Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Second-Hand Smoke Exposure Among Coronary Heart Disease Patients
Authors Abu-Baker NN ![]() , AL-Jarrah EA, Suliman M
, AL-Jarrah EA, Suliman M
Received 17 November 2019
Accepted for publication 10 January 2020
Published 31 January 2020 Volume 2020:13 Pages 109—116
DOI https://doi.org/10.2147/JMDH.S238984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nesrin N Abu-Baker,1 Elham A AL-Jarrah,1 Mohammad Suliman2
1Faculty of Nursing, Community and Mental Health Nursing Department, Jordan University of Science & Technology, Irbid, Jordan; 2Faculty of Nursing, Community and Mental Health Nursing, Al-alBayt University, Mafraq, Jordan
Correspondence: Nesrin N Abu-Baker
School of Nursing, Community and Mental Health Nursing Department, Jordan University of Science & Technology, P.O Box 3030, Irbid 22110, Jordan
Tel +962 2 7201000 Ext. 23620
Fax +962 2 7201065
Email [email protected]
Purpose: The objectives of this study were to assess second-hand smoke (SHS) exposure among coronary heart disease (CHD) patients at home, in transportation, workplace, public and social places; to examine the demographic factors that predict SHS exposure; and to investigate the relationship between SHS exposure and CHD complications, age at the time of diagnosis, and number of admissions in the last year.
Patients and Methods: A descriptive cross-sectional design was used with a convenient sample of 400 CHD patients from three hospitals in Jordan. A modified version of the Smoking Scale for Adults (SS-A) was used.
Results: The percentage of SHS exposure was 64% in public places, 51.5% in social places, 48.5% in the household, 31% in transportation, while it was only 14.8% in the workplace. In addition, being male, employed, having a younger age and lower education significantly predicted higher exposure to SHS. Exposure to SHS was positively associated with CHD complications and the number of admissions, while it was negatively associated with the age at diagnosis with CHD.
Conclusion: Collaboration is needed among all health care sectors to adopt educational strategies about SHS exposure and to activate policies to prohibit smoking in public places.
Keywords: exposure, second-hand smoke, coronary heart disease, patients, Jordan
Introduction
Worldwide, smoking is considered the single largest preventable cause of death and disease. In 2015, the World Health Organization (WHO) estimated that over 1.1 billion people were smokers. Although the smoking number is decreasing worldwide in many countries, the prevalence of tobacco smoking appears to be increasing in the Eastern Mediterranean and the African Regions.1 As a result, more than a third of all people are exposing regularly to the harmful effects of smoke. Around 600,000 deaths are related to this exposure per year. This risk factor is prevalent in nearly every region of the world.2 Second-hand smoking (SHS) is defined as the exposure to a mixture of exhaled mainstream smoke and sidestream smoke from the lighted end of a cigarette, pipe, or cigar, or tobacco burning in a hookah.3
Coronary Heart disease (CHD) is the number one cause of death globally, more people die yearly from CHD than from any other cause. It is estimated that 17.9 million people died from cardiovascular diseases in 2016, they represent 31% of all global deaths. Of these deaths, 85% are attributable to CHD and stroke. Furthermore, over three-quarters of CHD deaths take place in low- and middle-income countries.4 Coronary heart disease develops when a waxy substance called plaque builds up inside the coronary arteries, which is called atherosclerosis. Over many years, the plaque leads to narrowing or clot formation, which can cause blocking of the blood flow to the coronary artery.5 Most cardiovascular diseases including CHD could be prevented by using population-wide strategies in adopting healthy lifestyles, such as quitting smoking, healthy diet, and increasing physical activity.4
Second-hand smoke exposure, which consists of the home, workplace, public places, and transportation, is considered highly significant because people spend 80–90% of their time in these places.6 The extent of exposure to SHS is varied, most of the studies among CHD patients focused on exposure at home and in the workplace because people usually spend more time presenting in these two places. For instance, exposure to SHS among patients who are diagnosed with CHD was conducted in 22 European regions for 8729 participants. The study revealed that 10.3% of the participants were exposed to SHS at home, 7.2% at work, and 13.8% at other locations.7 Another study assessed SHS exposure among 214 hospitalized CHD patients in the USA, Boston. The study revealed that the exposure between 30 and seven days before admission was 12.6% and 7.9% at home, 15.9% and 5.6% inside the car, and 7.1% and 7.4% at work, respectively.8
Many demographic and personal factors have a relationship with exposure to SHS. This relationship was evidenced by many studies. For example, a study was conducted in Bangladesh among 2813 nonsmoker adults. The percentage of exposure to SHS in the household was 43%. Moreover, the main predictors of SHS exposure were: being female, being aged 15–24, having lower education, and lower monthly income (p < 0.05).9 In addition, a study was conducted in the USA among 5032 subclinical cardiovascular disease patients. The study revealed that participants with higher SHS exposure were more likely to have lower income and education.10
Exposure to SHS has a negative impact on the function of the heart. It contributes to the initiation of cardiovascular diseases (CVDs), as well as the significant progression of cardiovascular outcomes.11 For example, a study in Germany estimated that the population prevalence of Ischemic Heart disease in 2040 will be decreased by 50%, if the exposure to SHS eradicates.12 Furthermore, a study in the USA found that individuals who had a stroke have 50% greater odds of SHS exposure, and SHS is associated with a 2-fold increase in mortality rate after getting a stroke.13
In Jordan, the prevalence of smoking is considered high compared with international prevalence. 33.2% of Jordanians were considered as current smokers among the age of 15 years or more.14 High prevalence and lack of awareness about the SHS consequences are considered a challenge in Jordan. On other hand, among 11,885 Jordanian families, 61% have an active smoker at home according to the Department of Statistics Jordan, while the prevalence of exposure to SHS is 44% among non-smoker persons at home and 30% at work place.15
Worldwide, 93% of people are still living in countries not covered by 100% smoke-free public health regulations.2 The current policy in Jordan which prohibits smoking is activated in health care, government, and educational facilities. Also, smoking is prohibited in public transportation. Unfortunately, other places do not fully activate smoking bans, such as indoor offices and restaurants.7 There is a lack of studies about SHS exposure among CHD patients in Jordan.16 Nurses worldwide are in a vital position to address SHS exposure to reduce the impact of this exposure on the health of individuals and the community.
The objectives of this study are: (1) to assess SHS exposure among CHD patients at home, transportation, workplace, public and social places, in terms of the number of smoked cigarettes, the number of surrounding smokers daily, and the duration of exposure; (2) to examine the demographic factors that predict SHS exposure such as: age, gender, educational level, income, and occupation; (3) to investigate the relationship between SHS exposure and the following: CHD complications, age at the time of diagnosis, and number of admissions in the last year.
Materials and Methods
Design, Sample, and Setting
A descriptive cross-sectional design was used to assess the extent of exposure to SHS among Jordanian patients who were diagnosed with CHD.
The target population was all patients from both genders, who have been diagnosed with CHD and attending medical and cardiac clinics in Jordan. The accessible population was all patients who have been diagnosed with CHD and attending cardiac clinics in the three selected hospitals. The inclusion criteria were adult patients aged ≥ 18, who were non-smokers for at least two years,17 and diagnosed with CHD by cardiac catheterization from the medical records. The sample size determination was based on G-power for multiple regression analysis including six predictors (medium effect size= 0.5, alpha= 0.05). Thus, 393 subjects were needed but the sample was enlarged to avoid loss of data from participants’ attrition.
The number of patients who met the inclusion criteria and were approached to participate was 440 patients, among those 40 patients refused to participate in the study (response rate = 91%). Thus, a convenient sample of 400 patients who were diagnosed with CHD was recruited from these hospitals. The sample was divided into three proportions according to the number of patients who were attending cardiac clinics. It was 200 patients from a major hospital in the capital city of Amman. In addition, 200 patients from two selected hospitals in Irbid city in the North part of Jordan (100 patients from each hospital).
Measurements
A structured questionnaire was used, and it consists of three main sections; demographic data, medical history, and exposure to SHS in the five settings. A modified version of the Second-Hand Smoking questionnaire for adults (SS-A) was adopted after taking the author`s permission.18 The SS-A questionnaire was valid, as there was a significant agreement with the nicotine measurement (z = 2.961, p = 0.003). It was also reliable as the scores of the two forms of the instrument were highly correlated (p< 0.001) and there were no statistically significant differences between them (z = -1.88, p = 0.06).18 In the current study, a minor modification of the original questionnaire, translation to Arabic, and back translation to English were done to achieve study purposes.
The first section about demographic data consists of six items: age, gender, marital status, educational level, occupation, and total household income per month. The second section of the questionnaire was about medical history related to CHD. This section of the questionnaire was also verified by the medical files. It included the medical history of other diseases, and CHD diagnosis confirmation by cardiac catheterization result, duration of being diagnosed with coronary artery disease, and the number of admissions in the last year.
The third section of the questionnaire was about exposure to SHS in the five settings, and it consists of four parts. The first part was measuring daily exposure to SHS at home, and it consists of six items. The second part was measuring weekly exposure to SHS in the public and social places (public areas and friend’s or relative’s houses), and it consists of eleven items. The third part was measuring weekly exposure to SHS in transportation, and it consists of five items. The fourth part was measuring daily exposure to SHS in the workplace, and it consists of seven items. The items in each set included: If smoking was allowed in this setting, with a yes =1 or no = 2 answer. In addition the number of surrounding smokers, the average number of cigarettes smoked by them, and the average time spent with these smokers (Appendix 1).
Data Collection Procedure
The recruitment process of the sample took around two months, from October 2017 to December 2017, and data collection from the three hospitals was conducted through recurrent visits by the researcher to each hospital two to three times per week. Through a structured face to face interview, an explanation of the structured questionnaire was offered to ensure understanding of all items, and the researcher asked all participants the same questions, in the same manner, to avoid missing data and to ensure the comfort of the participants. In addition, filling out the questionnaire was done during the structured interview in a private room of the cardiac clinics for each hospital. The second source of data was the medical electronic and paper files for each patient. Data was obtained from any patient who met the inclusion criteria, agreed to participate, and was available at the time of data collection.
Ethical Consideration
Approval from the Institutional Review Board (IRB) at Jordan University of Science and Technology was obtained. This study was also conducted in accordance with the Declaration of Helsinki. Formal approval was also obtained from the directors of the three hospitals where the study was conducted. In addition, the cover page of the questionnaire consists of a code of ethics. The researcher explained to each participant the main objectives of the study, permission from patients and the medical team was obtained for data collection from the participant`s medical files. Anonymity, confidentiality, voluntary participation, and the right to withdraw at any time were explained. Informed consent was signed by each participant in the study. Agreement of the patients and the medical team was obtained to access information from the medical files. Furthermore, each questionnaire was coded by a different number, and the draft which includes the participant`s name was kept with the researcher in a closed envelope until the analysis process was completed.
Data Analysis Procedures
Data analysis was performed using the Statistical Package for Social Sciences (SPSS 20). To describe all variables in the study, descriptive statistics were used and it includes means, standard deviation, frequencies, and percentage. Inferential statistics were used to describe the correlation between continuous variables. The relationships between variables in the study were described using regression analysis.
Results
Sample Description
The entire participants’ age ranged from 29 to 80 years old with a mean age of 61.1 years (SD= 9.34). Moreover, 67% of the participants were males, 37.8% were diagnosed with hypertension and diabetes mellitus. The age of the participants at diagnosis with CHD ranged from 22 to 72 years old with a mean age of 54.9 (SD= 8.2) (Table 1).
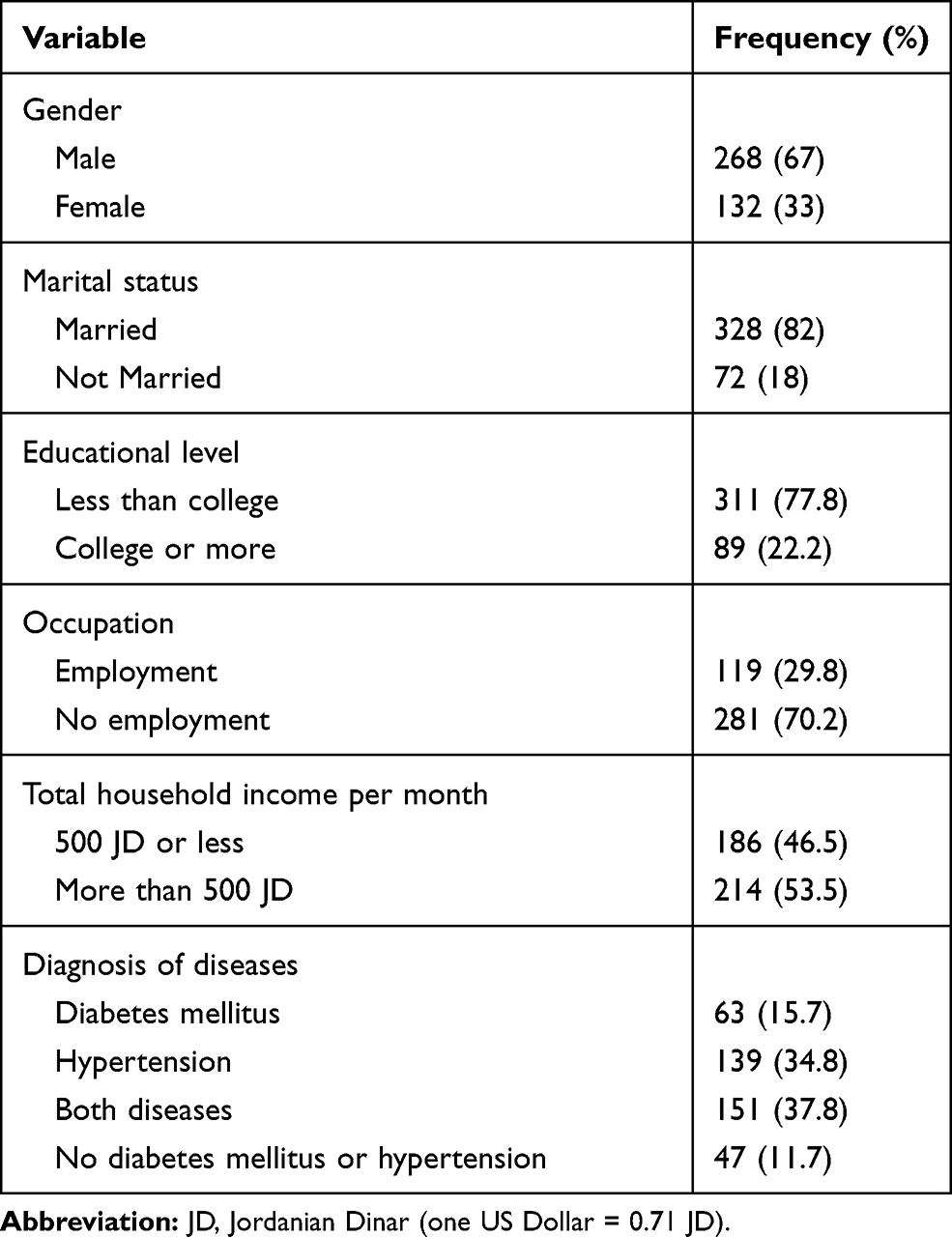 |
Table 1 Demographic Characteristics of Study Sample (n=400) |
Second-Hand Smoke Exposure at Home, Transportation, Workplace, Public and Social Places
Regarding the five settings, the highest exposure to SHS was in the public and social areas [in public areas 64% (n = 256) and friend`s or relative`s house with 51.5% (n = 206)], followed by household 48.5% (n = 194), transportation 31% (n = 124), while the lowest exposure to SHS was in the workplace with 14.8% (n = 59). The extent of SHS exposure was measured by three components: the number of surrounding smokers, the number of cigarettes, and the number of hours of SHS exposure. Means and standard deviations of each component are presented in Table 2.
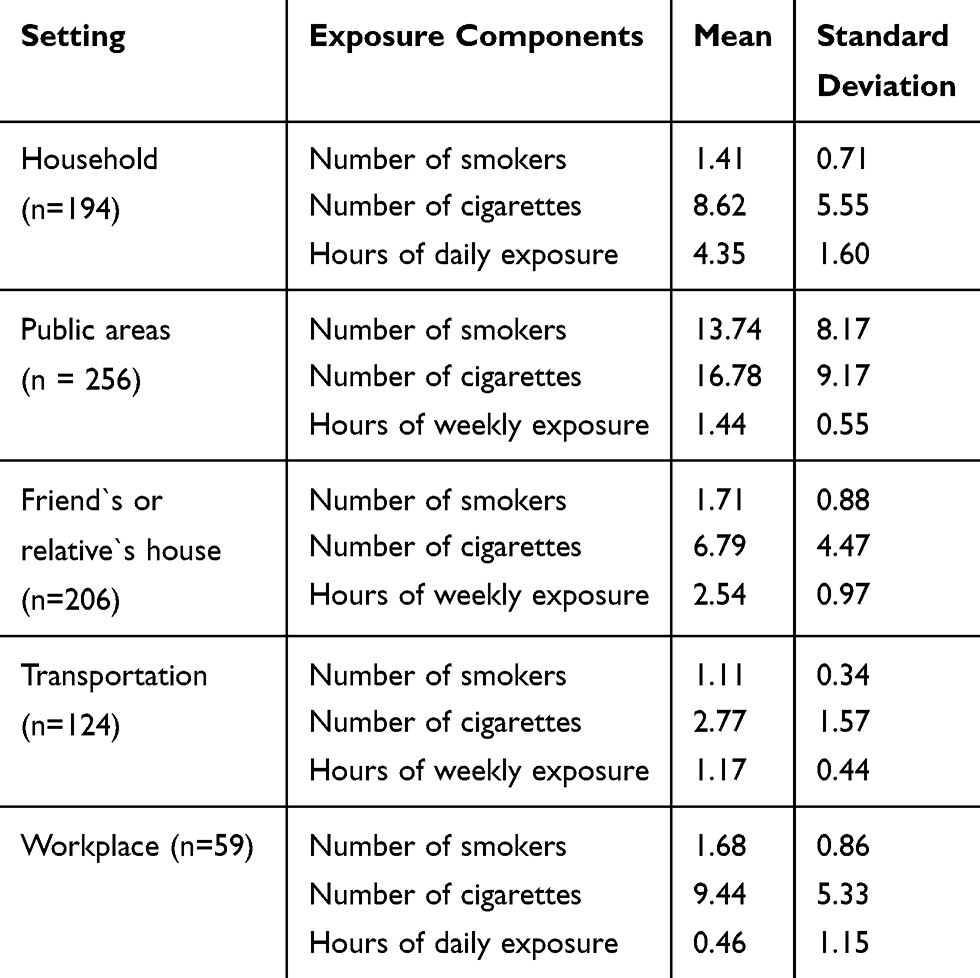 |
Table 2 The Extent of Exposure to SHS in the Five Settings (n=400) |
Participants’ Demographical Factors and Second-Hand Smoke Exposure
The dependent variable, which was exposure to SHS consists of three components (the number of surrounding smokers, the number of smoked cigarettes, and hours of exposure). Participants” demographic consists of independent variables (age, gender, educational level, income, and occupation).
Regarding the number of surrounding smokers and demographic and personal variables of the participants, a significant regression equation was found (R2 = 0.351, F (5, 394) = 44.099, p = 0.000). The model as a whole explained 35% of the variance in exposure to SHS from the number of surrounding smokers. The only significant predictor of the model was gender (p <0.05). Being male significantly predicted higher exposure to SHS (Beta = −0.548, p = 0.000) (Table 3).
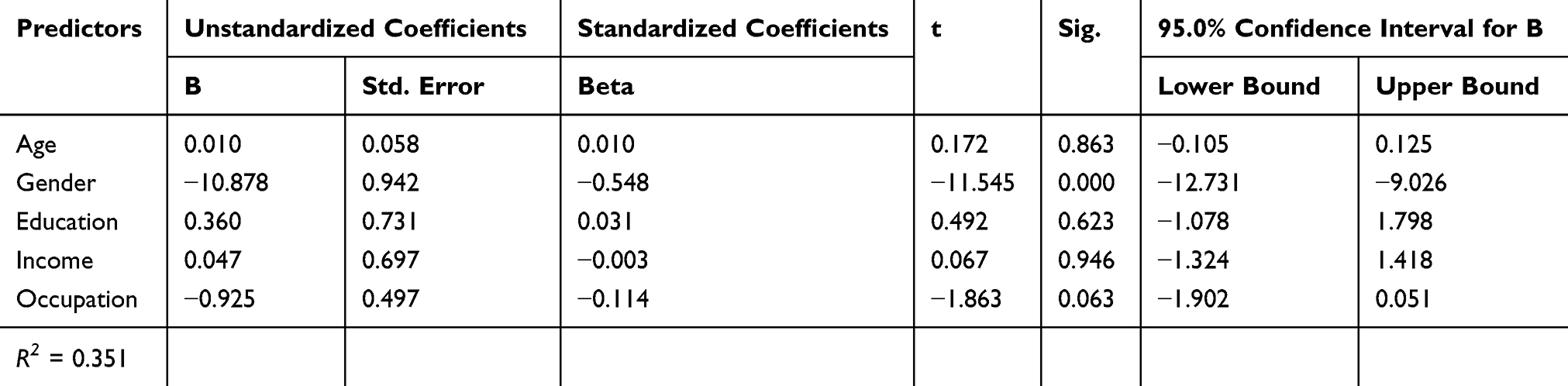 |
Table 3 Multiple Linear Regression Analysis of Demographic Variables and the Number of Surrounding Smokers (n=400) |
On the other hand, regarding the number of smoked cigarettes and demographic and personal variables of the participants, a significant regression equation was found (R2= 0.192, F (5, 394) = 18.739, p= 0.000). The model as a whole explained 19% of the variance in exposure to SHS from the number of smoked cigarettes. The significant predictors of the model were age and gender (p <0.05). Having younger age and being male significantly predicted higher exposure to SHS (Beta = −0.135, p = 0.040; Beta = −0.352, p = 0.000) (Table 4).
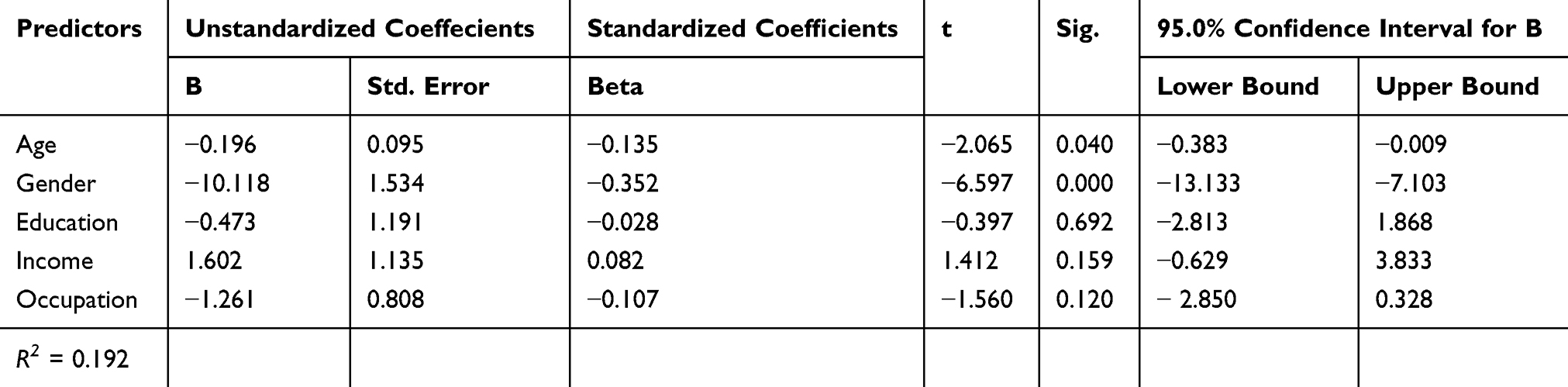 |
Table 4 Multiple Linear Regression Analysis of Demographic Variables and the Number of Smoked Cigarettes (n=400) |
Finally, regarding the total hours of exposure to SHS and demographic and personal variables of the participants, a significant regression equation was found (R2 = 0.127, F (5, 394) = 11.478, p =0.000). The model as a whole explained 13% of the variance in exposure to SHS from the total hours of exposure. The significant predictors of the model were age, level of education and occupation (p <0.05). being younger age, lower education, and being employed significantly predicted higher exposure to SHS (Beta = −0.160, p =0.019; Beta = −0.194, p = 0.008; Beta = −0.287, p = 0.000 respectively) (Table 5).
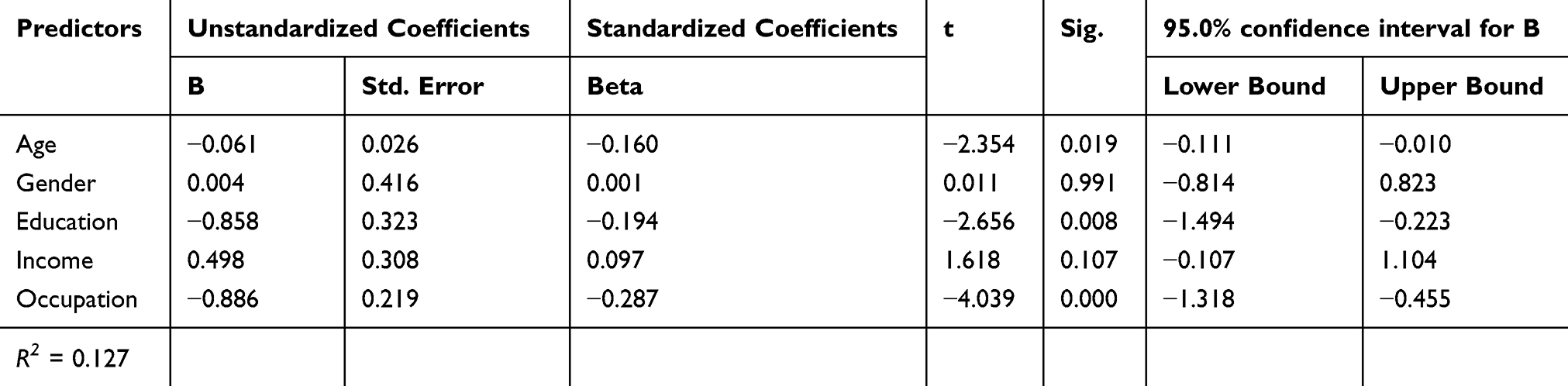 |
Table 5 Multiple Linear Regression Analysis of Demographic Variables and the Total Hours of Exposure (n=400) |
The Association Between Exposure to SHS and CHD Complications, Age at Diagnosis, and Number of Admissions
In terms of the association between CHD complications and the three components of exposure to SHS; the results showed a positive significant correlation between CHD complications and each of the following: the number of smoked cigarettes (r = 0.102, p = 0.041), and hours of exposure (r = 0.191, p = 0.000) where n = 400. It means that as the exposure increased, CHD complications increased as well.
Concerning the correlation between the age at diagnosis with CHD and the three components of exposure to SHS; the results showed a negative significant correlation between the age at diagnosis and each of the following: the number of smoked cigarettes (r = −0.231, p = 0.000), the number of surrounding smokers (r = −0.102, p = 0.041), and hours of exposure (r = −0.230, p = 0.000) where n = 400. It means that as the exposure increased, the age of CHD diagnosis decreased.
Finally, the correlation between the number of admissions for CHD in the last year and the three components of exposure to SHS was also investigated. A positive significant correlation was found only between the number of admissions in the last year and the number of smoked cigarettes and (r = 0.111, p = 0.026, n = 400). It means that as the exposure increased, the number of CHD admissions also increased.
Discussion
The current study aimed to assess SHS exposure among CHD patients. The results showed that the highest exposure to SHS was in the public and social places (64% and 51.5%, respectively). This result could be explained by the fact that although there are national legislation and penalties that prohibit smoking in public places, it still not fully activated in public places. In addition, smoking at other’s homes and social events such as weddings and consolations is considered an acceptable habit according to our culture. Inconsistent study in Europe reported that exposure to SHS was only 13.8% in locations other than home and work.7 The reason behind this inconsistency could be explained by the cultural and belief differences. In addition, the presence of fully implemented smoke-free policies and smoking bans in developed countries could be another reason for that inconsistency.
On the other hand, the current study revealed that 48.5% of CHD patients reported SHS exposure in the household. This exposure is close to SHS exposure at home among the general population in Jordan (44%).15 This result could be explained by the social norms and culture as people are not used to prohibiting smoking at their homes, which needs to intensify multiple programs to resist this problem and raise the awareness in the Jordanian community. Comparable results were reported in previous studies. For example, a study in China consisting of 910 stroke patients revealed a home exposure of 44%.19 Moreover, An 11-year follow-up study in Norway consisted of 11,762 men and 13,206 women to estimate the risk factors of myocardial infarction. It revealed that 58% of men and 41% of women reported spending time in rooms filled with smokers.20
Furthermore, the current study revealed that 31% of CHD patients reported SHS exposure in transportation. This exposure is higher than the exposures of two previous studies conducted in the USA among CHD patients. They both reported 16% of transportation exposure.8,21 A reasonable explanation might be that Jordanian people are less committed to the prohibition of smoking in transportation vehicles. Besides, in the current study, the lowest exposure to SHS was in the workplace (15%). This exposure is less than SHS exposure at work (30%) among the general population in Jordan.15 The reason behind this result could be related to the recent enforcement of the legislation more effectively in the workplace. While this exposure is still higher than the exposure reported in two previous studies conducted in Europe and the USA, where exposure in the workplace was only 7%.7,8
This study aimed also to examine the demographic factors that predict SHS exposure. The result showed that being male, employed, having a younger age, and lower education were significant predictors of higher exposure to SHS. These results are in concordance with the previous studies. For instance, a study in Bangladesh found that people with younger age and lower education are more likely to become exposed to SHS.9 Furthermore, a study was conducted in Germany showed that exposure to SHS was associated with younger age, being male, and being employed.22 Some explanations of the results of the current study could be that the awareness of the harmful effects of exposure to SHS differs according to the different age groups. Moreover, according to the culture and traditions in Jordan; the number of male smokers especially in public places is higher than female smokers.
Finally, this study aimed to investigate the relationship between SHS exposure and CHD complications, age at the time of diagnosis, and number of admissions in the last year. The result showed that exposure to SHS was positively correlated to CHD complications and the number of admissions, while it was negatively correlated to the age at diagnosis with CHD (p< 0.05). A previous study reported that SHS was associated with a 2-fold increase in mortality after stroke.13 Moreover, a study in the USA reported that exposure to SHS was independently associated with an increased risk of stroke by 30% (95% CI= 2%-67%).23 Correspondingly, the American Heart Association (AHA, 2019) recommended the avoidance of SHS exposure to minimize the risk of cardiovascular disease events. The AHA stated that there is no safe lower limit of SHS exposure, even a brief exposure to SHS can activate a myocardial infarction.24 In congruence with the previous results and recommendations, the current study confirms that exposure to SHS leads to an occurrence of CHD at a younger age, as well as increases the possibility of developing more CHD complications and hospital admissions.
Limitations of the Study
The current study should be interpreted in light of some limitations. The generalizability of the finding of the current study is limited due to the convenient sampling approach. The current study used the retrospective approach, which may lead to inaccurate recall, and subject’s biases. In addition, the current study used a self-report questionnaire, which used closed-ended questions. This type of question may reduce participants’ ability to fully express their experience with exposure to SHS, and enhance the self-report bias. Finally, the current study used a sample of CHD patients, and it did not compare their exposure with the exposure of a sample from the general population.
Study Implications
Professional nurses could benefit from the findings of the current study. Nurses can increase the patient`s awareness of the harmful effects of exposure to SHS on their health. Increasing awareness of the community will encourage them to prohibit smoking in their houses and to avoid it in other places. Moreover, one of the nursing roles is to implement a recurrent assessment of exposure to SHS in each visit. The AHA (2019) also recommended that clinicians should advise patients to avoid SHS exposure in homes, vehicles, public places, and workplaces.24 In light of the current study, it is essential to include SHS exposure in the nursing curriculum for university students, as guidelines for health promotion and primary prevention. Practical training should be provided too, to present a proper assessment, counseling, and health education. Also, the policymakers should activate community-based comprehensive policies, to prohibit exposure to SHS and to maintain a smoke-free environment. This could be achieved by applying smoking penalties in all public places, and continuous monitoring to ensure the implementation and compliance of smoking bans. A Literature review paper concluded that the toxic elements of SHS are responsible for significant cardiovascular morbidity and mortality. Consequently, the vital goal at a societal level must be zero SHS exposure through legislative efforts resulting in 100% smoke-free policies in workplaces and public spaces. Informed individuals and groups can further encourage these efforts in their own settings by eliminating all forms of SHS exposure.25
Recommendations for Future Research
Based on the current study, there are many recommendations for future studies. One of them is to use a prospective study to investigate the exposure of SHS among patients who are diagnosed with CHD and compare it with the exposure of the general population. This may be useful in giving a better view of the problem of SHS exposure. Further studies could be implemented using a random sample and a biometric measure to examine SHS exposure. Additional studies could be implemented on other vulnerable groups, who are affected by exposure to SHS, such as children and elderly people.
Conclusion
Based on the current study, exposure to SHS was relatively high among CHD patients in different settings. Many factors were related to SHS exposure among CHD patients such as age, gender, education, and occupation. Therefore, it is essential to focus on building strategies to educate the community about the harmful effects of exposure to SHS. Collaboration is needed among all health sectors to adopt educational strategies about SHS exposure and its consequences. Finally, it is also, important to assess exposure to SHS among CHD patients to enable counseling if needed.
Acknowledgment
This study was funded by the Deanship of Research in Jordan University of Science and Technology.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Health Observatory (GHO) data: prevalence of tobacco smoking; 2018. Available from: https://www.who.int/gho/tobacco/use/en/.
2. World Health Organization. Global Health Observatory (GHO) data: second-hand smoker; 2018. Available from: https://www.who.int/gho/phe/secondhand_smoke/en/.
3. American Cancer Society. Health risks of second-hand smoke; 2015. Available from: https://www.cancer.org/cancer/cancer-causes/tobacco-andcancer/secondhand-smoke.html.
4. World Health Organization. Cardiovascular diseases (CVDs); 2017. Available from: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
5. National Institute of Health. Coronary heart disease; 2018. Available from: https://www.nhlbi.nih.gov/health-topics/coronary-heart-disease.
6. Bentayeb M, Simoni M, Norback D, et al. Indoor air pollution and respiratory health in the elderly. J Environ Sci Health A. 2013;48(14):1783–1789. doi:10.1080/10934529.2013.826052
7. Prugger C, Wellmann J, Heidrich J, et al. Passive smoking and smoking cessation among patients with coronary heart disease across Europe: results from the EUROASPIRE III survey. Eur Heart J. 2013;35(9):590–598. doi:10.1093/eurheartj/eht538
8. Japuntich SJ, Eilers MA, Shenhav S, et al. Secondhand tobacco smoke exposure among hospitalized nonsmokers with coronary heart disease. JAMA Intern Med. 2015;175(1):133–136. doi:10.1001/jamainternmed.2014.5476
9. Abdullah AS, Driezen P, Sansone G, et al. Correlates of exposure to secondhand smoke (SHS) at home among non-smoking adults in Bangladesh: findings from the ITC Bangladesh survey. BMC Pulm Med. 2014;14(1):117. doi:10.1186/1471-2466-14-117
10. Jones MR, Magid HS, Al‐Rifai M, et al. Secondhand smoke exposure and subclinical cardiovascular disease: the multi‐ethnic study of atherosclerosis. J Am Heart Assoc. 2016;5(12):e002965. doi:10.1161/JAHA.115.002965
11. Messner B, Bernhard D. Smoking and cardiovascular disease significance: mechanisms of endothelial dysfunction and early atherogenesis. Arterioscler Thromb Vasc Bio. 2014;34(3):509–515. doi:10.1161/ATVBAHA.113.300156
12. Fischer F, Kraemer A. Health impact assessment for second-hand smoke exposure in germany—quantifying estimates for ischemic heart diseases, COPD, and stroke. Int J Environ Res Public Health. 2016;13(2):198. doi:10.3390/ijerph13020198
13. Lin MP, Ovbiagele B, Markovic D, Towfighi A. Association of secondhand smoke with stroke outcomes. Stroke. 2016;47(11):2828–2835. doi:10.1161/STROKEAHA.116.014099
14. World Health Organization. WHO report on the global tobacco epidemic: Country profile, Jordan; 2015. Available from: http://www.who.int/tobacco/surveillance/policy/country_profile/jor.
15. Department of Statistics Jordan (DOS). Statistical yearbook; 2011. Available from: http://www.dos.gov.jo/dos_home_a/main/Analasis_Reports/Smoking_2010/Smoking_2010.pdf.
16. The Tobacco Atlas. Country: Jordan; 2017. Available from: https://tobaccoatlas.org/country/jordan/.
17. Mason K, Borman B. Burden of disease from second-hand smoke exposure in New Zealand. NZ Med J. 2016;129:1432.
18. Misailidi M, Tzatzarakis MN, Kavvalakis MP, Koutedakis Y, Tsatsakis AM, Flouris AD. Instruments to assess secondhand smoke exposure in large cohorts of never smokers: the smoke scales. PLoS One. 2014;9(1):e85809. doi:10.1371/journal.pone.0085809
19. He Y, Jiang B, Li LS, et al. Secondhand smoke exposure predicted COPD and other tobacco-related mortality in a 17-year cohort study in China. Chest. 2012;142(4):909–918. doi:10.1378/chest.11-2884
20. Iversen B, Jacobsen BK, Løchen ML. Active and passive smoking and the risk of myocardial infarction in 24,968 men and women during 11 year of follow-up: the Tromsø Study. Eur J Epidemiol. 2013;28(8):659–667. doi:10.1007/s10654-013-9785-z
21. Rigotti NA, Park ER, Streck J, et al. An intervention to address secondhand tobacco smoke exposure among nonsmokers hospitalized with coronary heart disease. Am J Cardiol. 2014;114(7):1040–1045. doi:10.1016/j.amjcard.2014.07.017
22. Peinemann F, Moebus S, Dragano N, et al. Secondhand smoke exposure and coronary artery calcification among nonsmoking participants of a population-based cohort. Environ Health Perspec. 2011;119(11):1556. doi:10.1289/ehp.1003347
23. Malek AM, Cushman M, Lackland DT, Howard G, McClure LA. Secondhand smoke exposure and stroke: the reasons for geographic and racial differences in stroke (REGARDS) study. Am J Prev Med. 2015;49(6):e89–e89. doi:10.1016/j.amepre.2015.04.014
24. Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease. J Am Coll Cardiol. 2019;17:26029.
25. DiGiacomo SI, Jazayeri MA, Barua RS, Ambrose JA. Environmental tobacco smoke and cardiovascular disease. Int J Environ Res Public Health. 2019;16(1):96. doi:10.3390/ijerph16010096
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.