Back to Journals » Patient Preference and Adherence » Volume 17
Safety and Efficacy of Dexamethasone Intravitreal Implant Given Either First-Line or Second-Line in Diabetic Macular Edema
Authors Taloni A, Coco G ![]() , Rastelli D, Buffon G, Scorcia V
, Rastelli D, Buffon G, Scorcia V ![]() , Giannaccare G
, Giannaccare G
Received 31 August 2023
Accepted for publication 6 December 2023
Published 12 December 2023 Volume 2023:17 Pages 3307—3329
DOI https://doi.org/10.2147/PPA.S427209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Andrea Taloni,1,* Giulia Coco,2,* Davide Rastelli,3 Giacinta Buffon,2 Vincenzo Scorcia,1 Giuseppe Giannaccare4
1Department of Ophthalmology, University “Magna Graecia” of Catanzaro, Catanzaro, Italy; 2Department of Clinical Sciences and Translational Medicine, University of Rome Tor Vergata, Rome, Italy; 3Department of Ophthalmology, Policlinico Casilino, Rome, Italy; 4Eye Clinic, Department of Surgical Sciences, University of Cagliari, Cagliari, Italy
*These authors contributed equally to this work
Correspondence: Giuseppe Giannaccare, Full Professor of Ophthalmology, Eye Clinic, Department of Surgical Sciences, University of Cagliari, Via Università 40, Cagliari, 09124, Italy, Tel +0039 09613647041, Fax +0039 09613647094, Email [email protected]
Abstract: Diabetic macular edema (DME) is a common sight-threatening complication of diabetic retinopathy (DR) and the leading cause of severe visual impairment among the working-age population. Several therapeutic options are available for the management of DME, including intravitreal corticosteroids. They have been traditionally used as second-line treatment, due to the risk of intraocular pressure increase and cataract-related adverse events. However, attention has recently been focused on the primary or early use of intravitreal corticosteroids, due to growing evidence of the crucial role of inflammation in the pathogenesis of DME. Furthermore, intravitreal steroid implants offer the additional advantage of a longer duration of action compared to anti-vascular endothelial growth factor agents (anti-VEGF). This review aims to summarize the available evidence on the efficacy and safety profile of dexamethasone (DEX) intravitreal implant, with a specific focus on clinical scenarios in which it might be considered or even preferred as first-line treatment option by adequate selection of patients, considering both advantages and possible adverse events. Patients with contraindications to anti-VEGF, DME with high inflammatory OCT biomarkers, pseudophakic patients and phakic patients’ candidates to cataract surgery as well as vitrectomized eyes may all benefit from first-line DEX implant. Additionally, DME not responders to anti-VEGF should be considered for a switch to DEX implant and a combination therapy of DEX implant and anti-VEGF could be a valid option in severe and persistent DME.
Keywords: diabetic macular edema, DME, dexamethasone intravitreal implant, DEX implant, corticosteroids, Ozurdex
Introduction
Diabetic retinopathy (DR) affects about one-third of diabetic population and represents the main cause of visual disability and blindness among the working-age population in developed countries.1,2 Among sight-threatening complications of DR, diabetic macular edema (DME) is the most frequent cause of vision loss, with an estimated global prevalence among diabetic patients varying between 1.4% and 12.8%, influenced by the type of diabetes, race, ethnicity, and disease duration.3 Diabetic macular edema is characterized by the accumulation of exudative fluid intraretinally and, less commonly, subretinally, with consequent retinal thickening within the macular area.4 This condition can cause decreased vision, metamorphopsia, impaired color perception and, if prolonged, visual loss due to irreversible retinal damage.
Several therapeutic options are currently available for the management of DME, including intravitreal anti-vascular endothelial growth factor (VEGF) agents, intravitreal corticosteroids, laser photocoagulation and surgery. In 2017, the European Society of Retina Specialists (EURETINA) guidelines recommended intravitreal anti-VEGF agents as first-line treatment in patients with DME, and intravitreal steroids as second-choice treatment.5 Indeed, although many studies demonstrated the non-inferiority of intravitreal dexamethasone (DEX) implant (Ozurdex®; Allergan, Inc., Irvine, CA, United States) compared to anti-VEGF agents in terms of efficacy, the former is considered a second-line choice for DME, mainly due to the relatively higher risk of ocular side effects, particularly intraocular pressure (IOP)-related and cataract-related adverse events (AEs).5 However, it was also pointed out that intravitreal steroids may be the first-line option in patients with a history of recent cardiovascular events, pregnant or breast-feeding women as well as those not keen on undergoing monthly injections.5 In addition, recent literature focused on specific subgroups of patients aiming to identify those who might benefit more from early or first-line treatment with steroids, for instance vitrectomized eyes, pseudophakic eyes and/or non-compliant patients.6–8
Currently, DEX and fluocinolone acetonide (FA) implants are available and approved for intravitreal administration in DME. DEX intravitreal implant has been developed first and its use in patients with DME was approved by FDA and EMA in 2014. To date, it represents the first option when an intravitreal steroid is needed.6
The purpose of this review is to describe the efficacy and safety profile of DEX intravitreal implant, highlighting clinical scenarios in which it might be considered or even preferred as first-line treatment option.
Methods
Literature search was conducted on PubMed, Web of Science, Scopus, and Google Scholar using the following keywords: diabetic macular edema/oedema or DME/DMO; dexamethasone implant; DEX implant; Ozurdex; intravitreal steroids; intravitreal steroid implant; switching; poor response; cataract surgery; vitrectomized eyes; and combinations of them.
Randomized controlled trials (RCTs), large real-life studies, meta-analyses and systematic reviews assessing efficacy and safety of intravitreal DEX implant were included in this review. With regard to specific topics for which RCT was not available, for instance the comparison of DEX implant in vitrectomized versus non-vitrectomized eyes, prospective and retrospective studies were also included. The references of the examined articles were further investigated for additional publications. Only articles published in English were considered for our review (Figure 1). All authors had the opportunity to make suggestions and comments to achieve a consensus on the collected data, in agreement with the literature evidence. A summary of results from clinical trials involving patients affected by DME who received DEX implant has been reported in Table 1. The risk of bias assessment has been summarized in Figure 2.
 |
Table 1 Design and Results of Clinical Studies Involving Patients Affected by Diabetic Macular Edema Who Received Dexamethasone Intravitreal Implant |
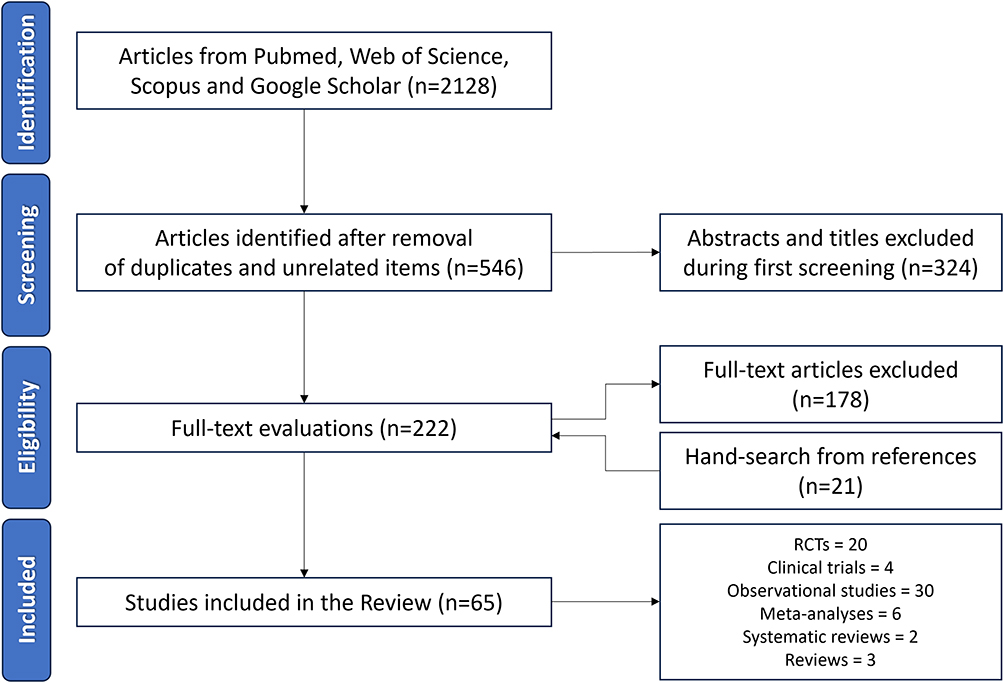 |
Figure 1 Preferred Reporting Items for a Systematic Review and Meta-Analyses (PRISMA) flowchart for the article selection process. |
 |
Figure 2 Risk of bias assessment for clinical studies involving patients affected by diabetic macular edema (DME) who received dexamethasone (DEX) intravitreal implant. Notes: D1, randomization process; D2, deviations from the intended interventions; D3, missing outcome data; D4, measurement of the outcome; D5, selection of the reported result; “+”, low risk; “!”, some concerns; “–”, high risk. |
Rationale for DEX Implant Use in DME
Inflammation is a pivotal pathogenetic factor in DME development and maintenance.28 Several pro-inflammatory mediators are over-expressed in the vitreous and humor aqueous of patients with DR: angiogenic factors, cytokines, chemokines, complement and coagulation cascade proteins, proteins involved in ROS production, etc.29,30
Intravitreal corticosteroids, due to their anti-inflammatory and anti-edematous effects, can well counteract the multifaceted pathways involved in the pathogenesis of DME, and may therefore be a high-performance treatment option in the therapeutic armamentarium of DME. In particular, corticosteroids inhibit phospholipase A2 and arachidonic acid pathways, reduce the VEGF expression and suppress the activity of inflammatory cytokines, thereby stabilizing the blood-retinal barrier, blocking the leukostasis, enhancing density and activity of tight junctions in the retinal capillary endothelium, ameliorating retinal oxygenation and preventing endothelial cell injury and apoptosis.31,32
Several optical coherence tomography (OCT) imaging biomarkers have been identified for DME and used to make diagnosis, monitor, and provide prognostic information on both disease progression and potential responses to different treatments.30,33 In addition, some of these biomarkers are considered to correlate with intraocular inflammation levels and responsiveness to anti-VEGF and steroid therapy.34
In summary, the OCT-biomarkers identified so far are the following:
- Increased retinal thickness: result of the intraretinal and/or sub-retinal accumulation of fluid, but also intracellular edema. This OCT parameter is commonly used in clinical studies to define cutoff for eligibility to a certain treatment, evaluate the activity as well as the course of the disease, and treatment response.35 However, central macular thickness (CMT) poorly correlates with BCVA, especially in long-standing DME.36
- Intraretinal cystoid spaces: due to intraretinal fluid accumulation; size, location, and chronicity have been associated with functional prognosis in diabetic eyes.37
- Hyperreflective retinal foci (HRF): intraretinal dots in the inner or outer retinal layer showing similar reflectivity to the retinal nerve fiber layer, diameter <30 μm and absence of back-shadowing. It has been hypothesized that these dots may represent extravasated lipoproteins or aggregates of activated microglial cells,38 and that they are strictly linked to inflammation.39
- Hyperreflective cystoid walls: consisting of collagen-like material or gliotic tissues; usually detected in association with HRF, hyperreflective cystoid walls are considered a sign of increased inflammatory activity.40
- Exudates: located within the outer retinal layers, showing similar reflectivity to the RPE–Bruch’s membrane complex, characterized by a size >30 μm and by the presence of back-shadowing. They are associated with lipid levels and other systemic risk factors.41
- Disorganization of retinal inner layers (DRIL): disorganization or destruction of cells within the inner retinal layers; it is a negative prognostic factor for visual outcome in eyes with DME.42
- Disorganization of Retinal Outer Layer (DROL): damage of the outer retinal layers, particularly of the photoreceptor outer segment, correlates with poor visual prognosis and macular ischemia.43
- Subfoveal subretinal fluid (SRF): due to the disruption of the external limiting membrane that allows fluid and protein to migrate to the subretinal space. It is a sign of inflammation and a biomarker for functional and anatomical treatment response.44
- Central choroidal thickness (CCT): a consequence of both increased luminal and stromal structures, it also can be correlated with the presence of subretinal fluid. CCT usually increases during DR progression and its reduction after treatment can be used as a predictive biomarker of treatment response.45
- Vitreomacular interface: mechanical traction on the fovea is correlated to a worse prognosis and may suggest a surgical add-on therapy.46
As anticipated above, large intraretinal cystoid spaces and HRF have been associated with a significant inflammatory component that, therefore, may suggest favorable treatment response to corticosteroids.47 It has been recently suggested that large intraretinal cysts (≥250 µm), DRIL, HRF and SRF in chronic DME may be OCT biomarkers to select candidates for intravitreal steroids as first-line treatment.33,47
Randomized Controlled Trials Supporting the Use of DEX in DME
The first RCT evaluating the efficacy and safety of DEX implant in patients with macular edema was conducted in 2007: 315 patients with persistent macular edema due to different etiologies were randomized to either receive a single 0.7 mg or 0.35 mg DEX implant injection or to be observed for 6 months.9 The analysis of the subgroup of 171 patients with DME confirmed the superiority of DEX implant 0.7 mg in terms of proportion of patients achieving ≥10-letters and ≥15-letters BCVA improvement as well as anatomical improvement, suggesting a dose–response relationship.10 Similarly, the proportion of patients showing a significant reduction in both fluorescein leakage and central retinal thickness (CRT) was higher in the DEX implant 0.7 mg group.10
In 2014, the MEAD studies represented the registration trials for DEX implant in patients with DME, and were designed as two randomized, multicenter, masked, sham-controlled, Phase III trials with identical protocol.11 A total of 1048 patients with center involving DME were randomized to receive either 0.7 mg or 0.35 mg of DEX implant or a sham procedure and followed up for 3 years. Percentage of patients with ≥15-letter improvement in BCVA and average CRT reduction were significantly higher in the DEX implant groups (always p < 0.02).
RCTs also compared the efficacy of DEX implant with laser photocoagulation therapy, which was considered the standard of care for DME for almost 30 years. Specifically, the PLACID trial demonstrated the superiority of 0.7 mg DEX implant plus laser photocoagulation versus laser photocoagulation alone in terms of BVCA gain at 1- and 9-month follow-up (FU) (31.7% vs 11%, p < 0.001, and 31.7% vs 17.3%, p = 0.007, respectively), but not at 12-month FU. Central macular thickness (CMT) reduction and decrease of the area of vascular leakage were also greater in the DEX implant plus laser group.12 Later on, the OZLASE clinical trial compared the efficacy and safety of combined repeated DEX implant plus macular laser therapy (MLT) and MLT only in 80 patients with center involving DME over a 1-year period. Although the CST decrease was higher in the combination group (p < 0.001), no difference in BCVA improvement was noted between groups (p > 0.05).
More recently, DEX implant was compared to laser photocoagulation by Wei et al, in a phase III RCT including 284 Chinese and Filipino patients with DME.14 The BCVA gain was significantly higher for DEX implant (p = 0.001); however, the proportion of patients with BCVA improvement ≥15 letters did not differ significantly between groups (p > 0.05). Both CRT reduction and decrease in the leakage area on FA were significantly higher in the DEX implant group at 12 months.14
DEX Intravitreal Implant and Anti-VEGF Injections for DME
Dexamethasone vs Anti-VEGF
The BEVORDEX study was the first RCT comparing anti-VEGF injections and DEX implant for DME treatment;15,48 88 eyes were randomized to receive either bevacizumab or DEX implant for 24 months. No difference was found in terms of BCVA gain at 2 years in pseudophakic eyes, and results remained similar at 5 years.49 Although significantly higher CRT reduction in the DEX implant group was noted at 12 months (187 µm vs 122 µm in the bevacizumab group; p = 0.015), this became not significant at both 2 and 5 years.48,49 At 5 years, eyes initially randomized to receive DEX implant had significantly fewer treatments but were more likely to develop proliferative diabetic retinopathy (PDR) compared to eyes initially randomized to bevacizumab.49
Subsequently, a multicenter, randomized study by Callanan et al evaluated the non-inferiority of DEX implant compared to ranibizumab in 363 eyes with DME.16 DEX implant matched the prespecified noninferiority criteria of BCVA gain at 12 months, which was defined as a mean BCVA change within 5 ETDRS letters compared to ranibizumab, even if BCVA gain was significantly higher in the ranibizumab group (7.6 vs 4.3 ETDRS letters, p < 0.05). In addition, Sharma et al did not find statistically significant differences between DEX implant and anti-VEGF (bevacizumab or ranibizumab) in terms of BCVA change in 40 naïve eyes with DME;17 while better anatomical results were observed in the DEX implant group in a short follow-up of 3 months. Similar better anatomical results were found by Ozsaygili et al comparing DEX implant with aflibercept in treatment-naive patients with DME and inflammatory biomarkers over a 12-month FU, showing a significantly higher mean CRT reduction in the DEX group (p < 0.05). In their study functional results favored the aflibercept group, however, this superiority ceased to exist when considering pseudophakic eyes only, with the advantage of a lower number of injections in the DEX implant group.18
The INVICTUS study, a real-life study comparing intravitreal ranibizumab (RAN), aflibercept (AFL) and dexamethasone on naïve patients with DME, did not show significant differences among treatments both in BCVA gain (DEX = +9.4 letters; RAN = +7.2; AFL = +8.5) and CRT reduction (DEX = −162.7 μm; RAN = −99.3 μm; AFL = −101.5 μm).19
A few meta-analyses also compared the effectiveness and safety of DEX implant and VEGF-inhibitors in DME treatment. He et al found comparable visual acuity improvements and CMT reduction at 12 months, with fewer injections in the DEX implant group. However, authors stated that visual acuity benefit could not be fully reflected in the DEX implant group due to cataract progression, and therefore recommended DEX implant as first-line therapy only in selected cases.6 Kodjikian et al reviewed only observational studies evaluating the efficacy of anti-VEGF and DEX implant. Although reaching similar final BCVA (62 and 61.2 for anti-VEGF and DEX implant respectively), the reported BCVA gain from baseline was + 4.7 letters in the anti-VEGF group and + 9.6 letters in DEX implant group. However, only the naïve status appeared to confer the best functional response in the DEX-implant studies. The authors suggested this difference could be partially explained by the lower baseline BCVA in patients receiving the DEX implant or the less frequency of anti-VEGF injections in real-life observational studies compared to interventional ones.50
More recently, two additional meta-analyses were conducted. Chi et al51 included 2409 eyes and showed no significant differences between anti-VEGF and DEX implant in terms of BCVA improvement from the pooled analysis of non-resistant eyes (mean difference = 0.00). Similarly, Patil et al included fourteen RCTs for a total of 827 eyes, reporting no significant difference in BCVA gain at 3, 6 and 12 months (p = 0.11, p = 0.21 and p = 0.24, respectively) as well as at final follow-up (p = 0.91). Significantly lower retinal thickness at 3 and 6 months (p = 0.04 and p < 0.00001 respectively) and final follow-up (weighted mean difference of 39.99 μm, p = 0.002) were noted in the DEX implant group; however, no significant difference was reported at 12 months (p = 0.18).52
Dexamethasone in DME Refractory to Anti-VEGF
Resistance to anti-VEGF therapy is a major concern in DME management, and DEX implant has been used as alternative or adjuvant therapy in eyes with no satisfactory DME regression after at least three anti-VEGF injections.53
In 2016, Totan et al evaluated the efficacy of DEX implant in 30 eyes with chronic DME resistant to at least 3 bevacizumab injections. Significant improvements in BCVA and CRT were noted at 1 and 3 months; however, such improvements were not sustained over time and tended to decrease between the third and sixth months after the injection.20 Similar results were found in other studies, with BCVA improvements at 6 months in about one-fourth of the patients.21 These results were consistent with other reports: Shah et al reported comparable visual acuity improvement at 7 months comparing intravitreal bevacizumab monotherapy and DEX implant monotherapy for persistent DME; however, reduced CRT and fewer injections in the DEX implant group were noted;22 Thomas et al in a contralateral eye-to-eye comparison showed no differences in BCVA change at 3 months between the eye that continued with ranibizumab injections and the eye that switched to DEX implant; CRT reduction, although similar in both eyes, reached statistical significance compared to baseline in the DEX implant treated eye only.23
Interestingly, Busch et al evaluated 110 eyes with refractory DME in a real-world setting, showing that eyes that were switched to DEX implant had better visual and anatomical outcomes at 12 months compared to those that continued treatment with anti-VEGF therapy.24
More recently, a report by Koc et al confirmed the absence of any difference in BCVA and CMT in 94 eyes with DME resistant to ranibizumab or aflibercept injections, which either continued with the anti-VEGF or switched to DEX implant.25
Lately, a systematic review and meta-analysis revealed the DEX implant to be associated with significantly greater BCVA improvement and CRT decrease compared to anti-VEGF therapy in resistant DME (mean difference = 0.12 [95% CI, 0.02–0.21] and 65.37 [95% CI, 3.62–127.13] respectively) with, however, high heterogeneity between included studies.51
DEX implant has also been used as adjuvant therapy in refractory DME. A Diabetic Retinopathy Clinical Research Network (DRCR.net) study Protocol U, a Phase II multicenter randomized clinical trial, explored the role of adjunctive therapy with Ozurdex in 129 eyes with persistent DME after at least 3 ranibizumab injections.26 DEX implant (65 eyes) or sham injection (64 eyes) was added to monthly ranibizumab protocol. No differences in BCVA were found between groups, as mean (SD) improvement at 24 weeks was +2.7 (9.8) letters in the DEX implant plus ranibizumab group, and +3.0 (7.1) in the ranibizumab only group (p = 0.73). However, the anatomical outcome favored the combination group (−110 μm vs −62 μm; p < 0.001) and the percentage of DME resolution was 52% in the DEX implant plus ranibizumab group vs 31% in the ranibizumab only group.
Considering DME refractory to a large number of intravitreal injections, a recent non-randomized interventional study explored the potential role of DEX implant in a small sample of such eyes.54 Six eyes with failed clinical response after a mean of 43.5 (range 15–58) prior anti-VEGF injections, and all with failed aflibercept, underwent DEX implant plus a breakthrough anti-VEGF injection when required. At 1 year, the mean BCVA improved from 0.475 to 0.375 logMAR and central subfield thickness (CST) reduced from 386.5 to 315 μm. The authors concluded that DEX implant appeared effective in eyes with DME refractory to multiple intravitreal injections, with excellent anatomic improvement and modest visual improvement.
Simultaneous DEX Implant and Anti-VEGF for DME
Besides studies evaluating the efficacy of DEX implant in comparison or sequential to anti-VEGF treatments, a few studies explored the efficacy of the simultaneous administration of DEX implant and anti-VEGF for the treatment of DME. Although being small-sized studies, results seem to suggest the superiority of such simultaneous combined treatment compared to VEGF inhibitors alone, with a favorable visual and anatomic outcome and an acceptable safety profile.27,55–57
Kaya et al assessed the efficacy and safety of simultaneously administered DEX implant and ranibizumab in comparison with ranibizumab only as the first-line treatment of DME in 68 eyes (34 in each group) with follow-up at 12 and 24 months.27,57 At both time-points, the simultaneous double protocol therapy significantly improved the visual outcomes (+21.6 vs +9.6 letters in the ranibizumab only group at 12 months, p < 0.001; and +20.2 vs +9.1 at 24 months), with 65.4% of patients in the simultaneous double protocol group gaining ≥15 ETDRS letters from baseline (vs 26.2% in ranibizumab only group; p < 0.001). Moreover, FT reduced more in the simultaneous double protocol group at 12 months (−413 µm vs −282 µm; p = 0.001) and at 24 months (−394 µm vs −275 µm; p < 0.05); and inflammatory OCT biomarkers improved more in the simultaneous double protocol group at both 12 and 24 months. However, IOP elevations of ≥5mmHg were more frequent in the simultaneous double protocol group (38% vs 18%; p = 0.012), as well as cataract progression (27% vs 12.5%; p = 0.032). Overall, the simultaneous double protocol resulted an effective first-line treatment option for DME with inflammatory OCT biomarkers or/and decreased visual acuity.27,57
Economic Considerations on DEX Implant and Anti-VEGF for DME
A relevant concern regarding DME involves treatment costs. Simultaneous therapy with DEX implant and anti-VEGF may be justified by outcome improvements; however, health authorities have not yet approved such combination protocols. The current trend is to minimize the frequency of intravitreal injections. Monthly protocols for anti-VEGF injections have significantly reduced in popularity, and the new standard of care is now represented by treat-and-extend protocols, which can reduce economic burden, while maintaining similar degree of efficacy.58
Treatments with intravitreal corticosteroids require even fewer injections, and a recent study suggested that switching to DEX implant after the first 3-monthly anti-VEGF injections may be more cost-effective than extending the treatment to 6-monthly injections.59 However, longer-acting anti-VEGF drugs, such as brolucizumab or faricimab, have been recently produced, which still need to be compared to DEX implant for the purpose of cost-efficiency.60–62
Ocular Adverse Events in DEX Implant vs Anti-VEGF
Beyond their therapeutic effect, steroids are able to bind tissues, inducing various effects on cell proliferation, transmembrane transport and reactive oxygen species activity.63 Water solubility intensely impacts the wash-out time of intravitreal drugs and the exposure time is considered a key factor in determining the steroid-binding properties to intraocular tissues.64 Among steroids approved for intravitreal use, dexamethasone is the most soluble in water, due to its reduced lipophilicity, thus showing faster clearance compared to other intravitreal steroids;28 thus, it is not surprising that DEX implant showed a lower incidence of intraocular adverse events compared to triamcinolone acetonide and FA.65,66
Intravitreal steroids showed particular affinity for lens and trabecular meshwork cells and this may explain the high incidence of cataract worsening and IOP increase.65 For instance, it has been demonstrated that dexamethasone may interfere with pivotal pathways which regulate lens cell homeostasis, migration and differentiation.67 Moreover, dexamethasone showed to increase the stiffness of trabecular meshwork cells in vitro, by inducing over-expression of contractile proteins and synthesis of extracellular matrix.68 In addition, the accumulation of steroid molecules in the trabecular meshwork may determine increase in intraocular volume and obstruction due to precipitation which also play a role in IOP elevation.65
The incidence of adverse events is largely variable among studies (Table 2).11,31,65,69–72
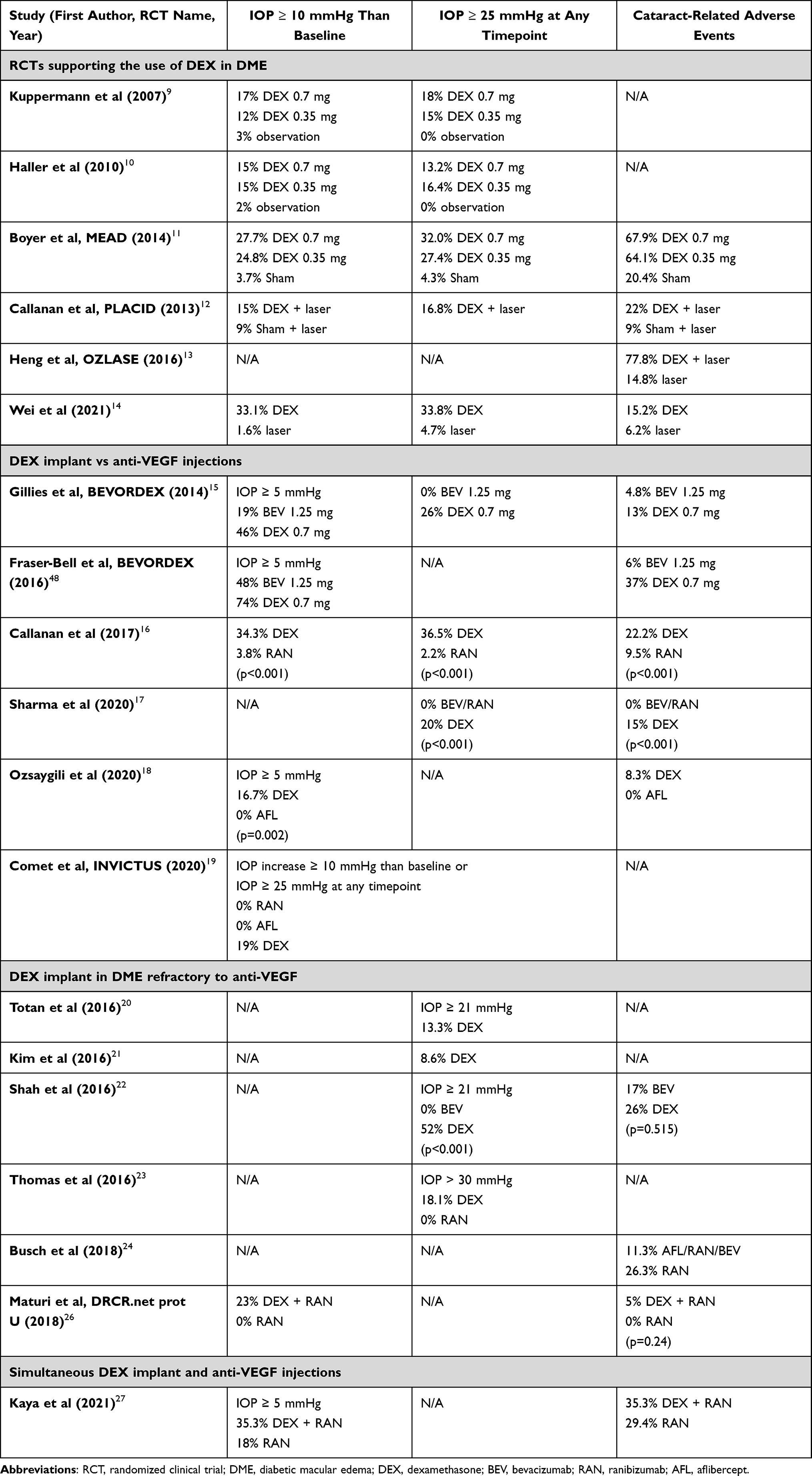 |
Table 2 Adverse Events of Clinical Studies Involving Patients Affected by Diabetic Macular Edema Who Received Dexamethasone Intravitreal Implant |
In the MEAD registration trial for Ozurdex,11,69 the percentages of IOP-related adverse events were 36.0%, 34.1% and 5.1% in the DEX implant 0.7 mg, 0.35mg, and sham groups, respectively; 6.6% of patients in the DEX implant 0.7 mg (the approved dose) group experienced a measured IOP ≥ 35 mmHg, compared to 0.9% in the sham group. IOP rises were usually managed with IOP-lowering drops or no treatment, and only 0.6% of patients in the 0.7mg group required glaucoma surgery. There was no cumulative effect of repeated dexamethasone implants on IOP, as the incidence and level of IOP elevations did not increase over time, nor the proportion of patients using IOP-lowering medications over the 3-year observation time. Cataract-related adverse events in phakic eyes were 67.9%, 64.1%, and 20.4% in the DEX implant 0.7 mg, 0.35 mg, and sham groups, respectively. However, cataract surgery successfully restored vision without further complications.11
Additionally, a more recent large study on the safety of over 6000 intravitreal dexamethasone implants reported a frequency of 26.5% of eyes developing IOP ≥ 25 mmHg during follow-up, with only 0.5% requiring glaucoma surgery, and 32.5% requiring cataract surgery, with an additional 14.6% experiencing not-significant cataract worsening.72
Compared to other steroids approved for intravitreal use, a systematic review and meta-analysis reported an incidence of increased IOP in 11–15% of patients treated with dexamethasone implants (0.35 and 0.7 mg doses, respectively), significantly lower compared to the 32% of 4mg triamcinolone acetonide, and 66–79% with FA implants (0.59 mg and 2.1 mg doses, respectively).65
Other ocular side effects of dexamethasone implant are relatively rare and mostly related to the surgical procedure rather than to the drug itself. Endophthalmitis (sterile or not), retinal detachment, vitreous hemorrhage, implant dislocation in the anterior chamber, conjunctival hyperemia or hemorrhage have been reported in some studies, generally with an incidence lower than 1%.72,73
Many studies reported higher number of eyes which underwent cataract surgery in DEX implant groups compared to anti-VEGF groups. However, literature reports conflicting results regarding cataract development rates, with some studies showing significant differences, while others do not.6,16,17,22,26,48,49,52 In the BEVORDEX study, 37% of patients treated with DEX implant underwent cataract surgery at 24 months, compared to 6% of patients in the bevacizumab group, and similar rates were found by Callanan et al16,48 He et al reported higher incidence of cataract-related AEs in the DEX implant group compared to the anti-VEGF group (RR = 2.68, p = 0.0005)6 and the risk of developing cataract was even higher in a recent meta-analysis of RCTs (OR = 4.70, p = 0.0002).74 Conversely, Patil et al did not find differences in cataract-related AEs between DEX implant and anti-VEGF in their systematic review and meta-analysis.52 Actual differences between DEX implant and anti-VEGF drugs in terms of cataract progression rates remain unclear, probably due to differences in follow-up times, protocols and proportions of pseudophakic patients at baseline among studies. Despite this, phakic status remains one of the most important factors to consider, and anti-VEGF still represents the first-line treatment in phakic patients with DME.5
A Cochrane meta-analysis of two clinical trials demonstrated that the need for IOP-lowering therapy increased more than 4 times with DEX implant compared to anti-VEGF, with moderate-certainty evidence,16,48 and these results were consistent with those of He et al (RR = 4.14; 95% CI, 1.89–8.65; p = 0.0002)6 and Patil et al.52 The INVICTUS study showed a significantly higher proportion of patients with IOP ≥ 25 mmHg or an increase of ≥10 mmHg in the DEX implant group compared to the aflibercept or ranibizumab group.19 In addition, 23% of eyes that switched to DEX implant plus ranibizumab experienced an increase ≥10 mmHg compared to 0% of eyes in the ranibizumab only group in the DRCR.net protocol U,26 and similar percentages were also reported by Sharma et al.17 A recent meta-analysis of RCTs also reported higher incidence of high IOP following DEX implant compared to anti-VEGF (OR = 13.77, p < 0.00001).74 Surprisingly, recent meta-analysis by Chi et al did not reveal significant difference in IOP change between DEX implant group and anti-VEGF group (MD = −0.42).51
Overall, intravitreal dexamethasone has an excellent systemic safety profile. Its slow-release technology and the intravitreal route of administration allow to achieve the maximum therapeutic concentration into the vitreous body and the minimum systemic absorption, limiting the incidence of systemic adverse events.75 In clinical trials, the incidence of systemic AEs after Ozurdex administration is extremely rare and usually with no differences compared to sham treatments.11 Compared to anti-VEGF agents, DEX implant offers a better systemic safety profile and is indicated as first-line treatment in patients at high risk for cardiovascular events, in which anti-VEGF is contraindicated.5
DEX Implant vs FA Implant for DME
The FA implant presents different pharmacokinetics compared to the DEX implant: in its current formulation, it releases 0.2 μg of FA/day, maintaining a steady-state concentration over a longer period of 36 months; however, peak functional and anatomical efficacy is achieved more slowly, usually 6 months after implantation.76
Both RCTs and real-life studies have provided insights about the efficacy and safety profiles of the FA implant.77–79 In the phase 3 trials FAME A and B, Campochiaro et al compared the effect of 0.2 μg/day (low dose) or 0.5 μg/day (high dose) FA implants on subjects with persistent DME. After a period of 2 years, both the low and high dose FA implants significantly improved both BCVA (mean changes of +4.4 and +5.4 letters, respectively; p = 0.02 and p = 0.016 vs sham) and foveal thickness (mean changes of −168 μm and −177 μm, respectively; p = 0.005 and p < 0.001 vs sham); however, the safety profile was more favorable towards the low-dose insert, with significantly lower incidence of glaucoma and cataract surgery.78
In the PALADIN study, a Phase 4, nonrandomized, open-label observational study,77 Singer et al analyzed the functional and anatomical outcomes of 202 eyes during a follow-up period of 36 months, reporting a mean BCVA change of +3.61 letters (p = 0.02) and a mean CST change of −60.69 μm (p < 0.0001) compared with baseline.77 These positive results were confirmed in a meta-analysis of real-world studies by Fallico et al.80
Retrospective observational studies were conducted to evaluate the efficacy, safety and timing for switching FA implant to DEX implant.81,82 Baillif et al reported results of 113 eyes switched to FA implant after a mean time of 11.12 ± 22 weeks. BCVA improved from 54.1 to 59.8 letters at month 4 and remained stable during the observation period. A significant reduction was noted in CMT, with a minimum of 320.9 μm at month 3. Finally, a mean IOP remained below 19 mmHg at all evaluated timepoints. A longer time between the last DEX and the first FA implant was a risk factor for additional treatments; however, no significant outcome differences were reported between eyes that received their last DEX implant either less than or more than 8 weeks prior to switching to FA implant.81
More recently, in the ILUVI1MOIS study, 41 pseudophakic eyes with chronic DME (time to recurrence ≤6 months) were switched to FA implant 1 month after the last DEX implant. BCVA and CMT remained stable during a follow-up of at least 6 months (mean 13.1 ± 4.4 months), with 14% of patients requiring additional treatments at 12 months. The mean IOP at month 12 did not differ significantly from that measured at baseline.82
According to a retrospective study by Cicinelli et al, the anatomical outcomes and IOP elevation of FA implant seem to be predicted by the previous response to DEX implant; however, no significant relationship was found between BCVA improvement after DEX and after FA.83
To our knowledge, only one study by Coelho et al directly compared the effectiveness and safety of the FA and DEX implants for the treatment of DME. However, the sample size was limited, and the follow-up time between the two groups was different.84 Comparing the outcomes of FA and DEX implants is challenging because of the different pharmacokinetics of the two drugs.
Overall, switching from DEX to FA implants is effective and safe, and can be justified in patients who might not respond adequately to DEX implant, who obtained only short-term improvements or who are willing to undergo a lower number of injections. Notably, FDA has approved the use of FA implant for DME patients who previously underwent DEX implant, as long as they did not experience a significant increase in IOP.81
DEX Implant in Diabetic Eyes Undergoing Cataract Surgery
Diabetic patients, especially those with type 2 diabetes, have a higher risk of developing early cataracts,85 with an incidence almost two-fold higher compared to non-diabetic subjects (20.4 vs 10.8 per 1000 person/years).86 In fact, chronic hyperglycemia causes increased oxidative stress and non-enzymatic glycation of eye lens proteins that may precipitate the formation of cataract.87 As a result, cataract surgery is often necessary. Among complications after cataract surgery, post-cataract macular edema (PCME) has an incidence after uncomplicated surgeries ranging between 0.1% and 2.3% which, however, can be significantly higher in diabetic patients, reaching values around 16.3% in patients with DR and/or previous DME, with a risk proportional to the severity of DR, mainly due to a compromised blood-retinal barrier even before the surgery.88–91
Chronic and persistent DME represents the major risk factor for edema worsening after cataract surgery, owing to the combination of chronic inflammation in DR and surgery-related inflammation. Therefore, performing intravitreal dexamethasone implant injection at the same time of cataract surgery would be a safe and effective option for treating both diabetic and post-cataract edema.92
Several studies showed the beneficial effects of DEX implant in eyes with DME undergoing cataract surgery. In the MEAD study, the subgroup of eyes that underwent phacoemulsification during the follow-up period experienced an increase in CRT after cataract surgery in the sham group, but not in the DEX implant group, suggesting a protective role of DEX implant following cataract surgery.11 Subsequently, Panozzo et al evaluated the role of DEX implant at the time of cataract surgery in reducing DME worsening. However, with no control group, their results showed that intraoperative DEX implant was effective in preventing DME worsening after phacoemulsification with maximum efficacy at 4–8 weeks after the injection and lasting for at least 3 months.93 A control group was included in the retrospective-comparative study conducted by Furino et al on diabetic patients with DME and cataract,94 which showed that phacoemulsification combined with DEX implant (phaco-DEX group) had better functional and tomographic outcomes compared to standard phacoemulsification (phaco-alone group). Specifically, BCVA improved significantly after surgery in the phaco-DEX group (p = 0.0005), while no significant changes were noted in the phaco-alone group. Similarly, CST was significantly lower in the phaco-DEX group compared to the phaco-alone group.94
In this context, compared to anti-VEGF therapy, DEX implant seems to better antagonize the inflammatory storm that comes from DME pathogenesis and after cataract surgery. A recent meta-analysis conducted by Fallico et al found that cataract surgery combined with DEX implant showed a 3-month mean change in CMT of −98.35 µm, significantly higher compared to cataract surgery combined with anti-VEGF therapy (−21.61 µm; p < 0.001). However, no differences were found in visual gain between the two groups (p = 0.13).95
The protective effect of DEX implant after cataract surgery is compatible with the well-known effects of the preoperative prophylaxis with topical steroids and nonsteroidal anti-inflammatory drugs. Laursen et al conducted a meta-analysis of 6 RCTs with nearly 900 patients to compare prophylactic interventions with (1) nonsteroidal anti-inflammatory drugs (NSAIDs) alone or in combination with topical steroids, (2) depot and topical steroids, and (3) anti-VEGF alone or in combination with topical steroids. Intravitreal corticosteroids showed similar protective effect against macular edema in comparison to both topical steroids alone and to topical steroids in combination with NSAIDs.96
A series of studies were carried out to establish the optimal timing of DEX implant in diabetic patients undergoing cataract surgery. Barone et al compared DEX implant administered either 1 month before or at the time of cataract surgery in 40 patients with treatment naïve DME; in a twenty-week follow-up, no difference was found in terms of visual acuity gain or anatomical outcomes between the two groups.97 A larger retrospective study with similar design was conducted on 221 patients with cataract and DME.98 BCVA gain was comparable between groups, but better anatomical results were noticed in the group receiving DEX implant at the time of cataract surgery (p < 0.001). Lastly, Corbelli et al, in a sample of 40 eyes with DME and cataract, found that DEX implant injection performed at the time of cataract surgery achieved similar long-term anatomical and functional outcomes compared to a 1-month deferred injection.99
Even if there is no general agreement about the optimal timing of DEX implant (before, during, or after cataract surgery), the combination of the two procedures may protect against the acute surgical-induced inflammation, potentially preventing short-term subclinical damages and may decrease the burden of the number of visits and examinations.99 Therefore, consensus statements of experts recommend the use of DEX implant in patients with DME at the time of phacoemulsification to prevent the surgery-related inflammatory load and to protect from potential decompensation of DME.100,101
DEX Implant in Vitrectomized Eyes with Macular Edema
Persistent vitreous hemorrhages and tractional retinal detachment are well-known complications of proliferative diabetic retinopathy (PDR), and pars plana vitrectomy (PPV) is the only available therapy to treat these sight-threatening conditions; therefore, it is not uncommon for patients with PDR to undergo PPV during their lifetime.102,103 Interestingly, in addition to its main mechanical effect, PPV has shown several secondary positive effects on the course of diabetic retinopathy: for instance, it reduces the concentration of pro-inflammatory cytokines and VEGF near the macular area,104 improves the oxygen diffusion to the ischemic inner retinal layers,105 and accelerates the washout from the vitreous cavity of signaling molecules involved in diabetic retinopathy progression.106 Due to the chronic nature of PDR, as well as the potential pro-inflammatory effect of the surgery itself, even patients who undergo PPV may show DME development or worsening.104
Management of DME in vitrectomized patients may be challenging; vitreous replacement with other media may alter the pharmacokinetic profile of intravitreal drugs, thus limiting their beneficial effects.107 According to the law of Stokes-Einstein, molecular transport by diffusion or convection is inversely related to the viscosity of the medium,105 and in saline solution diffusion results quicker than in vitreous humor.108 Previous studies demonstrated that several molecules such as anti-VEGF agents, antibiotics and triamcinolone acetonide have faster clearance in vitrectomized eyes,109–111 which may result in a reduction of their efficacy in vivo.112 DEX implant, due to its slow-release properties, has shown long-lasting clearance even in patients who underwent PPV, showing no differences in efficacy on DME treatment comparing vitrectomized and non-vitrectomized eyes.113–117
The CHAMPLAIN study was the first designed to evaluate the efficacy of a single injection of 0.7 mg DEX implant in a cohort of 55 patients with a history of PPV and refractory DME.113 A significant reduction of CCT was noticed at week 8 (−156 μm; p < 0.001) and maintained at 26 weeks (39 μm; p=0.004); similarly, BCVA significantly improved at week 8 (+6.0 letters; p < 0.001) and maintained at 26 weeks (+3.0 letters; p = 0.046) with an acceptable safety profile. Maximum efficacy was seen at week 8 after injection.113
Many subsequent studies explored the differences in DME treatment efficacy between eyes with and without previous PPV. Medeiros et al compared BCVA and foveal thickness in 58 patients with refractory DME (24 vitrectomized and 34 non-vitrectomized) which received DEX implant with a follow-up of 6 months.114 Both groups showed significant improvements in BCVA and foveal thickness, with no significant difference between treatment groups at any time point (1, 3 and 6 months). Later, Bastakis et al evaluated the efficacy and duration of action of DEX implant in 18 eyes with persistent DME after anti-VEGF injection. Ten out of 18 eyes were vitrectomized.115 Each eye received 1 to 3 injections and was followed-up for 6 to 18 months. No difference in BCVA and CMT variations after dexamethasone injections were observed between vitrectomized and non-vitrectomized eyes and DEX implant showed its maximum efficacy within the first 3 months of implantation. A further observational, retrospective, real-life study including 186 eyes (59 vitrectomized and 127 non-vitrectomized) showed no difference in BCVA gain and CMT decrease between groups, with a similar intraocular pressure profile. Although no difference was noted in the overall number of injections, the mean interval between injections was significantly shorter in vitrectomized eyes (5.2 vs 6.9 months in non-vitrectomized eyes; p = 0.001).116 The same group also analyzed a small sample of 15 eyes with macular edema secondary to different conditions, including diabetes, that received DEX implant both before and after PPV, with each eye acting as its own control.116 No significant differences in CMT reduction, BCVA improvement, number of injections required, interval between the injections and IOP profile were noticed before and after PPV.116
Recently, the VITDEX study, a multicenter, retrospective, interventional study, investigated the effect of DEX implant in 236 eyes with DME with or without previous PPV with a follow-up of 12 months; 130 eyes were vitrectomized and 106 were non-vitrectomized.117 Both groups showed improvements in BCVA and CST with no statistically significant difference between groups. In addition, no differences were found in the number of DEX implants, the need for additional treatments and the proportion of patients who underwent cataract surgery or started IOP-lowering medications during the follow-up period. Thus, the authors concluded that both efficacy and safety of DEX implant were not influenced by PPV.
Finally, a systematic review and meta-analysis including 7 retrospective studies with a total of 582 eyes (374 non-vitrectomized and 208 vitrectomized) and a follow-up ranging from 4 to 26 months showed no significant difference between groups in terms of BCVA improvement, CMT reduction, number of injections and number or magnitude of adverse events at 1, 3, 6 and 12 months; however, the duration of action of DEX implant was significantly shorter in vitrectomized eyes, with a mean difference of 0.8 months (p = 0.005), confirming that vitreous removal may accelerate drug clearance after injections. However, this difference was not deemed clinically relevant.8
Conclusion
The EURETINA guidelines recognized the importance of corticosteroids in the treatment armamentarium of DME; however, they were largely defined on a second-choice level compared to anti-VEGF, mainly due to the relatively higher risk of ocular side effects.5
More recent literature and expert recommendations using a Delphi approach have partially moved beyond these guidelines, suggesting the use of DEX implant as a viable first-line treatment option in pseudophakic patients and recommending its use as first-choice in vitrectomized eyes, given the better pharmacokinetic profile in this setting compared to anti-VEGF.101,118,119
Furthermore, DEX implant could also be the preferred choice in phakic patient candidates for cataract surgery, by protecting from potential decompensation of previous DME,101,118–120 and in patients with DME with high inflammatory component, evaluated through the presence of inflammatory OCT biomarkers (large intraretinal cysts, DRIL, HRF and SRF).33,101,118,119,121 Additionally, in patients not responding to anti-VEGF injections, clinicians should consider switching to DEX implant after the loading dose of 3–6 consecutive anti-VEGF injections, while patients with severe and persistent DME can benefit from a combination of DEX implant and anti-VEGF (Figure 3).101,118
 |
Figure 3 Flowchart summarizing possible determinants in patient selection for DEX implant in DME. |
Conversely, exclusion criteria for the administration of the DEX implant include torn or ruptured posterior lens capsule, due to the risk of implant migration in the anterior chamber, as well as glaucoma and intraocular hypertension. In these cases, anti-VEGF injections should be preferred.
Overall, when appropriate, using DEX implant as first-line treatment option in the real-world setting can facilitate treatment compliance by reducing the number of injections and visits, potentially improving treatment outcomes.19,24,101
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015;2(1). doi:10.1186/S40662-015-0026-2
2. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/DC11-1909
3. Tan GS, Cheung N, Simó R, Cheung GCM, Wong TY. Diabetic macular oedema. Lancet Diabetes Endocrinol. 2017;5(2):143–155. doi:10.1016/S2213-8587(16)30052-3
4. Zhang J, Zhang J, Zhang C, et al. Diabetic Macular Edema: current Understanding, Molecular Mechanisms and Therapeutic Implications. Cells. 2022;11(21). doi:10.3390/CELLS11213362
5. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the Management of Diabetic Macular Edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
6. He Y, Ren XJ, Hu BJ, Lam WC, Li XR. A meta-analysis of the effect of a dexamethasone intravitreal implant versus intravitreal anti-vascular endothelial growth factor treatment for diabetic macular edema. BMC Ophthalmol. 2018;18(1). doi:10.1186/S12886-018-0779-1
7. Hussain RM, Ciulla TA. Treatment strategies for refractory diabetic macular edema: switching anti-VEGF treatments, adopting corticosteroid-based treatments, and combination therapy. Expert Opin Biol Ther. 2016;16(3):365–374. doi:10.1517/14712598.2016.1131265
8. Yuan Q, Liu Y, Gou Y, et al. Efficacy and safety of the dexamethasone implant in vitrectomized and nonvitrectomized eyes with diabetic macular edema: a systematic review and meta-analysis. Front Pharmacol. 2022;13:1029584. doi:10.3389/FPHAR.2022.1029584/FULL
9. Kuppermann BD, Blumenkranz MS, Haller JA, et al. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007;125(3):309–317. doi:10.1001/ARCHOPHT.125.3.309
10. Haller JA, Kuppermann BD, Blumenkranz MS, et al. Randomized controlled trial of an intravitreous dexamethasone drug delivery system in patients with diabetic macular edema. Arch Ophthalmol. 2010;128(3):289–296. doi:10.1001/ARCHOPHTHALMOL.2010.21
11. Boyer DS, Yoon YH, Belfort R, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914. doi:10.1016/J.OPHTHA.2014.04.024
12. Callanan DG, Gupta S, Boyer DS, et al. Dexamethasone intravitreal implant in combination with laser photocoagulation for the treatment of diffuse diabetic macular edema. Ophthalmology. 2013;120(9):1843–1851. doi:10.1016/J.OPHTHA.2013.02.018
13. Heng LZ, Sivaprasad S, Crosby-Nwaobi R, et al. A prospective randomised controlled clinical trial comparing a combination of repeated intravitreal Ozurdex and macular laser therapy versus macular laser only in centre-involving diabetic macular oedema (OZLASE study). Br J Ophthalmol. 2016;100(6):802–807. doi:10.1136/BJOPHTHALMOL-2015-307136
14. Wei W, Chen Y, Hu B, et al. Multicenter, Prospective, Randomized Study of Dexamethasone Intravitreal Implant in Patients with Center-Involved Diabetic Macular Edema in the Asia-Pacific Region. Clin Ophthalmol. 2021;15:4097–4108. doi:10.2147/OPTH.S325618
15. Gillies MC, Lim LL, Campain A, et al. A randomized clinical trial of intravitreal bevacizumab versus intravitreal dexamethasone for diabetic macular edema: the BEVORDEX study. Ophthalmology. 2014;121(12):2473–2481. doi:10.1016/J.OPHTHA.2014.07.002
16. Callanan DG, Loewenstein A, Patel SS, et al. A multicenter, 12-month randomized study comparing dexamethasone intravitreal implant with ranibizumab in patients with diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2017;255(3):463–473. doi:10.1007/S00417-016-3472-1
17. Sharma A, Bellala K, Dongre P, Reddy P. Anti-VEGF versus dexamethasone implant (Ozurdex) for the management of Centre involved Diabetic Macular Edema (CiDME): a randomized study. Int Ophthalmol. 2020;40(1):67–72. doi:10.1007/S10792-019-01151-3
18. Ozsaygili C, Duru N. Comparison Of Intravitreal Dexamethasone Implant And Aflibercept In Patients With Treatment-Naive Diabetic Macular Edema With Serous Retinal Detachment. Retina. 2020;40(6):1044–1052. doi:10.1097/IAE.0000000000002537
19. Comet A, Gascon P, Ramtohul P, Donnadieu B, Denis D. INVICTUS: intravitreal anti-VEGF and dexamethasone implant comparison for the treatment of diabetic macular edema: a 12 months follow-up study. Eur J Ophthalmol. 2021;31(2):754–758. doi:10.1177/1120672120930603
20. Totan Y, Güler E, Güraʇaç FB. Dexamethasone Intravitreal Implant for Chronic Diabetic Macular Edema Resistant to Intravitreal Bevacizumab Treatment. Curr Eye Res. 2016;41(1):107–113. doi:10.3109/02713683.2014.1002048
21. Kim M, Cho YJ, Lee CH, Lee SC. Effect of intravitreal dexamethasone implant on retinal and choroidal thickness in refractory diabetic macular oedema after multiple anti-VEGF injections. Eye. 2016;30(5):718–725. doi:10.1038/EYE.2016.23
22. Shah SU, Harless A, Bleau L, Maturi RK. Prospective Randomized Subject-Masked Study Of Intravitreal Bevacizumab Monotherapy Versus Dexamethasone Implant Monotherapy In The Treatment Of Persistent Diabetic Macular Edema. Retina. 2016;36(10):1986–1996. doi:10.1097/IAE.0000000000001038
23. Thomas BJ, Yonekawa Y, Wolfe JD, Hassan TS. Contralateral eye-to-eye comparison of intravitreal ranibizumab and a sustained-release dexamethasone intravitreal implant in recalcitrant diabetic macular edema. Clin Ophthalmol. 2016;10:1679–1684. doi:10.2147/OPTH.S110789
24. Busch C, Zur D, Fraser-Bell S, et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018;55(8):789–796. doi:10.1007/S00592-018-1151-X
25. Koc H, Alpay A, Ugurbas SH. Comparison of the efficacy of intravitreal Anti-VEGF versus intravitreal dexamethasone implant in treatment resistant diabetic Macular Edema. BMC Ophthalmol. 2023;23(1):1–7. doi:10.1186/S12886-023-02831-6/TABLES/4
26. Maturi RK, Glassman AR, Liu D, et al. Effect of Adding Dexamethasone to Continued Ranibizumab Treatment in Patients With Persistent Diabetic Macular Edema: a DRCR Network Phase 2 Randomized Clinical Trial. JAMA Ophthalmol. 2018;136(1):29. doi:10.1001/JAMAOPHTHALMOL.2017.4914
27. Kaya M, Kocak N, Ozturk T, Bolluk V, Ayhan Z, Kaynak S. Intravitreal ranibizumab and dexamethasone implant injections as primary treatment of diabetic macular edema: simultaneously double protocol. Eye. 2021;35(3):777–785. doi:10.1038/S41433-020-0949-2
28. Whitcup SM, Cidlowski JA, Csaky KG, Ambati J. Pharmacology of Corticosteroids for Diabetic Macular Edema. Invest Ophthalmol Vis Sci. 2018;59(1):1–12. doi:10.1167/IOVS.17-22259
29. Loukovaara S, Nurkkala H, Tamene F, et al. Quantitative Proteomics Analysis of Vitreous Humor from Diabetic Retinopathy Patients. J Proteome Res. 2015;14(12):5131–5143. doi:10.1021/ACS.JPROTEOME.5B00900
30. Vujosevic S, Simó R. Local and Systemic Inflammatory Biomarkers of Diabetic Retinopathy: an Integrative Approach. Invest Ophthalmol Vis Sci. 2017;58(6):BIO68–BIO75. doi:10.1167/IOVS.17-21769
31. Bucolo C, Gozzo L, Longo L, Mansueto S, Vitale DC, Drago F. Long-term efficacy and safety profile of multiple injections of intravitreal dexamethasone implant to manage diabetic macular edema: a systematic review of real-world studies. J Pharmacol Sci. 2018;138(4):219–232. doi:10.1016/J.JPHS.2018.11.001
32. Urbančič M, Topčić IG. Dexamethasone implant in the management of diabetic macular edema from clinician’s perspective. Clin Ophthalmol. 2019;13:821–828. doi:10.2147/OPTH.S206769
33. Munk MR, Somfai GM, de Smet MD, et al. The Role of Intravitreal Corticosteroids in the Treatment of DME: predictive OCT Biomarkers. Int J Mol Sci. 2022;23(14). doi:10.3390/IJMS23147585
34. Vujosevic S, Toma C, Villani E, et al. Diabetic macular edema with neuroretinal detachment: OCT and OCT-angiography biomarkers of treatment response to anti-VEGF and steroids. Acta Diabetol. 2020;57(3):287–296. doi:10.1007/S00592-019-01424-4
35. Cao J, You K, Jin K, et al. Prediction of response to anti-vascular endothelial growth factor treatment in diabetic macular oedema using an optical coherence tomography-based machine learning method. Acta Ophthalmol. 2021;99(1):e19–e27. doi:10.1111/AOS.14514
36. Chawan-Saad J, Wu M, Wu A, Wu L. Corticosteroids for Diabetic Macular Edema. Taiwan J Ophthalmol. 2019;9(4):233–242. doi:10.4103/TJO.TJO_68_19
37. Suciu CI, Suciu VI, Nicoara SD. Optical Coherence Tomography (Angiography) Biomarkers in the Assessment and Monitoring of Diabetic Macular Edema. J Diabetes Res. 2020;2020:550. doi:10.1155/2020/6655021
38. Lee H, Jang H, Choi YA, Kim HC, Chung H. Association Between Soluble CD14 in the Aqueous Humor and Hyperreflective Foci on Optical Coherence Tomography in Patients With Diabetic Macular Edema. Invest Ophthalmol Vis Sci. 2018;59(2):715–721. doi:10.1167/IOVS.17-23042
39. Midena E, Pilotto E, Bini S. Hyperreflective Intraretinal Foci as an OCT Biomarker of Retinal Inflammation in Diabetic Macular Edema. Invest Ophthalmol Vis Sci. 2018;59(13):5366. doi:10.1167/IOVS.18-25611
40. Framme C, Schweizer P, Imesch M, Wolf S, Wolf-Schnurrbusch U. Behavior of SD-OCT-detected hyperreflective foci in the retina of anti-VEGF-treated patients with diabetic macular edema. Invest Ophthalmol Vis Sci. 2012;53(9):5814–5818. doi:10.1167/IOVS.12-9950
41. Sasaki M, Kawasaki R, Noonan JE, Wong TY, Lamoureux E, Wang JJ. Quantitative measurement of hard exudates in patients with diabetes and their associations with serum lipid levels. Invest Ophthalmol Vis Sci. 2013;54(8):5544–5549. doi:10.1167/IOVS.13-11849
42. Sun JK, Lin MM, Lammer J, et al. Disorganization of the retinal inner layers as a predictor of visual acuity in eyes with center-involved diabetic macular edema. JAMA Ophthalmol. 2014;132(11):1309–1316. doi:10.1001/JAMAOPHTHALMOL.2014.2350
43. Forooghian F, Stetson PF, Meyer SA, et al. Relationship between photoreceptor outer segment length and visual acuity in diabetic macular edema. Retina. 2010;30(1):63–70. doi:10.1097/IAE.0B013E3181BD2C5A
44. Zur D, Iglicki M, Busch C, et al. OCT Biomarkers as Functional Outcome Predictors in Diabetic Macular Edema Treated with Dexamethasone Implant. Ophthalmology. 2018;125(2):267–275. doi:10.1016/J.OPHTHA.2017.08.031
45. Kim JT, Lee DH, Joe SG, Kim JG, Yoon YH. Changes in choroidal thickness in relation to the severity of retinopathy and macular edema in type 2 diabetic patients. Invest Ophthalmol Vis Sci. 2013;54(5):3378–3384. doi:10.1167/IOVS.12-11503
46. Sadiq MA, Soliman MK, Sarwar S, et al. Effect of Vitreomacular Adhesion on Treatment Outcomes in the Ranibizumab for Edema of the Macula in Diabetes (READ-3) Study. Ophthalmology. 2016;123(2):324–329. doi:10.1016/J.OPHTHA.2015.09.032
47. Castro-Navarro V, Monferrer-Adsuara C, Navarro-Palop C, Montero-Hernández J, Cervera-Taulet E. Effect of Dexamethasone Intravitreal Implant on Visual Acuity and Foveal Photoreceptor Integrity in Macular Edema Secondary to Retinal Vascular Disease. Ophthalmologica. 2021;244(1):83–92. doi:10.1159/000512195
48. Fraser-Bell S, Lim LL, Campain A, et al. Bevacizumab or Dexamethasone Implants for DME: 2-year Results (The BEVORDEX Study). Ophthalmology. 2016;123(6):1399–1401. doi:10.1016/J.OPHTHA.2015.12.012
49. Cornish EE, Teo KYC, Gillies MC, et al. Five-year outcomes of eyes initially enrolled in the 2-year BEVORDEX trial of bevacizumab or dexamethasone implants for diabetic macular oedema. Br J Ophthalmol. 2023;107(1):79–83. doi:10.1136/BJOPHTHALMOL-2021-319839
50. Kodjikian L, Bellocq D, Mathis T. Pharmacological Management of Diabetic Macular Edema in Real-Life Observational Studies. Biomed Res Int. 2018;2018:82. doi:10.1155/2018/8289253
51. Chi SC, Kang YN, Huang YM. Efficacy and safety profile of intravitreal dexamethasone implant versus antivascular endothelial growth factor treatment in diabetic macular edema: a systematic review and meta-analysis. Sci Rep. 2023;13(1). doi:10.1038/S41598-023-34673-Z
52. Patil NS, Mihalache A, Hatamnejad A, Popovic MM, Kertes PJ, Muni RH. Intravitreal Steroids Compared with Anti-VEGF Treatment for Diabetic Macular Edema: a Meta-Analysis. Ophthalmol Retina. 2023;7(4):289–299. doi:10.1016/J.ORET.2022.10.008
53. Wells JA. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203. doi:10.1056/NEJMOA1414264
54. Wilkins CS, Sobol EK, Lema GMC, Lee JG, Rosen RB, Deobhakta A. Intravitreal dexamethasone insert in diabetic macular edema super-refractory to anti-vascular endothelial growth factor therapy. Eur J Ophthalmol. 2022;32(5):NP37–NP41. doi:10.1177/11206721211004391
55. De Andrade FL. Simultaneous Therapy with Intravitreal Dexamethasone Implant and Bevacizumab for the Treatment of Macular Edema. Med Hypothesis Discov Innov Ophthalmol. 2016;5(1):4.
56. Saatci AO, Ayhan Z, Engin CD, Saatci AO, Ayhan Z, Engin CD. Simultaneous Intravitreal Ranibizumab and Dexamethasone Implant Administration at the Same Setting in Eyes with Severe Diabetic Macular Edema. Open J Ophthalmol. 2016;6(2):112–118. doi:10.4236/OJOPH.2016.62016
57. Kaya M, Atas F, Kocak N, Ozturk T, Ayhan Z, Kaynak S. Intravitreal Ranibizumab and Dexamethasone Implant Injections as Primary Treatment of Diabetic Macular Edema: the Month 24 Results from Simultaneously Double Protocol. Curr Eye Res. 2023;48(5):498–505. doi:10.1080/02713683.2023.2168013
58. Lim SY, Wong WM, Seah I, et al. Treat and extend regimen for diabetic macular oedema-a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2023;261(2):303–315. doi:10.1007/S00417-022-05770-Y
59. Ruiz-Moreno JM, Ruiz-Medrano J. Early-switch versus late-switch in patients with diabetic macular edema: a cost-effectiveness study. Graefe’s Arch Clin Exp Ophthalmol. 2023;261(4):941. doi:10.1007/S00417-022-05892-3
60. Liberski S, Wichrowska M, Kocięcki J. Aflibercept versus Faricimab in the Treatment of Neovascular Age-Related Macular Degeneration and Diabetic Macular Edema: a Review. Int J Mol Sci. 2022;23(16). doi:10.3390/IJMS23169424
61. Kuo BL, Singh RP. Brolucizumab for the treatment of diabetic macular edema. Curr Opin Ophthalmol. 2022;33(3):167–173. doi:10.1097/ICU.0000000000000849
62. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729–740. doi:10.1016/S0140-6736(22)00010-1
63. James ER. The etiology of steroid cataract. J Ocul Pharmacol Ther. 2007;23(5):403–420. doi:10.1089/JOP.2006.0067
64. Thakur A, Kadam R, Kompella UB. Trabecular meshwork and lens partitioning of corticosteroids: implications for elevated intraocular pressure and cataracts. Arch Ophthalmol. 2011;129(7):914–920. doi:10.1001/ARCHOPHTHALMOL.2011.39
65. Kiddee W, Trope GE, Sheng L, et al. Intraocular pressure monitoring post intravitreal steroids: a systematic review. Surv Ophthalmol. 2013;58(4):291–310. doi:10.1016/J.SURVOPHTHAL.2012.08.003
66. Bandello F, Toni D, Porta M, Varano M. Diabetic retinopathy, diabetic macular edema, and cardiovascular risk: the importance of a long-term perspective and a multidisciplinary approach to optimal intravitreal therapy. Acta Diabetol. 2020;57(5):513–526. doi:10.1007/S00592-019-01453-Z
67. Yoo WS, Seong H, Song C, et al. Role of Chondroitin Sulfate Proteoglycan 5 in Steroid-Induced Cataract. Cells. 2023;12(13):1705. doi:10.3390/CELLS12131705/S1
68. Raghunathan VK, Morgan JT, Park SA, et al. Dexamethasone Stiffens Trabecular Meshwork, Trabecular Meshwork Cells, and Matrix. Invest Ophthalmol Vis Sci. 2015;56(8):4447. doi:10.1167/IOVS.15-16739
69. Maturi RK, Pollack A, Uy HS, et al. Intraocular Pressure In Patients With Diabetic Macular Edema Treated With Dexamethasone Intravitreal Implant In The 3-Year Mead Study. Retina. 2016;36(6):1143–1152. doi:10.1097/IAE.0000000000001004
70. Rezkallah A, Mathis T, Abukhashabah A, et al. Long-Term Incidence And Risk Factors Of Ocular Hypertension Following Dexamethasone-Implant Injections: the Safodex-2 Study. Retina. 2021;41(7):1438–1445. doi:10.1097/IAE.0000000000003080
71. Mello Filho P, Andrade G, Maia A, et al. Effectiveness and Safety of Intravitreal Dexamethasone Implant (Ozurdex) in Patients with Diabetic Macular Edema: a Real-World Experience. Ophthalmologica. 2019;241(1):9–16. doi:10.1159/000492132
72. Rajesh B, Zarranz-Ventura J, Fung AT, et al. Safety of 6000 intravitreal dexamethasone implants. Br J Ophthalmol. 2020;104(1):39–46. doi:10.1136/BJOPHTHALMOL-2019-313991
73. Li X, Wang N, Liang X, et al. Safety and efficacy of dexamethasone intravitreal implant for treatment of macular edema secondary to retinal vein occlusion in Chinese patients: randomized, sham-controlled, multicenter study. Graefe’s Arch Clin Exp Ophthalmol. 2018;256(1):59. doi:10.1007/S00417-017-3831-6
74. Xiaodong L, Xuejun X. The Efficacy and Safety of Dexamethasone Intravitreal Implant for Diabetic Macular Edema and Macular Edema Secondary to Retinal Vein Occlusion: a Meta-Analysis of Randomized Controlled Trials. J Ophthalmol. 2022;2022:548. doi:10.1155/2022/4007002
75. Hosseini K, Matsushima D, Johnson J, et al. Pharmacokinetic study of dexamethasone disodium phosphate using intravitreal, subconjunctival, and intravenous delivery routes in rabbits. J Ocul Pharmacol Ther. 2008;24(3):301–308. doi:10.1089/JOP.2007.0117
76. Kodjikian L, Bandello F, de Smet M, et al. Fluocinolone acetonide implant in diabetic macular edema: international experts’ panel consensus guidelines and treatment algorithm. Eur J Ophthalmol. 2022;32(4):1890–1899. doi:10.1177/11206721221080288
77. Singer MA, Sheth V, Mansour SE, Coughlin B, Gonzalez VH. Three-Year Safety and Efficacy of the 0.19-mg Fluocinolone Acetonide Intravitreal Implant for Diabetic Macular Edema: the PALADIN Study. Ophthalmology. 2022;129(6):605–613. doi:10.1016/j.ophtha.2022.01.015
78. Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4). doi:10.1016/J.OPHTHA.2010.12.028
79. Mathis T, Papegaey M, Ricard C, et al. Efficacy and Safety of Intravitreal Fluocinolone Acetonide Implant for Chronic Diabetic Macular Edema Previously Treated in Real-Life Practice: the REALFAc Study. Pharmaceutics. 2022;14(4). doi:10.3390/PHARMACEUTICS14040723
80. Fallico M, Maugeri A, Lotery A, et al. Fluocinolone acetonide vitreous insert for chronic diabetic macular oedema: a systematic review with meta-analysis of real-world experience. Sci Rep. 2021;11(1). doi:10.1038/S41598-021-84362-Y
81. Baillif S, Staccini P, Weber M, et al. Management of Patients with Diabetic Macular Edema Switched from Dexamethasone Intravitreal Implant to Fluocinolone Acetonide Intravitreal Implant. Pharmaceutics. 2022;14(11). doi:10.3390/PHARMACEUTICS14112391
82. Rousseau N, Lebreton O, Masse H, et al. Fluocinolone Acetonide Implant Injected 1 Month after Dexamethasone Implant for Diabetic Macular Oedema: the ILUVI1MOIS Study. Ophthalmol Ther. 2023;12(5):2781–2792. doi:10.1007/S40123-023-00749-2
83. Cicinelli MV, Rosenblatt A, Grosso D, et al. The outcome of fluocinolone acetonide intravitreal implant is predicted by the response to dexamethasone implant in diabetic macular oedema. Eye. 2021;35(12):3232–3242. doi:10.1038/S41433-020-01373-1
84. Coelho J, Malheiro L, Beirão JM, Meireles A, Pessoa B. Real-world retrospective comparison of 0.19 mg fluocinolone acetonide and 0.7 mg dexamethasone intravitreal implants for the treatment of diabetic macular edema in vitrectomized eyes. Clin Ophthalmol. 2019;13:1751–1759. doi:10.2147/OPTH.S201611
85. Klein BEK, Klein R, Moss SE. Incidence of cataract surgery in the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Am J Ophthalmol. 1995;119(3):295–300. doi:10.1016/S0002-9394(14)71170-5
86. Becker C, Schneider C, Aballéa S, et al. Cataract in patients with diabetes mellitus-incidence rates in the UK and risk factors. Eye. 2018;32(6):1028–1035. doi:10.1038/S41433-017-0003-1
87. Kyselova Z, Stefek M, Bauer V. Pharmacological prevention of diabetic cataract. J Diabetes Complications. 2004;18(2):129–140. doi:10.1016/S1056-8727(03)00009-6
88. Chu CJ, Johnston RL, Buscombe C, Sallam AB, Mohamed Q, Yang YC. Risk Factors and Incidence of Macular Edema after Cataract Surgery: a Database Study of 81984 Eyes. Ophthalmology. 2016;123(2):316–323. doi:10.1016/J.OPHTHA.2015.10.001
89. Denniston AK, Chakravarthy U, Zhu H, et al. The UK Diabetic Retinopathy Electronic Medical Record (UK DR EMR) Users Group, Report 2: real-world data for the impact of cataract surgery on diabetic macular oedema. Br J Ophthalmol. 2017;101(12):1673–1678. doi:10.1136/BJOPHTHALMOL-2016-309838
90. Dowler JGF, Sehmi KS, Hykin PG, Hamilton AMP. The natural history of macular edema after cataract surgery in diabetes. Ophthalmology. 1999;106(4):663–668. doi:10.1016/S0161-6420(99)90148-3
91. Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Curr Opin Ophthalmol. 2012;23(1):26–32. doi:10.1097/ICU.0B013E32834CD5F8
92. Sze AM, Luk FO, Yip TP, Lee GK, Chan CK. Use of intravitreal dexamethasone implant in patients with cataract and macular edema undergoing phacoemulsification. Eur J Ophthalmol. 2015;25(2):168–172. doi:10.5301/EJO.5000523
93. Panozzo GA, Gusson E, Panozzo G, Dalla Mura G. Dexamethasone intravitreal implant at the time of cataract surgery in eyes with diabetic macular edema. Eur J Ophthalmol. 2017;27(4):433–437. doi:10.5301/EJO.5000920
94. Furino C, Boscia F, Niro A, et al. Diabetic Macular Edema And Cataract Surgery: phacoemulsification Combined With Dexamethasone Intravitreal Implant Compared With Standard Phacoemulsification. Retina. 2021;41(5):1102–1109. doi:10.1097/IAE.0000000000002974
95. Fallico M, Lotery A, Maugeri A, et al. Intravitreal dexamethasone implant versus anti-vascular endothelial growth factor therapy combined with cataract surgery in patients with diabetic macular oedema: a systematic review with meta-analysis. Eye. 2022;36(12):2239–2246. doi:10.1038/S41433-021-01847-W
96. Laursen SB, Erichsen JH, Holm LM, Kessel L. Prevention of macular edema in patients with diabetes after cataract surgery. J Cataract Refract Surg. 2019;45(6):854–869. doi:10.1016/J.JCRS.2019.04.025
97. Barone A, Russo V, Maggiore G, et al. Dexamethasone intravitreal implant in patients with cataract and naïve diabetic macular edema. Eur J Ophthalmol. 2022;32(1):364–371. doi:10.1177/11206721211004395
98. Fallico M, Avitabile T, Castellino N, et al. Intravitreal dexamethasone implant one month before versus concomitant with cataract surgery in patients with diabetic macular oedema: the dexcat study. Acta Ophthalmol. 2021;99(1):e74–e80. doi:10.1111/AOS.14516
99. Corbelli E, Fasce F, Iuliano L, et al. Cataract surgery with combined versus deferred intravitreal dexamethasone implant for diabetic macular edema: long-term outcomes from a real-world setting. Acta Diabetol. 2020;57(10):1193–1201. doi:10.1007/S00592-020-01509-5
100. Alessio G, Boscia F, Caporossi A, et al. Dexamethasone implants in patients with diabetic macular edema undergoing cataract surgery: Italian expert panel consensus statements. Eur J Ophthalmol. 2021;31(3):1122–1127. doi:10.1177/1120672120939500
101. García Layana A, Adán A, Ascaso FJ, et al. Use of intravitreal dexamethasone implants in the treatment of diabetic macular edema: expert recommendations using a Delphi approach. Eur J Ophthalmol. 2020;30(5):1042–1052. doi:10.1177/1120672119861623
102. Altan T, Acar N, Kapran Z, Unver YB, Ozdogan S. Transconjunctival 25-gauge sutureless vitrectomy and silicone oil injection in diabetic tractional retinal detachment. Retina. 2008;28(9):1201–1206. doi:10.1097/IAE.0B013E3181853D3C
103. Chaudhry NA. Early Vitrectomy for Severe Vitreous Hemorrhage in Diabetic Retinopathy: four-Year Results of a Randomized Trial: diabetic Retinopathy Study Report 5. Archives of Ophthalmology. 1990;108(7):958–964. doi:10.1001/archopht.1990.01070090060040
104. Laidlaw DAH. Vitrectomy for diabetic macular oedema. Eye. 2008;22(10):1337–1341. doi:10.1038/EYE.2008.84
105. Stefánsson E. Physiology of vitreous surgery. Graefes Arch Clin Exp Ophthalmol. 2009;247(2):147–163. doi:10.1007/S00417-008-0980-7
106. Yoshida S, Ishikawa K, Matsumoto T, Yoshida A, Ishibashi T, Kono T. Reduced concentrations of angiogenesis-related factors in vitreous after vitrectomy in patients with proliferative diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2010;248(6):799–804. doi:10.1007/S00417-010-1301-5
107. Beer PM, Bakri SJ, Singh RJ, Liu W, Peters GB, Miller M. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology. 2003;110(4):681–686. doi:10.1016/S0161-6420(02)01969-3
108. Gisladottir S, Loftsson T, Stefansson E. Diffusion characteristics of vitreous humour and saline solution follow the Stokes Einstein equation. Graefes Arch Clin Exp Ophthalmol. 2009;247(12):1677–1684. doi:10.1007/S00417-009-1141-3
109. Doft BH, Weiskopf J, Nilsson-Ehle I, Wingard LB. Amphotericin clearance in vitrectomized versus nonvitrectomized eyes. Ophthalmology. 1985;92(11):1601–1605. doi:10.1016/S0161-6420(85)33838-1
110. Chin HS, Park TS, Moon YS, Oh JH. Difference in clearance of intravitreal triamcinolone acetonide between vitrectomized and nonvitrectomized eyes. Retina. 2005;25(5):556–560. doi:10.1097/00006982-200507000-00002
111. Yanyali A, Aytug B, Horozoglu F, Nohutcu AF. Bevacizumab (Avastin) for diabetic macular edema in previously vitrectomized eyes. Am J Ophthalmol. 2007;144(1):124–126. doi:10.1016/J.AJO.2007.02.048
112. Chen YY, Chen PY, Chen FT, Chen YJ, Wang JK. Comparison of efficacy of intravitreal ranibizumab between non-vitrectomized and vitrectomized eyes with diabetic macular edema. Int Ophthalmol. 2018;38(1):293–299. doi:10.1007/S10792-017-0462-1
113. Boyer DS, Faber D, Gupta S, et al. Dexamethasone intravitreal implant for treatment of diabetic macular edema in vitrectomized patients. Retina. 2011;31(5):915–923. doi:10.1097/IAE.0B013E318206D18C
114. Medeiros MD, Alkabes M, Navarro R, Garcia-Arumí J, Mateo C, Corcóstegui B. Dexamethasone intravitreal implant in vitrectomized versus nonvitrectomized eyes for treatment of patients with persistent diabetic macular edema. J Ocul Pharmacol Ther. 2014;30(9):709–716. doi:10.1089/JOP.2014.0010
115. Bastakis GG, Dimopoulos D, Stavrakakis A, Pappas G. Long-term efficacy and duration of action of dexamethasone implant, in vitrectomised and non-vitrectomised eyes with persistent diabetic macular oedema. Eye. 2019;33(3):411–418. doi:10.1038/S41433-018-0219-8
116. Rezkallah A, Malclès A, Dot C, et al. Evaluation of Efficacy and Safety of Dexamethasone Intravitreal Implants of Vitrectomized and Nonvitrectomized Eyes in a Real-World Study. J Ocul Pharmacol Ther. 2018;34(8):596–602. doi:10.1089/JOP.2018.0007
117. Iglicki M, Busch C, Lanzetta P, et al. Vitrectomized vs non-vitrectomized eyes in DEX implant treatment for DMO-Is there any difference? The VITDEX study. Eye. 2023;37(2):280–284. doi:10.1038/S41433-022-01931-9
118. Giovannini A, Parravano M, Ricci F, Bandello F. Management of diabetic macular edema with intravitreal dexamethasone implants: expert recommendations using a Delphi-based approach. Eur J Ophthalmol. 2019;29(1):82–91. doi:10.1177/1120672118781236
119. Kodjikian L, Baillif S, Couturier A, et al. Recommendations for the management of diabetic macular oedema with intravitreal dexamethasone implant: a national Delphi consensus study. Eur J Ophthalmol. 2022;32(5):2845–2856. doi:10.1177/11206721211052852
120. Avery RL, Gordon GM. Systemic Safety of Prolonged Monthly Anti-Vascular Endothelial Growth Factor Therapy for Diabetic Macular Edema: a Systematic Review and Meta-analysis. JAMA Ophthalmol. 2016;134(1):21–29. doi:10.1001/JAMAOPHTHALMOL.2015.4070
121. Kodjikian L, Bellocq D, Bandello F, et al. First-line treatment algorithm and guidelines in center-involving diabetic macular edema. Eur J Ophthalmol. 2019;29(6):573–584. doi:10.1177/1120672119857511
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Evidence in the Management of Diabetic Macular Edema with Intravitreal Anti-VEGFs in Asia: A Systematic Literature Review
Yuen YS, Tan GSW, Gan NY, Too IHK, Mothe RK, Basa P, Shaikh J
Clinical Ophthalmology 2022, 16:3503-3526
Published Date: 19 October 2022
Treatment of Diabetic Macular Edema or Macular Edema Following Retinal Vein Occlusion Based on Repeated Injection of the Dexamethasone Intravitreal Implant: A Retrospective Real-World Analysis
Sanders FW, Dumont Jones R, Jones DR, Phillips SV, Williams GS
Clinical Ophthalmology 2023, 17:3177-3187
Published Date: 24 October 2023
Role of Intravitreal Dexamethasone Implant in the Management of Treatment-Naive Diabetic Macular Edema: A Pre-Cataract Surgical Approach for Patients with Systemic Contraindications to Anti-VEGF Therapy
Chakraborty S, Ganguly S, Sheth JU
Clinical Ophthalmology 2024, 18:227-233
Published Date: 23 January 2024
Comparative Analysis of Intravitreal Dexamethasone Implant (Ozurdex) and Brolucizumab Injection in the Treatment of Diabetic Macular Edema with Hyperreflective Intraretinal Dots: A Retrospective Study
Chakraborty S, Sheth JU
Clinical Ophthalmology 2024, 18:2897-2905
Published Date: 15 October 2024