Back to Journals » Orthopedic Research and Reviews » Volume 11
Salvage of failed dynamic hip screw fixation of intertrochanteric fractures
Authors Taheriazam A, Saeidinia A
Received 10 May 2019
Accepted for publication 23 July 2019
Published 22 August 2019 Volume 2019:11 Pages 93—98
DOI https://doi.org/10.2147/ORR.S215240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Afshin Taheriazam,1 Amin Saeidinia2,3
1Department of Orthopedics Surgery, Tehran Medical Sciences Branch, Islamic Azad University, Tehran, Iran; 2Faculty of Medicine, Guilan University of Medical Sciences, Rasht, Iran; 3Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Afshin Taheriazam
Department of Orthopedics Surgery, Tehran Medical Sciences Branch, Islamic Azad University, Khaghani Street, Shariati Avenue, Tehran, Iran
Tel +98 912 111 3486
Email [email protected]
Amin Saeidinia
Medical Faculty, Mashhad University of Medical Sciences, Azadi Square, Mashhad, Iran
Tel +98 911 945 1607
Email [email protected]
Background and aim: Failure of intertrochanteric fracture fixation can occur in patients with poor bone quality, extreme osteoporosis, or unstable fracture arrangement. Although hip replacement is a commonly successful process, it includes technical problems, such as implant removal, bone loss, low bone quality, nonunion of trochanter, and difficult surgical exposure. The goal of this study was to restore total hip replacement for failed intertrochanteric fractures to assess the outcomes.
Methods: During April 2009 to October 2015, 203 patients (203 hips) underwent total hip arthroplasty through the direct lateral approach, as salvage of failed intertrochanteric fracture management by dynamic hip screw (DHS). The restoration process was done by a direct lateral approach (Hardinge) in all hips. The operation details, such as duration, blood transfusion volume, blood loss, and duration of hospital stay, were recorded. Modified Harris hip score (MHHS) was applied for assessment of clinical outcome before and after the operation, and during the follow-up.
Results: Overall, 112 patients were male (55.17%) and 91 patients (44.8%) were female and the mean of age was 72.58±10.60 years old. Average operation time was 93.96±10.72 minutes. The mean blood loss volume during the operation was 355.86±84.11 mL. The mean preoperative MHHS score was 39.55±6.74 (range: 30–50). The MHHS score improved to 90.55±2.24, 92.34±1.26, and 94.34±1.85 during the first, second, and final follow-up, respectively (P<0.0001). Infection was found in only two patients, who had undergone one stage revision and linear of the cup was exchanged. Total rate of complications during the follow-up was 4.92%.
Conclusion: The current research was a large population study and indicated that sufficient functional outcome could be obtained by total hip replacement in geriatrics with failed intertrochanteric fractures. Therefore, well-performed hip replacement could be a suitable choice for restoring failed DHS in unsuccessfully managed intertrochanteric fractures in the elderly.
Keywords: failed intertrochanteric fracture, total hip arthroplasty, trochanteric nonunion, dynamic hip screw
Introduction
Intertrochanteric hip fractures are the most frequent kind of fracture with a growing incidence in the elderly population. Unstable peritrochanteric fractures are difficult to fix and are currently a problematic issue in managing these kinds of fractures.1 According to previous reports of higher complications due to management of these patients, different internal fixation instruments and operational methods have been developed to diminish adverse events.1–3 The most common instruments utilized for this purpose are compression hip screws with side plate attachments, such as dynamic hip screw (DHS) and intramedullary fixation instruments. Despite existence of controversy in using favored fixation instruments, intramedullary fixative devices are progressively becoming the favored choice because of their advantages.4,5 All of these methods can lower the occurrence of adverse events in the perioperative or postoperative period. Two basic processes are change in design of implant and altered reduction method for reaching greater stability. Such devices should establish the fracture across distorting efforts until union formation. There are some undisciplined characteristics in lowering operation-contributed adverse events, such as pattern of fracture, existence of other chronic disorders, and bone density. Nevertheless, operation-related adverse events can be diminished by more advanced methods using new fixator instruments, enhancement of the technical operative process, and reduction of hospital stay duration.1
The majority of intertrochanteric femur fractures can be managed by internal fixation.6 Failure rate of internal fixation has been reported as 56%, which contributes to poor bone quality, suboptimal fixation, comminution, and fracture patterns.7 Unsuccessful management of intertrochanteric hip fractures generally provokes deep functional impairment and pain. Hip replacement is recognized as a salvage procedure for older subjects, patients with osteoporosis, patients with avascular necrosis of the femoral head, or patients with injured acetabular side.8–10 The goal of this investigation was to determine the outcomes of total hip arthroplasty (THA) as the alternative management for failed fixation of intertrochanteric hip fractures.
Methods
During the study period (from April 2009 to October 2015), 203 patients (203 hips) underwent THAthrough the direct lateral approach as salvage of failed management of intertrochanteric hip fractures by a DHS. This was a prospective study, in which the researchers analyzed functional results and adverse events of this salvage treatment. The study included early and late DHS failures in adults and the elderly with intertrochanteric hip fractures. Patients with active infection and united fractures with acceptable function were excluded. All patients were followed-up by clinical and radiological assessment. The fractures were classified based on AO classification.11 There were four treatment groups: (1) patients that had undergone THA, (2) patients that had undergone THA and trochanteric osteotomy, (3) patients with THA and acetabular salvage with cage (graft augmentation prosthesis (GAP) II), and (4) patients that had undergone bipolar arthroplasty.
Surgical procedures and prosthesis
The salvage process was performed through a direct lateral approach (Hardinge) in the hips. In order to prevent femoral shaft fracture during the operation, before removing the implant, the hip was dislocated, as the hip is usually quite stiff and the bone has poor quality. The standard direct lateral approach (Hardinge) was utilized for all subjects. An identical surgical team and the same main surgeon (senior author of this study) performed the operations (Figure 1). In some cases, trochanteric osteotomy was used besides THA. In addition, in acetabular defects, salvage of acetabulum was performed with cage (GAP II). General anesthesia was used for 174 patients (85.71%) and spinal anesthesia for 29 subjects (14.29%). Postoperative pelvic radiograph was taken. Standard care for preventing infection, embolism, and deep vein thrombosis (DVT) was performed as mentioned in previous reports.9
 |
Figure 1 Postoperative radiography of a 95-year old patient that had undergone reconstructive total hip arthroplasty (THA). |
A cemented prosthesis was used in 28 hips (13.79%), a cement-less prosthesis in 170 hips (83.74%), and a hybrid prosthesis in five hips (2.46%). Bone grafting was not done for any of the patients.
The following cup prostheses were used in the procedures: Tripolar® cup (Stryker Orthopaedics, Mahwah, NJ, USA), Trident Multihole® cup (Stryker Orthopaedics), Continuum cup (Zimmer, Warsaw, IN, USA), and Trilogy (Zimmer). The following stem prostheses were used in the current study: Accolade® stem (Stryker Orthopaedics), Wagner SL® revision stem (Zimmer) and cone/conical® modular femoral revision stem (Stryker, Newbury, UK).
Preoperative prophylaxis against infection was given to all patients (cefazolin 1 g, intravenously, before the surgery followed by 1 g three times daily on the first day). Subcutaneous low molecular weight heparin (40 mg once daily), starting on the day of surgery, was given to all patients for 14 days in addition to anti-embolism stockings as prophylaxis against DVT. Early mobilization was used both to prevent DVT and to facilitate functional recovery. Full weight-bearing was allowed with walker, from the day after surgery onwards, in all cases. They used a walker for the first three weeks and physiotherapy was performed for the outpatients on the first week.12
Follow-up
The operation details, such as length of operation, blood loss, volume of blood transfusion, and duration of hospital stay, were recorded. Modified Harris hip score (MHHS)13 was used for clinical results before and after the surgery, and at the final follow-up. Radiologic assessment of the validity of the fixation was performed at each follow-up visit. Confirmation of erosion of acetabulum, decline of the stem, migration of acetabular component, and heterotopic ossification were recorded. Outcome assay was performed using limb shortening, pain, and walking ability. The definition of cementless cup loosening was considered as a complete radiolucent line at the implant–bone interface, implant migration, or fixation screws breakage.14 The Harris score criteria15 were used for cemented stems and Hodgkinson16 criteria for cemented cups. Data forms were used to record the details of the procedure. Adverse events were recorded during the follow-up and hospital stay. Subjects were followed closely for a period of 51.93±7.73 months (range: 36–60). The ability of patients' walking was evaluated. Complications, including infection, DVT, pulmonary thromboembolism (PTE), periprosthetic fracture, dislocation, mortality, and re-operation were recorded. Systemic adverse events, such as gastrointestinal, cardiac complications, phlebitis or pulmonary embolism, cerebrovascular accidents, and urinary tract infection were also recorded. An independent evaluator team performed the clinical and functional evaluations.
Statistical analysis
Descriptive statistical analyses were used to explain mean and standard deviation of quantitative factors. The outcomes were compared between groups for significance by a Student's t-test or a Mann–Whitney U test. Dichotomous characters were analyzed using chi-squared or Fisher’s exact tests. For all analyses, the SPSS software was used (SPSS 16.0 for Windows; SPSS Inc. Chicago, IL, USA). P-values of <0.05 were considered meaningful.
Ethics
The researchers observed all ethical issues for patient’s data and procedures, according to the ethical committee of Tehran branch of Azad University and ethical statements. This study was approved by the ethical committees of both Milad and Erfan Hospitals. Written informed consent was obtained from each subject before surgery, and patients were completely instructed of the probable benefits and adverse events. This study was conducted in accordance with the Declaration of Helsinki.
Results
Demographic data
In total, 112 patients were male (55.17%) and 91 patients (44.8%) were female and the mean age was 72.58±10.60 years (range: 57–93 years). The reasons of the treatment failure were nail cut out in 174 (85.7%), non-union in 15 (7.3%), and screw breakage in side-plate interface in 14 cases (6.8%). The average time from primary fixation to salvage arthroplasty was 7.2 months (4–24 months). Surgical treatment direction was right in 98 hips (48.27%) and left in 105 hips (51.72%). All fractures were unstable (100%). Other demographic data are summarized in Table 1, based on the treatment groups.
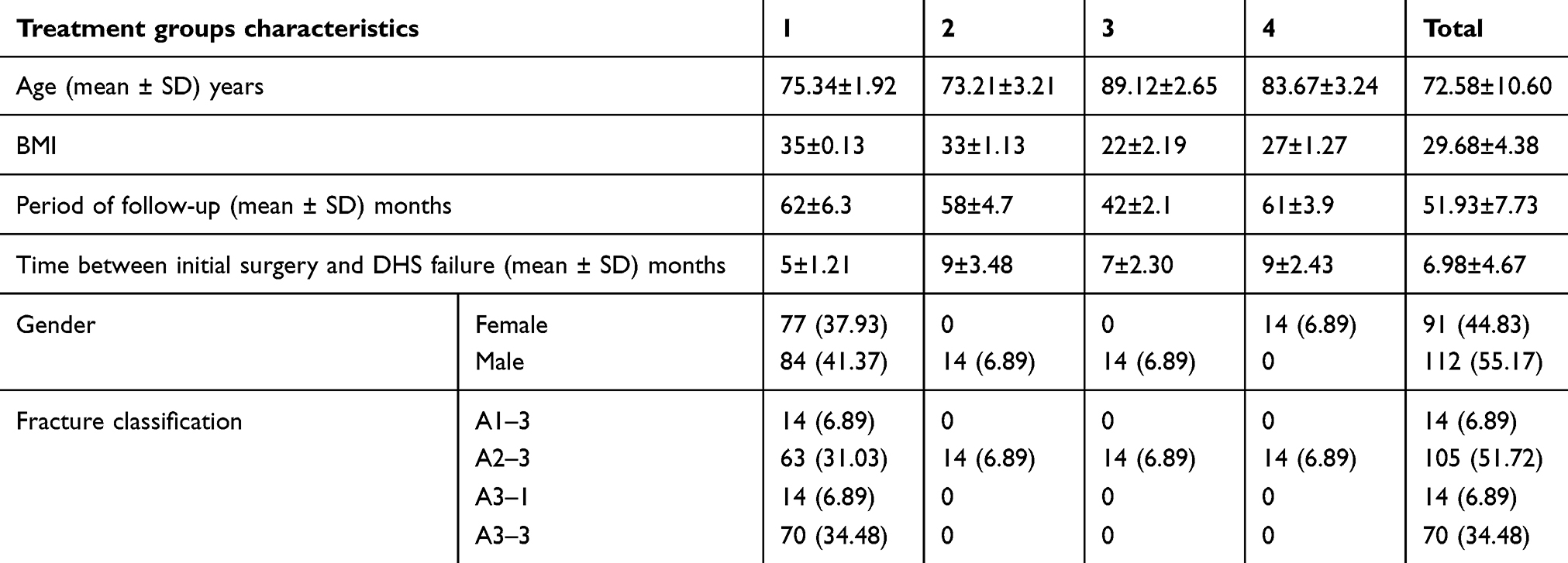 |
Table 1 Demographic data of patients with failed dynamic hip screw (DHS) |
Operation data
Preoperative clinical evaluation showed that the mean limb shortening was 3.13±0.58 cm. Femoral head in nearly all patients were excavated (96.6%) and most acetabular states were osteoporosis (79.3%). Average operation time was 93.96±10.72 minutes (range: 80–120). The mean blood loss volume during the operation was 355.86±84.11 mL (range: 220–500). Average number of blood transfusions volume was 0.55±0.63 (range: 0–2). The mean hospitalization duration was 4.63±1.08 days (range: 3.5–8).
Functional outcome
The mean preoperative MHHS score was 39.55±6.74 in the patients (range: 30–50). The MHHS score improved to 90.55±2.24 (range 85–95), 92.34±1.26 (range 90–95), and 94.34±1.85 (range: 90–97) in the first, second, and final follow-up, respectively (P<0.0001). Preoperative average limb shortening was 3.13±0.58 cm (range: 1.5–4 cm) and reached 0.85±0.12 cm, postoperatively (P<0.002). All patients at the last follow-up had lower pain score and the VAS score was decreased, significantly (from 9.32±2.28 to 2.37±1.44; P<0.001). All patients in each treatment group were able to walk without support at the final follow-up.
Complications
Infection was seen in only two patients, who had undergone one stage revision and linear of the cup was exchanged. They were then treated and the patients received antibiotic therapy for three weeks. Infection was found in two patients (0.98%). Dislocation was reported in one patient (0.49%). Re-operation was reported in three patients (1.47%). One patient had an intraoperative fracture, which was treated (0.49%). There was no evidence of DVT, PTE, periprosthetic fracture or mortality. There was a hematoma (0.49%) in patients with a history of anticoagulant therapy, which was resolved in three days after discontinuation of anticoagulant therapy.
The last accessible radiography follow-up demonstrated that all greater trochanter fractures had been repaired (Figure 2). No evidence of loosening of any components or sign of heterotopic bone formation were observed. Total rate of complications during the follow-up was 4.92%.
 |
Figure 2 Radiography of final available follow-up for patients showing improvement of greater trochanter fractures. |
Discussion
Failed intertrochanteric hip fracture was a challenging issue for orthopedic surgeons. Young adult subjects have better salvage and all attempts will be made to save the hip joint by redoing internal fixation procedures. However, in elderly subjects, prosthetic replacement is a reliable salvage choice.17 Hip arthroplasty/replacement procedure markedly relieved pain and helped the majority of subjects regain their previous function.18 This is a sign of an effective salvage procedure.19,20 There is little work on the outcomes of hip arthroplasty/replacement for restoration of failed internal fixation in intertrochanteric hip fractures. The range of published failure rate of internal fixation procedure for intertrochanteric hip fracture is between 3% and 12% with non-union (2–5%), instrument penetration (2–12%), and mal-union resulting in varus deformity (5–11%).8
During the switch of the failed internal fixation intertrochanteric hip fractures to hip replacement/arthroplasty, there are different challenging issues. In general, proximal femur anatomy is dislocated if the reduction of the fractured hip was incomplete or there was comminution of medial bony edges. In this process, bone intensity is poor due to previous existence of osteoporosis. Additionally, due to a lack of use, bone quality can decrease to a greater extent after failure of the internal fixation process. Another problem is the healing process of certain parts, such as greater trochanter, which cannot heal solidly and can be re-crushed after hip arthroplasty. This issue can result in a higher rate of dislocation and has an inverse effect on ambulatory status.21 In the current study, the rate of dislocation was 0.49% (one subject), which was surgically treated. Another study reported three dislocations (14.2%), which was higher in comparison to the current study.21 This study showed a sufficient short-term outcome after THA salvage and significant improvement in patients’ functional results besides low complication rate. To the best of the author’s knowledge, there have been only a few studies that have evaluated such outcomes in this large population. Similar to the current study, Haidukewych and Berry demonstrated rather few adverse events and lowering pain and function in their large series of reconstructive THA after failed intertrochanteric hip fractures.22 They evaluated 60 patients in their study and 44 patients were followed for a mean time of five years and reported two hips for aseptic loosening, one patient with dislocation, and seven-year survival rate of free-revision arthroplasties as 100% and 88% at ten years. Mehlhoff et al assessed 13 subjects followed for an average follow-up time of 34 months and showed five subjects with good to excellent outcomes, and three with dislocation (two requiring revision for their instability).19 In Tabsh et al’s study, comparison of 53 routine THAs with 53 THAs performed after failed proximal femoral fracture, revealed higher occurrence of adverse events and surgical problems in subjects with a previous hip fracture.23 D’Arrigo et al evaluated 16 female and five male patients with a mean age of 75.8 years, of whom 14 patients had failure of a previous nail fixation procedure, five had failure of a plate fixation, one of hip screw fixation, and one of Ender nail fixation. In 19 out of 21 patients, a THA was performed and a marked progression was reported comparing pre- and postoperative outcomes.24 Wu et al reported on 14 intertrochanteric hip fractures with failed DHS. They were managed by reuse of a lag screw inferiorly in the femoral head, cement augmentation, and subtrochanteric valgus osteotomy. All improved during a mean duration of five months.25 Some other studies showed unsatisfactory results. McKinley and Robinson expressed poor results in their series of management of THA for failed subcapital fractures.26 Srivastav et al’s analysis of THA for failed internal fixation in intertrochanteric hip fractures and intracapsular neck fracture did not show any difference in adverse events rate or clinical results. However, most of their patients had good pain improvement and significant functional progression.21
Conclusion
The strengths of the current study were higher sample size and a sufficient rate of follow-up in this intertrochanteric hip fracture population with low rate of complications with one approach for THA. The shortcoming of this investigation was the multiple prosthetic design. Hip arthroplasty/replacement after failed treatment of an intertrochanteric hip fracture is methodologically more difficult than routine primary THA. Most subjects that entered in this midterm follow-up had good pain alleviation and significantly better functional improvement. Although there are many technical difficulties, there were a few major complications. It could be concluded that THA after failed DHS internal fixation of intertrochanteric hip fracture is the best choice and can be used for all patients.
Acknowledgment
The authors thank the nurses and personnel of Erfan and Milad hospitals for their cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee S-R, Kim S-T, Yoon MG, Moon M-S, Heo J-H. The stability score of the intramedullary nailed intertrochanteric fractures: stability of nailed fracture and postoperative patient mobilization. Clin Orthop Surg. 2013;5(1):10–18. doi:10.4055/cios.2013.5.1.10
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip fracture. J Orthop Trauma. 2003;17(1):53–56.
3. Taheriazam A, Saeidinia A, Keihanian F. Total hip arthroplasty and cardiovascular complications: a review. Ther Clin Risk Manag. 2018;14:685–690. doi:10.2147/TCRM.S155918
4. Utrilla AL, Reig JS, Muñoz FM, Tufanisco CB. Trochanteric gamma nail and compression hip screw for trochanteric fractures: a randomized, prospective, comparative study in 210 elderly patients with a new design of the gamma nail. J Orthop Trauma. 2005;19(4):229–233.
5. Bojan AJ, Beimel C, Speitling A, Taglang G, Ekholm C, Jönsson A. 3066 consecutive Gamma Nails. 12 years experience at a single centre. BMC Musculoskelet Disord. 2010;11(1):1. doi:10.1186/1471-2474-11-133
6. Hammad A, Abdel-Aal A, Said HG, Bakr H. Total hip arthroplasty following failure of dynamic hip screw fixation of fractures of the proximal femur. Acta Orthop Belg. 2008;74(6):788.
7. Haidukewych GJ, Israel TA, Berry DJ. Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am. 2001;83(5):643–650. doi:10.2106/00004623-200105000-00001
8. Haentjens P, Casteleyn P, Opdecam P. Hip arthroplasty for failed internal fixation of intertrochanteric and subtrochanteric fractures in the elderly patient. Arch Orthop Trauma Surg. 1994;113(4):222–227.
9. Taheriazam A, Saeidinia A. Conversion of failed hemiarthroplasty to total hip arthroplasty: a short-term follow-up study. Medicine. 2017;96(40):e8235. doi:10.1097/MD.0000000000008235
10. Taheriazam A, Saeidinia A. Concurrent one-stage total knee and hip arthroplasty due to sequel of juvenile rheumatoid arthritis: a case report. Medicine. 2017;96(46):e8779. doi:10.1097/MD.0000000000008779
11. Müller ME, Allgöwer M, Perren SM, Osteosynthesefragen A. Manual of INTERNAL FIXATION: Techniques Recommended by the Ao-Asif Group. Berlin: Springer Berlin Heidelberg; 1991.
12. Taheriazam A, Saeidinia A. Cementless one-stage bilateral total hip arthroplasty in osteoarthritis patients: functional outcomes and complications. Orthop Rev (Pavia). 2017;9(2):6897. doi:10.4081/or.2017.6897
13. Wamper KE, Sierevelt IN, Poolman RW, Bhandari M, Haverkamp D. The Harris hip score: do ceiling effects limit its usefulness in orthopedics?: a systematic review. Acta Orthop. 2010;81(6):703–707. doi:10.3109/17453674.2010.537808
14. Larsson S. Treatment of osteoporotic fractures. Scand J Surg. 2002;91(2):140–146. doi:10.1177/145749690209100202
15. Mariani EM, Rand JA. Nonunion of intertrochanteric fractures of the femur following open reduction and internal fixation. Results of second attempts to gain union. Clin Orthop Relat Res. 1987;(218):81–89.
16. Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990;72(1):26–31.
17. Haidukewych GJ, Berry DJ. Salvage of failed treatment of hip fractures. J Am Acad Orthop Sur. 2005;13(2):101–109.
18. Taheriazam A, Saeidinia A. Short-term results of total hip arthroplasty for post traumatic arthritis in acetabular fracture internal fixation. Int J Adv Biotechnol Res. 2016;7(4):2058–2066.
19. Mehlhoff T, GC LANDON, HS TULLOS. Total hip arthroplasty following failed internal fixation of hip fractures. Clin Orthop Relat Res. 1991;269:32–37.
20. Taheriazam A, Saeidinia A. Bilateral total hip arthroplasty in femoral head avascular necrosis: functional outcomes and complications. Health Sci. 2016;5(6):51–56.
21. Srivastav S, Mittal V, Agarwal S. Total hip arthroplasty following failed fixation of proximal hip fractures. Indian J Orthop. 2008;42(3):279. doi:10.4103/0019-5413.41851
22. Haidukewych GJ, Berry DJ. Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures. J Bone Joint Surg Am. 2003;85(5):899–904. doi:10.2106/00004623-200305000-00019
23. Tabsh I, Waddell JP, Morton J. Total hip arthroplasty for complications of proximal femoral fractures. J Orthop Trauma. 1997;11(3):166–169.
24. D’Arrigo C, Perugia D, Carcangiu A, Monaco E, Speranza A, Ferretti A. Hip arthroplasty for failed treatment of proximal femoral fractures. Int Orthop. 2010;34(7):939–942. doi:10.1007/s00264-009-0834-x
25. Wu C, Shih C, Chen W, Tai C. Treatment of cutout of a lag screw of a dynamic hip screw in an intertrochanteric fracture. Arch Orthop Trauma Surg. 1998;117(4–5):193–196.
26. McKinley J, Robinson C. Treatment of displaced intracapsular hip fractures with total hip arthroplasty: comparison of primary arthroplasty with early salvage arthroplasty after failed internal fixation. J Bone Joint Surg. 2002;84(11):2010–2015. doi:10.2106/00004623-200211000-00016
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.