Back to Journals » Risk Management and Healthcare Policy » Volume 12
School health for migrant children: a myth or a must?
Authors Tuangratananon T, Julchoo S ![]() , Wanwong Y, Sinam P, Suphanchaimat R
, Wanwong Y, Sinam P, Suphanchaimat R ![]()
Received 28 September 2018
Accepted for publication 29 May 2019
Published 10 July 2019 Volume 2019:12 Pages 123—132
DOI https://doi.org/10.2147/RMHP.S189081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Titiporn Tuangratananon1,2, Sataporn Julchoo,1 Yaowaluk Wanwong,1 Pigunkaew Sinam,1 Rapeepong Suphanchaimat1,3
1International Health Policy Program, Ministry of Public Health, Nonthaburi 11000, Thailand; 2Department of Health, Ministry of Public Health, Nonthaburi 11000, Thailand; 3Bureau of Epidemiology, Department of Disease Control, Ministry of Public Health, Nonthaburi 11000, Thailand
Background: School health plays a vital role in lifelong health outcomes. Migrant children are a vulnerable population that seem to have inadequate health promotion interventions, and limited studies have assessed their health status and personal hygiene at schools. This study aimed to evaluate school health promotion and health outcomes of migrant children in Thai public schools (TPSs) and migrant learning centers (MLCs).
Methods: A cross-sectional study was applied. Data were collected from questionnaires focusing on health care access, nutritional status, and personal hygiene of migrant children in two MLCs and four TPSs, along with Thai children in the same TPSs. Descriptive analysis and logistic regression model were used to compare access to health promotion and the health status of migrant children with the Thai counterparts.
Results: Blended school health services were generally found in TPSs, which led to indifferent vaccination rates between Thai and migrant children in TPSs (odds ratio [OR] 0.457 (0.186–1.120)). However, vaccination rates of migrant children in MLCs are noticeably around fourfold lower. Overall, migrant children received fewer dental health services than Thai children, both in TPSs (OR 0.198 (0.076,0.517)) and MLCs (OR 0.156 (0.004,0.055)). Other personal hygiene behaviors and nutritional statuses saw no significant difference between Thai children and migrant children in either TPSs or MLCs. The uninsured status among migrant children posed another challenge to health care access, as 81.7% of the migrant children in MLCs and 56.6% in TPSs were uninsured.
Conclusion: Migrant children in MLCs received a lower rate of essential vaccinations compared to those in TPSs. Dental services appeared to be the most neglected area of care in migrant children. The findings indicate the necessity of supportive policy for MLCs, while regulating quality and standards concurrently. Multisectoral collaboration is critically needed for sustainably improving the quality of life of migrant children.
Keywords: migrant children, migrants learning center, school health promotion, education
Introduction
Migrants are considered one of the most vulnerable populations in many countries, and migrant children are possibly the most vulnerable among the vulnerable. Multiple resolutions have been made at the global level at the United Nations General Assembly (UNGA) meeting in 2006,1 and the Joint United Nations Programme on HIV and AIDS (UNAIDS) Board meeting in 2009.2 The World Health Organization (WHO) has also turned the spotlight on the health of migrants through the World Health Assembly Resolutions (WHRs), including the WHR61.17 (2008)3 and the latest in WHR70.15 (2017).4
In the Southeast Asia region, Thailand is one of the major countries for migrant intake, including an estimated 3.5 million migrant workers from Cambodia, Laos, and Myanmar.5 Among them, the number of children is estimated to be 250,000–270,000, with around 70,000 left uneducated.6 Limited and inadequate access to health, education, appropriate sanitary conditions, and nutrition contributes to poor health outcomes among migrant children. The health problems commonly found in migrant children seem to have strong links with poor living conditions.7 Migrant families tend to live in confined and overcrowded spaces with very limited clean water supplies. This contributes to poor personal hygiene of migrant children, including inadequately bathing, teeth brushing, and hair washing. Malnutrition, resulting in migrant children being underweight, was also frequently reported in many studies.8–11 However, some literature also shows the bright side of health services for migrant children. The majority of migrant children received essential vaccines on schedule under the policy of concurrently boosting the health of migrant children and protecting health of the society.12
The literature also demonstrates a strong relationship between health and education. In the context of Thailand, the Cabinet Resolution in Education for Unregistered Persons of the Kingdom of Thailand in 200513 has provided rights for non-Thai children to be enrolled in Thai public schools (TPSs) regardless of their immigration status. The Resolution encompassed a wide range of non-Thai children, including first-generation and second-generation migrant children as well as unaccompanied minors. Nevertheless, certain obstacles, including language barriers, financial difficulties, unsupportive parental perspectives, and cultural differences, implicitly led to some migrant parents declining to have their children enrolled in TPSs.14 To resolve the issue, “migrant learning centers” (MLCs) have been established and serve as alternatives for migrant children, especially in migrant-populated communities. Yet, there is still limited research on the success and operational challenges faced by the MLCs.15
Focusing on school hygiene in Thailand, the “Health Promoting School” program was initiated in 1999 by the Department of Health, Ministry of Public Health. The program aims to set standards of healthy environments in schools and promotes all school pupils (regardless of nationalities) to receive health education, school food, school milk, and regular health check-up.16 So far, the program has been settled in more than 90% of the Thai schools in Thailand. However, the program has not been officially implemented in MLCs yet.
Henceforth, the objective of this study is to explore and compare the nutritional status and personal hygiene of migrant children with Thai children, in the context of both in TPSs and MLCs. In addition, this study also aims to identify possible explanations for the health promotion situation among migrant children in the MLCs and more importantly to provide practical policy recommendations to strengthen health promotion activities for migrant children in Thailand.
Materials and methods
Study design and population
The study applied a cross-sectional survey conducted in Ranong province, Thailand. Ranong is located in the southern region of Thailand. The province shares natural borders with Myanmar and has the greatest share of migrants to total populations compared to other provinces in the country. Within the province, the two most migrant-populated districts were selected, namely Muang district (headquarter district) and Kraburi district. Then, two TPSs with the largest share of migrant children to Thai children were selected from each district. Additionally, two MLCs were also selected as the distinctive education site of migrant children. Note that MLCs are located only in Muang district.
The sample size was calculated from the formula17 n= z2*p*(1-p)/d2, when the 95% confidence interval of z is 1.96, p is the proportion of interested variable, and d is errors. In this study, p represented the proportion of stunting from the Multiple Indicator Cluster Survey (MICS), which accounted for 23%.18 The value of d was substituted by 0.1. According to sample calculation, the prospective responses were 84 students with additional non-response rates of 15–20%. As a result, at least 25 students were needed from each school/center. However, we found that there was a possibility of obtaining more samples from each school/center, leading to the total number of 375 students in the study. Therefore, students were selected from four TPSs and two MLCs by census method. Questionnaires were mainly distributed to students over the age of six; for those below six, teachers were asked to assist students to complete the questionnaires. In some complicated questions (for instance, insurance status and vaccination history) that could not be answered by the students, the authors had asked teachers and/or parents of these children to answer the questions on their behalf.
Questionnaire
The questionnaire was modified from Akiyama et al19 and translated into Burmese for students in MLCs by a certified linguistic professional. During the questionnaire development phase, the content validity consensus was made between researchers and teachers. There were three parts in the questionnaire; 1) demographic data which including date of birth, sex, race, education level (pre-school, primary school, and secondary and high school), parental occupations (no specific work, construction labor, housemaid, vendor, fisherman, and others) and places of birth (Thailand and Myanmar), facilities at birth (hospital and home), and health insurance profile (Health Insurance Card [HIC], universal coverage scheme, civil servant benefit scheme, private insurance, others, and no insurance); 2) nutritional status data which consist of height and weight, and will be converted to weight for age, height for age, and weight for height; and 3) hygiene behaviors composed of shoes wearing, bathing, tooth brushing, vaccination, and dentist visits. The levels of answers were divided into adequate, occasional, and never.
Variables management and data analysis
The demographic data and health insurance profiles were analyzed by descriptive statistics. For nutritional profiles, we determined to use “height for age”, “weight for age”, and “weight for height”, in accordance with the Thai nutritional surveillance guideline provided by the Department of Health, Ministry of Public Health in 1995. Each parameter was obtained electronically from the web-based calculator provided by the Institute of Nutrition, Mahidol University, Thailand.20 Height for age was classified as short, slightly short, normal, slightly tall, and tall. Weight for age was also classified as underweight, slightly underweight, normal, slightly overweight, and overweight. Likewise, weight for height was categorized as thin, slightly thin, normal, possible risk of overweight, overweight, and obese. Then, we created new binary variables based on values from the variables mentioned earlier. For instance, a new variable called “normal_height_for_age” was created and coded 0 (below_normal) if the height for age variable presented as either short and coded 1 if otherwise. The same logic was applied to weight for age and weight for height variables. These new variables were served as dependent variables in the logistic regression analysis, which was detailed later. Dependent variables for hygiene behaviors consist of shoes wearing, nails cutting, hair washing, bathing, tooth brushing, dentist visiting, and vaccination. The levels of frequency were divided into three categories, which were “adequate”, “occasional”, and “never”.
All data were analyzed by both descriptive and inferential statistics. For inferential statistics, logistic regression was applied. The nutrition status variables and hygiene behaviors enlisted earlier served as dependent variables in the logistic regression. Whereby, the independent variables were 1) education levels, which were pre-school (kindergarten), primary school, and secondary and high school, and 2) a combination of races and education sites, that is, Thai students in TPSs, migrant children in TPSs, and migrant children in MLCs. All statistical analyses were performed by STATA version 12.
Ethical considerations
At the beginning of the study, school teachers and guardians of children were informed about the purpose of the study and the procedures to collect questionnaires. The participation of students was voluntary, and data remain confidentially protected. Verbal inform and written consent were obtained from parental or legal guardians. Children over age of 12 years old were also required to sign their own consent forms. The ethics committees of the Institute for the Development of Human Research Protections, Thailand, have accepted and approved the study.
Results
Demographic data
In total, 375 students answered the questionnaire with ages ranging from 3.8 to 19.6 years (mean=10.4 y, SD=3.9 y) as shown in Table 1. Almost all students in MLCs were Burmese, while in TPSs the total number of Burmese students (58.9%) was higher than Thai students (35.5%). Most students were in primary school grades (78.6% for TPSs and 42.1% for MLCs). Most participants live with their parents. Regarding parental occupations, parents of MLCs students mostly worked as fishermen (56.6%) and non-specific labors (17.8%), while parents of TPSs students mainly worked as non-specific labors (62.4%) and vendors (17.9%).
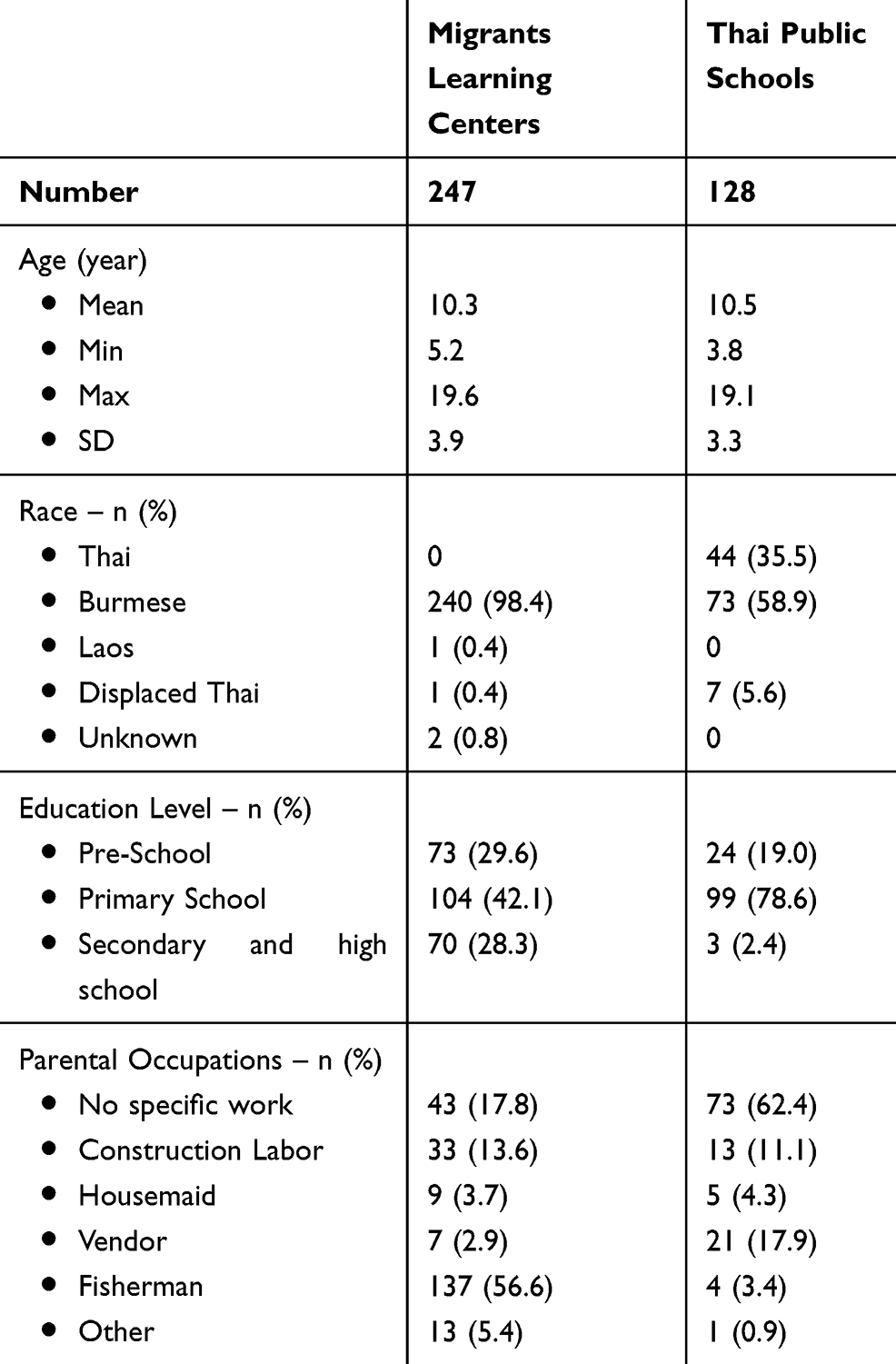 |
Table 1 Demographic data |
The main insurance scheme for migrants is the Health Insurance Card, issued by the ministry of Public Health. As displayed in Figure 1, most migrant students were non-insured for their health. The percentage of non-insured students was higher in MLCs than in TPSs (81.7% compared to 56.6%).
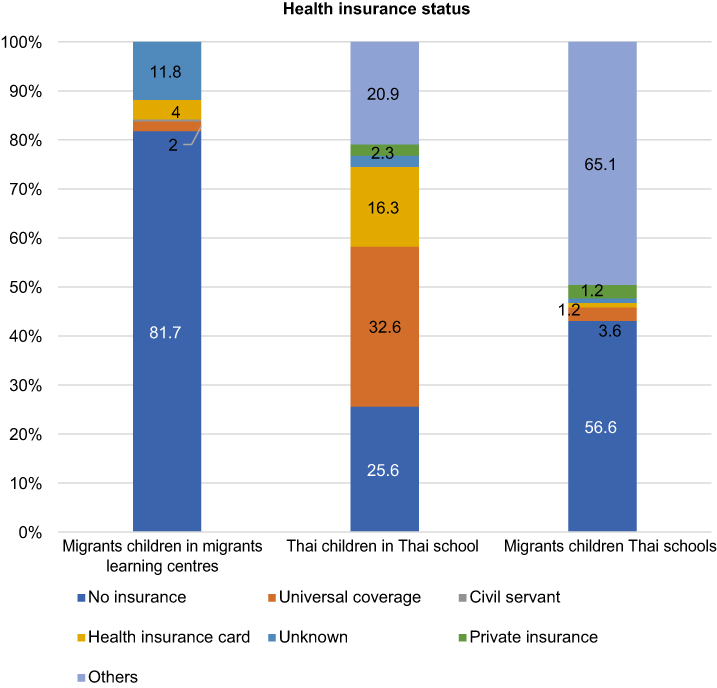 |
Figure 1 Health insurance status of Thai and migrant children. |
As can be seen in Figure 2, most Thai children were born in hospitals (92.9%). Among migrant children born in Thailand generally, only 78.2% were born in hospitals. In contrast, merely 53.3% of the Myanmar-born migrant children were born in hospitals.
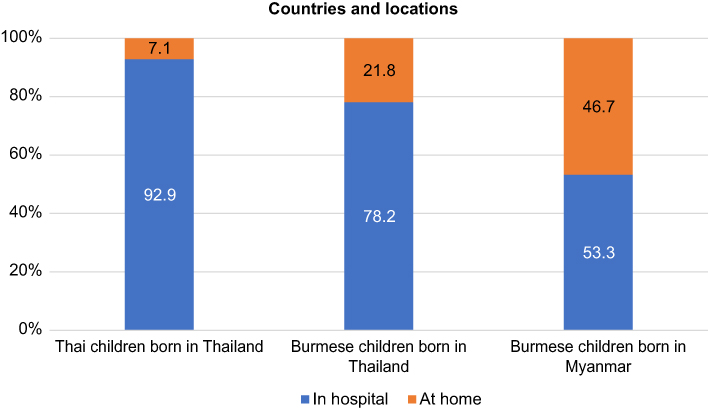 |
Figure 2 Birth countries and locations for Thai and migrant children. |
Nutritional status
The majority of migrant children in the study, regardless of race, were within the range of normal height and weight for age, and identical to Thai children at 73.39%. As shown in Figure 3, when focusing on undernutrition status, we observed that migrant children with chronic malnutrition status labeled as “short” accounted for 8.47%. Meanwhile, acute malnutrition status, which can be indicated by being underweight, was 4.44%. Similar to both indicators earlier, most children had normal weight for height (68.15%), as shown in Figure 3. The percentage of children who were classified into “slightly thin” and “thin” categories were 6.05% and 8.06%, respectively.
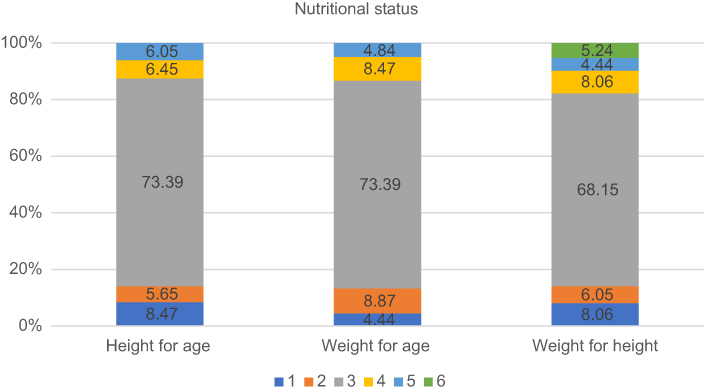 |
Figure 3 Physical status descriptive analyses for height for age, weight for age, and weight for height. Height for age: 1 - short, 2 - slightly short, 3 - normal, 4 - slightly tall, 5 - tall. Weight for age: 1 - underweight, 2 - slightly underweight, 3 - normal, 4 - slightly overweight, 5 - overweight. Weight for height: 1 - thin, 2 - slightly thin, 3 - normal, 4 - possible risk of overweight, 5 - overweight, 6 - obese. |
Results of logistic regression on nutritional status of migrant children are demonstrated in Table 2, and significant differences existed across education levels, races, and education sites. Overall, primary school migrant students were about 4.6 times (p-value 0.002 (1.738–12.407)) more likely to have adequate height than Thai students. Likewise, primary school migrant students were 4.5 times (p-value 0.002 (1.758–11.672)) more likely to gain normal weight for age, compared with pre-school students. Migrant children in TPSs were more vulnerable to being underweight than Thai children for about 81% (p-value 0.04, 95%CI 0.039–0.930). Other nutritional indicators did not show statistically significant differences.
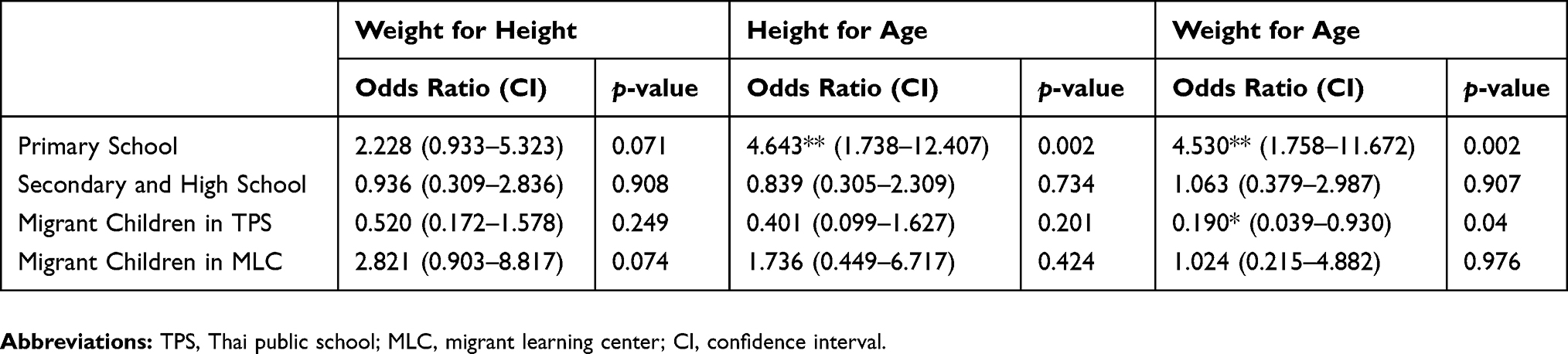 |
Table 2 Physicall status logistic regression analysis |
Hygiene behaviors
Figure 4 demonstrates the result of descriptive analysis of personal hygiene status of all students. Most migrant children had proper hygiene behaviors in terms of shoe wearing, nail cutting, tooth brushing, hair washing, and bathing. However, a noticeable difference was found in dental care and vaccination, as only 14.56% of the respondents reported to have regular dental care visits, and only 66.01% of the migrant children received adequate vaccination.
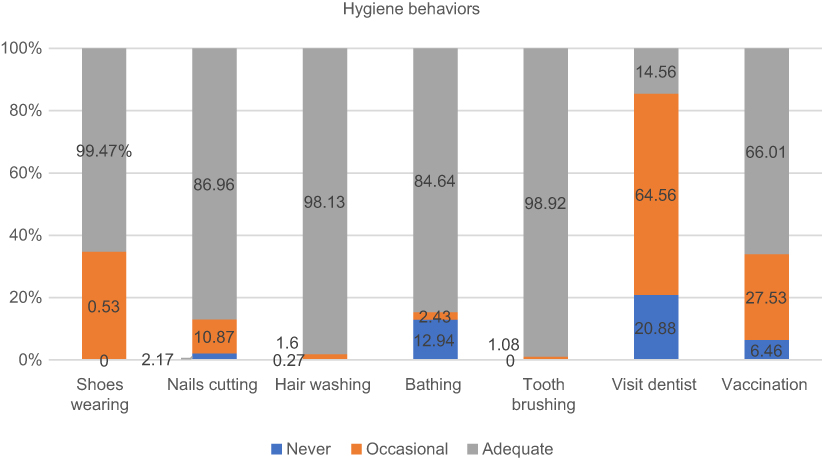 |
Figure 4 Hygiene behaviors descriptive analysis. |
Table 3 presents the results of logistic regression analysis on hygiene behaviors. Among seven health behaviors, the most significant difference between migrant and Thai children was found in dental check-up and vaccinations. Specifically, migrant children in MLCs had an 84.4% (p-value<0.001, 95%CI 0.004–0.005) lower possibility of receiving adequate dental check-ups than Thai children. Similarly, migrant children in TPSs also had an 80.22% (p-value 0.001, 95%CI 0.076–0.517) lower chance of visiting dentists regularly than Thai children. In general, migrant children in TPSs had significantly fewer regular dental visits than Thai children, and the number of dentist visitors was even lower among migrant children in MLCs.
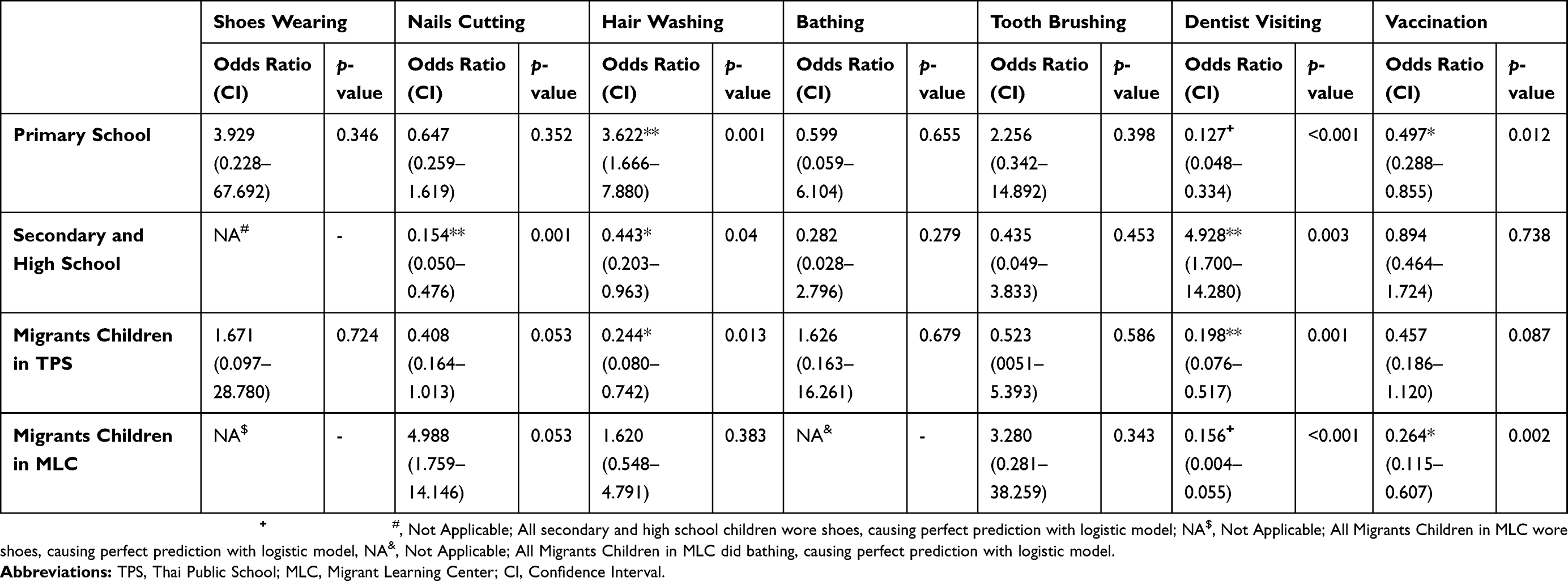 |
Table 3 Hygiene behaviors logistic regression analysis |
For vaccine completion, primary school students were found to be 50.3% (p 0.012, 95%CI 0.228–0.855) less likely to receive adequate vaccination than pre-school children. Migrant children in MLCs were more likely to have incomplete vaccinations by 73.6% (p 0.002, 95%CI 0.115–0.607) compared to Thai children. Note that migrant children in TPS also had inadequate vaccinations, despite non-statistically significant differences when compared to Thai children. The remaining five health behaviors saw no statistically significant difference between migrant children and Thai children.
Discussion
The results show that migrant children in TPSs received similar health prevention and promotion interventions as Thai children, for instance, similar school health education and vaccinations. In contrast, migrant children in MLCs have a 74% higher chance than Thai children to be inadequately vaccinated (Table 3). This finding is in line with a previous study by Salmon et al that reported the shortage of cooperation between MLCs and local health-promoting hospitals, which are the key institutions in delivering vaccines.7 Other possible determining factors include birthing place and facility. We found that among migrant children who were born in Thailand, 78.2% were born in hospitals; in contrast, merely 53.3% of the Myanmar-born migrant children were born in hospitals (in Figure 2). Interestingly, a link between birthing plaperperce/facility and vaccination rate was also identified in the report of the Voluntary Service Overseas Thailand/Myanmar.7
Overall, there a noticeable disparity in health behaviors and nutritional status between Thai and migrant children in both TPSs and MLCs and in the extent of access to dental services. Our study shows that migrant children have more than 80% chance of inaccessibility to dental services compared with Thai children (Table 3). In fact, providing dental care is part of local health-promoting hospitals’ duties. Furthermore, regular dental check-up services in TPSs are served by local health-promoting hospitals but reserved solely for Thai citizens due to insufficient budget and human resources. Local health care providers also struggle with project development especially in the context of concerns of the need to target Thai citizens first, to avoid questions about use of public resources intended for non-Thai children.
In nutritional status, migrant children may not be significantly different to Thai children. However, migrant children in TPSs have slightly lower weight for age than Thai children as shown in Table 2. A possible explanation could be that migrant children in MLCs tended to reside in urban areas and were classified in a higher socioeconomic status, as parents need to pay tuition fee for MLCs. Other personal hygiene behaviors are quite similar between Thai and migrant children, which may be a result of health education efforts of non-governmental organizations in the past.7
The deficit of appropriate dental access might refer to the limited insurance subscription of migrant children. In addition, though not directly related to nutritional profiles in the studies, 56.6% of the migrant children in TPSs and 81.7% in MLCs are uninsured (Figure 1). Even though migrant children have the right to purchase a HIC or enroll in the Social Security Scheme, many remain uninsured.21 Other studies suggest the possible underlying reasons for this including: 1) having a high number of dependents in a family leading to the financial difficulty; 2) parents are unaware of purchasing HIC for their children; 3) undocumented migrants are unwilling to purchase HIC; and 4) Hospital staff deny migrants the HIC due to narrow legal interpretations.7,21
School health plays a fundamental role in shaping student personal hygiene. Education and health also have a strong relationship with each other. In Ranong province, heterogeneity exists in MLC education due to the lack of standardized operations across centers. Although MLCs offer attractive transferable curricula taught in the Burmese language, the health situation of students remains questionable due to the limited capacities of MLCs. Most MLCs experience scarcity of school lunch and milk provision, insufficient toilet installation, overcrowded classrooms, and poor air ventilation in buildings. Recent studies revealed that MLCs may not consider school health as a priority.22 The number of migrant children in MLCs was almost three times as large as those in TPS, yet education and related health interventions are undoubtedly necessary for child development. This is worth exploring further and should serve as the focus for future studies.
Health care professionals provide health education, health surveillance and vaccinations to all students in TPS.23 In principle, Thai health care professionals should equitably promote school health to all students without discrimination. However, equity in practice often applies only in TPS contexts. In MLCs, limited health staff and low budgets directly inhibit efforts to promote health. In the past, there was no responsible authority to regulate MLCs in the province, as MLCs are not officially considered as schools, and were overlooked by Ministry of Education (MoE) and Ministry of Public Health (MoPH). MLCs are initiatives originating from NGOs and charitable organizations.
Some key policy recommendations are proposed as a result of findings. First, government authorities should consider establishing multisectoral committees to regulate, develop, and adequately support MLCs and their response to migrant children’s health needs. Relevant ministries such as Ministry of Education, Ministry of Public Health, and Ministry of Social Development and Human Security should collaborate and develop appropriate strategies to oversee MLCs, and then further develop a database of migrant children to allow for tracking and support. In the long run, related legislative tools and bodies should be made more flexible in terms of health promotion budget allocation based upon the principle of universal health coverage in order to cover migrant children more easily. This is especially the case for health promotion related to hygiene behaviors, dental care and vaccinations, as they are currently overlooked. Separated vaccine budgets for migrant children should be established to strengthen national health security. Further studies addressing migrant children insurance options are recommended to ensure the health rights of all children.
Limitations
It is worthy to note the limitations of this study. In particular, drawing generalizations from findings at our single specific study site (Ranong province) should be done with the full awareness of provincial differences. Another key limitation point is a lack of economic-status variable in the analysis. This might lead to omitted variable bias. Normally for Thai households, the National Statistical Office of Thailand routinely conducts nationwide survey on the households’ economic level. Asset index which is a valid proxy of household’s economy will be produced from the survey. Unfortunately, the survey did not include migrants’ households. This issue demonstrates gaps in knowledge on socioeconomic data of migrant populations and demand for future work in the research arena on migrant health. Furthermore, the study relies on a cross-sectional questionnaire survey, which may have limitations in identifying the causal effect between migrant children’s demographic profile and their personal hygiene and health status. There was also a possible error from respondents, as some teachers provided help with some of the questionnaires. In addition, some acquiescence bias might have occurred with informants during the interview, due to the fact that all respondents knew that the researchers were the MoPH officials.
Conclusion
Health promotion to migrant children in schools remains underserved, in spite of the continuous effort of local health care providers. Children in MLCs are significantly inadequately vaccinated, compared with migrant children in TPSs. Moreover, all migrant children in both MLCs and TPSs have limited access to school dental services and have high rates of being uninsured. Migrant children are more likely to be undernourished but have adequate personal hygiene compared with Thai children. Rigorous actions should be taken by related agencies, either government or private organizations, to support and promote migrant children’s quality of life, especially in the area of health promotion.
Acknowledgments
The authors gratefully acknowledge longstanding support from Dr Viroj Tangcharoensathien and Dr Suwit Wibulpolprasert. We thank MLC and TPS coordinator, Provincial Public Health and Health-promoting hospital officers, the World Vision officers, and International Health Policy Program Foundation staff for their great collaborations and contributions.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. The United Nations. UN population: high level dialogue on international migration and development; 2006. Available from: http://www.un.org/esa/population/migration/hld/.
2. Joint United Nations Programme on HIV/AIDS. Resolution 2009/6 Joint United Nations Programme on HIV/AIDS (UNAIDS). Geneva; 2007. Available from: https://www.un.org/ecosoc/sites/www.un.org.ecosoc/files/documents/2009/resolution-2009-6.pdf.
3. Sixty-first World Health Assembly. WHA 61.17 Health of Migrants. Geneva; 2008. Available from: http://apps.who.int/iris/bitstream/10665/23533/1/A61_R17-en.pdf.
4. Seventieth World Health Assembly. WHA 70.15: Promoting the Health of Refugees and Migrants [Internet]. Geneva; 2017. Available from: http://www.un.org/en/development/desa/population/migration/generalassembly/docs/globalcompact/WHA_RES_70.15.pdf.
5. Migration Data Hub. International migration statistics. 2017; Available from: https://www.migrationpolicy.org/programs/migration-data-hub.
6. Kantayaporn T, Sinhkul N, Ditthawongsa N, Chinworasopark P, Silwutthaya S, Phanathanasarn K. Estimation of Transnational Population for Developing Maternal and Child Health in Bangkok. Nonthaburi: HSRIO; 2013.
7. Salmon A, Thanwai SA, Wongsaengpaiboon H. In School, in Society: Early Childhood Development in Myanmar Migrant Communities in Thailand. Bangkok; 2013. Available from: https://reliefweb.int/sites/reliefweb.int/files/resources/. In school in society Early childhood development in Myanmar migrant communities in Thailand.pdf. Accessed March 25, 2019.
8. ADM Capital Foundation. Thai-Burmese Border. Educating Burmese Migrant Children in Thailand - ADMCF. ADM Cap. Found. 2018; Available from: http://admcf.org/2011/12/01/thai-burmese-border-l-educating-burmese-migrant-children-thailand/.
9. Hjern A, Bouvier P. Migrant children - A challenge for European paediatricians. Acta Paediatr Int J Paediatr. 2004;93(11):1535–1539. doi:10.1111/j.1651-2227.2004.tb02643.x
10. Shah AY. Prevalence of Anemia and Malnutrition among Refugee Children Entering DeKalb County. Georgia. In: 2012 AAP National Conference and Exhibition, 2012 Oct 20. American Academy of Pediatrics; 2012.
11. Fabio M. Nutrition for refugee children: risks, screening, and treatment. Curr Probl Pediatr Adolesc Health Care. 2014;44:188–195. doi:10.1016/j.cppeds.2014.03.003.
12. Akiyama T, Win T, Maung C, et al. Making schools healthy among burmese migrants in Thailand. Health Promot Int. 2013;28(2):223–232. doi:10.1093/heapro/das010.
13. The Thai Cabinet. Draft Guideline of the Ministry of Education in Ratifying Rights to Education for non-Thai Children and Children with Citizenship Problems. Bangkok: The Government of Thailand; 2005.
14. Punpuing S, Kusakabe K, Holumyong C, Chamchan C, Darawuttimaprakorn N. Migrant Children’s Education in Thailand. Bangkok; 2014. Available from: http://www.ipsr.mahidol.ac.th/ipsrbeta/FileUpload/PDF/Report-File-503.pdf.
15. Nawarat N. Schooling and activism in a zone of exception: migrant learning centres on the thai-burma border. J Soc Sci Chiang Mai Univ. 2012;23(1–2):117–157.
16. Bureau of Health Promotion. Health Promoting School Implementation Guideline. Nonthaburi: Bureau of Health Promotion, Ministry of Public Health; 2015.
17. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol from Bed to Bench . 2013;6(1):14–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24834239. Accessed October 9, 2017.
18. National Statistical Office, United Nations Children’s Fund, Ministry of Public Health, National Health Security Office, Thai Health Promotion Foundation, International Health Policy Program.Thailand. Monitoring the situation of children and women. Multiple indicator cluster survery; 2012; 2013. Available from: https://mics-surveys-prod.s3.amazonaws.com/MICS4/East Asia and the Pacific/Thailand/2012-2013/Final/Thailand 2012 MICS_English.pdf.
19. Akiyama T, Win T, Maung C, et al. Making schools healthy among Burmese migrants in Thailand. Health Promot Int. 2013. doi:10.1093/heapro/das010
20. Institute of Nutrition. INMU-ThaiGrowth. Mahidol Univ; 2009. Available from: http://www.inmu.mahidol.ac.th/thaigrowth/#.
21. Suphanchaimat R. “Health insurance card scheme” forcross-border migrants in Thailand: responsesin policy implementation & outcome evaluation. 2017. Available from: http://researchonline.lshtm.ac.uk/3817560/.
22. Tuangratananon T, Suphanchaimat R, Poungkantha W, et al. Situation analysis in providing education services and health promotion and disease promotion activities in schools for migrant children in Thailand: A case study of Ranong province. Nonthaburi: HSRIO; 2018.
23. Putthasri W, Suphanchaimat R, Nipaporn S, et al. System Management and Budget Estimation for Supporting Health Promotion and Disease Prevention Services for Migrant Children in Thailand. Nonthaburi: IHPP, Ministry of Public Health; 2017.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.