Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Scoring Of Post Stroke Pneumonia In Uttaradit Hospital
Authors Leangpanich N, Chuphanitsakun Y, Pakaranodom K, Kerdjarern K, Poonual W
Received 7 June 2019
Accepted for publication 7 October 2019
Published 15 November 2019 Volume 2019:12 Pages 917—923
DOI https://doi.org/10.2147/JMDH.S218654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Watcharapol Poonual.
Views: 1751
Nichakarn Leangpanich,1 Yanin Chuphanitsakun,1 Kanyaros Pakaranodom,1 Kunlachat Kerdjarern,1 Watcharapol Poonual2
1Medical Education Center, Faculty of Medicine, Naresuan University, Uttaradit Hospital, Uttaradit 53000, Thailand; 2Medical Education Research Center, Uttaradit Hospital, Uttaradit 53000, Thailand
Correspondence: Watcharapol Poonual
Medical Education Center Uttaradit Hospital, Jadsadabordin Road, Tambon Ta – it Amphur Muang, Uttaradit 53000, Thailand
Tel +6655 832601-3
Fax +66 55 411543
Email [email protected]
Background: Stroke is a disease which occurs when the blood supply to the brain is interrupted, depriving brain tissue of oxygen, resulting in cell death. The symptoms of stroke include: numbness, paraplegia, dysarthria, ataxia, etc. The most common complication is infection. The highest death rates among hospitalized stroke patients are from pneumonia.
Objective: To develop a score for predicting post-stroke pneumonia infection and identify risk factors for patients with post-stroke pneumonia.
Study design: Retrospective case-control.
Setting: Uttaradit hospital (the tertiary hospital), Thailand.
Method: A retrospective data study was conducted at Uttaradit hospital, Thailand from January 2014 to October 2018 in which all of the subjects were diagnosed with either stroke with pneumonia or without pneumonia by a physician. The selected 324 stroke patients were divided into two groups: 108 patients were stroke with pneumonia and 216 patients were stroke without pneumonia. This study involved data collection and analysis of study characteristics to develop a predictive score for post-stroke pneumonia.
Results: This study identified risk factors and developed a score for predicting post-stroke pneumonia infection by using significant covariates (duration of admission; 1–10 days=0 points, 11–20 days=1 point, more than 20 days=2.5 points, Cardiovascular disease=1.5 points, Nasogastric tube=2 points, Urinary tract infection=1 point). This score was interpreted to three groups; low risk (<2 points), moderate risk (2.5–4 points), and high risk (>4 points). Sensitivity was 80.56% and specificity was 93.52%.
Conclusion: A simple prediction tool was developed that uses only four clinical variables to predict risk of post-stroke pneumonia with high sensitivity and specificity.
Keywords: pneumonia, stroke, risk factor, risk score
Background
Stroke occurs when a blood vessel is either blocked by a clot or ruptured, causing damage to the brain tissue.1 That causes a variety of symptoms such as weakness or numbness of the face, arm, or leg, difficulty speaking or understanding speech, difficulty walking, and difficulty seeing with one or both eyes.2 Some stroke patients develop complications while hospitalized, which are mostly brain edema, pneumonia, urinary tract infection, seizures, clinical depression, bedsores, limb contractures, shoulder pain, and deep venous thrombosis (DVT).3
According to the literature review, the most common complications of stroke are post-stroke infection (30%). Rate of pneumonia and urinary tract infection after stroke were 10%.4 Pneumonia has a mortality rate of 35% of all post-stroke death.5,6 Symptoms of pneumonia may include fever, cough, and dyspnea.7 Meanwhile fever is usually hidden by using aspirin in a stroke patient,8 also cough is barely found in stroke patients as well.9 Dyspnea may be a result of underlying disease such as heart failure or COPD.10 The initially normal chest x-rays are more likely in pneumonia.11
Therefore, we developed a score for predicting post-stroke pneumonia infection with proper surveillance and management.
Objectives
- To develop a score for predicting post-stroke pneumonia infection;
- To identify risk factors of patients with post-stroke pneumonia while admitted to Uttaradit hospital.
Methods
Study design: Retrospective case controlled.
Population: stroke patients admitted at Uttaradit hospital between January 2014 and August 2018.
Target population: 108 Stroke patients with pneumonia. (Pneumonia was recorded by the treating physician based on clinical symptoms of lung infection in combination with clinical signs such as rales on chest auscultation and chest X ray findings suggestive for pneumonia supported by laboratory tests such as complete blood count.)
Control Population: 216 stroke patients without pneumonia.
Exclusion Criteria: Community-acquired pneumonia patients.
The study was designed as a case-control analysis of data from an academic affiliated community hospital that retrospectively collects data from stroke patients admitted at Uttaradit hospital between January 2014 and August 2018. The study was divided into two stroke patient groups: with or without pneumonia (108 and 216, respectively). The exclusion criteria was Community-acquired pneumonia.
Statistical Methods
From 6,088 stroke patients who were hospitalized in Uttaradit hospital between 2014–2018, stroke with pneumonia was diagnosed in 409, and 5,679 were stroke patients without pneumonia.
A retrospective case-control study accumulated with a related literature review proved that atrial fibrillation12 is one of the predisposing risk factors among pneumonia statistically. So we used two independent proportions of the presence and absence of pneumonia in stroke patients by using power 90%, alpha=0.05, p1=0.249, p2=0.513, and the index to reference proportion is 1:2 which sampled 324 patients to 10 index cases, and 216 reference cases.
Variable Data
Independent variable: age group, sex, length of stay, lesion, NIHSS SCORE, underlying disease, medical treatment such as Endotracheal intubation, Nasogastric tube, Percutaneous gastrostomy, and Urinary catheter, other complications, eg, epileptic seizure, Sepsis, Urinary tract infection, Heart failure, and arrhythmia.
Dependent variable: pneumonia in stroke patients.
Descriptive Statistics
Categorical data: count data and percentage were analyzed using the chi-squared test and Fisher’s exact test.
Numerical data: Median, Interquartile Range was analyzed using student t-test or Wilcoxon rank-sum test.
Analytic Statistics
A univariable logistic regression model was used to analyze each explanatory variable, interpreted as odds ratio, 95% CI, and p-value.
A multivariable logistic regression model was used to analyze all explanatory variables interpreted as odds ratio, 95% CI, and p-value.
Results
General Characteristics
General characteristics analysis from 324 stroke patients of whom 108 had pneumonia and 206 didn’t have pneumonia were not different between the groups in sex, age group, lesion of right hemisphere, both hemisphere, brain stem or cerebellum, and ventricle or sinus, Diabetes, atrial fibrillation, cardiovascular disease, Hyperlipidemia, and COPD.
The stroke without pneumonia group had more lesions of the left hemisphere than the pneumonia group statistically.
The length of stay, lesion at Basal ganglion or thalamus, and Hypertension were significantly higher in those stroke patients who had pneumonia (Table 1).
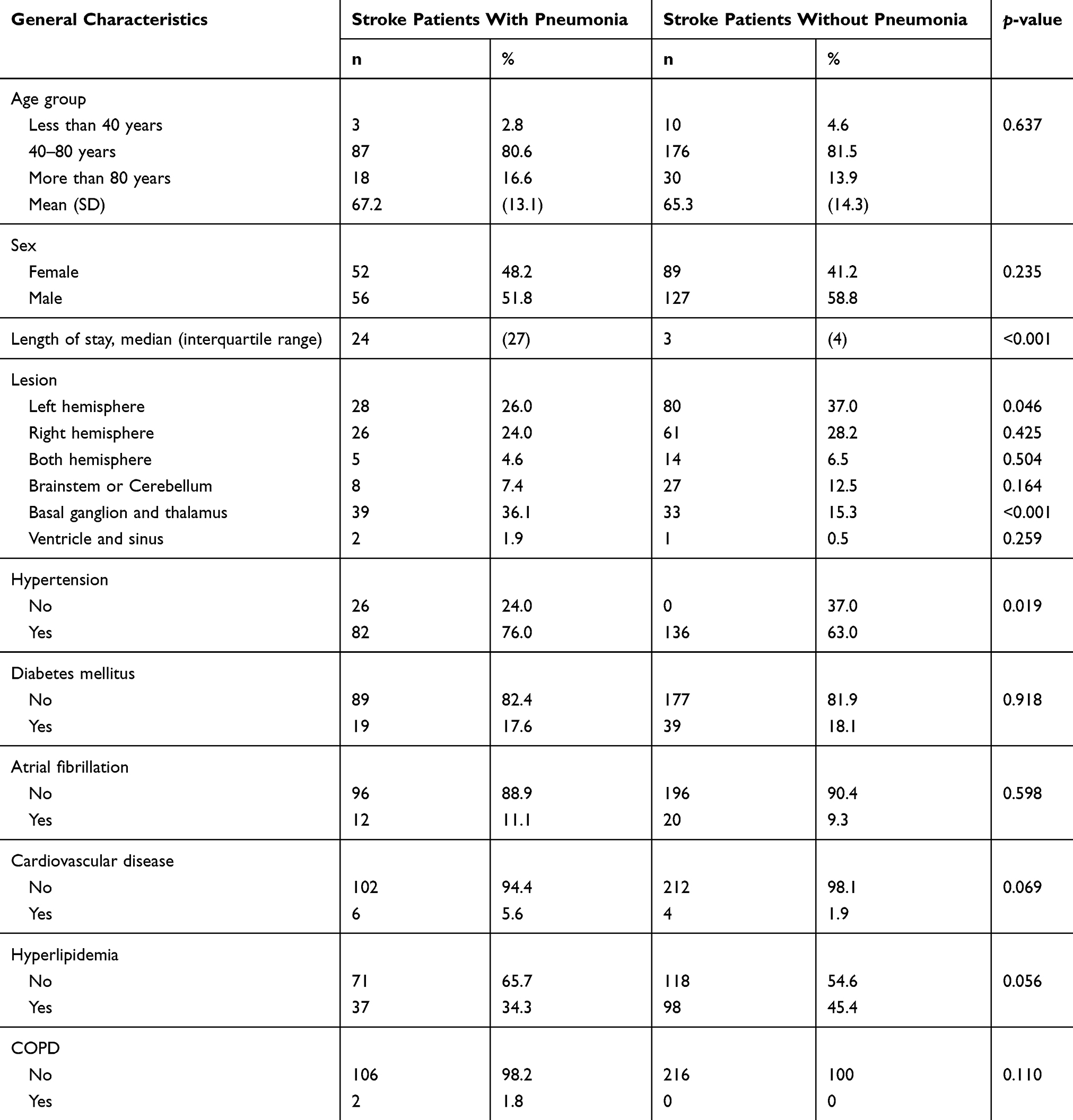 |
Table 1 General Characteristics Of Stroke Patients With Pneumonia Versus Without Pneumonia |
Medical Treatment
In sites with pneumonia, endotracheal intubation, Nasogastric tube, and Urinary catheter were significantly higher than those sites without pneumonia (Table 2).
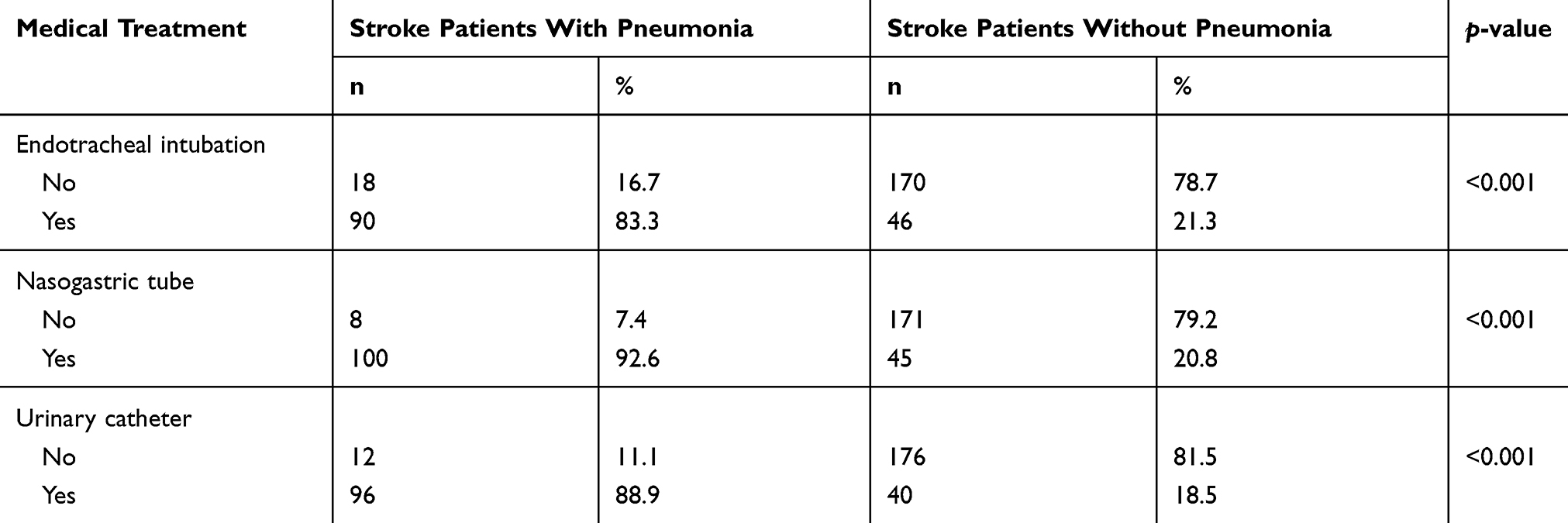 |
Table 2 Medical Treatment Of Stroke Patients With Pneumonia Versus Without Pneumonia |
Other Complications
Those stroke patients who developed pneumonia had significantly higher rates of epileptic seizure, Sepsis, Urinary tract infection, and Heart failure (Table 3).
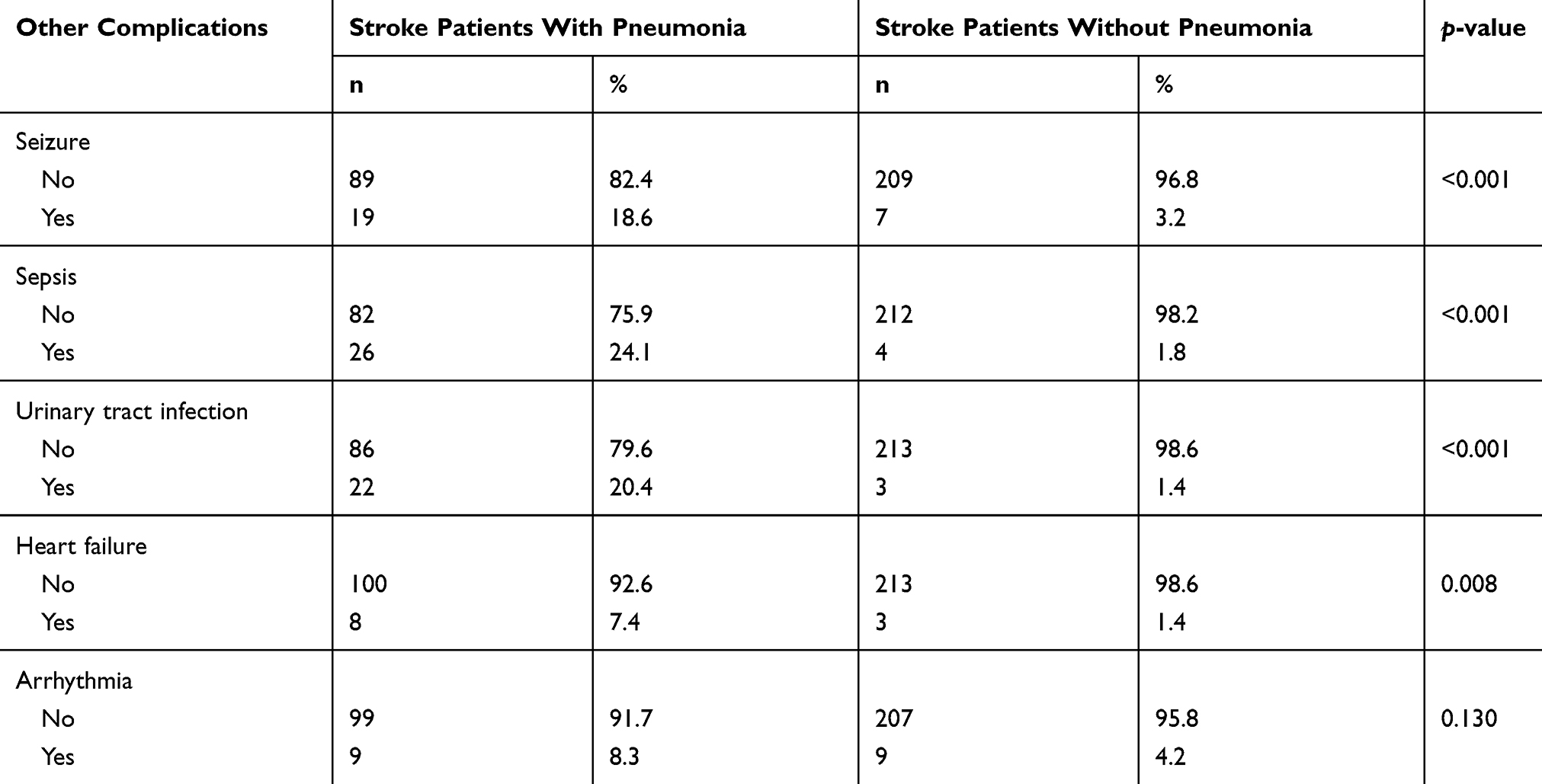 |
Table 3 Other Complications Of Stroke Patients With Pneumonia Versus Without Pneumonia |
Odds Ratio Of Pneumonia In Stroke Patients
The 40–80 years age groups of stroke patients had a 1.6-fold increaded odds of developing pneumonia. Likewise, a stay of 11–20 days and more than 20 days increased the odds 11.5- and 141.8-fold, respectively. The complications of cardiovascular disease and urinary tract infection increased the odds 3.1- and 18.2-fold, respectively. Meanwhile, stroke patients had a nasogastric tube had an increased risk of developing pneumonia of 47.5-fold (Table 4).
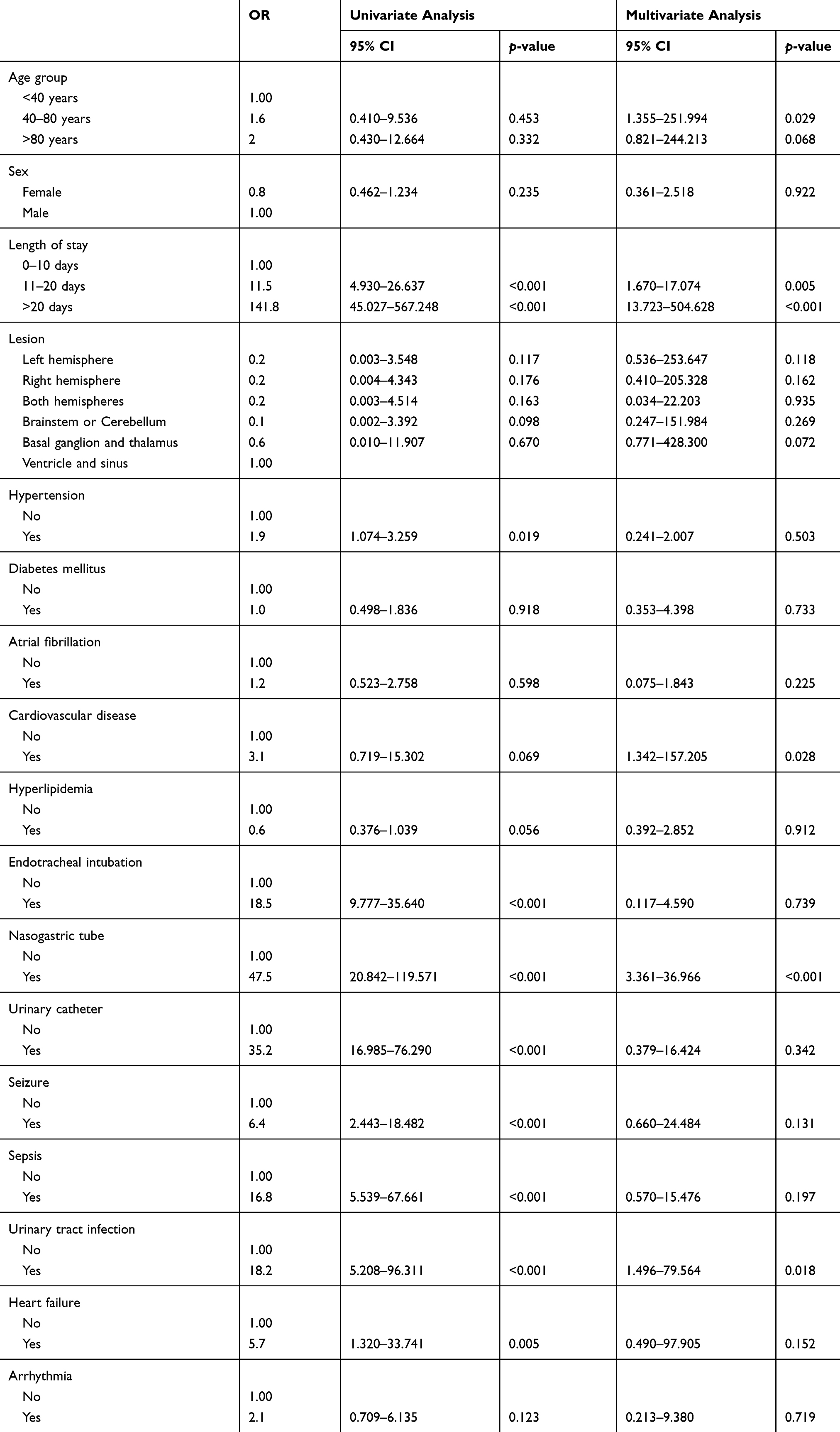 |
Table 4 Odd Ratio Of Developing Pneumonia In Stroke Patients |
Score For Predicting Post-Stroke Pneumonia Infection
After analysis by multivariable logistic regression, there were four variables to make a score for predicting post-stroke pneumonia infection, which is Length of stay that divided into three intervals (1–10 days=0, 11–20 days=1, and more than 20 days=2.5), 1.5 points for cardiovascular disease, 2 points for nasogastric tube, and 1.5 points for urinary tract infection.
The score was divided into three groups, those with lower than 2 points were defined as a lower risk group, while the medium risk group was counted for 2.5–4 points, and more than 4 points for the high risk group (Table 5) with 80.56% sensitivity and 93.52% specificity. There was a positive predictive value of 86.14 and a negative predictive value of 90.58.
 |
Table 5 Score For Predicting Post-Stroke Pneumonia Infection |
Discussion
Risk factors of post-stroke pneumonia patients were identified and predicting score was developed with high sensitivity and specificity by using four variables that are easy and convenient for screening and setting priority to proper surveillance in stroke patients who are likely to have pneumonia.
Stroke patients in the age group 40–80 years, longer length of stay, complications of cardiovascular disease and urinary tract infection, or nasogastric tube use increase the risk of developing pneumonia. It is possible that patients with a longer length of stay will have a longer time exposed to pathogens in the hospital. Elderly people tend to be more at risk of developing pneumonia because their immune system is weaker. The association with procedures such as nasogastric tube is possibly related to severe illness leading to prolonged bed rest.
This study is limited in that the data cannot collect the variables of NIHSS score, smoking and alcohol use history, since this is a retrospective case controlled study and these data were not completely found in medical records, despite another study providing this; these are associated risk factors to develop post-stroke pneumonia statistically.12 Therefore this predicting score would cover all risk factors and may decrease accuracy. Moreover, this score will still not be used in general practice so it could not be confirmed to assess in other populations.
Conclusion
The score for predicting post-stroke pneumonia infection can be assessed as a screening program, but this study did not yet use in practice. However, interpretation was limited by missing some important data that leads to potential risk factors to generate a score. We suggest that the next study should require the prospective case control study for improving the quality of the data collection.
Ethics Statement
The authors wish to acknowledge the Research Ethics Committee of the Uttaradit Public Health Office, Uttaradit, Thailand, which has approved the following study which is to be carried out in compliance with the International guidelines for human research protection as Declaration of Helsinki, The Belmont Report, CIOMS Guideline and International Conference on Harmonization in Good Clinical Practice (ICH-GCP). The authors receive the approval of granted subject to this condition from the official affiliated name of the institutional review board which approved this study are: The patient consent to review the medical records in this research was not required by the IRB because the study design of this research is retrospective with no harm to patients and no conflict of interest.
Acknowledgement
The authors wish to acknowledge the head of the medication education research center of Uttaradit Hospital, Dr. Surasak Saokaew, Associate Professor, School of Pharmaceutical Sciences, University of Phayao, Dr. Jirawan Deelua, Assist Professor, faculty of nursing, Chiang Mai university, and Uttaradit hospital’s medical record audit for their support in this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sacco R, Kasner S, Broderick J, et al. An updated definition of stroke for the 21st Century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
2. Who.int. [Internet]. Stroke, Cerebrovascular accident. WHO; 2018. Available from: http://www.who.int/topics/cerebrovascular_accident/en/.
3. Strokeassociation.org [Internet]. Complication after stroke; 2018 Available from: https://www.strokeassociation.org/idc/groups/stroke-public/@wcm/@hcm/@sta/documents/downloadable/ucm_474388.pdf.
4. Westendorp W, Nederkoorn P, Vermeij J, Dijkgraaf M, de Beek D. Post-stroke infection: a systematic review and meta-analysis. BMC Neurology. 2011;11:1. doi:10.1186/1471-2377-11-110
5. Walter U, Knoblich R, Steinhagen V, Donat M, Benecke R, Kloth A. Predictors of pneumonia in acute stroke patients admitted to a neurological intensive care unit. J Neurol. 2007;254:1323–1329. doi:10.1007/s00415-007-0520-0
6. Hinchey JA, Shephard T, Furie K, Smith D, Wang D, Tonn S. Formal dysphagia screening protocols prevent pneumonia. Stroke. 2005;36:1972–1976. doi:10.1161/01.STR.0000177529.86868.8d
7. Pneumonia [Internet]. World Health Organization; 2018 Available from: http://www.who.int/news-room/fact-sheets/detail/pneumonia.
8. Bachert C, Chuchalin AG, Eisebitt R, et al. Aspirin compared with acetaminophen in the treatment of fever and other symptoms of upper respiratory tract infection in adults: a multicentre, randomized, double-blind, double-dummy, placebo-controlled, parallel-group, single dose, 6 hour dose-ranging study. Clin Ther. 2005;27:993–1003. doi:10.1016/j.clinthera.2005.06.002
9. Miles A, Moore S, McFarlane M, Lee F, Allen J, Huckabee ML. Comparison of cough reflex test against instrumental assessment of aspiration. Physiol Behav. 2013;118:25–31. doi:10.1016/j.physbeh.2013.05.004
10. Kishore A, Vail A, Chamorro A, et al. How is pneumonia diagnosed in clinical stroke research?: A systematic review and meta-analysis. Stroke. 2015;46(5):1202–1209. doi:10.1161/STROKEAHA.114.007843
11. Esayag Y, NikitinI B-ZJ, Cytter R, et al. Diagnostic value of chest radiographs in bedridden patients suspected of having pneumonia. Am J Med. 2010;123:
12. Matz K, Seyfang L, Dachenhausen A, Teuschl Y, Tuomilehto J, Brainin M. Post-stroke pneumonia at the stroke unit – a registry based analysis of contributing and protective factors. BMC Neurology. 2016;16:1. doi:10.1186/s12883-016-0627-y
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.