Back to Journals » Clinical Ophthalmology » Volume 13
School bus accommodation-relaxing skiascopy
Authors Arnold AW ![]() , Arnold SL, Sprano JH, Arnold RW
, Arnold SL, Sprano JH, Arnold RW ![]()
Received 11 June 2019
Accepted for publication 22 August 2019
Published 8 October 2019 Volume 2019:13 Pages 1841—1851
DOI https://doi.org/10.2147/OPTH.S219031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Robert W Arnold.
Views: 528
Andrew W Arnold,1 Stephanie L Arnold,1 Jacob H Sprano,2 Robert W Arnold3
1Pacific Northwest University College of Osteopathic Medicine, Yakima, WA, USA; 2Kansas City University of Osteopathic Medicine, Kansas City, MO, USA; 3Alaska Blind Child Discovery, Alaska Children’s Eye & Strabismus, Anchorage, AK, USA
Correspondence: Robert W Arnold
Alaska Blind Child Discovery, Alaska Children’s Eye & Strabismus, 3500 Latouche #280, Anchorage, AK 99508, USA
Tel +1 907 561 1917
Fax +1 907 563 5373
Email [email protected]
Objective: Accurate estimation of hyperopia and astigmatism is challenging in delayed children. Conventional skiascopy holds rows of increasing power ± lenses vertically in front of one eye. The school bus accommodation-relaxing skiascopy (SBA-RS) design holds child-friendly, lenses +1 to +10D horizontally so that a higher power fogs the nontested eye-relaxing accommodation without cycloplegia.
Methods: Design: Evaluation of diagnostic test. Subjects: Patients undergoing comprehensive eye examination in a pediatric ophthalmology practice. Cycloplegic (cyclopentolate 1%) retinoscopy was compared to dry SBA-RS and Retinomax (Righton, Japan) during pediatric eye examinations. Outcome measures: correlations, Chi-square and receiver operating characteristic (ROC) curve.
Results: Of 470 patients with a median age 6 years, 238 were under the age of 60 months and 110 had developmental delays. For those with cycloplegic spherical equivalent hyperopia over 0.7 D, median (90% CI) value for retinoscopy was +2.63 D (+0.75, +6.88), for SBA-RS was +2.50 D (+0.50, +6.75) and less for 184 with Retinomax +1.88 D (−1.56, +6.13) but similar despite delays. Astigmatic cylinder SBA-RS +1.50 D (+0.25, +4.00) lagged retinoscopy +1.75 D (+0.75,+4.50) but Retinomax was greater +2.00 D (+0.25, +4.64). Cycloplegic refractive components such as spherical equivalent, cylinder, and J0 and J45 power vectors correlated highly and were near unity with SBA-RS and Retinomax with the latter deviating greater. SBA-RS screened for amblyopia risk factors up to 92% sensitive and 94% specific.
Conclusion: Accommodation-relaxing horizontal skiascopy very precisely estimates astigmatism power and axis and only lags cycloplegic refraction by about 0.15D in hyperopic patients fairly independent of neurodevelopmental delay. This technique can quickly estimate refraction even in delayed patients potentially reducing some need for cycloplegia.
Clinical Trials Registry: NCT03668067.
Keywords: hyperopia, retinoscopy, cycloplegia, skiascopy
Introduction
Cycloplegia is considered an integral component of a confirmatory pediatric ophthalmology examination because it aims to uncover all hyperopia and minimize over-minus, and it affords mydriasis for a wide view of the retina.1 The downsides of cycloplegia include 1) painful, unwanted drops,2–4 2) incomplete absorption and effect,5,6 and 3) prolonged exam time.7,8 Pediatric and developmentally delayed patients often dislike, or are emotionally traumatized by, cycloplegic instillation, especially repeated instillation.2,3 Hyperopia above 3.5 diopters is a recognized risk factor for amblyopia;9 however there exists a disparity; the risk factor prevalence for high hyperopia (8%) far exceeds the prevalence of amblyopia of 2.5%.10 It is likely that latent hyperopia is a better predictor of amblyopia than cycloplegic hyperopia because many children compensate for their hyperopia with robust accommodation.11 An abbreviated examination combined with latent hyperopia revealing photoscreening may obviate cycloplegia in some children.12
Dynamic retinoscopy is a technique that can expose some hyperopia and compensatory accommodation.11,13 Noncycloplegic retinoscopy was found to be the most sensitive of all 11 screening techniques prospectively evaluated in Phase 1 of the landmark NIH-funded Vision in Preschoolers study (VIPS),14 even though it underestimated some cases of hyperopia and astigmatism. A better method for revealing hyperopia, especially in children and developmentally delayed adults is desired.
We modified the conventional vertically oriented, double-row skiascopy rack: 1) to include a single row of increasing integer convex lenses from +1 through +10, 2) to hold horizontally so a higher plus lens covers the contralateral, fixing eye for fogging,15 3) to utilize a child-friendly design of a school bus, 4) to add millimeter ruler and 5) one wheel with a concave −5 lens and the other with a translucent occluder. We call this the school bus accommodation-relaxing skiascopy (SBA-RS, Eye Care and Cure, Tuscon, AZ, USA).
Retinomax (model K +3, Righton, Tokyo) is a handheld autorefractor with sufficiently high reliability16 such that it was chosen to determine gold-standard refractive error in the Multi-Ethnic Pediatric Eye Disease study.17 We studied the relative merit of SBA-RS compared to Retinomax in estimating cycloplegic refraction in patients with and without developmental delay.
Methods
This prospective study is covered by Institutional Review Board at Providence Hospital with Clinical Trial Registry (NCT03668067) and de-identified data access from www.ABCD-Vision.org. The study complies with HIPAA and the Declaration of Helsinki. Images and video of children examined by this technique are included. Written parental informed consent with appropriate translation was obtained.
The SBA-RS rack (Eye Care and Cure: 22 cm × 6 cm × 0.5 cm) has one row of convex (plus) lenses from 1 to 10 diopters arranged continuously so extra plus lens can be placed horizontally over the nonretinoscoped eye to achieve fogging. The rack appears like a yellow school bus with a millimeter ruler (Figure 1). One “wheel” has a −5 concave lens and the other a translucent occluder.
The retinoscopy technique presented the previously hidden school bus as a surprise (brought forward from a back pocket) and handed to the child asking if any older siblings ride a bus. Then, sitting behind the windows was demonstrated by the retinoscopist gently transferring the bus toward the child’s eye covering the nonscoped eye with adjacent, higher plus “windows.” The desired response was more “with” retinoscopy reflex 1–3 seconds looking through the skiascopy lens, and sliding the bus back and forth toward higher plus lenses watching for more “with” reflex and mydriasis accompany-relaxed accommodation. Neutralization required confirmation of astigmatism power and axis for the first eye. Then, the “bus” was reversed “to come home from school.” Often accommodation was already relaxed for the second eye as soon as the reversed-direction bus was in place (Supplementary video).
Since SBA-RS has just one row of integer-value plus spherical lenses, retinoscopy made liberal use of 1) adjusting the working distance to determine fractional refractive values for sphere and cylinder power and 2) sliding the bus back and forth to relax more accommodation uncovering more hyperopia. For higher myopic patients, the concave −5 lens in one of the “bus wheels” was utilized. Utilizing this simple device, the single −5 lens and the +1 through +10 convex lenses, sphero-cylinder refraction could be determined with a range from −10D to +8.5D. For the extremely high hyperopic patients, the SBA-RS was checked by holding an additional +12 lens to allow fogging when refracting through the +10 lens.
Patients undergoing initial or follow-up comprehensive ophthalmic examination were screened with SBA-RS before retinoscopy with our “gold-standard” cycloplegia at least 20 mins following instillation of cyclopentolate 1%. For objective comparison, many of the patients also had Retinomax automated refraction before cycloplegic refraction. Data were collected regarding age, indication for examination and neurodevelopmental delay such as autism, syndrome, attention-deficit hyperactivity disorder (ADHD), fetal alcohol syndrome (FAS), etc. The clinician performing the cycloplegic examination mainly used phoropter with refinement and was usually not aware of the Retinomax findings at the time of the refraction.
Refractive values were organized to afford the best comparison. Spherical equivalent was sphere plus 0.5× cylinder power in plus format. Power vectors for astigmatism (J0 Horizontal Jackson-Cross and J45 oblique Jackson-Cross) were calculated by (J0) = [−(Ksteep−Kflat)/2] × cos2α and (J0) = [−(Ksteep−Kflat)/2] × cos2α where K represents cylinder power and alpha (α) the axis in radians.18 We classified cases of hyperopia as those whose cycloplegic spherical equivalent exceeded 0.7 diopters and those with astigmatism as those whose plus cylinder power exceeded 0.7 diopters. Bland-Altman analysis and interclass correlation coefficient (ICC) were determined for these refractive values.
Correlations were assessed by linear regression with Spearman product moment coefficient. Medians between groups were compared with Mann–Whitney test. Proportions were compared with Chi-square test. A probability of 0.05 was considered significant.
Sample size calculation for linear regression with 2 predictors: statistical power level 0.9, probability level 0.01, and the anticipated effect size of 0.05 indicate a minimal sample size of 351.
Results
Refractions by both SBA-RS and cycloplegic retinoscopy techniques were completed by 470 patients age 0.3–60.3, median 5.99 years. Retinomax autorefraction was also completed by 184. There were 238 younger children aged 0.3–6.0 years of whom 99 were infants aged 4–30 months, 42 were toddlers aged 31–48 months and 97 were preschool aged 49–60 months.9 Indication for referral or examination of the younger children included strabismus 62, photoscreen refer 56, retinopathy of prematurity follow-up 15, refraction/amblyopia 14, developmental delay new referral 13, and tear duct/ptosis 8 with 70 miscellaneous. The number with various types of developmental delay was 110.
Table 1 shows compared refractive values between SBA-RS and Retinomax versus cycloplegic refraction. The spherical equivalent hyperopia (median with 90% CI). for the SBA-RS separated by neurologic status: delays +2.50 (+0.50,+5.83) and normals +2.50 (+0.43,+7.00) were not significantly different (Mann–Whitney z=1.55, p=0.12). The median value with 90% CI for astigmatic patients with cylinder power in both eyes combined with cycloplegic refraction was +1.75 D (+0.75,+4.50), for SBA-RS +1.50 D (+0.25,+4.00) and for Retinomax +2.00 D (+0.25, +4.64). When SBA-RS and Retinomax refractive components were compared to cycloplegic refraction, Retinomax differed substantially for spherical equivalent, J0 vector and J45 vector for the right eye. SBA-RS was slightly less than cycloplegic refraction in the right eye only for cylinder power and J0 vector.
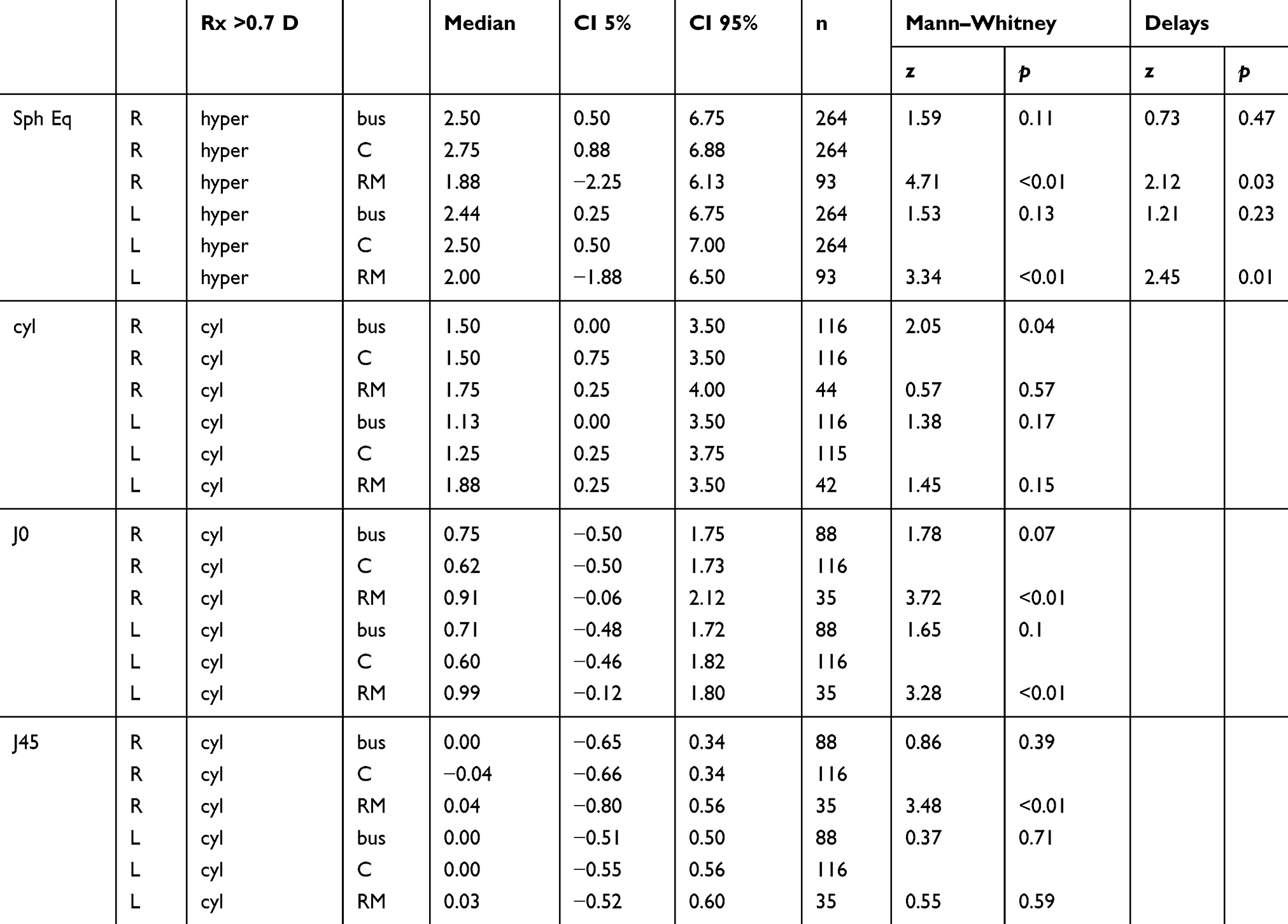 |
Table 1 Compared refractive values for spherical equivalent (Sph Eq) hyperopia (hyper) and astigmatism (cyl) greater than 0.7 diopters for right eye and left eyes (R and L). Median and 90% CIs are given. Medians compared between SBA-RS and cycloplegic refractions (bus and C; upper of each Mann–Whitney z value) and Retinomax compared to cycloplegic refraction (RM and C; lower of each z with p= probability). Patients with developmental delays compared for impact on relaxing accommodation |
Table 2 gives the relevant slope and intercept parameters for linear regression with cycloplegic refraction (ordinate) versus SBA-RS and Retinomax (abscissa). Included are CIs for slope allowing comparison with ideal unity line and Pearson product-moment correlation. Figure 2 shows how SBA-RS is closer to unity for spherical equivalent compared to Retinomax. Figure 3 shows the similarity for spherical equivalent SBA-RS separated into linear fits for hyperopia >0.7D and also separated by developmental delays versus normals. Figure 4 shows astigmatic plus cylinder power, Figure 5 shows J0 power vector, and Figure 6 shows J45 power vector, revealing that the SBA-RS is a bit closer to unity line than Retinomax. Figures 7 and 8 show Bland–Altman plots of refractive components J0 vector and J45 vector comparing SBA-RS with cycloplegic retinoscopy for patients with greater than 0.7 diopters cylinder. ICC for J0 vector was 0.39 (from 0.01 to 0.72) and for J45 vector −0.03 (from −0.11 to 0.06).
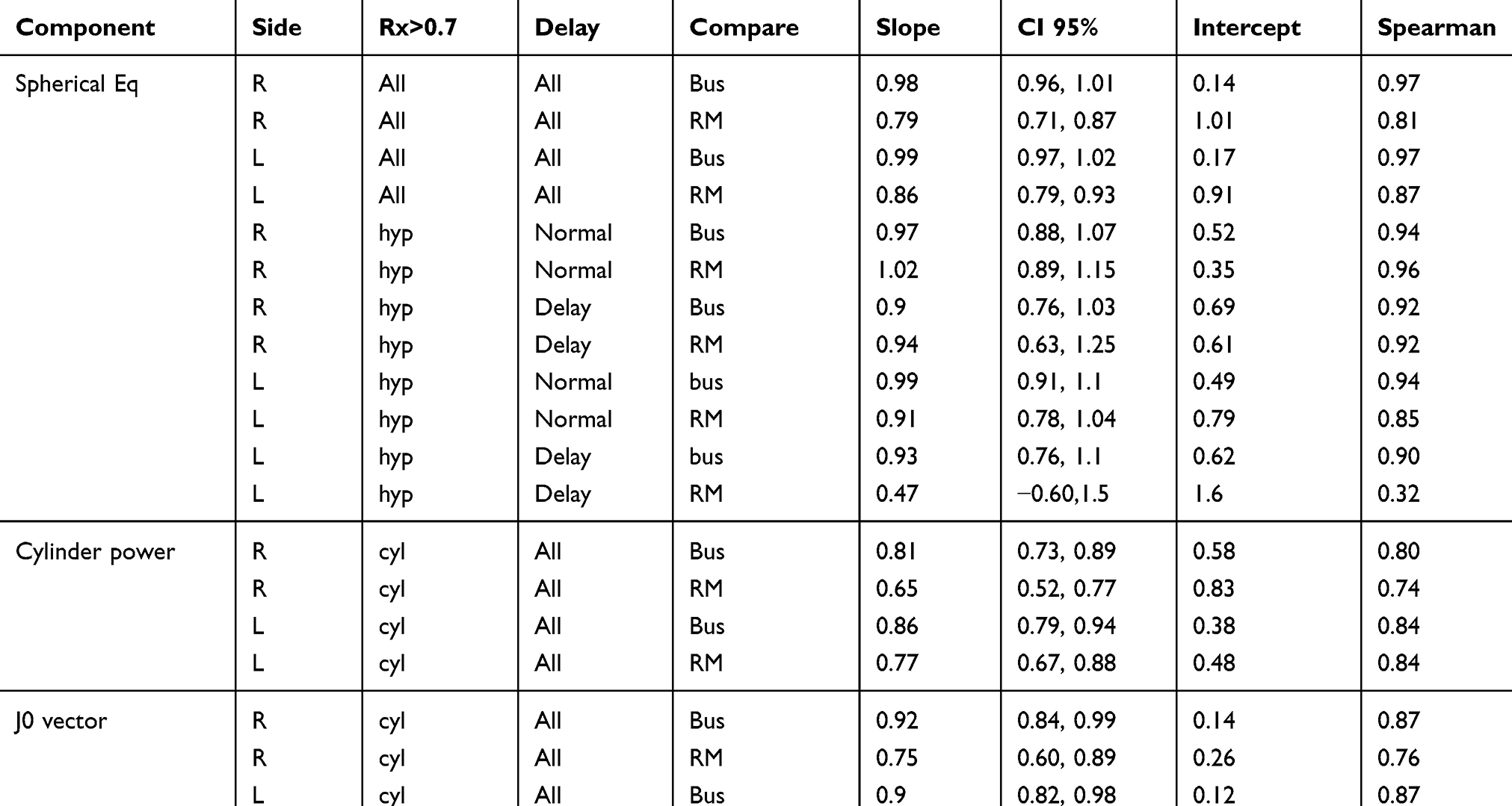 |
Table 2 Regressions: For each refractive component comparing a noncycloplegic screen with either bus (SBA-RS) or Retinomax with cycloplegic actual refraction. Refractive values of hyperopia (hyp) and astigmatism (cyl) sorted to those greater than 0.7 diopters (Rx>0.7) |
Figure 9 shows two receiver operating characteristic (ROC) curves with SBA-RS screening for amblyopia risk factors (ARF) by AAPOS preschool 200319 and age-stratified 20139 uniform guidelines. SBA-RS by 2003 guidelines with prescreening probability of ARFs of 71% achieved 92% sensitivity and 94% specificity. With 2013 guidelines, SBA-RS had 86% sensitivity and 76% specificity. Retinomax with prescreening probability 56% had lower validity: 81% sensitivy/71% specificity by 2003 guidelines and 77% sensitivity/75% specificity by 2013 guidelines.
Table 3 shows the proportion of SBA-RS and Retinomax refractive readings that differed from cycloplegic by more than 1 diopter for spherical equivalent and astigmatic cylinder power, and by more than 10° cylinder axis. Chi-square calculations indicate that the discrepancy from cycloplegic was greater for Retinomax than for SBA-RS.
 |
Table 3 Discrepancies between SBA-RS and Retinomax for spherical equivalent more than 1D diffference (sphEq), astigmatism cylinder power more than 1 diopter (cyl) and astigmatism axis beyond 10° (axis). Chi-square value z and probability p |
Conclusion
For normal and developmentally delayed patients, dry SBA-RS closely resembled cycloplegic refraction in terms of sphere and cylinder. The performance was slightly better than noncycloplegic Retinomax. In terms of estimating cycloplegic hyperopia, SBA-RS underestimated it by about 6%, whereas Retinomax underestimated cycloplegic hyperopia by about 26%.
Retinoscopy can be difficult in uncooperative children and developmentally delayed adults. A major hurdle is surmounted if the patient accepts trial lenses to be held in front of the eye for a moment of retinoscopy; we still had a few (n=25) patients who objected to the school bus in front of their eyes. However, we noted very similar linear regression for SBA-RS versus cycloplegic retinoscopy for the majority of our developmentally delayed patients because many participated with the child-friendly design.
True refraction can be estimated in several ways, but several modern methods require patient participation with the face held close to a table-top instrument. Subjective refraction may be slightly less reliable than automated refraction in adults,20 but cooperation is required. Retinomax is considered highly reliable and was used to perform uniform cycloplegic endpoints for MEPEDS and BPEDS.17 For children and young adults with latent hyperopia, cycloplegia offers the gold-standard method of estimating hyperopia. Cyclopentolate is clinically practical but painful with 1 day of mydriasis and blur.4 Some patients may require several days pre-examination dilation with atropine prolonging blur and photosensitivity even if the drop is less painful.21 Mydriasis and cycloplegia alter the optics of the eye; many patients have better acuity with under-plus spectacles compared to full cycloplegia and mydriasis, especially in patients for whom full plus is not required to treat accommodative esotropia.
Dynamic retinoscopy induces accommodation, while the pupillary reflex is observed.22 Fogging with a plus lens over the contralateral eye is effective in relaxing accommodation in cooperative patients. Fogging with a +2 lens on Grand Seiko binocular autorefractometer successfully relaxed accommodation in young adults similar to cyclopentolate.23 SBA-RS seems to offer a practical reversing effect to dynamic retinoscopy- and the two techniques can be used interchangeably.
If SBA-RS is able to uncover a sufficient portion of true hyperopia for a patient with a given presentation, the retina still needs to be examined. Current nonmydriatic cameras and small-pupil indirect ophthalmoscopes24 offer better alternatives to mydriasis than was available previously.
Strengths of the study include ample numbers to detect small differences and high prevalence of young patients with developmental challenges. The study benefitted from a large number of photoscreening and strabismus referrals. The vast majority of cycloplegic refractions was done by an experienced pediatric ophthalmologist refined with a phoropter. The new skiascopy rack was compared to state-of-the-art handheld autorefractor. Astigmatism was compared using the method consistent with Alpins.25
Weaknesses of the study include only partial blinding of the solo confirmatory retinoscopist to the screening values. This was not a community screening study but instead had enhanced prescreening probability. Cycloplegia was produced with a single instillation of cyclopentolate recognizing that repeat instillation of cyclopentolate or atropine may uncover even more hyperopia. We failed to carefully document the time of examination as if cycloplegia was avoided.
Cycloplegia remains the gold standard for comprehensive eye examinations especially when esotropia is suspected. For children and developmentally delayed adults, the SBA-RS technique may have a beneficial role when cooperation or examination time is at a premium.
 |
Figure 1 The school bus accommodation-relaxing skiascopy (SBA-RS) technique being utilized by author RWA in a remote Burma clinic demonstrating a higher plus lens over the nonstreaked eye to produce fogging effect (written informed parental consent given to share photo). |
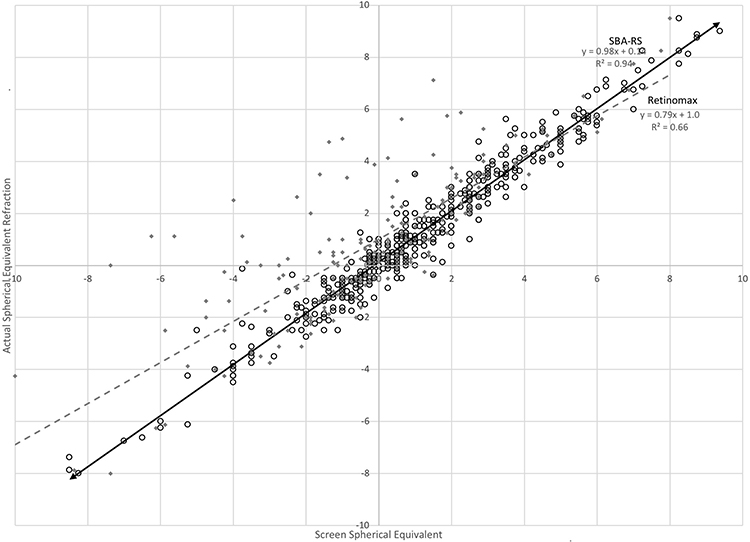 |
Figure 2 Linear regression for spherical equivalent comparing two screening methods (abscissa) SBA-RS (open black circles and solid black regression line) and Retinomax (solid gray diamonds with dashed gray regression line) compared to cycloplegic refraction in diopters (ordinate). |
 |
Figure 3 Linear regressions for SBA-RS versus cycloplegic spherical equivalent refraction for patients with and without developmental delays separating those with hyperopia (spherical equivalent greater than 0.7 D). |
 |
Figure 4 Linear regression for astigmatism cylinder power comparing two screening methods (abscissa) SBA-RS (open black circles and solid black regression line) and Retinomax (solid gray diamonds with dashed gray regression line) compared to cycloplegic refraction in diopters (ordinate). |
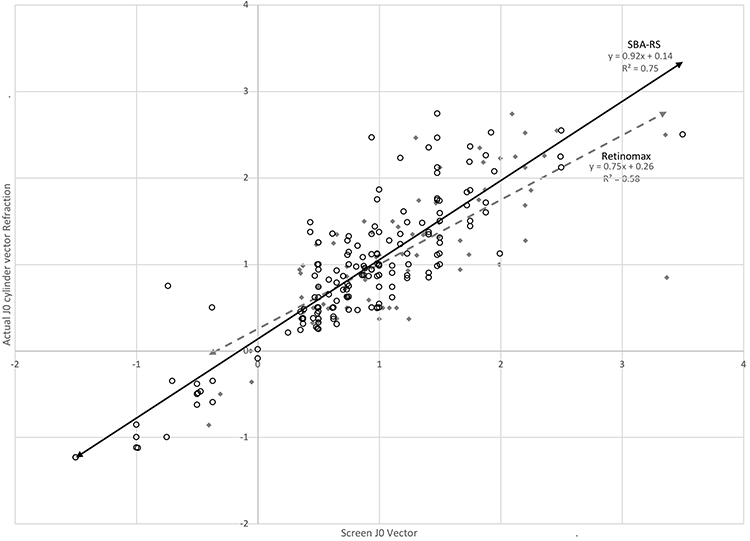 |
Figure 5 Linear regression for astigmatism J0 vector comparing two screening methods (abscissa) SBA-RS (open black circles and solid black regression line) and Retinomax (solid gray diamonds with dashed gray regression line) compared to cycloplegic refraction in diopters (ordinate). |
 |
Figure 6 Linear regression for astigmatism J45 vector comparing two screening methods (abscissa) SBA-RS (open black circles and solid black regression line) and Retinomax (solid gray diamonds with dashed gray regression line) compared to cycloplegic refraction in diopters (ordinate). |
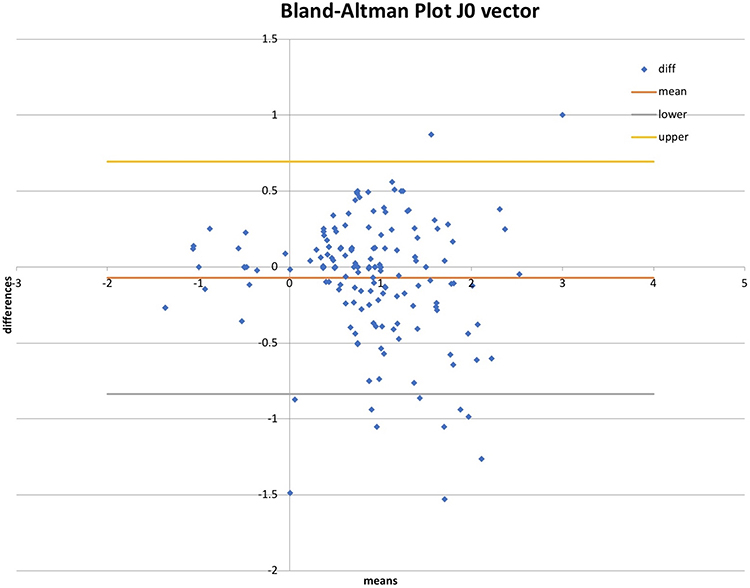 |
Figure 7 Bland–Altman plot comparing patients with astigmatism 0.75 and greater measured by school bus accommodation relaxing skiascopy (SBA-RS) and cycloplegic refraction for J0 vector. |
 |
Figure 8 Bland–Altman plot of J45 vector for patients with astigmatism 0.75 diopters and greater measured with SBA-RS compared to cycloplegic refraction. |
 |
Figure 9 Receiver operating characteristic (ROC) curve for screening cycloplegic refractive amblyopia risk dactors (ARF) with school bus accommodation-relaxing skiascopy (SBA-RS, black) and Retinomax (gray). Two published uniform gold-standard guidelines from the American Association for Pediatric Ophthalmology and Strabismus (AAPOS) 2003 (solid squares) and age-stratified from 2013 (dashed circles). |
Data sharing statement
Data can be obtained from http://www.abcd-vision.org/references/2WIN%20Bus%20de-identified%209-6-18.pdf.
Acknowledgment
This paper was presented as the poster at the annual meeting of the American Association for Pediatric Ophthalmology and Strabismus (AAPOS), San Diego 3/2019.
Disclosure
Robert W Arnold coordinates the Alaska Blind Child Discovery which has received discounted vision screen technology from several vendors. He serves unpaid on advisory boards for several photoscreeners. He is on the boards of PDI Check that makes vision screen game for Nintendo 3DS and also for Glacier Medical Software that markets ROP Check NICU cloud-based monitoring software. He is also an investigator and protocol developer for PEDIG. Dr Arnold also has a patent pending with PDI Check. No author has a financial stake in SBA-RS from Eye Care and Cure. The authors report no other conflicts of interest in this work.
References
1. Wallace DK, Morse CL, Melia M, et al. Pediatric eye evaluations preferred practice pattern(R): I. vision screening in the primary care and community setting; II. comprehensive ophthalmic examination. Ophthalmology. 2018;125(1):P184–P227. doi:10.1016/j.ophtha.2017.09.032
2. Shah P, Jacks AS, Adams GG. Paediatric cycloplegia: a new approach. Eye (Lond). 1997;11(Pt 6):845–846. doi:10.1038/eye.1997.216
3. Sutherland MS, Young JD. Does instilling proxymetacaine before cyclopentolate significantly reduce stinging? The implications of paediatric cycloplegia. Br J Ophthalmol. 2001;85(2):244–245. doi:10.1136/bjo.85.2.238g
4. Fan DS, Rao SK, Ng JS, Yu CB, Lam DS. Comparative study on the safety and efficacy of different cycloplegic agents in children with darkly pigmented irides. Clin Exp Ophthalmol. 2004;32(5):462–467. doi:10.1111/j.1442-9071.2004.00863.x
5. Mohan K, Sharma A. Optimal dosage of cyclopentolate 1% for cycloplegic refraction in hypermetropes with brown irides. Indian J Ophthalmol. 2011;59(6):514–516. doi:10.4103/0301-4738.86329
6. Rosenbaum AL, Bateman JB, Bremer DL, Liu PY. Cycloplegic refraction in esotropic children. Cyclopentolate versus atropine. Ophthalmology. 1981;88(10):1031–1034. doi:10.1016/s0161-6420(81)80032-2
7. Silva PS, Cavallerano JD, Tolls D, et al. Potential efficiency benefits of nonmydriatic ultrawide field retinal imaging in an ocular telehealth diabetic retinopathy program. Diabetes Care. 2014;37(1):50–55. doi:10.2337/dc13-1292
8. Gomez-Ulla F, Alonso F, Aibar B, Gonzalez F. A comparative cost analysis of digital fundus imaging and direct fundus examination for assessment of diabetic retinopathy. Telemed J E Health. 2008;14(9):912–918. doi:10.1089/tmj.2008.0013
9. Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013;17(1):4–8. doi:10.1016/j.jaapos.2012.09.012
10. Arnold RW. Amblyopia risk factor prevalence. J Pediatr Ophthalmol Strabismus. 2013;50(4):213–217. doi:10.3928/01913913-20130326-01
11. McClelland JF, Saunders KJ. Accommodative lag using dynamic retinoscopy: age norms for school-age children. Optom Vis Sci. 2004;81(12):929–933.
12. Silbert DI, Matta NS, Andersen K. Plusoptix photoscreening may replace cycloplegic examination in select pediatric ophthalmology patients. J AAPOS. 2013;17(2):163–165. doi:10.1016/j.jaapos.2012.11.008
13. Hunter DG. Dynamic retinoscopy: the missing data. Surv Ophthalmol. 2001;46(3):269–274.
14. VIPS. Comparison of preschool vision screening tests as administered by licensed eye care professionals in the vision in preschoolers study. Ophthalmology. 2004;111(4):637–650. doi:10.1016/j.ophtha.2004.01.022
15. O’Brien J, Bannon R. The fogging method of refraction. Am J Ophthalmol. 1948;31(11):1453–1459. doi:10.1016/s0002-9394(48)91809-1
16. Ying GS, Maguire M, Quinn G, Kulp MT, Cyert L. ROC analysis of the accuracy of Noncycloplegic retinoscopy, Retinomax Autorefractor, and SureSight Vision Screener for preschool vision screening. Invest Ophthalmol Vis Sci. 2011;52(13):9658–9664. doi:10.1167/iovs.11-8559
17. MEPEDS, Varma R, Deneen J, et al. The multi-ethnic pediatric eye disease study: design and methods. Ophthalmic Epidemiol. 2006;13(4):253–262. doi:10.1080/09286580600719055
18. Miller JM. Clinical applications of power vectors. Optom Vis Sci. 2009;86(6):599–602. doi:10.1097/OPX.0b013e3181a6a211
19. Donahue S, Arnold R, Ruben JB. Preschool vision screening: what should we be detecting and how should we report it? Uniform guidelines for reporting results from studies of preschool vision screening. J AAPOS. 2003;7(5):314–316. doi:10.1016/S1091853103001824
20. Bullimore MA, Fusaro RE, Adams CW. The repeatability of automated and clinician refraction. Optom Vis Sci. 1998;75(8):617–622.
21. Arnold RW, Gionet E, Hickel J, Owen M, Armitage MD. Duration and effect of single-dose atropine: paralysis of accommodation in penalization treatment of functional amblyopia. Binocul Vis Strabismus Q. 2004;19(2):81–86.
22. Guyton DL, O’Connor G. Dynamic retinoscopy. Binocul Vis Eve Muscle Surg Q. 1994;9(1):15–17.
23. Queirós A, Jorge J, Gonzáles-Méijome J. Influence of fogging lenses and cycloplegia on peripheral refraction. J Optom. 2009;2(2):59–100. doi:10.3921/joptom.2009.83
24. Woldoff HS, Stumpf JG. A small pupil binocular indirect ophthalmoscope. Ann Ophthalmol. 1978;10(2):138–142.
25. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg. 2001;27(1):31–49. doi:10.1016/s0886-3350(00)00798-7
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.