Back to Journals » Clinical Interventions in Aging » Volume 18
Safety and Effectiveness of Transarterial Chemoembolization in Hepatocellular Carcinoma Patients Aged Greater versus Less Than 80 Years
Authors Zhang L ![]() , Hong W, Wang Z, Zheng C, Liang B
, Hong W, Wang Z, Zheng C, Liang B ![]() , Shi H
, Shi H ![]()
Received 27 July 2023
Accepted for publication 5 November 2023
Published 14 November 2023 Volume 2023:18 Pages 1883—1892
DOI https://doi.org/10.2147/CIA.S429259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Lijie Zhang,1,2,* Wei Hong,1,2,* Zizhuo Wang,1,2 Chuansheng Zheng,1,2 Bin Liang,1,2 Heshui Shi1,2
1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China; 2Key Laboratory of Molecular Imaging of Hubei Province, Wuhan, Hubei, China
*These authors contributed equally to this work
Correspondence: Bin Liang; Heshui Shi, Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China, Tel +86 27 85726432, Fax +86 27 85727002, Email [email protected]; [email protected]
Background: Population aging has emerged as a pressing global concern and a significant medical challenge. The use of transarterial chemoembolization (TACE) has been extensively employed for managing unresectable hepatocellular carcinoma (HCC). However, there is limited evidence regarding the safety and effectiveness of TACE specifically in individuals aged 80 years and above.
Aim: To examine the safety and effectiveness of TACE in elderly patients (≥ 80 years) compared to younger patients (< 80 years) with HCC, and the potential risk factors that may impact the progression-free survival (PFS) for TACE were also identified.
Methods: A retrospective analysis was conducted on a consecutive cohort of unresectable HCC patients who were initially treated with TACE. The patients were categorized into two groups based on the age at which they underwent TACE, and the efficacy and safety of the treatment were evaluated. The PFS was investigated, and the prognostic factors were analyzed using the Kaplan-Meier method and Cox proportional hazard models.
Results: A total of 198 patients were included in this study, with 44 patients aged 80 years or older and 154 patients younger than 80 years. The cumulative risk of PFS after TACE was similar between the two groups (P = 0.800). In the multivariate analysis, a lower ECOG score (P = 0.039) and an earlier BCLC stage (P = 0.004) were identified as independent predictors of better PFS. Patients in both groups tolerated the TACE treatment well.
Conclusion: The impact of aging on poor PFS is not significant. In patients with HCC, TACE therapy is both safe and effective for octogenarians, similar to younger patients. Furthermore, the better PFS is associated with a low ECOG score and an early BCLC stage.
Keywords: transarterial chemoembolization, hepatocellular carcinoma, elderly patients, octogenarians
Introduction
Liver cancer is a common malignancy, ranking sixth in frequency and third in terms of cancer-related deaths worldwide. Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer, accounting for 75%-85% of cases, and is associated with poor prognosis.1 While surgical resection, liver transplantation, and ablation are potentially curative options, only a small number of patients are eligible for these treatments. For patients with unresectable HCC, transarterial chemoembolization (TACE) has been recommended as an effective palliative therapy, showing promising survival outcomes.2
Population aging has emerged as a global issue and a significant medical concern. In Europe, the average life expectancy has surpassed 80 years and continues to rise.3 In the USA, individuals aged over 65 years make up 13% of the population, with 1.8% being over 85 years old.4 Notably, China is experiencing a particularly pronounced aging trend. According to the 2021 census data from the Central People’s Government of the People’s Republic of China, the average life expectancy of residents is projected to increase from 77.93 years in 2020 to 78.2 years in 2021.5 Consequently, there is an urgent need to investigate the effectiveness and safety of TACE for elderly patients with HCC.
Previous studies have confirmed the effectiveness of TACE in elderly cohorts with different age cutoffs.6–8 However, the widespread use of TACE in elderly patients, especially octogenarians, remains controversial. This controversy may be attributed to the scarcity and heterogeneity of data and study populations.6 Furthermore, most of the research studies have used a cutoff age of 70 or 75 years.7–9 According to the latest statement from the World Health Organization (WHO),10 individuals aged 80 years or older are considered elderly. To our knowledge, there are few studies that have specifically investigated the value of TACE in patients aged 80 years or older compared to those younger than 80 years.
The objective of this study was to assess the safety and efficacy of TACE in two cohorts of patients with HCC, categorized by age: those aged 80 years or older and those younger than 80 years. Additionally, the study aimed to identify the factors that influence progression-free survival (PFS) in patients undergoing TACE.
Methods
Patients
This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology, and it was conducted in accordance with the ethical guidelines outlined in the 1975 Declaration of Helsinki. Informed consent was waived from all participants because of the retrospective nature of the study. All patient names and private data were kept anonymous and confidential. A retrospective analysis was performed on a consecutive series of HCC patients who underwent TACE as their initial treatment at our institution between January 2015 and December 2021.
The eligibility criteria for the present study were as follows: 1) patients aged over 18 years with HCC confirmed by pathological or clinical diagnosis according to the European Association for the Study of the Liver (EASL) criteria;2 2) patients who received TACE as the initial treatment option without undergoing any other treatment until experiencing the primary endpoint, including surgery, ablation, or systemic therapy; 3) patients who were ineligible or unwilling to receive liver transplant, resection, or ablation; 4) patients with liver function classified as Child-Pugh Class A or B without ascites; and 5) patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2.
The exclusion criteria for this study were as follows: 1) diffuse liver cancer observed on imaging; 2) HCC with vascular invasion (lobar or main portal trunk) or extrahepatic spread; 3) tumor burden exceeding 70% liver involvement; 4) technically unsuccessful TACE procedure; and 5) irregular follow-up or loss to follow-up within six months after the TACE operation.
The patients were divided into two groups: the elderly HCC group (E-HCC group, aged 80 years or older) and the non-elderly HCC group (Non-e HCC group, younger than 80 years).
Treatment Protocol
Conventional Transarterial Chemoembolization (C-TACE) or TACE with CalliSpheres® microspheres (CSM-TACE, Jiangsu Hengrui Medicine Co., Ltd., Jiangsu Province, China) was conducted in two cohorts. A 5F visceral catheter was inserted to catheterize the celiac trunk and the superior mesenteric artery after gaining vascular access through the common femoral artery. Selective arteriography was performed to identify potential hypervascular tumors. In case of need, the potential extrahepatic collateral vessels were examined to rule out malignant parasitization of blood flow. A coaxial microcatheter system (Progreat, Terumo, Tokyo, Japan) with a diameter of 2.7F was used to advance into the tumor-feeding arteries. Subsequently, either conventional- or CSM-TACE was performed following previously described methods.11
Doxorubicin was the only used chemotherapeutic drug in this study. The dosage of chemotherapeutic drug used could be body surface area-based, liver function-based, weight-based, or even empiric. Currently used dose of doxorubicin was 10–100 mg. The ethiodized oil and chemotherapeutic drugs should be mixed into an emulsion and configured as a “water-in-oil” emulsifier to improve its stability. The volume ratio of ethiodized oil to drug aqueous solution is usually 2:1. The volume of ethiodized oil injected is generally determined by the size and vascularity of the tumor, with common usage of 5–15 mL.
Technical success was determined by the successful placement of the catheter into the tumor-feeding arteries and the administration of transarterial therapy according to the planned procedure. The endpoint for embolization was stasis of blood flow in the arterial feeders to the tumor. The assessment was conducted for each TACE procedure.
Follow-Up and Efficacy Assessment
Follow-up CT or MR examinations were conducted on patients 1–3 months after each TACE treatment. Tumor response was assessed using contrast-enhanced CT or MRI scans obtained 6 months after TACE. Two radiologists (Bin Liang and Heshui Shi) evaluated the images independently and in a blinded manner to determine tumor characteristics and response. Tumor response was categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD), following the modified Response Evaluation Criteria in Solid Tumors (mRECIST) scheme.12 The objective response rate (ORR) was calculated by adding the complete response (CR) and partial response (PR) rates. The disease control rate (DCR) was calculated by adding the CR, PR, and SD rates. Progression-free survival (PFS) was defined as the time from the initiation of treatment to either radiological progression or death, which served as the primary endpoint in this study. Patients who were lost to follow-up within six months after the first TACE were considered censored.
To identify potential predictors of PFS, the study analyzed several variables, including age, gender, pathogeny, comorbidity, Child-Pugh class, alanine aminotransferase (ALT), aspartate aminotransferase (AST), Eastern Cooperative Oncology Group (ECOG) score, a-fetoprotein (AFP), number of transarterial chemoembolization (TACE) sessions, and tumor characteristics such as Barcelona Clinic Liver Cancer (BCLC) stage, number of tumors, tumor size, and tumor burden.
Assessment of Safety
Safety was assessed by recording the occurrence of postembolization syndrome and severe adverse events during the periprocedural and follow-up periods. The postembolization syndrome typically manifested as fever, nausea or vomiting, and pain. It was important to note that the syndrome itself is not considered an adverse event, but rather an expected outcome of embolization. Adverse events (AEs) were evaluated based on the Common Terminology Criteria for Adverse Event, version 4.0.13 A severe adverse event was defined as any event that necessitates additional therapy, such as an increased level of care, hospitalization beyond observation status (including readmission after initial discharge), permanent adverse sequelae resulting in significant morbidity and disability, or death.
Statistical Analysis
Continuous data were expressed as mean ± standard deviation. Statistical analyses were conducted using the Wilcoxon Signed Rank Test, Mann–Whitney U-test, Pearson Chi-square test, Fisher Exact test, and McNemar-Bowker test, as appropriate. The PFS was evaluated using the Kaplan-Meier method, and 95% confidence intervals (CI) were provided for proportions. Variables associated (P ≤ 0.2) with survival in the univariate analysis were included in the Cox multivariate stepwise regression model to identify independent prognostic factors. The adjusted relative risk (hazard ratio, HR) and 95% CI were calculated for each independent predictive factor. Statistical analyses were performed using software (SPSS, version 26.0; SPSS Inc., Chicago, Illinois, USA). A two-tailed P value less than 0.05 was considered to indicate a statistically significant difference.
Results
Patient Characteristics
A total of 198 HCC patients were enrolled in this study. Among these patients, 44 (22.2%) were aged 80 or older (E-HCC group), whereas 154 (77.8%) were aged less than 80 (Non-e HCC group). Elderly patients were more likely to be infected by the hepatitis B virus than the younger patients, while the etiology of younger patients was associated with alcohol abuse or steatohepatitis. The younger patients underwent multiple TACE sessions compared to the elderly patients (P < 0.001), which may be attributed to the earlier BCLC stage (P = 0.004) and fewer tumor nodules (P = 0.034) observed in the elderly group. There was no statistical difference in tumor size and tumor burden between the two study groups. The demographic and clinical characteristics of the recruited patients are summarized in Table 1.
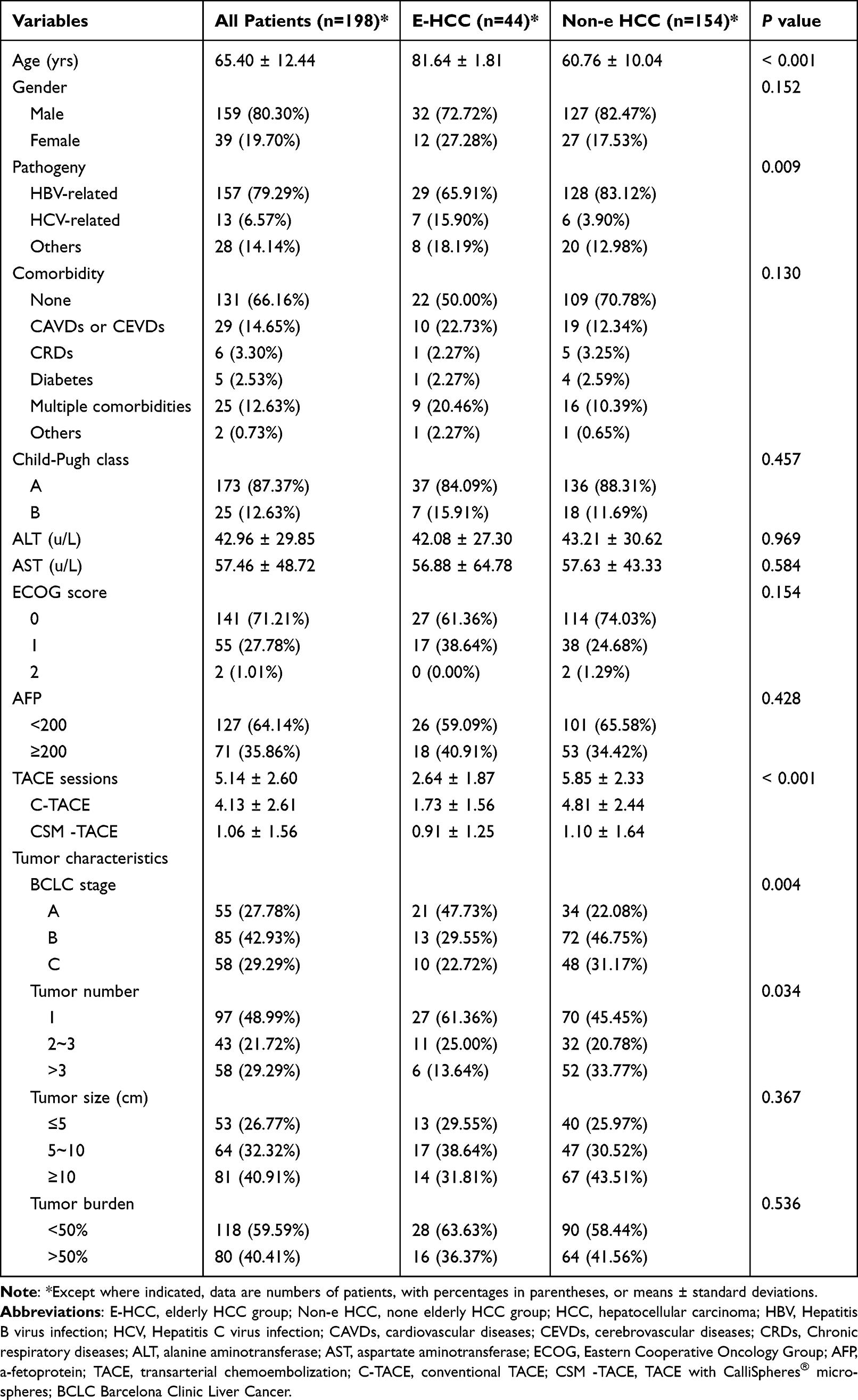 |
Table 1 Demographic and Clinical Characteristics of Patients Between the Different Groups |
Treatment Process
All patients underwent technically successful TACE treatment. In the elderly group, 11 patients received one TACE session, 18 patients received two sessions, and 15 patients received three or more sessions. The median number of TACE treatments per patient was two (range, 1–8). In contrast, all of the patients in the non-elderly group had received at least three TACE sessions. Specifically, 27 patients received three TACE sessions, 24 patients received four sessions, and 103 patients received five or more sessions. The median number of TACE treatments was six (range, 3–12).
Furthermore, in the E-HCC group, eight patients accepted CSM-TACE treatment alone with a median number of one (range, 1–3), while 23 patients received a total of 54 C-TACE-only treatments with a median number of two (range, 1–8). Both of the two TACE procedures were performed in 13 patients.
In the Non-e HCC group, four patients underwent CSM-TACE operation alone, with a median number of three treatments (range: 3–4). A total of 477 C-TACE-only treatments were performed in 86 patients, with a median number of five treatments (range: 3–12). Additionally, 64 patients underwent both CSM and C-TACE operations.
Follow-Up, Tumor Response and Clinical Examinations
The median follow-up period was 13.5 months (range, 8–68 months). In the E-HCC group, 11 patients achieved CR, 19 patients achieved PR, 11 patients had SD, and 3 patients had PD. Therefore, the ORR was 68.18% (30/44) and the DCR was 93.18% (41/44). In the Non-e HCC group, 31 patients achieved CR, 71 patients achieved PR, 38 patients had SD, and 14 patients had PD. The ORR was 66.23% (102/154) and the DCR was 90.91% (140/154). There was no significant difference in treatment response six months after TACE between the two groups (Table 2).
 |
Table 2 Tumor Response at 6 Months After TACE |
Regarding clinical examinations, there was no statistically significant difference in the Child-Pugh class among E-HCC patients before and after TACE. However, it was observed that younger patients had worse liver function after TACE (P = 0.038), and there was no significant difference between the two cohorts at six months after the operation. In terms of ECOG, there was no statistical difference before and after TACE in the same group of patients. However, repeated TACE sessions worsened the condition of younger patients (P < 0.001). An increase in ALT was observed in the E-HCC group after TACE (P < 0.001), while ALT levels decreased in the younger group (P < 0.001). There was no significant difference between the two groups postoperatively (P = 0.159). The levels of AST and AFP decreased in the same group before and after TACE. However, there was no statistical difference between the two groups during the follow-up period (Table 3).
 |
Table 3 Changes of Laboratory Examination Results and ECOG Score Before and at 6 Months After TACE |
Risk Factors for PFS
In the univariate analysis, several factors were found to be significant in terms of progression-free survival (PFS), including Child-Pugh class (P = 0.151), ECOG score (P = 0.179), AFP level (P = 0.143), BCLC stage (P < 0.001), tumor number (P = 0.017), tumor size (P = 0.034), and tumor burden (P = 0.002). However, in the multivariate analysis, only ECOG score and BCLC stage remained significant after adjusting for other variables (Table 4). Patients with lower ECOG score and earlier BCLC stage had longer PFS. Age was not found to be an independent predictor of PFS (P = 0.800).
 |
Table 4 Results of Univariate and Multivariate Analysis of Factors Associated with PFS |
The Kaplan-Meier curves of PFS were analyzed based on BCLC stage and divided into three groups. Patients with BCLC stage A had a median survival time of 19.0 months (95% CI 15.101–22.899), while patients with BCLC stage B had a median survival time of 9.0 months (95% CI 7.344–10.656). Patients with BCLC stage C had a median survival of 7.5 months (95% CI 6.671–8.329). There was a significant difference between the survival times of these groups (Figure 1A). Additionally, Figure 1B displayed the Kaplan-Meier estimates of PFS for younger and elderly patients, although statistical significance was not indicated.
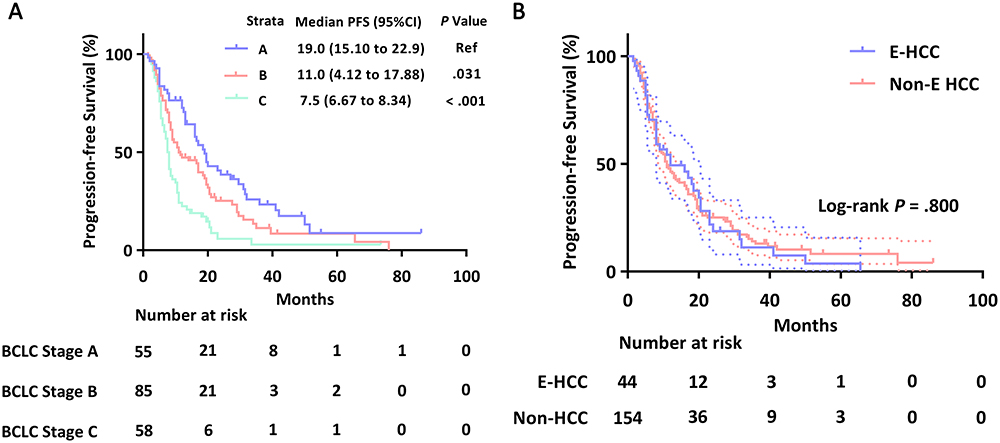 |
Figure 1 Kaplan-Meier analysis of progression-free survival (PFS) based on BCLC staging system and age. (A) Kaplan-Meier curves illustrating the division into three groups according to the BCLC staging system. (B) Kaplan-Meier curves based on age. Abbreviations: PFS, progression-free survival; BCLC, Barcelona Clinic Liver Cancer; Ref, reference. |
Safety
No treatment-related deaths were observed during the hospitalization and follow-up periods. Out of the total 169 patients, both groups experienced postembolization syndrome, which included symptoms such as fever, abdominal pain, vomiting, or nausea, during the periprocedural period. However, there was no statistically significant difference between the two groups. Groin hematoma occurred in six patients, but the P value was greater than 0.05, indicating no significant difference. The aforementioned symptoms were relieved within three to five days after receiving symptomatic treatment.
Additionally, six patients in both groups developed severe AEs, such as liver dysfunction and hepatorenal syndrome. However, these symptoms were resolved after active treatment with guidance from multidisciplinary teams, and no statistical difference was found between the two groups (Table 5).
 |
Table 5 AEs After TACE Treatment |
Discussion
With the increasing incidence rate of HCC and the average age of patients at diagnosis, there is still a need to define the optimal management strategy for elderly HCC patients.14 Previous research has examined the outcome and safety of TACE in elderly patients, but these studies have been limited to those aged 65, 70, or 75 years. There has been little research focusing on the efficacy of TACE in octogenarians. In our research, we found that advanced age was not an independent risk factor for contraindication to TACE, shorter PFS, or severe AEs. A low ECOG score and early BCLC stage were identified as positive predictive factors for long-term PFS.
Although advanced age was not considered a contraindication in this study, elderly patients, particularly octogenarians, were often excluded from clinical trials or practice.15 Overall, elderly patients have a significantly higher prevalence of comorbidities compared to younger patients, which may increase the risk of complications related to TACE.8 In this study, there were no significant differences in the baseline characteristics of comorbidities between the two groups. There are several possible reasons for this. Firstly, older patients with severe comorbidities were excluded from TACE treatment due to their lower level of physical activity compared to younger cohorts. Secondly, the extension of average life expectancy among the elderly has led to an improvement in their quality of life16 and overall physical condition. Additionally, there was a significant difference in the pathogeny of HCC between the two cohorts (P = 0.009). Most elderly individuals were hepatitis B carriers, while younger patients were more likely to be diagnosed with non-alcoholic fatty liver disease (NAFLD) or alcoholic hepatitis. This difference is worth noting.
This study found no significant difference in PFS or treatment efficacy between the two groups, which is consistent with previous research on the effectiveness of TACE in elderly cohorts with different age cutoffs. Mirici-Cappa et al7 observed comparable overall survival (OS) rates between patients over 70 years old and those under 70 years old. Nishikawa et al8 compared the outcomes of intermediate hepatocellular carcinoma (HCC) patients who underwent TACE in two groups: 66 patients over 75 years old and 84 patients under 75 years old, and found no difference in OS. Yau et al9 demonstrated that elderly patients (> 70 years) had higher OS and disease-specific survival compared to younger patients (< 70 years). There was no significant difference in TACE-related mortality between the two age groups. Our research further supports these findings by showing that octogenarian HCC patients treated with TACE had similar tumor response and PFS as patients under 80 years of age. These results provide additional evidence that age does not significantly affect the efficacy of TACE.
The prognosis of HCC patients is closely related to their ECOG score and BCLC stage. The treatment of HCC is determined by the BCLC staging system, which considers the extent of the disease, liver function assessed by the Child-Pugh score, and performance status (PS) assessed by the ECOG.2 Numerous studies have demonstrated that HCC patients with better performance status and those in earlier or intermediate BCLC stages, including elderly patients, can benefit from TACE treatment.2,17 Consistent with previous findings, our data demonstrated that the prognosis after TACE was heavily influenced by the pretreatment ECOG score and disease stage, irrespective of patient age. Our evaluation of other prognostic variables revealed no significant differences in PFS between the two cohorts. Notably, the older group exhibited earlier tumor stages (P = 0.004) and a lower number of tumor nodules (P = 0.034), which might have contributed to the implementation of more aggressive treatment strategies.
Safety and tolerability in our study population were comparable to previous experiences with TACE in elderly patients aged 60 to 75 years.7–9 The most common side effect after TACE in both groups was post-embolization syndrome. We noticed a higher occurrence of nausea and vomiting in younger patients (P < 0.001), which may suggest that the treatment procedure, including higher concentrations of chemotherapy drugs or more extensive embolization, was more aggressive in the younger population.
Our study had several limitations. Firstly, the patients received either standard or CSM-TACE during the course of the study. To further discuss the impact of different embolic materials used in the TACE operation on the elderly population, a subgroup analysis with a large sample size is needed. Secondly, the degree of histologic differentiation was not included in the multivariable analysis due to the insufficient number of biopsy-proven HCCs in the study population. This omission may have potential clinical implications on TACE therapy. Lastly, the retrospective design of this study introduces inherent bias that could not be avoided.
Conclusions
In conclusion, the findings of this study suggested that advanced age does not have a negative impact on the selection of TACE therapy in HCC patients. The safety and prognosis of 80-year-old HCC patients who underwent TACE were similar to those of younger patients. Additionally, lower ECOG score and earlier BCLC stage were identified as positive predictive factors for PFS in HCC patients treated with TACE.
Abbreviations
HCC, hepatocellular carcinoma; TACE, transarterial chemoembolization; OS, overall survival; WHO, World Health Organization; PFS, progression-free survival; ECOG, Eastern Cooperative Oncology Group; BCLC, Barcelona Clinic Liver Cancer; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CSM, CalliSpheres® microspheres; mRECIST, modified Response Evaluation Criteria in Solid Tumors; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; ORR, objective response rate; DCR, disease control rate; AEs, adverse events; NAFLD, non-alcoholic fatty liver disease; PS, performance status.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
3. The European Commission and the Economic Policy Committee (AWG). The 2012 Ageing Report: Economic and Budgetary Projections for the EU27 Member States (2010–2060). Brussels: European Union; 2012.
4. Administration on Ageing, Administration for Community Living. A profile of Older Americans 2013: Washington US Department of Health and Human Services; 2014.
5. The Central People’s Government of the People’s Republic of China. Statistical Bulletin of China’s Health Development in 2021. Available from: http://www.gov.cn/xinwen/2022-07/12/content_5700670.htm.
6. Mosconi C, Gramenzi A, Biselli M, et al. Survival and tolerability of transarterial chemoembolization in greater versus less than 70 years of age patients with unresectable hepatocellular carcinoma: a propensity score analysis. Cardiovasc Intervent Radiol. 2020;43(7):1015–1024. doi:10.1007/s00270-020-02451-3
7. Mirici-Cappa F, Gramenzi A, Santi V, et al. Treatments for hepatocellular carcinoma in elderly patients are as effective as in younger patients: a 20-year multicentre experience. Gut. 2010;59(3):387–396. doi:10.1136/gut.2009.194217
8. Nishikawa H, Kita R, Kimura T, et al. Transcatheter arterial chemoembolization for intermediate-stage hepatocellular carcinoma: clinical outcome and safety in elderly patients. J Cancer. 2014;5(7):590–597. doi:10.7150/jca.9413
9. Yau T, Yao TJ, Chan P, et al. The outcomes of elderly patients with hepatocellular carcinoma treated with transarterial chemoembolization. Cancer. 2009;115(23):5507–5515. doi:10.1002/cncr.24636
10. The World Health Organization (WHO). New age classification standard-65 years old is still young. Available from: https://en.brilio,net/news/65-years-old-is-still-young-1601205.html#.
11. Liang B, Xiang H, Ma C, et al. Comparison of chemoembolization with CalliSpheres® microspheres and conventional chemoembolization in the treatment of hepatocellular carcinoma: a multicenter retrospective study. Cancer Manag Res. 2020;12:941–956. doi:10.2147/CMAR.S187203
12. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
13. Common Terminology Criteria for Adverse Events v.4.0 (CTCAE). NIH publication #09-7473. National Cancer institute; 2009. Available from: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
14. Cammarota A, D’Alessio A, Pressiani T, Rimassa L, Personeni N. Systemic treatment for older patients with unresectable Hepatocellular carcinoma. Drugs Aging. 2021;38(7):579–591. doi:10.1007/s40266-021-00871-5
15. Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related Hepatocellular Carcinoma After Resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.CCR-17-2899
16. Yang J, Siri JG, Remais JV, et al. The Tsinghua-Lancet Commission on Healthy Cities in China: unlocking the power of cities for a healthy China. Lancet. 2018;391(10135):2140–2184. doi:10.1016/S0140-6736(18)30486-0
17. Cheng HM, Tanaka T, Nishiofuku H, et al. Safety and prognosis of transarterial chemoembolization for octogenarians with hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2019;42(10):1413–1419. doi:10.1007/s00270-019-02290-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Early TACE Refractoriness on Survival in Patients with Hepatocellular Carcinoma: A Real-World Study
Yang C, Luo YG, Yang HC, Yao ZH, Li X
Journal of Hepatocellular Carcinoma 2022, 9:621-631
Published Date: 21 July 2022
Comparison of the Efficacy and Safety of Transarterial Chemoembolization with or without Lenvatinib for Unresectable Hepatocellular Carcinoma: A Retrospective Propensity Score–Matched Analysis
Chen YX, Zhang JX, Zhou CG, Liu J, Liu S, Shi HB, Zu QQ
Journal of Hepatocellular Carcinoma 2022, 9:685-694
Published Date: 1 August 2022
Retrospective Study of the Efficacy and Safety of Chemoembolization with Drug-Eluting Microspheres Combined with Intra-Arterial Infusion of Bevacizumab for Unresectable Hepatocellular Carcinoma
Ueda S, Hori S, Hori A, Makitani K, Wan K, Sonomura T
Journal of Hepatocellular Carcinoma 2022, 9:973-985
Published Date: 12 September 2022
Predicting Outcome in Combination Treatment of TACE and Camrelizumab for Advanced Hepatocellular carcinoma: Tumor Hypervascularity and Reactive Cutaneous Capillary Endothelial Proliferation
Yin L, Liu KC, Lv WF, Xu SB, Lu D, Zhou CZ, Cheng DL, Gao ZG, Shi CS, Su MX
Drug Design, Development and Therapy 2022, 16:3421-3429
Published Date: 30 September 2022
Adjuvant Transarterial Chemoembolization Plus Immunotherapy for Huge Hepatocellular Carcinoma: A Propensity Score Matching Cohort Study
Huang H, Liao W, Zhang K, Wang H, Cheng Q, Mei B
Journal of Hepatocellular Carcinoma 2024, 11:721-735
Published Date: 8 April 2024