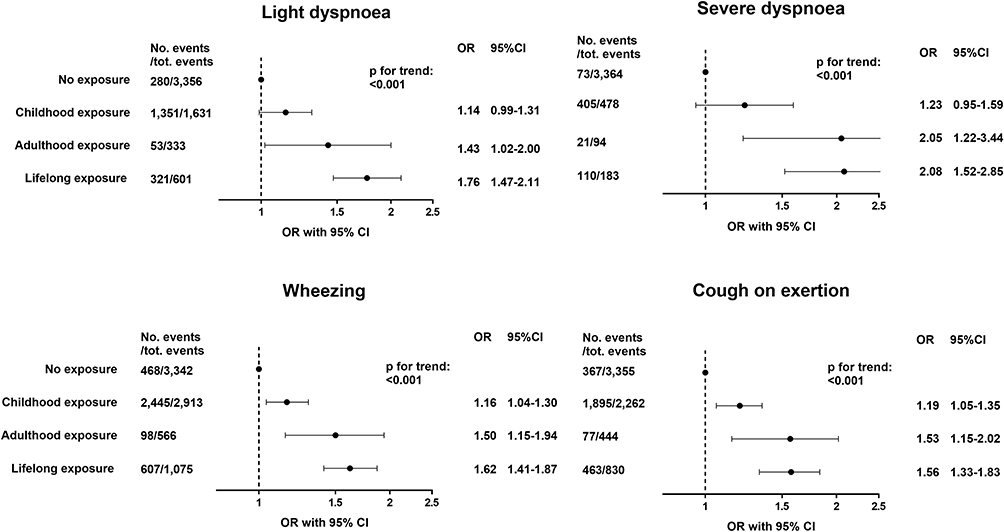 |
Figure 1 Risk of light dyspnoea, severe dyspnoea, wheezing, and cough on exertion in individuals exposed to second-hand smoking in the general population. Logistic regression models adjusted for age, sex, and smoking status. |
Lung Function
FEV1% predicted and FVC% predicted were significantly reduced as a function of second-hand smoke exposure in the general population (Ps<0.001, Figure 2). Individuals who had been exposed to second-hand smoking lifelong, in adulthood only, or in childhood only had reduced FEV1% predicted values of 93%, 95%, and 95%, respectively, compared with 97% in non-exposed individuals. Corresponding values for FVC% predicted were 97%, 97%, and 99% versus 100% in non-exposed individuals.
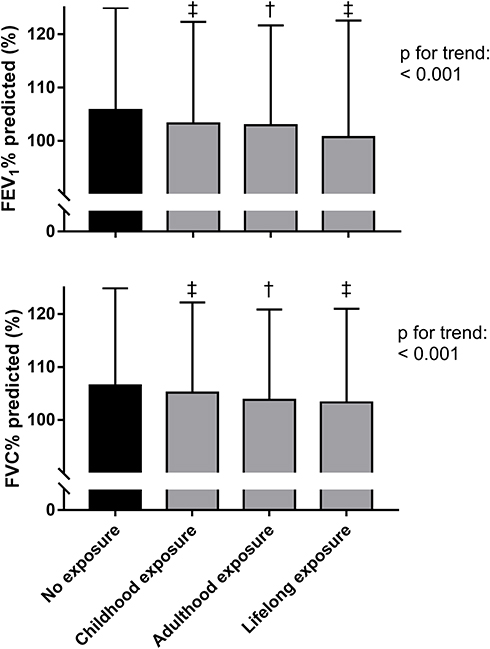 |
Figure 2 FEV1% predicted and FVC% predicted in individuals exposed to second-hand smoking in the general population. Values are mean and SD. †P<0.01, ‡P<0.001 versus individuals not exposed to second-hand smoking. |
The reduction of 4% in FEV1% predicted in individuals who had been exposed to lifelong second-hand smoking versus non-exposed corresponds to a 102 mL reduction of FEV1 in an average 55 year old female of 165 cm height, or a 118 mL reduction of FEV1 in an average 55 year old male of 180 cm height. Corresponding values for the 3% reduction in FVC% predicted related to lifelong second-hand smoking were 85 mL in a 55 year old female of 165 cm height and 101 mL in a 55 year old male of 180 cm height.
Risk of Asthma and COPD
The multiple adjusted odds ratios for physician-diagnosed asthma increased as a function of second-hand smoke exposure, but not for COPD (Figure 3). Individuals who had been exposed to second-hand smoking lifelong, in adulthood only, or in childhood only had increased odds ratios for physician-diagnosed asthma of 1.36 (1.14–1.63), 1.49 (1.09–2.05), and 1.13 (0.99–1.30), respectively, compared with non-exposed individuals (Figure 3). Corresponding values for COPD were 1.24 (1.03–1.48), 1.25 (0.90–1.74), and 1.09 (0.96–1.24). When the definition of asthma included individuals receiving daily asthma medication, similar results were seen (Supplementary Figure 1). Individuals who had been exposed to second-hand smoking lifelong, in adulthood only, or in childhood only had odds ratios for atopy of 1.14 (0.99–1.32), 1.22 (0.93–1.59), and 1.22 (1.10–1.36), respectively, compared with non-exposed individuals (Supplementary Figure 2).
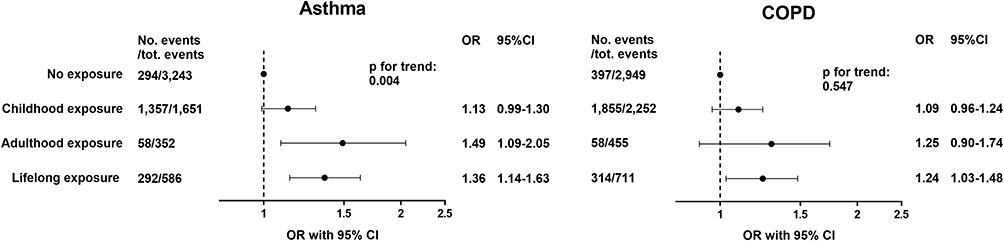 |
Figure 3 Risk of asthma and COPD in individuals exposed to second-hand smoking in the general population. Logistic regression models adjusted for age, sex, and smoking status. |
In sensitivity analyses when stratifying according to smoking status, similar results were seen, except for COPD risk, which was elevated in ever smokers but not in never smokers (Supplementary Figures 3–5). When stratifying according to sex, similar results were seen, except for asthma risk, which was elevated in females but not in males (Supplementary Figures 6–8). When stratifying according to the presence of airway obstruction, similar results were seen, except for asthma risk, which was increased in individuals without airway obstruction but not in individuals with airway obstruction (Supplementary Figures 9–11). When analyzing only those individuals who were below 40 years with estimated fewer years of memory recall, similar results were seen for asthma risk, and similar but elevated results were seen for two out of three of the analyses for COPD, although the differences did not achieve statistical significance for all the analyses (Supplementary Figure 12). Because of the small size of the subgroups analyses, these results should be interpreted with care.
Discussion
Our study of a cohort of 20,421 adults contributes results from the hitherto largest study of second-hand smoke exposure at different life stages in the general population. The main finding of this study is of a dose–response relation between exposure to second-hand smoking and respiratory symptoms, pulmonary function, and risk of asthma in the general population. We found that individuals who had been exposed lifelong to second-hand smoking versus non-exposed had more light dyspnoea, severe dyspnoea, wheezing, and cough on exertion, 3–4% reductions in FEV1% predicted and FVC% predicted, a 1.36-fold increased risk of physician-diagnosed asthma, and a 1.24-fold increased risk of COPD. The study also revealed that second-hand smoke exposure in adulthood was associated with reduced lung function, and with increased risks for dyspnoea, wheezing, cough, and asthma, while second-hand smoke exposure in childhood was associated with reduced lung function, and with increased risks of wheezing and cough in adults.
Consistent with our finding of an elevated odds ratio for physician-diagnosed asthma of 1.36, previous reports have also observed positive associations between second-hand smoke exposure and asthma risk or asthma-related symptoms in adults.5,9,12 An American study of 46,182 women found an elevated hazard ratio for incident asthma of 1.21 in those individuals who had been exposed to second-hand smoking for at least 1 hour per day for 12 consecutive months or more,17 and a Korean study of 820,710 adults found odds ratios for ever asthma of 1.13 (95% CI=1.02–1.26) and 1.14 (0.94–1.39) in those who had been exposed to second-hand smoking for at least 1 hour per day at work or at home, respectively.18 Three other recent studies of adults found no significant associations between passive smoking and asthma risk in overall analyses, but found significant associations for wheeze, asthma symptom score, and/or lung function decline supporting that second-hand smoking exposure may contribute to asthma-related symptoms and asthma in adults.19–21
In the current study, we showed that individuals who had been exposed to second-hand smoking lifelong or in adulthood only had more dyspnoea, wheeze, cough, and reduced lung function. These respiratory symptoms in adults who had been exposed to second-hand smoking corroborate the results from previous studies,19–21 and accord with the observed higher prevalence of asthma in our study. In support, the results also showed that individuals who had been exposed to second-hand smoking in childhood only had more wheezing, cough, reduced lung function, and a trend towards higher risk of asthma. If our results show the true magnitude of the effect of second-hand smoke exposure on asthma in the general population, it can be estimated as a population attributable fraction that lifelong second-hand smoking may account for 4.3% of asthma in the study sample. This indicates that exposure to second-hand smoking contributes to a significant number of asthma cases in the general population. Estimates of population attributable fractions from previous studies using other study populations and designs ranged from 8.8% to 44% for asthma,22 suggesting that second-hand smoke exposure may contribute to a considerable fraction of asthma cases in populations in other parts of the World.
Previous studies examining second-hand smoke exposure also reported susceptibility to COPD,1,11,23,24 supporting the observations in the current study. A Chinese study of 6,497 adults found an increased odds ratio for spirometry-defined COPD of 1.48 in those individuals who had been exposed to second-hand smoking at home and work for 40 hours a week or more for more than 5 years,1 and two meta-analyses have found elevated risk estimates for COPD of 1.20 and 1.66 among non-smokers who had been exposed to second-hand smoking.23,24 We found an elevated odds ratio for COPD of 1.24 in individuals exposed to lifelong second-hand smoking in the general population, present irrespective of adjustments for age, sex, and smoking status. In addition, previous studies have also reported reduced lung function in individuals exposed to second-hand smoking.19,20 The 4% lower value of FEV1% predicted in individuals who had been exposed to lifelong second-hand smoking in the current study corresponded to reductions of 102 mL and 118 mL in FEV1 in women and men, respectively. These reductions may not be trivial as they are comparable in magnitude to the minimally clinically important difference of 100 mL proposed for through FEV1 in clinical trials.25 If our results show the true magnitude of the effect of second-hand smoke exposure on COPD in the general population, it can be estimated as a population attributable fraction that lifelong second-hand smoking may account for up to 2.9% of COPD in the study sample, which compares with values ranging from 4% to 27% in studies using other study populations and designs.22
In our study second-hand smoke exposure was more common in childhood and less common in adulthood, which accords well with the high frequency of Danish people who previously smoked26 and with the current smoking ban instigated in 2007, leading to more smoke-free environments and an increased awareness of the harmful effects of second-hand smoke exposure at home and at work. Daily exposure to second-hand smoking has decreased in the Danish population from 73% in nonsmokers in 198727 to 24% in nonsmokers in the present study. A recent Canadian study showed that the most important contributor to elevated cotinine in non-smokers who had reported second-hand smoke exposure was “at home” exposure, and that cotinine levels were especially high for those individuals who were living in apartments compared to those living in single-detached homes.28 In the current study the reported second-hand smoke exposures probably more likely reflect “at home” exposure than exposure outside home since childhood exposure was defined as parental smoking at home and/or maternal smoking, and because current adulthood exposure outside the home has been considerably reduced after the current smoking ban was instigated in 2007. Information regarding people’s homes in the current study are unfortunately not available, but in Næstved municipality about 11,000 (28%) out of the 39,398 established homes are apartments according to Statistics Denmark.
The strengths of our study include a randomly chosen sample of an ethnically homogenous population, and blinding of investigators to risk factor status and clinical outcomes investigated. A potential limitation of our study is that the second-hand smoke exposures were by self-report. However, because sensitivity analyses stratified for smoking habits, sex, and airway obstruction showed almost similar results, and since we observed an independent dose–response relationship, we do not think that potential recall bias substantially influenced the results. The definition of childhood second-hand smoke exposure did not include information on the number of smokers in the household, years through age 20 living with smokers, and amount of exposure to passive smoking. Thus, there might be subgroups with high childhood exposure and even higher increased risk of some of the outcomes examined. We used prebronchodilator FEV1/FVC<0.7 instead of postbronchodilator spirometry for defining COPD, but excluded asthmatics, as in our previous study.29 Because the previous study found similar results for pre- and postbronchodilator COPD and since using a more stringent COPD definition in the current study showed similar results to those presented (Supplementary Figure 1), we do not think that possible misclassification of COPD considerably affected our results. However, if misclassification of COPD exists this may have pulled the results for COPD away from the null hypothesis, increasing the risk of a false positive finding. Another potential limitation is that some of the individuals suffering from pulmonary symptoms and disease may not have attended the physical examination and participated in the study. This could theoretically tend to bias the results toward the null hypothesis and lead us to underestimate the associations observed in the cohort. Finally, we used a sample of the Danish population, and generalizability of our data to other populations may potentially be constrained.
Conclusions
The results show a dose–response relation between second-hand smoke exposure and reduced lung function, and increased risks of dyspnoea, wheezing, cough, and asthma in the general population. Individuals who had been exposed lifelong to second-hand smoking had 1.6–2.1-fold increased risk of respiratory symptoms, 3–4% reductions of FEV1% predicted and FVC% predicted, a 1.4-fold increased risk of asthma, and a 1.2-fold increased risk of COPD in the general population.
Abbreviations
CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in first second; FVC, forced vital capacity.
Data Sharing Statement
Data are available upon reasonable request. Summarized data and scripts are available according to Danish law.
Ethics Approval and Informed Consent
The study was approved by the institutional review board at Zealand University Hospital (Dept of Production, Forskning og Innovation, REG-077-2018) and the local ethical committee of Region Zealand (SJ-113, SJ-114) and was conducted according to the Declaration of Helsinki. All participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Region Zealand Research Foundation, Novo Nordisk Foundation and Alpha-1 Foundation. The sponsors of the study are public or non-profit organizations and support science in general. They had no role in gathering, analysing, or interpreting the data and could neither approve nor disapprove the submitted manuscript.
Disclosure
None of the authors have any competing interests to declare.
References
1. Yin P, Jiang C, Cheng K, et al. Passive smoking exposure and risk of COPD among adults in China: the Guangzhou Biobank Cohort Study. Lancet. 2007;370:751–757. doi:10.1016/S0140-6736(07)61378-6
2. Skorge TD, Eagan TML, Eide GE, et al. Exposure to environmental tobacco smoke in a general population. Respir Med. 2007;101:277–285. doi:10.1016/j.rmed.2006.05.010
3. Brownson RC, Eriksen MP, Davis RM, et al. Environmental tobacco smoke: health effects and policies to reduce exposure. Annu Rev Public Health. 1997;18:163–185. doi:10.1146/annurev.publhealth.18.1.163
4. Hagstad S, Bjerg A, Ekerljung L, et al. Passive smoking exposure is associated with increased risk of COPD in never smokers. Chest. 2014;145:1298–1304. doi:10.1378/chest.13-1349
5. Skorge TD, Eagan TML, Eide GE, et al. The adult incidence of asthma and respiratory symptoms by passive smoking in utero or in childhood. Am J Respir Crit Care Med. 2005;172:61–66. doi:10.1164/rccm.200409-1158OC
6. Vardavas CI, Hohmann C, Patelarou E, et al. The independent role of prenatal and postnatal exposure to active and passive smoking on the development of early wheeze in children. Eur Respir J. 2016;48:115–124. doi:10.1183/13993003.01016-2015
7. Kostikas K, Minas M, Nikolaou E, et al. Secondhand smoke exposure induces acutely airway acidification and oxidative stress. Respir Med. 2013;107:172–179. doi:10.1016/j.rmed.2012.10.017
8. Vanker A, Gie RP, Zar HJ. The association between environmental tobacco smoke exposure and childhood respiratory disease: a review. Expert Rev Respir Med. 2017;11:661–673. doi:10.1080/17476348.2017.1338949
9. Guerra S, Stern DA, Zhou M, et al. Combined effects of parental and active smoking on early lung function deficits: a prospective study from birth to age 26 years. Thorax. 2013;68:1021–1028. doi:10.1136/thoraxjnl-2013-203538
10. Behrooz L, Balekian DS, Faridi MK, et al. Prenatal and postnatal tobacco smoke exposure and risk of severe bronchiolitis during infancy. Respir Med. 2018;140:21–26. doi:10.1016/j.rmed.2018.05.013
11. Johannessen A, Bakke PS, Hardie JA, et al. Association of exposure to environmental tobacco smoke in childhood with chronic obstructive pulmonary disease and respiratory symptoms in adults. Respirology. 2012;17:499–505. doi:10.1111/j.1440-1843.2012.02129.x
12. Hersoug LG, Husemoen LLN, Sigsgaard T, et al. Indoor exposure to environmental cigarette smoke, but not other inhaled particulates associates with respiratory symptoms and diminished lung function in adults. Respirology. 2010;15:993–1000. doi:10.1111/j.1440-1843.2010.01758.x
13. Jordan RE, Cheng KK, Miller MR, et al. Passive smoking and chronic obstructive pulmonary disease: cross-sectional analysis of data from the Health Survey for England. BMJ Open. 2011;1:1–9. doi:10.1136/bmjopen-2011-000153
14. Bergholdt HKM, Bathum L, Kvetny J, et al. Study design, participation and characteristics of the Danish general suburban population study. Dan Med J. 2013;60:1–7.
15. Juul K, Tybjærg-Hansen A, Mortensen J, et al. Factor V Leiden homozygosity, dyspnea, and reduced pulmonary function. Arch Intern Med. 2005;165:2032–2036. doi:10.1001/archinte.165.17.2032
16. Løkke A, Marott JL, Mortensen J, et al. New Danish reference values for spirometry. Clin Respir J. 2013;7:153–167. doi:10.1111/j.1752-699X.2012.00297.x
17. Coogan PF, Castro-Webb N, Yu J, et al. Active and passive smoking and the incidence of asthma in the Black Women’s Health Study. Am J Respir Crit Care Med. 2015;191:168–176. doi:10.1164/rccm.201406-1108OC
18. Kim SY, Sim S, Choi HG. Active and passive smoking impacts on asthma with quantitative and temporal relations: a Korean Community Health Survey. Sci Rep. 2017;7:1–8.3.
19. Flexeder C, Zock JP, Jarvis D, et al. Second-hand smoke exposure in adulthood and lower respiratory health during 20 year follow up in the European Community Respiratory Health Survey. Respir Res. 2019;20:33. doi:10.1186/s12931-019-0996-z
20. Dai X, Bui DS, Perret JL, et al. Exposure to household air pollution over 10 years is related to asthma and lung function decline. Eur Respir J. 2021;57:2000602. doi:10.1183/13993003.00602-2020
21. Wang J, Janson C, Jogi R, et al. A prospective study on the role of smoking, environmental tobacco smoke, indoor painting and living in old or new buildings on asthma, rhinitis and respiratory symptoms. Environ Res. 2021;192:110269. doi:10.1016/j.envres.2020.110269
22. Carreras G, Lugo A, Gallus S, et al. Burden of disease attributable to second-hand smoke exposure: a systematic review. Prev Med (Baltim). 2019;129:105833. doi:10.1016/j.ypmed.2019.105833
23. Fischer F, Kraemer A. Meta-analysis of the association between second-hand smoke exposure and ischaemic heart diseases, COPD and stroke environmental health. BMC Public Health. 2015;15:1202. doi:10.1186/s12889-015-2489-4
24. Lee PN, Forey BA, Coombs KJ, et al. Epidemiological evidence relating environmental smoke to COPD in lifelong non-smokers: a systematic review. F1000Research. 2018;7:146. doi:10.12688/f1000research.13887.1
25. Jones PW, Beeh KM, Chapman KR, et al. Minimal clinically important differences in pharmacological trials. Am J Respir Crit Care Med. 2014;189:250–255. doi:10.1164/rccm.201310-1863PP
26. Dahl M, Nordestgaard BG, Lange P, et al. Molecular diagnosis of intermediate and severe α1-antitrypsin deficiency: MZ individuals with chronic obstructive pulmonary disease may have lower lung function than MM individuals. Clin Chem. 2001;47:56–62. doi:10.1093/clinchem/47.1.56
27. Kristensen TS, Møller L, Holstein BE. [Occurrence of passive smoking in Denmark]. Ugeskr Laeger. 1990;152:2498–2501. Danish.
28. Levesque J, Mischki T. Exposure to tobacco smoke among Canadian nonsmokers based on questionnaire and biomonitoring data. Health Rep. 2021;32:16–26.
29. Landt E, Colak Y, Lange P, Laursen LC, Nordestgaard BG, Dahl M. Chronic cough in individuals with COPD. A population-based cohort study. Chest. 2020;157:1446–1454. doi:10.1016/j.chest.2019.12.038
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.