")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Safety of Biologics for Psoriatic Patients with Latent Tuberculosis
Authors Yuan L, Li Y, Lin J, Lin X, Yang B, Man MQ , Wang X
Received 16 June 2023
Accepted for publication 20 August 2023
Published 28 August 2023 Volume 2023:16 Pages 2333—2336
DOI https://doi.org/10.2147/CCID.S426253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Liyan Yuan,* Yang Li,* Junjie Lin, Xiuqiu Lin, Bin Yang, Mao-Qiang Man, Xiaohua Wang
Dermatology Hospital, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohua Wang, Dermatology Hospital, Southern Medical University, No. 2 Lujing Road, Guangzhou, 510095, People’s Republic of China, Tel +86-20-87255286, Email [email protected]
Although biologics are effective for psoriasis, immunosuppressive therapy can increase the risk of tuberculosis (TB) reactivation. To determine whether biological therapy for psoriasis increases the risk for TB reactivation, we performed a patients’ chart review to determine the incidence and the relative risk of TB reactivation in psoriatic patients with latent TB infection (LTBI), who received biological therapy, with vs without prior anti-TB therapy.
In addition to routine test for HIV, a total of 1208 patients, including 881 males and 327 females aged 39.0 ± 11.4 years, with moderate-to-severe psoriasis were screened for TB infection prior to biological therapy at our department from January 2020 to June 2021. All patients were negative for HIV and syphilis. LTBI was defined as a positive for Interferon-gamma release assay (IGRA) without any indications of active TB infection according to chest X-rays or CTs, and clinical symptoms. TB reactivation means development of active TB or re-infection of TB in patients who have recovered from previous TB infection. All patients included in this analysis were positive for Interferon-gamma release assay, without any indications of active TB infection at baseline, indicating that they had recovered from previous TB infection. TB reactivation was diagnosed by specialists at the Chest Hospital, based on the findings of chest CTs or X-rays, and clinical symptoms. Of 180 patients who were LTBI (IGRA positive), 69 patients were given prophylaxis therapy (either isoniazid in combination with rifampicin or isoniazid alone) prior to biological therapy. Among the 111 patients without prophylaxis therapy, 37 patients received biological therapy. Thirteen out of the 37 patients without prophylaxis therapy and 43 out of 69 patients with prophylaxis therapy completed 12-week follow-up. Thirty cases receiving prophylaxis therapy and 11 cases receiving no prophylaxis therapy completed 24-week follow-up (Detailed in Figure S1). At the end of 24-week follow-up, the rates of TB reactivation in LTBI patients with and without prophylaxis therapy were 13% (4/30) and 27% (3/11) (relative risk=2.045, 95% CI: 0.5604–6.899. P>0.05), respectively (Table 1). The rates of other adverse events also did not differ significantly between the groups with vs without prophylaxis therapy at either 12-week (46% vs 70%, p=0.19) or 24-week follow-up (91% vs 77%, p=0.41) (Table 2). However, the incidence of overall adverse events was significantly higher at 24-week follow-up compared to 12-week follow-up in the group without prophylaxis therapy (91% vs 46%, p<0.05). In contrast, the incidence of overall adverse events did not differ significantly between 12-week and 24-week in the group with prophylaxis therapy (70% vs 77%, p=0.60) (Table 2).
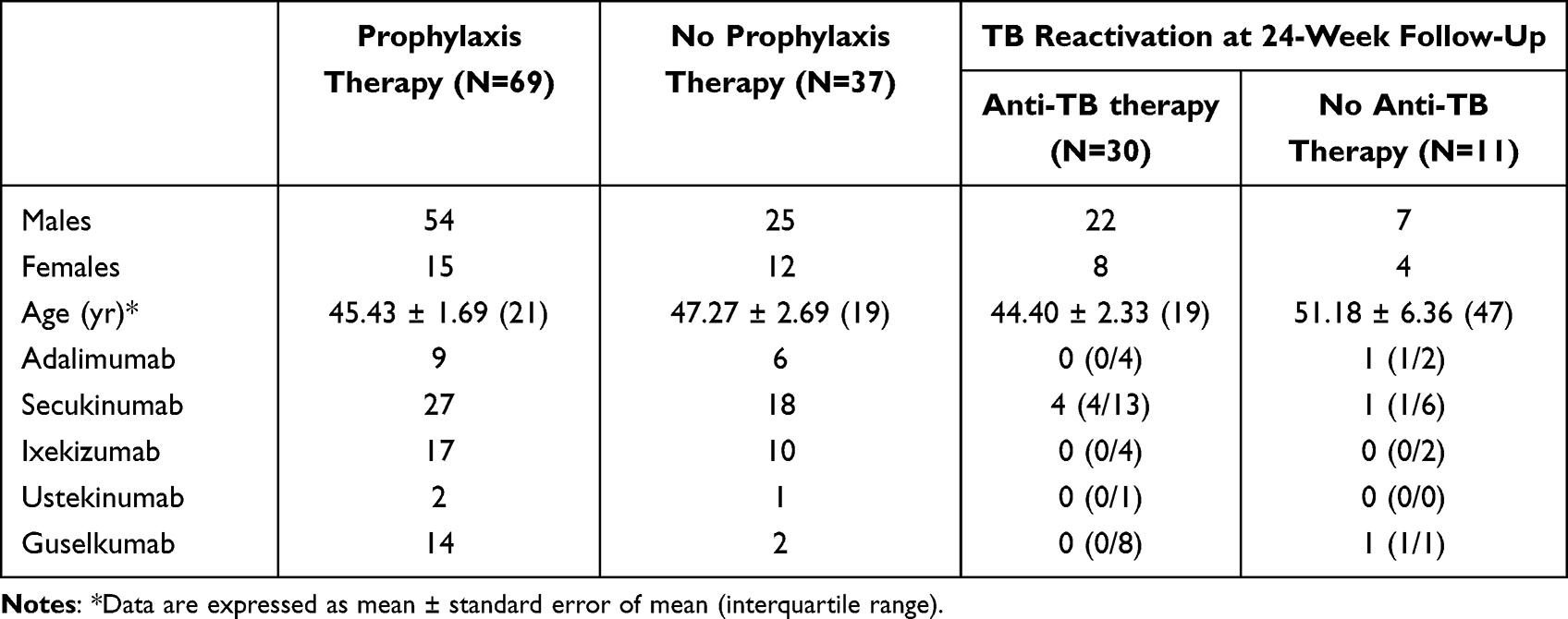 |
Table 1 TB Reactivation at 24-Week Follow-up |
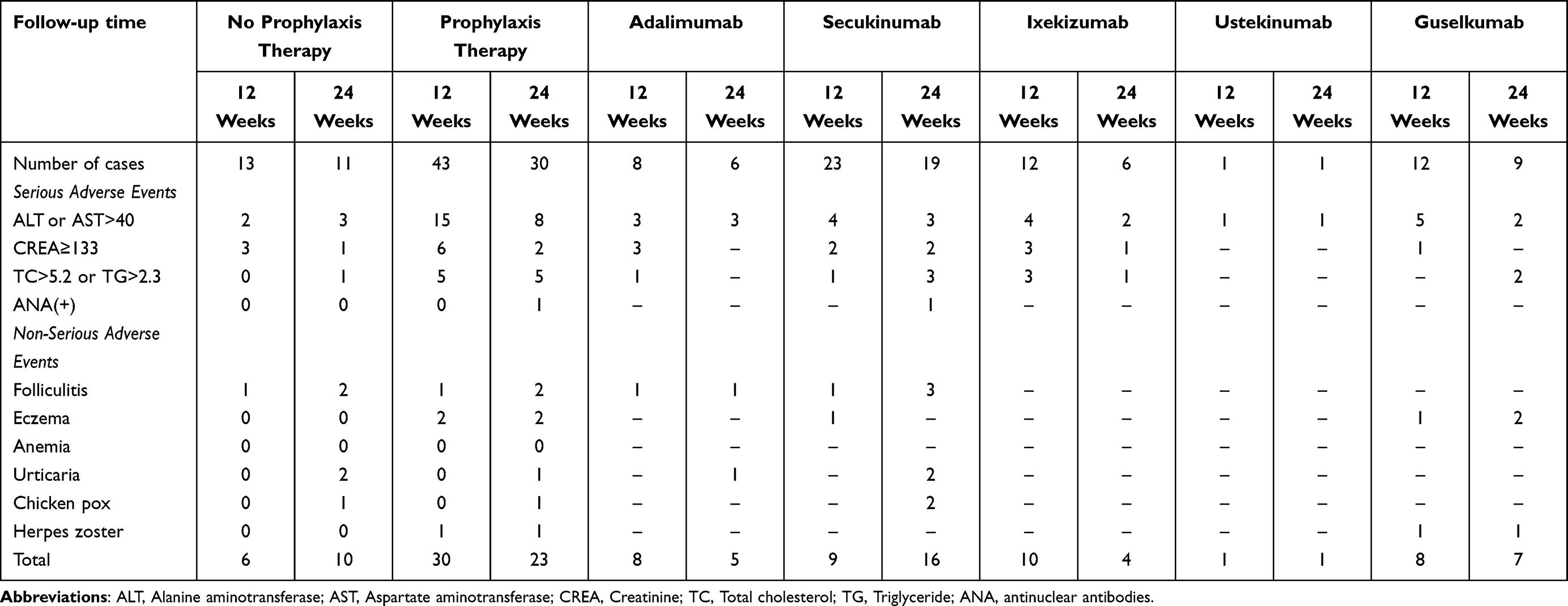 |
Table 2 Adverse Events |
Active TB occurs in approximately 0.1–0.2% of psoriatic patients receiving biological therapy.1 Anti-TB therapy has been recommended for individuals receiving immunosuppressive agents.2 Studies suggest that prophylaxis therapy can prevent TB reactivation in individuals who receive biologics and anti-TB therapy has been recommended.3,4 We demonstrate here that pretreatments with prophylaxis therapy reduced the rate of TB reactivation in psoriatic patients receiving biologics (13% vs 27%). However, a solid conclusion cannot be drawn due to the small sample size. Although evidence suggests that it may not be necessarily crucial to screen LTBI prior to some biological therapies when weighing benefits and costs,5 prophylaxis therapy becomes necessary when using biologics in patients with LTBI because some biological agents such as Ustekinumab and etanercept can increase the risk for TB reactivation.6,7 In addition, the incidence of overall adverse events was higher at 24-week than at 12-week follow-up in patients without prophylaxis therapy. Whether the increased adverse events at 24 weeks were associated with TB reactivation is unclear. Nonetheless, the present study shows that pretreatment with prophylaxis therapy tends to lower the incidence of TB reactivation and overall adverse events in psoriatic patients, suggesting the possible benefits of prophylaxis therapy for psoriatic patients with LTBI, who are undergoing biological treatment. However, study in large cohort is needed to confirm the results of the present study and to differentiate the contribution of individual biological agent to TB reactivation and adverse events. Additionally, it cannot exclude the possibility that the incidence of active TB following biological treatment may include some new infected cases because the positive rate of TB is extremely high in Guangdong, China.
Data Sharing Statement
All data pertinent to this report are presented in the manuscript.
Ethics Statement
This work was reviewed and approved by the ethics committee of Dermatology Hospital, Southern Medical University (#GDDHLS-20190304). Patients’ consent was not required because this was a retrospective study in which all patients’ information was deidentified. This study was carried out in compliance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest.
References
1. World health Organization. Global tuberculosis report 2020. https://www.who.int/publications/i/item/9789240013131.
2. Pradhan S, Madke B, Neema S, Kabra P, Singh AL, Yadav S. Screening of latent tuberculous infection (LTBI) before starting anti-tumor necrosis factor therapy in patients with psoriasis: a primer for clinical dermatologist. Indian J Dermatol. 2021;66:501–507.
3. Puig L, Tsai TF, Bhutani T, et al. Safety in moderate-to-severe plaque psoriasis patients with latent tuberculosis treated with guselkumab and anti-tuberculosis treatments concomitantly: results from pooled Phase 3 VOYAGE 1 & VOYAGE 2 trials. J Eur Acad Dermatol Venereol. 2020;34(8):1744–1749. doi:10.1111/jdv.16460
4. Kaushik SB, Lebwohl MG. Psoriasis: which therapy for which patient: focus on special populations and chronic infections. J Am Acad Dermatol. 2019;80(1):43–53. doi:10.1016/j.jaad.2018.06.056
5. Nogueira M, Warren RB, Torres T. Risk of tuberculosis reactivation with interleukin (IL)-17 and IL-23 inhibitors in psoriasis - time for a paradigm change. J Eur Acad Dermatol Venereol. 2021;35:824–834. doi:10.1111/jdv.16866
6. Elewski BE, Baddley JW, Deodhar AA, et al. Association of secukinumab treatment with tuberculosis reactivation in patients with psoriasis, psoriatic arthritis, or ankylosing spondylitis. JAMA Dermatol. 2021;157(1):43–51. doi:10.1001/jamadermatol.2020.3257
7. Khanna U, Gallop J, Ellis A, et al. Routine rescreening for latent tuberculosis has low utility in patients with chronic immune-mediated inflammatory diseases treated with biologics: a single-center, retrospective cohort study. J Am Acad Dermatol. 2022;87:841–843. doi:10.1016/j.jaad.2022.05.027
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.