Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Screening for attention deficit and hyperactivity disorder, autism spectrum disorder, and developmental delay in Taiwanese aboriginal preschool children
Authors Chan HL ![]() , Liu WS, Hsieh YH, Lin CF, Ling TS, Huang YS
, Liu WS, Hsieh YH, Lin CF, Ling TS, Huang YS ![]()
Received 30 May 2016
Accepted for publication 22 July 2016
Published 4 October 2016 Volume 2016:12 Pages 2521—2526
DOI https://doi.org/10.2147/NDT.S113880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Wai Kwong Tang
Hsiang-Lin Chan,1,2,* Wen-Sheng Liu,3–6,* Yi-Hsuan Hsieh,1,2 Chiao-Fan Lin,1,2 Tiing-Soon Ling,2,7 Yu-Shu Huang1,2
1Department of Child Psychiatry, Chang Gung Memorial Hospital, 2College of Medicine, Chang Gung University, Taoyuan, 3Division of Nephrology, Department of Medicine, Taipei City Hospital, Zhong-Xing Branch, Taipei, Taiwan; 4School of Medicine, National Yang-Ming University, Taipei, Taiwan; 5Institute of Environmental and Occupational Health Sciences, School of Medicine, National Yang-Ming University, Taipei, Taiwan; 6College of Science and Engineering, Fu Jen Catholic University, New Taipei City, Taiwan; 7Department of Family Medicine, Chang Gung Memorial Hospital, Taoyuan, Taiwan, Republic of China
*These authors contributed equally to this work
Objectives: This study aimed to estimate the percentages of attention deficit and hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) in Taiwanese aboriginal preschool children. Child development level was compared between the two groups.
Methods: Teachers completed screening questionnaires for ADHD, ASD, and development level for 36- to 72-month-old children in kindergartens in Taiwan. The questionnaire results were compared between the aboriginal and nonaboriginal children. One child psychiatrist then interviewed the aboriginal preschool children to determine if they had ADHD and/or ASD.
Results: We collected 93 questionnaires from the aboriginal group and 60 from the nonaboriginal group. In the aboriginal group, 5.37% of the children were identified to have ADHD, while 1.08% were identified to have ASD. Significantly fewer aboriginal children had developmental delays for situation comprehension and personal–social development (P=0.012 and 0.002, respectively) than nonaboriginal children.
Conclusion: Aboriginal children in Taiwan had typical percentages of ADHD and ASD compared to those published in the literature. Aboriginal children showed relative strengths in situation comprehension and personal–social skills. Further studies are required to understand the learning styles of the aboriginal children and to develop effective screening and intervention strategies for ADHD and ASD.
Keywords: attention deficit and hyperactivity disorder, autism spectrum disorder, aboriginal children, child development, developmental delay
Introduction
Few studies have been published regarding attention deficit and hyperactivity disorder (ADHD) and child development in aboriginal children, and none of them has discussed autism spectrum disorder (ASD) in aboriginal children. The Australian longitudinal birth cohort study of urban aboriginal infants reported that 3-year-old Australian aboriginal children performed better in locomotor and personal–social domains and had weakness in language, fine motor, and performance skills.1 Jorm et al found a higher prevalence of behavioral problems in Australian aboriginal children and adolescents than in nonaboriginal children, according to data collected from parents and caregivers.2 Baydala et al had indicated that ADHD characteristics, including hyperactivity, rapidly shifting attention, and impulsivity may have offered selective advantage in early hunter–gatherer society, many of whom were represented by aboriginal populations.3 In their study, a high prevalence of ADHD is reported in Canadian aboriginal children, and the authors suggested that this finding could indicate a particular aboriginal learning behavior or style, which may be misdiagnosed as ADHD.3
In Taiwan, the aboriginal population is 534,007, which accounts for 2.28% of the total population distributed among 14 tribes.4 Most of the aboriginal communities are located in the central mountain areas. The Atayal tribe resides in the area we studied. The aboriginal communities in Taiwan have experienced socioeconomic changes and related difficulties due to industrialization. Most of the aboriginal adults have moved to urban cities for jobs,5 whereas their elderly family members and children remain in their hometown. According to a survey conducted in the elementary schools, compared to families of nonaboriginal students, aboriginal families had higher prevalence of “grandparenting” in their families (5.04% vs 1.66%), single parenting (13.69% vs 6.37%), and low household income (9.12% vs 1.92%).6
The etiology of ADHD involves genetic factors and environmental disadvantages,7 whereas genetic factors predominate in the etiology of ASD.8 The most recent studies have shown overlapping features between ADHD and ASD, and have provided new understanding of the combined phenotype (ADHD + ASD).9,10 Although developmental delay is reportedly associated with several biological and environmental risk factors,11 the environmental risk factors appear to occur more frequently among aboriginal families than nonaboriginal families in Taiwan.6,12,13 Yen et al revealed more severe psychopathology in Taiwanese aboriginal adolescents than nonaboriginal adolescents.14 Adverse environmental factors, including, but not limited to, low socioeconomic status and family disruption, have been reported to make an important contribution to aboriginal adolescents mental health.14 Thus, the aim of this study was to screen ADHD and ASD in Taiwanese aboriginal preschool children and to determine if differences existed in childhood development between the aboriginal and nonaboriginal groups with different genetic constitutions and environmental backgrounds.
Methods
Participants
The Atayal tribal leader was consulted before conducting the study regarding Atayal tribal culture and the study design and methods. The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital. Aboriginal children from four kindergartens in the mountain areas of northern Taiwan with Atayal communities and nonaboriginal children from a kindergarten in a nonaboriginal community in the city were enrolled in the study.
Data collection and measurements
A two-stage survey was conducted. First, we collected data about preschool age (36–72 months) aboriginal children with the written informed consent of their parents. We invited their teachers to complete the screening questionnaires for ADHD and ASD. A total of 93 questionnaires were collected. Second, we informed the teachers about the results of the questionnaires and arranged diagnostic interviews with a child psychiatrist after the initial screening of the children. The child psychiatrist had 15 years of clinical experience working with children with ADHD and/or ASD. Nineteen children screened positive for developmental disorders or developmental delay. In the nonaboriginal group, we collected the same data from preschool children in one kindergarten in a nonaboriginal community. We also invited their teachers to complete the same questionnaire used for the aboriginal community. Sixty questionnaires were completed and all were valid.
Questionnaires
We used questionnaires to screen the children for developmental disorders or developmental delays. The questionnaires were completed by the teachers under the supervision of the child psychiatrist. The questionnaires covered several developmental variables, including inattention and hyperactivity/impulsivity symptoms, autistic symptoms, and developmental level.
Inattention and hyperactivity/impulsivity symptoms
We used the Chinese version of the Swanson, Nolan, and Pelham, Rating Scale-IV (SNAP-IV) to evaluate inattention and hyperactivity/impulsivity symptoms. This questionnaire consisted of 26 questions. It was filled out according to the severity of the symptoms. A score of 0 was for “not at all”; 1 for “just a little”; 2 for “quite a bit”; and 3 for “very much”. Additionally, the first 18 questions include two subsets of symptoms: nine for inattention symptoms (questions 1–9) and nine for hyperactivity/impulsivity symptoms (questions 10–18). Both were consistent with the core symptoms of the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) for ADHD.15 The Chinese version of SNAP-IV used in this study had been verified as a reliable and valid instrument for rating ADHD symptoms.16 A score of 2 or 3 meant the presence of the symptom. The DSM-IV defined children with at least six inattention symptoms as having significant inattention problems, and children with at least six hyperactivity/impulsivity symptoms as having significant hyperactivity/impulsivity problems.
Autistic symptoms
The Chinese version of the Clancy Behavior Scale is the most commonly used valid clinical screening tool for ASD in Taiwan.17,18 Its 14 questions are completed by teachers or parents according to the frequency of the behaviors. A score of 0 is applied for “not at all”, 1 for “occasionally”, and 2 for “frequently”. The cutoff point for the total score is 14/15.
Developmental level
The Chinese Children Developmental Inventory (CCDI), a 320-item questionnaire, is used to evaluate the developmental level of children aged 36–72 months. It is the most commonly used clinical screening tool in Taiwan. The validity and reliability of the CCDI are >0.83 and 0.88, respectively.19 It contains eight developmental domains, including gross motor, fine motor, expressive language, concept comprehension, situation comprehension, self-help, and personal–social and general development. The developmental quotient is defined as the developmental age divided by the chronological age multiplied by 100. Developmental delay is defined as a developmental quotient <70.
Diagnostic interview
After the initial screening, questionnaires were completed and analyzed, and a child psychiatrist interviewed the children with positive screening results. The child psychiatrist interviewed each aboriginal child for 30 minutes to identify ADHD and/or ASD or neither, according to the DSM-IV Text Revision criteria.20
Statistical analysis
SPSS, version 18.0 (SPSS Inc., Chicago, IL, USA) was used for all analyses in this study. We used the chi-square test and Student’s t-test to analyze the demographic data. Moreover, the chi-square test was used to analyze differences in ADHD symptoms in the SNAP-IV and the rates of significant developmental delay identified in the CCDI. The statistical significance was set at P=0.05.
Results
We collected 153 questionnaires (93 from the aboriginal group and 60 from the control nonaboriginal group).
Among the 93 aboriginal children, 56 were boys (60.2%), 37 were girls (39.8%), and their mean age was 53.5±8.6 months (range, 36–72 months) (Table 1). Among the 60 nonaboriginal children, 38 were boys (63.3%), 22 were girls (36.7%), and their mean age was 55.3±5.7 months (range, 40–68 months). No significant difference in sex composition (χ2=0.150, P=0.699) or age (t=−1.508, P=0.134) was observed between the two groups. The child psychiatrist identified ADHD and ASD only by in the aboriginal group.
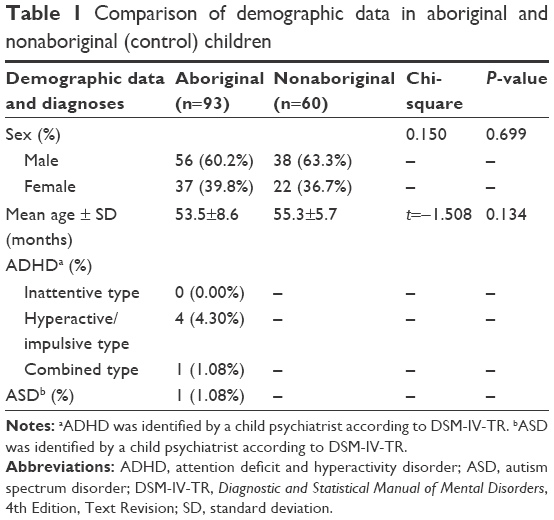 | Table 1 Comparison of demographic data in aboriginal and nonaboriginal (control) children |
Table 2 shows the numbers of aboriginal and nonaboriginal children with ADHD symptoms and autistic behaviors identified in the SNAP-IV and Clancy Behavior Scale, respectively. The questionnaire results indicated no significant differences between the aboriginal and nonaboriginal children.
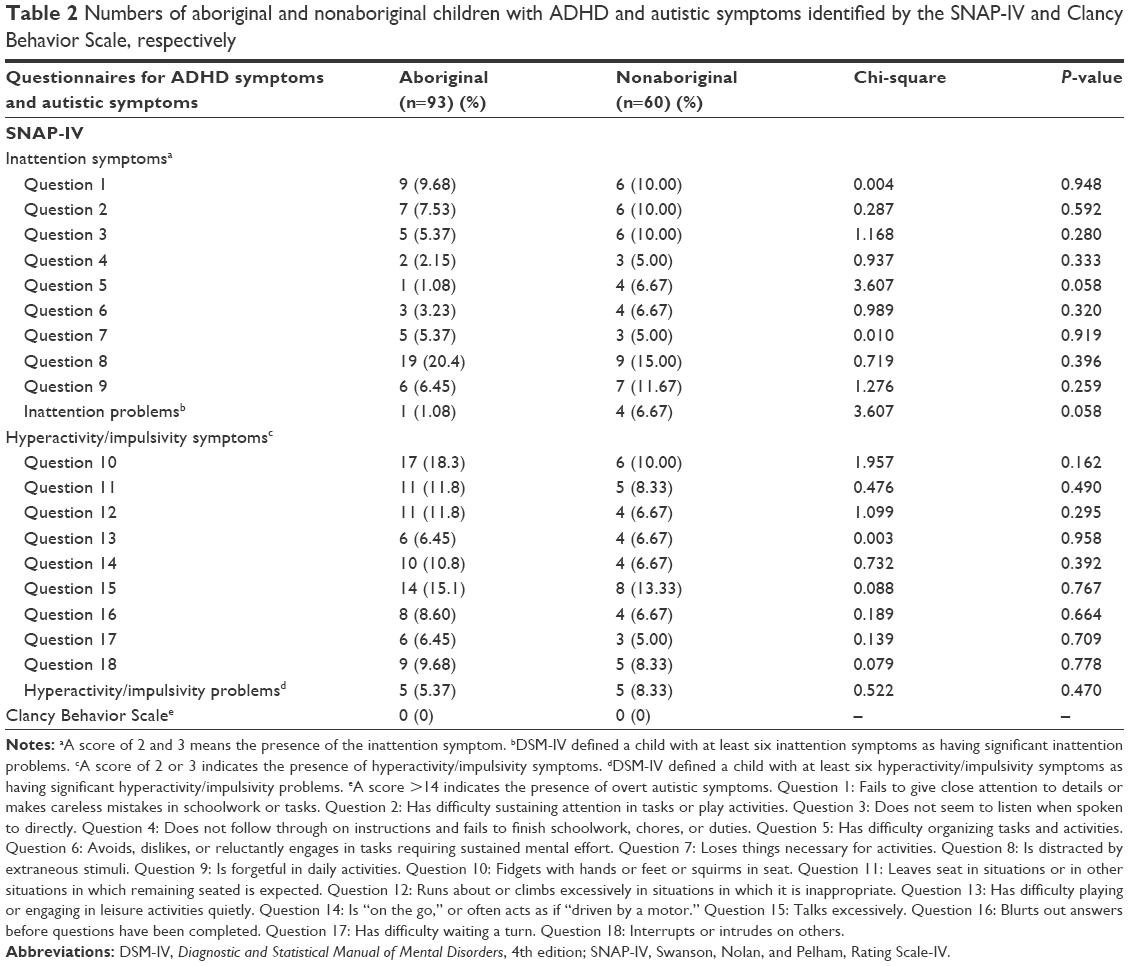 | Table 2 Numbers of aboriginal and nonaboriginal children with ADHD and autistic symptoms identified by the SNAP-IV and Clancy Behavior Scale, respectively |
Table 3 provides a comparison of development delays according to CCDI domain between aboriginal and nonaboriginal children. No significant difference was observed between the two groups for delays in gross motor, fine motor, expressive language, concept comprehension, self-help, or general development. However, significantly fewer aboriginal children had delays in situation comprehension (χ2=6.366, P=0.012) and personal–social development (χ2=9.599, P=0.002).
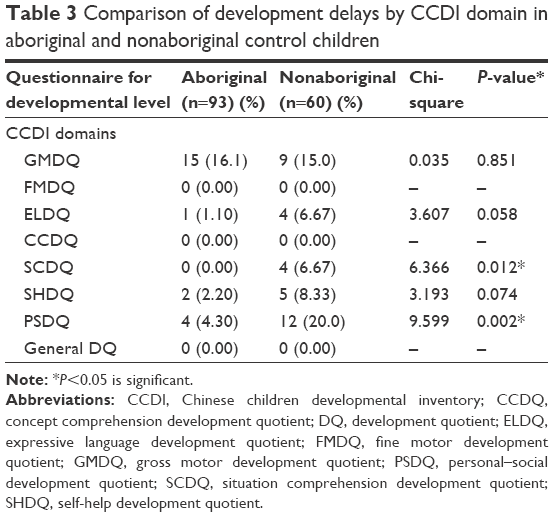 | Table 3 Comparison of development delays by CCDI domain in aboriginal and nonaboriginal control children |
After the interviews, five children (5.37%) were identified with ADHD, four of them had the hyperactive/impulsive type while one had the combined type. One (1.08%) child was identified with ASD. All children with ADHD or ASD were boys (Table 1). The percentage of boys with ADHD was 8.93% and with ASD was 1.79%. However, the percentage of girls with ADHD and/or ASD was zero.
Discussion
ADHD and ASD are significant developmental disabilities that impair function, learning, and family relationships. The diagnosis of these disorders is stable over time.21,22 Of the preschool children with ADHD, 89% will meet ADHD symptom and impairment diagnostic criteria by the time they are 6 years old.22 In our study, the percentage of ADHD in aboriginal preschool children was 5.37%, which is nearly the same as the worldwide prevalence of ADHD (5.29%) in school-age children23 but lower than that previously reported in Taiwan (7.5%) by Gau et al.24 Additionally, our finding was inconsistent with the conclusion of Baydala et al, which indicated that the percentage of ADHD in aboriginal children was higher than the general population due to evolutionary advantage in early aboriginal society.3 Different genetic constitutions may help to explain this discrepancy. From the findings of aboriginal genetic studies, the ancestors of Canadian aborigines were traced to a population of people migrating across the Bering Strait (Beringia) to North America.25 The genetic constitution of Taiwan aborigines was traced to Austronesian people, especially close to the Maori people of New Zealand.26
Previous studies have estimated the prevalence of ASDs to range from 0.7/10,000 to 72.6/10,000 people.27 Several studies have shown the prevalence of ASDs as 0.9% in South Korea28,29 and 1.7% in the UK.30 Moreover, one meta-analysis collected past studies from People’s Republic of China, Hong Kong, and Taiwan and estimated the pooled prevalence of ASDs as 26.6/10,000.31 Nonetheless, we did not find any studies of ASD conducted in aboriginal populations in Taiwan. The percentage of ASD (1.08%) of aboriginal children in our study was close to those reported in South Korea28,29 and the UK.30 According to our experience, children with ASD need intense behavior therapy, but we found that the resources needed for special education were lacking in the aboriginal community. We have reported the existence of ASD in aboriginal children; therefore, it is necessary to support the development of special education related to the disorder in the aboriginal community.
Although existing data showed significant socioeconomic disadvantage in the aboriginal population in Taiwan,6 we did not find poorer child development in aboriginal preschool children. McDonald et al analyzed data from the Gudaga study, in which the Griffiths Mental Development Scales, Extended Revised, and the Peabody Picture Vocabulary Test, Fourth Edition were used to evaluate the development of children.1 Consistent with their findings, we also found aboriginal children had better personal-social development.1 We propose that genetic and cultural differences may help to explain this finding. The daily schedule for aboriginal kindergarten children emphasized more team work, interpersonal interaction, and play, while the nonaboriginal kindergarten tended to focus on knowledge learning and sedentary activities such as learning English, science, reading books, and playing chess. Aboriginal children were given more time for outdoor activities and less time for watching television or playing computer games.
Limitations
This study had some limitations. First, the sample size was small. Second, teachers may be biased because they observed only aboriginal students or only nonaboriginal students. Finally, we did not conduct diagnostic interviews in the control group, so we can only compare the percentages of ADHD and ASD in the aboriginal group with those published in the literature.
Despite these limitations, this is the first study to compare the development of aboriginal children with those of nonaboriginal children and identify ASD in aboriginal children. Moreover, the identification of ADHD and ASD was not only made according to the screening questionnaires but was also confirmed by the child psychiatrist.
Conclusion
Aboriginal preschool children in Taiwan showed the typical percentages of ADHD and ASD and better social ability. Further studies are needed to characterize the learning styles of aboriginal children in order to help to develop effective screening and intervention strategies.
Acknowledgments
We are grateful to all the children and their teachers and parents who participated in the study. This study was supported by intramural grant (CORPG3C0021, CORPG3C0022, CORPG3C0023).
Disclosure
The authors disclose no conflict of interest.
References
McDonald J, Webster V, Knight J, Comino E. The Gudaga Study: development in 3-year-old urban Aboriginal children. J Paediatr Child Health. 2014;50(2):100–106. | ||
Jorm AF, Bourchier SJ, Cvetkovski S, Stewart G. Mental health of indigenous Australians: a review of findings from community surveys. Med J Aust. 2012;196:118–121. | ||
Baydala L, Sherman J, Rasmussen C, Wikman E, Janzen H. ADHD characteristics in Canadian Aboriginal children. J Atten Disord. 2006;9(4):642–647. | ||
Ministry of the Interior. Monthly Bulletin of Interior Statistics, Republic of China. Taipei, Executive Yuan, Taiwan. 2014 (In Chinese). | ||
Huang CH. Discussion on the status for career development of aboriginal students. Taipei County Education. 2008;63:65–68 (In Chinese). | ||
Council of Indigenous people. Education statistics in Taiwanese Indigenous People in 2011. Taipei, Taiwan, 2011 (In Chinese). | ||
Sandberg S. Hyperkinetic or attention deficit disorder. Br J Psychiatry. 1996;169(1):10–17. | ||
Freitag CM. The genetics of autistic disorders and its clinical relevance: a review of the literature. Mol psychiatry. 2007;12(1):2–22. | ||
Craig F, Lamanna AL, Margari F, Matera E, Simone M, Margari L. Overlap between autism spectrum disorders and attention deficit hyperactivity disorder: searching for distinctive/common clinical Features. Autism Res. 2015;8(3):328–337. | ||
Craig F, Margari F, Legrottaglie AR, Palumbi R, de Giambattista C, Margari L. A review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiatr Dis Treat. 2016;12:1191–1202. | ||
Laucht M, Esser G, Schmidt MH, et al. “Risk children”: the importance of biological and psychological risks for child development in the first two years of life. Prax Kinderpsychol Kinderpsychiatr. 1992;41(8):274–285 (abstract) (In German). | ||
Chen TM. The current condition of aboriginal families in Alishan. E-Soc Journal. 2004;43 (In Chinese). | ||
Chang TM. Implement of learning family. In: Collection of strategies for aboriginal learning family implement. National Chiayi University Family Education Center. 2000:37–85 (In Chinese). | ||
Yen CF, Hsu CC, Liu SC, Huang CF, Yang MS. Psychopathology of aboriginal and non-aboriginal adolescents living in the mountainous region of southern Taiwan. Kaohsiung J Med Sci. 2006;22(11):560–569. | ||
Swanson JM, Kraemer HC, Hinshaw SP, et al. Clinical relevance of the primary findings of the MTA: success rates based on severity of ADHD and ODD symptoms at the end of treatment. J Am Acad Child Adolesc Psychiatry. 2001;40(2):168–179. | ||
Gau SS, Lin CH, Hu FC, et al. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, Version IV Scale-Teacher Form. J Pediatr Psychol. 2009;34(8):850–861. | ||
Clancy H, Dugdale A, Rendle-Short J. The diagnosis of infantile autism. Dev Med Child Neurol. 1969;11:432–442. | ||
Hsieh CF, Soon WT, Hsu CC. Autism: Clancy Behavior Scale validity study. Chinese Society of the Neurology and Psychiatry Bulletin. 1983;9(1):17–26 (In Chinese). | ||
Hsu CC, Shao SJ, Lin CC, Soong WT, Chang C. Chinese child developmental inventory: a tentative normative data. Acta Paediatr Taiwan. 1978;19:142–157 (In Chinese). | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR. 4th ed. (Text Revision). Arlington, VA: American Psychiatric Publishing, Inc; 2000. | ||
Woolfenden S, Sarkozy V, Ridleyb G, Williamsc K. A systematic review of the diagnostic stability of autism spectrum disorder. Res Autism Spect Dis. 2012;6(1):345–354. | ||
Riddle MA, Yershova K, Lazzaretto D, Paykina N, Yenokyan G, Greenhill L, et al. The preschool attention-deficit/hyperactivity disorder treatment study (PATS) 6-year follow-up. J Am Acad Child Adolesc Psychiatry. 2013;52(3):264–278.e2. | ||
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–948. | ||
Gau SS, Chong MY, Chen TH, Cheng AT. A 3-year panel study of mental disorders among adolescents in Taiwan. Am J Psychiatry. 2005;162(7):1344–1350. | ||
Zegura SL, Karafet TM, Zhivotovsky LA, Hammer MF. High-resolution SNPs and microsatellite haplotypes point to a single, recent entry of Native American Y chromosomes into the Americas. Mol Biol Evol. 2004;21(1):164–175. | ||
Jin F. Genetic study of native Taiwan populations based on the investigation of red cell enzyme genetic markers, unpublished thesis, University of Tokyo; 1992. (unpublished). | ||
Fombonne E. Epidemiology of pervasive developmental disorders. Pediatr Res. 2009;65(6):591–598. | ||
Kim YS, Leventhal BL, Koh YJ, Fombonne E, Laska E, Lim EC, et al. Prevalence of autism spectrum disorders in a total population sample. Am J Psychiatry. 2011;168(9):904–912. | ||
Baxter AJ, Brugha TS, Erskine HE, Scheurer RW, Vos T, Scott JG. The epidemiology and global burden of autism spectrum disorders. Psychol Med. 2015;45(3):601–613. | ||
Russell G, Rodgers LR, Ukoumunne OC, Ford T. Prevalence of parent-reported ASD and ADHD in the UK: findings from the millennium cohort study. J Autism Dev Disord. 2014;44(1):31–40. | ||
Sun X, Allison C, Matthews FE, et al. Prevalence of autism in mainland China, Hong Kong and Taiwan: a systematic review and meta-analysis. Mol Autism. 2013;4(1):7. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.