Back to Journals » Nature and Science of Sleep » Volume 9
Schizophrenia and sleep disorders: links, risks, and management challenges
Authors Kaskie RE, Graziano B, Ferrarelli F
Received 6 July 2017
Accepted for publication 24 August 2017
Published 21 September 2017 Volume 2017:9 Pages 227—239
DOI https://doi.org/10.2147/NSS.S121076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Steven Shea
Rachel E Kaskie,1 Bianca Graziano,2 Fabio Ferrarelli1
1Department of Psychiatry, University of Pittsburgh, Pittsburgh, PA, USA; 2Department of Health Sciences, Università degli Studi di Milano, Milan, Italy
Abstract: Schizophrenia is a major psychiatric disorder that has a massive, long-lasting negative impact on the patients as well as society. While positive symptoms (i.e., delusions and hallucinations), negative symptoms (i.e., anhedonia, social withdrawal), and cognitive impairments are traditionally considered the most prominent features of this disorder, the role of sleep and sleep disturbances has gained increasing prominence in clinical practice. Indeed, the vast majority of patients with schizophrenia report sleep abnormalities, which tend to precede illness onset and can predict an acute exacerbation of psychotic symptoms. Furthermore, schizophrenia patients often have a comorbid sleep disorder, including insomnia, obstructive sleep apnea, restless leg syndrome, or periodic limb movement disorder. Despite accumulating data, the links between sleep disorders and schizophrenia have not been thoroughly examined, in part because they are difficult to disentangle, as numerous factors contribute to their comorbidity, including medication status. Additionally, sleep disorders are often not the primary focus of clinicians treating this population, despite studies suggesting that comorbid sleep disorders carry their own unique risks, including worsening of psychotic symptoms and poorer quality of life. There is also limited information about effective management strategies for schizophrenia patients affected by significant sleep disturbances and/or sleep disorders. To begin addressing these issues, the present review will systematically examine the literature on sleep disorders and schizophrenia, focusing on studies related to 1) links between distinct sleep disorders and schizophrenia; 2) risks unique to patients with a comorbid sleep disorder; and 3) and management challenges and strategies.
Keywords: psychosis, sleep disturbances, insomnia, obstructive sleep apnea
Introduction
Schizophrenia is a severe psychiatric disorder that affects less than 1% of the population worldwide, and represents an immense burden for the patients and the entire society.1 Schizophrenia is characterized by positive symptoms, including hallucinations, delusions, and disorganized behavior; negative symptoms, such as social withdrawal, apathy, and affective flattening; as well as a variety of cognitive impairments.2 Although sleep disturbances are not included in the diagnostic criteria for schizophrenia, they are consistently reported in those patients. Similarly, while research in schizophrenia has primarily and traditionally focused on waking-related abnormalities, sleep has been increasingly studied in schizophrenia populations and consistently found to be disturbed.
Sleep and sleep disorders can be studied and assessed in a variety of ways. Self-report questionnaires are commonly used in sleep research and assess general sleep quality, like the Pittsburgh Sleep Quality Index3 and Epworth Sleepiness Scale.4 Questionnaires can also determine risk for specific sleep disorders, such as the STOP-BANG for obstructive sleep apnea (OSA).5 While not diagnostic tools per se, these questionnaires are important for determining whether further assessments are needed. Other methods can more objectively assess sleep, such as polysomnography (PSG) and actigraphy, and can be useful in revealing sleep disturbances of which patients may not be fully aware. More recently, the availability of high-density (hd)-electroencephalogram (EEG) (e.g., 64–256 channels) has allowed characterization of differences in sleep-specific rhythms, such as slow waves and sleep spindles, between healthy and psychiatric populations, including schizophrenia.6,7
Disrupted sleep appears to be closely tied to schizophrenia, and it is often observed in individuals even prior to illness onset. Specifically, disturbed sleep, with insomnia being the most frequent sleep disturbance, has been found to be the most commonly reported symptom during the prodromal phase of illness, which is characterized by a wide range of unspecific, diagnostically-inconclusive symptoms.8–10 In addition to self-reports of poor sleep quality, objective sleep abnormalities have been observed in clinical high risk (CHR) subjects using PSG, including increased sleep disruptions.11,12 Alongside other symptoms, disturbed sleep has even been found to be a predictive factor in determining who, among those at high risk, will develop psychosis.13 Among those diagnosed with schizophrenia, poor sleep quality has been observed in the majority of patients.14 In patients with chronic schizophrenia, sleep continuity and architecture are significantly different from healthy populations – something that has also been observed in young patients with childhood-onset schizophrenia. Furthermore, sleep disturbances appear to be related to symptom severity.15,16 Based on these findings, it is clear that sleep dysfunction is an important aspect of schizophrenia, and for some patients, sleep abnormalities may meet diagnostic criteria for a sleep disorder. Indeed, increased rates of OSA, restless leg syndrome (RLS), periodic limb movement disorder (PLMD), and circadian rhythm dysfunction have been observed in schizophrenia patients. Thus, the relationships between schizophrenia and sleep disorders, including their links, risks, and possible management, are a highly relevant topic for both research and clinical purposes. Nonetheless, the evidence about these relationships has not been previously, comprehensively reviewed.
In this article, we will review findings from studies investigating the links between schizophrenia and a variety of sleep disorders. We will also present the risks that individuals with schizophrenia may face in developing or coping with a comorbid sleep disorder. Finally, we will discuss the challenges that both health care providers and patients face in treating sleep disturbances and schizophrenia, and suggest possible strategies to effectively manage these comorbid conditions.
Methods
We conducted an online literature search using the MEDLINE database. We considered original research identified using the search terms “(schizophreni*) AND (sleep disturbance* OR sleep disorder* OR insomnia).” Record titles and abstracts were screened; review articles, articles not written in English, case studies, and articles unrelated to sleep disorders or schizophrenia were excluded. The remaining articles were evaluated for their relevance in identifying schizophrenia and sleep disorders links, risks, and management. Figure 1 details the process of review and selection.
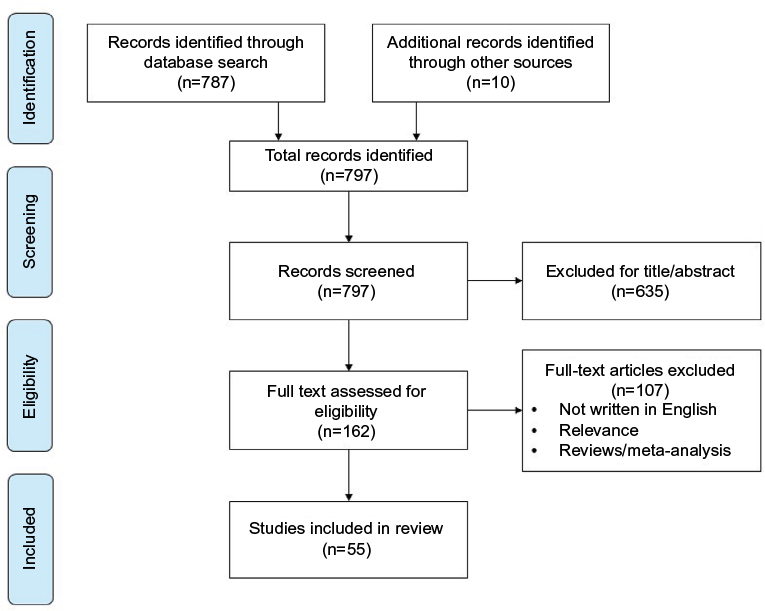 | Figure 1 PRISMA diagram detailing the literature search and review process. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Results
The specified search yielded 787 articles, and an additional eight were identified through other sources. After assessing all articles for eligibility, a total of 54 studies related to schizophrenia and sleep disorders were selected for inclusion. Table 1 summarizes the results of these studies.
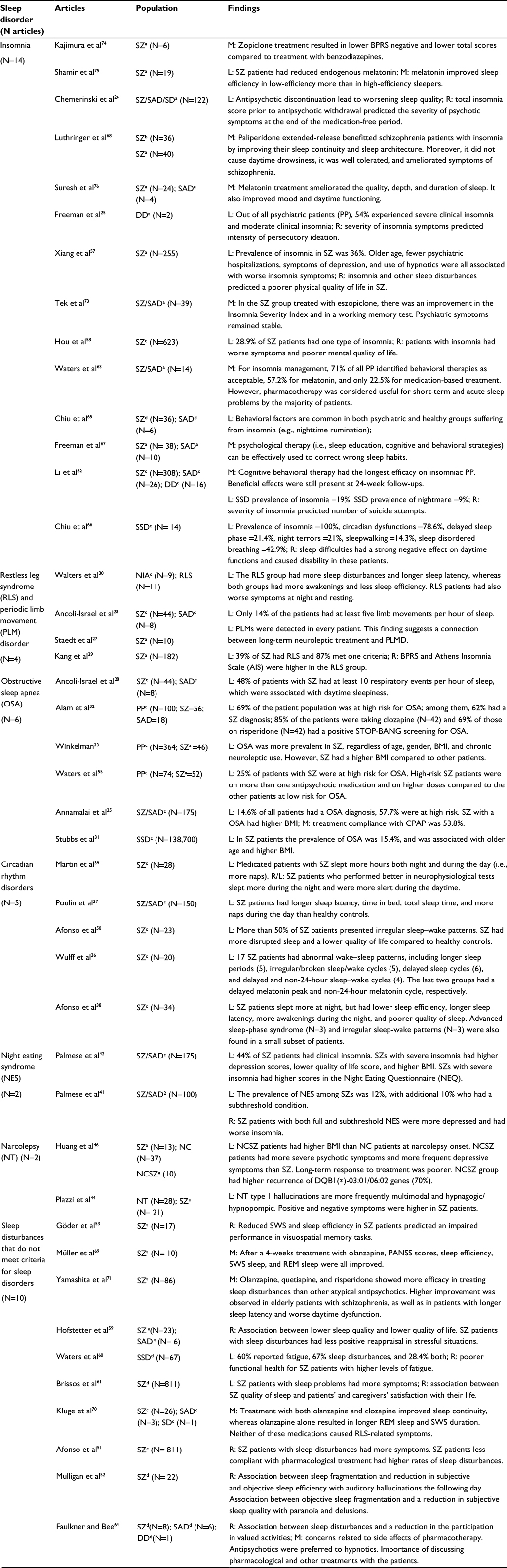 | Table 1 Notes: aTreated, buntreated, ccombination, dpartial or data absent. Abbreviations: BMI, body mass index; BPRS, Brief Psychiatric Rating Scale; CPAP, continuous positive airway pressure; DD, delusional disorder; NC, narcoleptic-cataplectic; NCSZ, narcoleptic-cataplectic schizophrenia; NIA, neuroleptic-induced akathisia; PANSS, Positive and Negative Syndrome Scale; PLMD, periodic limb movement disorder; REM, rapid eye movement; SAD, schizoaffective disorder; SD, schizophreniform disorder; SSD, schizophrenia spectrum disorder; SWS, slow-wave sleep; SZ, schizophrenia; L, links; R, risks; M, management. |
Links
Insomnia
Schizophrenia and insomnia frequently co-occur. Insomnia has been found to be a risk factor for development of mood disorders, and patients with schizophrenia often experience severe insomnia, including prior to onset of a psychotic episode.17–19 It has been suggested that dysfunction of dopamine D2 receptors underlie this clinical observation. Specifically, the overactivity of D2 receptors in the striatum has been associated to the positive symptoms of schizophrenia and may also result in increased wakefulness, ultimately leading to insomnia.20 The importance of dopamine in sleep–wake regulation is also suggested by animal experiments. Mice exposed to high levels of dopamine developed REM-like electrophysiological patterns during waking hours, while dopamine-deprived mice showed electrophysiological brain activity resembling slow-wave sleep (SWS). This state is characterized by a partial inhibition of SWS and a total suppression of REM sleep, a condition from which mice can recover after treatment with D2 dopamine receptors agonists. Conversely, hyperdopaminergic mice recover from the REM-like activity intrusion during wakefulness when treated with haloperidol.21 Other studies have investigated dopamine’s effect on human sleep behavior. One study focused on the effect of the dopamine D1 antagonist NNC-687 on the sleep behavior of a group comprised of 20 healthy young males. Sleep recordings were performed after administering a placebo or different doses of the D1 antagonist for the night. This study showed that the effect of this medication was greatest in the first non-REM period, resulting in a duration 47% longer than during baseline. D1 antagonist increased spindles (total number, incidence, and burst duration) and delta waves activity (reduced peak amplitude but increased their instantaneous frequency).22 Nearly all antipsychotic medications (APs) are, at least in part, D2 receptor antagonists, making them successful in treating positive symptoms by lowering the overactivity of these receptors and preventing the binding of dopamine.23
While APs are often effective in the treatment of the positive symptoms of schizophrenia, many patients fail to adhere to their prescribed medication regimen. Intriguingly, abrupt discontinuation of APs leads to a progressive deterioration of sleep quality. For those individuals who experience insomnia prior to discontinuation, the severity of insomnia is strongly associated with severity of psychotic symptoms after discontinuation.24 Such findings suggest that schizophrenia patients with sleep disturbances are at a greater risk of developing severe psychotic symptoms following APs discontinuation than those without prior sleep disturbances and might benefit from treating insomnia alongside schizophrenia. Further supporting the role of insomnia in development and/or exacerbation of psychosis, a study in the general population found a strong correlation between insomnia and paranoid thinking.25
RLS and PLMD
Though APs may ameliorate some of the sleep disturbances observed in schizophrenia, they might also induce or exacerbate others. RLS and PLMD are sleep movement disorders characterized by a distressing desire to move the legs and other limbs during sleep, respectively, that ultimately leads to deteriorated sleep quality. As both RLS and PLMD respond to dopamine agonists, a dopamine deficiency is a component of their pathophysiology. Unfortunately, APs’ efficacy lies with their action of blocking D2 receptors and may contribute to or exacerbate RLS and PLMD.26 One study investigated the presence of periodic limb movement during sleep in 10 patients with chronic schizophrenia, who were under neuroleptic therapy for a mean of 27 years. In all 10 patients, insomnia related to limb movement was detected, consistent with a relationship between long-term neuroleptic therapy and PLMD occurrence.27 However, in a study of late-life psychosis, only a small proportion (7 of 52 patients) had a myoclonus index greater than 5, which would qualify for a diagnosis of PLMD. Furthermore, there was no significant difference in age, neuroleptic use, or duration of neuroleptic treatment between those with PLMD and those without, thus suggesting that the role of APs in PLMD needs to be further investigated.28
In a study on RLS in schizophrenia, the prevalence of RLS in 182 APs treated schizophrenia patients was investigated and compared to 108 healthy comparison subjects. The incidence of RLS as well as the prevalence of RLS symptoms was significantly higher in the schizophrenia group (21.4% and 47.8%) relative to the control group (9.3% and 19.4%, respectively). Among schizophrenic patients, those with RLS showed more anxiety, depressive and thinking disturbance symptoms. A relationship between RLS and insomnia was also found. However, within the schizophrenia group there was no significant difference in age, duration of illness, cumulative exposure to neuroleptics, dose, or combination of therapy between those diagnosed with RLS and those who were not.29
Neuroleptic-induced akathisia is a medication-induced movement disorder that can closely resemble RLS. Distinguishing those conditions can be challenging in schizophrenic patients. In a sleep study, a group of patients with neuroleptic-induced akathisia was compared to a group of patients with idiopathic RLS. Although both of these conditions were characterized by an increased number of awakenings and decreased sleep efficiency, in neuroleptic-induced akathisia sleep disturbances were milder. In addition, patients with neuroleptic-induced akathisia tend to experience inner restlessness, whereas for RLS patients it is more common to experience leg paresthesia as well as worsening of symptoms at night and while resting.30
OSA
Numerous studies indicate that OSA is strongly associated with schizophrenia, with a meta-analysis reporting a prevalence of 15.4% in these patients.31 One study in patients with severe mental illness treated at a primary care clinic found that 69% had high scores for the STOP-BANG, a screening questionnaire for OSA, and among this group 62% had a diagnosis of schizophrenia.32 Another study found that among schizophrenia patients referred to a sleep clinic while hospitalized in a psychiatric inpatient unit, nearly half met criteria for OSA.32 Age, gender, body mass index (BMI), and chronic neuroleptic use all have a significant independent effect on the presence of OSA in psychiatric patients, with the schizophrenic group having significantly higher BMI and increased rates of sleep apnea.33
Obesity is a likely factor responsible for the association between schizophrenia and OSA. Excessive weight gain is a common side effect of APs, and both genetically determined and medication-induced obesity can lead to OSA. In addition to AP-related weight gain, schizophrenia patients have poorer physical health than the general population.34 In a study of 175 outpatients with schizophrenia, a high prevalence of OSA (14%) was observed. BMI was found to be significantly higher in those patients diagnosed with OSA when compared with those without an OSA diagnosis.35 Another study investigated an elderly schizophrenia group (N=44), since the prevalence of sleep-disordered breathing tends to increase with age. Forty-eight percent of these patients had 10 respiratory events per hour of sleep and reported more daytime sleepiness compared to a small group (N=8) of seasonal affective disorder patients, although these symptoms were unrelated to their BMI.28
Circadian rhythm disorders
Circadian rhythm disorders are characterized by a persistent or recurrent pattern of sleep disruption, which results from an alteration of the circadian system or a misalignment between the endogenous circadian rhythm and the sleep–wake schedule required by an individual’s physical environment, social, or professional schedule.2 There are two main types of circadian rhythm disorders: a delayed phase type, in which the timing of the desired sleep period is significantly delayed, and an advanced phase type, in which one is unable to remain awake until the desired or socially accepted time. An irregular sleep–wake type, in which one has no discernible 24-hour sleep–wake cycle and may suffer from insomnia and daytime sleepiness, has also been reported.
Significant circadian rhythm disruption is well documented in patients with mental disorders, including schizophrenia. In one study utilizing actigraph recording, 20 schizophrenia patients were found to have significant disruptions, and half had severe circadian misalignment.36 In general, time spent asleep, time from sleep start to sleep end, as well as sleep latency were all increased in these patients.36,37 A subgroup of these patients showed a delayed phase shift, in which melatonin and physical activity peaked much later in the day, and timing of the sleep period was also delayed. Importantly, these findings were unrelated to having a daily routine, as all subjects in the patient and control groups were unemployed and did not follow a daily schedule. Another study also found disturbed sleep–wake patterns in schizophrenia, with patients sleeping more at night overall, but with poorer efficiency than healthy controls. A small subsample (N=6) of these patients was also found to have advance sleep phase syndrome and irregular sleep–wake rhythm.38 Disturbed circadian rhythm is affected by lifestyle, behavioral factors, and presence and intensity of psychiatric symptoms. It is also associated to medication status, as suggested by the observation that long treatment with high doses of APs was associated with weaker circadian rhythms in schizophrenia.39
Night eating syndrome
Night eating syndrome (NES), although not considered a sleep disorder, has been associated to both schizophrenia and sleep disturbances. NES, which is included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition under “Other Specified Feeding or Eating Disorder,” is characterized by evening hyperphagia, insomnia with awakenings followed by nocturnal eating, and morning hypophagia.2 NES disproportionately affects obese individuals, with a prevalence anywhere from 8.9% to 27% compared to 1.5% in the general population.40 NES has not been thoroughly researched in schizophrenia, but a handful of studies suggest that a greater proportion of schizophrenia patients may be affected. For example, a study of obese patients with schizophrenia and schizoaffective disorder found the rate of NES to be 12%.41 An additional 10% met criteria for subthreshold NES, whereas those who engaged in night eating behaviors were also found to suffer from increased insomnia and depression.41 Among patients with schizophrenia, those with clinical insomnia were more frequently affected by night eating syndrome and were more likely to be clinically obese.42
Narcolepsy
The links between narcolepsy and schizophrenia have been investigated by just a handful of studies. One of those, which assessed the frequency of narcolepsy with cataplexy in schizophrenia, screened 366 outpatients and found that only five patients were HLA DQB1*06:02 positive (an HLA haplotype found almost exclusively in those with narcolepsy-cataplexy type 1). Of these five patients, three underwent lumbar puncture and were found to have normal hypocretin-1 levels. The investigators concluded that narcolepsy with cataplexy is not an unrecognized disease in this patient population.43 Another study found that narcolepsy type 1 (NT1) and schizophrenia patients share some psychotic symptoms, which can be responsible for delayed diagnoses of either disorders, although hypnagogic/hypnopompic hallucinations and overall Positive and Negative Syndrome Scale (PANSS) score are the most distinctive clinical characteristics between these disorders.44 Furthermore, it was found that four patients with narcolepsy experienced psychotic symptoms (hallucinations) during treatment with sodium oxybate, and that hallucinations resolved in two of four patients following tapering of this medication.45 Finally, in a study investigating individuals with comorbid narcolepsy-catalepsy (N-C) with schizophrenia (study group) compared with subjects with either N-C (control group 1) or schizophrenia (control group 2) alone, the study group had higher BMI, weight at onset of narcolepsy, and higher frequency of DQ B1(∗)-03:01/06:02 antigens compared to the control groups, which was associated with longer persistence of severe psychotic symptoms.46
Risks
A diagnosis of schizophrenia is associated with increased risk for other health issues, such as greater likelihood of obesity and being a smoker. It also carries a higher risk of comorbidities, including developing sleep disorders like OSA.47 Having a sleep disorder, or sleep disturbances in general, carries its own health risks per se, and patients with both schizophrenia and sleep disturbances tend to have a poorer quality of life, more severe symptoms, higher mortality, and poorer outcome than those with either condition alone.26
Here we will focus on three main risks for patients with schizophrenia in relation to sleep disturbances: 1) experiencing worsening psychotic symptoms; 2) having a higher incidence of sleep disorders, especially OSA, than the general population; and 3) having a poorer quality of life in case of concurrent sleep disturbance or disorder.
Worsening psychotic symptoms with sleep disturbances
In individuals at high risk for psychosis and in those diagnosed with schizophrenia, several studies have found associations between sleep disturbances and symptom severity. In a study of adolescents at ultra-high risk for psychosis, those who displayed poorer sleep quality, as determined by increased wake time after sleep onset, more movements during sleep, and decreased sleep efficiency, had worsening positive symptoms after 12 months.48 Insomnia is thought to be a heralding sign of impending psychosis,24 whereas fragmented circadian rhythms in individuals at CHR for psychosis were associated with more severe psychotic symptoms, and could predict symptom severity 1 year later.49 Among patients diagnosed with schizophrenia, those with positive symptoms tend to have more disrupted sleep–wake patterns and worse quality of sleep,50 while those more compliant with APs treatment are less symptomatic.51 Objective and subjective sleep quality and efficiency can predict next-day symptom severity, including increased auditory hallucinations, paranoia, and delusions in chronic patients with schizophrenia.52 Moreover, a study showed that schizophrenia patients with sleep disturbances and weaker circadian rhythms had worse performance in neuropsychological tests.39 Abnormalities in sleep-specific EEG patterns are also related to selective deficits in learning and memory in schizophrenia. For example, a study showed a correlation also between the reduction in SWS and lower scores in a visuospatial memory test in chronic patients with schizophrenia, which underlines the important role of SWS in memory consolidation.53 There is also evidence that psychotic symptoms can lead to sleep disturbances. Specifically, psychotic experiences interfere with the ability to sleep well, and resulting sleep problems lead to daytime tiredness, thus impairing the ability of schizophrenia patients to cope with their psychotic symptoms.54
Higher incidence of sleep disorders, including OSA
A diagnosis of schizophrenia significantly increases the risk of developing a sleep disorder, especially OSA. For example, in a recent meta-analysis on the prevalence and predictors of OSA in individuals with severe mental illness, it was found that individuals with schizophrenia had higher prevalence (15.4%) compared to the general population (~5%), and that increased age and BMI were associated with higher rates of OSA.31 AP types and doses can also increase this risk for OSA. One study reported the proportion of schizophrenia patients at high risk for OSA based on the medication(s) being taken. Among APs, 85% of the patients who were taking clozapine had a positive STOP-BANG (i.e., a screening questionnaire for OSA risk), whereas 69% of those who were on risperidone, 36% of those taking olanzapine, and 25% on fluphenazine had positive STOP-BANG scores.32 While the proportion of patients who actually had OSA was not reported, such results suggest that certain medications may carry a greater risk for OSA than others. In another study, a smaller proportion of hospitalized patients with schizophrenia (25%) were classified as being at high risk of OSA, and these patients were taking a greater total number of medications and at higher doses than those at lower risk for OSA.55 Other sleep disorders, such as RLS, night eating syndrome, somnambulism, and rhythm disorders have been described as possible adverse effects of antipsychotics and should be considered in the differential diagnosis of disturbed or unrestful sleep in schizophrenia patients.56
Poorer quality of life with concurrent sleep disturbance or disorder
Patients with schizophrenia and concurrent sleep disturbances tend to have poorer quality of life, which is generally determined by assessing four domains: physical health, psychological well-being, social relationships, and environmental factors. A study of 255 chronic, stable patients with schizophrenia found that 36% had at least one type of insomnia, and these patients had significantly poorer quality of life, as measured by the World Health Organization Quality of Life Schedule-Brief, on all four domains.57 After adjusting for sociodemographic and clinical variables, however, only physical health remained significantly poorer in those with sleep disturbances. Insomnia, therefore, may be a significant independent factor in quality of life outcomes for schizophrenia. Another study reported a similar rate of insomnia (28.9%) in Chinese patients with schizophrenia and found that mental health, but not physical health, was significantly poorer in those with disturbed sleep.58 Quality of life and coping were also investigated in a study on 29 patients with schizophrenia or schizoaffective disorder. Data analysis showed that sleep quality was predictive of low quality of life and reduced use of positive reappraisal in stressful situations.59 Notably, fatigue has been associated with low functional health, whereas sleep disturbances themselves did not necessarily impact health.60 Schizophrenia patients with sleep disturbances also report significantly lower satisfaction with life, as do their caregivers, than those without sleep disturbances,61 and the presence of insomnia and comorbid nightmares in these patients has been associated with an increased risk for suicide attempts.62
Management
Challenges: reduced insight/compliance, individual biases
Numerous treatment options exist for sleep disorders, including pharmacotherapy, psychological, and behavioral interventions, but choosing a strategy to which patients with schizophrenia will adhere can be challenging, given the reduced insight and treatment compliance that characterize this patient population. A study of insomnia treatment in individuals with schizophrenia sought the perspective of the patients themselves to understand what they perceived to be the most helpful treatment and found that the majority of patients believed that pharmacotherapy was not an acceptable intervention, due to unwanted side effects and drug interactions; they also felt that constant adjustment in type or dose of medications negatively impacted their sleep.63 Cognitive and behavioral interventions were perceived more positively, but a group of patients were skeptical of their efficacy. Nonetheless, active engagement in the treatment process was viewed positively, as it could provide a sense of autonomy and control. Furthermore, some patients developed their own strategies to improve sleep, such as maintaining regular bedtimes and routines, which closely follow general recommendations for improving sleep.63,64 Overall, patients believed that there is no single treatment for insomnia that is ideal for everyone and that pharmacotherapy might be beneficial in some scenarios, such as for acute sleep problems. For insomnia, therefore, a discussion with patients about various treatments may help identify the best option and yield better outcomes.
Nonpharmacological interventions for sleep disturbances
It is likely that different subgroups of patients require different forms of treatment for sleep disturbances. For example, some patients with sleep disturbances and schizophrenia have negative cognitions associated with sleep, such as nighttime rumination, negative beliefs about the cause of sleep problems, overestimating the health impact of poor sleep, and lack of knowledge of sleep hygiene.65,66 These patients may require targeted psychological interventions to change cognitions surrounding sleep and improve sleep-related habits, rather than implementing a pharmaceutical intervention. Cognitive behavioral therapy has been shown to effectively treat insomnia in patients with schizophrenia, with treatment strategies including stimulus control and increasing daytime activity levels.67
Pharmacological treatment of disrupted sleep
Patients might be wary of pharmacotherapy for sleep problems, but medications can be an effective strategy to improve sleep. AP medications are being increasingly used to ameliorate sleep disturbances. For example, paliperidone, a second-generation AP medication, has been shown to improve sleep architecture in schizophrenic patients who complained of insomnia. This medication was well tolerated by patients and improved the symptoms of schizophrenia without causing drowsiness during the day.68 Olanzapine, another second-generation AP medication, has also demonstrated a positive effect on sleep efficiency, SWS sleep, and REM sleep,69 and in a more recent study olanzapine was shown to be superior to clozapine in improving sleep architecture (longer SWS and REM sleep), whereas both APs improved sleep continuity without inducing RLS symptoms.70 Switching from first-generation to second-generation APs has been found to have positive effects in schizophrenia, especially in elderly patients.71 Atypical antipsychotics, such as quetiapine, have also been shown to be effective in treating insomnia in patients with schizophrenia and are frequently prescribed by clinicians.72
Among hypnotic agents, it has been shown that eszopiclone, a nonbenzodiazepine sleep-inducing compound, can significantly improve insomnia in schizophrenia patients over placebo treatment, with psychiatric symptoms remaining stable throughout treatment.73 A study comparing the effects of zopiclone, another nonbenzodiazepine hypnotic agent, relative to benzodiazepines in schizophrenia patients showed a more beneficial effect of zopiclone on the sleep architecture and the severity of symptoms in these patients.74
Melatonin is a hormone made by the pineal gland that helps regulate the sleep and wake cycle in humans. Notably, one study assessing urinary melatonin output established a lower production of this hormone in schizophrenia patients relative to healthy controls.75 The same study also found that melatonin replacement improved sleep efficiency, and this improvement was more prominent in low-efficiency than high-efficiency sleepers. Melatonin is thought to improve the quality and the duration of sleep primarily by reducing the number of awakenings during the night. Also, it does not produce hangover effects in the morning and improves some symptoms, such as depressed mood, fatigue, and irritability, thus ameliorating daytime functioning.76 Furthermore, a study performed on patients with chronic schizophrenia showed that melatonin increased the first-night effect, which is usually observed in healthy subjects but it is absent in schizophrenia, thus suggesting that melatonin can enhance schizophrenia patients’ alertness and responsiveness in unfamiliar surroundings.77
Discussion
Based on the above-mentioned findings, it is clear that sleep disturbances afflict the vast majority of patients with schizophrenia, and that these disturbances often reach the level of clinical significance. It appears that insomnia most commonly occurs in schizophrenia patients, both prior to illness onset and throughout the course of the disease. Several factors may contribute to insomnia in these patients, including lack of daytime activity and routine, preoccupation with being able to fall and/or stay sleep, as well as intrusion of unwanted thoughts or hallucinations when trying to sleep. A variety of approaches may be successful in treating patients with insomnia. Cognitive behavioral therapy can address issues with engaging in enough activity during the day and adhering to a bedtime routine, whereas AP medications and hypnotic agents can facilitate falling/staying asleep and address acute episodes of insomnia, respectively. Regardless of the specific approach selected, increasing evidence suggests that patients should be actively engaged in the treatment process.
As previously reviewed, beside insomnia other sleep disorders can affect schizophrenia patients. OSA is observed in a greater proportion of schizophrenia patients compared to the general population. A variety of factors can account for this observation, including general health decline and reduced ability of schizophrenia patients to engage in self-care behaviors such as exercising and maintaining a healthful diet. Furthermore, weight gain is the strongest link to OSA, and several APs lead to unwanted weight gain. For this group of patients, clinicians can follow the standard of care to treat OSA. It is important to highlight that many studies suggest that those at risk for OSA may go unnoticed, and so it may be beneficial to implement screening for OSA and related sleep disorders more widely.
RLS and PLMD have also been reported in schizophrenia patients, though studies suggest that patients are not affected in greater numbers than the general population. APs may be responsible for these disorders, as they have an antagonistic effect on dopaminergic receptors. This assumption is supported by the observation that dopamine agonists, such as ropinirole and pramipexole, are the most effective treatment for RLS and PLMD. For these conditions, medication management may be most effective in providing patients with restful sleep.
In sum, in this article we have reviewed studies investigating schizophrenia and sleep disorders, including their links, risks, and possible management. While there is overwhelming evidence and sleep disturbances are pervasive in schizophrenia patients, and often contribute to an exacerbation of psychotic symptoms, the association between schizophrenia and specific sleep disorders has been far less explored. Among sleep disorders, insomnia is the most strongly associated with schizophrenia, whereas OSA and, to lesser extent, circadian sleep disorders and RLS/PLMD appear to be more represented in schizophrenia patients relative to the general population. Future studies will help confirming and extending these links in larger groups of patients, including medication-naïve and early-course schizophrenia. Longitudinal studies are also needed to establish the risk of developing a sleep disorder (e.g., insomnia, OSA) while being affected by schizophrenia and vice versa. Preliminary evidence suggests that individuals affected by insomnia are more likely to experience psychotic symptoms, and that psychosis can disrupt the ability of falling and staying asleep, but assessing for causality will require longitudinal observation in patient populations affected by either schizophrenia or insomnia to see whether having one disorder will increase the risk of developing the other. Finally, it would be important to increase awareness and improve management of sleep disturbances in schizophrenia patients, which could in turn significantly improve the quality of life of individuals affected by this devastating mental illness.
Disclosure
The authors report no conflicts of interest in this work.
References
Saha S, Chant D, Welham J, McGrath J. A systematic review of the prevalence of schizophrenia. PLoS Med. 2005;2(5):e141. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub; 2013. | ||
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. | ||
Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. | ||
Chung F, Yegneswaran B, Liao P, et al. STOP Questionnaire: a Tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812–821. | ||
Castelnovo A, D’Agostino A, Casetta C, Sarasso S, Ferrarelli F. Sleep spindle deficit in schizophrenia: contextualization of recent findings. Curr Psychiatry Rep. 2016;18(8):1–10. | ||
Massimini M, Tononi G, Huber R. Slow waves, synaptic plasticity and information processing: insights from transcranial magnetic stimulation and high-density EEG experiments. Eur J Neurosci. 2009;29(9):1761–1770. | ||
Zanini M, Castro J, Coelho FM, et al. Do sleep abnormalities and misaligned sleep/circadian rhythm patterns represent early clinical characteristics for developing psychosis in high risk populations? Neurosci Biobehav Rev. 2013;37(10):2631–2637. | ||
Tan HY, Ang YG. First-episode psychosis in the military: a comparative study of prodromal symptoms. Aust N Z J Psychiatry. 2001;35(4):512–519. | ||
Yung AR, McGorry PD. The initial prodrome in psychosis: descriptive and qualitative aspects. Aust N Z J Psychiatry. 1996;30(5):587–599. | ||
Zanini MA, Castro J, Cunha GR, et al. Abnormalities in sleep patterns in individuals at risk for psychosis and bipolar disorder. Schizophr Res. 2015;169(1):262–267. | ||
Lunsford-Avery JR, Orr JM, Gupta T, et al. Sleep dysfunction and thalamic abnormalities in adolescents at ultra high-risk for psychosis. Schizophr Res. 2013;151(1):148–153. | ||
Ruhrmann S, Schultze-Lutter F, Salokangas RK, et al. Prediction of psychosis in adolescents and young adults at high risk: results from the prospective European prediction of psychosis study. Arch Gen Psychiatry. 2010;67(3):241–251. | ||
Sharma P, Dikshit R, Shah N, Karia S, De Sousa A. Excessive daytime sleepiness in schizophrenia: a naturalistic clinical study. J Clin Diagn Res. 2016;10(10):VC06. | ||
Yang C, Winkelman JW. Clinical significance of sleep EEG abnormalities in chronic schizophrenia. Schizophr Res. 2006;82(2):251–260. | ||
Mattai AA, Tossell J, Greenstein DK, et al. Sleep disturbances in childhood-onset schizophrenia. Schizophr Res. 2006;86(1):123–129. | ||
Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders: an opportunity for prevention? JAMA. 1989;262(11):1479–1484. | ||
Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry. 1996;39(6):411–418. | ||
Herz MI, Melville C. Relapse in schizophrenia. Am J Psychiatry. 1980;137(7):801–805. | ||
Monti JM, BaHammam AS, Pandi-Perumal SR, et al. Sleep and circadian rhythm dysregulation in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2013;43:209–216. | ||
Dzirasa K, Ribeiro S, Costa R, et al. Dopaminergic control of sleep–wake states. J Neurosci. 2006;26(41):10577–10589. | ||
Eder DN, Zdravkovic M, Wildschiødtz G. Selective alterations of the first NREM sleep cycle in humans by a dopamine D1 receptor antagonist (NNC-687). J Psychiat. Res. 2003;37(4):305–312. | ||
Jones HM, Pilowsky LS. Dopamine and antipsychotic drug action revisited. Br J Psychiatry. 2002;181(4):271–275. | ||
Chemerinski E, Ho BC, Flaum M, Arndt S, Fleming F, Andreasen NC. Insomnia as a predictor for symptom worsening following antipsychotic withdrawal in schizophrenia. Compr Psychiatry. 2002;43(5):393–396. | ||
Freeman D, Pugh K, Vorontsova N, Southgate L. Insomnia and paranoia. Schizophr Res. 2009;108(1):280–284. | ||
Benson KL. Sleep in schizophrenia: pathology and treatment. Sleep Med Clin. 2015;10(1):49–55. | ||
Staedt J, Dewes D, Danos P, Stoppe G. Can chronic neuroleptic treatment promote sleep disturbances in elderly schizophrenic patients? Int J Geriatr Psychiatry. 2000;15(2):170–176. | ||
Ancoli-Israel S, Martin J, Jones DW, et al. Sleep-disordered breathing and periodic limb movements in sleep in older patients with schizophrenia. Biol Psychiatry. 1999;45(11):1426–1432. | ||
Kang SG, Lee HJ, Jung SW, et al. Characteristics and clinical correlates of restless legs syndrome in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(5):1078–1083. | ||
Walters AS, Hening W, Rubinstein M, Chokroverty S. A clinical and polysomnographic comparison of neuroleptic-induced akathisia and the idiopathic restless legs syndrome. Sleep. 1991;14(4):339–345. | ||
Stubbs B, Vancampfort D, Veronese N, et al. The prevalence and predictors of obstructive sleep apnea in major depressive disorder, bipolar disorder and schizophrenia: a systematic review and meta-analysis. J Affect Disord. 2016;197:259–267. | ||
Alam A, Chengappa KR, Ghinassi F. Screening for obstructive sleep apnea among individuals with severe mental illness at a primary care clinic. Gen Hosp Psychiatry. 2012;34(6):660–664. | ||
Winkelman JW. Schizophrenia, obesity, and obstructive sleep apnea. J Clin Psychiatry. 2001;62(1):8–11. | ||
Smith DJ, Langan J, McLean G, Guthrie B, Mercer SW. Schizophrenia is associated with excess multiple physical-health comorbidities but low levels of recorded cardiovascular disease in primary care: cross-sectional study. BMJ Open. 2013;3(4):e002808. | ||
Annamalai A, Palmese LB, Chwastiak LA, Srihari VH, Tek C. High rates of obstructive sleep apnea symptoms among patients with schizophrenia. Psychosomatics. 2015;56(1):59–66. | ||
Wulff K, Dijk DJ, Middleton B, Foster RG, Joyce EM. Sleep and circadian rhythm disruption in schizophrenia. Br J Psychiatry. 2012;200(4):308–316. | ||
Poulin J, Chouinard S, Pampoulova T, Lecomte Y, Stip E, Godbout R. Sleep habits in middle-aged, non-hospitalized men and women with schizophrenia: a comparison with healthy controls. Psychiatry Res. 2010;179(3):274–278. | ||
Afonso P, Figueira ML, Paiva T. Sleep–wake patterns in schizophrenia patients compared to healthy controls. World J Biol Psychiatry. 2014;15(7):517–524. | ||
Martin J, Jeste DV, Caliguiri MP, Patterson T, Heaton R, Ancoli-Israel S. Actigraphic estimates of circadian rhythms and sleep/wake in older schizophrenia patients. Schizophr Res. 2001;47(1):77–86. | ||
Birketvedt GS, Florholmen J, Sundsfjord J, et al. Behavioral and neuroendocrine characteristics of the night-eating syndrome. JAMA. 1999;282(7):657–663. | ||
Palmese LB, Ratliff JC, Reutenauer EL, Tonizzo KM, Grilo CM, Tek C. Prevalence of night eating in obese individuals with schizophrenia and schizoaffective disorder. Compr Psychiatry. 2013;54(3):276–281. | ||
Palmese LB, DeGeorge PC, Ratliff JC, et al. Insomnia is frequent in schizophrenia and associated with night eating and obesity. Schizophr Res. 2011;133(1):238–243. | ||
Sansa G, Gavaldà A, Gaig C, et al. Exploring the presence of narcolepsy in patients with schizophrenia. BMC Psychiatry. 2016;16(1):177. | ||
Plazzi G, Fabbri C, Pizza F, Serretti A. Schizophrenia-like symptoms in narcolepsy type 1: shared and distinctive clinical characteristics. Neuropsychobiology. 2015;71(4):218–224. | ||
Sarkanen T, Niemelä V, Landtblom AM, Partinen M. Psychosis in patients with narcolepsy as an adverse effect of sodium oxybate. Front Neurol. 2014;5:136. | ||
Huang YS, Guilleminault C, Chen CH, Lai PC, Hwang FM. Narcolepsy–cataplexy and schizophrenia in adolescents. Sleep Med. 2014;15(1):15–22. | ||
Harrison C, Charles J, Britt H. Comorbidities and risk factors among patients with schizophrenia. Aust Fam Physician. 2015;44(11):781. | ||
Lunsford-Avery JR, LeBourgeois MK, Gupta T, Mittal VA. Actigraphic-measured sleep disturbance predicts increased positive symptoms in adolescents at ultra high-risk for psychosis: a longitudinal study. Schizophr Res. 2015;164(1):15–20. | ||
Lunsford-Avery JR, Gonçalves BD, Brietzke E, et al. Adolescents at clinical-high risk for psychosis: circadian rhythm disturbances predict worsened prognosis at 1-year follow-up. Schizophr Res. Epub 2017 Feb 4. | ||
Afonso P, Brissos S, Figueira ML, Paiva T. Schizophrenia patients with predominantly positive symptoms have more disturbed sleep–wake cycles measured by actigraphy. Psychiatry Res. 2011;189(1):62–66. | ||
Afonso P, Brissos S, Cañas F, Bobes J, Bernardo-Fernandez I. Treatment adherence and quality of sleep in schizophrenia outpatients. Int J Psychiatry Clin Pract. 2014;18(1):70–76. | ||
Mulligan LD, Haddock G, Emsley R, Neil ST, Kyle SD. High resolution examination of the role of sleep disturbance in predicting functioning and psychotic symptoms in schizophrenia: a novel experience sampling study. J Abnorm Psychol. 2016;125(6):788. | ||
Göder R, Boigs M, Braun S, et al. Impairment of visuospatial memory is associated with decreased slow wave sleep in schizophrenia. J Psychiatr Res. 2004;38(6):591–599. | ||
Waite F, Evans N, Myers E, et al. The patient experience of sleep problems and their treatment in the context of current delusions and hallucinations. Psychol Psychother. 2016;89(2):181–193. | ||
Waters F, Hanken K, Rock D. Sleep-disordered breathing in schizophrenia: an audit. Schizophr Res. 2013;143(2):393–394. | ||
Cohrs S. Sleep disturbances in patients with schizophrenia: impact and effect of antipsychotics. CNS Drugs. 2008;22(11):939–962. | ||
Xiang YT, Weng YZ, Leung CM, Tang WK, Lai KY, Ungvari GS. Prevalence and correlates of insomnia and its impact on quality of life in Chinese schizophrenia patients. Sleep. 2009;32(1):105–109. | ||
Hou CL, Li Y, Cai MY, et al. Prevalence of insomnia and clinical and quality of life correlates in Chinese patients with schizophrenia treated in primary care. Perspect Psychiatr Care. 2015;53(2):80–86. | ||
Hofstetter JR, Lysaker PH, Mayeda AR. Quality of sleep in patients with schizophrenia is associated with quality of life and coping. BMC Psychiatry. 2005;5(1):13. | ||
Waters F, Naik N, Rock D. Sleep, fatigue, and functional health in psychotic patients. Schizophr Res Treatment. 2013;2013:425826. | ||
Brissos S, Afonso P, Cañas F, Bobes J, Bernardo Fernandez I, Guzman C. Satisfaction with life of schizophrenia outpatients and their caregivers: differences between patients with and without self-reported sleep complaints. Schizophr Res Treatment. 2013;2013:502172. | ||
Li SX, Lam SP, Zhang J, et al. Sleep disturbances and suicide risk in an 8-year longitudinal study of schizophrenia-spectrum disorders. Sleep. 2016;39(6):1275–1282. | ||
Waters F, Chiu VW, Janca A, Atkinson A, Ree M. Preferences for different insomnia treatment options in people with schizophrenia and related psychoses: a qualitative study. Front Psychol. 2015;6:990. | ||
Faulkner S, Bee P. Experiences, perspectives and priorities of people with schizophrenia spectrum disorders regarding sleep disturbance and its treatment: a qualitative study. BMC Psychiatry. 2017;17(1):158. | ||
Chiu VW, Harvey RH, Sloan NB, et al. Cognitive and behavioral factors associated with insomnia in inpatients with schizophrenia and related psychoses. J Nerv Ment Dis. 2015;203(10):798–803. | ||
Chiu VW, Ree M, Janca A, Waters F. Sleep in Schizophrenia: exploring subjective experiences of sleep problems, and implications for treatment. Psychiatr Q. 2016;87(4):633–648. | ||
Freeman D, Waite F, Startup H, et al. Efficacy of cognitive behavioural therapy for sleep improvement in patients with persistent delusions and hallucinations (BEST): a prospective, assessor-blind, randomised controlled pilot trial. Lancet Psychiatry. 2015;2(11):975–983. | ||
Luthringer R, Staner L, Noel N, et al. A double-blind, placebo-controlled, randomized study evaluating the effect of paliperidone extended-release tablets on sleep architecture in patients with schizophrenia. Int Clin Psychopharmacol. 2007;22(5):299–308. | ||
Müller MJ, Rossbach W, Mann K, et al. Subchronic effects of olanzapine on sleep EEG in schizophrenic patients with predominantly negative symptoms. Pharmacopsychiatry. 2004;37(04):157–162. | ||
Kluge M, Schacht A, Himmerich H, et al. Olanzapine and clozapine differently affect sleep in patients with schizophrenia: results from a double-blind, polysomnographic study and review of the literature. Schizophr Res. 2014;152(1):255–260. | ||
Yamashita H, Mori K, Nagao M, Okamoto Y, Morinobu S, Yamawaki S. Influence of aging on the improvement of subjective sleep quality by atypical antipsychotic drugs in patients with schizophrenia: comparison of middle-aged and older adults. Am J Geriatr Psychiatry. 2005;13(5):377–384. | ||
Cates ME, Jackson CW, Feldman JM, Stimmel AE, Woolley TW. Metabolic consequences of using low-dose quetiapine for insomnia in psychiatric patients. Community Men Health J. 2009;45(4):251–254. | ||
Tek C, Palmese LB, Krystal AD, et al. The impact of eszopiclone on sleep and cognition in patients with schizophrenia and insomnia: a double-blind, randomized, placebo-controlled trial. Schizophr Res. 2014;160(1):180–185. | ||
Kajimura N, Kato M, Okuma T, Sekimoto M, Watanabe T, Takahashi K. A comparative study of benzodiazepine hypnotics and zopiclone in schizophrenia: effects on polysomnograms and BPRS scores. Psychiatry Clin Neurosci. 1994;48(4):815–822. | ||
Shamir E, Laudon M, Barak Y, et al. Melatonin improves sleep quality of patients with chronic schizophrenia. J Clin Psychiatry. 2000;61(5):373–377. | ||
Suresh KP, Andrade C, Bhakta SG, Singh NM. Melatonin in schizophrenic outpatients with insomnia: a double-blind, placebo-controlled study. J Clin Psychiatry. 2007;68(2):237–241. | ||
Shamir E, Rotenberg VS, Laudon M, Zisapel N, Elizur A. First-night effect of melatonin treatment in patients with chronic schizophrenia. J Clin Psychopharmacol. 2000;20(6):691–694. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.