Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
Scabies increased the risk and severity of COPD: a nationwide population-based study
Authors Chen J ![]() , Liu J
, Liu J ![]() , Chang F
, Chang F ![]() , Chang H, Cheng K, Yeh C, Wei Y
, Chang H, Cheng K, Yeh C, Wei Y ![]() , Hsu R
, Hsu R ![]()
Received 3 June 2016
Accepted for publication 10 August 2016
Published 9 September 2016 Volume 2016:11(1) Pages 2171—2178
DOI https://doi.org/10.2147/COPD.S114256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jung-Yueh Chen,1,* Jui-Ming Liu,2,* Fung-Wei Chang,3 Hung Chang,4,5 Kuan-Chen Cheng,6,7 Chia-Lun Yeh,2 Yu-Feng Wei,1 Ren-Jun Hsu8–10
1Division of Chest Medicine, Department of Internal Medicine, E-DA Hospital, I-Shou University, Kaohsiung, 2Division of Urology, Department of Surgery, Taoyuan General Hospital, Ministry of Health and Welfare, Taoyuan, 3Department of Obstetrics & Gynecology, Tri-Service General Hospital, National Defense Medical Center, Taipei, 4Division of Thoracic Surgery, Department of Surgery, Taichung Armed Forces General Hospital, Taichung, 5Department of Physiology, National Defense Medical Center, 6Graduate Institute of Food Science and Technology, National Taiwan University, 7Institute of Biotechnology, National Taiwan University, 8Graduate Institute of Life Sciences, National Defense Medical Center, 9Department of Pathology, Graduate Institute of Pathology and Parasitology, Tri-Service General Hospital, National Defense Medical Center, 10Biobank Management Center, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
*These authors contributed equally to this work
Background: Scabies is a common parasitic infectious disease, and COPD is a major pulmonary disease. However, there have been no previous studies that have investigated the relationship between scabies and COPD.
Materials and methods: This nationwide population-based study included a total of 3,568 patients with scabies as the study group and 14,255 patients as a control group. We followed up patients in both groups for a 5-year period to identify any new diagnoses of COPD. We then followed them up for an additional 2-year period to determine the severity of any newly diagnosed cases of COPD as indicated by acute respiratory events. Cox proportional hazard regression analyses were performed to calculate the hazard ratio (HR) of COPD during the 5-year follow-up period and COPD complication during the additional 2-year follow-up period.
Results: Of the 17,823 patients in the study, 2,765 (15.5%) were newly diagnosed with COPD during the 5-year follow-up period; 904 (32.7%) were from the scabies group; and 1,861 (67.3%) were from the control group. Compared to the patients without scabies, the adjusted HR (aHR) for COPD for the subjects with scabies was 1.72 (95% CI: 1.59–1.87) during the 5-year follow-up period. For those newly diagnosed with COPD, the aHR for COPD with acute exacerbation was 1.85 (95% CI: 1.67–2.06), the aHR for COPD with pneumonia was 3.29 (95% CI: 2.77–3.92), the aHR for COPD with acute respiratory failure was 4.00 (95% CI: 3.08–5.19), and the aHR for COPD with cardiopulmonary arrest was 3.95 (95% CI: 2.25–6.95) during the additional 2-year follow-up period.
Conclusion: The results of this study indicate a 72% increased risk for COPD among patients with scabies. The results also reveal an increased risk of severe COPD complications such as acute respiratory failure, cardiopulmonary arrest, pneumonia, and acute exacerbation among patients with scabies. This useful information may help physicians in treating scabies and remaining alert to the potential development of COPD and its severe complications.
Keywords: scabies, chronic obstructive pulmonary disease, National Health Insurance Research Database
Introduction
Scabies is a common parasitic infectious disease that is caused by the mite Sarcoptes scabiei.1 The worldwide prevalence of scabies infection is ~300 million cases per year.2 The typical clinical findings of scabies are generalized itching skin, erythematous papules, and burrows.3 Men and women are infected with scabies at similar rates. Pannell et al4 reviewed 5 million patients in England who had been followed up for 10 years and found that the incidence of scabies was 351 per 100,000 person-years among men and 437 per 100,000 person-years among women. Scabies is mostly transmitted from person to person through skin-to-skin contact. There are many factors that affect the spread of scabies, including age, overcrowding, hygiene, socioeconomic status, and season.5 Scabies is most common in young children and also relatively common among the elderly5 and during winter.6
COPD is a major cause of morbidity and mortality worldwide7 and is expected to become the third leading cause of death by 2020.8 A recent epidemiological survey found that the prevalence of COPD in Taiwan is 6.1%.9 COPD is characterized by persistent airflow limitation that is usually progressive. A chronic inflammatory response to the presence of noxious particles or gases in the airways is the main pathogenesis of such airflow limitation.10 Tobacco smoking, occupational pollution, and indoor air pollution are major risk factors for COPD.11 The rates of morbidity and mortality due to COPD increase with age.12 Previous studies had found that the prevalence of COPD was greater among men than among women, but more recent data from developed countries have indicated that the prevalence of COPD is roughly equal among men and women.13 The symptoms of COPD are often worse in winter because bronchospasms can be easily induced by cold weather and airway infections. Frequent acute exacerbations of COPD have been found to be correlated with the deterioration of pulmonary function and elevated mortality.14
Scabies and COPD exacerbations are more common in the winter. Wang et al15 conducted a study of risk factors for scabies in Taiwan and showed that 5.7% of patients with scabies also had COPD. A review of the English literature on PubMed indicated that there have been no other previous reports discussing the connection between scabies and COPD. As such, the present 14-year nationwide population-based study was intended to, 1) evaluate the relationship between scabies and COPD, and 2) determine whether there is a relationship between scabies and the severity of COPD.
Materials and methods
Data source and collection
This study is a retrospective population-based study using data from Taiwan’s National Health Insurance Research Database (NHIRD). The NHIRD is a huge database that contains data from the National Health Insurance (NHI) program. The NHI program is the unique health and medical insurance system of Taiwan, and was started in 1995. As of the end of 2013, the NHI program covered 99.9% of Taiwan’s 23 million residents.16 The NHIRD contains demographic data, medical records, and data on the clinical procedures administered to all inpatients, outpatients, and emergency room patients. We used a sub-dataset of the NHIRD, which is called the Longitudinal Health Insurance Database 2000 (LHID2000). The LHID2000 is a database that contains data for 1 million people randomly selected from the larger NHIRD in 2000. The LHID2000 and NHIRD are similar in terms of demographic data and origin population.17 For this study, we used LHID2000 data covering the period from January 2000 to the end of December 2013. The clinical diagnoses for the patients in the database were made according to the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM).18 This retrospective study was approved by the Institutional Review Board of the Tri-Service General Hospital (approval number: TSGHIRB B-105-06). As this was a retrospective study and all data was anonymous, the Institutional Review Board department agreed with the authors that it was not necessary to obtain patient consent.
Study population
The study subjects were selected using LHID2000 data from January 2001 to December 2006. The patients who were newly diagnosed with scabies infection (ICD-9-CM: 133.0) between 2001 and 2006 were enrolled in this study (Figure 1). The scabies infection diagnoses were made by licensed physicians. The exclusion criteria in this study were as follows: 1) patients who were diagnosed before January 1, 2001 (n=1,425), 2) patients who were younger than 40 years (n=5,510), 3) patients who had a previous history of scabies or COPD (n=1,341), and 4) patients with incomplete medical records (n=113). A total of 3,568 patients with scabies infection were ultimately enrolled in the study group.
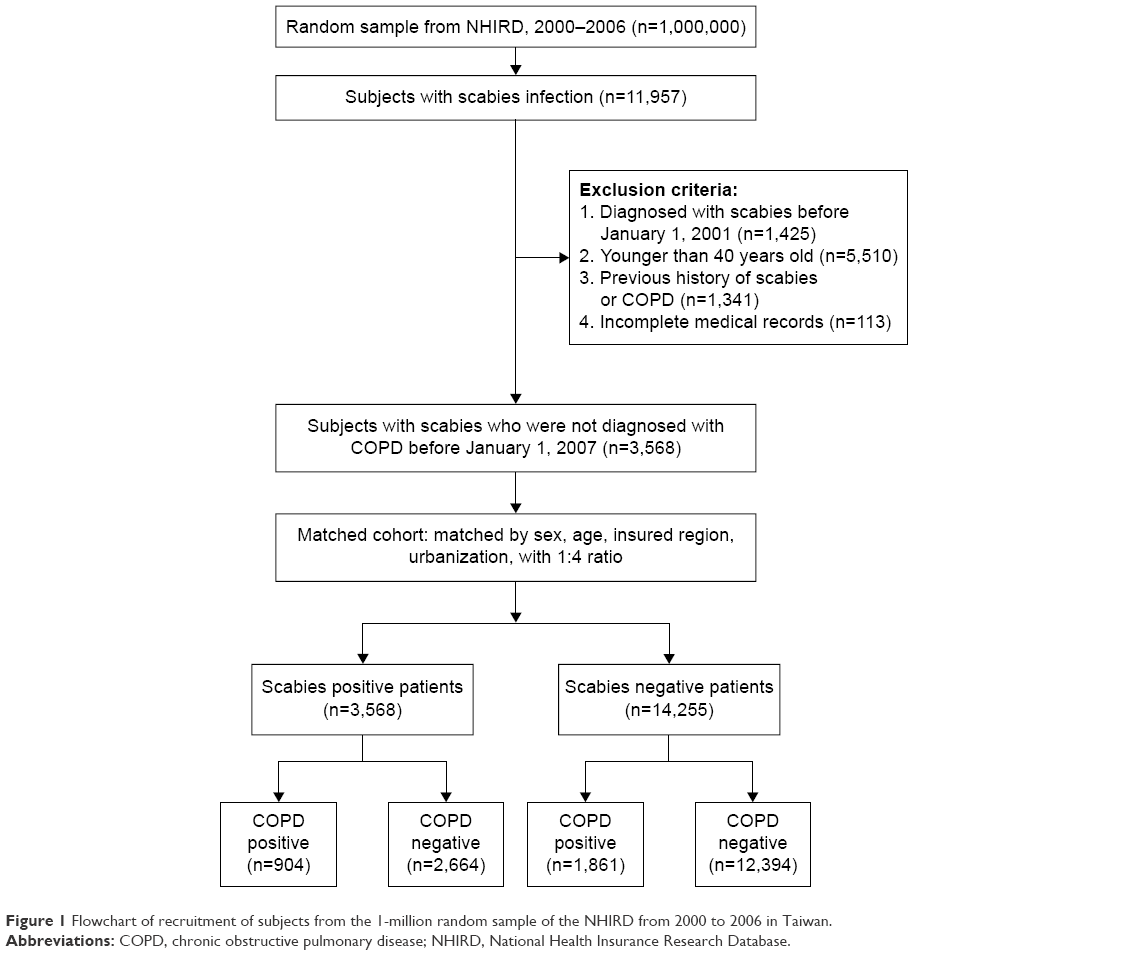 | Figure 1 Flowchart of recruitment of subjects from the 1-million random sample of the NHIRD from 2000 to 2006 in Taiwan. |
The control group was determined by matching with the study group with regard to gender, age, insured region, and urbanization at a ratio of 1:4 (one study group patient to four control group patients). Ultimately, there were 14,255 subjects enrolled in the control group. For the patients in the study group, each patient’s date of diagnosis of scabies was assigned as the index date and considered the starting point for the investigation of that patient, whereas for the control group, the year of the index date was a matched year in which the control subjects had utilized a medical service.
Outcomes
There were 17,823 subjects in this study, with 3,568 patients in the study group and 14,255 patients in the control group. Each subject was followed up for a 5-year period starting with their index date to identify those who were newly diagnosed with COPD (ICD-9-CM: 491, 492, and 496) during that time. We also followed up those who were diagnosed with COPD during the initial 5-year period for an additional 2-year period to determine the severity of their COPD and whether they suffered from acute respiratory events subsequent to being diagnosed with COPD. The primary outcome of this study was the number of patients in each group who were diagnosed with COPD. The secondary outcomes of this study were the numbers of patients in each group who suffered acute respiratory events complicated by COPD including acute exacerbation (ICD-9-CM: 491, 492, and 496), pneumonia (ICD-9-CM: 480–486), acute respiratory failure (ICD-9-CM: 518.81), and cardiopulmonary arrest (ICD-9-CM: 799.1, 798, and 427.5).
All the medical diagnoses of the patients, as well as any procedures and drugs administered to them, were recorded completely during the follow-up period. Each diagnosis of COPD (ICD-9-CM: 491, 492, and 496) was made by chest physicians based on at least two outpatient department visits or at least one admission during the follow-up period. The clinical diagnosis of COPD was made according to typical symptoms such as chronic cough, dyspnea, and sputum production; exposure to risk factors such as tobacco smoking, occupational pollution, and indoor air pollution; and on the basis of spirometry test results.11 Patients with diagnoses of COPD without pulmonary function tests were excluded.
The diagnoses of acute respiratory events subsequent to COPD including pneumonia (ICD-9-CM: 480–486), acute exacerbation (ICD-9-CM: 491, 492, and 496), acute respiratory failure (ICD-9-CM: 518.81), and cardiopulmonary arrest (ICD-9-CM: 799.1, 798, and 427.5) were also done by chest physicians, cardiologists, or emergency physicians based on emergency room and admission records during the follow-up period. We selected patients older than 40 years due to the prevalence of COPD being extremely low in patients younger than 40 years.12
The diagnosis of scabies (ICD-9-CM: 133.0) was made by licensed physicians based on the patient’s history and physical examinations. Typical findings for scabies include generalized itching sparing the face, severe pruritus (especially at night), inflammatory pruritic papules, burrows, and nodules.3
Variables
The selected variables of comorbidities in this study were diabetes mellitus (DM, ICD-9-CM: 250), hypertension (HTN, ICD-9-CM: 401–405), congestive heart failure (CHF, ICD-9-CM: 428), coronary heart disease (CHD, ICD-9-CM: 410–414), chronic kidney disease (CKD, ICD-9-CM: 585, 586, and 588), and osteoporosis (ICD-9-CM: 733.0). The patients were classified into four groups according to age: 40–49 years, 50–59 years, 60–69 years, and older than 70 years. The patients were also categorized into four groups based on their monthly income in New Taiwan Dollars (NTD): < NTD 20,000; NTD 20,000–39,999; NTD 40,000–59,999; and ≥ NTD 60,000. The NHI program is mainly financed by the premiums shared by the insured, employers, and the government. The premiums received by the National Health Insurance Administration are used to help the insured pay for their health care expenses. The aforementioned patients’ income data were provided by the National Health Insurance Administration and are included in NHIRD. The patients were also categorized into seven groups based on their level of urbanization.19 Finally, the patients were also categorized into four groups according to their place of residence in Taiwan: northern region, central region, southern region, and other regions (eastern and outlying islands).
Statistical analysis
All statistical methods were performed using the SPSS software Version 19.0 (IBM Corp, Armonk, NY, USA), and data management was performed using Microsoft® SQL Server® 2008 software (Microsoft Corporation, Redmond, WA, USA). The chi-square test was used for descriptive analyses concerning the distribution of demographic characteristics, income, geography, level of urbanization, and comorbidities between the patients with and without scabies.
We used Cox proportional hazards regression models to estimate the effects of risk factors on the hazard ratios (HRs) accompanying 95% confidence intervals (CIs). All the models were adjusted for the variables (gender, age, income, geography, urbanization, and comorbidities). The level of statistical significance was set at P<0.05 for a two-sided test.
Results
A total of 3,568 patients diagnosed with scabies from January 2001 through December 2006 were enrolled as the study group in this study. After performing matching at a ratio of 1:4 (one study group patient to four control group patients), a total of 17,823 patients were enrolled in the study, including 3,568 patients with scabies and 14,255 control subjects. The mean age of all 17,823 subjects was 59.31±14.21 years. The demographic characteristics of the study group and control group are listed in Table 1. The patients with scabies were mostly middle-aged and residents of Northern Taiwan. HTN, DM, and CHD were the three most common comorbidities among the patients with scabies. There were significantly higher prevalences of DM, HTN, CHF, CHD, and CKD among the patients with scabies than among the control group.
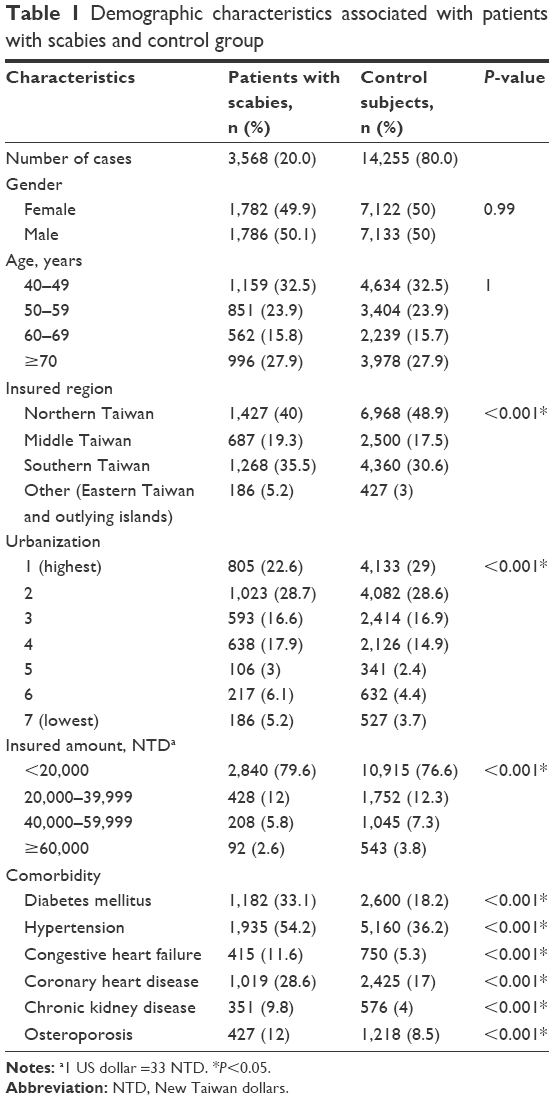 | Table 1 Demographic characteristics associated with patients with scabies and control group |
Table 2 shows the incidence of COPD and the results of the multivariable analysis during the 5-year follow-up for the patients with scabies and the control group. Among 17,823 subjects, 2,765 (15.5%) were diagnosed with COPD during the 5-year follow-up period; 904 (25.3%) were from the scabies group; and 1,861 (13.1%) were from the control group. The incidence rates of COPD were significantly different in the scabies and control groups. There were 904 (25.3%) newly diagnosed COPD patients in the scabies group and 1,861 (13.1%) in the control group. Compared with the control group, the crude HR for COPD for the scabies group was 2.15 (95% CI: 1.98–2.32).
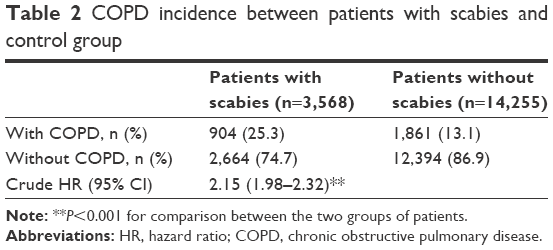 | Table 2 COPD incidence between patients with scabies and control group |
Table 3 shows the Cox regression analysis results for the independent risk factors associated with COPD. After adjusting for gender, age, income, geography, urbanization, and comorbidities, the adjusted HR (aHR) of scabies was 1.72 (95% CI: 1.59–1.87). Male patients (aHR 1.27; 95% CI: 1.18–1.38) had a higher aHR than female patients. In terms of age, the patients aged 40–49 years were used as the reference group. The aHR of the group aged 50–59 years was 1.35 (95% CI: 1.19–1.53), that of the group aged 60–69 years was 1.59 (95% CI: 1.39–1.81), and that of the group older than 70 years was 2.03 (95% CI: 1.80–2.28). HTN (aHR 1.77; 95% CI: 1.62–1.94), CHF (aHR 1.74; 95% CI: 1.56–1.94), CHD (aHR 1.81; 95% CI: 1.66–1.98), CKD (aHR 1.15; 95% CI: 1.01–1.30), and osteoporosis (aHR 1.26; 95% CI: 1.13–1.40) were all significantly associated with COPD.
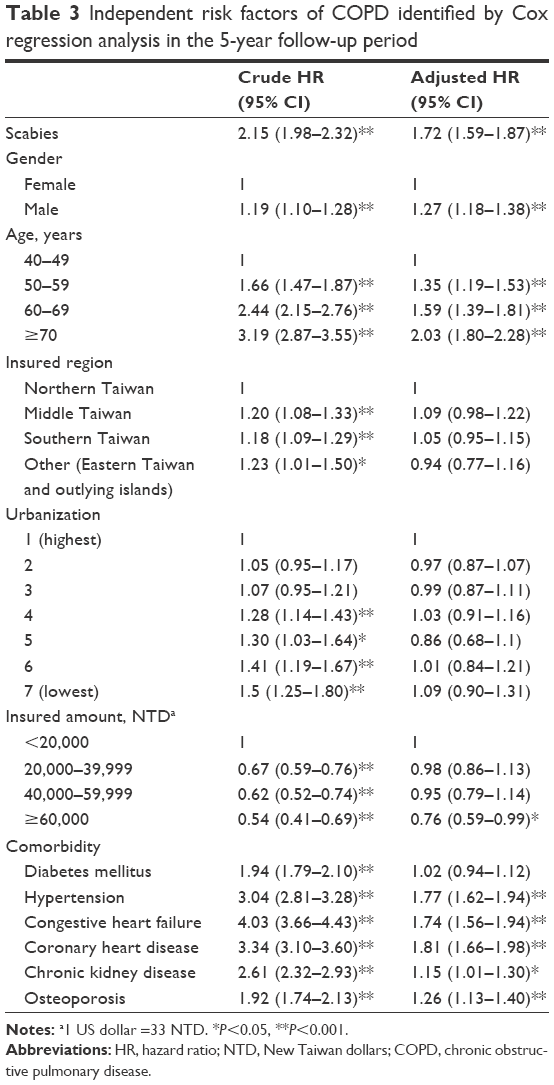 | Table 3 Independent risk factors of COPD identified by Cox regression analysis in the 5-year follow-up period |
The incidence of acute respiratory events and the results of the multivariable analysis of acute respiratory events complicated by COPD during the additional 2-year follow-up period are shown in Table 4. After adjusting for gender, age, income, geography, urbanization, and comorbidities, the aHR of acute respiratory events complicated by COPD was higher in the scabies group than in the control group, especially for major acute respiratory complications. For the scabies group, the aHR was 4.00 (95% CI: 3.08–5.19) for COPD with acute respiratory failure, 3.95 (95% CI: 2.25–6.95) for COPD with cardiopulmonary arrest, 3.29 (95% CI: 2.77–3.92) for COPD with pneumonia, and 1.85 (95% CI: 1.67–2.06) for COPD with acute exacerbation.
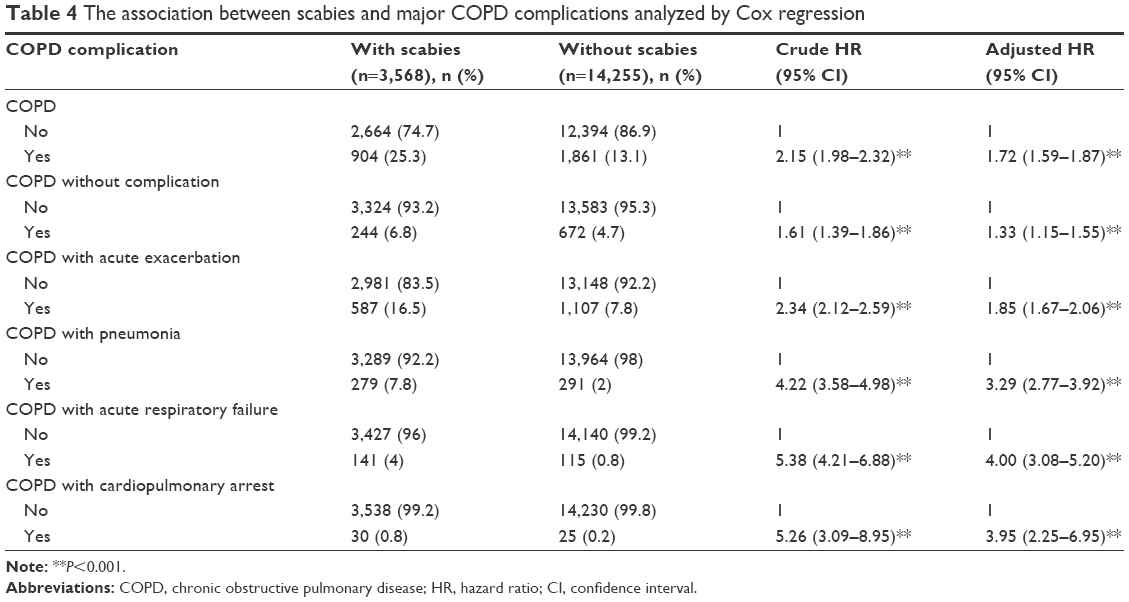 | Table 4 The association between scabies and major COPD complications analyzed by Cox regression |
Discussion
To the best of our knowledge, this is the first study specifically investigating the relationship between scabies and COPD. In this population-based study, a sample consisting of data for 1 million patients randomly selected from among the 23 million people in the NHIRD of Taiwan was analyzed. This study demonstrated that patients diagnosed with scabies had an increased risk of COPD during a 5-year follow-up period. Our study also revealed an increased risk of severe COPD complications such as acute respiratory failure, cardiopulmonary arrest, pneumonia, and acute exacerbation in patients with scabies during a subsequent 2-year follow-up period.
There was no research specifically investigating correlation between COPD and scabies infection in previously available literature. Scabies infection and COPD share similar risk factors, including being predominant among elderly people and during winter. Another explanation of the connection between COPD and scabies infection is thought to be chronic inflammation. According to in vitro studies, there are several proinflammatory cytokines, including interleukin (IL)-1, IL-6, IL-8, and TNF-a, as well as the immunomodulatory cytokines IL-10 and IL-12, that are responsible for immune reactions after exposure to scabies.20 An immune response indicated by increased numbers of CD8+ (cytotoxic) Tc1 lymphocytes is characteristic of COPD.21 Increased levels of IL-1β, IL-6, IL-8, and TNF-α have also been observed in sputum and bronchoalveolar lavage fluid from patients with stable COPD.22
In addition to the aforementioned cytokines, IL-17 plays an important role in inflammation caused both by COPD and scabies infection. IL-17 induces the production of mediators involved in the recruitment and activation of neutrophils.23,24 Other than this physiological response, IL-17A has also been shown by animal model to be related to the development of emphysema, which is relevant to COPD pathology.25 Furthermore, IL-17A drives neutrophilic inflammation in COPD acute exacerbation. Scabies infections in humans have been hypothesized to be correlated with an IgE-driven Th2 response to severe disease.26 However, further evidence has revealed the complexity of immune responses to scabies infection. A porcine model of S. scabiei infection demonstrated that IL-17-related pathways may contribute to the immunopathology of crusted scabies.27 Inhalation of long-acting beta agonist combined with corticosteroids is one of the major medications used for COPD. However, corticosteroids do not effectively reduce neutrophilic inflammation.28 The results of our study may explain why the scabies infection group have more possibilities of developing major COPD complications after a further 2-year follow-up period.
Male patients and elderly patients had increased risks of COPD, especially in patients older than 70 years. These findings are consistent with the prevalence rates indicated by a meta-analysis including data from 28 countries and by a cohort study.29,30 In addition, patients with scabies with HTN, CHF, CHD, and CKD had higher risks of developing COPD during the 5-year follow-up period. The Global initiative for chronic Obstructive Lung Disease (GOLD) guideline mentions that cardiovascular disease and metabolic syndrome are frequently combined with COPD.10 Many other comorbidities associated with COPD have also been reported, including HTN,31 DM,31 coronary artery disease,31 osteoporosis,32 heart failure,33 pulmonary infections, and lung cancer.10 Miller et al32 showed that the morbidity and mortality rates of patients with COPD were increased in those who also had comorbidities such as CHF, CHD, osteoporosis, and DM. The possible reasons that HTN, CHF, CHD, and CKD are associated with an increased risk of COPD include the presence of chronic inflammation and that these conditions share similar risk factors, such as tobacco smoking. The risk of COPD was not significantly increased among patients with DM in our study, but Ehrlich et al34 reported that patients with DM had a 22% increased risk of COPD.
There are several limitations in our study. First, all the diagnoses made using the ICD-9-CM coding system were sourced from the NHIRD. Detailed data of pulmonary function tests, forced expiratory volume in 1 s/forced vital capacity ratios (FEV1/FVC ratios), chest X-rays, computed tomography scans, and arterial blood gas analyses were not available in the NHIRD. Furthermore, instead of using the GOLD classifications, we used acute respiratory events such as pneumonia, acute exacerbation, acute respiratory failure, and cardiopulmonary arrest to evaluate the severity of COPD. Scabies and COPD patients were identified according to ICD-9-CM codes that were assigned to the patients by licensed physicians, and, while there are medical guidelines for making the relevant diagnoses, every physician’s method of diagnosis and management is inevitably at least slightly different from those of other physicians. Second, we could not adjust for confounding factors that were not included in the NHIRD, such as cigarette smoking status and occupational exposure. This study showed that scabies is related to COPD. However, further studies are needed to determine whether there is a bidirectional relationship between scabies and COPD. Further studies with animal models or scabies antigen/antibody to reinforce the relationship between scabies and COPD are warranted. Finally, our study is a retrospective population-based study. Further randomized prospective studies are necessary to further evaluate the relationship between scabies and COPD.
Conclusion
This is the first study to show that patients with scabies have an increased risk for COPD. This study also showed an increased risk of severe COPD complications, including acute respiratory failure, cardiopulmonary arrest, pneumonia, and acute exacerbation, among patients with scabies. Scabies infection may be a determining factor for COPD incidence. This useful information may help physicians in treating scabies and remaining alert to the potential development of COPD and its severe complications.
Acknowledgments
The work was supported by grants from the Ministry of Health and Welfare (10510), the Taoyuan General Hospital, Ministry of Health and Welfare (10415), the Ministry of Science and Technology Taiwan (MOST 104-2320-B-016-012-MY3), and the Tri-Service General Hospital (TSGH-C105-168) in the analysis and interpretation of data. The implications and conclusions of this study do not represent the opinions of the Bureau of National Health Insurance, the Department of Health, Ministry of Science and Technology Taiwan, Tri-Service General Hospital, or the National Health Research Institute.
Author contributions
JYC wrote the manuscript. JML wrote the proposal and designed the manuscript. FWC and HC contributed to the conception of the study. KCC conducted data analysis. CLY collected the data and conducted data analysis. YFW revised the manuscript. RJH revised the manuscript and data analysis. All authors contributed toward data analysis, drafting and critically revising the paper, read and approved the final manuscript, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Service MW. Medical Entomology for Students. London: Chapman and Hall; 1996. | ||
Orkin M. Scabies: what’s new? Curr Probl Dermatol. 1995;22:105–111. | ||
Chosidow O. Scabies. N Engl J Med. 2006;354(16):1718–1727. | ||
Pannell R, Fleming D, Cross K. The incidence of molluscum contagiosum, scabies and lichen planus. Epidemiol Infect. 2005;133(6):985–991. | ||
Hay R, Steer A, Engelman D, Walton S. Scabies in the developing world – its prevalence, complications, and management. Clin Microbiol Infect. 2012;18(4):313–323. | ||
Downs A, Harvey I, Kennedy C. The epidemiology of head lice and scabies in the UK. Epidemiol Infect. 1999;122(3):471–477. | ||
Divo M, Cote C, de Torres JP, et al; BODE Collaborative Group. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. | ||
Chen JC, Mannino DM. Worldwide epidemiology of chronic obstructive pulmonary disease. Curr Opin Pulm Med. 1999;5(2):93–99. | ||
Cheng SL, Chan MC, Wang CC, et al. COPD in Taiwan: a National Epidemiology Survey. Int J Chron Obstruct Pulmon Dis. 2015;10:2459–2467. | ||
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD; 2016. Available from: http://www.goldcopd.org/. Accessed August 11, 2016. | ||
Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. | ||
Menezes AM, Perez-Padilla R, Jardim JB, et al; PLATINO Team. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. | ||
Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance – United States, 1971–2000. MMWR Surveill Summ. 2002;51(6):1–16. | ||
Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. | ||
Wang CH, Lee SC, Huang SS, Kao YC, See LC, Yang SH. Risk factors for scabies in Taiwan. J Microbiol Immunol Infect. 2012;45(4):276–280. | ||
Cheng TM. Reflections on the 20th anniversary of Taiwan’s single-payer national health insurance system. Health Aff. 2015;34(3):502–510. | ||
National Health Research Institutes. National Health Insurance Research Database. Available from: http://nhird.nhri.org.tw/en/Data_Subsets.html#S3. Accessed October 1, 2013. | ||
US Department of Health and Human Services PHS, Health Care Financing Administration. The International Classification of Diseases: 9th Revision, Clinical Modification: ICD-9-CM. Washington, DC: US Department of Health and Human Services; 1989. | ||
Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006;4:1–22. | ||
Arlian LG, Morgan MS, Neal JS. Modulation of cytokine expression in human keratinocytes and fibroblasts by extracts of scabies mites. Am J Trop Med Hyg. 2003;69(6):652–656. | ||
Barnes PJ, Shapiro S, Pauwels R. Chronic obstructive pulmonary disease: molecular and cellularmechanisms. Eur Respir J. 2003;22(4):672–688. | ||
Keatings VM, Collins PD, Scott DM, Barnes PJ. Differences in interleukin-8 and tumor necrosis factor-alpha in induced sputum from patients with chronic obstructive pulmonary disease or asthma. Am J Respir Crit Care Med. 1996;153(2):530–534. | ||
Hoshino H, Laan M, Sjöstrand M, Lötvall J, Skoogh BE, Lindén A. Increased elastase and myeloperoxidase activity associated with neutrophil recruitment by IL-17 in airways in vivo. J Allergy ClinImmunol. 2000;105(1 pt 1):143–149. | ||
Tan HL, Rosenthal M. IL-17 in lung disease: friend or foe? Thorax. 2013;68(8):788–790. | ||
Chen K, Pociask DA, McAleer JP, et al. IL-17RA is required for CCL2 expression, macrophage recruitment, and emphysema in response to cigarette smoke. PLoS One. 2011;6(5):e20333. | ||
Walton SF. The immunology of susceptibility and resistance to scabies. Parasite Immunol. 2010;32(8):532–540. | ||
Liu X, Walton SF, Murray HC, et al. Crusted scabies is associated with increased IL-17 secretion by skin T cells. Parasite Immunol. 2014;36(11):594–604. | ||
Bozinovski S, Vlahos R. Multifaceted role for IL-17A in the pathogenesis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;191(11):1213–1214. | ||
Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28(3):523–532. | ||
Lindberg A, Jonsson AC, Rönmark E, Lundgren R, Larsson LG, Lundbäck B. Ten-year cumulative incidence of COPD and risk factors for incident disease in a symptomatic cohort. Chest. 2005;127(5):1544–1552. | ||
Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. | ||
Miller J, Edwards LD, Agustí A, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Comorbidity, systemic inflammation and outcomes in the ECLIPSE cohort. Respir Med. 2013;107(9):1376–1384. | ||
Havranek EP, Masoudi FA, Westfall KA, Wolfe P, Ordin DL, Krumholz HM. Spectrum of heart failure in older patients: results from the National Heart Failure project. Am Heart J. 2002;143(3):412–417. | ||
Ehrlich SF, Quesenberry CP, Van Den Eeden SK, Shan J, Ferrara A. Patients diagnosed with diabetes are at increased risk for asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and pneumonia but not lung cancer. Diabetes Care. 2010;33(1):55–60. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.