Back to Journals » Clinical Ophthalmology » Volume 15
Same-Day versus Next-Day Dexamethasone Intracanalicular Insert Administration for Inflammation and Pain Control Following Cataract Surgery: A Retrospective Analysis
Authors Foster B ![]()
Received 24 August 2021
Accepted for publication 28 September 2021
Published 18 October 2021 Volume 2021:15 Pages 4091—4096
DOI https://doi.org/10.2147/OPTH.S335764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Brian Foster.
Views: 402
Brian Foster
The Eye Associates, Bradenton, FL, USA
Correspondence: Brian Foster
The Eye Associates, 6002 Pointe West Blvd, Bradenton, Fl, 34209-5531, USA
Tel +1 941-220-5987
Email [email protected]
Background: The dexamethasone 0.4mg intracanalicular insert (Dextenza, Ocular Therapeutix, Bedford, MA) is approved for control of postoperative pain and inflammation following ocular surgery. This study compared pain and inflammation resolution following phacoemulsification in eyes that received the insert immediately postoperatively versus the next day.
Methods: This was a retrospective analysis of existing electronic health records. Consecutive qualifying eyes were included for analysis. All patients received perioperative antibiotics and nonsteroidal anti-inflammatory drugs. Pain and inflammation were assessed at baseline and on postoperative days 1, 7, and 30. Pain was assessed by dichotomous patient report (present/absent). Anterior chamber cell (0, 0.5+, 1– 4+) and flare (0– 4+) were graded using the Standardization of Uveitis Nomenclature rubric.
Results: Data from 17 eyes of 17 subjects were analyzed; 8 received the insert immediately postoperative and 9 in the office the next day. In both groups, trace cell was present in all eyes at day 1 and had resolved in all but 1 eye in each group at days 7 and 30. Flare was absent in all eyes at every time point, and transient pain was reported in a single same-day eye on day 7. No insert-related adverse events were observed, and no eyes required rescue corticosteroid therapy or insert removal.
Conclusion: Similar rates of inflammation and pain resolution after phacoemulsification were observed with the dexamethasone intracanalicular insert placed either immediately postoperatively or the next day.
Keywords: dexamethasone, Dextenza, phacoemulsification, anterior chamber inflammation, ocular pain, sustained-release drug delivery
Background
Postoperative anterior chamber inflammation is among the most common complications following modern phacoemulsification cataract surgery. Up to 95% of eyes will develop inflammation—characterized by cells and flare in the aqueous humor—within the first few postoperative days whether or not prophylactic anti-inflammatory therapy is applied.1 Inflammation also contributes to the development of acute postoperative pain, occurring in ~40–50% of patients without anti-inflammatory prophylaxis and 3–42% of patients receiving anti-inflammatory therapy.2–4 Other sequelae of postoperative inflammation include elevations of intraocular pressure (IOP) and cystoid macular edema.5–7
The current standard of care for perioperative prophylaxis of inflammation and infection is the use of patient self-administered topical anti-inflammatory and antimicrobial drugs,8 and these are widely prescribed by cataract surgeons in the United States.9 Multiple large-scale studies of intracameral antibiotics at the end of surgery have challenged the necessity of postoperative topical antibiotics, and the recent commercialization of 2 sustained-release formulations of dexamethasone—an intracanalicular insert containing dexamethasone (Dextenza (Dextenza, Ocular Therapeutix, Bedford, MA) and an intraocular dexamethasone suspension (Dexycu, dexamethasone 517 µg, EyePoint Pharmaceuticals, Watertown, MA)—has similarly challenged the need for topical dosing of corticosteroids postoperatively, leading many surgeons to propose a paradigm shift to dropless cataract surgery.10–13
The intracanalicular insert is a polyethylene glycol hydrogel rod impregnated with 0.4 mg of preservative-free dexamethasone, conjugated with fluorescein for visualization, that is inserted through the punctum into the inferior or superior canaliculus. Upon hydration, the insert swells and self-anchors, dissolving over time with sustained and tapered delivery of dexamethasone for up to 30 days.14 It can be inserted preoperatively, intraoperatively, or postoperatively as desired by surgeons and patients. Phase 3 clinical trials have demonstrated its efficacy in controlling postoperative pain and inflammation following phacoemulsification cataract surgery.14,15 Complementary to the findings of randomized trials, in this report we compare the effectiveness of same-day versus next-day administration of the dexamethasone intracanalicular insert after phacoemulsification on pain and inflammation outcomes in a real-world setting.
Methods
This was a retrospective analysis of existing electronic health records at a single practice. A de-identified data set was prepared for analysis. The study was conducted in accordance with the tenets of the Declaration of Helsinki. The study protocol was reviewed and approved by the Western Institutional Review Board on 12 June 2020 with a waiver of informed consent granted. Requests for data sharing will be considered by the authors on a case-by-case basis.
Data were included for subjects aged 18 years or older with visually significant cataract undergoing phacoemulsification who received the dexamethasone insert either immediately postoperatively in the operating room or the next day in the office. Exclusion criteria included use of topical or intravitreal corticosteroids in the study eye or systemically within 3 months of surgery, or any of the following in either eye: corneal pathology, previous corneal surgery, active or past chronic or recurrent inflammatory eye disease, pain, proliferative diabetic retinopathy, or macular pathology seen on optical coherence tomography.
Phacoemulsification surgery was performed using standard techniques through a temporal clear corneal incision. The dexamethasone insert was placed in the inferior punctum of the operative eye, positioned just below the level of the punctal opening to optimize visibility while avoiding insert-cornea contact, and hydrated with 1–2 drops of balanced salt solution to anchor the insert into position. The perioperative medical regimen included bromfenac 0.07% (Prolensa, Bausch & Lomb, Bridgewater, NJ) once daily beginning the day before surgery through 3 weeks postoperatively, and besifloxacin 0.6% (Besivance, Bausch & Lomb) twice daily the day before surgery, three times daily the day of surgery, and twice daily for 1 week postoperatively.
Data recorded from health records included visual acuity (best corrected visual acuity [BCVA] at baseline and day 30), pain, and anterior chamber inflammation (cells and flare) preoperatively and 1, 7, and 30 days postoperatively. Pain was assessed by dichotomous patient report (present/absent). Anterior chamber cell (0, 0.5+, 1–4+) and flare (0–4+) were graded using the Standardization of Uveitis Nomenclature (SUN) classification system.16
The primary effectiveness outcomes of this analysis were the proportions of patients with pain, anterior chamber cells, and anterior chamber flare at each postoperative time point (days 1, 7, and 30); these were analyzed using descriptive statistics. Secondary effectiveness outcomes included mean changes from baseline in IOP and BCVA (after transformation to the minimum angle of resolution [logMAR]) using paired t-tests. Primary effectiveness outcomes were stratified by time of dexamethasone insert placement (same day or next day). Safety outcomes included the incidence and severity of adverse events. No specific hypothesis was tested, and therefore no power/sample size analysis was conducted. A convenient sample of all subjects meeting eligibility criteria since the authors’ adoption of use of the dexamethasone insert was utilized.
Results
Data from 17 eyes of 17 subjects were analyzed. Demographic data are given in Table 1. Subjects’ mean (standard deviation) age was 69.7 (6.7) years, 10/17 (58.8%) were female, and 14/17 (82.4%) were White. Eight eyes received the insert immediately postoperatively (same day) and 9 eyes received the insert in the office on the first postoperative day (next day). All subjects were examined on postoperative day 1; at day 7, 9 subjects were evaluated and the remaining subjects were seen by co-management partners outside the practice; all but 1 subject were seen at day 30.
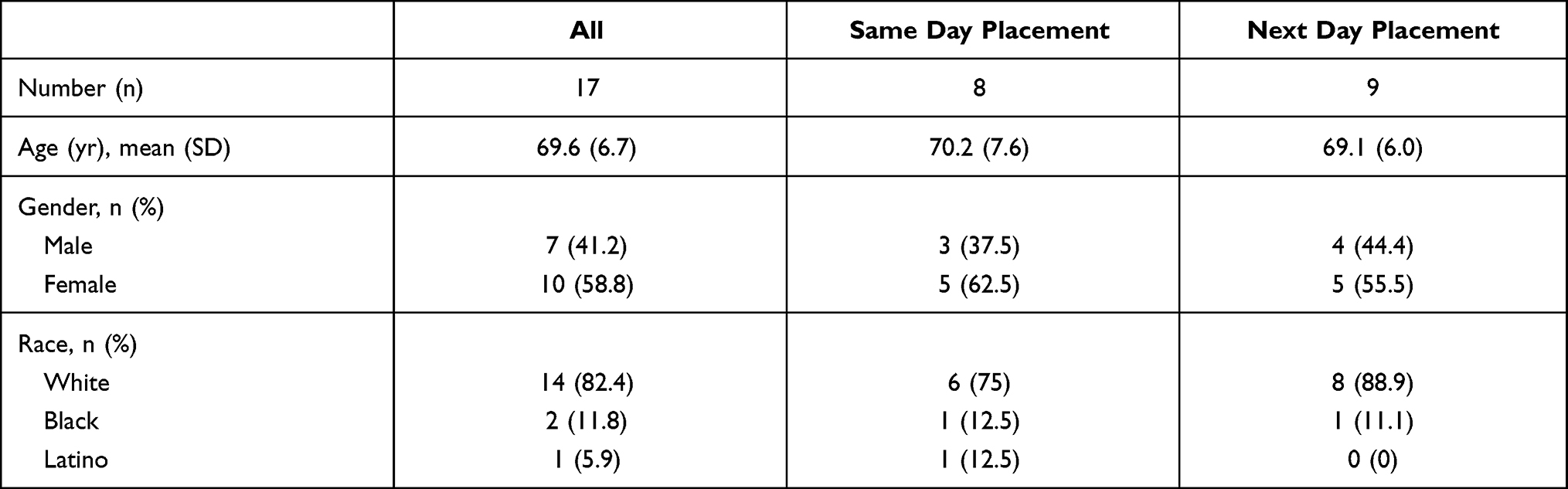 |
Table 1 Demographic Data for the Full Study Sample and by Treatment Group |
Anterior chamber cell and flare data for the full cohort as well as the same-day and next-day dosing subgroups are given in Table 2. Among the 8 eyes receiving same-day administration, anterior chamber cell was present in all eyes (100%) at day 1, in 1 of 2 eyes (50%) at day 7, and in 1 of 7 eyes (14.3%) seen at day 30. Among the 9 eyes receiving next-day administration, the corresponding values were 9/9 (100%), 1/7 (14.3%), and 0/9 (0%), respectively. In all cases, cell was graded as 0.5+ (1–5 cells per high-powered field). Flare was absent in all eyes at all time points. Pain was reported in a single eye at a single time point: at day 7 in an eye receiving same-day administration.
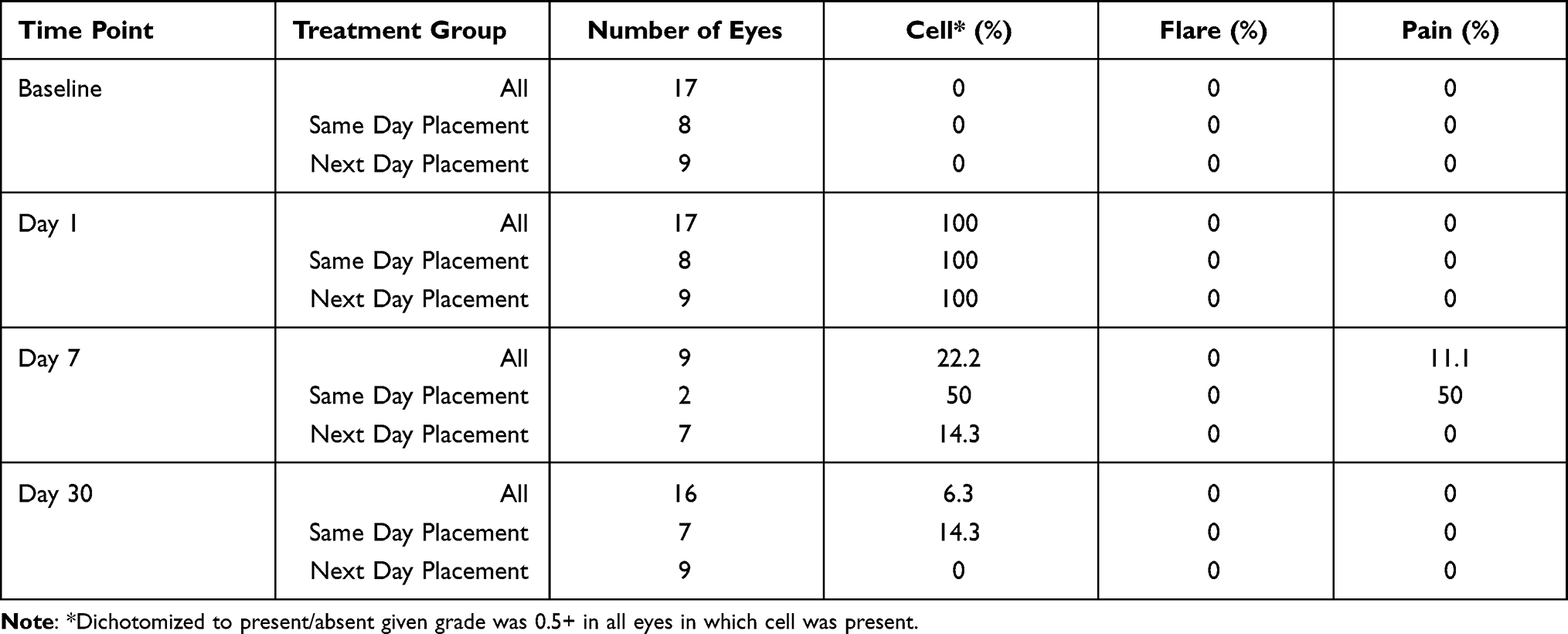 |
Table 2 Incidence of Anterior Chamber Cell, Flare, and Pain at Each Time Point by Treatment Group |
No intraoperative adverse events occurred. Mean logMAR BCVA improved from 0.382 (0.349) preoperatively to 0.198 (0.237) at day 30, and mean IOP remained unchanged from baseline (15.7 [2.9] mmHg) at day 1 (17.5 [3.5] mmHg), was lower than baseline at day 7 (12.0 [1.9] mmHg), and was unchanged from baseline at day 30 (14.0 [4.3]). No eyes manifested IOP elevations >10 mmHg from baseline at any postoperative time point. Five eyes developed posterior capsular opacification by day 30; 4 of these were in the next day insert placement group and 1 in the same day group. No other adverse events, including epiphora, foreign body sensation, or cystoid macular edema, were observed. No eyes required rescue therapy with topical corticosteroid therapy, and no inserts required removal at any point.
Discussion
The results of this study demonstrate that the dexamethasone 0.4mg intracanalicular insert effectively controlled postoperative inflammation and pain following phacoemulsification, with no clinically relevant differences in outcomes when the insert was placed either in the operating room at the completion of surgery or in the office the next day. The insert exhibited excellent safety, with stable mean IOP, no clinically significant IOP elevations, and no insert-related adverse events.
In this study, anterior chamber cells were ubiquitous on the first postoperative day and resolved in all but 1 eye by day 7. Flare was not seen in any eye at any time, and only a single eye reported pain at a single time point. No insert-related adverse events occurred, no eyes required rescue corticosteroid therapy, and no eyes required insert removal. These results are at least as favorable as those reported in prior studies.14,15 In three phase 3 trials of the dexamethasone insert versus vehicle (a similar intracanalicular insert not containing dexamethasone) placed immediately postoperatively on the day of surgery in a total of 926 eyes undergoing phacoemulsification,14,15 postoperative pain was absent at day 8 in ~80% of insert eyes versus ~45–60% of vehicle eyes (with the differences being significant in all 3 studies), and anterior chamber cells were absent at day 14 in ~35–50% of insert eyes and ~15–30% of vehicle eyes (with the differences being significant in 2 of the 3 studies). Rescue therapy with topical steroids in the first 2 postoperative weeks was required in ~5–15% of insert eyes and ~10–45% of vehicle eyes. Given the similar or better outcomes seen in both groups in the current study, it is reasonable to consider that the timing of insert administration—same-day versus next day—is safely flexible based on individual surgeon and patient characteristics.
Existing approaches to ocular drug delivery are limited by numerous issues that compromise clinical outcomes in a number of disease states, and there remains unmet need for improvement in ocular drug delivery for a variety of ocular conditions, particularly those that require chronic therapy. Topical medical therapy for glaucoma remains the mainstay of treatment, yet its most important limitation—poor adherence17—is a key cause of disease progression.18 Inhibitors of vascular endothelial growth factor (VEGF) have revolutionized therapy for many retinal vascular disorders, yet the burden of treatment—monthly or every few months for life—results in significant undertreatment and suboptimal outcomes.19,20 Sustained drug delivery platforms that remove the responsibility for daily self-dosing would significantly improve the management of glaucoma, and longer-acting formulations of anti-VEGF agents would similarly be of great benefit in treating retinal vascular diseases such as age-related macular degeneration and diabetic retinopathy.
The perioperative anti-inflammatory and antimicrobial regimen for cataract surgery can also benefit from advances in therapy. Almost 90% of American Medicare beneficiaries undergoing cataract surgery in 2016 were prescribed perioperative topical medications, including antibiotics (89%), steroids (86%), and nonsteroidal anti-inflammatory drugs (66%), with 55% receiving all three drugs.9 Therapy with these three drugs poses a complex regimen that may require different drugs to be dosed once, twice, three, or even four times daily, with the added complexity of a tapering steroid dosing frequency over time. This would be challenging under the best of circumstances and is likely even more so among the elderly population typically undergoing cataract surgery, many of whom may have temporary blurred vision in the acute postoperative period. Such a regimen is even more problematic in the COVID-19 pandemic era, in which elderly patients may have less access to postoperative caregivers and in whom repeated contact between hands and face are discouraged to minimize infection risk. Perhaps not surprisingly, half of patients are poorly adherent to their perioperative medication regimen following cataract surgery,21 and most demonstrate improper and potentially unsafe self-instillation techniques.22 All patients in the current received perioperative NSAIDs for prophylaxis against cystoid macular edema, which may have provided some additional degree of inflammation control; however, as evidenced by current clinical practice, steroids and NSAIDs are routinely co-prescribed for postoperative care9 and this practice was mimicked in our study.
Sustained-release corticosteroid formulations—as with the dexamethasone intracanalicular insert or the dexamethasone intraocular suspension (Dexycu, EyePoint Pharmaceuticals, Watertown, MA)—are an important step in the paradigm shift to dropless cataract surgery. This approach—utilizing intracameral antibiotics and sustained-release steroid products—has been advocated by multiple surgeons as an important step forward in optimizing therapeutic efficacy and postoperative quality of life in patients undergoing the most commonly performed outpatient surgery in adults in the United States.10–13 Replacing self-administered topical therapy with surgeon-administered therapy reduces risks associated with improper instillation technique and eliminates nonadherence, resulting in better efficacy, safety, and quality of life outcomes.
These attributes of sustained dexamethasone delivery with the intracanalicular insert are valued by both physicians and patients. In the phase 3 insert trials, 98% of surgeons rated the insert as easy or moderately easy to insert, and 99.5% of inserts were easily visualized at day 14.23 A patient experience study was conducted in a subset of phase 3 participants.24 Among 25 subjects undergoing a semi-structured survey, 100% reported that the insert was comfortable, and the majority (84%) were unaware of its presence in the canaliculus. Overall, 92% reported being very satisfied with the insert, and 96% rated it convenient or very convenient compared to their prior experience with topical eye drop use. Also, a recent study evaluating the effectiveness of the insert placed in the office the day after femtosecond-assisted phacoemulsification demonstrated complete resolution of anterior chamber cells and flare within the first 2 postoperative weeks in all eyes.25
This study was intended to complement the phase 3 investigations by characterizing outcomes in the real-world setting, in a less artificially homogenous patient sample and with less rigorous protocol requirements. Particular to this study was the flexibility in administering the insert either immediately postoperatively or the next day (no outcome differences were observed), which expands treatment timing options for surgeons and patients. The study is limited by a small sample size, but as no specific hypotheses were proposed or tested (and thus no inferential testing was undertaken), the sample size was deemed adequate to characterize the outcomes of interest, namely resolution of postoperative pain and inflammation.
Conclusion
Similar rates of inflammation and pain resolution after phacoemulsification were achieved with the dexamethasone intracanalicular insert placed either immediately postoperatively or the next day. These early experience findings in a small sample provide evidence for greater flexibility in the timing of insert placement in developing perioperative pain and inflammation control strategies.
Abbreviations
BCVA, best corrected visual acuity; COVID, corona virus disease; IOP, intraocular pressure; logMAR, logarithm of the minimum angle of resolution; SUN, Society of Uveitis Nomenclature; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The datasets generated during and analyzed during the current study are not publicly available due to not being published prior but are available by the author upon request.
Ethics Approval and Informed Consent to Participate
The study protocol was reviewed and approved by the Western Institutional Review Board on 12 June 2020 with a waiver of informed consent granted.
Acknowledgments
The author acknowledges assistance with manuscript preparation provided by Tony Realini, MD, MPH, with support from Ocular Therapeutix. This paper was presented in part at the 2021 ASCRS annual meeting as a conference talk with interim findings.
Funding
Sponsorship for this study was provided by Ocular Therapeutix.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Walters TR, Goldberg DF, Peace JH, Gow JA. Bromfenac ophthalmic solution 0.07% dosed once daily for cataract surgery: results of 2 randomized controlled trials. Ophthalmology. 2014;121:25–33. doi:10.1016/j.ophtha.2013.07.006
2. Porela-Tiihonen S, Kokki H, Kaarniranta K, Kokki M. Recovery after cataract surgery. Acta Ophthalmol. 2016;94(Suppl 2):1–34. doi:10.1111/aos.13055
3. Porela-Tiihonen S, Kaarniranta K, Kokki M, Purhonen S, Kokki H. A prospective study on postoperative pain after cataract surgery. Clin Ophthalmol. 2013;7:1429–1435.
4. Porela-Tiihonen S, Kaarniranta K, Kokki H. Postoperative pain after cataract surgery. J Cataract Refract Surg. 2013;39:789–798. doi:10.1016/j.jcrs.2013.03.012
5. Mohammadpour M, Jafarinasab MR, Javadi MA. Outcomes of acute postoperative inflammation after cataract surgery. Eur J Ophthalmol. 2007;17:20–28. doi:10.1177/112067210701700104
6. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21 000 cases in the United States. Ophthalmology. 2016;123:723–728. doi:10.1016/j.ophtha.2015.12.020
7. Dua HS, Attre R. Treatment of post-operative inflammation following cataract surgery – a review. Eur Ophthalmic Rev. 2012;6:98–103. doi:10.17925/EOR.2012.06.02.98
8. American Academy of Ophthalmology. Cataract in the Adult Eye Preferred Practice Pattern. San Francisco, CA: American Academy of Ophthamology; 2016.
9. Zafar S, Wang P, Schein OD, Srikumaran D, Makary M, Woreta FA. Prescribing patterns and costs associated with postoperative eye drop use in medicare beneficiaries undergoing cataract surgery. Ophthalmology. 2020;127:573–581. doi:10.1016/j.ophtha.2019.11.005
10. Shorstein NH, Myers WG. Drop-free approaches for cataract surgery. Curr Opin Ophthalmol. 2020;31:67–73. doi:10.1097/ICU.0000000000000625
11. Lindstrom RL, Galloway MS, Grzybowski A, Liegner JT. Dropless cataract surgery: an overview. Curr Pharm Des. 2017;23:558–564. doi:10.2174/1381612822666161129150628
12. Assil KK, Greenwood MD, Gibson A, Vantipalli S, Metzinger JL, Goldstein MH. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction. Curr Opin Ophthalmol. 2020. doi:10.1097/ICU.0000000000000708
13. Bardoloi N, Sarkar S, Pilania A, Das H. Efficacy and safety of dropless cataract surgery. Indian J Ophthalmol. 2020;68:1081–1085. doi:10.4103/ijo.IJO_1186_19
14. Walters T, Bafna S, Vold S, et al. Efficacy and safety of sustained release dexamethasone for the treatment of ocular pain and inflammation after cataract surgery: results from two phase 3 studies. J Clin Exp Ophthalmol. 2016;7:1–11. doi:10.4172/2155-9570.1000572
15. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2019;45:204–212. doi:10.1016/j.jcrs.2018.09.023
16. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516.
17. Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009;116:S30–S36. doi:10.1016/j.ophtha.2009.06.024
18. Sleath B, Blalock S, Covert D, et al. The relationship between glaucoma medication adherence, eye drop technique, and visual field defect severity. Ophthalmology. 2011;118:2398–2402. doi:10.1016/j.ophtha.2011.05.013
19. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99:220–226. doi:10.1136/bjophthalmol-2014-305327
20. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119:1175–1183. doi:10.1016/j.ophtha.2011.12.016
21. Hermann MM, Ustundag C, Diestelhorst M. Electronic compliance monitoring of topical treatment after ophthalmic surgery. Int Ophthalmol. 2010;30:385–390. doi:10.1007/s10792-010-9362-3
22. An JA, Kasner O, Samek DA, Levesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40:1857–1861. doi:10.1016/j.jcrs.2014.02.037
23. McCabe CM, Berdahl JP, Tyson S, et al. Patient and physician preference for an intracanalicular dexamethasone insert for treating inflammation and pain following cataract surgery.
24. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (Dextenza): results of a qualitative survey. Patient Prefer Adherence. 2017;11:487–494. doi:10.2147/PPA.S126283
25. Stephenson PDG. Real-world evaluation of postoperative in-office Dexamethasone intracanalicular insert administration for control of postoperative inflammation following cataract surgery. J Clin Ophthalmol. 2020;4:273–278.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.