")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Safinamide in the management of patients with Parkinson’s disease not stabilized on levodopa: a review of the current clinical evidence
Authors Bette S , Shpiner DS , Singer C, Moore H
Received 16 April 2018
Accepted for publication 20 June 2018
Published 18 September 2018 Volume 2018:14 Pages 1737—1745
DOI https://doi.org/10.2147/TCRM.S139545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Video abstract presented by Henry Moore.
Views: 2643
Sagari Bette, Danielle S Shpiner, Carlos Singer, Henry Moore
Department of Neurology, Division of Parkinson’s Disease and Movement Disorders, University of Miami – Miller School of Medicine, Miami, FL, USA
Abstract: Safinamide (Xadago®) is a novel medication with both dopaminergic and non-dopaminergic effects, approved first by the European Commission and more recently by the US Food and Drug Administration (FDA) as an adjunctive treatment to carbidopa/levodopa in patients with mid- to late-stage Parkinson’s disease (PD) and motor fluctuations. It works through multiple mechanisms, namely as a reversible selective monoamine oxidase-B inhibitor and through modulation of glutamate release. Safinamide is extensively metabolized via oxidation to several inactive metabolites that are excreted primarily through the urine. Several large Phase III clinical trials of patients with advanced PD with motor fluctuations have shown that safinamide, administered orally at doses of 50–100 mg daily, increased ON time with no or non-troublesome dyskinesia, decreased daily OFF time, improved overall motor function (as measured by Unified Parkinson’s Disease Rating Scale [UPDRS] part III total score), and quality of life (as measured by Clinical Global Impression-Change and 39-item Parkinson’s Disease Questionnaire). In large clinical trials of patients with early PD on a single dopamine agonist, safinamide administered orally at a dose of 100 mg daily improved overall motor function as measured by UPDRS part III total score; however, some of the results reported were exploratory. Safinamide is generally well-tolerated and safe, with few to no treatment-related adverse events. Safinamide does not cause new or worsening dyskinesia and may be able to reduce this symptom in patients reporting it at baseline. Evidence suggests that safinamide is a good option for add-on therapy to carbidopa/levodopa in patients with advanced PD with motor complications, but there is still insufficient evidence to recommend it as monotherapy or add-on therapy in patients with early PD.
Keywords: Parkinson’s disease, safinamide, MAO-B inhibitor, motor fluctuations, dyskinesia
Introduction
Parkinson’s disease (PD) is a neurodegenerative condition characterized pathologically by the progressive loss of dopaminergic neurons in the substantia nigra and the presence of Lewy bodies, and clinically by the development of both motor and non-motor symptoms. A shortage of dopamine is the hallmark neurochemical abnormality early on; however, as the disease advances, additional brain regions and neurotransmitters become involved.1,2 Motor symptoms including tremor, rigidity, and bradykinesia can be managed with a combination of dopamine-precursor levodopa, dopamine agonists (DA), and monoamine oxidase-B (MAO-B) inhibitors. Levodopa is often used in combination with aromatic L-amino acid decarboxylase and/or catechol-O-methyl-transferase (COMT) inhibitors to prolong its half-life and optimize the amount that reaches the brain. The goal of these therapies is to increase stimulation of post-synaptic dopamine receptors, through agonist activity (DA) or by increasing the amount of dopamine available (others).2,3 Amantadine is an N-methyl-D-aspartate (NMDA) receptor blocker which is primarily used as an anti-dyskinetic agent; though it has also been shown to enhance dopamine release and inhibit its reuptake.2 Anticholinergic agents including trihexyphenidyl and benztropine can also be useful.1,2 However, over time, fluctuating levels of these medications (particularly levodopa) in the setting of disease progression lead to the development of motor complications characterized by dyskinesia and periods of OFF time when medication effects diminish and PD motor symptoms recur, at times unpredictably.1
The loss of tonic dopamine regulation in PD as well as the relatively short half-life of levodopa are hypothesized to play a role in the development of motor complications. It has therefore been suggested that using MAO-B or COMT inhibitors to block dopamine metabolism, thereby maintaining a more stable level of dopamine in the postsynaptic cleft, may be useful in the treatment of these complications.3
Safinamide (Xadago®; US WorldMeds LLC, Louisville, KY, USA) is a novel MAO-B inhibitor with both dopaminergic and non-dopaminergic mechanisms of action. It was approved in February 2015 in the European Union and in March 2017 by the US Food and Drug Administration (FDA), either as add-on to levodopa or in combination with other PD medications, for the treatment of patients with mid- to late-stage (advanced) PD with motor fluctuations. When compared to the other currently available MAO-B inhibitors, safinamide has several unique features which may provide an advantage to some PD patients.4,5 A summary of safinamide’s key characteristics can be found in Table 1.
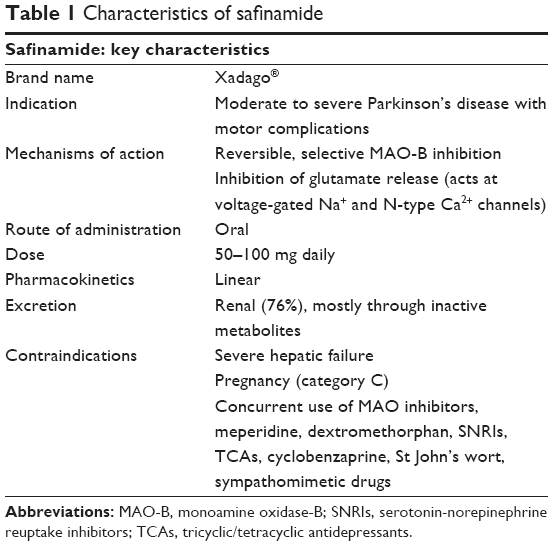 | Table 1 Characteristics of safinamide |
Pharmacokinetics
The recommended dosage of safinamide is 50–100 mg daily, administered orally. The drug shows linear pharmacokinetics up to a dose of 300 mg (three times the maximum recommended daily dose). It is absorbed rapidly, with maximum concentration (Cmax) reached 2–4 hours after ingestion in fasting conditions, with steady-state concentration reached in 1 week. First-pass effect is negligible and food does not impact absorption.6,7 The absolute bioavailability is 95%, with a volume of distribution of 165 L, suggesting extensive extravascular distribution.
Safinamide’s elimination half-life is approximately 20–26 hours, and only 5% is excreted unchanged through the urine.6 This is significantly longer than the half-lives of the other MAO-B inhibitors, which may be advantageous in certain circumstances or patient populations (for example, in patients undergoing long surgical procedures under anesthesia). Metabolism occurs via three pathways: amide hydrolytic oxidation (to safinamide acid), oxidative cleavage of the ether bond (to O-debenzylated safinamide), and oxidation of safinamide or safinamide acid (to N-dealkylated acid). None of these metabolites are pharmacologically active. Excretion is primarily through the urine (76%).6,8
Moderate to severe renal impairment does not impact serum concentrations and no dosage adjustment is required. However, mild to moderate hepatic impairment has been shown to increase plasma concentrations by 30% and 80%, respectively, as assessed by area under the plasma concentration-time curve; therefore, in patients with moderate hepatic impairment the maximum recommended daily dose is 50 mg. Safinamide is contraindicated for patients with severe hepatic impairment.2,9,10 No dose adjustments are recommended for age, gender, or race. Safinamide is pregnancy category C and is not recommended for use in breastfeeding mothers due to evidence of teratogenicity seen in animal models.11,12 Animal studies also identified a risk of retinal degeneration, and for this reason safinamide should be used with caution in patients with a history of retinal/macular degeneration, uveitis, personal or family history of hereditary retinal disease, albinism, retinitis pigmentosa, or retinopathy. According to the manufacturer, these patients should be monitored closely for vision changes while on safinamide.12
Pharmacodynamics
MAO-B is an enzyme occurring naturally in glial cells that metabolizes biogenic amines, including dopamine. It also plays a role in the production of reactive oxygen species, which contribute to the production of neurotoxins shown to accelerate neurodegenerative processes. It follows that MAO-B inhibitors may be neuroprotective, a theory that has been supported by several studies. Proposed mechanisms include direct stabilization of mitochondrial membranes, activation of nuclear transcription factors (promoting cellular survival), and the promotion of anti-apoptotic processes.13–16
Two classes of selective MAO-B inhibitors are currently available. The first consists of the irreversible selective MAO-B inhibitors and includes selegiline and rasagiline. Notably, these drugs lose their MAO-B selectivity at high doses (>20 mg/day for selegiline and >2 mg/day of rasagiline); therefore, there is a low risk of tyramine-related hypertension (the so-called “cheese effect”, caused by simultaneous inhibition of MAO-A) associated with these drugs. Safinamide belongs to the second class: the reversible selective MAO-B inhibitors. Safinamide is vastly more selective for MAO-B than MAO-A (1,000 times more selective in humans), when compared with rasagiline (203 times) or selegiline (127 times).17 Therefore, while it is still contraindicated in combination with other MAO inhibitors or sympathomimetic drugs, the “cheese effect” has not been demonstrated in safinamide and in theory the risk is much lower.18–20
Safinamide is unique in that in addition to its MAO-B effects, it also inhibits voltage-gated sodium and N-type calcium channels, modulating glutamate release and causing NMDA receptor-antagonizing effects similar to amantadine.5 Furthermore, its pharmacology suggests that it may also affect the metabolism of other biogenic amines besides dopamine. Consequently, it has been suggested that safinamide may have some benefit for non-motor symptoms of PD including apathy, depression, and cognition (perhaps through increased vigilance, similar to effects seen in patients taking other NMDA receptor antagonists).21 Due to its effects on dopamine and sodium and calcium channels, it has also been tried, and shown promise, in the treatment of pain syndromes in PD patients.22
Finally, there is some evidence, both in vitro and in vivo (animal models), that safinamide has neuroprotective properties thought to be related to both its MAO-B inhibition and ion channel blocking activity.16
Drug interactions
Safinamide’s pharmacodynamic properties pose its greatest danger for drug interactions. Specifically, there is a risk of hypertensive crisis when used in combination with other MAO inhibitors, or serotonin syndrome when used in combination with dextromethorphan, meperidine (or similar opioids), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic/tetracyclic antidepressants (TCAs), cyclobenzaprine, St John’s wort, and/or other sympathomimetic medications. For this reason, the concurrent use of safinamide with these drugs is not recommended by the manufacturer. Safinamide may be used with selective serotonin reuptake inhibitors, but caution is advised.10,12
Safinamide has not been found to inhibit or induce any of the CYP/CYP450 enzymes that have been tested (CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, or CYP3A3/5). There were no interactions found when safinamide was combined with CYP1A2 substrate caffeine, CYP3A4 substrate midazolam, or CYP3A4 inhibitor ketoconazole.10,23 Safinamide is not a substrate for P-glycoprotein, BCRP, OAT1B1, OAT1B3, OATP1A2, or OATP2B1. Safinamide acid (a safinamide metabolite) is a substrate for OAT3, but this is not believed to be clinically relevant; it is not a substrate for OAT1 or OCT2. Safinamide acid has not been found to inhibit OCT2, MATE1, or MATE2-K.10
Therapeutic efficacy
A summary of the therapeutic efficacy of safinamide, demonstrated by pivotal trials, can be found in Table 2.
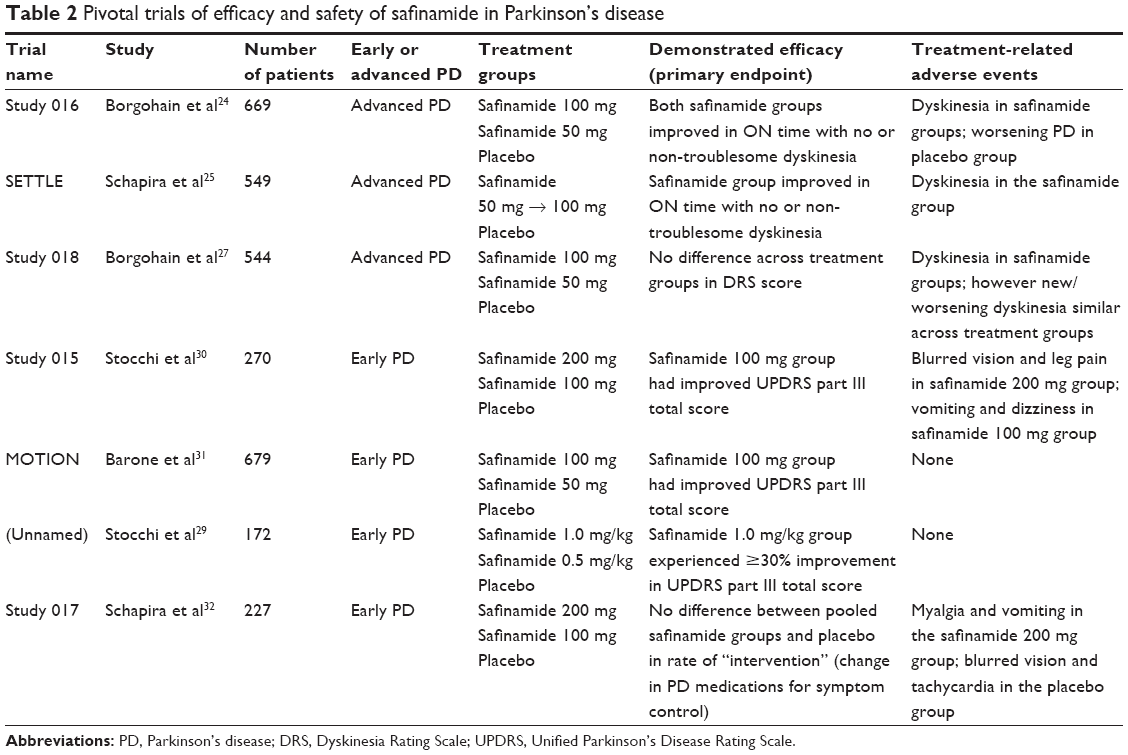 | Table 2 Pivotal trials of efficacy and safety of safinamide in Parkinson’s disease |
Advanced PD
Short-term treatment
Study 016 was a 24-week, double-blind, placebo-controlled Phase III trial of 669 patients with PD and motor fluctuations taking levodopa who were randomized to once-daily safinamide 100 mg, safinamide 50 mg, or placebo. The study used hierarchical analysis of data collected by patient diaries and clinician assessment. Compared to placebo, both safinamide 100 mg and safinamide 50 mg significantly improved the primary endpoint of change in mean daily total ON time with no or non-troublesome dyskinesia (0.55 hours; 95% CI: 0.12–0.99; P=0.0130 and 0.51 hours; 95% CI: 0.07–0.94; P=0.0223, respectively). For secondary endpoints, both safinamide 100 mg and safinamide 50 mg showed significant improvement compared to placebo in total daily OFF time (−0.6; 95% CI: −1.0 to −0.2; P=0.0034 and −0.6; 95% CI: −0.9 to −0.2; P=0.0043, respectively) and Unified Parkinson’s Disease Rating Scale (UPDRS) part III score (−2.6; 95% CI: −4.1 to −1.1; P=0.0006 and −1.8; 95% CI: −3.3 to −0.4; P=0.0138, respectively). Other secondary and tertiary endpoints that showed significant improvement for both safinamide groups vs placebo included Clinical Global Impression-Change (CGI-C) score (64.3% of patients improved; P=0.0089 for safinamide 100 mg; 66.4% of patients improved; P=0.0010 for safinamide 50 mg) and OFF time after the morning levodopa dose (−1.2; 95% CI: −1.0 to −0.2; P=0.0011 for safinamide 100 mg; −1.1; 95% CI: −0.9 to −0.2; P=0.0031 for safinamide 50 mg).24
The safinamide treatment as add-on to levodopa in idiopathic PD (SETTLE) study was a 24-week, double-blind, placebo-controlled Phase III trial of 549 patients with PD and motor fluctuations on a stable dose of levodopa and other PD medications who were randomized to safinamide (50 mg, increased to 100 mg after 2 weeks) or placebo. For the primary endpoint of mean increase in daily ON time with non-troublesome dyskinesia, safinamide showed significant improvement compared to placebo (1.42 hours vs 0.57 hours, respectively; mean difference 0.96 hours; 95% CI: 0.56–1.37; P<0.001). This improvement was seen at 2 weeks and maintained for the duration of the study. Safinamide also showed significant improvement compared to placebo in key secondary outcomes of decrease in daily OFF time (−1.56 to −0.54 hours, respectively; mean difference −1.03; 95% CI: −1.40 to −0.67; P<0.001), improvement in UPDRS part III score (−3.43 to −1.83, respectively; mean difference −1.82; 95% CI: −3.01 to −0.62; P=0.003), improvement in CGI-C score (57.7% vs 41.8%, respectively; odds ratio 1.92; 95% CI: 1.36–2.70; nominal P<0.001), and improvement in 39-item Parkinson’s Disease Questionnaire (PDQ-39) score (−3.17 to −0.68, respectively; mean difference −2.33; 95% CI: −3.98 to −0.68; nominal P=0.006).25
Cattaneo et al performed a post hoc analysis of pooled data of 971 patients in the safinamide 100 mg and placebo groups from study 016 and SETTLE. Safinamide 100 mg showed significant improvement in both ON time with no or non-troublesome dyskinesia and OFF time in patients taking levodopa monotherapy (safinamide as the first adjunct to levodopa) and in patients taking levodopa and other PD medications (DA, COMT inhibitor, and amantadine, alone or in combination). Patients termed “mild fluctuators” (4 hours of daily OFF time) who were in the safinamide 100 mg group also showed significant improvement in both ON time with no or non-troublesome dyskinesia and OFF time. Safinamide 100 mg significantly improved several secondary endpoints including mean UPDRS part II score (activities of daily living), mean UPDRS part III score, and scores of individual PD cardinal symptoms (including bradykinesia, rigidity, tremor, and gait), with the exception of postural stability, compared to placebo.26
In summary, safinamide improves ON time with no or non-troublesome dyskinesia in patients with PD and motor fluctuations taking levodopa only or levodopa with other PD medications. Safinamide also improves total daily OFF time, UPDRS part III total score, and CGI-C score, when compared to placebo.
Long-term treatment
Study 018 was an 18-month extension of 544 patients from study 016. There was no significant difference in the primary endpoint of Dyskinesia Rating Scale (DRS) score, using a modified scoring system of the DRS, between safinamide 100 mg vs placebo or safinamide 50 mg vs placebo (−0.59; 95% CI: −1.40–0.21; P=0.1469 and −0.51; 95% CI: −1.32–0.29; P=0.2125, respectively). However, an ad hoc sub-group analysis of moderate to severe dyskinetic patients (DRS >4) taking safinamide 100 mg had significant improvement in DRS score compared to placebo (−1.50; 95% CI: −2.33 to −0.11; P=0.0317). This significant improvement was sustained even when excluding patients who had a reduction in levodopa dose during the 2-year study. This improvement in DRS score may be related to safinamide’s known NMDA receptor antagonizing effect.5 A dose-dependent relationship may exist to explain the difference between the 100 mg and 50 mg doses, though this has not been formally studied. Furthermore, for the secondary endpoint of increase in total daily ON time with non-troublesome dyskinesia, both safinamide 100 mg and safinamide 50 mg were superior to placebo (1.18 hours; 95% CI: 0.39–1.27; P=0.0002 and 1.01 hours; 95% CI: 0.23–1.11; P=0.0031, respectively). Other endpoints that showed significant improvement for both safinamide doses compared to placebo included total daily OFF time, ON time without dyskinesia, and CGI-Severity score. Patients taking safinamide 100 mg were able to reduce their mean dose of levodopa during the 2-year study.27
Cattaneo et al also performed a post hoc analysis of study 018 on the long-term effects of safinamide on dyskinesia. In patients with or without dyskinesia and with no changes in levodopa dose during the 2-year study, patients in both safinamide groups had improvement in DRS score compared to placebo, with statistical significance for the safinamide 100 mg group (P=0.0488). In patients with dyskinesia at baseline, with or without changes in levodopa dose, patients in both safinamide groups had improvement in DRS score compared with placebo, again with statistical significance for the safinamide 100 mg group (P=0.0153). In patients with dyskinesia at baseline and no change in levodopa dose, patients in both safinamide groups had improvement in DRS score compared with placebo, but the safinamide 100 mg group did not reach statistical significance (P=0.0546). Finally, in patients without dyskinesia at baseline, DRS score remained relatively unchanged throughout the 2-year study in all treatment groups.28
In summary, safinamide provides sustained improvement over 2 years in ON time with no or non-troublesome dyskinesia and OFF time in patients with PD and motor fluctuations taking levodopa only or levodopa with other PD medications. Patients who took safinamide 100 mg daily had improvement in DRS score, unrelated to change in levodopa dose. Patients without dyskinesia at baseline did not develop dyskinesia on safinamide.
Early PD
Short-term treatment
An early study of safinamide by Stocchi et al investigated 172 patients with early PD on no therapy or on a stable dose of a single DA who were randomized to safinamide 1.0 mg/kg (median dose 70 mg), safinamide 0.5 mg/kg (median dose 40 mg), or placebo. For the primary endpoint of ≥30% improvement in UPDRS part III score, the safinamide 1.0 mg/kg group showed significant improvement compared with placebo (37.5% of patients improved vs 21.4%; P=0.016). This effect was enhanced by sub-group analysis showing that 47.1% of patients on stable DA therapy in the safinamide 1.0 mg/kg group improved compared with placebo (47.1% vs 20.6%; P=0.024). The authors state that the reason for this effect is not well-understood.29
Study 015 was a 24-week, double-blind, placebo-controlled Phase III trial of 270 patients with early PD on a stable dose of a single DA who were randomized to once-daily safinamide 200 mg, safinamide 100 mg, or placebo. Using hierarchical analysis, the study showed mean improvement from baseline to week 24 in the primary outcome measure of UPDRS part III total score of −3.90 (SD ±6.01) for safinamide 200 mg, −6.0 (SD ±7.18) for safinamide 100 mg, and −3.60 (SD ±7.08) for placebo. Only safinamide 100 mg vs placebo was significant (point estimate: −1.9; 95% CI: −3.7 to −0.1; P=0.0419), considered an exploratory analysis. Secondary exploratory analyses of CGI-C score and UPDRS part II score for safinamide 100 mg vs placebo also showed significant improvement (P=0.0293 and P=0.0248, respectively).30
The safinamide add-on to DA in early idiopathic PD (MOTION) study was a 24-week, placebo-controlled Phase III trial of 679 patients with early PD on a stable dose of a single DA who were randomized to once-daily safinamide 100 mg, safinamide 50 mg, or placebo. Hierarchical analysis of the primary endpoint of improvement in UPDRS part III score showed significant improvement for safinamide 100 mg and borderline significant improvement for safinamide 50 mg. Safinamide 100 mg also had significant improvement in the secondary endpoint of PDQ-39 score but borderline improvement in activities of daily living.31
In summary, safinamide 100 mg improves UPDRS part III total score in patients with early PD on a stable dose of a single DA.
Long-term treatment
Study 017 was a 12-month extension of 227 patients from study 015. The primary endpoint was time from baseline randomization to “intervention,” ie, increase in DA dose; addition of another DA, levodopa, or other PD treatment; or discontinuation of safinamide due to lack of efficacy. Pooled data from the safinamide 200 mg and safinamide 100 mg groups did not reach statistical significance. However, post hoc analysis showed that safinamide 100 mg had a lower rate of intervention than placebo (25% vs 51%; P<0.05). For secondary endpoints, safinamide 100 mg vs placebo had a greater change in UPDRS part III score (−4.3 vs −1.0; point estimate: −2.96; 95% CI: −5.45 to −0.46; P=0.0207) and UPDRS part II score (−1.7 vs −0.3; point estimate: −1.74; 95% CI: −2.88 to −0.61; P=0.0029).32
In summary, over 18 months, safinamide 100 mg resulted in a lower rate of intervention (increase in DA dose; addition of another DA, levodopa or other PD treatment; or discontinuation of safinamide) and greater improvement in UPDRS part III and part II total scores in patients with early PD on a stable dose of a single DA.
Other trials
A prospective open-label study of safinamide in clinical practice assessed 50 patients with PD and motor fluctuations. Patients were treated with either safinamide 50 mg or 100 mg and CGI-C and change in daytime OFF time were the primary endpoints assessed at 3 months. A total of 57.4% of patients improved in motor and/or non-motor fluctuations, with significant decrease in daytime OFF time (0.9±0.6 hours/day). Of patients taking safinamide, 27.6% were able to lower their levodopa equivalent daily dose (LEDD).33 As with other studies,27,28 safinamide 100 mg was more effective in reducing dyskinesia, though no mechanism was specifically postulated.33
A retrospective study of safinamide in clinical practice assessed 91 patients with PD and motor fluctuations. If patients were already taking a MAO-B inhibitor, it was stopped 2 weeks prior to initiation of safinamide. Patients were started on safinamide 50 mg daily with the possibility of being increased to safinamide 100 mg daily. All primary endpoints showed improvement at 12 months: change in UPDRS part III score (P<0.0001), change in OFF time (P<0.0001), change in ON time with dyskinesia (P<0.0008), and change in Unified Dyskinesia Rating Scale walking and balance item nine score (P<0.0001). The 21 patients who switched to safinamide from another MAO-B inhibitor showed significant improvement in OFF time and in decrease of LEDD.34
Currently there are no head-to-head randomized clinical trials comparing safinamide to other MAO-B inhibitors. Therefore, there is no data to guide choice of safinamide vs other MAO-B inhibitors or how to switch between safinamide and other medications with a similar mechanism of action.
In summary, in regular clinical practice, safinamide reduces motor fluctuations (improves OFF time, reduces dyskinesia) and improves UPDRS part III score. In patients taking another MAO-B inhibitor who still have uncontrolled motor fluctuations, switching to safinamide may be of benefit, though this result needs to be further verified in randomized clinical trials.
Tolerability/adverse events
A summary of the tolerability of and adverse events related to safinamide therapy demonstrated by pivotal trials can be found in Table 2.
Advanced PD
Short-term treatment
Study 016 showed that 67% of patients experienced treatment-emergent adverse events (TEAEs), with similar incidence across treatment groups. The majority of TEAEs were rated mild or moderate in severity. Dyskinesia was the only treatment-related TEAE reported more frequently in the safinamide groups, without a dose-dependent relationship. The study noted that other measures indicated that the dyskinesia was non-troublesome and that safinamide did not worsen the severity of dyskinesia. Worsening PD was the only treatment-related TEAE reported more frequently in the placebo group. The incidence of serious adverse events (SAEs) was higher in the safinamide 100 mg and placebo groups, without a clear pattern and not considered treatment-related. Seven deaths occurred during the study, none considered treatment-related.24
The SETTLE study showed similar incidence of TEAEs across treatment groups, with the majority of TEAEs rated as mild to moderate in severity. There was a similar incidence of TEAEs that led to interruption of study drug treatment across treatment groups. Dyskinesia was the only frequently reported TEAE that was more common in the safinamide group than the placebo group (14.6% vs 5.5%, respectively). There was a low incidence of SAEs, with fewer SAEs in the safinamide group than the placebo group (6.6% vs 9.5%, respectively) and none considered treatment-related. The three deaths during the study were not considered treatment-related.25
Long-term treatment
Study 018 mirrored the findings of study 016 and showed similar incidence of TEAEs across treatment groups. Again, only dyskinesia occurred more frequently in the safinamide 100 mg and safinamide 50 mg groups than the placebo group (27.8% and 31.2%, respectively, vs 21.7%). However, the incidence of new or worsening dyskinesia was similar between treatment groups.27
Early PD
Short-term treatment
The early study of safinamide by Stocchi et al showed similar incidence of TEAEs across treatment groups. No SAEs or specific treatment-related TEAEs or SAEs were described.29
Study 015 showed <10% incidence of common TEAEs for each treatment group. For safinamide 200 mg, blurred vision and leg pain were considered treatment-related. For safinamide 100 mg, vomiting and dizziness were considered treatment-related. Four patients experienced SAEs, none considered treatment-related.30
The MOTION study showed similar common TEAEs to Study 015, with a low incidence of SAEs that was similar across treatment groups.31
Long-term treatment
Study 017 had similar findings to study 015. It showed a similar incidence of TEAEs across treatment groups, with 67.2% of total patients reporting TEAEs, most of which were mild to moderate in severity. Only two were considered possibly treatment-related: myalgia and vomiting in a patient taking safinamide 200 mg and blurred vision and tachycardia in a patient taking placebo. A total of 7.9% experienced SAEs, none of which were considered treatment-related in patients taking safinamide; vasovagal syncope was considered possibly treatment-related in a patient taking placebo. There were two deaths, neither of which was considered treatment-related.32
Other trials
In the prospective open-label study of clinical practice, safinamide was well-tolerated except in patients aged 75 years or older or with advanced stage PD; presumably, the seven patients who developed a confusional syndrome and had to discontinue safinamide were in these groups.33
In the retrospective study of clinical practice, the eight patients who discontinued safinamide in the first month were significantly older (aged 76.70±7.58 years) with significantly worse UPDRS part III scores (21.13±12.187) in the ON state.34
Summary of tolerability/adverse events
Incidence of TEAEs was similar across treatment groups and most TEAEs were mild to moderate in severity. Short-term and long-term studies of safinamide in early and advanced PD show low incidence of treatment-related TEAEs. While several studies found dyskinesia to be a treatment-related TEAE in patients with advanced PD, study 018 clarified that the incidence of new or worsening dyskinesia was similar across treatment groups over 2 years. No SAEs or deaths in any study were treatment-related in patients taking safinamide. In studies of clinical practice, patients aged 75 years or older and with more severe stage PD were less likely to tolerate safinamide. Overall, however, safinamide is well-tolerated in patients with PD.
Current status
Safinamide was approved by the FDA on March 21, 2017 as adjunctive therapy to carbidopa/levodopa in patients with PD with OFF time.35
The European Commission granted marketing authorization for safinamide throughout the European Union on February 24, 2015 as adjunctive therapy to levodopa, alone or in combination with other medications for PD, in patients with mid- to late-stage PD with motor fluctuations.36
Conclusions/future directions
Safinamide is a highly selective MAO-B inhibitor that also modulates glutamate release through action at voltage-gated sodium and N-type calcium channels. It is oxidized into several inactive metabolites and excreted primarily through the urine. It does not inhibit or induce CYP/CYP450 enzymes. It should not be taken with other MAO inhibitors, SNRIs, TCAs, certain opioids, dextromethorphan, cyclobenzaprine, or other medications that in combination may cause serotonin syndrome. There is no restriction on consumption of tyramine-containing foods while taking safinamide. Safinamide is approved by the FDA and European Commission for use as adjunctive treatment to levodopa (alone or in combination with other PD medications) in patients with advanced PD and motor fluctuations. This approval is based on multiple large Phase III clinical trials demonstrating that safinamide improves ON time with no or non-troublesome dyskinesia and OFF time in patients with advanced PD and motor fluctuations. Safinamide is well-tolerated and does not cause new or worsening dyskinesia.
While clinical trials of safinamide in early PD have shown positive results, there is still insufficient data to pursue approval for use in early PD, either as adjunctive treatment for patients taking a DA or as monotherapy. Only the MOTION study showed statistical significance for safinamide 100 mg vs placebo as adjunct therapy for patients taking a DA for the primary endpoint of improvement in UPDRS part III score during short-term follow-up,31 a finding that has not been replicated. Furthermore, the trials to date have not shown statistically significant improvement in primary endpoints for long-term therapy. In addition to confirming the efficacy of safinamide in early PD, such clinical trials could also investigate its potential neuroprotective effects. As Blair and Dhillon suggest, head-to-head trials of safinamide and other MAO-B inhibitors or other adjunctive treatments to levodopa could also provide meaningful clinical data to better inform clinicians on which drug to select based on patient demographics, symptoms, disease stage, and other factors.37 Finally, non-motor symptoms of PD continue to pose treatment challenges and deSouza and Schapira recommend investigating the effect of safinamide on non-motor symptoms as a primary endpoint.38 While other MAO-B inhibitors are not used to specifically treat non-motor symptoms, safinamide may have benefit given its unique combination of mechanisms of action.
Safinamide is a valuable addition to the menu of medications used to treat advanced PD complicated by motor fluctuations and holds promise for treatment of early PD and non-motor symptoms of PD.
Acknowledgment
Sagari Bette and Danielle S Shpiner are co-first authors for this study.
Author contributions
SB and DS: literature review and manuscript drafting; CS: manuscript review; HM: literature review and manuscript review. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Connolly BS, Lang AE. Pharmacological treatment of Parkinson disease: a review. JAMA. 2014;311(16):1670–1683. | ||
Müller T, Foley P. Clinical Pharmacokinetics and Pharmacodynamics of Safinamide. Clin Pharmacokinet. 2017;56(3):251–261. | ||
Riederer P, Gerlach M, Müller T, Reichmann H. Relating mode of action to clinical practice: dopaminergic agents in Parkinson’s disease. Parkinsonism Relat Disord. 2007;13(8):466–479. | ||
US Food and Drug Administration. FDA approves drug to treat Parkinson’s disease [press release]. Silver Spring, MD: US Food and Drug Administration; 2017 [March 21]. Available from: https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm547852.htm. Accessed June 28, 2018. | ||
Caccia C, Maj R, Calabresi M, Maestroni S, et al. Safinamide: from molecular targets to a new anti-Parkinson drug. Neurology. 2006;67(7 Suppl 2):S18–S23. | ||
Marzo A, dal Bo L, Monti NC, et al. Pharmacokinetics and pharmacodynamics of safinamide, a neuroprotectant with antiparkinsonian and anticonvulsant activity. Pharmacol Res. 2004;50(1):77–85. | ||
Seithel-Keuth A, Johne A, Freisleben A, et al. Absolute Bioavailability and Effect of Food on the Disposition of Safinamide Immediate Release Tablets in Healthy Adult Subjects. Clin Pharmacol Drug Dev. 2013;2(1):79–89. | ||
Leuratti C, Sardina M, Ventura P, et al. Disposition and metabolism of safinamide, a novel drug for Parkinson’s disease, in healthy male volunteers. Pharmacology. 2013;92(3–4):207–216. | ||
Deeks ED. Safinamide: first global approval. Drugs. 2015;75(6):705–711. | ||
US Food and Drug Administration. Xadago (safinamide): Clinical pharmacology biopharmaceutics review(s); FDA 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/207145Orig1s000TOC.cfm. Accessed June 28, 2018. | ||
European Medicines Agency. Safinamide: Summary of product characteristics; EMA 2014. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002396/human_med_001847.jsp&mid=WC0b01ac058001d124. Accessed June 28, 2018. | ||
Xadago® (safinamide) [package insert]. Louisville, KY: US WorldMeds; 2017. | ||
Akao Y, Maruyama W, Yi H, Shamoto-Nagai M, Youdim MB, Naoi M. An anti-Parkinson’s disease drug, N-propargyl-1(R)-aminoindan (rasagiline), enhances expression of anti-apoptotic bcl-2 in human dopaminergic SH-SY5Y cells. Neurosci Lett. 2002;326(2):105–108. | ||
Akao Y, Maruyama W, Shimizu S, Yi H, et al. Mitochondrial permeability transition mediates apoptosis induced by N-methyl(R)salsolinol, an endogenous neurotoxin, and is inhibited by Bcl-2 and rasagiline, n-propargyl-1(r)-aminoindan. J Neurochem. 2002;82(4):913–923. | ||
Müller T, Przuntek H, Rieks M, Mackowiak A. Selegiline reduces cisplatin-induced neuronal death in neuroblastoma cells. Neurol Res. 2008;30(4):417–419. | ||
Sadeghian M, Mullali G, Pocock JM, et al. Neuroprotection by safinamide in the 6-hydroxydopamine model of Parkinson’s disease. Neuropathol Appl Neurobiol. 2016;42(5):423–435. | ||
Binda C, Wang J, Pisani L, et al. Structures of human monoamine oxidase B complexes with selective noncovalent inhibitors: safinamide and coumarin analogs. J Med Chem. 2007;50(23):5848–5852. | ||
di Stefano AF, Rusca A. Pressor response to oral tyramine during co-administration with safinamide in healthy volunteers. Naunyn Schmiedebergs Arch Pharmacol. 2011;384(6):505–515. | ||
Marquet A, Kupas K, Johne A, et al. The effect of safinamide, a novel drug for Parkinson’s disease, on pressor response to oral tyramine: a randomized, double-blind, clinical trial. Clin Pharmacol Ther. 2012;92(4):450–457. | ||
Cattaneo C, Caccia C, Marzo A, Maj R, Fariello RG. Pressor response to intravenous tyramine in healthy subjects after safinamide, a novel neuroprotectant with selective, reversible monoamine oxidase B inhibition. Clin Neuropharmacol. 2003;26(4):213–217. | ||
Ambrozi L, Danielczyk W. Treatment of impaired cerebral function in psychogeriatric patients with memantine – results of a phase II double-blind study. Pharmacopsychiatry. 1988;21(3):144–146. | ||
Barone P, Cattaneo C, La Ferla R, Bonnizoni E, Sardina M. Significant reduction of pain treatments with safinamide administered as add-on therapy to levodopa in patients with parkinson’s disease and fluctuation [abstract]. Mov Disord. 2015;22(Suppl 1):293. | ||
Krösser S, Marquet A, Gallemann D, et al. Effects of ketoconazole treatment on the pharmacokinetics of safinamide and its plasma metabolites in healthy adult subjects. Biopharm Drug Dispos. 2012;33(9):550–559. | ||
Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229–237. | ||
Schapira AH, Fox SH, Hauser RA, et al. Assessment of Safety and Efficacy of Safinamide as a Levodopa Adjunct in Patients With Parkinson Disease and Motor Fluctuations: A Randomized Clinical Trial. JAMA Neurol. 2017;74(2):216–224. | ||
Cattaneo C, Sardina M, Bonizzoni E. Safinamide as Add-On Therapy to Levodopa in Mid- to Late-Stage Parkinson’s Disease Fluctuating Patients: Post hoc Analyses of Studies 016 and SETTLE. J Parkinsons Dis. 2016;6(1):165–173. | ||
Borgohain R, Szasz J, Stanzione P, et al. Two-year, randomized, controlled study of safinamide as add-on to levodopa in mid to late Parkinson’s disease. Mov Disord. 2014;29(10):1273–1280. | ||
Cattaneo C, Ferla RL, Bonizzoni E, Sardina M. Long-Term Effects of Safinamide on Dyskinesia in Mid- to Late-Stage Parkinson’s Disease: A Post-Hoc Analysis. J Parkinsons Dis. 2015;5(3):475–481. | ||
Stocchi F, Arnold G, Onofrj M, Kwiecinski H, et al. Improvement of motor function in early Parkinson disease by safinamide. Neurology. 2004;63(4):746–748. | ||
Stocchi F, Borgohain R, Onofrj M, et al. A randomized, double-blind, placebo-controlled trial of safinamide as add-on therapy in early Parkinson’s disease patients. Mov Disord. 2012;27(1):106–112. | ||
Barone P, Fernandez H, Ferreira J, et al. Safinamide as add-on therapy to a stable dose of a single dopamine agonist: Results from a randomized, placebo-controlled, 24-week multicenter trial in early idiopathic parkinson disease (PD) patients (MOTION study). Neurology. 2013;80(7 Supp1). | ||
Schapira AH, Stocchi F, Borgohain R, et al. Long-term efficacy and safety of safinamide as add-on therapy in early Parkinson’s disease. Eur J Neurol. 2013;20(2):271–280. | ||
Pagonabarraga J, Kulisevsky J. Safinamide from daily clinical practice: first clinical steps. Rev Neurol. 2017;65(10):433–438. | ||
Mancini F, di Fonzo A, Lazzeri G, et al. Real life evaluation of safinamide effectiveness in Parkinson’s disease. Neurol Sci. 2018;39(4):733–739. | ||
United States Department of Health and Human Services Food and Drug Administration. New drug application approval, NDA 207145: Xadago (safinamide). Silver Spring, MD: Food and Drug Administration; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2017/207145Orig1s000ltr.pdf. Accessed June 28, 2018. | ||
European Commission European Medicines Agency. EPAR summary for the public: Xadago (safinamide). European Medicines Agency; 2015. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002396/human_med_001847.jsp&mid=WC0b01ac058001d124. Accessed June 28, 2018. | ||
Blair HA, Dhillon S. Safinamide: A Review in Parkinson’s Disease. CNS Drugs. 2017;31(2):169–176. | ||
Desouza RM, Schapira A. Safinamide for the treatment of Parkinson’s disease. Expert Opin Pharmacother. 2017;18(9):937–943. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.