Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Safety and Efficacy of Mesotherapy with Placenta Polypeptide Injection for Moderate-to-Severe Sensitive Skin: A Multicenter, Randomized, Controlled Trial
Authors Shu C ![]() , Zhang XY, Han XF, Liu JW, Sun X, Sun QN
, Zhang XY, Han XF, Liu JW, Sun X, Sun QN
Received 12 September 2025
Accepted for publication 17 January 2026
Published 29 January 2026 Volume 2026:19 567103
DOI https://doi.org/10.2147/CCID.S567103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Chang Shu,1 Xin-Yu Zhang,2 Xue-Feng Han,2 Jia-Wei Liu,1 Xin Sun,1 Qiu-Ning Sun1
1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Department of Body Contouring and Liposuction Center, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100144, People’s Republic of China
Correspondence: Qiu-Ning Sun, Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China, Tel +86-10-69151502, Email [email protected]
Background: Sensitive skin (SS) is a prevalent condition characterized by cutaneous hyperreactivity and neurosensory inflammation, for which effective treatments remain limited. Placenta polypeptide injection (PPI), rich in anti-inflammatory cytokines and growth factors, presents a promising therapeutic candidate. This study aimed to rigorously evaluate the safety and efficacy of mesotherapy with PPI for treating moderate-to-severe SS.
Methods: In this multicenter, open-label, randomized controlled trial, 156 adults with moderate-to-severe SS were randomized (PPI group: control group = 2:1) to receive three sessions of mesotherapy with PPI (4 mL per session at 30-day intervals) or no treatment (control group) over a 90-day period. The primary endpoint was the change in total facial skin hemoglobin content, a proxy measure of cutaneous inflammation, from baseline to Day 90, quantified by a 3D skin analysis system. Safety was monitored through adverse events (AEs) and laboratory assessments.
Results: A total of 154 patients were included in the full analysis set (FAS; 103 PPI group, 51 control group). At Day 90, the PPI group demonstrated a significantly greater reduction in skin hemoglobin content compared to the control group (mean change, − 1705.82 ± 1808.17 vs − 756.65 ± 1493.17; P=0.001). Furthermore, a significantly higher proportion of patients in the PPI group reported aesthetic improvement on the GAIS (88.9% vs 5.9% rated as “improved” to “very much improved”; P < 0.001). The incidence of AEs was comparable between the PPI (5.8%) and control (9.6%) groups (P = 0.376), with no serious AEs reported.
Conclusion: Mesotherapy with placenta polypeptide injection is an effective and safe treatment for moderate-to-severe sensitive skin, leading to significant reductions in cutaneous inflammation metrics and high rates of patient-reported aesthetic improvement.
Trial Registration: This study was prospectively registered at Chinese Clinical Trial Registry (No. ChiCTR2400080988, Date: 20/02/2024).
Keywords: sensitive skin, placenta polypeptide injection, mesotherapy, inflammation, randomized controlled trial, hemoglobin content
Introduction
Sensitive skin (SS) is a globally recognized dermatological syndrome defined by exaggerated adverse reactions to various triggers, which can be physical, chemical, or environmental.1,2 Clinically, it presents with subjective sensations such as stinging, burning, itching, and tightness, often accompanied by objective signs like erythema, scaling, and telangiectasia.3,4 SS is highly prevalent, affecting a substantial portion of the population worldwide (approximately 60–70% in women and 50–60% in men), and significantly impairing quality of life by causing persistent unpleasant sensations such as burning, stinging, tightness, pain, and pruritus.5,6 The underlying pathophysiology is multifactorial, involving a compromised epidermal barrier function, heightened neurosensory responses, and dysregulated immune-inflammatory pathways.7,8 A key element in this process is the over-activation of sensory nerve endings via channels like the transient receptor potential vanilloid 1 (TRPV1), which triggers the release of neuropeptides and pro-inflammatory cytokines, perpetuating a state of chronic subclinical inflammation.9,10 Current management strategies, focusing on gentle skincare and avoiding triggers, often provide only partial relief, highlighting an unmet need for targeted therapies that can modulate the core inflammatory processes.
Human placental extract (HPE), a biological agent derived from post-delivery placenta, has a long history of use in regenerative medicine due to its rich composition of bioactive molecules.11,12 These extracts contain a complex mixture of growth factors (eg, EGF, FGF, HGF, TGF-β), anti-inflammatory cytokines, peptides, amino acids, and nucleic acids.11–13 Preclinical and clinical evidence suggests that HPE exerts potent anti-inflammatory, antioxidant, and tissue-regenerative effects in various conditions, including osteoarthritis, chronic wounds, and liver disease.11,14,15 The proposed mechanisms involve the modulation of key inflammatory signaling pathways, such as nuclear factor-kappa B (NF-κB) and JAK-STAT, promotion of anti-inflammatory macrophage polarization (M2 macrophage), and suppression of pro-inflammatory cytokine production.16–18 Specifically, placenta polypeptide injection (PPI), a refined form of HPE, has demonstrated efficacy in preclinical models of inflammatory skin disorders, such as atopic dermatitis, by dose-dependently inhibiting delayed-type hypersensitivity reactions with a favorable safety profile.17,19
Mesotherapy, a technique involving microinjections of therapeutic substances directly into the dermis, enhances local drug bioavailability and stimulates dermal remodeling.20,21 This administration method is increasingly utilized in aesthetic dermatology to improve skin quality and address various concerns such as lipolysis, skin rejuvenation, pigmentation and hair loss.22 By delivering PPI directly to the site of inflammation, mesotherapy could potentiate its therapeutic effects in SS. This study was conducted as a prospective, multicenter, randomized controlled trial to quantitatively evaluate the safety and efficacy of mesotherapy with PPI for moderate-to-severe SS. The primary hypothesis was that PPI would mitigate cutaneous inflammation and lead to an overall improvement in skin condition.
Methods
Trial Design and Oversight
This was a multicenter, open-label, randomized, parallel-group, controlled trial conducted at Peking Union Medical College Hospital and the Plastic Surgery Hospital of the Chinese Academy of Medical Sciences in Beijing, China, between March 2024 and November 2024. The trial was conducted in accordance with the principles of the Declaration of Helsinki, Good Clinical Practice guidelines, and applicable local regulations. The study protocol (TPDT-001, Version 4.0, January 2, 2024) and informed consent forms were approved by the independent ethics committee at the lead institution, Peking Union Medical College Hospital (No. I-24PJ0085). All participants provided written informed consent before enrollment. The trial was monitored by a contract research organization (Beijing Guoren Likang Medical Consulting Co., Ltd).
Inclusion and Exclusion Criteria
Eligible participants were selected based on the following criteria:
Inclusion Criteria
- Male or female adults aged 18 years or older.
- Clinical diagnosis of moderate-to-severe sensitive skin, confirmed by a positive lactic acid sting test (LAST). The LAST is performed by applying 50μL of 10% lactic acid solution onto the skin of the nasolabial fold. The contralateral side is treated with saline. The participants were asked to grade the intensity of sting using a 4-point scale (0–3) at 2.5 and 5 min after application of lactic acid. Cumulative scores at 2.5 and 5 min ≥3 were considered as the LAST positive group.
- Agreement to refrain from any other facial cosmetic treatments for the duration of the study.
Exclusion Criteria
- Pregnancy, planning pregnancy, or lactation.
- Known hypersensitivity or allergy to any component of the study product.
- Active infectious or inflammatory facial lesions requiring treatment.
- History of keloids or hypertrophic scarring.
- Any other condition that, in the investigator’s opinion, could interfere with the study results or pose a risk to the participant.
Randomization and Interventions
Eligible participants were centrally randomized in a 2:1 ratio to either the PPI group or the no-treatment control group. The randomization sequence was generated using computer software with block randomization. After enrollment, investigators assigned participants to treatment groups using sealed, sequentially numbered envelopes.
Participants in the PPI group received three treatment sessions at baseline (Day 0), Day 30 (±5 days), and Day 90 (±5 days). Before the first treatment, a skin prick test with the study drug was performed; participants with a positive reaction were excluded. During each session, 4 mL of placenta polypeptide injection (Guizhou Taibang Biological Products Co., Ltd., China; batch no. 202303006) was administered via mesotherapy across the entire face using a sterile single-use needle. The injection depth was controlled at 1.0 mm to 1.2 mm. The control group received no treatment during the study period.
Outcomes and Assessments
The primary efficacy endpoint was the change in total facial skin hemoglobin content from baseline to Day 90 (±5 days) (30 days after the last treatment). Skin hemoglobin, an objective proxy for cutaneous inflammation and erythema, was measured using the Antera 3D® skin analysis system (Miravex, Ireland). Measurements were taken on three facial regions (forehead, left cheek, and right cheek), and the total value was used for analysis.
Secondary efficacy endpoints, also assessed at baseline and scheduled follow-up visits (at 14±5, 30±5, 60±5 and 90±5 days after the operation), included: (1) change in facial erythema area (mm2) measured by Antera 3D®; (2) change in skin roughness (a composite score for forehead, left cheek, and right cheek) measured by Antera 3D®; (3) change in wrinkle score measured by the Visia® Complexion Analysis system (Canfield Scientific, USA); (4) change in dermal thickness (mm), assessed as the average of three measurement points using high-frequency skin ultrasound; and (5) Global Aesthetic Improvement Scale (GAIS) score was assessed by investigators at Day 90. The GAIS is a 5-point scale where investigators rate the overall aesthetic improvement compared to baseline as: “very much improved”, “much improved”, “improved”, “no change”, or “worse”.23–26
Safety was evaluated throughout the trial. All adverse events (AEs) were recorded, including their severity (mild, moderate, severe), duration, and relationship to the study intervention. Potential complications related to mesotherapy (eg, bleeding, bruising, swelling, infection, allergy, nodules, embolism) were specifically monitored. Laboratory safety assessments, including complete blood count, serum biochemistry, and coagulation profiles, were performed for the PPI group at screening, Day 14, and Day 90, and for the control group at screening.
Statistical Analysis
The sample size was calculated to provide adequate power for the primary endpoint. The calculation was based on a superiority statistical model. Based on this calculation, A total of 156 participants (104 in the PPI group and 52 in the control group) were planned for enrollment. All statistical analyses were performed using SAS software, version 9.4. Efficacy analyses were conducted on the full analysis set (FAS), defined as all randomized participants who received at least one dose of the study intervention and had at least one post-baseline efficacy assessment, following the intention-to-treat (ITT) principle. A per-protocol set (PPS) analysis, including only participants who completed the trial without major protocol deviations, was also performed for the primary endpoint. The safety set (SS) included all participants who received at least one treatment.
Continuous variables were summarized as mean ± standard deviation (SD) and compared between groups using an independent samples t-test or ANCOVA, adjusting for baseline values where appropriate. Categorical variables were summarized as frequencies and percentages and compared using the chi-squared test or Fisher’s exact test. For GAIS, the ordered categorical data were analyzed using the Cochran-Mantel-Haenszel (CMH) test. All statistical tests were two-sided, and a P-value of less than 0.05 was considered statistically significant.
Results
Participant Disposition and Baseline Characteristics
A total of 156 participants were enrolled and randomized between March 4, 2024, and November 12, 2024. Of these, 104 were assigned to the PPI group and 52 to the control group. In the PPI group, 99 participants (95.2%) completed the study, while 51 (98.1%) completed in the control group. Six participants withdrew during the study (5 in the PPI group, 1 in the control group), all citing personal reasons related to scheduling. The FAS included 154 participants (103 in the PPI group, 51 in the control group) after excluding two participants who were randomized but had no post-baseline efficacy data (Figure 1).
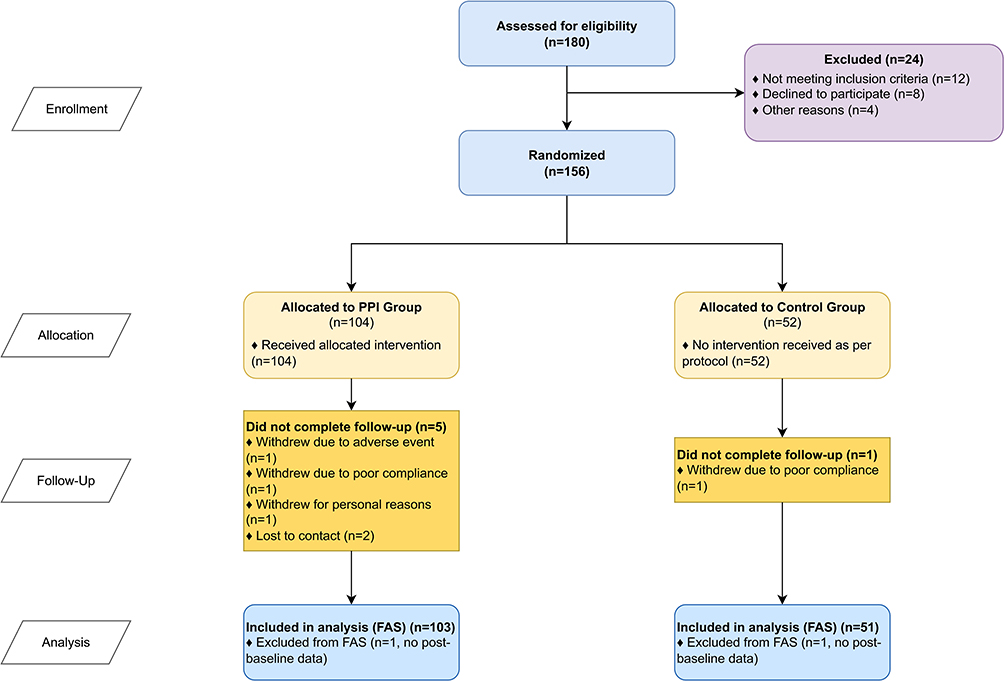 |
Figure 1 CONSORT 2010 Flow Diagram of the Trial. The diagram shows the flow of participants through each stage of the randomized trial, including enrollment, allocation to intervention groups, follow-up, and data analysis. Abbreviations: PPI, Placental Polypeptide Injection; FAS, Full Analysis Set. |
Baseline demographic and clinical characteristics were generally well-balanced between the two groups (Table 1). The mean age of participants was 34.95 ± 11.70 years in the PPI group and 31.90 ± 7.66 years in the control group (P = 0.055). The majority of participants were female (83.5% in the PPI group and 80.4% in the control group). At baseline, the mean total skin hemoglobin content was significantly higher in the PPI group compared to the control group (10075.69 ± 2629.22 vs 9127.07 ± 2516.36; P = 0.034). Other baseline efficacy parameters, including erythema area, skin roughness, wrinkle score, and dermal thickness, were comparable between the groups (all P > 0.05).
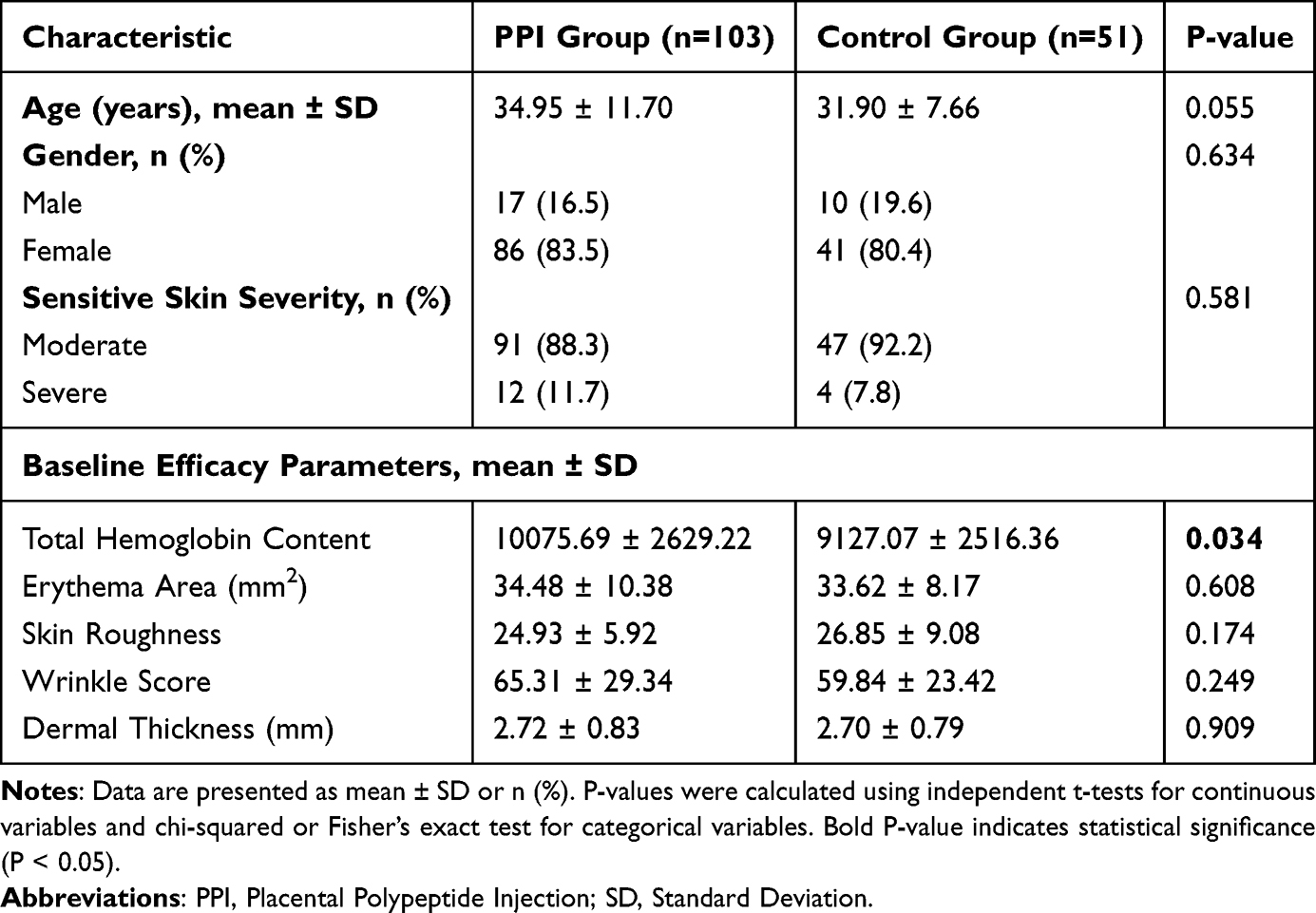 |
Table 1 Baseline Demographic and Clinical Characteristics of Participants |
Efficacy Outcomes
For the primary endpoint, participants in the PPI group experienced a significantly greater reduction in total skin hemoglobin content from baseline to Day 90 compared to the control group. The mean change (±SD) was −1705.82 ± 1808.17 in the PPI group versus −756.65 ± 1493.17 in the control group (P = 0.001) in the FAS analysis (Figure 2 and Table 2). The per-protocol set analysis yielded consistent results, demonstrating a similarly significant difference between the groups (Supplementary Table S1).
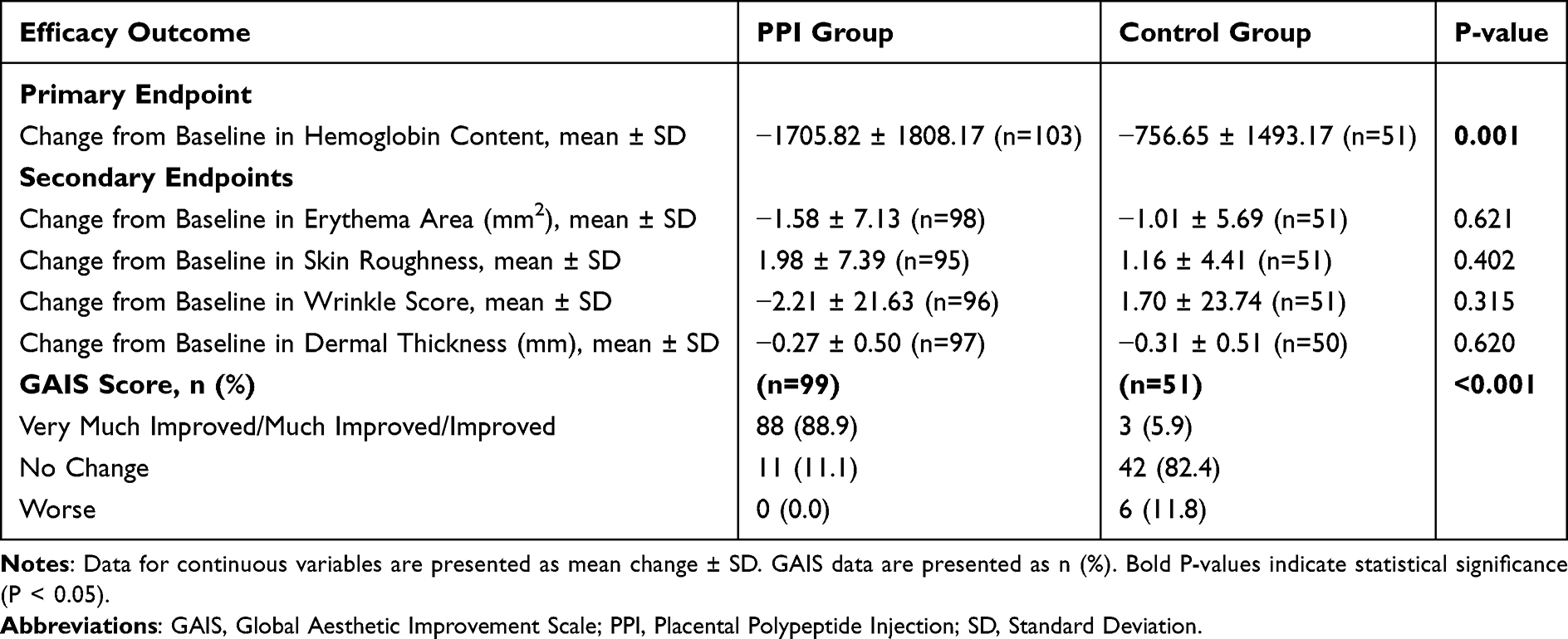 |
Table 2 Primary and Secondary Efficacy Outcomes at Day 90 |
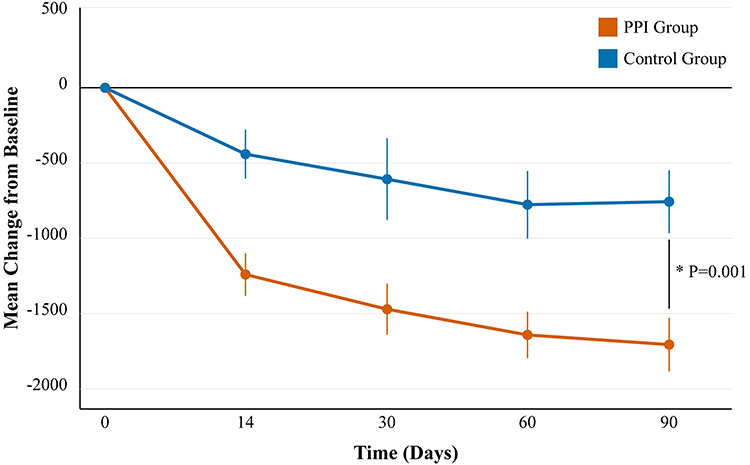 |
Figure 2 Change in Skin Hemoglobin Content from Baseline. Least-squares mean (± standard error) change from baseline in total facial skin hemoglobin content over 90 days in the Full Analysis Set. A greater negative value indicates a more substantial reduction in hemoglobin, reflecting decreased inflammation. *P=0.001 for the comparison between groups at Day 90, based on an independent t-test. |
Analysis of secondary endpoints revealed a marked difference in the GAIS scores. At Day 90, 88.9% of participants in the PPI group were rated by investigators as having improved (“improved”, “much improved”, or “very much improved”), compared to only 5.9% in the control group (P < 0.001) (Figure 3 and Table 2). Specifically, in the PPI group, 4.0% were “very much improved”, 17.2% were “much improved”, and 67.7% were “improved”. In contrast, no participants in the control group were rated as “very much improved” or “much improved”. Representative images from the Antera 3D® system visually demonstrate the reduction in redness and improvement in skin texture in a participant from the PPI group (Figure 4).
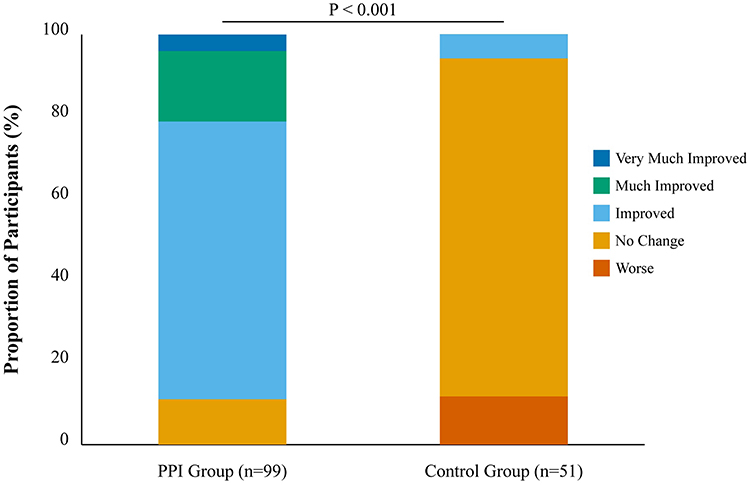 |
Figure 3 Global Aesthetic Improvement Scale (GAIS) Scores at Day 90. Distribution of investigator-assessed GAIS scores for the Placental Polypeptide Injection and Control groups in the Full Analysis Set. P<0.001 by the Cochran-Mantel-Haenszel test for the overall distribution of improvement categories, indicating a significant difference in favor of the PPI group. |
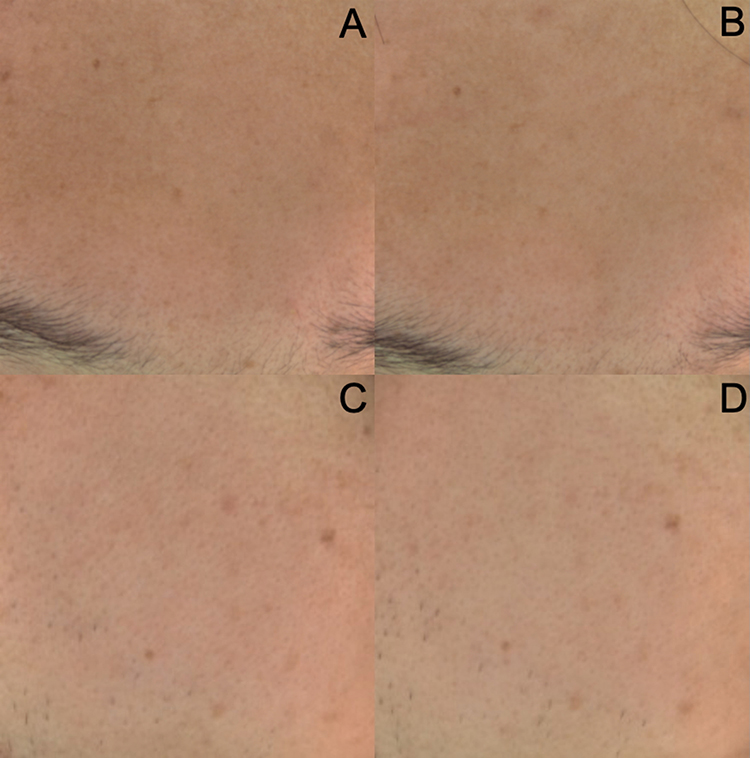 |
Figure 4 Representative Antera 3D® Skin Analysis Images mages from a participant in the Placental Polypeptide Injection group at baseline (Day 0) and final follow-up (Day 90). Panels (A) and (B) show the forehead region at baseline and Day 90, respectively. Panels (C) and (D) show the right cheek region at baseline and Day 90. The images demonstrate a visible reduction in erythema (redness) and an improvement in overall skin tone and texture following treatment. The quantitative scores for this participant showed a decrease in redness from 34 (moderate) to 23 (mild). |
There were no statistically significant differences between the two groups in the other secondary endpoints at Day 90, while slightly improvements of erythema area were observed (Table 2 and Supplementary Figures S1–S4). The mean changes from baseline for erythema area, skin roughness, wrinkle score, and dermal thickness were similar in the PPI and control groups (all P > 0.05). Transient improvements in wrinkle score were observed at earlier time points (Days 14–60).
Safety and Tolerability
Mesotherapy with PPI was well tolerated. The overall incidence of AEs was low and comparable between the groups, occurring in 6 participants (5.8%) in the PPI group and 5 participants (9.6%) in the control group (P = 0.376) (Table 3). No serious AEs or deaths occurred during the study. In the PPI group, three AEs were considered possibly related to the study intervention (facial peeling, facial pigmentation, and facial erythema); all were of moderate severity and resolved with appropriate management. The remaining AEs in the PPI group and all AEs in the control group were mild and deemed unrelated to the study (Supplementary Table S2). No treatment-related complications such as infection, allergy, or nodule formation were observed. Laboratory test results showed no clinically significant changes from baseline in either group. Concomitant medication use was also similar between groups (Supplementary Table S3).
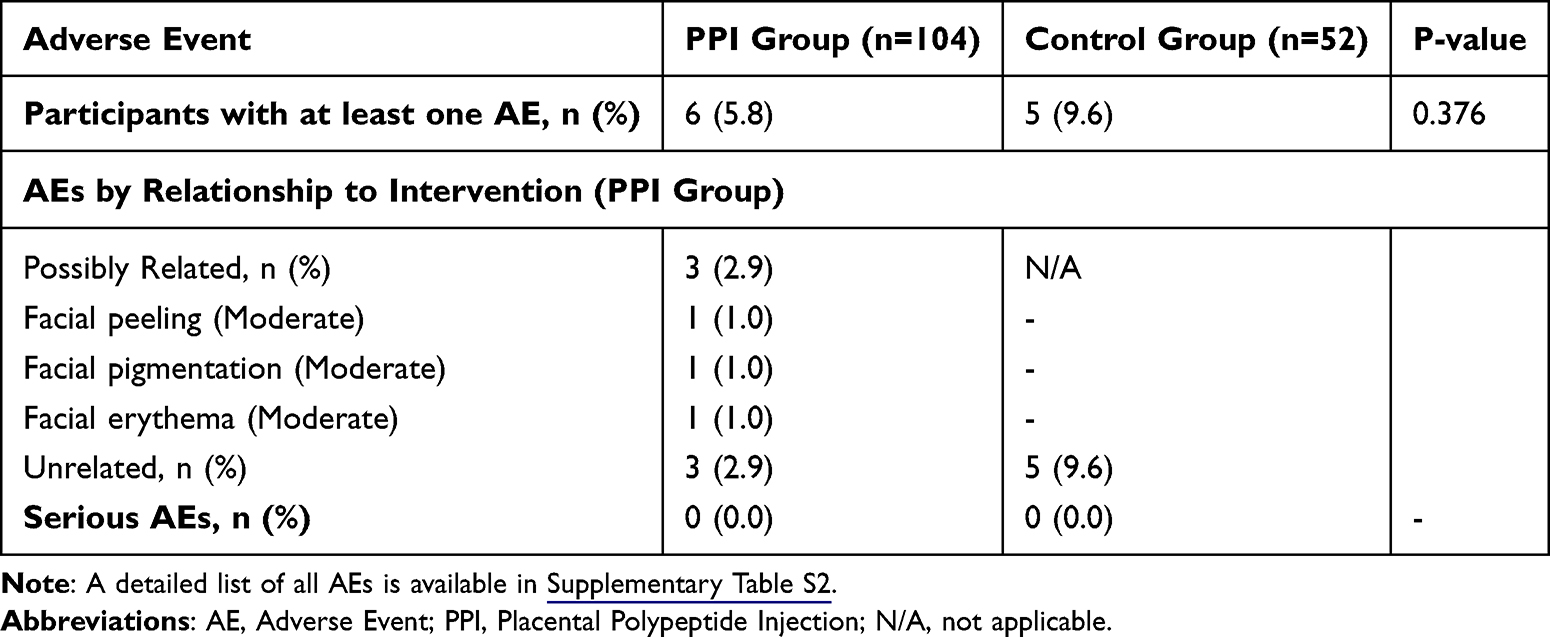 |
Table 3 Summary of Adverse Events |
Discussion
This multicenter, randomized controlled trial provides the first robust clinical evidence for the safety and efficacy of mesotherapy with PPI in the management of moderate-to-severe sensitive skin. The study met its primary endpoint, demonstrating that PPI treatment led to a statistically significant and clinically meaningful reduction in facial skin hemoglobin content compared to no treatment. As skin hemoglobin level is a validated, objective biomarker for cutaneous microvascular vasodilation and inflammation, this finding strongly supports the hypothesis that PPI exerts a potent anti-inflammatory effect on sensitive skin, potentially through modulating nitric oxide bioavailability and cellular NAD+ pathways to attenuate microvascular dysfunction and oxidative stress.27–29 The magnitude of this effect (−1705.82 in the PPI group vs −756.65 in controls) is substantial and suggests a direct modulation of the underlying inflammatory cascade responsible for the erythema characteristic of SS. This result is consistent with the known mechanisms of placental extracts, which are rich in bioactive molecules like TGF-β1 and IGFBPs that can suppress inflammatory pathways such as NF-κB and JAK-STAT3.16,30
The highly significant improvement observed in the GAIS scores further corroborates the clinical benefit of PPI. An overwhelming majority of PPI-treated participants (88.9%) were perceived by investigators as having achieved aesthetic improvement, compared to a mere 5.9% in the control group. This outcome is particularly important as it reflects a holistic clinical judgment that integrates both objective signs (eg, reduced redness) and overall skin appearance, which likely aligns with patient satisfaction. The discrepancy between the strongly positive GAIS results and the non-significant findings for some objective secondary measures (eg, roughness, wrinkles) may suggest that the primary benefit perceived by both patients and clinicians is the reduction in inflammatory signs and subjective symptoms, which are the main burden of SS.31
The lack of significant improvement in skin roughness, wrinkles, and dermal thickness is not entirely unexpected. The 90-day study duration may have been insufficient to detect structural changes in the skin matrix, such as collagen remodeling or hydration improvements, which typically require a longer timeframe to become apparent.32 Furthermore, the primary mechanism of PPI in this context appears to be centered on rapid anti-inflammatory and neurosensory modulation rather than long-term structural repair. The control group also showed some minor improvements in certain metrics, which could be attributed to natural fluctuations, seasonal variations, or increased attention to basic skincare (the Hawthorne effect), although this was not formally assessed. The early, non-significant improvements in erythema and wrinkle scores observed between Day 14 and Day 60 may reflect initial biological activity, such as reduced vascular reactivity and early extracellular matrix modulation, that may contribute cumulatively to the significant reduction in skin hemoglobin content (inflammation metrics) by Day 90. While these transient changes did not reach statistical significance individually, they may represent part of a continuum of skin repair and anti-inflammatory effects that collectively manifest as the significant improvement captured by the primary endpoint at the final visit.
The safety profile of PPI mesotherapy was excellent. The incidence of AEs was low and not significantly different from the no-treatment control group. The few AEs deemed possibly related to the treatment were localized, transient, and expected reactions to the injection procedure itself (eg, erythema, peeling), rather than a systemic or allergic reaction to the product. The absence of serious AEs, infections, or other significant complications reinforces the safety of this therapeutic approach for facial application.
PPI for skin conditions and aesthetic purposes are not recognized as standard therapies in major dermatological guidelines, and there is no consensus regarding their use. Although studies on microneedle patches and nanovesicle delivery system of PPI have been conducted, showing increased skin hydration, elasticity, and reduced wrinkle depth after topical or transdermal application, further high-quality and rigorous studies are needed to define their role, optimal dosing, and long-term efficacies.33–35
This study has several strengths, including its randomized controlled design, multicenter nature, and use of objective, quantitative endpoints. However, some limitations should be acknowledged. The open-label design could have introduced potential bias in subjective assessments, although the primary endpoint was objective. The control group did not receive a sham injection, which means we cannot entirely disentangle the effects of the PPI from the potential effects of the mesotherapy procedure (microneedling) itself. However, microneedling alone is generally associated with an initial increase in inflammation, making it less likely to be the sole driver of the observed reduction in hemoglobin.21 Future studies should incorporate a double-blind, sham-controlled design to further elucidate these effects. Additionally, a longer follow-up period would be valuable to assess the durability of the treatment effect and to monitor for any delayed structural improvements in the skin.
Conclusion
This trial demonstrates that three sessions of mesotherapy with placenta polypeptide injection over a 60-day period effectively reduce objective signs of skin inflammation and lead to significant overall aesthetic improvement in patients with moderate-to-severe sensitive skin. The treatment was safe and well-tolerated. These findings position PPI mesotherapy as a valuable new modality in the therapeutic armamentarium for sensitive skin, addressing the core inflammatory component of the condition.
Abbreviations
AEs, Adverse Events; CMH, Cochran-Mantel-Haenszel; FAS, Full Analysis Set; GAIS, Global Aesthetic Improvement Scale; HPE, Human Placental Extract; ITT, Intention-to-Treat; LAST, Lactic Acid Sting Test; NF-κB, Nuclear Factor-kappa B; PPS, Per-Protocol Set; PPI, Placenta Polypeptide Injection; SD, Standard Deviation; SS, Sensitive Skin; Safety Set; TRPV1, Transient Receptor Potential Vanilloid 1.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Qiu-ning Sun, upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The study protocol (TPDT-001, Version 4.0, January 2, 2024) and informed consent forms were approved by the independent ethics committee at Peking Union Medical College Hospital (No. I-24PJ0085). Written informed consent was obtained from all participants prior to their enrollment in the study.
Consent for Publication
Written informed consent for the publication of their clinical details and/or clinical images was obtained from the participants. A copy of the consent form is available for review by the Editor of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. XH and QS provided the platform support.
Funding
This study was funded by Guizhou Taibang Biological Products Co., Ltd. Platform was supported by Beijing Key Clinical Specialty Construction Project and National Key Clinical Specialty Project of China.
Disclosure
Guizhou Taibang Biological Products Co., Ltd. served as the sponsor of the study, providing the study product and research funding. The sponsor was not involved in the study design, data collection, data analysis, interpretation of data, or in writing the manuscript. The authors declare that they have no other competing interests in this work.
References
1. Misery L, Ständer S, Szepietowski JC, et al. Definition of sensitive skin: an expert position paper from the special interest group on sensitive skin of the international forum for the study of itch. Acta dermato-venereologica. 2017;97(1):4–11. doi:10.2340/00015555-2397
2. Duarte I, Silveira J, Hafner MFS, Toyota R, Pedroso DMM. Sensitive skin: review of an ascending concept. Anais brasileiros de dermatologia. 2017;92(4):521–525. doi:10.1590/abd1806-4841.201756111
3. Misery L, Loser K, Ständer S. Sensitive skin. J European Acad Dermatol Venereol. 2016;30 Suppl 1:2–8. doi:10.1111/jdv.13532
4. He L, Zheng J, Ma H, et al. Chinese expert consensus on the diagnosis and treatment of sensitive skin. Chin J Dermatovenerol. 2017;31:1–4.
5. Farage MA. The prevalence of sensitive skin. Front Med. 2019;6:98. doi:10.3389/fmed.2019.00098
6. Misery L, Jean-Decoster C, Mery S, Georgescu V, Sibaud V. A new ten-item questionnaire for assessing sensitive skin: the sensitive scale-10. Acta dermato-venereologica. 2014;94(6):635–639. doi:10.2340/00015555-1870
7. Inamadar AC, Palit A. Sensitive skin: an overview. Indian J Dermatol Venereol Leprol. 2013;79(1):9–16. doi:10.4103/0378-6323.104664
8. Brazzini B, Ghersetich I, Hercogova J, Lotti T. The neuro-immuno-cutaneous-endocrine network: relationship between mind and skin. Dermatol Ther. 2003;16(2):123–131. doi:10.1046/j.1529-8019.2003.01621.x
9. Buhé V, Vié K, Guéré C, et al. Pathophysiological study of sensitive skin. Acta Dermato Venereolog. 2016;96(3):314–318. doi:10.2340/00015555-2235
10. Shirolkar P, Mishra SK. Role of TRP ion channels in pruritus. Neurosci Lett. 2022;768:136379. doi:10.1016/j.neulet.2021.136379
11. Gwam C, Ohanele C, Hamby J, Chughtai N, Mufti Z, Ma X. Human placental extract: a potential therapeutic in treating osteoarthritis. Ann Translat Med. 2023;11(9):322. doi:10.21037/atm.2019.10.20
12. Chang PY, Chin LC, Kimura K, Nakahata Y. Human placental extract activates a wide array of gene expressions related to skin functions. Sci Rep. 2022;12(1):11031. doi:10.1038/s41598-022-15270-y
13. Ghoneum M, El-Gerbed MSA. Human placental extract ameliorates methotrexate-induced hepatotoxicity in rats via regulating antioxidative and anti-inflammatory responses. Cancer Chemother Pharmacol. 2021;88(6):961–971. doi:10.1007/s00280-021-04349-4
14. Bak DH, Na J, Choi MJ, et al. Anti‑apoptotic effects of human placental hydrolysate against hepatocyte toxicity in vivo and in vitro. Int J Mol Med. 2018;42(5):2569–2583. doi:10.3892/ijmm.2018.3830
15. Yamauchi A, Kamiyoshi A, Koyama T, et al. Placental extract ameliorates non-alcoholic steatohepatitis (NASH) by exerting protective effects on endothelial cells. Heliyon. 2017;3(9):e00416. doi:10.1016/j.heliyon.2017.e00416
16. Lee TH, Park DS, Jang JY, et al. Human placenta hydrolysate promotes liver regeneration via activation of the cytokine/growth factor-mediated pathway and anti-oxidative effect. Biol Pharm Bull. 2019;42(4):607–616. doi:10.1248/bpb.b18-00712
17. Wu T, He J, Yan S, et al. Human placental extract suppresses mast cell activation and induces mast cell apoptosis. Allergy Asthma Clin Immunol. 2023;19(1):98. doi:10.1186/s13223-023-00850-y
18. Manzoor T, Farooq N, Sharma A, et al. Exosomes in nanomedicine: a promising cell-free therapeutic intervention in burn wounds. Stem Cell Res Ther. 2024;15(1):355. doi:10.1186/s13287-024-03970-3
19. Guizhou Taibang Biological Products Co Ltd. Internal report: pharmacodynamic study of placental polypeptide injection in an OXA-induced atopic dermatitis mouse model. China: Guizhou Taibang Biological Products Co. Ltd.; 2023.
20. Lacarrubba F, Tedeschi A, Nardone B, Micali G. Mesotherapy for skin rejuvenation: assessment of the subepidermal low-echogenic band by ultrasound evaluation with cross-sectional B-mode scanning. Dermatol Ther. 2008;21 Suppl 3:S1–5. doi:10.1111/j.1529-8019.2008.00234.x
21. El-Domyati M, El-Ammawi TS, Moawad O, et al. Efficacy of mesotherapy in facial rejuvenation: a histological and immunohistochemical evaluation. Int J Dermatol. 2012;51(8):913–919. doi:10.1111/j.1365-4632.2011.05184.x
22. Kandhari R, Kaur I, Sharma D. Mesococktails and mesoproducts in aesthetic dermatology. Dermatol Ther. 2020;33(6):e14218. doi:10.1111/dth.14218
23. Hendawy AF, Aly DG, Shokeir HA, Samy NA. Comparative study between the efficacy of long-pulsed neodymium- YAG laser and fractional Co2 laser in the treatment of striae distensae. J Lasers Med Sci. 2021;12(1):e57. doi:10.34172/jlms.2021.57
24. DiBernardo GA, DiBernardo BE. Prediction of treatment outcomes for neck rejuvenation utilizing a unique classification system of treatment approach using a 1440-nm side-firing laser. Aesthetic Surg J. 2018;38(suppl_2):S43–s51. doi:10.1093/asj/sjy066
25. Lim TS, Liew S, Tee XJ. Chong I: polynucleotides HPT for Asian skin regeneration and rejuvenation. Clin Cosmet Invest Dermatol. 2024;17:417–431. doi:10.2147/CCID.S437942
26. Narins RS, Brandt F, Leyden J, Lorenc ZP, Rubin M, Smith S. A randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane versus Zyplast for the correction of nasolabial folds. Dermatol Surg. 2003;29(6):588–595. doi:10.1046/j.1524-4725.2003.29150.x
27. Fullerton A, Fischer T, Lahti A, Wilhelm KP, Takiwaki H, Serup J. Guidelines for measurement of skin colour and erythema. A report from the standardization group of the European society of contact dermatitis. Contact Dermatitis. 1996;35(1):1–10. doi:10.1111/j.1600-0536.1996.tb02258.x
28. Turner CG, Miller JT, Otis JS, Hayat MJ, Quyyumi AA, Wong BJ. Cutaneous sensory nerve-mediated microvascular vasodilation in normotensive and prehypertensive non-hispanic blacks and whites. Physiol Reports. 2020;8(9):e14437. doi:10.14814/phy2.14437
29. Katayoshi T, Yamaura N, Nakajo T, Kitajima N, Tsuji-Naito K. Porcine placental extract increase the cellular NAD levels in human epidermal keratinocytes. Sci Rep. 2022;12(1):19040. doi:10.1038/s41598-022-23446-9
30. Kwon TR, Oh CT, Choi EJ, et al. Human placental extract exerts hair growth-promoting effects through the GSK-3β signaling pathway in human dermal papilla cells. Int J Mol Med. 2015;36(4):1088–1096. doi:10.3892/ijmm.2015.2316
31. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two Phase 3 trials of dupilumab versus placebo in atopic dermatitis. New Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
32. Žmitek K, Žmitek J, Hristov H, Rogl Butina M, Keršmanc P, Pogačnik T. The effects of dietary supplementation with collagen and vitamin C and their combination with hyaluronic acid on skin density, texture and other parameters: a randomised, double-blind, placebo-controlled trial. Nutrients. 2024;16(12):1908. doi:10.3390/nu16121908
33. Tansathien K, Ngawhirunpat T, Rangsimawong W, Patrojanasophon P, Opanasopit P, Nuntharatanapong N. In vitro biological activity and in vivo human study of porcine-placenta-extract-loaded nanovesicle formulations for skin and hair rejuvenation. Pharmaceutics. 2022;14(9):1846. doi:10.3390/pharmaceutics14091846
34. Tansathien K, Suriyaamporn P, Ngawhirunpat T, Opanasopit P, Rangsimawong W. A novel approach for skin regeneration by a potent bioactive placental-loaded microneedle patch: comparative study of deer, goat, and porcine placentas. Pharmaceutics. 2022;14(6):1221. doi:10.3390/pharmaceutics14061221
35. Pintea A, Manea A, Pintea C, et al. Peptides: emerging candidates for the prevention and treatment of skin senescence: a review. Biomolecules. 2025;15(1):88. doi:10.3390/biom15010088
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.