")
Back to Journals » Clinical Ophthalmology » Volume 18
Safety of an Intracameral Fixed Combination for Mydriasis and Intraocular Anaesthesia During Cataract Surgery
Authors Nuijts RM, Cochener-Lamard B, Szaflik JP, Mencucci R, Chiambaretta F, Behndig A
Received 4 December 2023
Accepted for publication 8 April 2024
Published 25 April 2024 Volume 2024:18 Pages 1103—1115
DOI https://doi.org/10.2147/OPTH.S453257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rudy MMA Nuijts,1 Béatrice Cochener-Lamard,2 Jacek P Szaflik,3 Rita Mencucci,4 Frédéric Chiambaretta,5 Anders Behndig6
1University Eye Clinic, Maastricht University Medical Center, Maastricht, the Netherlands; 2Ophthalmology Department, CHU Morvan, University Hospital of Brest, and University of Bretagne Occidentale (UBO), Brest, France; 3Department of Ophthalmology, Medical University of Warsaw, Warszawa, Poland; 4Eye Clinic, Department of Neurosciences, Psychology, Pharmacology, and Child Health, University of Florence, Florence, Italy; 5Ophthalmology Department, CHU Gabriel Montpied, University Hospital of Clermont-Ferrand, Clermont-Ferrand, France; 6Department of Clinical Sciences/Ophthalmology, Umea University, Umea, Sweden
Correspondence: Anders Behndig, Department of Clinical Sciences/Ophthalmology, Umea University, SE-901 85 Umea, Sweden, Tel + 46 70 782 75 36, Fax + 46 90 13 34 99, Email [email protected]
Purpose: To compare the safety of a standardized, commercially available intracameral combination of mydriatics and anesthetic (ICMA) with a reference topical mydriatic regimen for cataract surgery.
Patients and Methods: The safety results from two international, randomized, controlled clinical studies were combined to compare ICMA at the beginning of cataract surgery (ICMA group) to the reference topical mydriatic regimen (reference group). Data were collected on ocular and systemic adverse events, corneal and anterior chamber examination, endothelial cell density, retinal thickness and visual acuity. Analysis was performed on a pooled safety set from both studies, preoperatively and up to 1 month postoperatively.
Results: 342 patients received ICMA and 318 the reference topical regimen. Ocular adverse events were reported in 17.0% of patients in the ICMA group and 18.6% in the reference group. No difference was shown between groups in endothelial cell density (2208 ± 498 cells/mm2 for ICMA group versus 2241 ± 513 cells/mm2 for the reference group; p=0.547) and retinal thickness (change from baseline less than 50 μm in 94.7% versus 95.0% of patients, respectively) at 1 month postoperatively. At 1-day post-surgery, less patients in the ICMA group had moderate or severe (Grades 2 and 3) superficial punctate corneal staining (3.9% versus 7.0% for the reference group; p=0.064). Postoperatively, some ocular symptoms were also less frequently reported in the ICMA group. Best-corrected visual acuity increased in 96.0% of patients in the ICMA group and 95.8% in the reference group at 1 month.
Conclusion: ICMA injection at the beginning of cataract surgery was demonstrated to be safe and may also provide perioperative and postoperative advantages over the standard topical mydriatic regimen.
Keywords: cataract surgery, intracameral mydriasis, topical mydriasis, safety, tolerability
Introduction
Cataract surgery is the most common ophthalmic surgery in economically developed countries.1 Although it is a cost-effective intervention,2 an aging population means larger surgical volumes and increased pressure on resources. Therefore efficiency,2–4 but also safety of the procedure remains fundamental to successful outcomes. The most common intraoperative complications associated with cataract surgery are posterior capsule rupture (PCR) and iris trauma.5–9 Postoperative complications include corneal and macular edema, endophthalmitis and uveitis.5–9
PCR can also affect post-surgical outcomes and is a risk factor for other complications, including cystoid macular edema and pseudophakic retinal detachment.10,11 In the majority of cases, pseudophakic macular edema has no clinical impact and does not affect visual outcome.5,6,8 However, clinically significant macular edema has been reported after routine cataract surgery at an incidence rate of between 1.2% and 3.3%.5,6,8,12,13
Other frequent complications of cataract surgery include superficial punctate keratitis (SPK) and endothelial cell loss.14–16 Factors related to postoperative endothelial cell loss include hardness of the nucleus, anterior chamber depth, excessive duration of phacoemulsification and endothelial pathologies such as Fuchs dystrophy.15,16 Endothelial cell loss may also occur due to toxicity of irrigation fluids or agents injected into the anterior chamber during surgery or to penetration of the eye drops given preoperatively.
The routine use of topical mydriatics during cataract surgery can pose a risk of cardiovascular events in the elderly patient population.16 Hence, systemic exposure to drugs that carry a risk of cardiovascular events should be limited.17 The possible local and systemic adverse events (AEs) of topically applied mydriatic agents have been well described,16–19 and the need for an appropriate and effective alternative to eye drops such as intracameral mydriatics has been recognized for the past two decades.20 The intracameral mydriatic route was developed to address some of the disadvantages associated with topically administered mydriatics, mainly (1) their slow penetration through the cornea, resulting in a slow onset of the mydriasis, which is often several times longer than the surgical procedure itself, and (2) the risk of cardiovascular side‐effects associated with their systemic passage via the lacrimal drainage system.17–20
Some surgeons have continued to administer “custom-blended” or “off-label” intracameral mydriatic preparations despite the potential risks of compounding errors, contamination, or the use of excipients inappropriate for ophthalmic use.21–25 In 2015, a standardized, commercially available preservative-free, intracameral fixed combination of two mydriatics (tropicamide 0.02% and phenylephrine 0.31%) and one anesthetic (lidocaine 1%) (Mydrane® hereafter referred to as Intracameral Combination of Mydriatics and Anesthetic (ICMA); Laboratoires Théa, Clermont Ferrand, France) was approved in the EU for use in cataract surgery. The current pooled safety analysis evaluates the local and systemic safety and tolerability of ICMA based on data combined from the two EU approval studies.26,27
Materials and Methods
General Design of the Studies
The safety and tolerability data analyzed in this paper were combined from two multicenter, international, randomized, clinical trials: a pilot, dose-finding Phase II study (EudraCT No. 2008–003279-28), and a pivotal Phase III study (EudraCT 2010–021188-34).26,27 Data from the phase II study included 3 groups of patients, who received either: 0.15 mL ICMA, 0.2 mL ICMA or a standard topical mydriatic treatment. The phase III study included two groups of patients who received either ICMA 0.2 mL (ICMA group) or a standard topical mydriatic treatment (reference group).
Both studies adhered to the ethical principles of the Declaration of Helsinki (2004) regarding biomedical research on human patients. Both studies were conducted in compliance with applicable regulatory requirements and in accordance with Good Clinical Practice using the guidance documents and practices of the International Conference on Harmonization and the European directive 2001/20/CE.
Independent ethics committee approval was obtained for each participating center prior to beginning local patient recruitment see (Supplementary File). All patients underwent a thorough discussion of the risks and benefits of the study with the local investigator, and written informed consent was required for enrollment.
Patients
The study population was comprised of adult cataract patients,18–85 years of age in the phase II study and 40–88 years of age in the phase III study, scheduled to undergo unilateral phacoemulsification cataract surgery under topical anesthesia with clear corneal self-sealing incisions. Patients were enrolled from 11 centers in four countries (Belgium, France, Portugal, Spain) in the phase II study, and from 68 centers in nine countries (Algeria, Austria, Belgium, France, Germany, Italy, Portugal, Spain, Sweden) in the phase III study.
Investigational Treatments
ICMA (Mydrane®; Laboratoires Théa, Clermont-Ferrand, France) is a proprietary formulation of two mydriatic agents (tropicamide 0.02% and phenylephrine 0.31%) and one anesthetic agent (lidocaine 1%) for intracameral administration as a single injection of 0.2 mL at the start of cataract surgery (just after the first corneal incision).28 In both studies, in cases of inadequate mydriasis (within 30 sec of ICMA injection in the phase II study and within 1.5 min in the phase III study) as judged by the surgeon, a supplementary 0.1 mL injection of ICMA was allowed. In practice, the second injection offered no extra efficacy,27 and accordingly ICMA has been registered for use as a single intracameral injection only.28
The standard topical mydriatic regimen was tropicamide 0.5% (Mydriaticum® 0.5%; Laboratoires Théa) and phenylephrine 10% (Neosynephrine® 10% Faure; Laboratoires Europhta, Monaco). In all cases of both studies, 1 or 2 drops of 1% tetracaine were instilled 5 minutes before surgery for topical anesthesia. In the phase II study, patients in the reference group received an additional drop of tetracaine one minute prior to surgery. In the phase III study, both groups also received tetracaine eye drops 1 minute before the first incision. All these products (including ICMA) used in both studies did not contain preservatives. Also, in both studies, the reference group did not receive any intracameral anesthesia during the surgical procedure.
Safety Parameters
Table 1 presents the schedule of safety/tolerance examinations. The surgery took place on day 0 and follow-up visits were performed at day 1, day 8, and day 28 (one month) postoperatively.
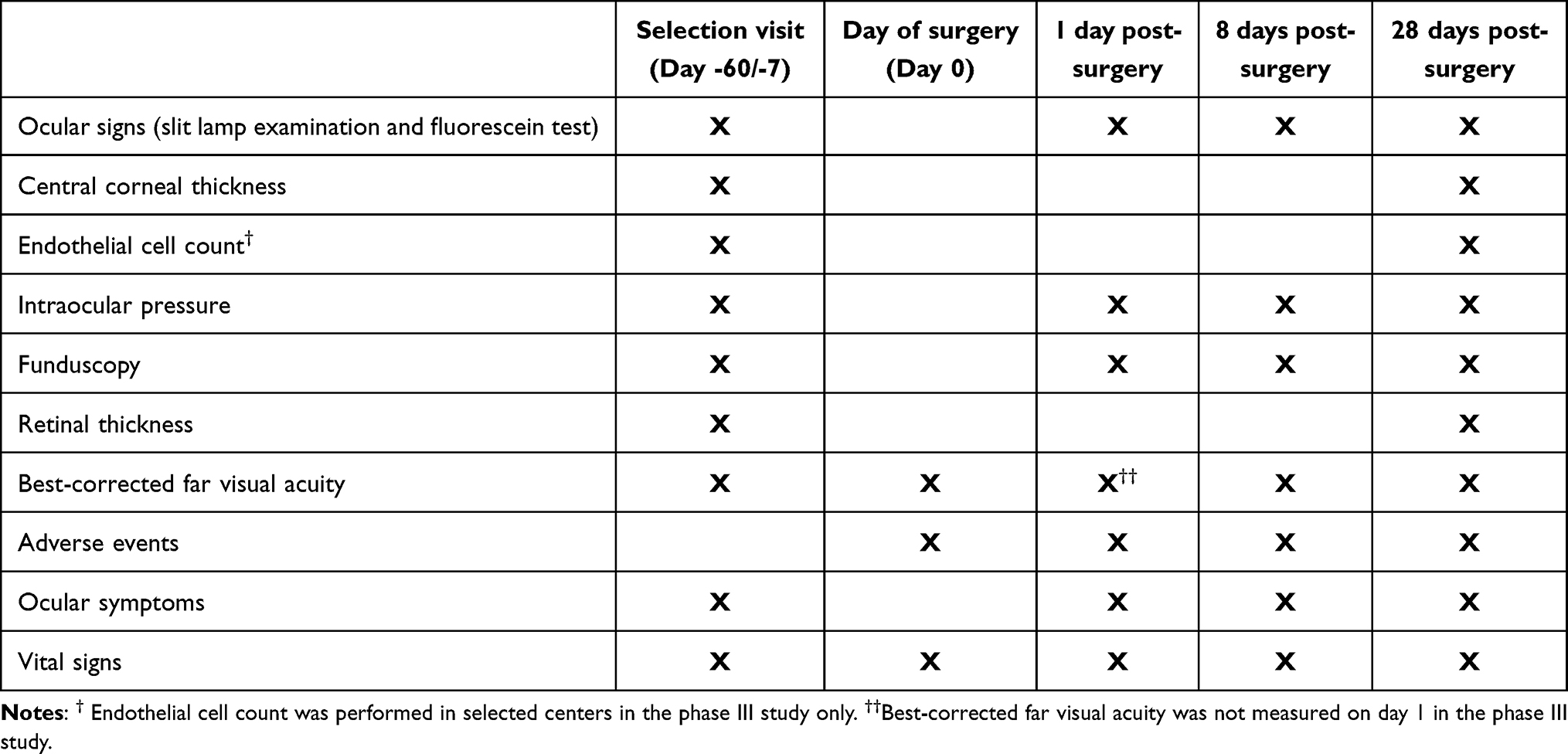 |
Table 1 Schedule of Safety/Tolerance Examination and Tests |
Ocular Safety
Patients underwent an ophthalmic evaluation including slit lamp examination, central corneal pachymetry, corneal endothelial cell count (cells/mm2 in the central cornea; performed in 50 out of 70 centers where specular microscopy was available), intraocular pressure (IOP) assessment (by air-puff or applanation tonometry), funduscopy, measurement of retinal thickness (RT) with optical coherence tomography (OCT) and best-corrected visual acuity (BCVA).
Slit lamp examination was used to evaluate the cornea and anterior segments for signs such as palpebral edema, chemosis, conjunctival hyperemia, conjunctival discharge, folliculo-papillary conjunctivitis, superficial punctate corneal staining and anterior chamber cells and flare.
Superficial punctate corneal staining was graded as follows: 0 = absent; 1 = some punctate staining <10% of the corneal area; 2 = diffuse punctate staining ≤50% of the corneal area; 3 = diffuse punctate staining >50% of the corneal area. For scores 1, 2 and 3, the investigator determined whether the staining could be considered to be clinically significant SPK. Anterior chamber cells were graded as follows: 0 = no cells; 1 = 1–5 cells; 2 = 6–15 cells; 3 = 16–30 cells; 4 = >30 cells. Anterior chamber flare was graded as follows: 0 = absent; 1 = trace (barely detectable); 2 = mild intensity (iris and lens details clear); 3 = moderate intensity (iris and lens details not clear); 4 = strong intensity (iris and lens details not visible and fibrin in the anterior chamber). Other clinical signs (palpebral edema, chemosis, conjunctival hyperemia, conjunctival discharge, folliculo-papillary conjunctivitis, other) were graded using the following 4-point scale: 0 = none; 1 = mild; 2 = moderate; 3 = severe.
Ocular treatment emergent adverse events (TEAEs) and their severity were noted by the investigator or reported by the patient at day 0 and at each postoperative visit. The potential relationship of AEs to the study treatment was also noted. Treatment-related AEs were defined as those with a causal relationship with the investigational drug that could not be formally excluded, including AEs assessed as “unlikely related” to “definitely related”.
Systemic Safety
Evaluation of systemic safety included collection of systemic TEAEs (reported in the same way as ocular TEAEs) and assessment of vital signs. Systolic blood pressure (SBP, in mmHg), diastolic blood pressure (DBP, mmHg) and heart rate (radial pulses in beats/minute, bpm) were measured at each visit. Two measurements were performed (with a resting time of 5 minutes between the two measurements), except during and at the end of the surgical procedure for practical reasons.
Subjective Ocular Symptoms and Patient Satisfaction
Ocular symptoms (pain, irritation/burning/stinging, photophobia, foreign body sensation or other ocular symptom) assessed by the patient in the operated eye before surgery and postoperatively were recorded according to the schedule in Table 1. Ocular symptoms were graded by the patient as follows: 0 = absent; 1 = mild; 2 = moderate; 3 = severe. Patient satisfaction with the surgery was evaluated on day 1 postoperatively as very satisfied, satisfied, not very satisfied or unsatisfied.
Assessment of Global Tolerance of Study Products by the Investigator
Assessment of tolerance of the study treatment by the investigator was conducted at all postoperative visits using the following scale: 0 = very satisfactory; 1 = satisfactory; 2 = not very satisfactory; 3 = unsatisfactory.
Statistical Methods
A pooled safety data set was created including all patients enrolled in both studies, for whom the study medication had been used and for whom follow-up data were available. Descriptive statistics are presented here.
Besides the summary statistics, comparisons of the two treatment groups were performed using the following statistical tests: the exact Cochran-Mantel-Haenszel (CMH) test stratified by study for the binary variables and for the ordinal variables (modified ridit scores were applied); an ANOVA model adjusting for treatment, study, and treatment by study interaction (and if relevant, the baseline value) for the quantitative variables. The results of these tests were interpreted two-sided, at 5% level of significance.
Results
Extent of Exposure
There were 342 patients in the ICMA group (including 252 who received a single ICMA injection and 90 who received more than one ICMA injection) and 318 in the reference group. Table 2 presents the extent of exposure to ICMA and the reference topical regimen for each study and the consolidated safety set.
 |
Table 2 Extent of Exposure |
Ocular Safety
Results from the main ocular safety evaluations are presented in Table 3 and described by category below.
 |
Table 3 Ocular Safety |
Adverse Events
Comparable percentages of patients in both groups experienced at least one ocular TEAE (17.0% in the ICMA group vs 18.6% in the reference group), TEAEs related to study medication (2.0% vs 2.5%, respectively) and serious ocular AEs (0.9% each; comprising 1 macular edema, 1 keratitis and 1 cataract operation complication [diagnosed as “persisting corneo-scleral tunnel”] in the ICMA group, and 1 eye hemorrhage [diagnosed as “hematoma of the orbit”], 1 retinal detachment and 1 PCR in the reference group). Two serious AEs in the ICMA group (macular edema and keratitis) were considered by the investigator to be (possibly) treatment related. The three serious events in the reference group were considered to be unrelated to treatment.
Regarding AEs of particular interest, PCR occurred in a single (0.3%) patient in the ICMA group and in 5 (1.6%) patients in the reference group. The incidence of macular edema was low in both groups. Visually significant macular edema (ie, having an impact on visual acuity) occurred in one patient in each group.
Cornea/Ocular Surface
The change in central corneal thickness was minimal in both groups, with similar corneal thicknesses at 1 month postoperatively (p=0.703). The median change in endothelial cell counts from baseline to 1 month postoperatively was −159 cells/mm2 in the ICMA group vs −116 cells/mm2 in the reference group. No statistically significant between-group difference was found in the number of endothelial cells at 1 month postoperatively (p=0.547).
The percentage of patients with superficial punctate corneal staining in the operated eye decreased in both groups between day 1 and 1 month postoperatively (from 29.0% [98 patients] to 9.3% [31 patients] in the ICMA group and from 36.3% [114 patients] to 12.2% [38 patients] in the reference group). Severe punctate corneal staining (grade 3) was less frequent in the ICMA group than the reference group at each assessment.
The percentage of patients with conjunctival hyperemia decreased from 25.9% (88 patients) at day 1 to 5.4% (18 patients) at 1 month postoperatively in the ICMA group, and from 32.0% (101 patients) at day 1 to 7.1% (22 patients) at 1 month in the reference group. Other ocular signs (palpebral edema, chemosis, conjunctival discharge, and folliculo-papillary conjunctivitis) were noted in a few patients in both groups after surgery (from 0.6% [2 patients] to 2.9% [10 patients] in the ICMA group and from 0.3% [1 patient] to 4.1% [13 patients] in the reference group).
Anterior Chamber
On day 1 postoperatively, anterior chamber cells were detected in the operated eye in 164 (48.7%) patients in the ICMA group and 172 (54.6%) patients in the reference group. Anterior chamber cells were generally few in number (≤5 cells) in both groups. At day 1, trace or mild anterior chamber flare was present in 114 (33.8%) patients in the ICMA group and in 129 (41.0%) patients in the reference group. One patient in the reference group had moderate anterior chamber flare. The number of patients with cells and flare declined at 1 week and 1 month postoperatively. The total score of anterior chamber cells and flare was similar between groups on day 1 (p=0.504), one week (p=0.743) and one month (p=0.885) postoperatively.
Mean postoperative IOP was generally similar to baseline values in both groups on day 1 and at one week postoperatively. At 1 month postoperatively, a small decrease from baseline IOP was observed in both groups (−2.00 mmHg in the ICMA group and −1.98 mmHg in the reference group).
On day 1 postoperatively, an abnormal pupil (mydriasis in 5 cases and miosis in 8 cases) in the operated eye was noted for 8 (2.4%) patients in the ICMA group and for 5 (1.6%) patients in the reference group. One patient (0.3%) in each group had a positive Seidel test in the operated eye.
Retina
Mean retinal thickness at 1 month postoperatively was similar between groups (p=0.606). The change from baseline was less than 50 µm for most patients in both groups (94.7% in the ICMA group and 95.0% in the reference group). The number of patients with RT of 300 µm or greater and a change from baseline of 50 µm or greater was low (5 [1.8%] and 6 [2.3%] patients, respectively).
The incidence of abnormal funduscopy was similar across visits for both treatment groups (7.9% to 10.5% of patients in the ICMA group and 7.7% to 9.7% in the reference group). Funduscopy outcomes were similar between groups at 1 month postoperatively (p=0.634).
Visual Acuity
The mean BCVA was increased in both groups postoperatively (Table 4). An increase in BCVA was seen in 312 (96.0%) patients in the ICMA group and 297 (95.8%) patients in the reference group. One (0.3%) patient in the ICMA group and 6 (1.9%) patients in the reference group had visual acuity ≤2/10 at 1 month postoperatively.
 |
Table 4 Best-Corrected Distance Visual Acuity at Each Assessment Time in the Eye to Be Operated/Operated Eye |
Systemic Safety
Fewer patients in the ICMA group (14 patients, 4.1%) than in the reference group (20 patients, 6.3%) experienced systemic TEAEs (Table 5). One patient (0.3%) in each group had a systemic TEAE that the investigator considered related to treatment (1 headache in the ICMA group and 1 nausea/migraine with aura in the reference group).
 |
Table 5 Systemic Adverse Events |
Similar increases in mean SBP between selection and during surgery were recorded in both groups. During follow-up, mean SBP returned to preoperative levels by 1 day following surgery and was maintained at that level until 1 month postoperatively. No relevant changes from baseline were observed at all postoperative visits in mean DBP (ranged from 76.6 to 78.4 mmHg across both treatment groups) and mean heart rate (ranged from 69.4 to 71.0 bpm). Fewer patients in the ICMA group (23 patients, 6.8%) than in the reference group (36 patients, 11.6%) presented with instances of hypertension or tachycardia events (either at least one DBP value>100 mmHg, one SBP value>200 mmHg, or one HR value>120 bpm) on the day of surgery (p=0.040).
Subjective Ocular Symptoms and Patient Satisfaction
Figure 1 presents the incidence of ocular symptoms in both groups from baseline to 1 month postoperatively. Most patients were free of symptoms or had mild symptoms following surgery (>97% in the ICMA group and >95% in the reference group for each symptom). At day 8 postoperatively, there were statistically significantly fewer patients who reported ongoing pain in the ICMA group (1.8%) compared with the reference group (4.1%; p=0.034). This was also noted for irritation/burning/stinging at 8 days (10.9% vs 15.9%, respectively; p=0.041) and one month (5.1% vs 11.5%; p=0.004).
 |
Figure 1 Individual ocular symptoms at each assessment time. (A): Pain; (B): Irritation/burning/stinging; (C) Photophobia; (D) Foreign body sensation. Each ocular symptom was rated overall for both eyes using a 4-point severity scale (none, mild, moderate, severe) at baseline (Day -60/-7, selection visit), and at day 1, 1 week, and 1 month postoperatively. |
Most patients assessed their study treatment as very satisfactory or satisfactory (99.1% [337 patients] in the ICMA group vs 97.2% [307 patients] in the reference group). Three (0.9%) patients in the ICMA group and 9 (2.8%) patients in the reference group were “not very satisfied” with the procedure.
Global Tolerance Assessment by the Investigator
Global tolerance of the study treatment, as assessed by the investigator, was very satisfactory or satisfactory for most patients (>96%) in both groups at each visit. The investigators assessed global tolerance of the study treatment as not very satisfactory or unsatisfactory for a lower percentage of patients in the ICMA group (0.9% [3 patients] at 1 day and one week, and 1.8% [6 patients] at one month) compared with the reference group (3.5% [11 patients], 2.9% [9 patients] and 1.6% [5 patients], respectively). A statistically significant difference was found between the two groups at 1 day (p=0.013).
Safety Profile of Patients Who Received More Than One Injection of ICMA
Ninety patients received more than the recommended dose (one single injection) of ICMA (Table 2). The incidence of ocular AEs was higher in patients who received ≥2 injections of ICMA (23.3% of patients) compared to 1 injection (14.7%). TEAEs that the investigator considered possibly related to the study treatment were noted in 2 (2.2%) patients (1 keratitis and 1 PCR). Serious AEs included keratitis and a persistent corneo-scleral tunnel associated with the surgical procedure. A systemic TEAE was experienced by 5.6% of patients receiving ≥2 injections versus 3.6% for 1 ICMA injection.
Ocular symptoms occurred mainly at day 1 postoperatively and were more frequently reported in patients who received ≥2 injections of ICMA (pain for 11 [12.4%] patients vs 8 [3.2%] patients who received 1 injection; irritation/burning/stinging in 24 [27.0%] vs 37 [14.7%] patients; foreign body sensation in 27 [30.3%] vs 38 [15.1%] patients, respectively).
The median decrease in endothelial cell density from baseline was also higher for patients who received ≥2 injections of ICMA (−213 cells/mm2) than for patients who received 1 injection (−149 cells/mm2).
Discussion
The current study evaluated the safety of an approved, commercially available, pharmaceutical standard ICMA for phacoemulsification cataract surgery. No ocular or systemic safety issues were observed during the development of this new fixed combination for intracameral use. This was further verified by the pooled safety analysis presented in the current study, indicating that ICMA is safe and well tolerated, and comparable to the standard topical regimen.
Ocular AEs related to treatment (or with an unknown relationship) were below 3% in both groups, and there were no serious AEs requiring hospitalization or resulting in permanent visual loss in either group. PCR was less frequent in the ICMA group than in the reference group. The better stability of mydriasis provided by administration via the intracameral route may have contributed to this difference.26,27,29 Incomplete or unstable mydriasis is associated with intraoperative and postoperative complications in general and PCR in particular.30–32 Adequate and stable mydriasis improves the surgical conditions, thereby reducing the risk of PCR. In the phase III study of ICMA, the different steps of the surgery were considered uncomplicated (not technically challenging) for more than 90% of the patients who received ICMA for mydriasis, and the intraocular lens implantation step was considered “technically challenging” for fewer cases in the ICMA group (0.4% of patients) compared to the reference group (1.8%), and this difference was statistically significant (p=0.047, CMH).26
Although macular edema was reported marginally more frequently in the ICMA group (4 events, 1.2% of patients) than in the reference group (2 events, 0.6%), there was no between-group difference in terms of the incidence of clinically significant macular edema (1 event in each group). The incidence of macular edema reported in the current study is among the lowest reported in the literature.5,6,8 One patient in the ICMA group with clinically significant macular edema underwent a complicated and protracted surgery and was non-adherent to the postoperative anti-inflammatory regimen. The patient was diagnosed with cystoid macular edema with retinal thickening of 455 μm, which was resolved with medical therapy at 12 months postoperatively. Two other patients in the ICMA group presented with subclinical macular edema. Postoperatively, the retinal thickness was within normal limits in most patients, there was a low incidence of macular edema with good mean postoperative BCVA. Combined, these observations indicate that ICMA does not increase the risk of clinically significant macular edema after cataract surgery.
Specular microscopy values were similar between groups indicating that there were no safety concerns regarding endothelial cell loss due to ICMA. Similarly, a comparable decrease in endothelial cell density was shown between the two mydriatic protocols in a more recent study.33 The endothelial cell loss observed in this study in the ICMA group (mean loss of 8.3%) is within the range reported for routine phacoemulsification cataract surgery (4.3% to 16.8% loss).34–38 Endothelial exposure to the constituents of ICMA is minimal and of short duration and is mitigated by prolonged and abundant rinsing of the anterior chamber during surgery. Endothelial toxicity due to ICMA was not anticipated on the basis of several preclinical animal studies using clinically relevant concentrations of lidocaine, either alone or in combination with tropicamide.39–41 In addition, clinical experience with intracameral administration of the components of ICMA is extensive and endothelial cell toxicity has not been shown to be clinically significant.20,41–43
The outcomes of the current study indicate that ICMA is safe and may offer advantages compared to standard eye drops regimen. ICMA avoids the risk of corneal epithelial toxicity induced by repeated instillations or the use of preserved topical preparations.16,19 In the present study, corneal staining of moderate or severe intensity (Grade 2 and 3) was about twice as common with the standard topical regimen (reference group) on day 1 postoperatively, compared with ICMA (3.9% vs 7.0%, respectively). Additionally, more patients in the reference group (4 patients, 1.2%) experienced ocular AEs suggestive of a more pronounced corneal damage (corneal epithelial defect, corneal erosion, ulcerative keratitis) compared to the patients who received ICMA (1 patient, 0.3%; data not shown). Corneal toxicity is a common AE of topical medications, particularly local anesthetics such as tetracaine and those containing preservatives.44 Repeated preoperative use of anesthetics and topical mydriatics that contain preservatives can damage the ocular surface and may play a pathogenic role in inducing or aggravating post-surgical discomfort. Of note, patients in both studies received the same amount of tetracaine drops preoperatively, except for patients in the reference group of the Phase II study who received an additional tetracaine drop 1 minute before surgery. However, this additional tetracaine drop had no impact on clinical outcomes such as corneal staining between the two groups (data not shown). More generally, the intracameral route also exposes patients to less discomfort associated with intensive topical mydriatic use, perhaps explaining the lower rates of some ocular symptoms (pain and irritation/burning/stinging) postoperatively in the ICMA group.20,22,45
In the current study, no notable changes in mean vital signs parameters were observed, indicating no systemic safety concerns with ICMA. ICMA may reduce the risk of systemic AEs due to the lower overall drug exposure provided by the intracameral route.46 As the bioavailability of the intracameral route is higher, the delivered dose of phenylephrine with a single ICMA injection of 0.2 mL (0.62 mg) is 16.5 times less than the recommended dose of phenylephrine 10% eye drops (10.2 mg for 3 drops) and up to 54.8 times less (34 mg for 10 drops) than the maximum dose of topical phenylephrine received during the phase III trial.26,46 In pharmacokinetic studies, only 14.3% of ICMA treated patients had detectable levels of phenylephrine in the blood (maximum concentration measured: 0.59 ng/mL).46 In contrast, all patients in the reference group had detectable levels of phenylephrine in the blood (maximum concentration: 1.42 ng/mL).46 Similarly, no ICMA patients had detectable plasma levels of tropicamide, whereas all patients in the reference group had detectable levels of tropicamide.46 Consistently with other studies,25 the present study suggested a safety advantage for ICMA over a topical regimen in terms of cardiovascular events, as more patients receiving the topical mydriatic regimen experienced meaningful instances of hypertension or tachycardia than those receiving ICMA. Moreover, the conditions of a controlled clinical trial may not accurately reflect those in a wider clinical practice.25 The use of low concentrations of the mydriatics in ICMA likely minimizes the risk of systemic, particularly cardiovascular AEs.
During the initial clinical trials for ICMA, delivering a second injection was left to the discretion of the surgeon. However, additional analyses of the mydriatic efficacy of ICMA demonstrated that a second injection conferred no additional benefits on pupil dilation compared to one injection.27 Therefore, ICMA has been approved for only one 0.2 mL injection.28 The basis of this approval is also supported by the current pooled safety analyses as 2 (or more) ICMA injections demonstrated a less favorable safety profile compared to one injection. This difference may be explained by a potential higher proportion of patients with more risk factors for cataract surgery complications and/or a high proportion of investigators with less experience or less confidence in ICMA than in their daily pupil dilation protocol. These risk factors combined with the longer surgery caused by the second ICMA injection could explain the observed difference. However, reassuringly, comparison of the AEs following 2 (or more) ICMA injections compared to a single injection did not raise any systemic safety concerns compared to the reference treatment regimen, and the product approval restricts ICMA to one injection, which addresses any potential issue regarding unexpected toxicity of repeated administration of ICMA.
Intracameral mydriatics and anesthetics are commonly used in cataract surgery. In 2013, a survey of 490 cataract surgeons indicates that mydriatics are administered in the operating room in 9% of cataract operations and that topical anesthesia is supplemented by off-label intracameral anesthetics in 21% of surgeries.21 These practices may increase the risk of contamination and toxicity due to the injection of products not specifically designed for intracameral use.21 Use of the intracameral route relieves staff from multiple instillations of mydriatics and additional local anesthetic during the preoperative period. In preparing 10 patients for surgery, 60 individual instillations of topical products are typically required. Multiple instillations of topical drops present risks for errors and cross-contamination, as well as engendering stress in the patient. In addition, the intracameral route allows surgeons to control the preoperative mydriatic delivery to the patients, and consequently, the risk of inadequate dosing is minimized. The presence of medical staff when administration of mydriatics takes place means prompt intervention is available in the case of systemic AEs due to phenylephrine. A single injection in the operating room may also prove to be less stressful for patients.
Conclusion
In summary, ICMA injection at the beginning of cataract surgery is safe and offers advantages over the standard topical mydriatic regimen. Repeat instillation of topical preparations are avoided which improves patient management in ophthalmology clinics and avoids corneal toxicity associated with topical administration. Moreover, the availability of a specific approved intracameral preparation eliminates the risks associated with “homemade” preparations and reduces the potential for dosing errors.
Data Sharing Statement
Since the data were collected from two clinical trials, these are not intended to be shared by the authors, and no other study-related documents will be made available.
Acknowledgments
This study was conceived and funded by Laboratoires Théa, Clermont Ferrand, France.
Disclosure
AB, BC, FC, and RM are consultants for Laboratoires Théa. BC reports personal fees from Thea consultant and clinical investigator, outside the submitted work; and Clinical investigator and consultant for: Hoya, Horus, J&J, B&L, Roche. The authors report no other conflicts of interest in this work.
References
1. Wang W, Yan W, Fotis K, et al. Cataract surgical rate and socioeconomics: a global study. Invest Ophthalmology Visual Science. 2016;57(14):5872–5881. doi:10.1167/iovs.16-19894
2. Ellwein LB, Lepkowski JM, Thulasiraj RD, Brilliant GE. The cost effectiveness of strategies to reduce barriers to cataract surgery. Operat Res Group. Int Ophthalmol. 1991;15(3):175–183.
3. Boisjoly H, Freeman EE, Djafari F, et al. Reducing wait time for cataract surgery: comparison of 2 historical cohorts of patients in Montreal. Can J Ophthalmol. 2010;45(2):135–139. doi:10.3129/i09-256
4. Bernhisel A, Pettey J. Manual small incision cataract surgery. Curr Opin Ophthalmol. 2020;31(1):74–79. doi:10.1097/ICU.0000000000000624
5. Greenberg PB, Tseng VL, W-C W, et al. Prevalence and predictors of ocular complications associated with cataract surgery in United States veterans. Ophthalmology. 2011;118(3):507–514. doi:10.1016/j.ophtha.2010.07.023
6. Jaycock P, Johnston RL, Taylor H, et al. The cataract national dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye. 2009;23(1):38–49. doi:10.1038/sj.eye.6703015
7. Behndig A, Montan P, Stenevi U, Kugelberg M, Lundstrom M. One million cataract surgeries: Swedish national cataract register 1992-2009. J Cataract Refract Surg. 2011;37(8):1539–1545. doi:10.1016/j.jcrs.2011.05.021
8. Zaidi FH, Corbett MC, Burton BJL, Bloom PA. Raising the benchmark for the 21st century--The 1000 cataract operations audit and survey: outcomes, consultant-supervised training and sourcing NHS choice. British J Ophthalmology. 2007;91(6):731–736. doi:10.1136/bjo.2006.104216
9. Lundström M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European registry of quality outcomes for cataract and refractive surgery database. J Cataract Refractive Surg. 2012;38(6):1086–1093. doi:10.1016/j.jcrs.2012.03.006
10. Stein JD, Grossman DS, Mundy KM, Sugar A, Sloan FA. Severe adverse events after cataract surgery among medicare beneficiaries. Ophthalmology. 2011;118(9):1716–1723. doi:10.1016/j.ophtha.2011.02.024
11. Segers MHM, Behndig A, van den Biggelaar FJHM, et al. Outcomes of cataract surgery complicated by posterior capsule rupture in the European registry of quality outcomes for cataract and refractive surgery. J Cataract Refractive Surg. 2022;48(8):942–946. doi:10.1097/j.jcrs.0000000000000901
12. Wielders LHP, Schouten JSAG, Winkens B, et al. ESCRS PREMED study group. randomized controlled European multicenter trial on the prevention of cystoid macular edema after cataract surgery in diabetics: ESCRS PREMED study report 2. J Cataract Refract Surg. 2018;44(7):836–847. doi:10.1016/j.jcrs.2018.05.015
13. Wielders LHP, Schouten JSAG, Winkens B, et al.; ESCRS PREMED Study Group. European multicenter trial of the prevention of cystoid macular edema after cataract surgery in nondiabetics: ESCRS PREMED study report 1. J Cataract Refract Surg. 2018;44(4):429–439. doi:10.1016/j.jcrs.2018.01.029
14. Ganekal S, Nagarajappa A. Comparison of morphological and functional endothelial cell changes after cataract surgery: phacoemulsification versus manual small-incision cataract surgery. Mid East African J Ophthalmology. 2014;21(1):56–60. doi:10.4103/0974-9233.124098
15. Rosado-Adames N, Afshari NA. The changing fate of the corneal endothelium in cataract surgery. Curr Opinion Ophthalmology. 2012;23(1):3–6. doi:10.1097/ICU.0b013e32834e4b5f
16. Rengstorff RH, Doughty CB. Mydriatic and cycloplegic drugs: a review of ocular and systemic complications. Am J Optom Physiol Opt. 1982;59(2):162–177. doi:10.1097/00006324-198202000-00008
17. Zakrzewski PA, Banashkevich AV, Friel T, Braga-Mele R. Monitored anesthesia care by registered respiratory therapists during cataract surgery: an update. Ophthalmology. 2010;117(5):897–902. doi:10.1016/j.ophtha.2009.10.005
18. Behndig A, Korobelnik JF. Mydriatic insert and intracameral injections compared with mydriatic eyedrops in cataract surgery: Controlled studies. J Cataract Refract Surg. 2015;41(7):1503–1519. doi:10.1016/j.jcrs.2014.12.050
19. Fraunfelder FW, Rich LF. Possible adverse effects of drugs used in refractive surgery. J Cataract Refract Surg. 2003;29(1):170–175. doi:10.1016/S0886-3350(02)01836-9
20. Lundberg B, Behndig A. Intracameral mydriatics in phacoemulsification cataract surgery. J Cataract Refract Surg. 2003;29(12):2366–2371. doi:10.1016/S0886-3350(03)00522-4
21. Behndig A, Cochener-Lamard B, Guell J, et al. Surgical, antiseptic, and antibiotic practice in cataract surgery: Results from the European observatory in 2013. J Cataract Refract Surg. 2015;41(12):2635–2643. doi:10.1016/j.jcrs.2015.06.031
22. Behndig A, Linden C. Aqueous humor lidocaine concentrations in topical and intracameral anesthesia. J Cataract Refract Surg. 1998;24(12):1598–1601. doi:10.1016/S0886-3350(98)80349-0
23. Behndig A, Eriksson A. Evaluation of surgical performance with intracameral mydriatics in phacoemulsification surgery. Acta Ophthalmol Scand. 2004;82(2):144–147. doi:10.1111/j.1600-0420.2004.00241.x
24. Nikeghbali A, Falavarjani KG, Kheirkhah A, Bakhtiari P, Kashkouli MB. Pupil dilation with intracameral lidocaine during phacoemulsification. J Cataract Refract Surg. 2007;33(1):101–103. doi:10.1016/j.jcrs.2006.08.044
25. Morgado G, Barros P, Martins J, Lima A, Martins N. Comparative study of mydriasis in cataract surgery: topical versus mydriasert versus intracameral mydriasis in cataract surgery. Eur J Ophthalmol. 2010;20(6):989–993. doi:10.1177/112067211002000618
26. Labetoulle M, Findl O, Malecaze F, et al. Evaluation of the efficacy and safety of a standardised intracameral combination of mydriatics and anaesthetics for cataract surgery. Br J Ophthalmol. 2016;100(7):976–985. doi:10.1136/bjophthalmol-2015-307587
27. Chiambaretta F, Pleyer U, Behndig A, et al. Pupil dilation dynamics with an intracameral fixed combination of mydriatics and anesthetic during cataract surgery. J Cataract Refract Surg. 2018;44(3):341–347. doi:10.1016/j.jcrs.2017.12.025
28. Laboratoires Thea. Mydrane summary of product characteristics latest updated on eMC: 02 sept 2021. Mydrane 0.2 mg/mL + 3.1 mg/mL + 10 mg/mL solution for injection - Summary of Product Characteristics (SmPC) - (emc) (medecines org.UK); 2023Available fromhttps://www.medicines.org.uk/emc/product/7254/smpc/print.
29. Segers MHM, Rosen P, van den Biggelaar FJHM, et al. Anesthesia techniques and the risk of complications as reflected in the European registry of quality outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2022;48(12):1403–1407. doi:10.1097/j.jcrs.0000000000001009
30. Guzek JP, Holm M, Cotter JB, et al. Risk factors for intraoperative complications in 1000 extracapsular cataract cases. Ophthalmology. 1987;94(5):461–466. doi:10.1016/S0161-6420(87)33424-4
31. Narendran N, Jaycock P, Johnston RL, et al. The cataract national dataset electronic multicentre audit of 55,567 operations: risk stratification for posterior capsule rupture and vitreous loss. Eye. 2009;23(1):31–37. doi:10.1038/sj.eye.6703049
32. Vukicevic M, Gin T, Al-Qureshi S. Prevalence of optical coherence tomography-diagnosed postoperative cystoid macular oedema in patients following uncomplicated phaco-emulsification cataract surgery. Clin Exp Ophthalmol. 2012;40(3):282–287. doi:10.1111/j.1442-9071.2011.02638.x
33. Nazim-Lipski G, Bolsega-Pacud J, Kubicka-Trzaska A, Markiewicz A, Romanowska-Dixon B. Mydrane intracameral injection site can be an alternative to mydriatic drops instillation in cataract surgery. J Physiol Pharmacol. 2020;71(2). doi:10.26402/jpp.2020.2.08
34. Bourne RR, Minassian DC, Dart JK, Rosen P, Kaushal S, Wingate N. Effect of cataract surgery on the corneal endothelium: modern phacoemulsification compared with extracapsular cataract surgery. Ophthalmology. 2004;111(4):679–685. doi:10.1016/j.ophtha.2003.07.015
35. Miyata K, Maruoka S, Nakahara M, et al. Corneal endothelial cell protection during phacoemulsification: low- versus high-molecular-weight sodium hyaluronate. J Cataract Refract Surg. 2002;28(9):1557–1560. doi:10.1016/S0886-3350(02)01540-7
36. O’Brien PD, Fitzpatrick P, Kilmartin DJ, Beatty S. Risk factors for endothelial cell loss after phacoemulsification surgery by a junior resident. J Cataract Refract Surg. 2004;30(4):839–843. doi:10.1016/S0886-3350(03)00648-5
37. Cho YK, Chang HS, La TY, et al. Anterior segment parameters using pentacam and prediction of corneal endothelial cell loss after cataract surgery. Korea J Ophthalmology. 2010;24(5):284–290. doi:10.3341/kjo.2010.24.5.284
38. Eggeling P, Pleyer U, Hartmann C, Rieck PW. Corneal endothelial toxicity of different lidocaine concentrations. J Cataract Refract Surg. 2000;26(9):1403–1408. doi:10.1016/S0886-3350(00)00379-5
39. Chang YS, Tseng SY, Tseng SH, Wu CL. Cytotoxicity of lidocaine or bupivacaine on corneal endothelial cells in a rabbit model. Cornea. 2006;25(5):590–596. doi:10.1097/01.ico.0000220775.93852.02
40. Kim EC, Park SH, Kim MS. A comparison of pupil dilation and induction of corneal endothelial apoptosis by intracameral 1% lidocaine versus 1:100,000 epinephrine in rabbits. J Ocul Pharmacol Ther. 2010;26(6):563–570. doi:10.1089/jop.2010.0078
41. Mori Y, Miyai T, Kagaya F, et al. Intraoperative mydriasis by intracameral injection of mydriatic eye drops: in vivo efficacy and in vitro safety studies. Clin Exp Ophthalmol. 2011;39(5):456–461. doi:10.1111/j.1442-9071.2010.02456.x
42. Poyales-Galan F, Pirazzoli G. Clinical evaluation of endothelial cell decrease with VisThesia in phacoemulsification surgery. J Cataract Refract Surg. 2005;31(11):2157–2161. doi:10.1016/j.jcrs.2005.07.016
43. Rigal-Sastourne JC, Huart B, Pariselle G, et al. Diffusion de la lidocaïne après injection intracamérulaire. J Fr Ophtalmol. 1999;22(1):21–24.
44. Baudouin C, Labbe A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
45. Soong T, Soultanidis M, Claoue C, Gallagher M, Thomson S. Safety of intracameral mydriasis in phacoemulsification cataract surgery. J Cataract Refract Surg. 2006;32(3):375–376. doi:10.1016/j.jcrs.2005.12.088
46. Guell J, Behndig A, Pleyer U, et al. Systemic exposure to intracameral vs topical mydriatic agents: in cataract surgery. Clin Ophthalmol. 2019;13:811–819. doi:10.2147/OPTH.S189671
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.