Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
Safety and Microvascular Effect of Four-Year Aminaphtone Administration in Systemic Sclerosis Patients
Authors Campitiello R, Sulli A, Hysa E, Pizzorni C, Cutolo M, Paolino S, Gotelli E
Received 12 April 2026
Accepted for publication 19 June 2026
Published 9 July 2026 Volume 2026:18 613596
DOI https://doi.org/10.2147/OARRR.S613596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Rosanna Campitiello,1,2,* Alberto Sulli,1,3,* Elvis Hysa,1,2 Carmen Pizzorni,1,3 Maurizio Cutolo,1,3 Sabrina Paolino,1,3,* Emanuele Gotelli1,3,*
1Laboratory of Experimental Rheumatology and Academic Division of Clinical Rheumatology, Department of Internal Medicine and Medical Specialties, University of Genova, Genova, Italy; 2Department of Experimental Medicine, University of Genova, Genova, Italy; 3IRCCS AOM Ospedale Policlinico San Martino, Department of Internal Medicine and Medical Specialties, Genova, Italy
*These authors contributed equally to this work
Correspondence: Maurizio Cutolo, Department of Internal Medicine and Medical Specialties, University of Genova, Viale Benedetto XV, 6, Genoa, 16132, Italy, Email [email protected]
Background: Endothelial and microvascular damage is a hallmark of systemic sclerosis (SSc), an autoimmune connective tissue disease characterized by progressive skin and organ fibrosis. Aminaphtone (3-Methyl-1,4-dioxo-1,4-dihydro-naphthalen-2-yl-amino-benzoate) is a synthetic molecule used to treat microvascular disorders. Nailfold videocapillaroscopy (NVC) is the most reliable non-invasive method for assessing microvascular status and disease progression in SSc patients.
Aim: To evaluate long-term safety and potential beneficial effects of aminaphtone on microcirculation in SSc.
Methods: Seventy-six SSc patients (68 females, 8 males; mean age 69 ± 15 years) fulfilling the 2013 ACR/EULAR criteria and presenting Raynaud’s phenomenon received aminaphtone (75 mg twice daily) in addition to stable standard therapy (ST). Forty age- and sex-matched SSc patients treated with ST alone served as controls. Side effects were monitored every six months. NVC was performed at baseline and after 1 and 4 years, using the Cutolo classification (“Early”, “Active”, “Late” patterns) to evaluate microvascular damage progression.
Results: Aminaphtone showed a high long-term retention rate (89.5%) over four years. Eight of 76 patients (10.5%) discontinued treatment due to mild transient intolerance or poor compliance; no serious adverse events were reported. NVC patterns remained stable in 91% of treated patients. Compared with controls, aminaphtone-treated patients showed a slower transition from “Active” to “Late” NVC pattern (120 ± 64 vs 50 ± 26 months, p = 0.05). Linear mixed-effects modelling showed a significantly slower capillary density decline in the aminaphtone group over 48 months (p < 0.05) in both “Early” and “Active” scleroderma pattern subgroups. On multivariate linear regression, this effect was independent of age, disease phenotype, and concomitant therapies.
Conclusion: Aminaphtone appears safe and well tolerated during long-term treatment in SSc patients with secondary Raynaud’s phenomenon. The stability of NVC scleroderma patterns and the independent protective effect on capillary loss suggest a potential adjunctive role of aminaphtone in limiting microvascular damage progression when added to ST in SSc.
Keywords: Raynaud’s phenomenon, systemic sclerosis, aminaphtone, capillaroscopy, microcirculation
Introduction
Systemic sclerosis (SSc) is a connective tissue autoimmune disease characterized by early and progressive microvascular impairments, immune system dysregulation, and a widespread fibrosis of the skin and of the internal organs.1,2
Raynaud’s phenomenon (RP) is a digital vasospasm with classic triphasic expression (ischaemic phase, cyanotic phase, and reactive hyperemic phases) commonly triggered by exposure to cold or emotional stressors which may be related to a functional regulatory response (primary RP) or underlying a broad range of medical conditions and rheumatologic disorders including SSc (secondary RP).2,3
The most frequent and earliest symptom of SSc microvascular damage is indeed RP, that is reported in up to 96% of patients.4–6 Aminaphtone (3-Methyl-1,4-dioxo-1,4-dihydro-naphthalen-2-yl 4-amino-benzoate) is a chemical compound (C18H15NO4) commercialized by Baldacci in Italy, Brazil, and Portugal. It has been used for over 40 years as an endothelial protector, indicated for reducing vascular leakage in capillary disorders, as well as for the treatment of chronic peripheral venous insufficiency.7 The beneficial effect of aminaphtone on endothelium has been demonstrated in both clinical and pre-clinical evidence concerning especially the endothelin production.8,9
Endothelin (ET) is a 21-amino-acid peptide produced by endothelial cells, smooth muscle cells, and macrophages. It is synthesized as pre-pro-endothelin-1 (PPET-1), which is cleaved into inactive big endothelin and then converted into active endothelin by endothelin-converting enzymes. Three isoforms exist (ET-1, ET-2, ET-3), with ET-1 being the most biologically active and clinically important. Endothelin acts through two G-protein-coupled receptors: ET-A and ET-B. Of note, ET-A receptor, mainly on vascular smooth muscle cells, mediate vasoconstriction and cell proliferation, while ET-B receptors, primarily on endothelial cells, promote vasodilation. Moreover, ET-A has high affinity for ET-1 and is strongly linked to pathological vasoconstrictive and proliferative effects.10 In-vitro pre-clinical studies showed how aminaphtone downregulates ET-1 production in ECV304 cell cultures by interfering with transcription of preproET-1 (PPET-1) gene expression in a dose-dependent manner.11 An in vitro study investigated the effects of aminaphtone on whole-genome gene expression and the production of inflammatory proteins. Microarray analysis showed a significant downregulation of a broad range of inflammatory genes. Furthermore, extended secretome analysis demonstrated a marked reduction in the release of 14 cytokines and chemokines, including TGF-β (Transforming Growth Factor beta) and VEGF (Vascular Endothelial Growth Factor), suggesting potential anti-inflammatory and vascular-modulating effects of the drug.12
The evidence of pre-clinical studies led to a growing body of spontaneous clinical reports supporting the use of aminaphtone in various clinical conditions, such as diabetic nephropathy, minor bleeding disorders, idiopathic cyclic edema syndrome, and Raynaud’s phenomenon, both primary and secondary to systemic sclerosis.6,13–16
In 2008, an open-label pilot study enrolled 24 patients with RP secondary to SSc. This cohort of patients was treated with aminaphtone 75 mg TID in addition to their standard therapy.
Results showed a reduction of the soluble adhesion molecule (E-selectin adhesion molecule 1) and vascular cell adhesion molecule 1 after 12 weeks of treatment.11 Of note, after almost 10 years aminaphtone efficacy in ameliorating microvascular function has been evaluated in patients affected by both in primary RP and in secondary RP to SSc showing improvement in peripheral blood perfusion along with a reduction in RP clinical symptoms.6 To date, RP is managed mainly with lifestyle measures and drugs. Patients are advised to avoid cold exposure, reduce caffeine intake, and stop smoking. First-line pharmacological treatment includes calcium channel blockers (eg, nifedipine), and in more severe cases intravenous prostanoids can be used, but they are often poorly tolerated due to side effects.
Other options for resistant cases include phosphodiesterase-5 inhibitors, topical nitrates, and, rarely, surgical or interventional procedures.16 In SSc-related Raynaud’s phenomenon, immunosuppressive therapy may be considered depending on the severity and extent of internal organ involvement; nevertheless, these more aggressive treatments are associated with a significant risk of adverse effects (eg: hypotension, headache, and nausea), which limits their use and requires careful patient selection and close monitoring.17,18 In this context, aminaphtone may be used in addition to standard therapy (ST) in the treatment of secondary RP. Microvascular damage associated with SSc is recognized as a key pathogenic feature of SSc since very early stage of disease, which can be assessed using nailfold videocapillaroscopy (NVC).19,20
Indeed, NVC is a safe, non-invasive tool able to detect morphological structure of peripheral capillaries evaluated at the periungual bed of the hands. NVC allows physicians to assess specific patterns related to disease progression.21
The present study mainly aimed to assess during a four-year treatment period with aminaphtone extended with a five-year long-term follow-up, the safety and its effect on nailfold capillaroscopy, combined with standard therapy, in a cohort of SSc patients versus aminaphtone-untreated patients.
Materials and Methods
Study Population
Seventy-six SSc Caucasian patients (68 females and 8 males, mean age 69 ± 15 years) (according to the 2013 EULAR/ACR criteria) with secondary Raynaud’s phenomenon (RP) started aminaphtone treatment for the management of the microvascular symptoms (Table 1).17
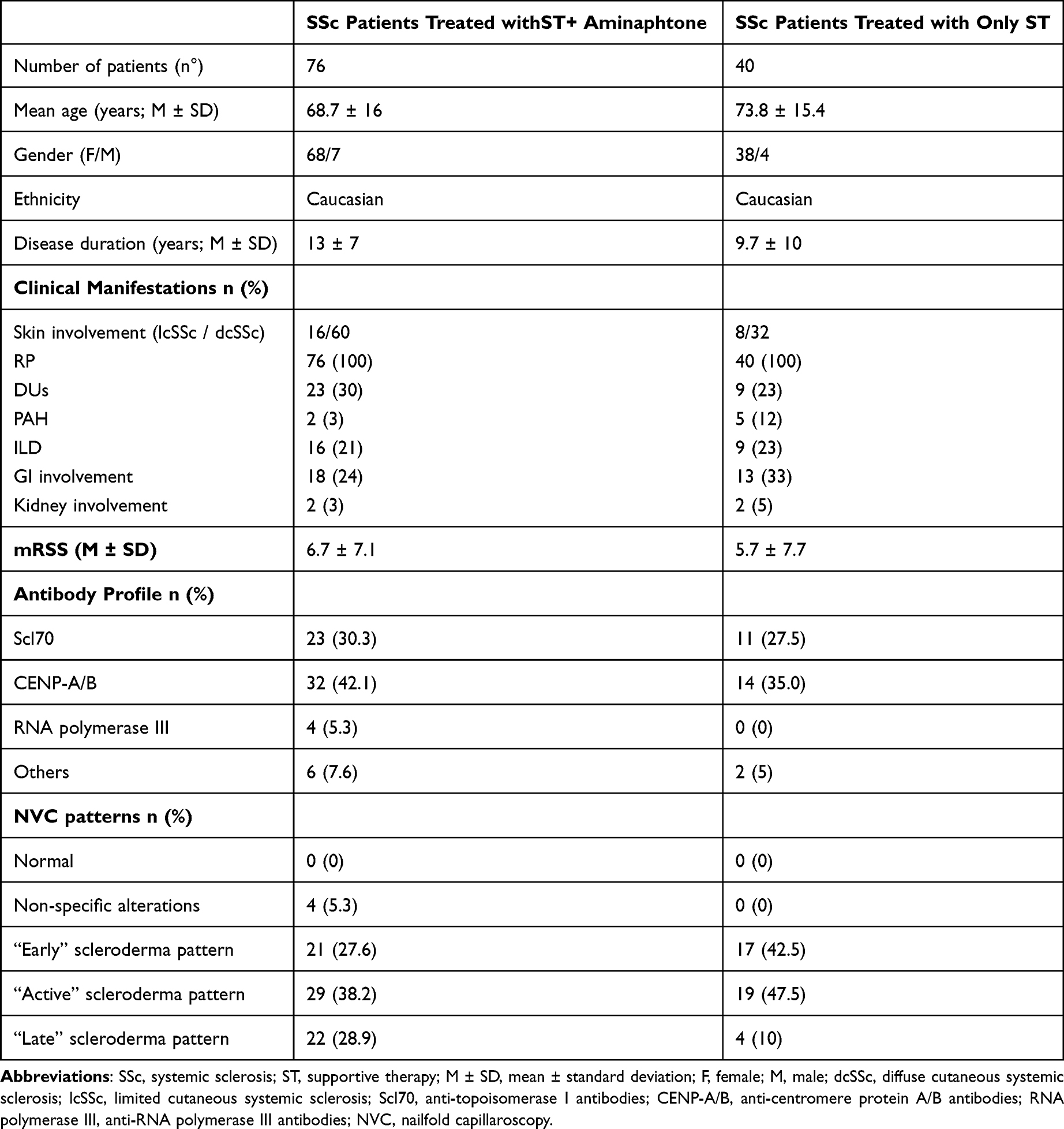 |
Table 1 Baseline Clinical, Demographic, and Laboratory Characteristics of SSc Patients |
The posology (75 mg, 1 tablet twice a day every 12 hours) was consistent with the dosage recommended in the drug’s official prescribing information. This long-term, four-year, retrospective, observational monocentric study based on the routine therapies and physical analyses was conducted at Clinical Rheumatology, Department of Internal Medicine, University of Genova, IRCCS AOM Ospedale Policlinico San Martino, Genova, Italy. The study was conducted in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki, following approval from the Ethics Committee of the Ospedale Policlinico San Martino (N. CET – Liguria: 16/2025 – id 14273-22/04/2025), and each patient provided informed consent for retrospective utilization of anonymized clinical data for research purposes (CONSAZQA_0001).
All patients were volunteers and did not receive any form of compensation for their involvement in the study. All patients at our Rheumatology Centre who initiated aminaphtone and fulfilled the inclusion criteria were enrolled; no patient was excluded on clinical grounds, corresponding to a 100% inclusion rate. Clinical data including disease onset, organ involvement, autoantibody profile, and concomitant therapy have been collected from medical records and stored in a dedicated database. Tight monitoring was performed, including vital signs measurements, complete blood counts, and assessments of renal and hepatic function, at baseline and at least every six months. Based on available clinical evidence, at our Rheumatology Center aminaphtone is used as a symptomatic treatment for Raynaud’s phenomenon (RP), particularly in systemic sclerosis (SSc)-related RP, from disease onset, either as monotherapy in primary RP, or as an adjunct to standard therapy in secondary RP. Patients received ST regimens according to organ involvement and disease severity, including intravenous prostanoids, phosphodiesterase-5 (PDE5) inhibitors, endothelin receptor antagonists, and immunosuppressive agents, in line with the EULAR recommendations for the management of SSc (Table 2).18 In this real-life setting, a control group comprising 40 SSc patients, who did not receive aminaphtone but was treated with the same ST as aminaphtone treated patients alone, was enrolled to evaluate comparative timings in capillaroscopic pattern transitions. This cohort was matched by age, gender, and ethnicity. Notably, despite the observational nature of the study, the control group was specifically enrolled to compare the timing of capillaroscopic SSc-pattern transitions, ensuring that there were no statistically significant differences regarding the baseline ST between the two groups.
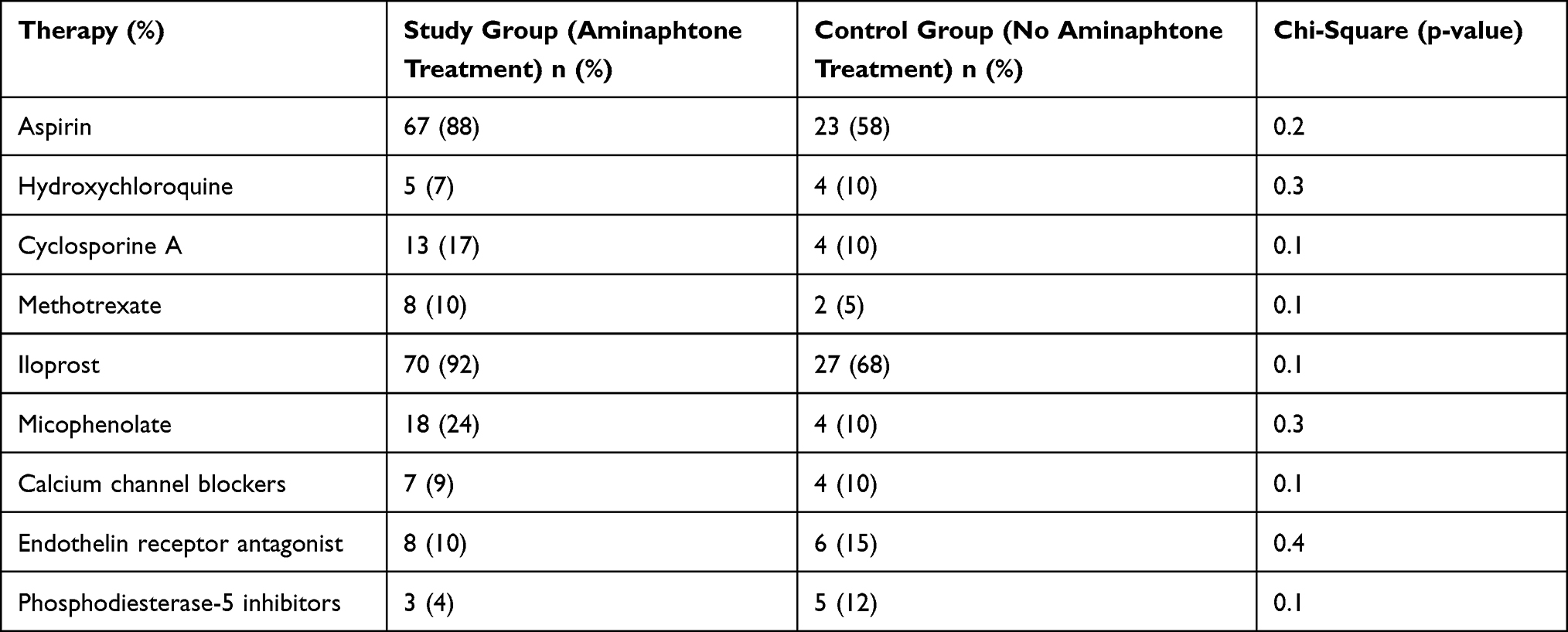 |
Table 2 Ongoing Therapies of SSc Patients |
Nailfold Videocapillaroscopy
All patients, after an acclimatization period of 20 min at 22–24°C, according to the standardised procedures, underwent NVC evaluation using an optical probe, equipped with a 200× contact lens connected to image analysis software (Videocap, DS Medica, Milan, Italy). For each subject, two images of the middle region of the nailfold bed (excluding the thumbs) were acquired, along with the following NVC parameters: dilated capillaries (capillary diameter increased to 20–50 µm), giant capillaries (uniformly dilated capillaries with a diameter ≥50 µm), microhaemorrhages (dark deposits indicative of hemosiderin accumulation), neoangiogenesis (abnormal shapes), and the absolute capillary count per linear millimeter (normal density defined as ≥7 capillaries).19 A validated algorithm was used to differentiate “non-scleroderma” patterns from “scleroderma” patterns.20 Severity of microangiopathy was reported according to the Cutolo et al SSc-pattern of microvascular damage (“Early”, “Active”, or “Late” NVC patterns).19 Comparative analysis between the treatment and control groups was specifically focused on patients presenting with “Early” and “Active” scleroderma patterns at baseline. Patients with a “Late” NVC scleroderma pattern were present in both cohorts but, by definition, have limited further capacity for measurable NVC progression (capillary density is already extensively reduced), and their inclusion in the transition-timing analysis would have introduced a relevant confounding factor.
The transition timing was calculated retrospectively, measuring the interval from the initial documentation of an “Early” or “Active” scleroderma pattern at NVC to the first evidence of progression. The NVC images were collected and evaluated. Data were collected retrospectively, and two independent raters (CP and RC) performed the analyses, both blinded to group allocation of enrolled patients.
Statistical Analysis
Statistical analyses were performed using DataTab (DataTab Team, Graz, Austria) and R (R Foundation for Statistical Computing, Vienna, Austria), with the normality of continuous variables assessed to determine the selection between parametric and non-parametric tests. Continuous variables are expressed as mean ± standard deviation (M ± SD) and categorical variables as frequencies or percentages. To ensure cohort matching, baseline demographic and clinical characteristics were compared between the study group receiving aminaphtone plus standard therapy (ST) and the control group receiving ST alone. The chi-square test was used to evaluate differences in categorical data. Furthermore, the timing of transition between SSc-patterns, specifically from “Early” to “Active” and “Active” to “Late”, was analyzed using the Mann–Whitney U-test for independent samples. For all conducted analyses, statistical significance was defined by a p-value <0.05. To evaluate longitudinal changes in capillary density over a four-year period, a linear mixed-effects model was employed. To assess changes over time and differences between groups, a linear mixed-effects model (LMM) was applied. Fixed effects included time (T0 vs T4), group (treated vs control). To account for within-subject correlation due to repeated measurements, a random intercept for each subject was included. The model was estimated using restricted maximum likelihood, and degrees of freedom were approximated using the Satterthwaite method. Post-hoc comparisons were conducted using estimated marginal means to evaluate differences over time within each group and between groups at each time point. To assess the independent effect of aminaphtone on capillary density change over 48 months, two multiple linear regression models were performed separately in patients with Early and Active NVC pattern at baseline, with treatment group as the primary predictor and age, disease subset (lcSSc vs dcSSc), and concomitant therapy (Table 1) as covariates.
Results
Study Population
Seventy-six patients with systemic sclerosis (SSc) treated with ST plus aminaphtone were compared with 40 patients treated with ST alone (Table 1). The mean age was 68.7 ± 16 years in the combination therapy group and 73.8 ± 15.4 years in the ST-only group. The female-to-male ratio was 68/7 and 38/4, respectively. All patients in both groups were Caucasian. Disease duration was longer in the ST+aminaphtone group (13 ± 7 years) compared to the ST-only group (9.7 ± 10 years). Regarding clinical manifestations, limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc) were distributed as 16/60 in the ST+aminaphtone group and 8/32 in the ST-only group. Raynaud’s phenomenon was present in all patients (100% in both groups). Digital ulcers were observed in 30% of patients in the combination group and 23% in the ST-only group. Pulmonary arterial hypertension was present in 3% vs 12%, interstitial lung disease in 21% vs 23%, gastrointestinal involvement in 24% vs 33%, and renal involvement in 3% vs 5%, respectively. Mean modified Rodnan skin score (mRSS) was 6.7 ± 7.1 in the ST+aminaphtone group and 5.7 ± 7.7 in the ST group. Autoantibody profiles were similar between groups, with anti-Scl70 positivity in 30.3% vs 27.5%, anti-centromere antibodies in 42.1% vs 35.0%, anti-RNA polymerase III in 5.3% vs 0%, and other antibodies in 7.6% vs 5%, respectively. Nailfold videocapillaroscopy patterns showed a predominance of active and early scleroderma patterns in both groups. In the ST+aminaphtone group, 27.6% had an early pattern, 38.2% active, and 28.9% late pattern, while in the ST-only group the distribution was 42.5%, 47.5%, and 10%, respectively; non-specific alterations were observed only in the combination group (5.3%), and no normal patterns were reported in either group (Table 1). All patients were treated with the ST according to the EULAR recommendations, and none of the included patients were treated with amainaphtone in monotherapy (Table 2).
Safety and Tolerability
During the four years of treatment with aminaphtone no life-threatening side effects were reported in our cohort of SSc patients. Overall, 8 out of 76 patients discontinued therapy, corresponding to a discontinuation rate of 10.5% due to mild intolerance attributed to already signaled adverse events and a treatment retention rate of 89.5% over the observation period. Specifically, 2.7% of patients reported headaches, 1.3% experienced itching, while an additional 6% discontinued treatment due to poor compliance despite not experiencing any side effects, which represented the main cause of discontinuation in this subgroup.
It is important to further underline that these adverse events occurred shortly after the initial administrations and resolved promptly upon discontinuation of the treatment, without leaving any lasting sequelae. Overall, the treatment demonstrated a high long-term retention rate of 90%, confirming that aminaphtone is well-tolerated and manageable for the majority of SSc patients over a four-year period. These findings underscore the critical need for vigilant monitoring, particularly during the initial administrations of aminaphtone, to detect any potential side effects.
Microvascular Evaluation
The timing of transition from “Early” to “Active” scleroderma pattern at NVC analysis and “Active” to “Late” scleroderma pattern was evaluated (Figure 1).
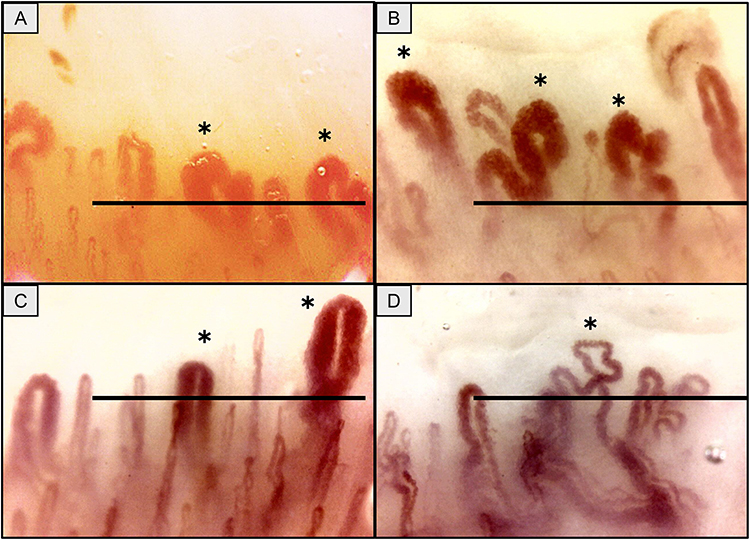 |
Figure 1 Nailfold videocapillaroscopy pictures of SSc patients during five years of follow-up (patterns according to Cutolo et al10,22. (A) “Active” scleroderma pattern observed at baseline in SSc patient prior to treatment with aminaphtone in addition to ST. Giant capillaries highlighted by asterisks (*), microhaemorrhages, capillary loss (5 capillaries per linear mm) and abnormal shapes are present. (B) “Active” scleroderma pattern after 4 years of follow-up. Giant capillaries highlighted by asterisks (*), microhaemorrhages, capillary loss (5 capillaries per linear mm) and abnormal shapes are present. (C) “Active” scleroderma pattern observed at baseline in SSc patient treated only with ST. Giant capillaries highlighted by asterisks (*), capillary loss (5 capillaries per linear mm) and no abnormal shapes. (D) “Late” scleroderma pattern in SSc patient observed after 4 years of follow-up treated only with ST. No giant capillaries, capillary loss (2 capillaries per linear mm) and one abnormal shape highlighted by asterisk (*). In each image, the black horizontal line represents a linear millimetre. Magnification ×200. Original images from MC and Genova Team, Laboratory of Experimental Rheumatology and Academic Clinical Division at University of Genova. |
Regarding baseline microvascular status, the aminaphtone group presented with “Early” 27.6%, “Active” 38.2%, and “Late” 28.9% NVC sclerodema pattern, while the control group showed a distribution of “Early” 42.5%, “Active” 47.5%, and “Late” 10% pattern.
Notably, the NVC pattern remained stable in 91% (n = 69) of the aminaphtone-treated patients throughout the observation period (4 years). Progression of NVC pattern was limited to a marginal subset: 6.6% transitioning from “Early” to “Active” and 3.4% from “Active” to “Late” scleroderma pattern.
The treatment group exhibited a significant trend toward a slower transition from the “Active” to the “Late” scleroderma pattern compared to the control group (120 ± 64 months vs 50 ± 26 months, p = 0.05).
Conversely, transition times from “Early” to “Active” NVC patterns remained similar between both groups (36 ± 30 months vs 36 ± 42 months; p > 0.05). These findings, observed under consistent therapeutic backgrounds with no significant differences in baseline ST, suggest that aminaphtone may delay the progressive microvascular damage observed at NVC.
In patients with “Early” scleroderma pattern the linear mixed-effects model revealed a significant main effect of time on capillary density (F(1, 27.77) = 33.74, p < 0.001), indicating an overall reduction over time (Figure 2 and Table 3).
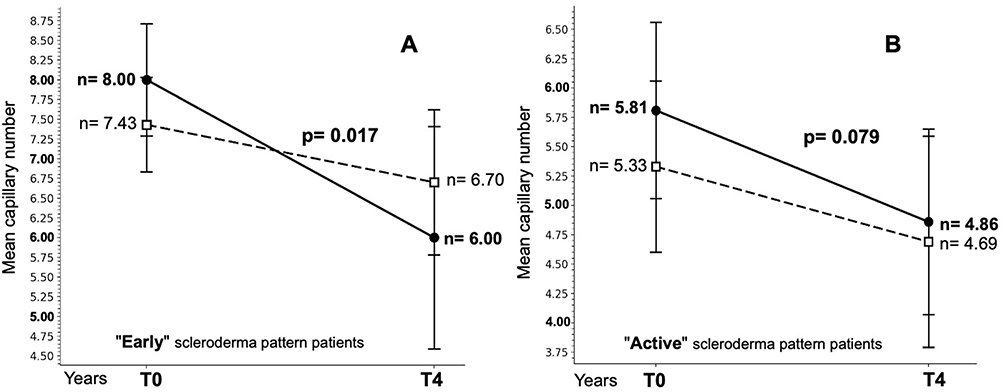 |
Figure 2 Longitudinal analysis of capillary density over 4 years of follow-up. (A) Patients with SSc showing an “Early” scleroderma pattern, comparing aminaphtone-treated vs untreated (only standard therapy (ST)). (B) Patients with SSc showing an “Active” scleroderma pattern, comparing aminaphtone-treated vs untreated (only ST). The continuous line represents the only ST group, while the dashed line represents the ST + aminaphtone group. Data are presented as mean capillary number (n) ± standard deviation (SD). |
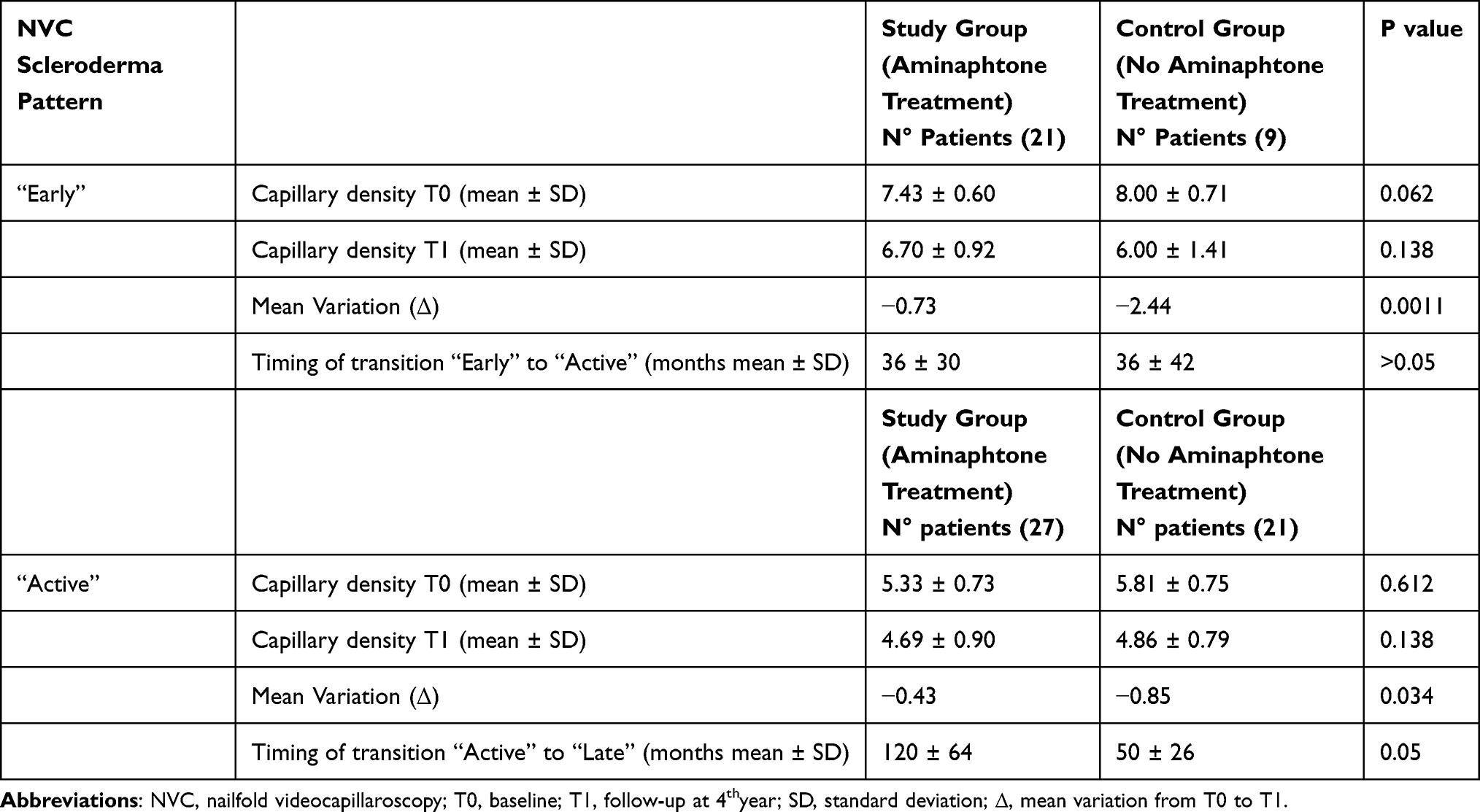 |
Table 3 Effect of Aminaphtone Treatment on Capillary Density During a 4-Year Follow-Up and Timing of NVC Pattern Transition in SSc Patients Treated with Aminaphtone in Addition to Standard Therapy vs Treated with Standard Therapy Alone |
Importantly, a significant interaction between time and group was detected (F(1, 27.77) = 7.28, p = 0.0117), indicating that the change in capillary density over time differed between the two groups. At baseline (T0), no significant differences were found between groups (p = 0.11). At T4, a trend toward higher capillary density was reported in the treated group compared to controls, although this did not reach statistical significance (p = 0.055). Post-hoc analysis showed that in the control group, capillary density significantly decreased from T0 to T4 (mean difference = −2.00; p < 0.0001). A significant but smaller reduction was also observed in the treated group (mean difference = −0.73; p = 0.0089).
In patients with “Active” scleroderma pattern the linear mixed-effects model revealed a significant main effect of time on capillary density (F(1, 46) = 34.89, p < 0.001), indicating an overall reduction from baseline (T0) to follow-up (T4). A significant interaction between time and group was detected (F(1, 46) = 6.75, p = 0.0125), indicating that the change in capillary density over time differed between treated and control subjects (Table 3).
Post-hoc analysis showed that in the control group, capillary density significantly decreased from T0 to T4 (mean difference = −0.95; p < 0.0001), whereas in the treated group, a smaller but still significant reduction was observed (mean difference = −0.37; p = 0.016).
Overall, these findings indicate that although both groups experienced a reduction in capillary density over time, the decrease was less pronounced in the treated group. To further investigate the potential confounding effect of concomitant standard therapies two separate multiple linear regression models were performed, stratified by NVC scleroderma pattern at baseline (“Early” and “Active”). In patients presenting with an “Early” pattern at baseline aminaphtone treatment was independently associated with significantly greater capillary preservation over four years (β = +1.71, SE = 0.66, p = 0.017, 95% CI [0.42–3.01]). Controls lost on average −2.10 ± 1.37 capillaries over the observation period, compared with −0.79 ± 1.08 in the aminaphtone-treated group (p = 0.009).
None of the concomitant therapies, including immunosuppressants, intravenous prostanoids, or PDE5 inhibitors, reached statistical significance as independent predictors of capillary density change (all p > 0.05).
In patients presenting with an “Active” pattern at baseline aminaphtone treatment showed a trend toward greater capillary preservation (β = +0.45, SE = 0.25, p = 0.079, 95% CI [−0.04–0.93]), which did not reach statistical significance after adjustment for covariates. However, the unadjusted comparison revealed a significant difference between groups (controls −0.95 ± 0.92 vs aminaphtone −0.29 ± 0.60 capillaries; p = 0.004), consistent with a biologically relevant effect. As in the “Early” pattern subgroup, no concomitant therapy was an independent predictor of capillary change (all p > 0.05). Taken together, these findings suggest that the protective effect of aminaphtone on capillary density is most evident in the earlier stages of SSc-related microangiopathy, when residual capillary reserve is still present. The attenuation of statistical significance in the Active pattern subgroup is likely attributable to the smaller absolute capillary loss observed in both groups at this more advanced stage of microvascular damage, combined with the limited sample size available for the stratified analysis.
Discussion
Aminaphtone appears to be as safe and well-tolerated therapeutic compound even during four-year long-term treatment. Indeed, the large cohort of Caucasian SSc patients enrolled in the study did not experience any severe adverse events during the follow-up of five years.
The stability of the scleroderma-pattern observed over a 4-year follow-up assessed by NVC suggests a potential adjunctive therapeutic effect of aminaphtone, particularly in mitigating vascular tissue damage when used alongside standard therapy in SSc patients (Table 1). Aminaphtone was administrated orally at a dosage of 75 mg twice a day (every 12 hours), thus no hospitalization or specialized personnel were needed.
Of note, only 10% of our cohort of patients presented mild intolerance due to already described and reversible adverse events (headache 2.7%, itching 1.3%, others 6%). Treatment was promptly discontinued in these patients, and the symptoms shortly resolved without leaving any sequelae. Pre-clinical testing included acute, subacute, and chronic toxicity studies in various animal models, with doses up to 3 g/kg showing no evidence of tissue damage or functional organ alterations.9
Notably, RP is associated with significant pain and complications in SSc, contributing to substantial disability and a marked reduction in quality of life.23
Indeed, prolonged tissue ischemia occurring during RP episodes along with imbalanced endothelial activation, such as increased release of endothelin 1 (ET-1), thromboxane, and thrombomodulin, and reduction of nitric oxide production may contribute to endothelial damage leading to fibrosis.24
Moreover, a complex sequence of vascular damage and aberrant immune responses leads to an excessive extracellular matrix (ECM) production resulting in impaired functionality across multiple affected organ systems.
The mechanism of actions of aminaphtone remains partially understood, as matter of fact, according to pre-clinical studies, aminaphtone showed to downregulate endothelial adhesion molecules (ie, VCAM, ICAM, Selectins), vasoconstrictor peptides (ie, Endothelin-1), and pro-inflammatory cytokine expression (ie, IL-6, IL-10, VEGF, TGF-beta) highlighting its protective role of endothelial in a wide range of diseases.11,13–15,25
Recently, the Cochrane Vascular Group summarised the most updated evidence of the potential role of aminaphtone as a phlebotonic agent for venous insufficiency.15,26,27
Interestingly, in vitro studies on human ECV304 endothelial cells demonstrated that aminaphtone treatment downregulates several gene sets and molecular pathways involved in fibrotic processes including those involving the TGF- β, which is known to be associated with M2 macrophage polarization and profibrotic activity especially in progressive ILD-SSc patients.25,28,29
An open-label feasibility study demonstrated the efficacy of aminaphtone in improving also peripheral blood perfusion, as assessed by Laser Speckle Contrast Analysis (LASCA), and in alleviating the clinical symptoms of Raynaud’s phenomenon in patients with either primary RP or secondary RP associated with SSc.8
The EULAR–EUSTAR and the 2016 British Society for Rheumatology provided treatment recommendations based first by calcium channel blockers and then phosphodiesterase 5 inhibitors or intravenous iloprost.18 However, these therapies are burned with side effects such as tachycardia, hypotension, and headache causing discontinuation.30
Therefore, alternative therapeutic strategies and/or combining targets therapy should be considered to achieve clinical responses maintaining a high safety profile over time. Noteworthy, NVC findings described as scleroderma pattern “Early”, “Active”, or “Late” mirror the severity of microvascular damage in SSc patients. Indeed, NCV was introduced in the 2013 classification criteria for SSc, remarking its utility especially in the early diagnosis, where RP may be the only disease manifestation.17,19
Prior investigations described the strong association between the endothelial damage observed at NVC and organ involvement in SSc patients.31,32 Moreover, the timing of transition through different NVC patterns reported in previous study was 28 ± 20 months from “Early” to “Active” and 36 ± 29 months from “Active” to “Late”.33
In the present study of SSc patients treated with aminaphtone in association with ST, a stable capillaroscopic pattern was observed in 91% of cases during the observational follow-up, while 9% presented a slower timing of transition compared with previous study reports.33 Likewise, a recent case report reported the potential of aminaphtone to improve microcirculation in a young patient affected by undifferentiated connective tissue disease with symptomatic Raynaud’s phenomenon.22
The present capillaroscopic results were compared to a control group of SSc patients treated with ST alone according to EULAR recommendations.18 In addition, a slower time of transition between NVC patterns in aminaphtone -treated compared to the control group of SSc patients treated with ST alone was reported. These results suggest that aminaphtone may represent a potential therapeutic support not only in chronic venous insufficiency, where its efficacy has been extensively evaluated, but also in connective tissue diseases characterized by microvascular damage.34
Several limitations should be acknowledged. The retrospective and monocentric real-world design may have introduced selection bias and limits the external validity of the findings. The unequal number of patients between the two groups may also have influenced the robustness of the comparisons, although the cohorts were specifically selected to avoid statistically significant differences in age, gender, ethnicity, and ST.
In addition, the inclusion of exclusively Caucasian patients reduces the generalisability of the results to other ethnic populations. Moreover, the availability of the drug is currently limited to selected countries, including Italy, which may further restrict the applicability of these findings in different healthcare settings.
Nevertheless, this study provides evidence regarding the safety profile of the treatment and suggests a potential beneficial effect on endothelial damage, as documented by nailfold videocapillaroscopy analysis.19
In conclusion, aminaphtone associated with ST therapy showed a good tolerability and safety profile in SSc patients with secondary RP, without any disabling or serious side effects, during four years of long-term treatment.
The NVC scleroderma-patterns stability over four-year follow-up, observed at NVC examination, suggests a potential supplementary therapeutic effect of aminaphtone when used alongside standard therapy in SSc patients, at least on reducing microvascular damage progression.
Studies on the long-term effects of aminaphtone administration on the microcirculation in SSc patients are ongoing and need further research.
Acknowledgment
The drug (aminaphtone) was produced by Laboratory Baldacci Spa (Pisa, Italy). Laboratory Baldacci Spa was not involved in study design, collection, analysis and interpretation of data, writing of the report, nor in the decision to submit the article for publication. Laboratory for Experimental Rheumatology received an unconditioned research grant from Laboratori Baldacci Spa, not related to the present manuscript. University of Genova and IRCCS AOM Ospedale Policlinico San Martino Genova Italy, are members of the European Reference Network on Rare Connective Tissue and Musculoskeletal Diseases (ERN-ReCONNET) and Centres of Excellence for Imaging of EULAR (European Alliance of Associations for Rheumatology). We gratefully acknowledge the continuous support of Prof. Vanessa Smith as senior clinical investigator of the Research Foundation - Flanders (Belgium) and chairman of EULAR Study Group on Microcirculation in Rheumatic Diseases and the Scleroderma Clinical Trials Consortium Group on Capillaroscopy. An earliest version of this paper was presented as an abstract at the EULAR 2024 Congress as a poster presentation with interim findings. The poster’s abstract was published in a special issue in Annals of the Rheumatic Diseases 2024;83:1929.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cutolo M, Soldano S, Smith V. Pathophysiology of systemic sclerosis: current understanding and new insights. Expert Rev Clin Immunol. 2019;15(7):753–11. doi:10.1080/1744666X.2019.1614915
2. Volkmann ER, Andréasson K, Smith V. Systemic sclerosis. Lancet. 2023;401(10373):304–318. doi:10.1016/S0140-6736(22)01692-0
3. Pauling JD, Hughes M, Pope JE. Raynaud’s phenomenon – an update on diagnosis, classification and management. Clin Rheumatol. 2019;38:3317–3330. doi:10.1007/s10067-019-04745-5
4. Varga J, Trojanowska M, Kuwana M. Pathogenesis of systemic sclerosis: recent insights of molecular and cellular mechanisms and therapeutic opportunities. J Scleroderma Relat Disord. 2017;2:137–152. doi:10.5301/jsrd.5000249
5. Hughes M, Herrick AL. Raynaud’s phenomenon. Best Pract Res Clin Rheumatol. 2016;30:112–132. doi:10.1016/j.berh.2016.04.001
6. Cutolo M, Sulli A, Smith V. Assessing microvascular changes in systemic sclerosis diagnosis and management. Nat Rev Rheumatol. 2010;6(10):578–587. doi:10.1038/nrrheum.2010.104
7. De Anna D, Mari F, Intini S, et al. Effects of therapy with aminaftone on chronic venous and lymphatic stasis [in Italian]. Minerva Cardioangiol. 1989;37:251–254.
8. Ruaro B, Pizzorni C, Paolino S, et al. Aminaphtone efficacy in primary and secondary Raynaud’s phenomenon: a feasibility study. Front Pharmacol. 2019;10:293. doi:10.3389/fphar.2019.00293
9. Gotelli E, Soldano S, Hysa E, et al. A systematic review of aminaphtone from pathophysiology to clinical applications: focus on new rheumatological acquisitions. Pharmaceuticals. 2023;16(4):569. doi:10.3390/ph16040569
10. Dupuis J. Endothelin-receptor antagonists in pulmonary hypertension. Lancet. 2001;358(9288):1113–1114. doi:10.1016/S0140-6736(01)06298-5
11. Scorza R, Santaniello A, Salazar G, et al. Effects of aminaftone 75 mg TID on soluble adhesion molecules: a 12-week, randomized, open-label pilot study in patients with systemic sclerosis. Clinical Therapeutics. 2008;30(5):924–929. doi:10.1016/j.clinthera.2008.05.009
12. Salazar G, Bellocchi C, Todoerti K, et al. Gene expression profiling reveals novel protective effects of Aminaphtone on ECV304 endothelial cells. Eur J Pharmacol. 2016;782:59–69. doi:10.1016/j.ejphar.2016.04.018
13. Pereira de Godoy JM, Paludetto G, Testoni BR, Sano PY. Aminaphtone for light bleeding in patients under oral anticoagulation. Open Cardiovasc Med J. 2010;4:146–147. doi:10.2174/1874192401004010146
14. Romano C, Tamburella C, Costa M, et al. Aminaphtone therapy in patients with type 1 diabetes and albuminuria: a case report. J Med Case Rep. 2014;8:443. doi:10.1186/1752-1947-8-443
15. Belczak SQ, Sincos IR, Campos W, et al. Veno-active drugs for chronic venous disease: a randomized, double-blind, placebo-controlled trial. Phlebology. 2014;29:454–460. doi:10.1177/0268355513489550
16. Ramahi A, Hughes M, Khanna D. Practical management of Raynaud’s phenomenon - a primer for practicing physicians. Curr Opin Rheumatol. 2022;34(4):235–244. doi:10.1097/BOR.0000000000000877
17. van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis. Ann Rheum Dis. 2013;72:1747–1755. doi:10.1136/annrheumdis-2013-204424
18. Kowal-Bielecka O, Fransen J, Avouac J, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. 2017;76:1327–1339. doi:10.1136/annrheumdis-2016-209909
19. Smith V, Herrick AL, Ingegnoli F, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud’s phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19:102458. doi:10.1016/j.autrev.2020.102458
20. Smith V, Vanhaecke A, Herrick AL, et al. Fast track algorithm: how to differentiate a “scleroderma pattern” from a “non-scleroderma pattern”. Autoimmun Rev. 2019;18:102394. doi:10.1016/j.autrev.2019.102394
21. Ickinger C, Campitiello R, Four D, et al. Nailfold capillaroscopy and organ involvement in systemic sclerosis: a systematic review. Best Pract Res Clin Rheumatol. 2025:102130.
22. Screm G, Mondini L, Salton F, et al. Assessment of treatment effects of aminaphtone by capillaroscopy in a patient with Raynaud’s phenomenon. Pharmaceuticals. 2025;18(2):203. doi:10.3390/ph18020203
23. Merkel PA, Herlyn K, Martin RW, et al. Measuring disease activity and functional status in patients with scleroderma and Raynaud’s phenomenon. Arthritis Rheum. 2002;46(9):2410–2420. doi:10.1002/art.10486
24. Herrick AL, Illingworth K, Blann A. von Willebrand factor, thrombomodulin, thromboxane, thromboglobulin and fibrinolysis markers in primary Raynaud’s phenomenon and systemic sclerosis. Ann Rheum Dis. 1996;55:122–127. doi:10.1136/ard.55.2.122
25. Sulli A, Soldano S, Campitiello R, et al. Effects of aminaphtone on TGF-beta1 serum concentration as concomitant treatment to standard therapy in systemic sclerosis patients: a pilot study [abstract number 2445]. Arthritis Rheumatol. 2024;76(suppl 9).
26. Martinez-Zapata MJ, Vernooij RW, Uriona Tuma SM, et al. Phlebotonics for venous insufficiency. Cochrane Database Syst Rev. 2016;4:CD003229. doi:10.1002/14651858.CD003229.pub3
27. Salazar G, Bellocchi C, Todoerti K, et al. Time-course gene expression data on the transcriptional effects of Aminaphtone on ECV304 endothelial cells. Data Brief. 2016;8:836–850. doi:10.1016/j.dib.2016.06.051
28. Campitiello R, Soldano S, Gotelli E, et al. The intervention of macrophages in progressive fibrosis characterizing systemic sclerosis: a systematic review. Autoimmunity Reviews. 2024;23(10):103637. doi:10.1016/j.autrev.2024.103637
29. Smith V, Soldano S, Campitiello R, et al. Circulating monocytes from systemic sclerosis patients with progressive interstitial lung disease preferentially express M2 phenotype markers: in vitro and ex vivo study. RMD Open. 2025;11(4):e006135. doi:10.1136/rmdopen-2025-006135
30. Pope JE, Bellamy N, Seibold JR, et al. Iloprost and cisaprost for Raynaud’s phenomenon in progressive systemic sclerosis. Cochrane Database Syst Rev. 1998:CD000953.
31. Smith V, Riccieri V, Pizzorni C, et al. Nailfold capillaroscopy for prediction of novel future severe organ involvement in systemic sclerosis. J Rheumatol. 2013;40(12):2023–2028. doi:10.3899/jrheum.130528
32. Correia AM, Campitiello R, Pizzorni C, et al. Differences in nailfold capillaroscopy findings between limited and diffuse cutaneous systemic sclerosis: a detailed analysis. RMD Open. 2025;11(3):e005716. doi:10.1136/rmdopen-2025-005716
33. Sulli A, Pizzorni C, Smith V, Zampogna G, Ravera F, Cutolo M. Timing of transition between capillaroscopic patterns in systemic sclerosis. Arthritis Rheum. 2012;64(3):821–825. doi:10.1002/art.33463
34. Miguel CB, Andrade RS, Mazurek L, et al. Emerging pharmacological interventions for chronic venous insufficiency: a comprehensive systematic review and meta-analysis of efficacy, safety, and therapeutic advances. Pharmaceutics. 2025;17(1):59. doi:10.3390/pharmaceutics17010059
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.