Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 7
Scanning electron microscopy analysis of the growth of dental plaque on the surfaces of removable orthodontic aligners after the use of different cleaning methods
Authors Levrini L ![]() , Novara F, Margherini S, Tenconi C, Raspanti M
, Novara F, Margherini S, Tenconi C, Raspanti M
Received 5 September 2015
Accepted for publication 13 October 2015
Published 15 December 2015 Volume 2015:7 Pages 125—131
DOI https://doi.org/10.2147/CCIDE.S95814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Luca Levrini, Francesca Novara, Silvia Margherini, Camilla Tenconi, Mario Raspanti
Department of Surgical and Morphological Sciences, Dental Hygiene School, Research Centre Cranio Facial Disease and Medicine, University of Insubria, Varese, Italy
Background: Advances in orthodontics are leading to the use of minimally invasive technologies, such as transparent removable aligners, and are able to meet high demands in terms of performance and esthetics. However, the most correct method of cleaning these appliances, in order to minimize the effects of microbial colonization, remains to be determined.
Purpose: The aim of the present study was to identify the most effective method of cleaning removable orthodontic aligners, analyzing the growth of dental plaque as observed under scanning electron microscopy.
Methods: Twelve subjects were selected for the study. All were free from caries and periodontal disease and were candidates for orthodontic therapy with invisible orthodontic aligners. The trial had a duration of 6 weeks, divided into three 2-week stages, during which three sets of aligners were used. In each stage, the subjects were asked to use a different method of cleaning their aligners: 1) running water (control condition); 2) effervescent tablets containing sodium carbonate and sulfate crystals followed by brushing with a toothbrush; and 3) brushing alone (with a toothbrush and toothpaste). At the end of each 2-week stage, the surfaces of the aligners were analyzed under scanning electron microscopy.
Results: The best results were obtained with brushing combined with the use of sodium carbonate and sulfate crystals; brushing alone gave slightly inferior results.
Conclusion: On the basis of previous literature results relating to devices in resin, studies evaluating the reliability of domestic ultrasonic baths for domestic use should be encouraged. At present, pending the availability of experimental evidence, it can be suggested that dental hygienists should strongly advise patients wearing orthodontic aligners to clean them using a combination of brushing and commercially available tablets for cleaning oral appliances.
Keywords: scanning electron microscopy, orthodontic appliances, oral hygiene, biofilm, clear aligners
Introduction
Treatment with fixed orthodontic devices such as brackets and bands creates numerous sites of plaque accumulation which may reduce the effectiveness of oral hygiene procedures and thus potentially lead to the development of white spot lesions, caries, and periodontitis.1–3 By contrast, the use of removable orthodontic appliances, particularly invisible aligners, allows adequate oral hygiene and can reduce the risk of these dental and periodontal complications.4–6 From the perspective of the protection of periodontal health, this is an important consideration, especially given the marked increase in the use of new digital technologies in orthodontics.
It is crucial to ensure that removable orthodontic aligners are clean before being inserted in order to prevent bacteria from building up on their surface and constituting a vehicle of infection for the oral cavity. Indeed, these devices can induce changes in the ecosystem of the oral cavity, which, in turn, can increase the risk of oral diseases, such as periodontal disease, halitosis, and caries lesions caused by bacterial growth. For this reason, they need to be thoroughly cleaned and disinfected daily.
The aim of the present study was to identify the most effective method of cleaning removable orthodontic aligners by comparing the growth of dental plaque observed under scanning electron microscopy (SEM) following the use of three different appliance-cleaning methods: 1) running water; 2) effervescent tablets containing sodium carbonate and sulfate crystals; and 3) toothbrush and toothpaste. This research, prompted by the lack of literature data on this topic, was intended to provide a simple SEM evaluation of aligners before and after wear and to confirm that they are subject to contamination by bacterial biofilm (Figure 1).
 | Figure 1 Clean orthodontic aligner not yet worn (A), after 2 weeks of use (B), and observed at higher magnification (C), observed under scanning electron microscopy. |
Materials and methods
Twelve subjects (six male and six female) aged between 19 and 24 years, with good oral and systemic health, and no caries or periodontal disease, all candidates for orthodontic treatment with removable orthodontic aligners, were selected. The clinical trial took place at the Dental Clinic of the University of Insubria in Varese (Italy). All the subjects were instructed to adopt the following domiciliary oral hygiene regime: to use a soft toothbrush with a rolling-action technique, a fluoride toothpaste, and dental floss. The study was carried out in accordance with the principles of the Declaration of Helsinki and in compliance with Good Clinical Practice. The study protocol was approved by the Ospedale di Circolo Fondazione Macchi Varese ethics committee. Before taking part in the study, each patient was required to sign an informed consent form to which was attached a detailed description of the study protocol. Each patient received three series of aligners, each to be worn for 2 weeks, and was asked to use different cleaning procedures over the 6 weeks of their application, as detailed below:
- For the first 2 weeks, the aligners were to be rinsed in cold running water for 15 seconds before being applied in the oral cavity and this procedure was to be repeated at least twice a day (water group).
- For the second 2 weeks, all the participants were asked to clean their appliances daily for at least 30 minutes by soaking them in cold water in which effervescent tablets containing sodium carbonate and sulfate (Invisalign® Cleaning System, Align Technology, San Jose, CA, USA) had been dissolved. Before wearing the aligners, the patients were also instructed to brush them for at least 30 seconds with a soft toothbrush and toothpaste with a relative dentin abrasion value of less than 150 (tablet and brushing group).
- For the last 2 weeks, all the participants were required to brush their aligners for at least 30 seconds with a soft toothbrush and toothpaste with a relative dentin abrasion value of less than 150 (brushing group).
At the end of each 2-week stage, SEM analysis was carried out. This was conducted at the Laboratory of Human Morphology, University of Insubria. In particular, the outer surface of the aligners at level of the interdental papilla between teeth 1.3 and 1.4, and the internal surface at the level of the cusps of 1.3 and 1.4 were analyzed. All samples were air-dried, reduced in size around the 1.3–1.4 region, mounted on standard SEM stubs with conductive carbon-based adhesive, and gold coated in an Emitech K-550 sputter-coater (Emitech Ltd, Ashford, UK) in a controlled argon atmosphere at a pressure of 1×10–1 mbar. All observations were carried out on a FEI XL-30 FEG field emission scanning electron microscope (FEI, Eindhoven, the Netherlands) operated at an acceleration voltage of 7 kV. All pictures were obtained directly in digital form as 1,424×968 pixel, 8 bpp grayscale TIFF images, and were subsequently hand-painted in false color in order to highlight their main features.
Results
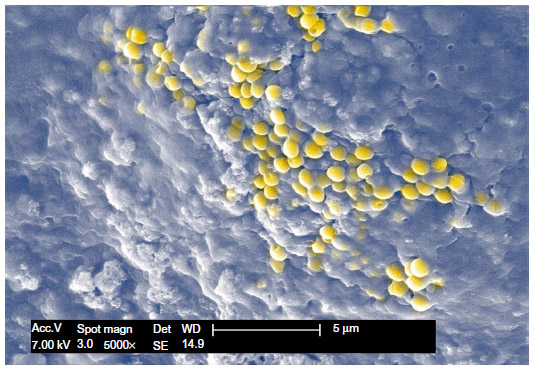
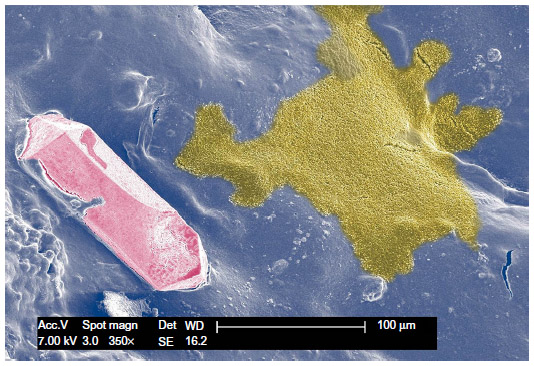
On analysis under SEM, the external surfaces of the aligners in the tablet and brushing group were found to be much cleaner, after treatment, than those of the uncleaned specimens (water group), while those of the aligners regularly treated with toothpaste and a toothbrush (brushing group) were cleaner still. Analysis of the internal surfaces instead revealed no appreciable differences between the three groups. It must be stressed, however, that all the specimens retained a degree of contamination on both surfaces. In all cases, the microbiological contamination was mostly organic, with occasional findings of inorganic, crystalline tartar (Figure 2). The bacterial presence apparently consisted of a single species of spheroidal microorganisms, ~2/3 of a micron in diameter and growing in immense colonies (Figure 3). The present morphological evaluation is not sufficient for a reliable classification. We infrequently obtained a clear view of these colonies because as soon as they grow into a confluent layer they cover themselves with an amorphous substance (Figure 4), forming a continuous film (Figure 5). This was especially evident on the interior surfaces of the aligners, which are more difficult to clean, being concave and also presenting tiny steps left by the manufacturing process. During the dehydration treatment, which is mandatory for high-resolution SEM, the bacterial film shrinks, cracks, and peels away from the surface of the specimen, at times remaining only in sparse patches (Figure 6). This is a common artifact and is easily recognized as such.
 | Figure 2 Scanning electron microscopy micrograph of the internal surface of an Invisalign specimen, treated with crystal cleaning tablets. |
 | Figure 3 Another location of the same specimen, occupied by an immense bacterial colony. |
 | Figure 4 A higher magnification image of a thinner bacterial film found on the external surface of a specimen cleaned by brushing. |
 | Figure 5 A bacterial colony (yellow) actively growing prior to becoming part of a preexisting biofilm (blue). |
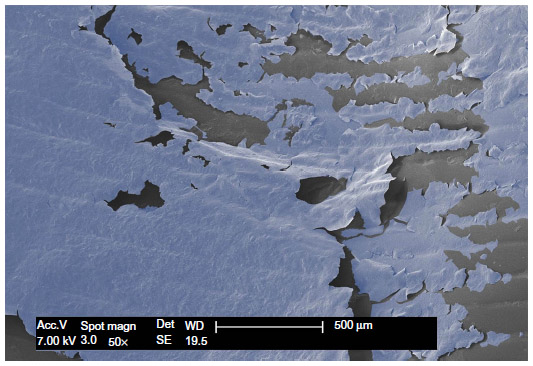 | Figure 6 The inner surface of a specimen cleaned only with water. |
Discussion
Patients today are tending to attach more and more importance to esthetic aspects and concerns, with the result that we are seeing an increase in the use of invisible orthodontic aligners, even in patients with only moderate malocclusions. In this setting, the dental hygienist has an important role to play, carrying out professional oral hygiene procedures with scrupulous care, giving correct instructions on domiciliary oral hygiene routines, and evaluating the use of electric toothbrushes and other useful devices.7–10 It is equally important to give patients a detailed take-home hygiene routine for appliances that are worn in the oral cavity, especially orthodontic aligners which are now very widely used. Proper cleaning of orthodontic aligners is important not only to prevent bacteria from getting into the oral cavity, but also to ensure that these appliances, chosen also for esthetic reasons and therefore meant to be attractive, remain bright and odor-free over time.
In this regard, the literature currently contains no data that indicate, beyond doubt, the best procedure to use for invisible aligners. As a result, orthodontists and dental hygienists suggest different methods on the basis of their own experience: toothbrush and toothpaste, effervescent tablets, and even somewhat bizarre methods, such as the use of washing up liquid, vinegar, or descaling products.
Batoni et al11 studied the effects of oral colonization by mutans streptococci in subjects wearing removable acrylic resin orthodontic appliances. They evaluated the frequency of isolation and serotype distribution of S. mutans in saliva in two groups of children: one group being treated with the removable appliances and the other group not undergoing any orthodontic treatment. The rate of bacterial colonization by S. mutans was found to be greater in the treated children due to the presence of numerous areas of plaque retention and the structure of the appliance; these results show that it is important to monitor the cleanliness of removable orthodontic devices in order to reduce the risk of onset and development of oral diseases.
Poor aligner hygiene can result in pigmentation of appliances, causing them to lose their gloss and transparency. A study of Invisalign appliances, performed to assess and document their short-term chemical and physical changes with use, showed that they underwent both morphological and structural changes. Aligners worn for 14 days showed microcracks, abraded and delaminated areas, localized calcified biofilm deposits, and loss of transparency. These changes are a precondition for bacterial contamination both of aligners and other removable orthodontic appliances.12 The colonization susceptibility of invisible aligners was recently documented in an SEM study conducted by Low et al13 who observed the presence of biofilm with a complex structure and greater biofilm accumulation in more recessed and sheltered areas of the appliance, such as the cusp tips and attachment dimples.
Although there currently exists no single method that can be considered able to reliably guarantee the hygiene of removable orthodontic devices, a recent study evaluated the effectiveness of three different cleansing methods, considering, among other factors, their ability to inhibit colonization of the surfaces of aligners. The study included two experimental stages: one performed in vitro to evaluate the ability of the removable thermoplastic appliance (RTA) to adsorb hygienic solution and inhibit bacterial growth in culture, and the other performed in vivo to examine the efficacy of three hygiene protocols in reducing bacterial biofilm adherence to RTAs. In this study, the RTA-treated patients were required to follow a sequence of three hygiene protocols: regular RTA brushing (baseline), immersion of RTAs in chlorhexidine (CHX) mouthwash, and use of a vibrating bath with cleaning solution. From the results of the in vitro analysis, it was deduced that the thermoplastic appliances lacked the ability to adsorb CHX or cleaning solution used for the purpose of reducing bacterial colonization of the appliances. In the in vivo stage, all the RTAs were stained with gentian violet, and biofilm presence was measured using a photodensitometer. The results showed that the CHX and vibrating bath with cleaning solution hygiene protocols significantly (P<0.001) reduced baseline biofilm adherence, by 16% and 50% respectively, with the vibrating bath with cleaning solution treatment found to be three times more efficient than CHX.14
Similar trials have been conducted on removable devices made from acrylic resin. Dietrich analyzed the microbial population on removable orthodontic appliances after three different hygiene procedures: brushing with a toothbrush and toothpaste, use of a self-acting cleansing agent, and ultrasound treatment. Bacterial colonization and the effects of these three procedures were evaluated using SEM. The results showed that use of a toothbrush and toothpaste alone did not allow adequate decontamination of the device, whereas ultrasound treatment was a very effective means of removing plaque buildup in certain areas. However, it was deduced that none of these procedures led to complete decontamination of the removable appliances.15 Faria et al,16 to test the reduction of bacterial biofilm on the surface of oral appliances and the quantity of S. mutans in saliva, compared three groups of individuals undergoing orthodontic treatment with removable acrylic resin appliances; in one group, the appliances underwent no cleansing procedure, in another they were immersed in a solution containing 0.12% CHX, while a third group of subjects wore appliances with 0.12% CHX incorporated into the acrylic resin. The results were not statistically significant, with no differences emerging between the three groups. In another study of methods for cleaning removable acrylic resin appliances, a spray containing 0.05% cetylpyridinium chloride was compared with one containing 0.12% CHX. Analysis of S. mutans colonization, by means of microbial culture and SEM, showed that both sprays were effective in reducing the bacterial load.17 Peixoto et al also used microbiological analysis and SEM to study the quantity of S. mutans on the surfaces of removable orthodontic appliances. The study involved a 3-week cycle, with 1-week intervals between the weeks. During each week, three groups of subjects each followed a different appliance-cleaning protocol: 1) toothbrushing + baseplate brushing + sterile tap water spraying once a day; 2) toothbrushing + baseplate brushing + spraying with a 0.20% CHX-based solution on the seventh day after appliance placement; and 3) toothbrushing + baseplate brushing + spraying with a 0.20% CHX-based solution on the fourth and seventh days after appliance placement. At the end of each week, the bacterial load of three randomly chosen appliances, one for each cleaning protocol, was analyzed under SEM. Bacterial biofilm was detected on the surfaces of all the devices; the quantity of S. mutans on the surfaces treated with 0.12% CHX spray was lower than the prevalence of S. mutans detected on the H2O spray-treated surfaces and no significant difference was found between the two CHX spay protocols.18
All these literature studies demonstrate, both through microbiological cultures and analysis under SEM, the formation of bacterial microfilm on the surfaces of removable appliances in acrylic resin, and also give consistent results as regards the use of CHX-based sprays or solutions, which are found to lead to a reduction of the total bacterial load on these surfaces.
In clinical practice, therefore, it is crucial that any orthodontic appliance inserted into the oral cavity is clean and free from bacteria.
The results of the present study show that use of effervescent tablets containing sodium carbonate and sulfate, combined with brushing, was found to be the best procedure, nevertheless failed to completely clean the surfaces of the orthodontic aligners; biofilm continued to be present to a minor degree and in particular on the internal surfaces, and this could give rise to different problems: discoloration of the aligners, an unpleasant odor, and synergistic interaction with bacteria already present in the oral cavity. The fact that bacteria continue to be present on the internal surfaces in particular might be due to the fact that patients tend to pay more attention to cleaning the external surfaces of their aligners. In view of this, it is clearly important that patients, on receiving these appliances, should be strongly urged by the dental hygienist to pay due attention to cleaning their internal surfaces.
Simple brushing with toothpaste nevertheless gave excellent results; biofilm, whether oral or present on an orthodontic appliance, has to be mechanically broken down in order to be removed. The result is improved by the additional use of effervescent tablets, although this makes the procedure more difficult, more time consuming, and more expensive. Brushing alone, without the use of any active chemical principle, has been found to favor the accumulation of biofilm on dentures; basically, it is always necessary to combine the mechanical action (exerted by the brush) with a chemical one.19,20 It would be worth attempting to identify the blend of cleansing agents and surfactants best able to chemically reduce the bacterial load and the formation of deposits on aligners; indeed, toothpastes, on account of their texture and abrasiveness, could affect the gloss and the characteristic transparency of aligners, and thus themselves encourage retention of plaque.
The same considerations also apply to the disinfection of pacifiers and toothbrushes for which spraying with CHX in combination with microwave irradiation has been shown to be effective.21 According to some authors, the mechanical action of ultrasonic devices on dentures may give good results even in the absence of any chemical action.22 Further studies need to be conducted to identify methods that are more rapid, more effective, and less expensive; the studies conducted on dentures may be useful to consider together with those conducted on removable orthodontic appliances made of acrylic resin, but their results are probably not relevant to aligners, which are made of thermoplastic material.
It could be particularly interesting to evaluate the daily use of ultrasonic baths for domestic use, also combining this method with mouth rinses containing CHX or hydrogen peroxide.15,23 Furthermore, given the growing use of prostheses and medical devices, for example, hearing aids, which are designed to remain in prolonged contact with the body and may facilitate infections related to the presence of biofilm bacteria, other suggestions might be derived from the clinical literature.24 Clearly, none of the procedures suggested should reduce the efficacy of the aligners or result in them becoming discolored. It is worth considering that orthodontic aligners, compared with intraoral appliances in orthodontic acrylic resin, have the advantage of being devices that after 2 weeks of use are replaced by new, and thus clean, ones. However, this obviously does not apply to aligners used to maintain the result of an orthodontic treatment (when orthodontic treatment is complete, it is customary to insert appliances designed to prevent relapses). These are usually devices that are similar in structure to orthodontic aligners, but exert no active forces. They can be worn for periods even longer than 6 months and kept in every night; for this reason, the methods used to keep them clean must be particularly scrupulous and effective. In addition to this advantage, it can be remarked that acrylic resin surfaces, compared with the surfaces of thermoplastic aligners, are more porous and present recesses, and may therefore be more susceptible to plaque retention.
Conclusion
The results of this study suggest that brushing associated with the use of effervescent tablets containing sodium carbonate and sulfate is the most effective method of cleaning removable thermoplastic aligners. We believe that these observations, on Invisalign aligners, can be considered useful for all orthodontic aligners; we suggest that different materials and devices methods do not significantly impact on hygiene practices. Further studies should be conducted to qualitatively assess the microbiological changes linked to the alternation of different cleansing methods and evaluate the effectiveness of physical methods, such as ultrasonic baths and of other chemical agents.
Disclosure
The authors report no conflicts of interest in this work.
References
Bollen AM, Cunha-Cruz J, Bakko DW, Huang GJ, Hujoel PP. The effects of orthodontic therapy on periodontal health: a systematic review of controlled evidence. J Am Dent Assoc. 2008;139(4):413–422. | |
Liu H, Sun J, Dong Y, et al. Periodontal health and relative quantity of subgingival Porphyromonas gingivalis during orthodontic treatment. Angle Orthod. 2011;81(4):609–615. | |
Ristic M, Vlahovic Svabic M, Sasic M, Zelic O. Effects of fixed orthodontic appliances on subgingival microflora. Int J Dent Hyg. 2008; 6(2):129–136. | |
Miethke RR, Brauner K. A Comparison of the periodontal health of patients during treatment with the Invisalign system and with fixed lingual appliances. J Orofac Orthop. 2007;68(3):223–231. | |
Levrini L, Abbate GM, Migliori F, Orrù G, Sauro S, Caprioglio A. Assessment of the periodontal health status in patients undergoing orthodontic treatment with fixed or removable appliances. A microbiological and preliminary clinical study. Cumhuriyet Dent J. 2013;16(4):296–307. | |
Abbate GM, Caria MP, Montanari P, et al. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J Orofac Orthop. 2015;76(3):240–250. | |
Migliorati M, Isaia L, Cassaro A, et al. Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: a systematic review. Eur J Orthod. 2015;37(3):297–307. | |
Rafe Z, Vardimon A, Ashkenazi M. Comparative study of 3 types of toothbrushes in patients with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2006;130(1):92–95. | |
Kaklamanos EG, Kalfas S. Meta-analysis on the effectiveness of powered toothbrushes for orthodontic patients. Am J Orthod Dentofacial Orthop. 2008;133(2):187. | |
Costa MR, Marcantonio RA, Cirelli JA. Comparison of manual versus sonic and ultrasonic toothbrushes: a review. Int J Dent Hyg. 2007;5(2):75–81. | |
Batoni G, Pardini M, Giannotti A, et al. Effect of removable orthodontic appliances on oral colonisation by mutans streptococchi in children. Eur J Oral Sci. 2001;109(6):388–392. | |
Gracco A, Mazzoli A, Favoni O, et al. Short-term chemical and physical changes in Invisalign appliances. Aust Orthod J. 2009;25(1):34–40. | |
Low B, Lee W, Seneviratne CJ, Samaranayake LP, Hägg U. Ultrastructure and morphology of biofilms on thermoplastic orthodontic appliances in ‘fast’ and ‘slow’ plaque formers. Eur J Orthod. 2011; 33(5):577–583. | |
Shpack N, Greenstein RB, Gazit D, Sarig R, Vardimon AD. Efficacy of three hygienic protocols in reducing biofilm adherence to removable thermoplastic appliance. Angle Orthod. 2014;84(1):161–170. | |
Dietrich P. Microbial colonization and various cleaning procedures for orthodontic appliances. Fortschr Kieferorthop. 1989;50(3):231–239. | |
Faria G, Santamaria M Jr, Mota dos Santos B, Yoko Ito I, Cinira Bregagnolo J, Sasso Stuani MB. The effect of chlorhexidine on plaque index and mutans streptococci in orthodontic patients: a pilot study. Open J Stomatol. 2013;3(6):323–328. | |
Lessa FC, Enoki C, Ito IY, Faria G, Matsumoto MA, Nelson P. In-vivo evaluation of the bacterial contamination and disinfection of acrylic baseplates of removable orthodontic appliances. Am J Orthod Dentofacial Orthop. 2007;132(6):705. | |
Peixoto IT, Enoki C, Ito IY, Matsumoto MA, Nelson-Filho P. Evaluation of home disinfection protocols for acrylic baseplates of removable orthodontic appliances: a randomized clinical investigation. Am J Orthod Dentofacial Orthop. 2011;140(1):51–57. | |
Shay K. Denture hygiene: a review and update. J Contemp Dent Pract. 2000;1(2):28–41. | |
Paranhos HF, Silva-Lovato CH, Souza RF, Cruz PC, Freitas KM, Peracini A. Effects of mechanical and chemical methods on denture biofilm accumulation. J Oral Rehabil. 2007;34(8):606–612. | |
Nelson-Filho P, Da Silva LA, Da Silva RA, da Silva LL, Ferreira PD, Ito IY. Efficacy of microwaves and chlorhexidine on the disinfection of pacifiers and toothbrushes: an in vitro study. Pediatr Dent. 2011;33(1):10–13. | |
Cruz PC, Andrade IM, Peracini A, et al. The effectiveness of chemical denture cleansers and ultrasonic device in biofilm removal from complete dentures. J Appl Oral Sci. 2011;19(6):668–673. | |
Palenik CJ, Miller CH. In vitro testing of three denture-cleaning systems. J Prosthet Dent. 1984;51(6):751–754. | |
Vergidis P, Patel R. Novel approaches to the diagnosis, prevention, and treatment of medical device-associated infections. Infect Dis Clin North Am. 2012;26(1):173–186. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.