")
Back to Journals » Clinical Ophthalmology » Volume 17
Seasonality of Tear Meniscus Volume and Dry Eye-Related Symptoms – A Cross-Sectional Retrospective Cohort Study
Received 26 October 2023
Accepted for publication 5 December 2023
Published 12 December 2023 Volume 2023:17 Pages 3809—3816
DOI https://doi.org/10.2147/OPTH.S442567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Masahiko Ayaki,1,2,* Kazuno Negishi1,*
1Department of Ophthalmology, Keio University School of Medicine, Tokyo, Japan; 2Otake Eye Clinic, Kanagawa, Japan
*These authors contributed equally to this work
Correspondence: Masahiko Ayaki, Email [email protected]
Purpose: We aimed to determine the seasonal variation in the tear meniscus level on strip meniscometry and its association with ocular parameters and symptoms. In Japan, there are four distinct seasons characterized by marked differences in temperature and humidity, which may contribute to an observed seasonality of ocular surface symptoms.
Methods: We conducted a cross-sectional study in two Japanese clinics and recruited first-visit patients for 3 years. Tear strip meniscometry, tear break-up time (BUT), Schirmer test, and corneal staining were examined, and major ocular symptoms (dryness, irritation, pain, fatigue, blurred vision, and photophobia) were determined through interviews.
Results: The 1196 participants had a mean age of 58.9± 15.2 years; 37.1% were of male sex. Strip meniscometry values and BUT revealed significant seasonality with one-way analysis of variance. The mean strip meniscometry value (mm) was 2.15± 2.59 in spring (p=0.025 vs winter), 2.37± 2.79 in summer (p< 0.001), 2.38± 2.80 in fall (p< 0.001), and 1.64± 2.29 in winter. Regression analysis indicated that strip meniscometry levels were correlated with BUT (p< 0.001), Schirmer test values (p< 0.001), corneal staining scores (p=0.022), and presence of dryness (p< 0.001).
Conclusion: Strip meniscometry values exhibited distinct seasonality, being lowest in winter when the ambient condition is dry and cool, and were correlated with BUT, Schirmer test values, corneal staining scores, and the presence of subjective dryness.
Keywords: dry eye, seasonality, strip meniscometry, Schirmer test, tear break-up time
Introduction
The Asia Dry Eye Society defines dry eye disease (DED) as
a multifactorial disease characterized by a persistently unstable and/or deficient tear film causing discomfort and/or visual impairment, accompanied by variable degrees of ocular surface epitheliopathy, inflammation, and neurosensory abnormalities.1
Accordingly, the diagnosis of DED rests on an unstable tear film and ocular discomfort. The evaluation of unstable tear film considers tear break-up time (BUT) as well as tear function tests, with the latter comprising a critical part of the clinical diagnosis and management of DED, especially in aqueous deficiency-type DED. A tear film-oriented diagnosis and treatment is recommended after BUT measurement and tear function tests, to classify the DED subtype for appropriate management.2,3
To measure aqueous availability at the lower meniscus, tear strip meniscometry was first proposed as an alternative to the Schirmer test in 2006.4 Strip meniscometry values correlate significantly with Schirmer test values, BUTs, corneal staining scores, and tear meniscus height measurements by anterior optical coherence tomography.5 Strip meniscometry is now used in clinical and experimental studies6–15 in both human and veterinary medicine.15 A strip is briefly applied to the lateral side of the lower lid tear meniscus and the length of the blue line indicates the tear meniscus value (Figure 1). The reproducibility and repeatability of the test have been proven,15 and the original cut-off value of 5 mm4,5 has been replaced with 2.5 mm.14 Strip meniscometry has been used up to seven times a day to assess diurnal fluctuations in tear volume, indicating sufficient accuracy and suitability for monitoring seasonal changes.12 The sensitivity and specificity of strip meniscometry combined with tear function and ocular surface tests were calculated in a previous study.5 The area under the curve (AUC) calculated by the receiver operating characteristics curve (ROC) technique was 0.79 (95% confidence interval 0.72–0.86), suggesting an acceptable sensitivity and specificity of strip meniscometry. When the cut-off value of the strip meniscometry result was set at 4 mm, the sensitivity and specificity of the strip meniscometry procedure were found to be 83.5% and 58.2%, respectively.
 |
Figure 1 Strip meniscometry. The strip is applied to the lateral side of the lower lid tear meniscus (top) and the length of the blue line indicates the tear meniscus volume (bottom). |
Tear meniscus level is closely associated with the pathology, signs, and symptoms of DED,10 and these signs and symptoms may worsen with different seasons.16–21 Ophthalmic practitioners often encounter patients complaining of dryness or other ocular surface symptoms in the drier seasons of winter and fall; however, little is known about which sign corresponds to which symptom in these seasons. Furthermore, the seasonality of tear meniscus level has not been determined.
Japan, the place of study, is characterized by four distinct seasons during which temperature and humidity vary markedly, and the seasonality of ocular surface symptoms can be observed every year. Summers are hot and humid, whereas winters are cold and dry. Between 1981 and 2010, the Tokyo area experienced average temperatures ranging from 5.2°C in winter to 25.0°C in summer and humidity between 52% in winter and 77% in summer.22 During examination, the temperature and humidity of the examination room were stably maintained between 25°C and 27°C and 30–40%, respectively. It could be postulated that tear meniscus volume may decrease in dry winters and increase in humid summers.
The aim of this study was to determine seasonal effects on the tear meniscus level measured by strip meniscometry. We analyzed the corneal findings, lacrimal function, and DED-related symptoms across several years. Finally, we attempted to explore any associations between strip meniscometry, DED symptoms, and other examination values, including BUT and corneal staining score.
Methods
Study Participants and Institutional Review Board Approval
This cross-sectional study was conducted at the Otake Eye Clinic (Kanagawa, Japan) and the Tsukuba Central Hospital (Ibaraki, Japan) near Tokyo in Japan. The study was performed in accordance with the Declaration of Helsinki, and approved by the institutional review boards and ethics committees of the Kanagawa Medical Association (approved 12 November 2018, approval number krec2059006), Keio University School of Medicine (approved 17 October 2019, approval number 20190131), and Tsukuba Central Hospital (approved 12 December 2014, permission number 141201). Participants were consecutively recruited on their first visit only from May 2018 to April 2021. The Ethics Committee of the Kanagawa Medical Association, Keio University School of Medicine, and Tsukuba Central Hospital waived the need for informed consent since the study was conducted in an opt-out fashion. The protocol was registered with the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (UMIN 000030325).
Inclusion and Exclusion Criteria
We included patients with best-corrected visual acuity above 20/30 on their first visit. We excluded patients who used eyedrops or contact lenses, as well as those with vitreoretinal disease, or acute ocular disease in the previous 2 weeks or any ocular surgery in the previous month.
Ophthalmological Examinations
We examined the ocular surface of each patient sequentially by strip meniscometry testing, BUT, corneal fluorescein staining, and Schirmer testing. BUT and corneal staining were assessed according to standard procedures.10,14 BUT was measured using a saline-soaked fluorescein filter paper strip (Ayumi Pharmaceutical, Tokyo, Japan) without excess saline applied to the lower lid margin, under a yellow light filter. The BUT was defined as the time interval between the third blink and the appearance of the first dark spot in the cornea, taking the mean of three measurements. A BUT of 5 seconds or less was considered a short BUT. Corneal staining was used to reveal corneal epitheliopathy.
Corneal staining scores were obtained by grading the stain intensity 1 minute after administering fluorescein dye in the eye. We applied the NEI/Industry Workshop classification system,23 with a grading scale of 0 to 2 for severity and area. All scores were obtained using the slit lamp’s cobalt blue illumination and a yellow barrier filter. The Schirmer test was performed without topical anesthesia. Strips of filter paper (Whatman no. 41; Showa Yakuhin Kako, Tokyo, Japan) were applied at the temporal lower conjunctival fornix for 5 minutes. The length of the wet area of the filter paper, in millimeters, was recorded. The strip meniscometry test was performed using single-use SMTube strips (Echo Electricity Co., Ltd, Fukushima, Japan) (Figure 1).10 The strip used for strip meniscometry is composed of polyethylene terephthalate. A urethane-based material of the same size, containing a central ditch of 0.40 mm in depth, is pasted on the strip. A nitrocellulose membrane filter paper strip with a pore size of 8 μm impregnated in natural blue dye is placed into the central ditch, and then the strip is applied for 5 seconds to the lateral side of the lower lid tear meniscus without touching the ocular surface.
Patient Interviews for DED Symptoms
We asked the patients about six common DED-related symptoms: dryness, irritation, pain, eye fatigue, blurred vision, and photophobia. All items were selected from the Dry Eye-Related Quality-of-Life Score questionnaire24 according to the most prevalent symptoms in the dry eye clinic in Keio University Hospital in 2014.
Statistical Analysis
Data are given as the mean ± standard deviation or as percentages where appropriate. We analyzed BUT, corneal staining score, Schirmer test, and strip meniscometry from the right eye only. We defined the four seasons as follows: March to May as spring, June to August as summer, September to November as autumn, and December to February as winter. The seasonal variations in symptoms and signs of DED were compared using one-way analysis of variance (ANOVA) and the Mann Whitney U-test. Regression analysis was performed to explore associations between examination values and DED signs and symptoms. All analyses were performed using StatFlex (Atech, Osaka, Japan), with p<0.05 indicating statistical significance.
Results
A total of 1196 study participants was enrolled, including 1196 (100%) tear strip meniscometry cases, 1181 (98.7%) BUT cases, 406 (33.9%) Schirmer test cases, and 1183 (98.9%) corneal staining cases. The mean age was 58.9±15.2 years (range 9–92 years), with 444 males (37.1%) in the cohort. According to the definition of the Asia Dry Eye Society,23 DED was diagnosed in 48.4% of participants in spring, 53.8% in summer, 50.4% in fall, and 46.6% in winter. The mean strip meniscometry value was 2.15±2.59 mm in spring (n=225; p=0.025 vs winter), 2.37±2.79 mm in summer (n=340; p<0.001), 2.38±2.80 mm in fall (n=365; p<0.001), and 1.64±2.29 mm in winter (n=266). The results of an ANOVA and multiple comparison test indicated that strip meniscometry values were significantly lower in winter compared with the other seasons (Table 1 and Figure 2). There was a weak seasonality in BUT (p=0.010), whereas there was no seasonality in the Schirmer test value or corneal staining score. Analysis of the contingency table indicated that none of the symptoms had seasonal variation: dryness (p=0.773), irritation (p=0.530), pain (p=0.718), fatigue (p=0.372), blurring (p=0.675), and photophobia (p=0.939) (Figure 3).
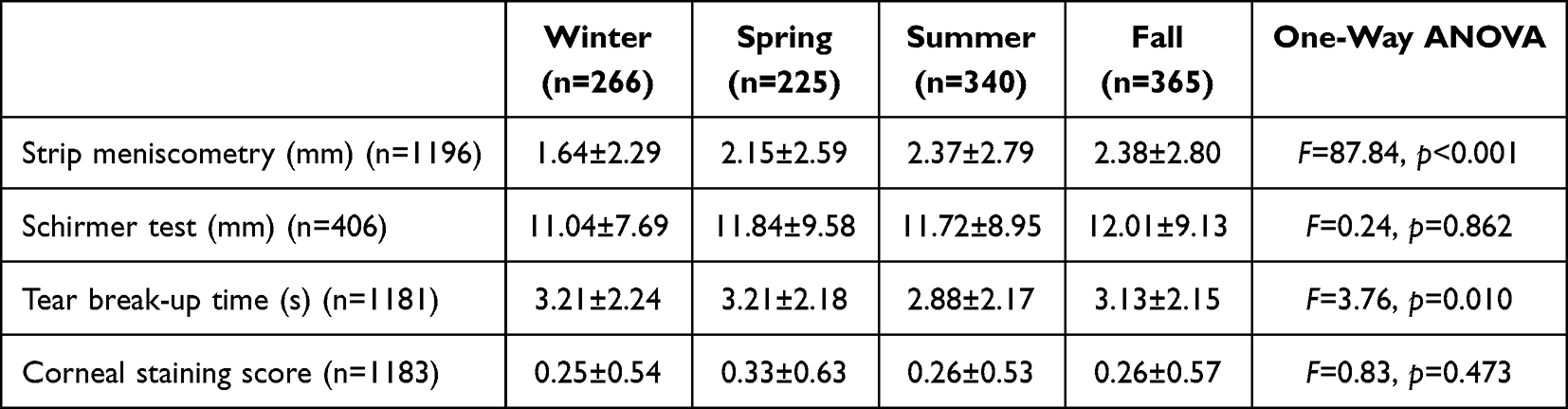 |
Table 1 Results of One-Way Analysis of Variance (ANOVA) for Seasonal Variation (n=1196) |
 |
Figure 2 Seasonal variation of ocular surface parameters. Corneal staining and tear strip meniscometry were worst in winter or spring, whereas Schirmer test and tear break-up time were worst in summer or fall. Abbreviations: BUT, tear break-up time; ST, Schirmer test value; SM, strip meniscometry value. |
 |
Figure 3 Seasonal variation of ocular symptoms. Contingency table analysis indicated that none of the symptoms showed seasonal variation. |
Regression analysis indicated that the strip meniscometry value was correlated with BUT (β=0.2432, p<0.001), Schirmer test value (β=0.198, p<0.001), corneal staining score (β=−0.0665, p=0.022), and dryness (β=−0.1492, p<0.001) (Table 2).
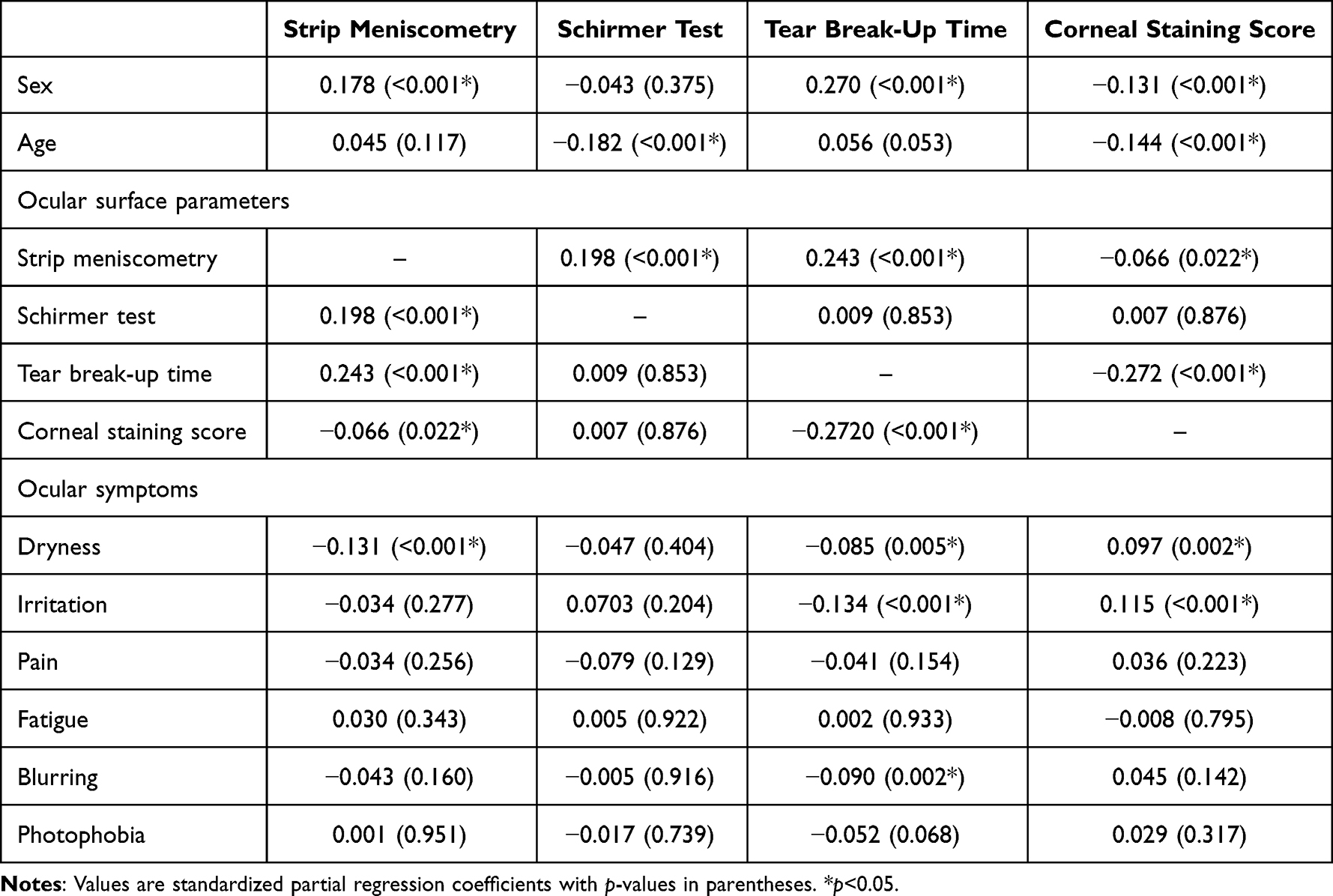 |
Table 2 Correlation Between Tear Function Tests and Ocular Surface Parameters and Symptoms |
Discussion
Strip meniscometry values showed seasonal variations, with the lowest being in winter. They were also associated with BUT and subjective dryness. A low strip meniscometry value could result from decreased tear secretion and increased evaporation. It is possible that the decrease in tear production may be attributable to sympathetic nervous system activation in winter. Hypertension investigators have described activation of the sympathetic nervous system as a potential mechanism and mediator of a seasonal blood pressure rise in winter,25–28 with an increase in urinary and plasma norepinephrine. Sano et al7 demonstrated that abdominal breathing increased the tear volume in healthy women, possibly owing to an activated parasympathetic nervous system. Taken together, tear secretion may decrease in winter, with a dominant sympathetic nervous system, and this hypothesis reasonably accounts for the current results. Dry weather further contributes to increased evaporation, leading to the low strip meniscometry values in winter.
A previous study suggested that tear function in DED patients measured with the Schirmer test was lowest in winter and highest in spring, in order to scavenge seasonal air pollen.16,18 DED patients may exhibit distinct seasonality in symptoms and signs, probably as a result of the vulnerability of the ocular surface, as well as systemic and neuropsychiatric factors.
Given that the majority of participants in the present study were from the general population without DED and did not use any eyedrops, the present results of ocular symptoms may be comparable with those of the non-DED group without notable seasonality from the previously mentioned study.16 There is a well-known discrepancy in signs and symptoms in DED, which is due to neuropathic pain and a complicated ocular surface environment.29–31 Nevertheless, strip meniscometry showed seasonality in this cohort, suggesting that strip meniscometry may be a sensitive indicator of tear volume that can be altered by seasonable tear production and evaporation. The Schirmer test results, however, showed no seasonality, and reflex secretion may be a potential confounder. We therefore suggest that strip meniscometry could be superior to Schirmer tests for evaluating lacrimal function with respect to patients’ symptoms.
Other investigations have indicated that seasonal changes in temperature, wind, and sunshine may all exacerbate DED.16–21 Eidet et al20 examined and interviewed 652 patients to determine a possible seasonality of signs and symptoms in DED, and found that neither DED severity level nor DED symptoms differed seasonally in Oslo, Norway. However, some parameters for DED showed seasonal variations (Schirmer test and tear meniscus height). Dermer et al18 reviewed ICD-9 codes for DED and routine medical examinations, and examined 365 patients in Miami, USA. They found that peak values for DED symptoms aligned with peak DED prevalence seen in a retrospective sample, occurring in spring and fall. A similar pattern was noted with DED signs. They concluded that both symptoms and signs of DED varied throughout the year and that symptoms were most severe in the peak allergy season and during weather fluctuations. Van Setten et al21 described seasonal and geographical variations in DED symptoms in five European countries. Their study suggested that environmental characteristics such as temperature and humidity, as well as wind, were the most commonly cited triggering factors, and the main seasons for DED complaints in Europe were winter and summer. Taking these results together, it is advisable that ophthalmologists consider season-specific diagnosis, treatment, and management of DED, considering the seasonal characteristics of ocular surface disease in their area of practice.
This study has several strengths. First, sample collection took place at two Japanese institutions, which allowed for a rigorous large-scale case–control study focusing on ophthalmic parameters. Analyses were conducted in 1196 participants, recruited according to strict inclusion and exclusion criteria, without any eyedrops or any ocular surgery, and with normal vision across 3 years. Moreover, the quality of examinations was consistent for each case, including tear strip meniscometry, BUT, and corneal staining. Consequently, the results were obtained with sufficient statistical power. Second, our exhaustive data collection of symptoms and signs associated with DED was evaluated by a single experienced ophthalmologist specializing in dry eye (MA), according to the standardized criteria of the Asia Dry Eye Society,32 thus contributing to the study’s validity.
Several limitations, however, exist. First, this was a hospital-based study and generalization may be needed; however, recruitment was on a walk-in basis and participants consisted of the general population. Second, psychological factors, lifestyle, systemic comorbidities, and medications, as well as local environmental characteristics, may play a role that remains to be examined to add to the results of the current study. Despite this, we recruited patients on their first visit only who were representative of the general population, including individuals with good overall health. Third, measurements of BUT and corneal staining were subjectively performed in the conventional fashion. Reproducibility and accuracy issues may be examined in statistical analysis. Objective methods using image analysis would be relevant for more precise analysis.
In conclusion, a seasonal variation in tear volume was successfully detected with tear strip meniscometry and it was associated with the patients’ subjective ocular dryness. The current results may indicate the clinical usefulness of strip meniscometry.
Abbreviations
BUT, tear break-up time; DED, dry eye disease.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank Keiichi Miyasaka PhD for valuable scientific advice. We also thank Hiroshi Otake MD, Tsutomu Sakai MD, Aya Ohira MD, and Mico Arai CO for help with data collection.
Funding
This research was funded by unrestricted grants from Kanagawa Ophthalmological Association and Santen Pharmaceutical Co., Ltd. The funders were not involved in the manuscript writing, editing, or approval.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tsubota K, Yokoi N, Watanabe H, et al. A new perspective on dry eye classification: proposal by the Asia Dry Eye Society. Eye Contact Lens. 2020;46(Suppl 1):S2–S13. doi:10.1097/ICL.0000000000000643
2. Yokoi N, Georgiev GA. Tear-film-oriented diagnosis for dry eye. Jpn J Ophthalmol. 2019;63(2):127–136. doi:10.1007/s10384-018-00645-4
3. Yokoi N, Georgiev GA. Tear film-oriented diagnosis and tear film-oriented therapy for dry eye based on tear film dynamics. Invest Ophthalmol Vis Sci. 2018;59(14):DES13–DES22. doi:10.1167/iovs.17-23700
4. Dogru M, Ishida K, Matsumoto Y, et al. Strip meniscometry: a new and simple method of tear meniscus evaluation. Invest Ophthalmol Vis Sci. 2006;47(5):1895–1901. doi:10.1167/iovs.05-0802
5. Ibrahim OMA, Dogru M, Ward SK, et al. The efficacy, sensitivity, and specificity of strip meniscometry in conjunction with tear function tests in the assessment of tear meniscus. Invest Ophthalmol Vis Sci. 2011;52(5):2194–2198. doi:10.1167/iovs.10-5986
6. Kojima T, Matsumoto Y, Ibrahim OMA, et al. Effect of controlled adverse chamber environment exposure on tear functions in silicon hydrogel and hydrogel soft contact lens wearers. Invest Ophthalmol Vis Sci. 2011;52(12):8811–8817. doi:10.1167/iovs.10-6841
7. Sano K, Kawashima M, Ikeura K, Arita R, Tsubota K. Abdominal breathing increases tear secretion in healthy women. Ocul Surf. 2015;13(1):82–87. doi:10.1016/j.jtos.2014.08.002
8. Shinzawa M, Dogru M, Miyasaka K, Shimazaki J, Sekiryu T. Application of CASIA SS-1000 optical coherence tomography tear meniscus imaging in testing the efficacy of new strip meniscometry in dry eye diagnosis. Eye Contact Lens. 2018;44(Suppl 1):S44–S49. doi:10.1097/ICL.0000000000000312
9. Shinzawa M, Dogru M, Miyasaka K, Kojima T, Tsubota K. The application of strip meniscometry to the evaluation of tear volume in mice. Invest Ophthalmol Vis Sci. 2019;60(6):2088–2091. doi:10.1167/iovs.19-26850
10. Negishi K, Ayaki M, Uchino M, Takei K, Tsubota K. Strip meniscometry correlates with ocular surface tests and symptoms. Trans Vis Sci Tech. 2020;9(12):31. doi:10.1167/tvst.9.12.31
11. Osawa I, Esaka Y, Kojima T, Simsek C, Kudo H, Dogru M. Feasibility of strip meniscometry for tear volume evaluation in lacrimal passage obstruction. Diagnostics. 2020;10(4):179. doi:10.3390/diagnostics10040179
12. Ayaki M, Tachi N, Hashimoto Y, Kawashima M, Tsubota K, Negishi K. Diurnal variation of human tear meniscus volume measured with tear strip meniscometry self-examination. PLoS One. 2019;14(4):e0215922. doi:10.1371/journal.pone.0215922
13. Miyasaka K, Kazama Y, Iwashita H, Wakaiki S, Saito A. A novel strip meniscometry method for measuring aqueous tear volume in dogs: clinical correlations with the Schirmer tear and phenol red thread tests. Vet Ophthalmol. 2019;22(6):864–871. doi:10.1111/vop.12664
14. Miyasaka K, Ayaki M, Negishi K. Tear strip meniscometry and its clinical application: analysis of more than 2000 cases. Transl Vis Sci Technol. 2022;11(5):3. doi:10.1167/tvst.11.5.3
15. Hao Y, Tian L, Cao K, Jie Y, Sacchetti M. Repeatability and reproducibility of SMTube measurement in dry eye disease patients. J Ophthalmol. 2021;2021:1589378. doi:10.1155/2021/1589378
16. Ayaki M, Kawashima M, Uchino M, Tsubota K, Negishi K. Possible association between subtypes of dry eye disease and seasonal variation. Clin Ophthalmol. 2017;11:1769–1775. doi:10.2147/OPTH.S148650
17. Zhong J-Y, Lee Y-C, Hsieh C-J, Tseng -C-C, Yiin L-M. Association between dry eye disease, air pollution and weather changes in Taiwan. Int J Environ Res Public Health. 2018;15(10):2269. doi:10.3390/ijerph15102269
18. Dermer H, Galor A, Hackam AS, Mirsaeidi M, Kumar N. Impact of seasonal variation in meteorological conditions on dry eye severity. Clin Ophthalmol. 2018;12:2471–2481. doi:10.2147/OPTH.S181637
19. Tesón M, López-Miguel A, Neves H, Calonge M, González-Garcí MJ, González-Méijome JM. Influence of climate on clinical diagnostic dry eye tests: pilot study. Optom Vis Sci. 2015;92:e284–e289. doi:10.1097/OPX.0000000000000673
20. Eidet JR, Chen X, Ræder S, Badian RA, Utheim TP. Seasonal variations in presenting symptoms and signs of dry eye disease in Norway. Sci Rep. 2022;12(1):21046. doi:10.1038/s41598-022-25557-9
21. van Setten G, Labetoulle M, Baudouin C, Rolando M. Evidence of seasonality and effects of psychometry in dry eye disease. Acta Ophthalmol. 2016;94(5):499–506. doi:10.1111/aos.12985
22. Japan Meteorological Agency. Kishocho [Average humidity and temperature (1981–2010)]. Japanese. Japanese: http://www.data.jma.go.jp.
23. Lemp MA. Report of the national eye institute/industry workshop on clinical trials in dry eyes. CLAO J. 1995;21(4):221–232.
24. Sakane Y, Yamaguchi M, Yokoi N, et al. Development and validation of the dry eye-related quality-of-life score questionnaire. JAMA Ophthalmol. 2013;131(10):1331–1338. doi:10.1001/jamaophthalmol.2013.4503
25. Miersch A, Vogel M, Gausche R, et al. Influence of seasonal variation on blood pressure measurements in children, adolescents and young adults. Pediatr Nephrol. 2013;28(12):2343–2349. doi:10.1007/s00467-013-2562-0
26. Hata T, Ogihara T, Maruyama A, et al. The seasonal variation of blood pressure in patients with essential hypertension. Clin Exp Hypertens. 1982;4:341–354.
27. Giaconi S, Ghione S, Palombo C, et al. Seasonal influences on blood pressure in high normal to mild hypertensive range. Hypertension. 1989;14(1):22–27. doi:10.1161/01.HYP.14.1.22
28. Winnicki M, Canali C, Accurso V, Dorigatti F, Giovinazzo P, Palatini P. Relation of 24-hour ambulatory blood pressure and short-term blood pressure variability to seasonal changes in environmental temperature in stage I hypertensive subjects. Results of the harvest trial. Clin Exp Hypertens. 1996;18(8):995–1012. doi:10.3109/10641969609081031
29. Rosenthal P, Borsook D. Ocular neuropathic pain. Br J Ophthalmol. 2016;100(1):128–134. doi:10.1136/bjophthalmol-2014-306280
30. Kikuchi K, Tagawa Y, Murata M, Ishida S. Effects of mirogabalin on hyperalgesia and chronic ocular pain in tear-deficient dry-eye rats. Invest Ophthalmol Vis Sci. 2023;64(5):27. doi:10.1167/iovs.64.5.27
31. Kaido M, Inoue S, Kawashima M, Ishida R, Nakamura S, Tsubota K. Capsaicin-induced pain sensitivity in short tear break-up time dry eye. Ocul Surf. 2020;18(4):620–626. doi:10.1016/j.jtos.2020.07.008
32. Tsubota K, Yokoi N, Shimazaki J, et al.; Asia Dry Eye Society. New perspectives on dry eye definition and diagnosis: a consensus report by the Asia Dry Eye Society. Ocul Surf. 2017;15(1):65–76. doi:10.1016/j.jtos.2016.09.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.