Back to Journals » Clinical Ophthalmology » Volume 17
Scheimpflug-Derived Keratometric, Pachymetric and Pachymetric Progression Indices in the Diagnosis of Keratoconus: A Systematic Review and Meta-Analysis
Authors Owusu S, Zaabaar E, Kwarteng MA ![]() , Ankamah S, Abowine JBV, Kyei S
, Ankamah S, Abowine JBV, Kyei S ![]()
Received 22 August 2023
Accepted for publication 7 December 2023
Published 20 December 2023 Volume 2023:17 Pages 3941—3964
DOI https://doi.org/10.2147/OPTH.S436492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sandra Owusu,1 Ebenezer Zaabaar,1,2 Michael Agyemang Kwarteng,3,4 Samuel Ankamah,5 John Baptist Vianney Abowine,6 Samuel Kyei1,7
1Department of Optometry and Vision Science, University of Cape Coast, Cape Coast, Ghana; 2Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong, Hong Kong; 3Department of Optometry, Bindura University of Science Education, Bindura, Zimbabwe; 4Discipline of Optometry, University of Kwazulu-Natal, Durban, South Africa; 5University of Ghana Library System, University of Ghana, Accra, Ghana; 6Dr. Rose Mompi Eye Hospital, Hohoe, Ghana; 7Biomedical and Clinical Research Center, University of Cape Coast, Cape Coast, Ghana
Correspondence: Samuel Kyei, Email [email protected]
Abstract: Scheimpflug Pentacam Tomography is becoming crucial in the diagnosis and monitoring of keratoconus, as well as in pre- and post-corneal refractive care, but there are still some inconsistencies surrounding its evidence base diagnostic outcome. Therefore, this study aimed at employing meta-analysis to systematically evaluate the keratometric, pachymetric, and pachymetric progression indices used in the diagnosis of Keratoconus. The review protocol was registered with PROSPERO (Identifier: CRD4202310058) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. PubMed, MEDLINE, Web of Science, and EMBASE were used for data search, followed by a quality appraisal of the included studies using the revised tool for the quality assessment of diagnostic accuracy studies (QUADAS-2). Meta-analysis was conducted using the meta (6.5.0) and metafor (4.2.0) packages in R version 4.3.0, as well as Stata. A total of 32 studies were included in the analysis. All keratometry (K) readings (flattest meridian, K1; steepest meridian, K2, maximum, Kmax) were significantly steeper in keratoconic compared to normal eyes: [MD (95% CI)], K1 [2.67 (1.81; 3.52)], K1-back [− 0.71 (− 1.03; − 0.39)], K1-front [4.06 (2.48; 5.63)], K2 [4.32 (2.89; 5.75)], K2-back [− 1.25 (− 1.68; − 0.82)], K2-front [4.82 (1.88; 7.76)], Kmax [7.57 (4.80; 10.34)], and Kmean [2.80 (1.13; 4.47)]. Additionally, corneal thickness at the center, CCT [− 61.19 (− 73.79; − 48.60)] and apex, pachy-apex [− 41.86 (− 72.64; − 11.08)] were significantly thinner in keratoconic eyes compared to normal eyes. The pooled estimates for pachymetric progression index (PPI): PPImin [0.66 (0.43; 0.90)], PPImax [1.26 (0.87; 1.64)], PPIavg [0.90 (0.68; 1.12)], and Ambrosio relational thickness (ART): ARTmax [− 242.77 (− 288.86; − 196.69)], and ARTavg [− 251.08 (− 308.76; − 195.39)] revealed significantly more rapid pachymetric progression in keratoconic eyes than in normal eyes. The Pentacam Scheimpflug-derived keratometric, pachymetric, and pachymetric progression indices are good predictors in discriminating KC from normal eyes.
Keywords: corneal topography, keratometric readings, central corneal thickness, keratoconus, pachymetric progression
Introduction
Keratoconus (KC) remains an important ocular disorder with enormous implications for affected persons’ quality of life.1,2 It is known to be characterised with progressive corneal asymmetry, steepening and alteration, apical thinning and central corneal scarring.3 There have been variations in the reported onset of the disease, including adolescence, early adulthood and childhood.4
As a disease of the cornea, the use of tomographic techniques for the diagnosis and progression of keratoconus is very crucial. In the advanced stages of the disease, it is easy to diagnose using the slit lamp assessment technique; however, in the early stages, its diagnosis can be tricky and easily missed.5
Posterior corneal and pachymetric measures have proven useful in the early-stage diagnosis of this corneal ectasia.6,7 The Scheimpflug system has incorporated a spectrum of indices for the objective diagnosis and staging of Keratoconus.8,9 The system characterizes the anterior corneal curvature-based topometric measures together with the posterior corneal and thickness-oriented Belin/Ambrosio Enhanced Ectasia Display (BAD) and Ambrosio’s related thickness maximum.10,11
The quest for refractive surgical interventions has brought to the fore the need for tests with high sensitivity and reliability, including non-tomographic techniques. The Scheimpflug imaging system, unlike others, allows for the visualization and measurement of corneal defects under standardized air puff indentation. The quality of published data on KC evaluation is often low due to various factors. Some studies had small sample sizes, which limited the generalizability of their findings. Other studies used different criteria in the classification of KC, leading to inconsistencies in the results. These limitations highlight the need for more rigorous research using standardized methods and larger sample sizes. The present study, therefore, investigated the use of the Scheimpflug -derived keratometric, pachymetric, and pachymetric progression indices in the diagnosis of Keratoconus.
Methods
The review protocol was registered with PROSPERO (Identifier: CRD42023410058), and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed.
Literature Search Strategy and Study Selection
We conducted a thorough literature search in PubMed, MEDLINE, Web of Science, and EMBASE to discover relevant articles, and the latest search was conducted on June 30, 2023. The search strategy was based on combinations of medical subject headings and free text words, and the search terms used included “Scheimpflug”, “Pentacam”, “keratoconus”, “ectatic cornea”, “diagnostic efficacy”, “tomography”, “topography”, “outcome”, “efficacy” “topographic”, “tomographic”, and “topometric” in varying combinations. The search was defined using the Boolean operators “AND” and “OR” and truncations. Figure 1 illustrates the PRISMA flowchart outlining the processes for obtaining the articles used in this review. The initial literature search turned up one hundred and ten (110) plausibly relevant articles, out of which thirty-seven12 were included. Full-text articles that seemed relevant were retrieved after three reviewers (A.J.B.V., S.A., and S.O.) independently evaluated the titles and abstracts for possible eligibility. The three reviewers then independently evaluated these full-text articles to determine their suitability for inclusion. We reached a consensus on how to classify the eligibility differences of the full-text articles through discussions, and where necessary, three other reviewers (S.K., M.A.K., and E.Z.) adjudicated the issue.
 |
Figure 1 PRISMA flow chart of study selection. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29;n71. Creative Commons.13 |
Published studies were considered eligible if they met the following criteria: Pentacam Scheimpflug Tomography was used in evaluating the cornea and compared any of the keratometry readings, pachymetric indices and/or pachymetric progression indices amongst participants with keratoconus and a control group (participants without keratoconus). Conference abstracts were included if they contained all relevant data. Review papers, studies without control groups, studies with no pertinent data, case reports, correspondence, and studies with missing or unidentifiable data were excluded from this review.
Study Appraisal and Data Extraction
Quality appraisal of the included studies was done using the revised tool for the quality assessment of diagnostic accuracy studies (QUADAS-2). The QUADAS-2 tool is commonly used in systematic reviews of diagnostic test accuracy studies to assess individual studies’ risk of bias and applicability. It comprises seven categories of bias which are classified as “high”, “low”, or “unclear”, but does not produce a single overall numerical score. For our study, two authors (S.O. and E.Z.) used the QUADAS-2 tool independently to evaluate the studies, and any disagreements were resolved by group discussion involving a third author (S.K.). This approach ensured a reliable and consistent assessment of the studies. Two authors (S.O. and A.J.B.V.) independently extracted data from each included study. Demographic characteristics of study subjects and means and standard deviations of the Scheimpflug Pentacam parameters were extracted using Microsoft Excel Spreadsheet, with accuracy confirmed by a third author (E.Z.). The parameters included in this review were keratometry readings (keratometric powers of the flat meridian [K1, K1-back, K1-front]; keratometric powers of the steep meridian [K2, K2-back, K2-front]; mean keratometric power, Kmean; keratometric power of the steepest point of the front surface, Kmax), pachymetric indices (central corneal thickness, CCT; corneal thickness at the apex, pachy-apex), and pachymetric progression indices (minimum pachymetric progression index, PPImin; maximum pachymetric progression index, PPImax, average pachymetric progression index, PPIavg; maximum Ambrosio relational thickness, ARTmax; average Ambrosio relational thickness, ARTavg).
Data Analysis
The meta-analysis (inverse variance random-effect model) was conducted using the meta (6.5.0) and metafor (4.2.0) packages in R version 4.3.0 (R Foundation) as well as Stata (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.). We reported the estimates of effect size as mean differences (MD) with a 95% confidence interval (CI). A meta-regression was conducted for parameters with at least 10 studies to examine whether potential effect modifiers, such as sample size and publication year, could account for any variation in effect sizes. A sensitivity analysis was performed to ensure the robustness of the pooled estimates using a leave-one-out meta-analysis approach, wherein the impact of a particular study on the final combined estimate was assessed by systematically excluding each study in turn. Additionally, we evaluated publication bias for parameters with at least 10 studies by visually inspecting funnel plots and addressed any potential bias using the Trim and Fill method developed by Duval and Tweedie.
Results
Table 1 presents a summary of the key characteristics of the studies that were analyzed in the review. All the studies included in the meta-analysis were published within the period spanning from 2009 to 2022. Table 2 presents the meta-regression conducted for parameters with at least 10 studies.
 |
Table 1 Summary of the Key Characteristics of the Studies That Were Analyzed |
 |
Table 2 Meta-Regression |
As shown in Figure 2, all keratometry readings were significantly steeper in eyes with keratoconus than in normal eyes, [MD (95% CI)], K1 [2.67 (1.81; 3.52)], K1-back [−0.71 (−1.03; −0.39)], K1-front [4.06 (2.48; 5.63)], K2 [4.32 (2.89; 5.75)], K2-back [−1.25 (−1.68; −0.82)], K2-front [4.82 (1.88; 7.76)], Kmax [7.57 (4.80; 10.34)], and Kmean [2.80 (1.13; 4.47)]. Further, CCT [−61.19 (−73.79; −48.60)] and pachy-apex [−41.86 (−72.64; −11.08)] were significantly thinner in keratoconic eyes compared to normal eyes (Figure 3). The pooled estimates for PPImin [0.66 (0.43; 0.90)], PPImax [1.26 (0.87; 1.64)], PPIavg [0.90 (0.68; 1.12)], ARTmax [−242.77 (−288.86; −196.69)], and ARTavg [−251.08 (−308.76; −195.39)] showed significantly more rapid pachymetric progression in keratoconic eyes than in normal eyes (Figures 4 and 5). Notably, we observed significant heterogeneity in the meta-analysis for all the parameters (I2>50%); however, the results of the leave-one-out sensitivity analysis indicated that the exclusion of any single study did not substantially alter the pooled effect size estimate for all parameters, suggesting that the overall findings were robust as the pooled effect size estimate remained relatively stable (Figures 6–9). The contour-enhanced funnel plots showed evidence of non-random publication bias for K2, CCT, PPImax, and PPIavg, with an excess of studies in the lower-right corners of the plots, implying that smaller studies with non-significant results may not have been published, and this might have over-estimated the treatment effects (Figures 10–13). Publication bias adjustments with Duval and Tweedie’s trim and fill are shown in Figure 14. Publication-bias-corrected estimates of the true effect sizes were [2.53 (0.78; 4.27); outliers removed: 2.80 (1.10; 4.54)], [−104.82 (−128.69; −80.96); outliers removed: −106.19 (−128.68; −83.69)], [0.94 (0.52; 1.36); outliers removed: 1.08 (0.73; 1.42)], and [0.64 (0.38; 0.89); outliers removed: 0.64 (0.40; 0.87)] for K2, CCT, PPImax, and PPIavg, respectively. The adjusted effect sizes were relatively smaller for K2, PPImax, and PPIavg and relatively larger for CCT, than the unadjusted estimates, suggesting that there may have been publication bias favoring studies with larger effect sizes; however, the effect sizes remained statistically significant after adjustment. The results of the meta-regression analysis showed that sample size (β = −0.07, P = 0.02) was a significant predictor of the effect size estimate for CCT. Specifically, studies with larger sample sizes tended to report larger effect sizes. None of the covariates was a significant predictor of the remaining parameters (Table 2 and Figures 15–18). The study further established transparency of evidence synthesis results and findings by assessing the risk of bias and quality of the studies (Figure 19).
 |
Figure 2 Forest Plots of keratometric readings in keratoconic and normal eyes (A-H) for K1, K1f, K1b, K2, K2f, K2b, Kmax and Kmean respectively. |
 |
Figure 3 Forest Plots of CCT and Pachy-apex (A and B respectively) in keratoconic and normal eyes. |
 |
Figure 4 Forest Plots for the Pachymetric Progression indices in keratoconic and normal eyes (A-C) for PPImax, PPImin and PPIavg respectively. |
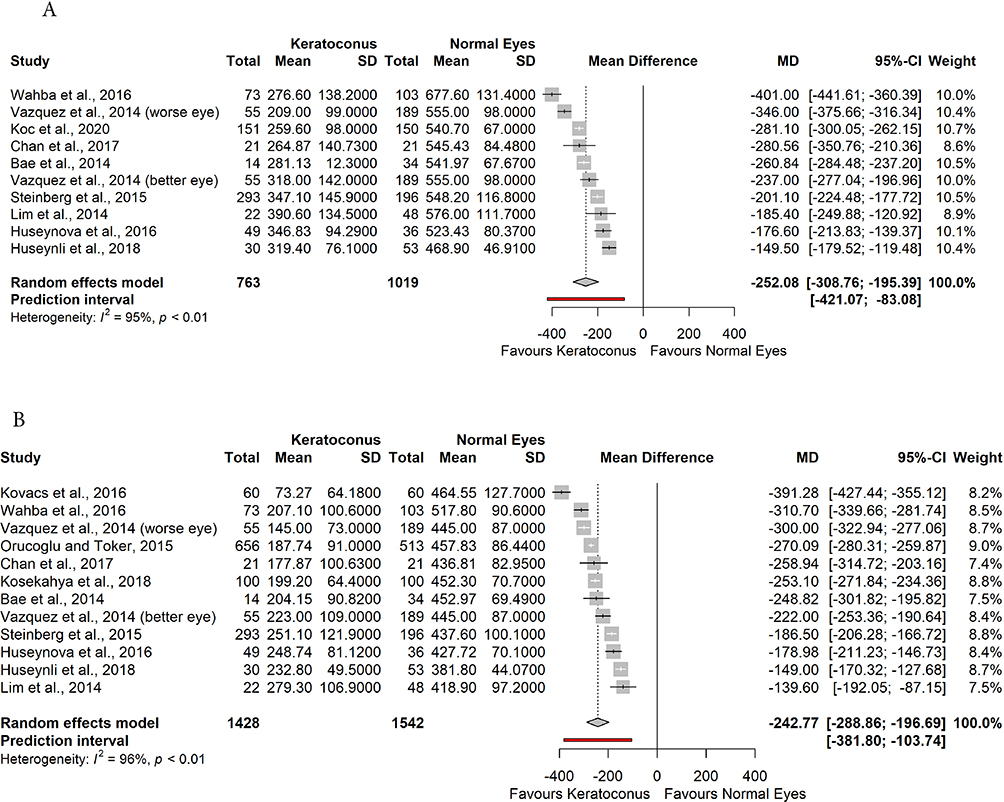 |
Figure 5 Forest Plots of the Ambrosio Relational Thickness (A and B respectively) for ARTavg and ARTmax in keratoconic and normal eyes. |
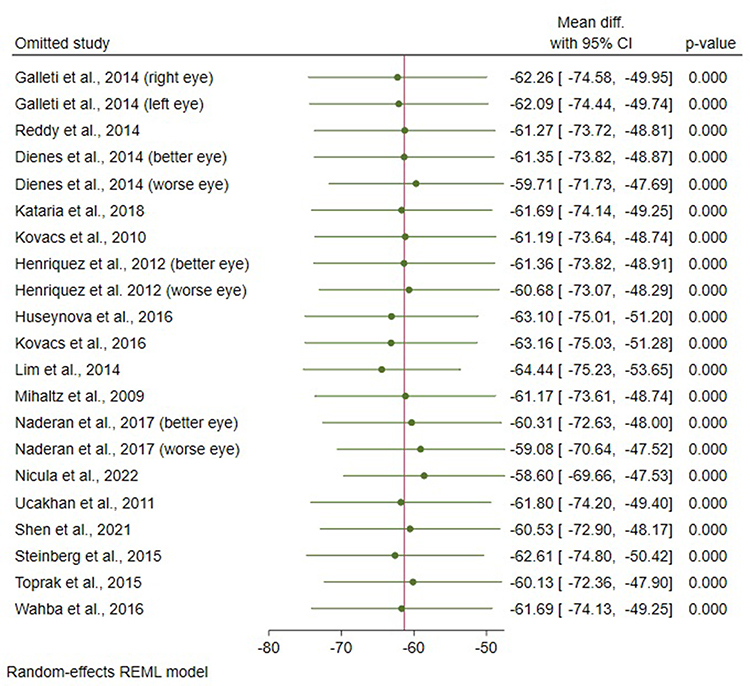 |
Figure 6 Leave-one-out meta-analysis for central corneal thickness (CCT). |
 |
Figure 7 Leave-one-out meta-analyses for K1b, K1f, K2b, K2f, Kmax and Kmean (A-F respectively). |
 |
Figure 8 Leave-one-out meta-analyses for Pachy-apex, ARTavg and ARTmax (A-C respectively). |
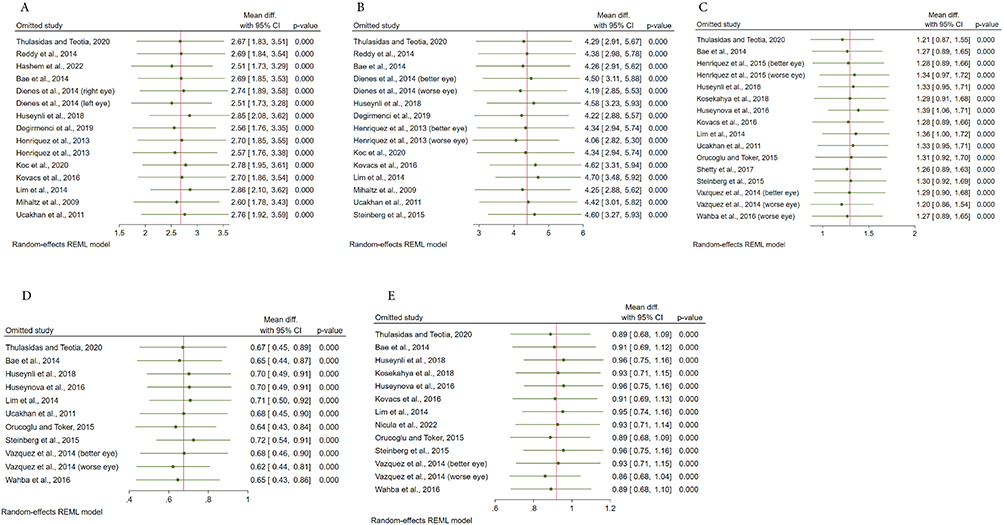 |
Figure 9 Leave-one-out meta-analyses for K1, K2, PPImax, PPImin and PPIavg (A-E respectively). |
 |
Figure 10 Contour-Enhanced Funnel Plot for the keratometric power at the steep Meridian (K2). |
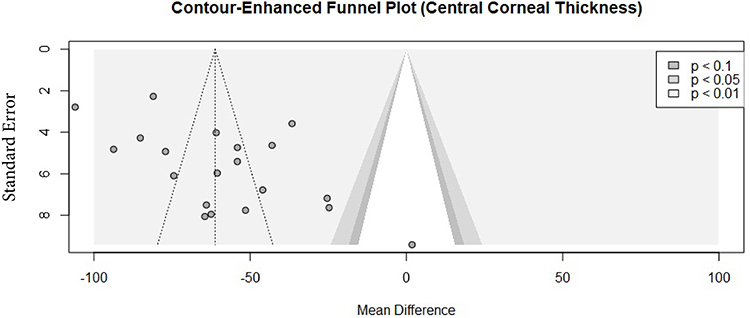 |
Figure 11 Contour-Enhanced Funnel Plot for the central corneal thickness (CCT). |
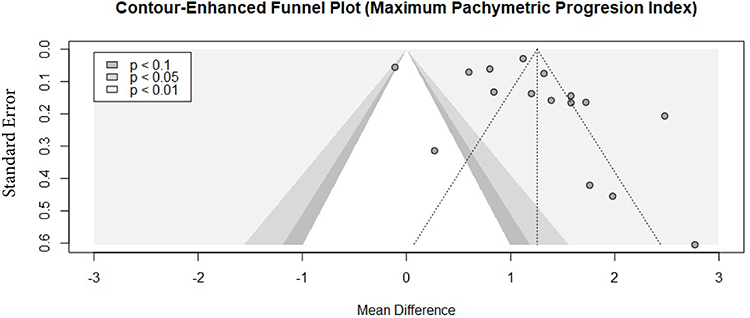 |
Figure 12 Contour-Enhanced Funnel Plot for the maximum pachymetric progression Indices (PPImax). |
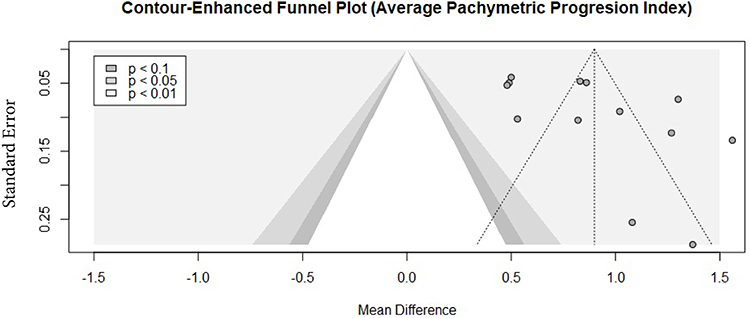 |
Figure 13 Contour-Enhanced Funnel Plot for the average pachymetric progression Indices (PPIavg). |
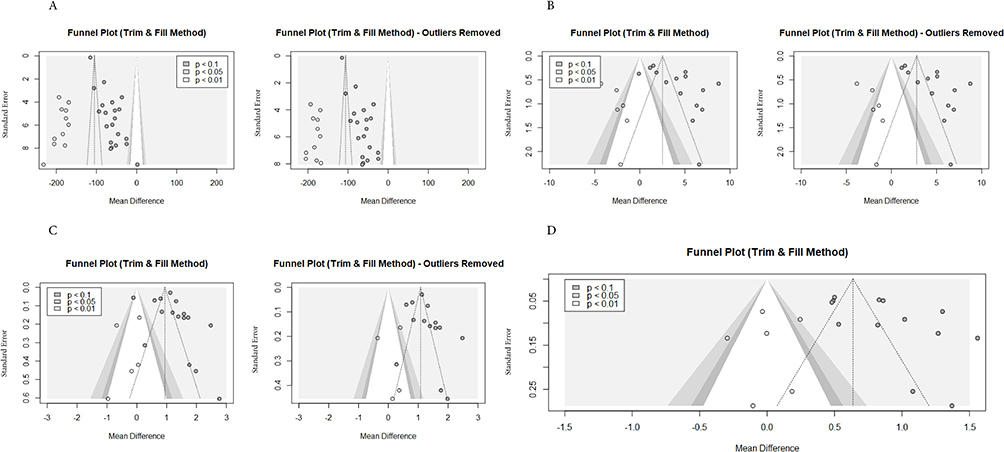 |
Figure 14 Tweedie’s trim and fill for CCT, K2, PPImax and PPIavg (A–D respectively). |
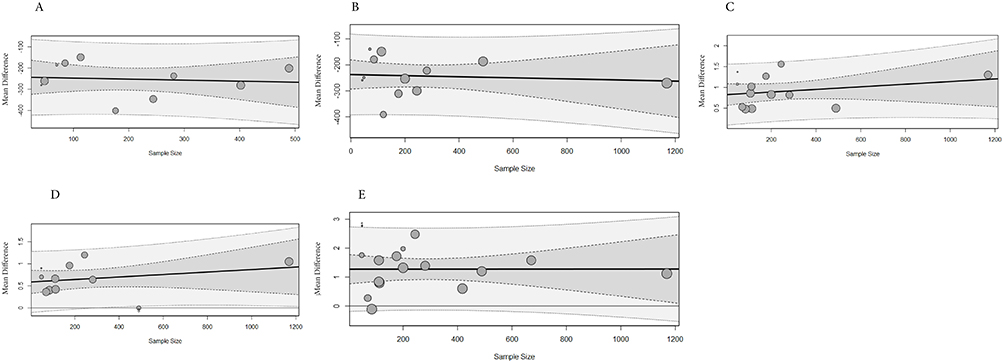 |
Figure 15 Bubble plots of meta-regression for the effect of sample sizes on ARTavg, ARTmax, PPIavg, PPImin and PPImax (A-E respectively). |
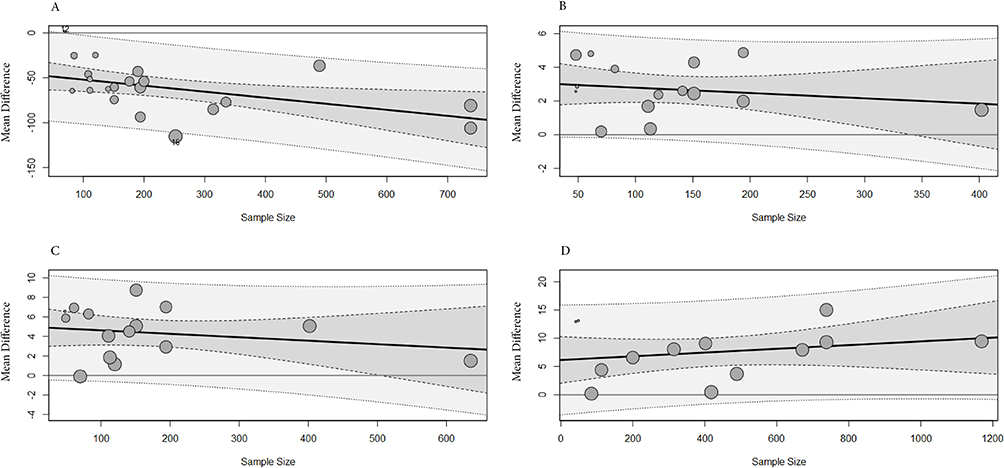 |
Figure 16 Bubble plots of meta-regression (A-D) for the effect of sample sizes on CCT, K1, K2 and Kmax respectively. |
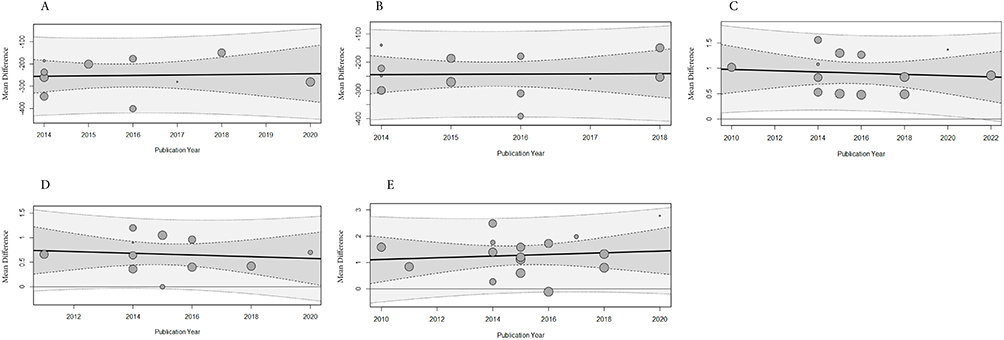 |
Figure 17 Bubble plots of meta-regression for the effect of publication year on ARTavg, ARTmax, PPIavg, PPImin and PPImax (A-E respectively). |
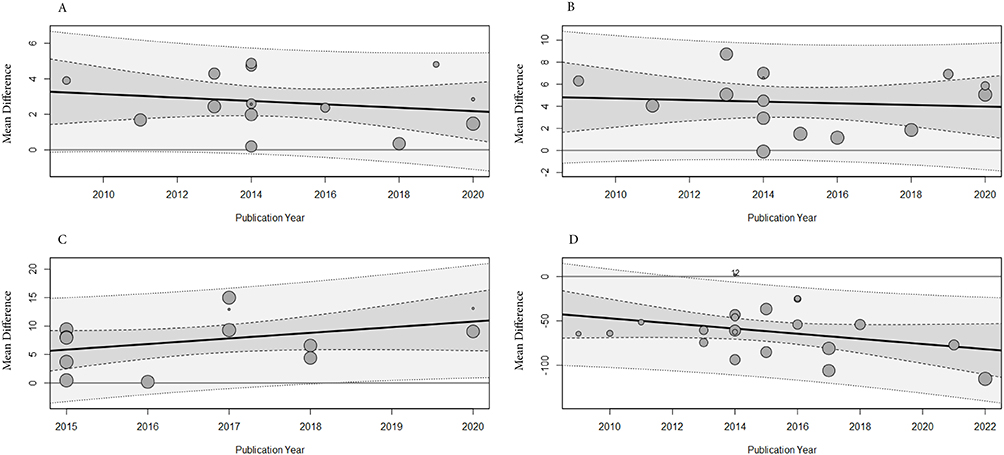 |
Figure 18 Bubble plots of meta-regression for the effect of publication year on K1, K2, Kmax and CCT (A-D respectively. |
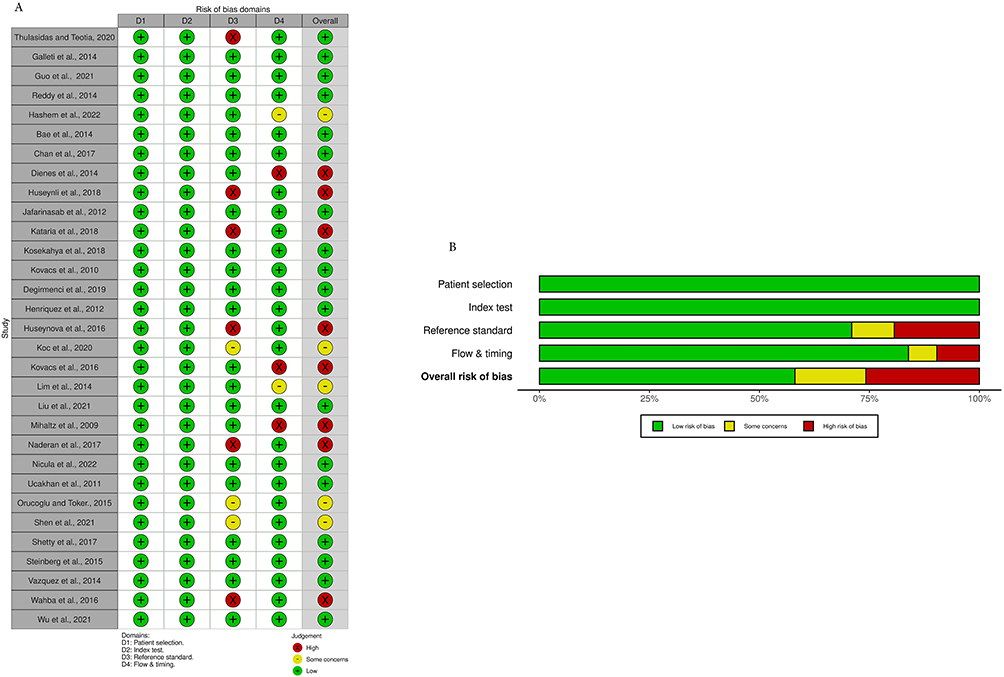 |
Figure 19 Traffic Light and Weighted Bar Plot for Risk of Bias Assessment using QUADAS-2 (A and B respectively). |
Discussion
Corneal topography is generally a non-invasive probing technique that examines qualitatively and quantitatively the anatomical structure of the cornea. It allows for geometric classification and affords a discriminating typical pattern of normal corneas from pathological ectatic ones.10,45–48 Existing corneal topographers operates on either one or more of these principles; light reflection on the cornea, projection of a slit light onto the cornea, and asymmetric reflection of multicolor light-emitting diodes (LEDs).49 Clinical characterization of the structure (shape) of the human cornea through topographic analysis is a common practice among eye care practitioners when the diagnosis of keratoconus is intended.
Recent technological advances such as Pentacam Scheimpflug tomography allow for the assessment of both the anterior and posterior surfaces of cornea at different points.41,49,50 Anteriorly, keratoconus is morphologically characterized by a cone-shaped protrusion of the cornea.49,51,52 This protrusion is typically eccentric but inferior-temporally positioned, read off as an area higher than the curve of the best adjustment surface in the elevation maps, and as an area more curved in the curvature map. The outcomes of the meta-analysis reveal evidence of significant mean differences in both anterior and posterior cornea keratometry readings between keratoconus and normal eyes. Specifically, the results indicate that the keratometry readings were significantly steeper in the keratoconus eyes compared to the normal eyes. Studies have suggested that early changes in eyes with keratoconus are also present on the posterior corneal surface.53 The geometric correlation between anterior and posterior cornea surfaces, have proven clinically useful in the discrimination of normal cornea from keratoconic corneas even at the subclinical stages.54–56 The disparities observed in keratometry readings provide valuable insights into the structural changes occurring in keratoconus, highlighting the complex nature of the condition. Understanding these differences can have important clinical implications, as they can aid in the accurate diagnosis and monitoring of keratoconus, as well as the development of targeted treatment approaches.
Also, this review highlights the significance of considering pachymetric and pachymetric progression indices in differentiating keratoconic eyes from normal ones. This study found that CCT and pachy-apex were significantly thinner in keratoconic eyes than normal ones. The pooled estimates for pachymetric progression indices also showed significantly more rapid pachymetric progression in keratoconic eyes than in normal eyes. These findings indicate that these indices provide valuable insights into discriminating KC from normal eyes considering the severity, and the progression of KC, aiding in its early detection and management. Several studies have used only the pachymetry indices in evaluating and diagnosing KC.57–59 Therefore, a comprehensive assessment of these factors is essential for an accurate diagnosis and personalised management of KC. In addition, using these indices can also help monitor the effectiveness of various treatment options for keratoconus. By regularly assessing these indices, healthcare professionals can make informed decisions with regards to the need for intervention or adjustment of treatment plans. This approach can potentially improve patient outcomes and minimise the risk of complications associated with advanced stages of keratoconus.
The results of the meta-regression analysis revealed sample size as a significant moderator of the effect size estimate for CCT, indicating that it plays a crucial role in explaining the heterogeneity observed among the studies. This finding suggests that the impact of sample size on CCT should be carefully considered when interpreting the results. However, other factors not accounted for in this analysis may also contribute to the between-study variation.
There is the need to acknowledge the limitations of this review study. Firstly, the included studies may have had variations in their methodologies and sample sizes, which introduced high heterogeneity in the pooled estimates. However, the leave-one-out sensitivity analysis results indicated that the pooled effect size estimate for all parameters was stable suggesting that the results were not heavily influenced by any single study or group of studies. Secondly, the review study focused primarily on keratometric, pachymetric and pachymetric progression indices, and other factors related to keratoconus were not explored. Future review studies should consider other elements used in diagnosing KC.
Conclusion
The Pentacam Scheimpflug-derived keratometric, pachymetric, and pachymetric progression indices are good predictors in discriminating KC from normal eyes. The findings of this review study have important implications for the diagnosis and management of keratoconus. By incorporating these indices into the diagnostic process, healthcare professionals can improve the accuracy of their assessments and provide personalised treatment plans.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kymes SM, Walline JJ, Zadnik K, Sterling J, Gordon MO. Changes in the Quality-of-Life of People with Keratoconus. Am J Ophthalmol. 2008;145(4):611–617.e1. doi:10.1016/j.ajo.2007.11.017
2. Pinto RDP, Abe RY, Gomes FC, et al. Quality of life in keratoconus: evaluation with keratoconus outcomes research questionnaire (KORQ). Sci Rep. 2021;11(1):12970. doi:10.1038/s41598-021-92346-1
3. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28(4):293–322. doi:10.1016/0039-6257(84)90094-8
4. Sabti S, Tappeiner C, Frueh BE. corneal cross-linking in a 4-year-old child with keratoconus and down syndrome. Cornea. 2015;34(9):1157–1160. doi:10.1097/ICO.0000000000000491
5. Fernández Pérez J, Valero Marcos A, Martínez Peña FJ. Early diagnosis of keratoconus: what difference is it making? Br J Ophthalmol. 2014;98(11):1465–1466. doi:10.1136/bjophthalmol-2014-305120
6. de Sanctis U, Loiacono C, Richiardi L, Turco D, Mutani B, Grignolo FM. Sensitivity and specificity of posterior corneal elevation measured by pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmology. 2008;115(9):1534–1539. doi:10.1016/j.ophtha.2008.02.020
7. Muftuoglu O, Ayar O, Ozulken K, Ozyol E, Akıncı A. Posterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patients. J Cataract Refract Surg. 2013;39(9):1348–1357. doi:10.1016/j.jcrs.2013.03.023
8. Piñero DP, Alió JL, Alesón A, Vergara ME, Miranda M. Corneal volume, pachymetry, and correlation of anterior and posterior corneal shape in subclinical and different stages of clinical keratoconus. J Cataract Refract Surg. 2010;36(5):814–825. doi:10.1016/j.jcrs.2009.11.012
9. Goebels S, Eppig T, Wagenpfeil S, Cayless A, Seitz B, Langenbucher A. Staging of keratoconus indices regarding tomography, topography, and biomechanical measurements. Am J Ophthalmol. 2015;159(4):733–738.e3. doi:10.1016/j.ajo.2015.01.014
10. Ambrósio R, Caiado ALC, Guerra FP, et al. Novel pachymetric parameters based on corneal tomography for diagnosing keratoconus. J Refrac Surg. 2011;27(10):753–758. doi:10.3928/1081597X-20110721-01
11. Duncan JK, Belin MW, Borgstrom M. Assessing progression of keratoconus: novel tomographic determinants. Eye and Vision. 2016;3(1):6. doi:10.1186/s40662-016-0038-6
12. Kovács I, Miháltz K, Kránitz K, et al. Accuracy of machine learning classifiers using bilateral data from a Scheimpflug camera for identifying eyes with preclinical signs of keratoconus. J Cataract Refract Surg. 2016;42(2):275–283. doi:10.1016/j.jcrs.2015.09.020
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29;n71
14. Thulasidas M, Teotia P. Evaluation of corneal topography and tomography in fellow eyes of unilateral keratoconus patients for early detection of subclinical keratoconus. Indian J Ophthalmol. 2020;68(11):2415–2420. doi:10.4103/ijo.IJO_2129_19
15. Galletti JD, Ruiseñor Vázquez PR, Minguez N, et al. Corneal asymmetry analysis by pentacam scheimpflug tomography for keratoconus diagnosis. J Refrac Surg. 2015;31(2):116–123. doi:10.3928/1081597X-20150122-07
16. Guo LL, Tian L, Cao K, et al. Comparison of the morphological and biomechanical characteristics of keratoconus, forme fruste keratoconus, and normal corneas. Semin Ophthalmol. 2021;36(8):671–678. doi:10.1080/08820538.2021.1896752
17. Reddy JC, Rapuano CJ, Cater JR, Suri K, Nagra PK, Hammersmith KM. Comparative evaluation of dual Scheimpflug imaging parameters in keratoconus, early keratoconus, and normal eyes. J Cataract Refract Surg. 2014;40(4):582–592. doi:10.1016/j.jcrs.2013.08.061
18. Hashem AO, Aziz BF, Wahba SS, Roshdy MM, Elawamry AI. Diagnostic accuracy of different keratoconus detection indices of pentacam in paediatric eyes. Eye. 2023;37(6):1130–1138. doi:10.1038/s41433-022-02070-x
19. Bae GH, Kim JR, Kim CH, Lim DH, Chung ES, Chung TY. Corneal topographic and tomographic analysis of fellow eyes in unilateral keratoconus patients using pentacam. Am J Ophthalmol. 2014;157(1):103–109.e1. doi:10.1016/j.ajo.2013.08.014
20. Chan TCY, Biswas S, Yu M, Jhanji V. Comparison of corneal measurements in keratoconus using swept-source optical coherence tomography and combined Placido-Scheimpflug imaging. Acta Ophthalmol. 2017;95(6):e486–94. doi:10.1111/aos.13298
21. Dienes L, Kránitz K, Juhász É, et al. Evaluation of intereye corneal asymmetry in patients with keratoconus. A scheimpflug imaging study. PLoS One. 2014;9(10):e108882. doi:10.1371/journal.pone.0108882
22. Henriquez MA, Izquierdo L, Belin MW. Intereye asymmetry in eyes with keratoconus and high ammetropia. Cornea. 2015;34(Supplement 10):S57–S60. doi:10.1097/ICO.0000000000000608
23. Huseynli S, Salgado-Borges J, Alio JL. Comparative evaluation of Scheimpflug tomography parameters between thin non-keratoconic, subclinical keratoconic, and mild keratoconic corneas. Eur J Ophthalmol. 2018;28(5):521–534. doi:10.1177/1120672118760146
24. Jafarinasab MR, Feizi S, Karimian F, Hasanpour H. Evaluation of corneal elevation in eyes with subclinical keratoconus and keratoconus using Galilei double Scheimpflug analyzer. Eur J Ophthalmol. 2013;23(3):377–384. doi:10.5301/ejo.5000226
25. Kataria P, Padmanabhan P, Gopalakrishnan A, Padmanaban V, Mahadik S, Ambrósio R. Accuracy of Scheimpflug-derived corneal biomechanical and tomographic indices for detecting subclinical and mild keratectasia in a South Asian population. J Cataract Refract Surg. 2019;45(3):328–336. doi:10.1016/j.jcrs.2018.10.030
26. Kosekahya P, Koc M, Caglayan M, Kiziltoprak H, Atilgan CU, Yilmazbas P. Repeatability and reliability of ectasia display and topometric indices with the Scheimpflug system in normal and keratoconic eyes. J Cataract Refract Surg. 2018;44(1):63–70. doi:10.1016/j.jcrs.2017.10.042
27. Kovács I, Miháltz K, Ecsedy M, Németh J, Nagy ZZ. The role of reference body selection in calculating posterior corneal elevation and prediction of keratoconus using rotating Scheimpflug camera. Acta Ophthalmol. 2011;89(3):e251–6. doi:10.1111/j.1755-3768.2010.02053.x
28. Değirmenci C, Palamar M, Ismayilova N, Eğrilmez S, Yağcı A. Topographic evaluation of unilateral keratoconus patients. Turk J Ophthalmol. 2019;49(3):117–122. doi:10.4274/tjo.galenos.2018.90958
29. Henriquez MA, Izquierdo L, Mannis MJ. Intereye asymmetry detected by scheimpflug imaging in subjects with normal corneas and keratoconus. Cornea. 2013;32(6):779–782. doi:10.1097/ICO.0b013e31827b14ae
30. Huseynova T, Abdulaliyeva F, Lanza M. Comparison of scheimpflug imaging parameters between steep and keratoconic corneas of caucasian eyes. Clinical Ophthalmology. 2016;603. doi:10.2147/OPTH.S102683
31. Krumeich JH, Daniel J, Knülle A. Live-epikeratophakia for keratoconus. J Cataract Refract Surg. 1998;24(4):456–463. doi:10.1016/S0886-3350(98)80284-8
32. Koc M, Tekin K, Kiziltoprak H, et al. Topometric and tomographic evaluation of subclinical keratoconus. Ophthalmic Epidemiol. 2020;27(4):289–297. doi:10.1080/09286586.2020.1741010
33. L LIM, Tan G, Hla Myint H, Lim HB. Comparison of keratometric and pachymetric parameters with Scheimpflug imaging in normal and keratoconic Asian eyes. Clinical Ophthalmology. 2014;8:2215. doi:10.2147/OPTH.S66598
34. Liu Y, Zhang Y, Chen Y. Application of a scheimpflug-based biomechanical analyser and tomography in the early detection of subclinical keratoconus in Chinese patients. BMC Ophthalmol. 2021;21(1):339. doi:10.1186/s12886-021-02102-2
35. Miháltz K, Kovács I, Takács Á, Nagy ZZ. Evaluation of keratometric, pachymetric, and elevation parameters of keratoconic corneas with pentacam. Cornea. 2009;28(9):976–980. doi:10.1097/ICO.0b013e31819e34de
36. Naderan M, Rajabi MT, Zarrinbakhsh P. Intereye asymmetry in bilateral keratoconus, keratoconus suspect and normal eyes and its relationship with disease severity. Bri J Ophthalmol. 2017;101(11):1475–1482. doi:10.1136/bjophthalmol-2016-309841
37. Nicula CA, Bulboacă AE, Nicula D, Nicula AP, Horvath KU, Bolboacă SD. Performances of corneal topography and tomography in the diagnosis of subclinical and clinical keratoconus. Front Med Lausanne. 2022;9. doi:10.3389/fmed.2022.904604
38. Uçakhan ÖÖ, Çetinkor V, Özkan M, Kanpolat A. Evaluation of Scheimpflug imaging parameters in subclinical keratoconus, keratoconus, and normal eyes. J Cataract Refract Surg. 2011;37(6):1116–1124. doi:10.1016/j.jcrs.2010.12.049
39. Orucoglu F, Toker E. Comparative analysis of anterior segment parameters in normal and keratoconus eyes generated by scheimpflug tomography. J Ophthalmol. 2015;2015:1–8. doi:10.1155/2015/925414
40. Shen Y, Xian Y, Han T, Wang X, Zhou X. Bilateral differential topography—a novel topographic algorithm for keratoconus and ectatic disease screening. Front Bioeng Biotechnol. 2021;9. doi:10.3389/fbioe.2021.772982
41. Chan TC, Wang YM, Yu M, Jhanji V. Comparison of corneal dynamic parameters and tomographic measurements using Scheimpflug imaging in keratoconus. Br J Ophthalmol. 2018;102(1):42–47. doi:10.1136/bjophthalmol-2017-310355
42. Shetty R, Rao H, Khamar P, et al. Keratoconus screening indices and their diagnostic ability to distinguish normal from ectatic corneas. Am J Ophthalmol. 2017;181:140–148. doi:10.1016/j.ajo.2017.06.031
43. Steinberg J, Aubke‐Schultz S, Frings A, et al. Correlation of the KISA% index and Scheimpflug tomography in ‘normal’, ‘subclinical’, ‘keratoconus‐suspect’ and ‘clinically manifest’ keratoconus eyes. Acta Ophthalmol. 2015;93(3):e199–207. doi:10.1111/aos.12590
44. Ruiseñor Vázquez PR, Galletti JD, Minguez N, et al. Pentacam scheimpflug tomography findings in topographically normal patients and subclinical keratoconus cases. Am J Ophthalmol. 2014;158(1):32–40.e2. doi:10.1016/j.ajo.2014.03.018
45. Maldonado MJ, Nieto JC, Piñero DP. Advances in technologies for laser-assisted in situ keratomileusis (LASIK) surgery. Expert Rev Med Devices. 2008;5(2):209–229. doi:10.1586/17434440.5.2.209
46. Piñero DP. Technologies for anatomical and geometric characterization of the corneal structure and anterior segment: a review. Semin Ophthalmol. 2015;30(3):161–170. doi:10.3109/08820538.2013.835844
47. Piñero DP, Nieto JC, Lopez-Miguel A. Characterization of corneal structure in keratoconus. J Cataract Refract Surg. 2012;38(12):2167–2183. doi:10.1016/j.jcrs.2012.10.022
48. Ambrósio R, Valbon BF, Faria-Correia F, Ramos I, Luz A. Scheimpflug imaging for laser refractive surgery. Curr Opin Ophthalmol. 2013;24(4):310–320. doi:10.1097/ICU.0b013e3283622a94
49. Cavas-Martínez F, De la Cruz Sánchez E, Nieto Martínez J, Fernández Cañavate FJ, Fernández-Pacheco DG. Corneal topography in keratoconus: state of the art. Eye and Vision. 2016;3(1):5. doi:10.1186/s40662-016-0036-8
50. Cui J, Zhang X, Hu Q, Zhou WY, Yang F. Evaluation of corneal thickness and volume parameters of subclinical keratoconus using a Pentacam Scheimflug system. Curr Eye Res. 2016;41(7):923–926. doi:10.3109/02713683.2015.1082188
51. Gomes JAP, Tan D, Rapuano CJ, et al. Global Consensus on Keratoconus and Ectatic Diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
52. McGhee CNJ, Kim BZ, Wilson PJ. Contemporary treatment paradigms in keratoconus. Cornea. 2015;34(Supplement 10):S16–23. doi:10.1097/ICO.0000000000000504
53. Schlegel Z, Hoang-Xuan T, Gatinel D. Comparison of and correlation between anterior and posterior corneal elevation maps in normal eyes and keratoconus-suspect eyes. J Cataract Refract Surg. 2008;34(5):789–795. doi:10.1016/j.jcrs.2007.12.036
54. Montalbán R, Piñero DP, Javaloy J, Alió JL. Scheimpflug photography–based clinical characterization of the correlation of the corneal shape between the anterior and posterior corneal surfaces in the normal human eye. J Cataract Refract Surg. 2012;38(11):1925–1933. doi:10.1016/j.jcrs.2012.06.050
55. Montalbán R, Piñero DP, Javaloy J, Alio JL. Correlation of the corneal toricity between anterior and posterior corneal surfaces in the normal human eye. Cornea. 2013;32(6):791–798. doi:10.1097/ICO.0b013e31827bf898
56. Tomidokoro A, Oshika T, Amano S, Higaki S, Maeda N, Miyata K. Changes in anterior and posterior corneal curvatures in keratoconus. Ophthalmology. 2000;107(7):1328–1332. doi:10.1016/S0161-6420(00)00159-7
57. Li Y, Meisler DM, Tang M, et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology. 2008;115(12):2159–2166. doi:10.1016/j.ophtha.2008.08.004
58. Owens H, Watters GA. An evaluation of the keratoconic cornea using computerised corneal mapping and ultrasonic measurements of corneal thickness. Ophthalmic Physiol Opt. 1996;16(2):115–123. doi:10.1046/j.1475-1313.1996.95000178.x
59. Avitabile T, Marano F, Uva MG, Reibaldi A. Evaluation of central and peripheral corneal thickness with ultrasound biomicroscopy in normal and keratoconic eyes. Cornea. 1997;16(6):639–644. doi:10.1097/00003226-199711000-00007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Descemetic Deep Anterior Lamellar Keratoplasty versus Penetrating Keratoplasty in Advanced Keratoconus: Comparison of Visual and Refractive Outcomes
Spadea L, Di Genova L, Trovato Battagliola E, Scordari S
Therapeutics and Clinical Risk Management 2024, 20:127-138
Published Date: 16 February 2024
AvaGen Genetic Testing versus Ocular Screening Assessments Including the Keratoconus Severity Score (KSS) and Randleman Ectasia Risk Score System (ERSS) in Refractive Surgery Candidates
Moshirfar M, Pandya S, Zhang S, Stoakes IM, Ayesha A, Hoopes PC
Clinical Ophthalmology 2024, 18:1245-1255
Published Date: 7 May 2024