Back to Journals » Research and Reports in Tropical Medicine » Volume 5
Safety of antimalarial drugs exposure during early pregnancy
Authors Tagbor H, Antwi G, Dogbe J
Received 10 February 2014
Accepted for publication 29 March 2014
Published 19 June 2014 Volume 2014:5 Pages 23—33
DOI https://doi.org/10.2147/RRTM.S34683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Video abstract presented by Harry Tagbor
Views: 20666
Harry Tagbor,1 Gifty Antwi,1 Joslin Dogbe2
1Department of Community Health, 2Department of Child Health, School of Medical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Introduction: Inadequately controlled malaria infection in pregnancy is associated with poor maternal and fetal outcomes. However, there are important questions about drug safety for mothers with malaria and their fetuses as, currently, there is limited safety data on many of the medications used. The objective of this review is to determine from published evidence the safety of antimalarial drugs exposure during early pregnancy, focusing on abortions, stillbirths, and congenital abnormalities.
Methods: We searched PubMed, Embase, Cochrane Library, and Malaria in Pregnancy databases from their inception to June 2013, inclusive, for reports published in English only. Data were extracted on exposure to antimalarial drugs during early pregnancy and adverse pregnancy outcomes including congenital abnormalities, stillbirth, and miscarriage.
Results: Twenty-two publications including one abstract with a total of 6,333 early pregnancy exposures to antimalarial agents used for treatment and/or prevention of malaria in pregnancy met the inclusion criteria. More than 40% of the pregnancies were exposed to mefloquine, about 10% to artemisinin based regimens and, 15.2% and 14.7% were exposed to chloroquine and quinine, respectively. A total of 1,199 adverse outcomes including abortions, stillbirths, and congenital abnormalities were reported. The reported absolute risks of adverse outcomes were similar for all the antimalarial exposures, but, in two publications, increased risk of stillbirths was linked to mefloquine exposure. Extensive heterogeneity and variability in the way in which authors assessed, recorded, and reported safety data precluded formal meta-analysis.
Conclusion: The absolute estimates of risks obtained in the included studies are difficult to interpret and the clinical significance of any association of adverse outcomes reported with antimalarial exposure in early pregnancy is uncertain. Well planned, executed, and analyzed studies are needed to confirm whether there is increased risk for adverse fetal outcomes attributable to exposure of first trimester pregnancies to antimalarials compared to relevant controls.
Keywords: malaria in pregnancy, first trimester, antimalarials, adverse outcomes, mefloquine, congenital abnormalities
Introduction
Since the thalidomide disaster, concerns have been expressed about the risk of adverse outcomes of maternal drug exposure on the developing fetus during the period of organogenesis.1,2 Drug use is, therefore, generally restricted during this period, and monitoring of the safety of commonly used medications is advocated.1 Medication use during early pregnancy may be because of pregnancy-induced conditions or other medical conditions, or may not be based on medical advice. Sometimes, the exposures occur before the women become aware of their pregnancy.1 Due to the potential harm to the fetus, drugs may be avoided during pregnancy, particularly in the first trimester, unless they become absolutely necessary to treat serious life threatening medical conditions such as malaria.1,2
Malaria infection during early pregnancy is associated with fetal growth restriction3–5 and attendant consequences,6 requiring early detection and prompt effective treatment for all pregnant women.6 However, there is a challenge. The challenge is in how to achieve a balance between the benefits of treating the mother with an effective treatment regimen and the risks to the fetus from medications with teratogenic potential.1,2 A limited number of antimalarials including chloroquine (CQ), quinine, proguanil, and clindamycin may be used in early pregnancy.7 At standard dosages for malaria treatment or prevention in pregnancy they are not embryotoxic or teratogenic.2 But the reduced efficacy of CQ and poor tolerability of quinine further limits the number of antimalarials that may be used in the first trimester.8 The World Health Organization (WHO) recommends that quinine singly or combined with clindamycin should be used to treat uncomplicated malaria in the first trimester or, when necessary, artesunate plus clindamycin coadministration is recommended.7 In this article, we review current knowledge of the adverse fetal outcomes of exposure of early pregnancies to antimalarial drugs.
Methods
Literature search and selection of studies
We searched the following electronic databases: PubMed; EMBASE; the Cochrane Library; and Malaria in Pregnancy Consortium library. We searched for articles reporting exposure of pregnant women in their first trimester to antimalarials for the purposes of controlling malaria in pregnancy, by combining keywords related to the target group and safety outcomes. The search strategy is detailed in Table 1. We searched free text terms and, when necessary, in singular and plural as well as in US and UK terminology including synonyms. We included only relevant English-language articles published in peer-reviewed journals with no restrictions on time, study design, or type or amount of data collected. The search excluded second and third trimester pregnancies, review articles, and reports on animal studies. The authors independently assessed the potential relevance of all titles and abstracts identified from the electronic searches. Full text copies of the articles identified as potentially relevant were retrieved and assessed for inclusion. An article reporting on the exposure of pregnant women in their first trimester to antimalarials for the purposes of controlling malaria in pregnancy with or without safety outcomes assessment was considered relevant. The bibliographies of all articles collected were checked for additional references. The process was repeated for all new references until no new information was found.
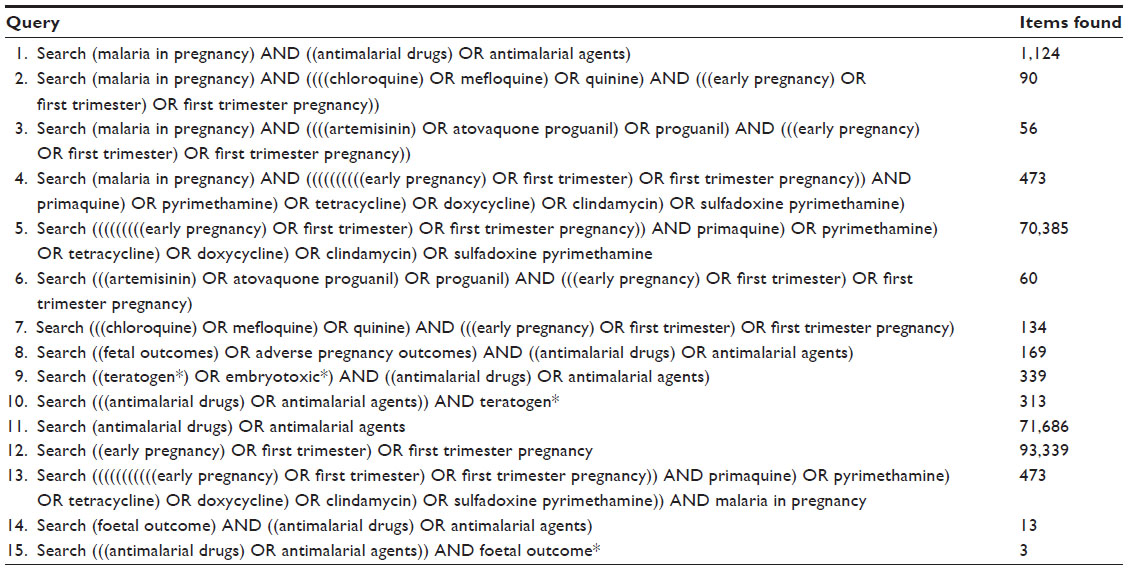 | Table 1 Search strategies and results in PubMed |
Data extraction
From each relevant paper we extracted data relating to the following: study setting; population and year; study design; number of pregnancies exposed; types of intervention; characteristics of study participants; drug regimens; occurrence and nature of adverse outcomes; and how these were assessed. For the outcome of interest we extracted data on fetal loss (abortions and stillbirths) and congenital abnormality. We attempted to use published checklists to assess methodological qualities of studies identified. This was difficult because, first, the studies did not meet the criteria for quality included in those checklists and, secondly, the included studies employed a wide range of study designs.
Results
Description of studies
A total of 602 unique records written in English were retrieved. We excluded 580 of them because: they were about nonpregnant subjects; the pregnancies were beyond first trimester; the reports were review papers; or they were about animal studies. Twenty-two records published between 1985 and 2012 found to contain information on exposure of first trimester pregnancies to antimalarial drugs for prevention and/or treatment purposes were included in this review. The included studies were from a wide range of geographical and epidemiological settings, but mainly from Africa and Asia. The rest are based on analyses of pharmaceutical databases of adverse reports from clinical trials, treatment records, or travel surveys. The study design and characteristics of the study population, type of intervention, and outcomes of each study included in this review are shown in Table 2.
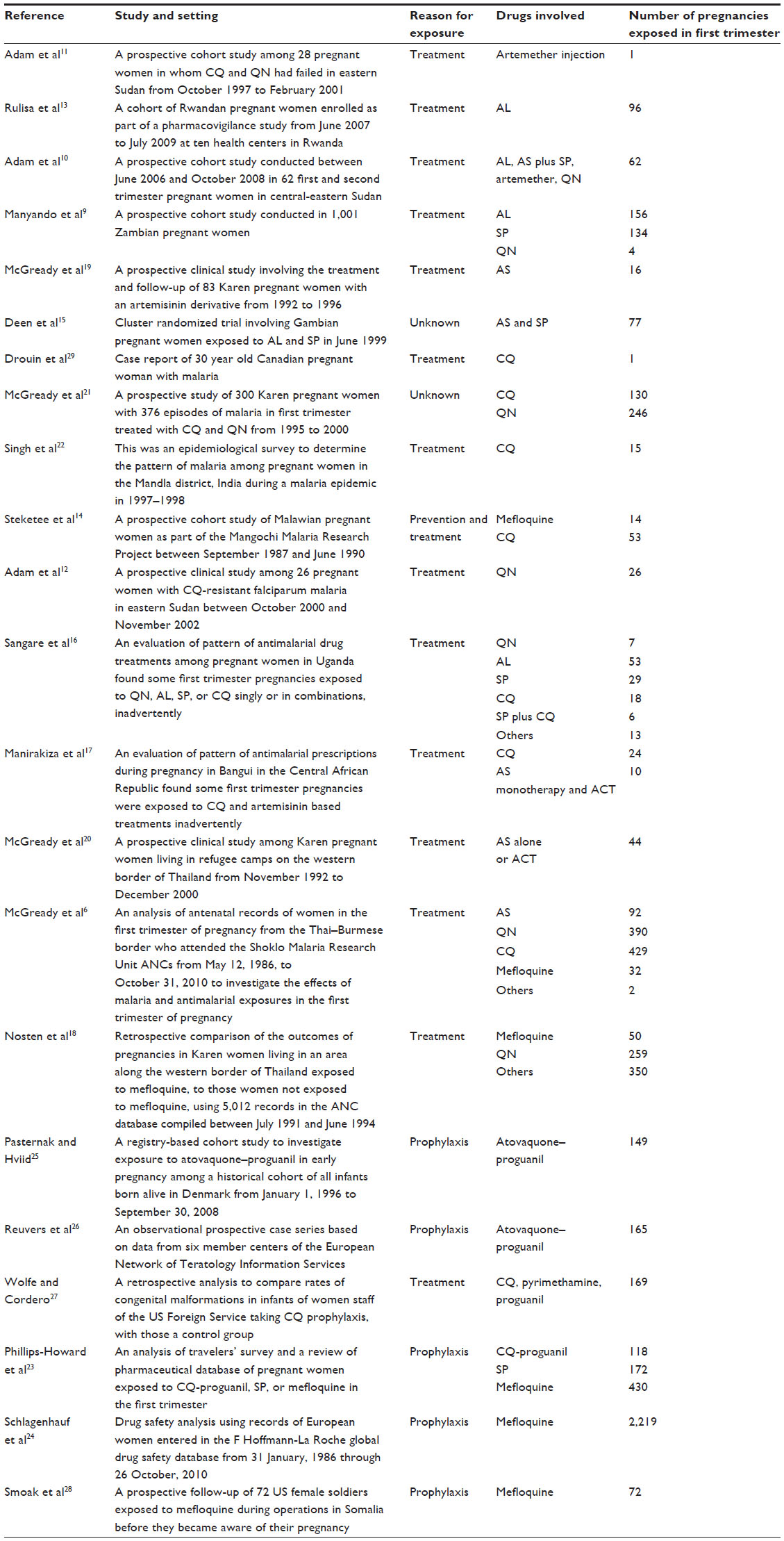 | Table 2 Characteristics of included studies |
Studies implemented in Africa
Nine studies were implemented in Africa in Zambia,9 Sudan,10–12 Rwanda,13 Malawi,14 The Gambia,15 Uganda,16 and Central African Republic.17 A cohort study conducted in Zambia between October 2004 and July 2008 enrolled pregnant women who had received artemether–lumefantrine (AL) or sulfadoxine–pyrimethamine (SP) for the treatment of malaria (clinically or parasitologically confirmed), and who were followed till delivery to investigate the occurrence of perinatal mortality (stillbirth or neonatal death within 7 days after birth). Exposure was ascertained from interviewing the women and cross-checking from outpatient files. Clinical assessment of mother and baby was done at birth and during the 1-year follow-up of 83.2% of babies. Seven abortions occurred in those exposed in the first trimester to AL, but a causal link could not be established as other factors (syphilis, multiple malaria episodes, and concomitant salbutamol ingestion) may have confounded the occurrence in four cases. No abortion occurred in those who received SP. Other events occurred in both groups, but in those who were exposed in later trimesters.9
Three studies implemented in Sudan reported exposure of early pregnancies to various antimalarials. One of them concerns a woman who was part of a hospital cohort of 28 pregnant women in whom initial treatment with CQ and quinine had failed. She was treated with artemether in the 10th week of gestation but went on to deliver a full term normal baby.11 Another was conducted among a hospital cohort of 26 pregnant women in whom initial treatment with CQ had failed, and who were treated with quinine and prospectively followed until delivery. The babies were followed until they were 1 year old. No adverse outcome was reported.12 A third study was conducted among 62 pregnant women in their first trimester who received treatment with artemether alone, artemether plus SP, or AL, and who were followed until they had an event (preterm delivery, miscarriage, or congenital malformation) or delivered at term. Term babies were followed until they were 1 year old. Two women who received artemether injection in the first trimester suffered a second bout of malaria in the second trimester and aborted while receiving quinine infusions. The remaining 60 pregnancies experienced no adverse outcomes and resulted in delivery of full term babies.10
In Rwanda, a cohort of 1,072 pregnant women (including 96 inadvertently exposed in the first trimester) was enrolled as part of a pharmacovigilance study. Exposure was ascertained from interviewing the women and cross-checking from prescription and treatment registers. Adverse outcomes including abortions, stillbirths, perinatal death, premature delivery, and congenital malformations occurred, but the report did not differentiate these according to the gestation at which exposure occurred. The authors, however, noted that, compared to a control group, there was no increased risk of adverse outcomes following AL exposure in early pregnancy.13
During a large prospective cohort study of Malawian pregnant women carried out between September 1987 and June 1990, 14 and 53 pregnancies were exposed to mefloquine (MQ) and CQ, respectively, during the first trimester. One stillbirth was reported in the CQ group.14 In The Gambia, Deen et al reported 173 early pregnancy exposures to artemisinin and derivatives but did not report whether adverse outcomes occurred in those exposed.15 In Uganda, 126 first-trimester pregnancies were exposed to quinine, AL, SP, or CQ singly or in combinations, but it was not clear how many pregnancies were exposed to each drug and no outcome was reported.16 Similarly, in Bangui in Central African Republic, during an evaluation of pattern of antimalarial prescription it was noted that 24 first-trimester pregnancies were exposed to CQ and another ten to artemisinin-based treatments, but no outcomes were reported.17
Studies implemented in Asia
Six studies were implemented in Asia including five on the Thai–Burmese border6,18–21 and one in India.22 Two studies reported from the Thai–Burmese border were based on retrospective analyses of antenatal records of women who attended antenatal clinics in that region.6,18 In the analysis by McGready et al, 945 pregnant women were exposed to various antimalarials in the first trimester. Of the 945 pregnancies exposed, 429 received CQ, 390 received quinine, 92 received artesunate, and 32 received MQ; the remaining 2 it was only mentioned in the text as “other”. A total of 223 adverse outcomes were recorded including 207 abortions, eleven stillbirths, and five congenital abnormalities. However, the analysis focused on artemisinin combination therapies mainly with respect to treatments and on miscarriages among the reported outcomes. The authors concluded that single episodes of symptomatic or asymptomatic Plasmodium falciparum or Plasmodium vivax malaria may cause more adverse outcomes than can be attributed to antimalarial treatment.6 In the analysis by Nosten et al, 659 first-trimester pregnancies were exposed to MQ (7.6%), quinine (39.3%), or other antimalarials (53.1%). The authors ascertained exposure by tracing and interviewing women using questionnaires and cross-checking their responses with their antenatal records and treatment records. The outcomes investigated in this analysis included stillbirth, abortion, and congenital malformation assessed at birth and neurological development of the infants assessed by the age of 1 year. However, only the incidence of stillbirths was selectively differentiated according to gestational age of exposure; those of abortions and congenital malformations were not. The authors concluded that MQ exposure during pregnancy was associated with an increased risk of stillbirth compared to exposure to quinine or no-malaria/no-antimalarial group. In this report, mention was also made of another cohort of 3,533 pregnant women exposed to MQ, quinine, and other antimalarials resulting in 55 stillbirths and 205 abortions. Timing of the exposure was not indicated, but, in this cohort also, MQ exposure during pregnancy was associated with an increased risk of stillbirth compared to exposure to quinine but not when compared with the no-malaria/antimalarial group.18
Also on the Thai–Burmese border, three prospective clinical studies were conducted. The first involved 83 pregnant women with P. falciparum infection treated with artemisinin antimalarials. Sixteen of the 83 were exposed during the first trimester. Three of the pregnancies among the 16 resulted in spontaneous abortion; the outcome of one is unknown but the remaining 12 resulted in full term babies who were externally and neurologically normal.19 The second involved 461 Karen pregnant women in whom 539 malaria episodes were recorded and treated with an artemisinin antimalarial. In 44 women, treatment was given in the first trimester either for primary infection (19) or for retreatment after treatment with quinine and MQ had failed (25). Ten of the 44 pregnancies resulted in abortions, three of which were inevitable at the beginning of treatment.20 In the third study, 376 pregnant women with malaria infection were treated with quinine (246) and CQ (130) in the first trimester. Among the two treatment groups, a total of 70 adverse outcomes were reported including three congenital anomalies, three stillbirths, and 62 abortions. These were similar to the background community rates and so the authors concluded that quinine and CQ were safe to use in the first trimester of pregnancy.21
In India, 15 first-trimester pregnancies were exposed to CQ with some resulting in unspecified numbers of spontaneous abortions and stillbirth. These were not explained further.22
Studies based on analyses of travel records or other databases
Some studies were based on the analyses of records from various sources including travel survey, birth defects registry, pharmaceutical databases, and treatment records. As part of their study, Phillips-Howard et al reviewed data on a prospective travel cohort of 118, 19, and 99 pregnant women exposed to CQ-proguanil, SP, and MQ, respectively, in the first trimester. They also reviewed the F Hoffmann-La Roche database that was holding records of women who became pregnant while taking MQ (446 between 1986 and 1993) and SP (165 between 1978 and 1993). This database was compiled from voluntary reports to the company of exposed women who subsequently were followed up prospectively around the time of delivery to assess pregnancy outcome. They suggested that use of MQ and other antimalarial drugs may be safe.23
Schlagenhauf et al reviewed records held in a pharmaceutical database to investigate the effect of exposure to MQ before or during pregnancy on pregnancy and offspring outcomes. Among 2,139 pregnancies exposed in the first trimester, pregnancy and fetal outcomes were prospectively assessed, while in 227 cases the outcomes were known at the time of reporting. A total of 484 abortions (spontaneous and induced), 74 congenital abnormalities, and three stillbirths were recorded.24
The analysis of the Danish Medical Birth Register to investigate the effect of atovaquone–proguanil exposure in early pregnancy reported two birth defects in babies whose mothers were exposed in early pregnancy to atovaquone–proguanil. The authors compared this incidence to population rates and concluded that atovaquone–proguanil may be safely used in pregnancy.25 The risk of major congenital malformations after exposure to atovaquone–proguanil during early pregnancy was also assessed in a prospective case series based on data from six member centers of the European Network of Teratology Information Services.26
Wolfe and Cordero, in a retrospective analysis, found that two of a cohort of 169 births to women staff of the US Foreign Service and their dependents who were exposed throughout pregnancy to CQ 300 mg base once a week for chemosuppression of malaria had congenital malformations. By comparing this rate with those of a control group of 454 births, the authors suggested that CQ use in pregnancy was safe.27 A similar analysis was carried out among 72 US female soldiers exposed to MQ during operations in Somalia before they became aware of their pregnancy. These data were characterized by high rates of elective and spontaneous abortions but, based on favorable records of 13 infants followed up to 1 year, the authors suggested that MQ does not cause gross congenital malformations.28
Summary of adverse fetal outcomes reported
Most of the studies reported multiple adverse fetal outcomes on the index pregnancies, which were also often exposed to more than one antimalarial. The majority of the studies did not indicate if the reported adverse outcomes were associated with the antimalarial drug exposure during the first trimester. Abortions, stillbirths, and congenital abnormalities were the most frequently reported adverse fetal outcomes. Abortion was defined as a pregnancy outcome of fetal death before 20 completed weeks of gestation or as expulsion of the fetus before 28 weeks of gestation. The abortions were either spontaneous or therapeutically induced but in one instance23 it was classified as missed if the fetus died before the 18th week of gestation but was retained in utero. Stillbirth was defined as the delivery after 28 weeks of gestation of a fetus that did not breathe or fetal death after 20 completed weeks of gestation. The number of exposures by antimalarial agent and reported adverse fetal outcomes by study is shown in Table 3, and the overall numbers of first trimester exposures and reported adverse outcomes by antimalarial drug is shown in Table 4.
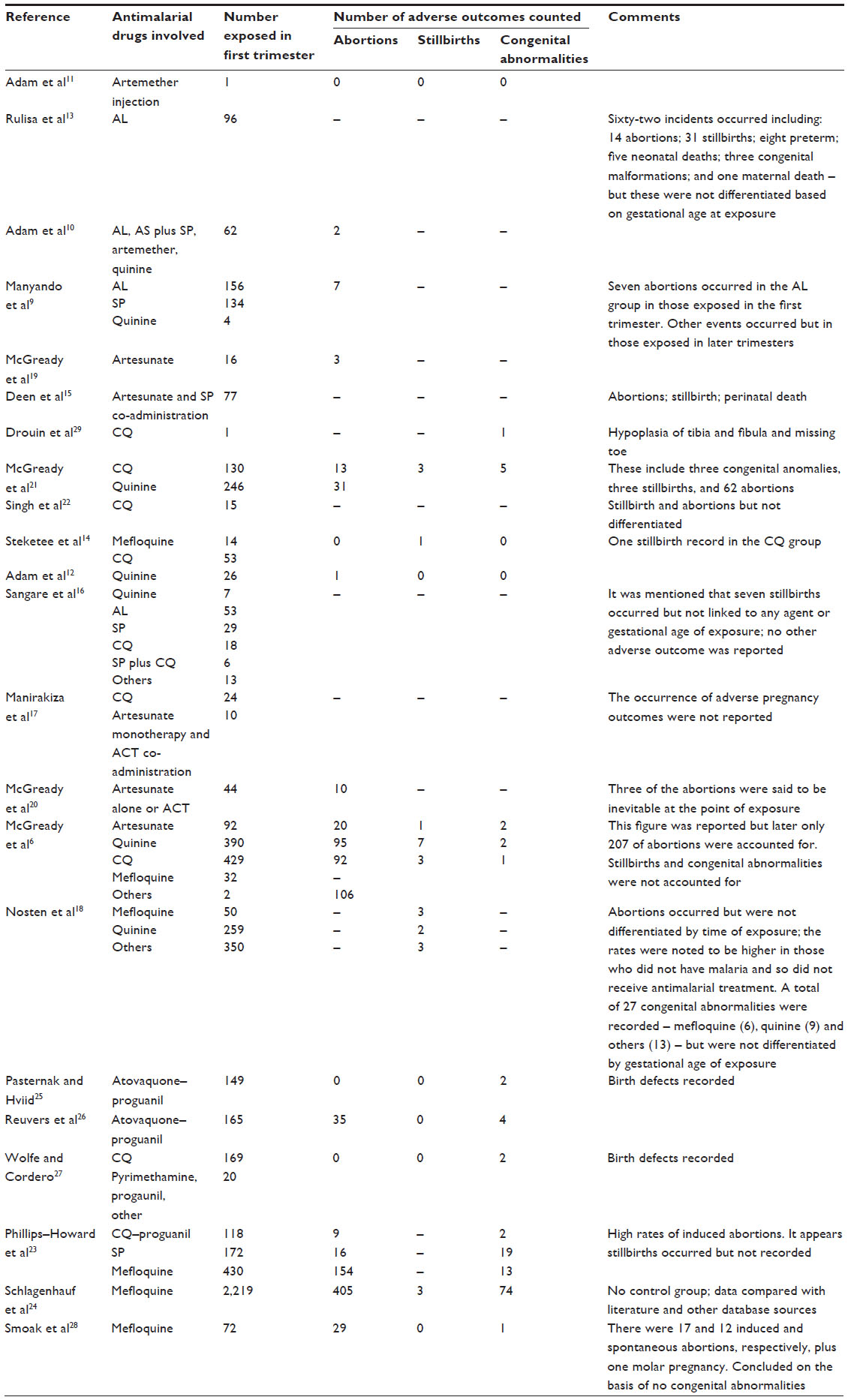 | Table 3 Number of exposures by antimalarial agent and reported adverse fetal outcomes |
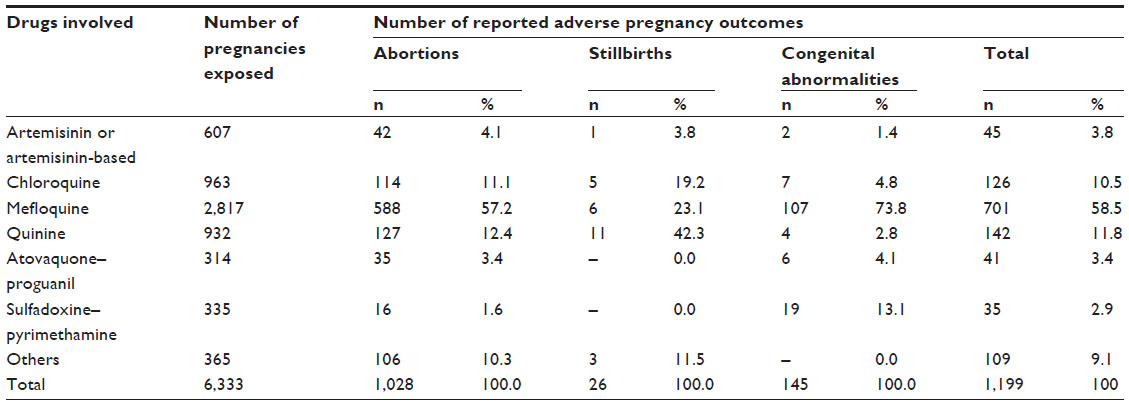 | Table 4 Overall numbers of first trimester exposures and reported adverse outcomes by drug |
Abortions/miscarriages
We counted a total of 1,028 abortions (induced and spontaneous) constituting 85.7% of all fetal adverse outcomes (Table 4) as reported in 12 publications (Table 3). However, very few of the publications provided an estimate of the effect of malaria and/or drug exposure on the incidence of abortion. The majority (87.3%) of the abortion cases were reported by three publications.6,23,24 The analysis by McGready et al found that the risk of spontaneous abortion was similar for woman treated with CQ (26%), quinine (27%), and artesunate (31%). The key finding is that even an episode of asymptomatic and symptomatic malaria can increase the risk for miscarriage by 2.7 times and four times, respectively, compared to women without malaria during pregnancy.6 The analysis of the effect of exposure to MQ before or during pregnancy on pregnancy and offspring outcome by Schlagenhauf et al recorded high number of cases of abortion (150 spontaneous abortions and 334 therapeutic abortions).24 Phillips-Howard et al showed from their analysis that MQ exposure resulted in a significant risk of therapeutically induced abortions compared with SP (26% compared with 7%, relative risk 1.32, 95% confidence interval 1.22–1.44).23
Stillbirths
Data on occurrence of 26 stillbirths were available from five publications.6,14,18,21,24 Three of the publications accounted for the majority of 22 stillbirths that occurred among women living in a camp for displaced persons in a remote rural area near the Thai–Burmese border and who were exposed to named antimalarials in early pregnancy.6,18,21 Nosten et al18 showed that pregnant women exposed to MQ are more than three times likely to be associated with an increased risk of stillbirth compared to women not exposed to MQ. They also showed that MQ exposure during pregnancy was associated with an increased risk of stillbirth (by at least seven times) relative to quinine and CQ exposures. No estimates of association between stillbirth risk and antimalarial exposure were given in the remaining publications.
Congenital abnormalities
Data on occurrence of 145 congenital abnormalities were available from eight publications (Table 3).6,21,23–28 Two publications accounted for 127 of this number. This includes 74 based on the analyses of a pharmaceutical database of women exposed to MQ24 and 53 based on the analysis of a travel cohort and pharmaceutical database of women exposed to MQ, SP, or CQ-proguanil.23 In all eight publications, no excess or specific patterns of congenital abnormalities were associated with the named antimalarials apart from one case report of a full term infant with hyperplasia of tibia and fibula and missing toe attributed to exposure to CQ in the first trimester of pregnancy.29
Discussion
We identified a total of 6,333 early pregnancies exposed to various antimalarials reported in 22 publications that reported or mentioned an adverse outcome. All of the studies included are those reporting antimalarial drug exposures in pregnancy for curative and/or preventive purposes in the control of malaria in pregnancy. Varied antimalarial regimens were used including CQ, CQ-proguanil, MQ, SP, artemisinin based treatments, atovaquone-proguanil, and others unspecified in the reports. More than 40% of the pregnancies were exposed to MQ, followed by CQ and quinine of similar frequencies; 15.2% and 14.7%, respectively. The majority of the MQ exposures were reported by Schlagenhauf et al24 who reviewed data held in a pharmaceutical database. Data on exposure to artemisinin combinations was relatively scarce, with only 9.6% of the early pregnancies identified in this review exposed to artemisinin or an artemisinin combination therapy.
A total of 1,199 fetal adverse outcomes including abortions (85.7%), stillbirths (2.2%), and congenital abnormalities (12.1%) were identified from the 6,333 early pregnancies exposed to a named antimalarial drug. Some of the studies reported antimalarial exposures in early pregnancy but did not indicate the occurrence of adverse fetal outcome. In some cases, adverse outcomes occurred, but the authors did not differentiate them according to the gestation at which exposure occurred or by agents involved. This, coupled with the fact that in most cases outcomes were unknown for some exposures, suggests that the actual number of adverse outcomes may be more than the number we counted. Most studies reported multiple adverse fetal outcomes on the index pregnancies, which were also often exposed to more than one antimalarial. So it is difficult to relate the outcomes to the number of pregnancies exposed to each drug.
The evidence obtained from the included studies is difficult to interpret, and the clinical significance of any association of adverse outcomes reported with antimalarial exposure in early pregnancy is uncertain; we cannot conclusively say that these drugs do not increase the risk of adverse outcomes. This notwithstanding, the possibility of adverse pregnancy outcomes is a major concern for all health policy makers as there is very little published evidence on the effects of antimalarial drugs exposure during the first trimester of pregnancy. MQ exposure seems to be associated with an increased risk of abortions and congenital anomalies compared to exposure to other antimalarials (Table 4). But, the rate of abortion might have been inflated by the high number of therapeutic abortions that occurred at a time when there was insufficient data on MQ safety, and so more women opted to abort after discovering fetal exposure to MQ. The picture may have been different if these pregnancies progressed to normal deliveries. Also, due to the safety concerns, MQ exposures were generally closely monitored and reported on more than would have occurred in a routine data collecting system. This may explain the high number of congenital anomalies associated with MQ.
Our review had limitations. First, we restricted our literature search to the English language, and it is possible that we may have missed other studies that were published in other languages. Second, we included only studies on antimalarial exposures for treatment and/or prevention for the control of malaria in pregnancy and not exposures involving antimalarial treatment of connective tissue diseases. Third, we did not restrict the type of study to include in the review to specific designs or methodological quality. So there is a substantial heterogeneity and variability in the way in which authors assessed, recorded, and reported safety data in the publications reviewed. This, coupled with the wide range of geographical and epidemiological settings of the studies and methods of ascertainment of exposure, make a meta-analysis inappropriate.
But the major limitation relates to the suboptimal quality of most of the reports reviewed. All of them scored very low when we attempted to use some of the known quality assessment checklist to assess their quality, because most of the items in the checklists did not apply to them.
The majority of the included studies were uncontrolled. Whenever comparisons were made, they were against population parameters or against unrelated controls. Since most of the reported outcomes were not extremely rare among unexposed pregnant women, absolute estimates of risk reported are difficult to interpret, and relative risks cannot be estimated. Only two studies6,18 attempted to adjust for confounders, although the risk of adverse outcomes reported may be due to the influence of other risk factors besides antimalarials. This also makes it difficult to assess the actual risk posed by early pregnancy antimalarials exposures.
Most of the studies reported multiple safety outcomes and often pregnancies were exposed to more than one antimalarial; but, as no standard criteria were followed in reporting safety data in all the studies, there appeared to be selective reporting of adverse outcomes. What got emphasized in these situations seemed to be at the discretion of the authors. In all these situations, the interaction between the different types of drugs and even the different time periods of the same drug taken multiple times, is not discussed.
Conclusion
The evidence on the safety of antimalarial exposures during early pregnancy appears limited and inconclusive, but antimalarial treatment may not be withheld in pregnancy since uncontrolled malaria in pregnancy may be harmful to the mother and the fetus. The risks associated with uncontrolled malaria in pregnancy thus have to be balanced against the potential risk of adverse outcomes from antimalarial drug exposure, particularly in the first trimester. The challenge is to identify antimalarials with minimum risks to the mother and the fetus for treatment and/or prevention for the control of malaria in pregnancy. No single approach seems optimum to identify possible teratogenicity of antimalarials and to assess the relation between exposures in early pregnancy and adverse fetal outcomes. So we recommend adherence to WHO recommendations to make appropriate antimalarial treatment available to pregnant women when necessary. We also recommend establishment of functional clinical monitoring systems that will ensure that data collected is complete and accurate to facilitate evaluation of the overall safety consequences of prenatal exposures.
Author contributions
HT, GA, and JD conceived and agreed on method adopted for the review. HT and GA independently assessed eligibility articles and extracted data. HT, GA, and JD wrote and approved the review.
Disclosure
The authors report no conflicts of interest in this work.
References
Koren G, Pastuszak A, Ito S. Drugs in pregnancy. N Engl J Med. 1998; 338(16):1128–1137. | |
Briggs GG, Freeman RK, Yaffe SJ. Drugs In Pregnancy And Lactation: A Reference Guide to Fetal and Neonatal Risk. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. | |
Rijken MJ, de Wit MC, Mulder EJ, et al. Effect of malaria in pregnancy on foetal cortical brain development: a longitudinal observational study. Malar J. 2012;11:222. | |
Rijken MJ, Papageorghiou AT, Thiptharakun S, et al. Ultrasound evidence of early fetal growth restriction after maternal malaria infection. PloS One. 2012;7(2):e31411. | |
Umbers AJ, Aitken EH, Rogerson SJ. Malaria in pregnancy: small babies, big problem. Trends Parasitol. 2011;27(4):168–175. | |
McGready R, Lee SJ, Wiladphaingern J, et al. Adverse effects of falciparum and vivax malaria and the safety of antimalarial treatment in early pregnancy: a population-based study. Lancet Infect Dis. 2012;12(5):388–396. | |
WHO. Guidelines for the Treatment of Malaria. 2nd ed. Geneva: WHO Press: 2010. | |
Bell D, Winstanley P. Current issues in the treatment of uncomplicated malaria in Africa. Br Med Bull. 2004;71:29–43. | |
Manyando C, Mkandawire R, Puma L, et al. Safety of artemether-lumefantrine in pregnant women with malaria: results of a prospective cohort study in Zambia. Malar J. 2010;9:249. | |
Adam I, Elhassan EM, Omer EM, et al. Safety of artemisinins during early pregnancy, assessed in 62 Sudanese women. Ann Trop Med Parasitol. 2009;103(3):205–210. | |
Adam I, Elwasila E, Mohammed Ali DA, Elansari E, Elbashir MI. Artemether in the treatment of falciparum malaria during pregnancy in eastern Sudan. Trans R Soc Trop Med Hyg. 2004;98(9):509–513. | |
Adam I, Idris HM, Elbashir MI. Quinine for chloroquine-resistant falciparum malaria in pregnant Sudanese women in the first trimester. East Mediterr Health J. 2004;10(4–5):560–565. | |
Rulisa S, Kaligirwa N, Agaba S, et al. Pharmacovigilance of artemether-lumefantrine in pregnant women followed until delivery in Rwanda. Malar J. 2012;11:225. | |
Steketee RW, Wirima JJ, Slutsker L, et al. Malaria treatment and prevention in pregnancy: indications for use and adverse events associated with use of chloroquine or mefloquine. Am J Trop Med Hyg. 1996;55(Suppl 1):50–56. | |
Deen JL, von Seidlein L, Pinder M, Walraven GE, Greenwood BM. The safety of the combination artesunate and pyrimethamine-sulfadoxine given during pregnancy. Trans R Soc Trop Med Hyg. 2001;95(4):424–428. | |
Sangare LR, Weiss NS, Brentlinger PE, et al. Patterns of anti-malarial drug treatment among pregnant women in Uganda. Malar J. 2011;10:152. | |
Manirakiza A, Soula G, Laganier R, et al. Pattern of the antimalarials prescription during pregnancy in Bangui, Central African Republic. Malar Res Treat. 2011;2011:414510. | |
Nosten F, Vincenti M, Simpson J, et al. The effects of mefloquine treatment in pregnancy. Clin Infect Dis. 1999;28(4):808–815. | |
McGready R, Cho T, Cho JJ, et al. Artemisinin derivatives in the treatment of falciparum malaria in pregnancy. Trans R Soc Trop Med Hyg. 1998;92(4):430–433. | |
McGready R, Cho T, Keo NK, et al. Artemisinin antimalarials in pregnancy: a prospective treatment study of 539 episodes of multidrug-resistant Plasmodium falciparum. Clin Infect Dis. 2001;33(12):2009–2016. | |
McGready R, Thwai KL, Cho T, et al. The effects of quinine and chloroquine antimalarial treatments in the first trimester of pregnancy. Trans R Soc Trop Med Hyg. 2002;96(2):180–184. | |
Singh N, Mehra RK, Srivastava N. Malaria during pregnancy and infancy, in an area of intense malaria transmission in central India. Ann Trop Med Parasitol. 2001;95(1):19–29. | |
Phillips-Howard PA, Steffen R, Kerr L, et al. Safety of mefloquine and other antimalarial agents in the first trimester of pregnancy. J Travel Med. 1998;5(3):121–126. | |
Schlagenhauf P, Blumentals WA, Suter P, et al. Pregnancy and fetal outcomes after exposure to mefloquine in the pre- and periconception period and during pregnancy. Clin Infect Dis. 2012;54(11):e124–e131. | |
Pasternak B, Hviid A. Atovaquone-proguanil use in early pregnancy and the risk of birth defects. Arch Intern Med. 2011;171(3):259–260. | |
Reuvers N, Vial T, Schaefer C, et al. Pregnancy outcome after first trimester exposure to malarone (atovaquone-proguanil):A prospective case-series. Birth Defects Res A Clin Mol Teratol. 2012;94(5):329. | |
Wolfe MS, Cordero JF. Safety of chloroquine in chemosuppression of malaria during pregnancy. Br Med J (Clin Res Ed). 1985;290(6480):1466–1467. | |
Smoak BL, Writer JV, Keep LW, Cowan J, Chantelois JL. The effects of inadvertent exposure of mefloquine chemoprophylaxis on pregnancy outcomes and infants of US Army servicewomen. J Infect Dis. 1997;176(3):831–833. | |
Drouin J, Rock G, Jolly EE. Plasmodium falciparum malaria mimicking autoimmune hemolytic anemia during pregnancy. Can Med Assoc J. 1985;132(3):265–267. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.