")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Safety Assessment of the Pharmacotherapy Process at the Nurse and Midwife Level – An Observational Study
Authors Witczak I, Uchmanowicz I , Tartaglia R , Rypicz Ł
Received 13 August 2020
Accepted for publication 26 September 2020
Published 4 November 2020 Volume 2020:16 Pages 1057—1065
DOI https://doi.org/10.2147/TCRM.S276901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Izabela Witczak,1 Izabella Uchmanowicz,2 Riccardo Tartaglia,3 Łukasz Rypicz1
1Department of Health Care Economics and Quality, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland; 2Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland; 3President of the Italian Network for Safety in Health Care, Florence, Italy
Correspondence: Izabella Uchmanowicz
Faculty of Health Sciences, Department of Clinical Nursing, Wroclaw Medical University, Bartla 5, Wroclaw 51-618, Poland
Tel +48 71 784 18 05
Fax +48 71 345 93 24
Email [email protected]
Purpose: Pharmacological errors are among the most common in the healthcare system. This study aimed to determine the level of safety of the pharmacotherapy process at the stage performed by nurses and midwives by indicating the key risk factors affecting patients’ safety.
Methods: A group of 1276 nurses and 136 midwives in Poland participated in the study. The survey was conducted in the period from May 2019 to August 2019. The original Nursing Risk in Pharmacotherapy (NURIPH) tool was used.
Results: The Cronbach alpha coefficient was 0.832. The low legibility of the medical orders (item 1) was indicated as the highest risk. A mean of 4.50 means that this factor’s significance is assessed between “very significant” and “significant.” The communication between physician, nurse and midwife, time pressure, and work organization were also rated high (Items 2, 3, and 4). The averages for these factors are higher than 4, so their evaluation is more than “significant.”.
Conclusion: Nurses and midwives involved in the pharmacotherapy process are exposed to many ergonomic factors triggering risk. A huge problem is the lack of readability of medical orders, which may be a factor triggering a medical error.
Keywords: patient safety, medication error, NURIPH tool, nurses and midwives, pharmacotherapy, risk management
Introduction
Pharmacotherapy errors are among the most common in the healthcare system and account for 10 to 18% of all medical errors. These errors can cause serious health consequences for the patient, and even his or her death.1,2
There is no single, accepted definition of medication errors. The World Health Organization (WHO) refers to the definition of the United States National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP), which describe a medical error as any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and systems, including prescribing, order communication, product labeling, packaging, and nomenclature, compounding, dispensing, distribution, administration, education, monitoring, and use.3
The pharmacotherapy process is burdened with a high risk of an adverse event, and nurses play a key role in this process.4 Usually, errors occur most often at the last stage of this process; therefore, it is the final stages and their leaders, ie, nurses and midwives, who are at the highest risk.5
In the process of pharmacotherapy, we can distinguish three key stages: ordering the drug by a physician, preparation of the drug by a pharmacist (or in some cases by a nurse/midwife), and administration of the drug by a nurse or midwife. An error can occur at each of these stages. Therefore, several categories of medication-related errors can be distinguished.6 Aronson7 classifies the medication errors in four categories: knowledge-based errors (through lack of knowledge), rule-based errors (using a bad rule or misapplying a good rule), action-based errors (called slips) and memory-based errors (called lapses).
The process approach in the health care system allows seeing the importance of nurses in ensuring patient safety and in ensuring high quality of services.8 The severe working conditions (eg overload, occupational stress, staffing) of this occupational group are potential risk factors. In order to build a safety culture and guarantee a high quality of provided services, ergonomic working conditions should be created, which should reduce the occurrence of adverse events, including medication errors.9–11
It is worth noting that the consequences of medication errors are multifaceted. The clinical consequences of such events are often mentioned, but the financial aspect is forgotten. Well, undesirable events resulting from medication errors are very costly for the healthcare sector. Walsh et al12 report that the average cost of medication errors for a patient ranges from EUR 2.58 to EUR 111 727.08. It is estimated that the total global cost of medication-related errors is $42 billion annually, which is almost 1% of total global health expenditure13 Among other things, due to the cost and frequency of medication errors, during The Second Global Summit of Health Ministers on Patient Safety in Bonn, Germany in 2017, The Third Global Patient Safety Challenge, Medication Without Harm was established, whose main objective is to reduce patient harm worldwide by half over five years.14
Based on a detailed literature review, own previous research and many years of experience of the authors in the field of hospital auditing, e.g., in the area of pharmacotherapy process safety, a tool for risk assessment in the pharmacotherapy process carried out by nurses and midwives called Nursing Risk in Pharmacotherapy (NURIPH) was developed. It can be used to identify the most dangerous areas that directly impact the risks to patients. Identifying risk factors allows early prevention of adverse events by introducing preventive measures.
The identification of risk triggers in the pharmacotherapy process, which was carried out in the present study, may play a significant role in improving the safety of the hospitalized patient and medical staff. The tool presented in the paper can be used as a checklist during audits of pharmacotherapy processes, thanks to which it is possible to mark critical factors in ensuring safety.
The aim of the study was to determine the level of safety of the pharmacotherapy process at the stage performed by nurses and midwives by indicating the key risk factors affecting patients’ safety directly.
Methods
Study Design and Settings
The survey was conducted in the period from May 2019 to August 2019 in cooperation with the Supreme Chamber of Nurses and Midwives of Poland. Messages were sent to the District Chambers of Nurses and Midwives with information about surveying the pharmacovigilance safety among nurses and midwives. The invitation to participate in the study was accompanied by a link to the website where the questionnaire was placed. The authors administered the website where the NURIPH tool was posted and made available to participants.
The study was fully anonymous and voluntary. The independent Bioethics Committee approved the research project of the Wroclaw Medical University (no. KB–610/2017). All participants gave their written informed consent after a thorough explanation of the procedures involved. The study was carried out in accordance with the tenets of the Declaration of Helsinki and guidelines of Good Clinical Practices.15
Study Participants
The criterion for inclusion in the study was the possession of the current license to practice as a registered professional nurse (RN) or midwives (RM) and their documented professional activity. The study involved 1412 participants from all over Poland, including 1276 nurses (the global percentage of study participants is 0.55%) and 136 midwives (the global percentage of study participants is 0.49%). The survey excluded 340 subjects who did not complete the questionnaire; thus, the results were not completed and, at the same time, rejected from further analysis.
Research Tools
NURIPH’s proprietary and new tool consists of a metric on sociodemographic data and a risk matrix to evaluate selected ergonomic factors triggering risk in the pharmacotherapy process. Nine risk factors were considered in the matrix: 1 – Poorly legible or illegible medical orders; 2 – Inappropriate communication between physician, nurse, and midwife regarding changes in drug ordinance; 3 – Pressure of time during nurse/medical supervisor; 4 – Inappropriate work organization: preparation of medicines for patients combined with the simultaneous performance of other activities by a nurse/midwife (e.g., answering calls, execution of current diagnostic orders); 5 – Lack of clarity or illegibility of medical orders of nurses and midwives; 6 – No physician ‘s prescription of specific solvent for this medicine; 7 – Shift work causing psychophysiological fatigue; 8 – Limited availability of training on the effects of medicines, side effects and adverse reactions to medicines used in patients; and 9 – Preparation of personalized sheets with the name and dosage of the medicine on the drug tray.
A five-step scale of risk assessment was applied (from 1 to 5) was used to assess the above ergonomic factors: 1 – minor risk, 2 – little risk, 3 – significant risk, 4 – more significant risk, and 5 – very significant risk.
The relationship between the levels of risk in the pharmacovigilance brochure and the likelihood of adverse health effects on the patient and the likelihood of a nurse/midwife being legally liable is shown in Table 1.
 |
Table 1 Linking Risk Levels in the Pharmacotherapy Process to Negative Health Consequences for the Patient and the Legal Responsibility of Nurses and Midwives |
Data Collection
The NURIPH questionnaire was available on the website throughout the survey. The link to the questionnaire was published on the Supreme Chamber of Nurses and Midwives website and the website of the District Chambers of Nurses and Midwives. Also, the study was promoted during the national conferences dedicated to nurses and midwives. Each participant completed an anonymous NURIPH questionnaire via the internet. After completing the questionnaire, participants validated and sent the questionnaire electronically to the platform where the data was collected.
Statistical Analysis
A significance level of 0.05 was adopted in the analysis. Thus, all p values below 0.05 were interpreted as statistically significant. The reliability of the scale used was checked by calculating the Cronbach alpha coefficient and the discriminating power of individual items. Mann–Whitney test was used to compare the significance of individual factors for two groups. Comparisons for three or more groups were made using the Kruskal–Wallis test. If statistically significant differences were detected, the post hoc analysis was performed using Dunn’s test to identify statistical significance between different groups. The analysis was performed in the R program, version 3.6.116
NURIPH Validation
The Cronbach alpha coefficient for the NURIPH tool is 0.832. Based on the obtained value of the Cronbach alpha coefficient, it should be concluded that the tool is reliable. All items have positive discrimination power (Table 2). It means that they positively correlate with other items in the scale (item-total correlation), which is a very desirable effect. We can also see that the exclusion of any item does not increase the alpha index. It should be stated that the tool is constructed correctly.
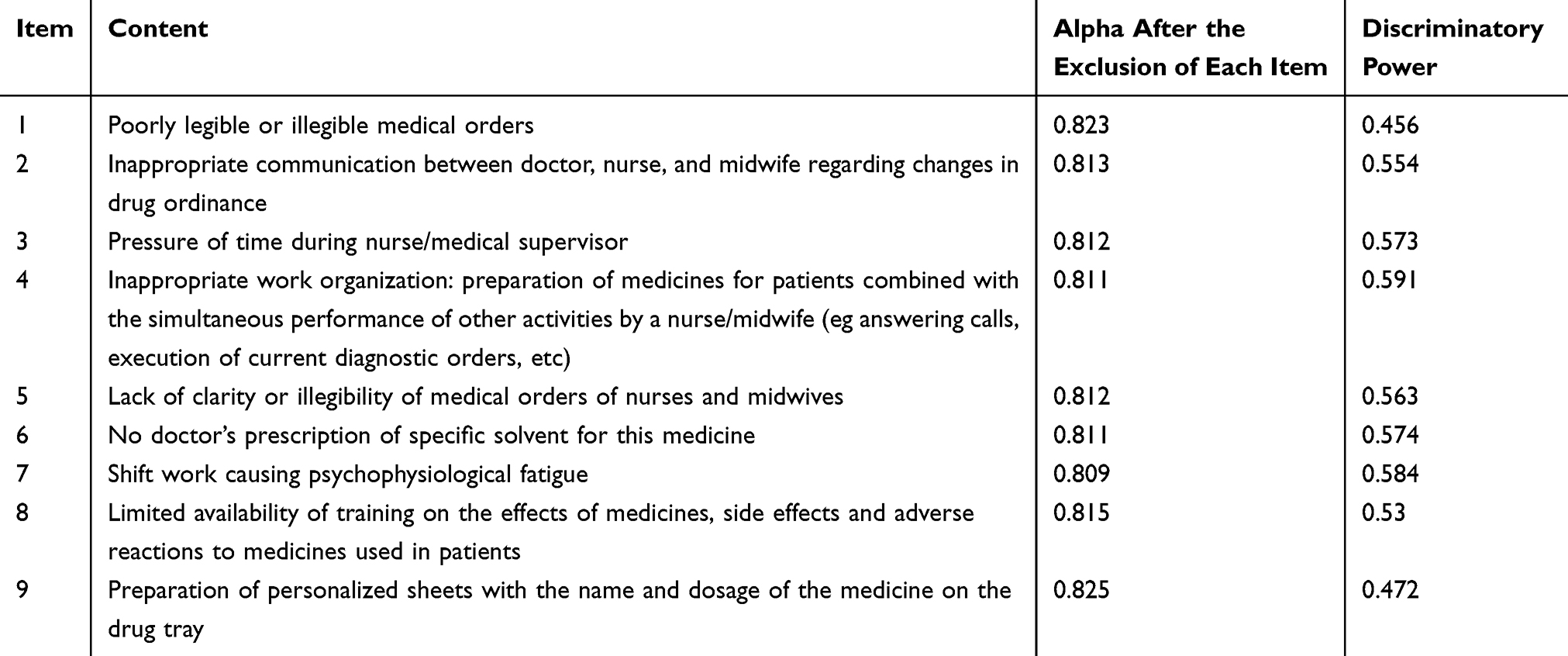 |
Table 2 Nursing Risk in Pharmacotherapy (NURIPH) Item Values for Alpha Cronbach and Discriminatory Power |
Results
Participants’ Characteristics
The professional group of nurses was represented by women (94.36%) and men (5.64%), while the professional group of midwives was represented only by women (100%). The nurses were older than midwives – they represented the 50–59 age bracket (38.48%), the 20–29 age bracket (29.41%), and the 50–59 age bracket (29.41%). Nurses also more often had lower education – 16.54% of respondents had secondary education and 8.82% of midwives. Midwives showed a shorter length of service than nurses – most often, they showed up to 5 years (26.47%), nurses 30 years, and more (39.81%). Nurses (8.86%) less often than midwives (15.44%) worked in primary health care (PCP). However, both professional groups often take up additional employment in the same way – 38.79% of nurses and 38.97% of midwives reported working in more than one place. Detailed characteristics of the examined group of nurses and midwives are presented in Table 2.
Results for the Individual “Items”
Respondents assigned the highest risk to low legibility of medical orders (item 1). A mean of 4.50 means that the significance of this factor is assessed between “very significant” and “significant.” The communication between physician, nurse, and midwife, time pressure, and work organization were also rated high (Items 2, 3, and 4). The averages for these factors are higher than 4, so their evaluation is more than “significant” (Table 3).
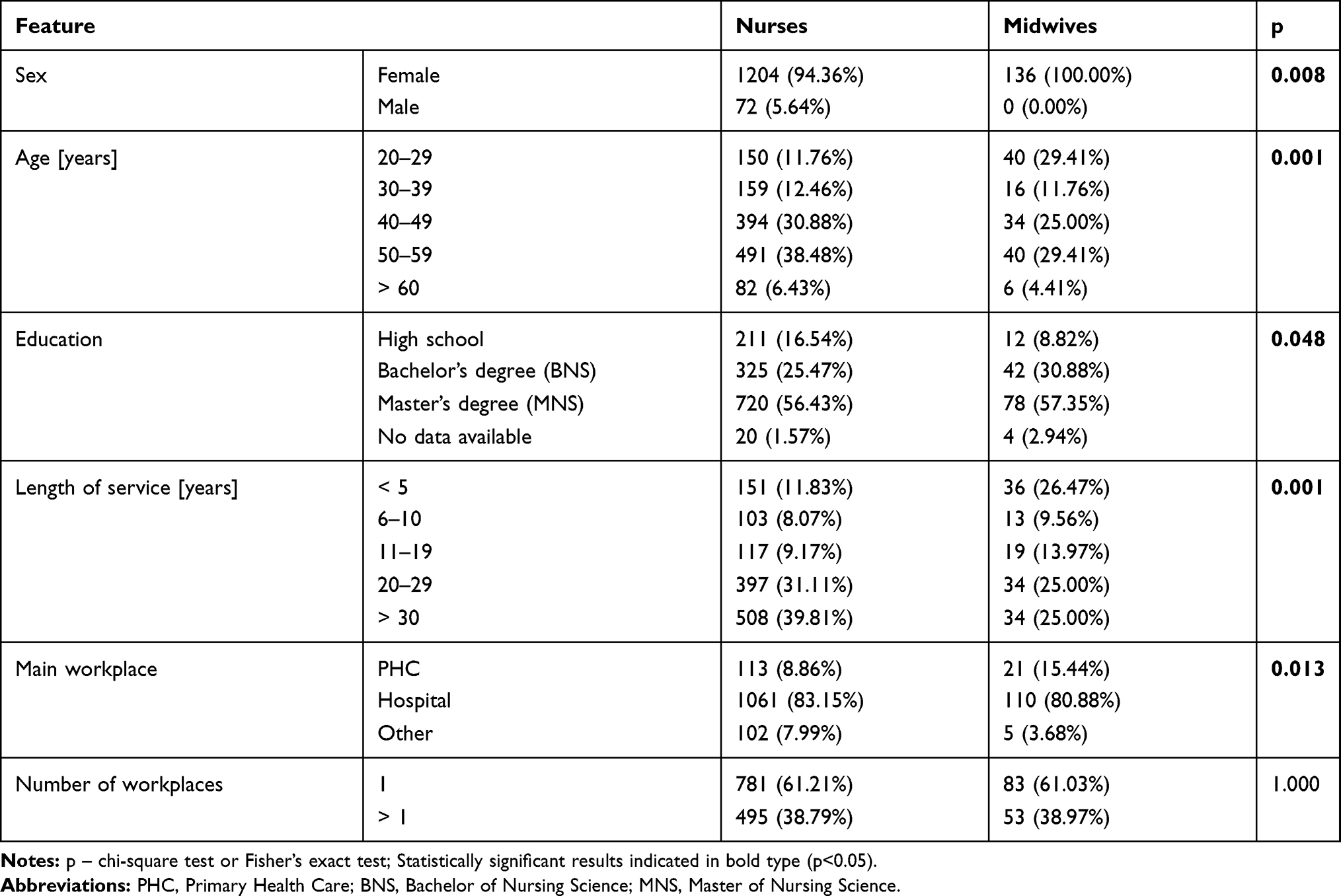 |
Table 3 Characteristics of the Study Group |
The least significant were the lack of orders for a specific solvent of a drug and the preparation of personal sheets with the name and dose of a drug on a tray with drugs (Items 6 and 9). However, the averages for them are only slightly below 3.5, which still means significant factors. Interestingly, the shift work (item 7) as a risk factor was rated “very significant” by only 35.62% of respondents, reaching an average value of 3.74, which corresponds to the level “significant” (Table 4).
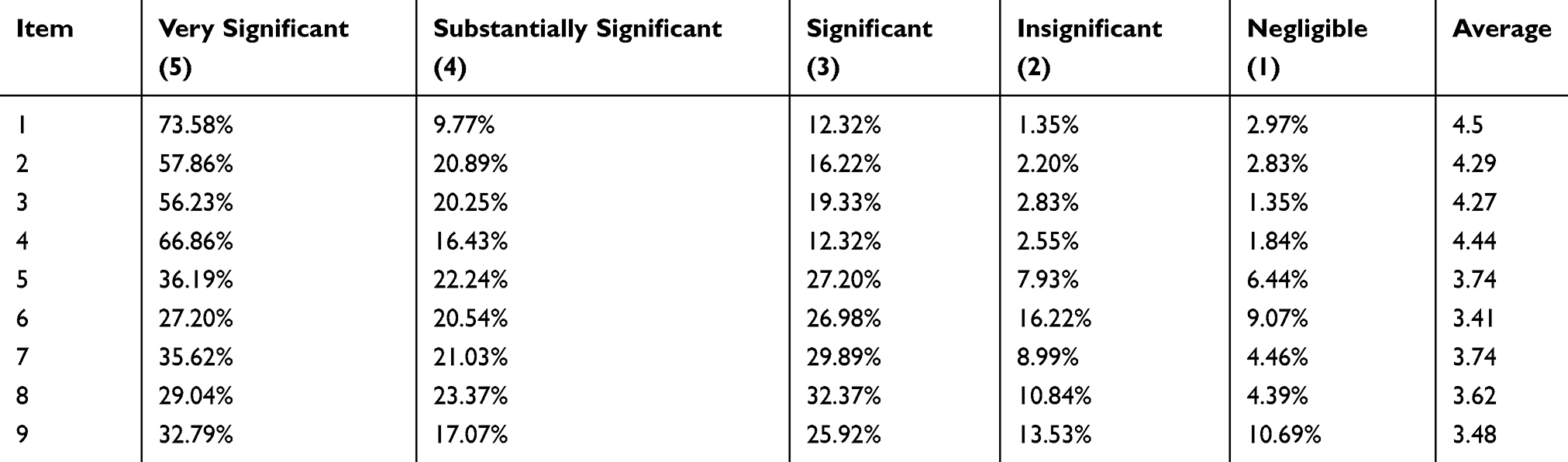 |
Table 4 Results for Individual Risk Factors in the Pharmacotherapy Process |
The analysis of results for particular risk factors in two occupational groups: nurses and midwives shows that nurses significantly more highly assess the importance of improper work organization (item 4) (Table 5).
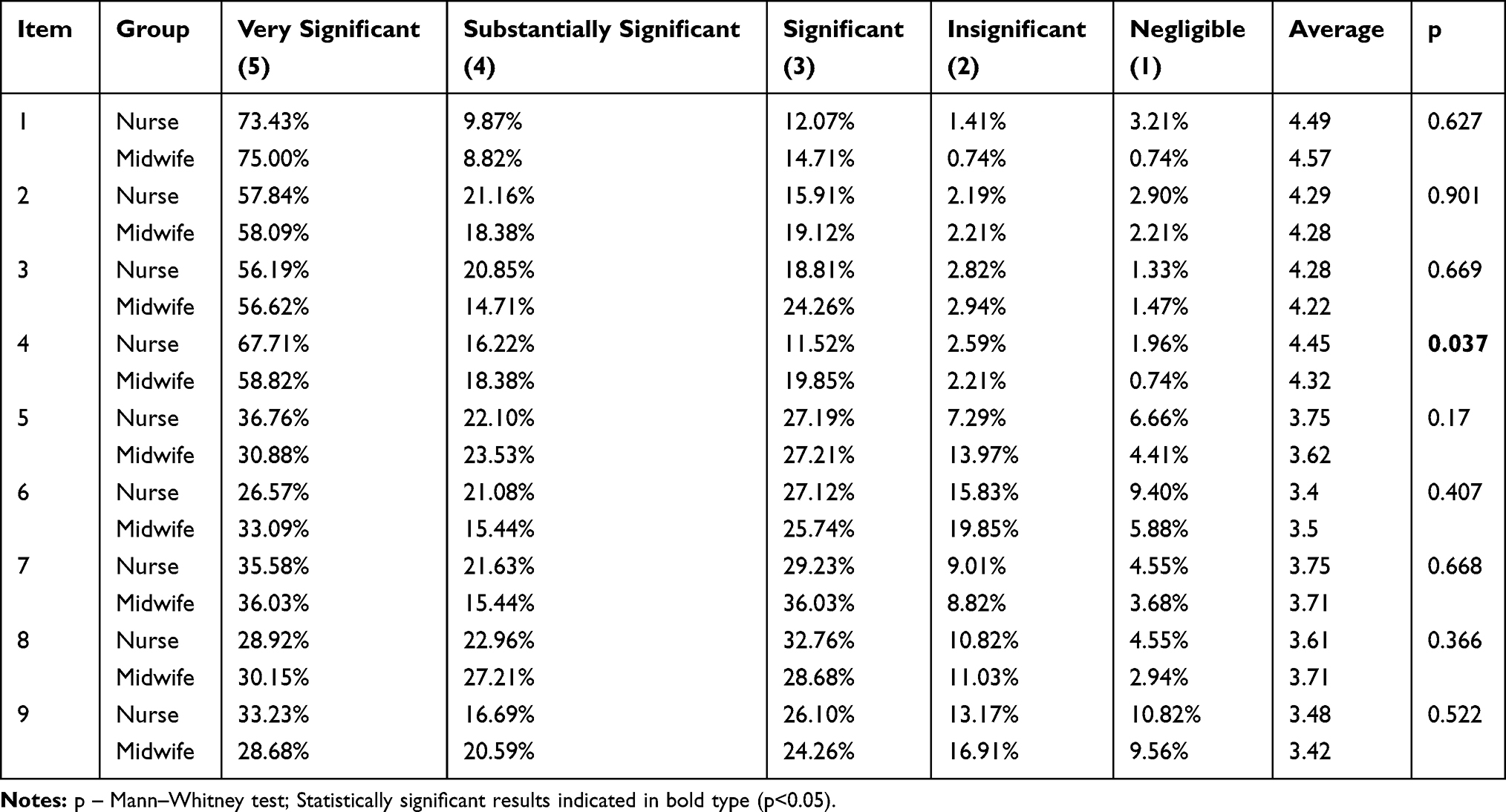 |
Table 5 Results for Individual Risk Factors in Pharmacotherapy in Nurses and Midwives |
The analysis also considered the impact of medication errors on nurses and midwives’ professional practice. It turned out that people who came into contact with medication errors rated the importance of improper communication and time pressure significantly higher (Items 2 and 3) (Table 6).
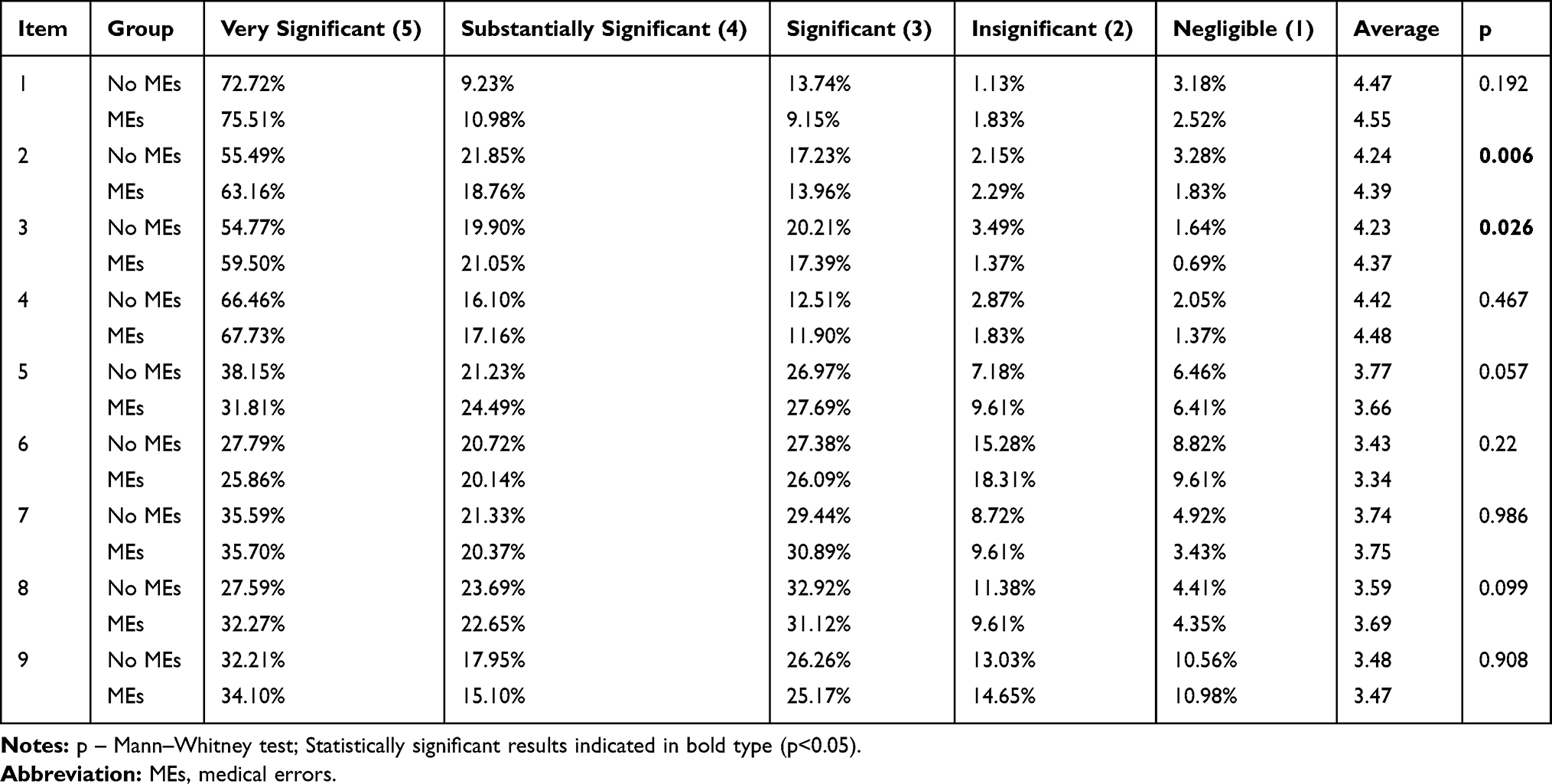 |
Table 6 Comparison of Results for Individual Risk Factors in Two Groups: A Group of People Who Experienced Medication Errors at Work and a Group of People Who Did Not Experience Medication Errors |
It should be stated that as many as four factors (items 1, 2, 3, and 4) reached the “significant” level (ie they reached the value of every 4 points on a five-degree scale) when analyzing the average values for individual risk factors. It means that it is similar that there are adverse health consequences for the patient resulting from medication errors, and it is also likely that the nurse/midwife is liable for the medication errors.
Discussion
Nowadays, in the health care system, great emphasis is placed on the broadly understood safety of the patient survives. For years now, we have been exploring quality and safety issues in health care, as evidenced by numerous publications and books. In 2019, on 17 September, we celebrated World Patient Safety Day for the first time. This action was initiated during The Third Global Ministerial Summit on Patient Safety, in 2018 in Japan, where 44 countries signed the Tokyo Declaration on Patient Safety. The Declaration commits all countries that have signed it to take action to improve patient safety, and the results are expected to be visible by 2030.17
Medication errors are among the most common errors that affect patients all over the world. One of the risk factors that was highly rated in the authors’ examination is the readability of medical orders – the average score was 4.5, which means that the significance of this factor is assessed between “very significant” and “significant.” At the moment in Poland, there is no obligation to conduct medical orders in electronic form; it is voluntary. The upcoming revolution in the digitization of medical records has been postponed, with the consequence that medical orders are still illegible — nurses and midwives involved in the pharmacotherapy process rate this as one of the most dangerous risk factors. Given the multitude of drugs that are very similar in name and used to treat completely different diseases, readability can be of great importance. In a life-threatening situation where seconds count, the inability of a nurse/midwife to read a physician’s order can have dramatic consequences for the patient. It would seem that one solution to this problem will be to keep medical records, within the scope of medical orders, in an electronic form.
In the study by Hartel et al,18 the errors in medical records related to medication errors were analyzed. The results of this study were worrying because of 43% of the patient cards contained at least one error. What is more, the legibility of handwriting was assessed as good, only in 2%, moderate in 42%, weak in 52%, and unreadable in 4%. It turns out that handwritten keeping of medical records, in particular, where its importance is at a premium, and any error can cost the patient his life, is very dangerous. Brits et al19 stress that in the United States alone each year 1.5 million patients suffer harm because of mistakes in the treatment process that was avoidable. Often these are errors resulting from illegible writing – unclear abbreviations and doses of medicines. This is an apparent premise for the introduction of electronic medical records, at least as far as the documentation of the pharmacovigilance process is concerned.
Another essential ergonomic factor that can trigger risks in the pharmacotherapy process is communication. In our study, inappropriate communication between a physician and a nurse/midwife was rated high, with a score above 4, which translates into a “significant” level and time pressure and inappropriate organization. These three factors are closely linked. Poor work organization can force staff to work under time pressure, which can translate into quality communication. Moreover, the study showed that nurses/midwives who experienced medication errors rate higher the importance of improper communication and time pressure in their work.
Many scientific reports are highlighting the importance of proper communication between a nurse and a physician. Soodabeh et al20 prove that the nurse-physician relationship is an aspect of the working environment that significantly affects the occurrence of errors in treatment. Another study by Sari21 shows that good information flow and processing have a significant impact on patient safety (such as good teamwork) and that an open and generative culture means better use of innovation and responding to danger signals.
Time pressure and medical card deficits can lead to fatigue among the staff. One study showed that during one 8-hour on-call time, one nurse working in the emergency room performed 50 clinical assessments of her competence. In anesthesiology and intensive care units, on the other hand, a nurse has to make a clinical decision every 30 seconds – this is due to the unit’s profile and the patients staying there.22,23
Factors triggering risk in administering medicines that are in contact with medical workers also include lack of experience of the personnel, multi-tasking, interruption of work during the task, fatigue, boredom, and lack of vigilance;24,25 as well as improper resting and poor quality of sleep.26
In the own study, shift work as a risk factor was assessed as “very significant” only by 35.62% of respondents, reaching the average value of 3.74, which corresponds to the level of “significant.” It would seem that work, especially at night when fatigue levels reach their maximum due to the internal biological clock, will be one of the top factors chosen by nurses and midwives. A review of the literature shows that shift work, including night work, has been a risk factor for the safety of medical processes. The study by Tanaka et al27 has shown that shorter breaks after night shifts and higher frequency of night shifts in three-shift systems, which shorten the time of return to work after night shifts, may be associated with increased medical errors the part of nurses.
Patient safety is becoming a top priority for healthcare managers today. However, our results and the literature review indicate that the problem of pharmacovigilance is worldwide.
So far, no tool exists to quickly identify weaknesses in the pharmacotherapy process in-hospital care, where the incidence of medication errors. Therefore, we hope that the risk matrix presented in this study will allow us to identify weak points and implement preventive measures in hospitals and consequently to improve patient safety. Also, comprehensive interventions containing organizational, technological, educational, and process optimization-based evaluations are needed to be implemented.28,29
Study Limitations
Based on the survey and the analysis of the results, the data collection method should be approached critically. The use of electronic survey available at the link is undoubtedly a very convenient solution – on the one hand, it allows us to quickly reach people who live on the other side of the country and quickly aggregates collected data, which saves time for entering data and reduces the risk of error during this process. On the other hand, this solution raises concerns among the respondents, namely whether this method is entirely anonymous. It was found that a significant proportion of the respondents did not complete their investigation, ie, did not send a reply to the server because they were afraid that it could be identified. The study was fully anonymous, did not collect the names of facilities where the subjects worked but contained questions about the occurrence of an adverse event during the pharmacotherapy process. It turns out that the fear of penalization among nurses and midwives is high – the respondents were afraid that based on an electronic questionnaire, it was possible to identify the hospital where the adverse event occurred. The selection of the data acquisition methodology must be appropriately selected, considering the questions that are included in the tool. In this case, the traditional form of data collection – in the form of a paper survey – could contribute to the increased manoeuvrability of the surveys. On the other hand, the use of the traditional method of data collection could take much longer and delay the study.
Practical Implications
Based on the results of this study, it should be noted that the proprietary NURIPH tool can be used to identify risk factors in the pharmacotherapy process in hospitals worldwide. A diagnosis based on the results obtained can contribute to the development of new procedures, the improvement of the patient’s quality and safety, and preventive action. It should be concluded that the NURIPH can be a universal tool for the rapid diagnosis of inpatient medicine risks worldwide. Moreover, training for nurses and midwives in the field of patient safety and medical staff should be promoted and implemented in hospitals. Low staff awareness negatively affects the safety of the services provided.
Conclusions
Nurses and midwives involved in the pharmacotherapy process are exposed to many ergonomic factors triggering risk in this process. A huge problem is the lack of readability of medical orders, which may be a factor triggering a medication error. Also, poor workplace organization, lack of space to prepare medicines, poor communication, or hurry and fatigue generate risks that can also trigger medication errors. This translates into a level of patient safety that is not sufficiently protected. Most adverse drug-related events result from poor quality and safety management systems and processes, not from individual mistakes.
In conclusion, it is essential to search for new techniques and tools that improve the pharmacovigilance process to identify potential risks and preventable errors and then implement system-related changes. Since many factors favor the possibility of medication errors (factors related to workplace organization, staff, drug characteristics – sound-alike, look-alike), medical and managing staff should identify, monitor, and minimize risk factors in the pharmacotherapy process.
Abbreviations
NCCMERP, National Coordinating Council for Medication Error Reporting and Prevention; NURIPH, Nursing Risk in Pharmacotherapy; RM, registered midwives; RN, registered nurse; WHO, World Health Organization.
Acknowledgments
There were no other contributors to the article than the authors as well as there was no writing assistance regarding our paper. The certified English language services were provided.
Funding
This study was conducted under a research project funded by the Ministry of Science and Higher Education of Poland as a statutory grant of the Wroclaw Medical University for maintaining research potential (no. SUB.E140.19.042).
Disclosure
No conflict of interest has been declared by the authors.
References
1. Berdot S, Roudot M, Schramm C, Katsahian S, Durieux P, Sabatier B. Interventions to reduce nurses’ medication administration errors in inpatient settings: a systematic review and meta-analysis. Int J Nurs Stud. 2016;53:342–350. doi:10.1016/j.ijnurstu.2015.08.012
2. Fathi A, Hajizadeh M, Moradi K, et al. Medication errors among nurses in teaching hospitals in the west of Iran: what we need to know about prevalence, types, and barriers to reporting. Epidemiol Health. 2017;39:e2017022. doi:10.4178/epih.e2017022
3. World Health Organization. Medication errors: technical series on safer primary care; 2016. Available from: https://www.who.int/patientsafety/topics/primary-care/technical_series/en/.
4. World Health Organization. Medication Safety. Curriculum Guide. World Health Organization; 2019. Available from: https://www.pharmacologyeducation.org/sites/default/files/WHO%20Medication%20Safety%20Curriculum%20Guide%202019.pdf.
5. Kavanagh C. Medication governance: preventing errors and promoting patient safety. Br J Nurs. 2017;26(3):159–165. doi:10.12968/bjon.2017.26.3.159
6. Renata Grou Volpe C, Moura Pinho DL, Morato Stival M, Gomes de Oliveira Karnikowski M. Medication errors in a public hospital in Brazil. Br J Nurs. 2014;23(11):552–559. doi:10.12968/bjon.2014.23.11.552
7. Aronson JK. Medication errors: what they are, how they happen, and how to avoid them. QJM. 2009;102(8):513–521. doi:10.1093/qjmed/hcp052
8. Hewitt P. Nurses’ perceptions of the causes of medication errors: an integrative literature review. Medsurg Nurs. 2010;19(3):159–167.
9. Institute of Medicine C on the RWJFI on the F of N. Transforming Practice. The Future of Nursing: Leading Change, Advancing Health. National Academies Press (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209871/.
10. Parry AM, Barriball KL, While AE. Factors contributing to registered nurse medication administration error: a narrative review. Int J Nurs Stud. 2015;52(1):403–420. doi:10.1016/j.ijnurstu.2014.07.003
11. Vrbnjak D, Denieffe S, O’Gorman C, Pajnkihar M. Barriers to reporting medication errors and near misses among nurses: a systematic review. Int J Nurs Stud. 2016;63:162–178. doi:10.1016/j.ijnurstu.2016.08.019
12. Walsh EK, Hansen CR, Sahm LJ, Kearney PM, Doherty E, Bradley CP. Economic impact of medication error: a systematic review. Pharmacoepidemiol Drug Saf. 2017;26(5):481–497. doi:10.1002/pds.4188
13. Karimian Z, Kheirandish M, Javidnikou N, Asghari G, Ahmadizar F, Dinarvand R. Medication errors associated with adverse drug reactions in Iran (2015-2017): a P-method approach. Int J Health Policy Manag. 2018;7(12):1090–1096. doi:10.15171/ijhpm.2018.91
14. Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny M-P, Sheikh A. Medication without harm: WHO’s third global patient safety challenge. Lancet. 2017;389(10080):1680–1681. doi:10.1016/S0140-6736(17)31047-4
15. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053.
16. R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing.; 2019. https://www.R-project.org/.
17. Flott K, Durkin M, Darzi A. The Tokyo Declaration on patient safety. BMJ. 2018;362:k3424. doi:10.1136/bmj.k3424
18. Hartel MJ, Staub LP, Röder C, Eggli S. High incidence of medication documentation errors in a Swiss university hospital due to the handwritten prescription process. BMC Health Serv Res. 2011;11:199. doi:10.1186/1472-6963-11-199
19. Brits H, Botha A, Niksch L, Terblanché R, Venter K, Joubert G. Illegible handwriting and other prescription errors on prescriptions at National District Hospital, Bloemfontein. South Afr Fam Pract. 2017;59(1):52–55. doi:10.1080/20786190.2016.1254932
20. Soodabeh J, Mahboobeh S, Abbas H, Sara R, Hamid H. The relationship between medication errors and nurses’ work environment. Med Surg Nurs J. 2016;4(4):30–39.
21. Sari AA. Assessing patient safety culture in the hospital: a pilot study using a modified Manchester Patient Safety Framework (MaPSaF). JMMR. 2017;6(3):159–168. doi:10.18196/jmmr.6141
22. Seki Y. Working condition factors associated with time pressure of nurses in Japanese hospitals. J Occup Health. 2008;50(2):181–190. doi:10.1539/joh.l7031
23. Thompson C, Dalgleish L, Bucknall T, et al. The effects of time pressure and experience on nurses’ risk assessment decisions: a signal detection analysis. Nurs Res. 2008;57(5):302–311. doi:10.1097/01.NNR.0000313504.37970.f9
24. World Health Organization. Patient Safety Curriculum Guide: Multi-Professional Edition.; 2011.
25. Di Simone E, Di Muzio M, Dionisi S, et al. Infodemiological patterns in searching medication errors: relationship with risk management and shift work. Eur Rev Med Pharmacol Sci. 2019;23(12):5522–5529. doi:10.26355/eurrev_201906_18224
26. Di Simone E, Fabbian F, Giannetta N, et al. Risk of medication errors and nurses’ quality of sleep: a national cross-sectional web survey study. Eur Rev Med Pharmacol Sci. 2020;24(12):7058–7062. doi:10.26355/eurrev_202006_21699
27. Tanaka K, Takahashi M, Hiro H, et al. Differences in medical error risk among nurses working two- and three-shift systems at teaching hospitals: a six-month prospective study. Ind Health. 2010;48(3):357–364. doi:10.2486/indhealth.48.357
28. Wang H-F, Jin J-F, Feng X-Q, et al. Quality improvements in decreasing medication administration errors made by nursing staff in an academic medical center hospital: a trend analysis during the journey to Joint Commission International accreditation and in the post-accreditation era. Ther Clin Risk Manag. 2015;11:393–406. doi:10.2147/TCRM.S79238
29. Chapuis C, Chanoine S, Colombet L, et al. Interprofessional safety reporting and review of adverse events and medication errors in critical care. Ther Clin Risk Manag. 2019;15:549–556. doi:10.2147/TCRM.S188185
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.