Back to Journals » Clinical Ophthalmology » Volume 17
Safety and Effectiveness of Smooth Incision Lenticular Keratomileusis (SILKTM) Using the ELITA(TM) Femtosecond Laser System for Correction of Myopic and Astigmatic Refractive Errors
Authors Sachdev MS, Shetty R, Khamar P, Malik R, Schwam BL, Wang Y, Fu H, Voorhees AP, Laron M ![]()
Received 22 August 2023
Accepted for publication 30 November 2023
Published 8 December 2023 Volume 2023:17 Pages 3761—3773
DOI https://doi.org/10.2147/OPTH.S432459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mahipal S Sachdev,1 Rohit Shetty,2 Pooja Khamar,2 Raghav Malik,1 Brian L Schwam,3 Ying Wang,3 Hong Fu,3 Andrew P Voorhees,3 Michal Laron3
1Centre for Sight, New Delhi, India; 2Narayana Nethralaya Eye Hospital, Bangalore, India; 3Johnson and Johnson Surgical Vision, Inc, Milpitas, CA, USA
Correspondence: Michal Laron, Johnson and Johnson Surgical Vision, Inc, 510 Cottonwood Drive, Milpitas, CA, 95035, USA, Tel +1 408 273 5802, Email [email protected]
Purpose: To evaluate visual outcomes following the Smooth Incision Lenticular Keratomileusis (SILKTM) procedure for correction of myopic refractive errors with and without astigmatism, using the ELITATM Femtosecond Laser System.
Patients and Methods: A prospective, multicenter, single-arm, open-label clinical study was conducted. Eighty-five myopic subjects (n = 170 eyes), aged 18 years or older, with manifest refractive spherical equivalent (MRSE) up to − 12.00 D and astigmatism up to − 6.00 D, were treated binocularly using the ELITA femtosecond laser and followed up for 6 months. Intended correction was emmetropia for all eyes. The primary outcome measures included post-operative uncorrected and corrected distance visual acuity (UDVA and CDVA). Secondary outcome measures included surgeon’s rating for ease of lenticule extraction, predictability, safety, and stability.
Results: A total of 170 eyes of 85 patients underwent SILK. Preoperative mean MRSE was − 4.14 D ± 1.32 D (range − 1.38 D to − 8.88 D) and the mean cylinder was − 0.77 D ± 0.62 D. Intraoperative surgeon ease of lenticule dissection was rated as grade 0 or 1 in 85.3% of eyes (no/only mild dissection needed). UDVA at 1 day, 1 week, 1 month, and 6 months was 20/20 or better in 65.9%, 85.4%, 91.5%, and 96% of eyes, respectively. No eyes lost any lines of CDVA at 6 months compared to the preoperative. The postoperative MRSE was stable over time, ranging from − 0.34 D ± 0.24 D at 1 month to − 0.33 D ± 0.23 D at 6 months. MRSE predictability (± 0.50 D) was 93.5% (129/138) at 3 months and 91.1% (113/124) at 6 months. No serious adverse events were noted.
Conclusion: The SILK procedure with the ELITA Femtosecond Laser System is safe and effective for the treatment of myopic refractive errors with and without astigmatism. Fast visual recovery was demonstrated, with stability achieved by 3 months.
Keywords: smooth incision lenticular keratomileusis, SILK, laser-assisted lenticule extraction, corneal refractive surgery, myopia, keratorefractive lenticule extraction
Corrigendum for this paper has been published.
A Letter to the Editor has been published for this article.
A Response to Letter by Professor Alpins has been published for this article.
Introduction
Femtosecond lasers are commonly used in cataract and refractive surgery procedures, such as laser-assisted lenticule extraction (LALEX). LALEX modifies the anterior corneal radius of curvature by creating an intrastromal lenticule that corresponds to the desired refractive correction, which is then removed.1,2 This alteration of corneal curvature is the foundation of all plano-convex tissue removal techniques, including laser in situ keratomileusis (LASIK), photorefractive keratectomy (PRK), small incision lenticule extraction (SMILE, VisuMax 500 and 800, Carl Zeiss Meditec AG Germany), SmartSight (ATOS, Schwind eye-tech-solutions, Germany), and CLEAR (Z8, Ziemer, Switzerland).1–6
Femtosecond lasers generate ultrashort laser pulses, which induce micron-scale incisions in target tissues by photodisruption.7 The small incision through the corneal epithelium used for lenticule removal during LALEX procedures leads to fewer epithelial defects, less postoperative pain and dryness, faster wound healing, and larger postoperative achieved functional optical zones compared to other corneal refractive surgery procedures.6,8–10 However, visual recovery can be impacted by femtosecond laser energy levels,9,11 scanning patterns,12 and surgical technique,13 and there is a longer learning curve for surgeons compared to conventional LASIK procedures.2,13 In procedures such as SMILE, tissue bridges are present between the cornea and the lenticule at the two lenticular interfaces after the femtosecond laser cuts are completed, requiring surgeon manipulation to separate the lenticule prior to extraction.14 This can compromise the quality of the lenticle interface and impact visual recovery time.15
ELITATM is a new generation ophthalmic femtosecond laser surgical system developed by Johnson and Johnson Surgical Vision, Inc. (Milpitas CA, USA), which received CE Mark approval in March 2023 for Smooth Incision Lenticular Keratomileusis (SILKTM) and LASIK flap creation.16 The ELITA system was designed to deliver low energy treatment (40–90 nJ per pulse) through a combination of small focus spot size (approximately 1 µm), ultrashort pulse duration (100–200 fs), and ultrafast pulse frequency (10 MHz). ELITA creates virtually no pulse separation (mean spot to spot is about 1 µm), which leads to continuous tissue resection with minimal residual tissue bridges, and therefore less lenticule manipulation for tissue removal required by the surgeon. Subsequently, less keratocyte activation and a reduced immune response are expected postoperatively,7 resulting in faster healing and visual recovery with fewer surgical complications. The system was also designed to produce a biconvex lenticule shape, where the anterior and posterior surfaces are matched, so that corneal micro-folding is minimized or eliminated following lenticule removal.
The purpose of this clinical trial was to evaluate visual outcomes of the new ELITA Femtosecond Laser System for the correction of myopic refractive errors, with and without astigmatism. Surgeon rating of ease of lenticule removal, intended versus achieved refractive outcomes, and adverse events were also assessed. The primary clinical hypothesis was that the SILK procedure using the new ELITA laser system would result in excellent visual outcomes for the treatment of myopic refractive errors with and without astigmatism.
Materials and Methods
This prospective, multicenter, single-arm, open-label clinical study was conducted at two sites in India (Centre for Sight, New Delhi and Narayana Nethralaya Eye Hospital, Bangalore) in accordance with the Declaration of Helsinki, ISO 14155:2011 and all other applicable laws and regulations. Human research ethics approval was obtained from the Centre for Sight Institutional Ethics Committee (New Delhi, India) and Narayana Nethralaya Ethics Committee (Bangalore, India) prior to beginning the study. The study was registered on www.clinicaltrials.gov as NCT04200898. After written informed consent was obtained and confirmation that all eligibility criteria were met, the SILK procedure was performed.
Inclusion and Exclusion Criteria
Subjects were eligible to have surgery on one or both eyes on the same day, based on their refractive correction needs. The inclusion criteria were age ≥18 years, myopic spherical equivalent (SE) refractive error of ≤−12.00 diopters (D) and astigmatism ≤−6.00 D, anticipated residual corneal stromal thickness of ≥250 microns,17 uncorrected distance visual acuity (UDVA) of 20/40 or worse, corrected distance visual acuity (CDVA) of 20/20 or better and CDVA ≥2 lines better than UDVA. Subjects were also required to have ≤0.75 D difference between cycloplegic and manifest refraction sphere, stable refractive error for at least 12 months, and discontinue contact lens wear for at least 4 weeks (rigid) or 2 weeks (soft) prior to surgery. Exclusion criteria included history of medical conditions or concurrent use of systemic medications that may impair wound healing, history of diabetes mellitus, implanted electronic device, pacemaker, or defibrillator, history of prior intraocular or corneal surgery, active ophthalmic disease or abnormality including clinically significant dry eye, glaucoma, keratoconus, corneal dystrophy or degeneration, pregnancy, lactating or planning pregnancy, and known sensitivity to any of the medications used in postoperative care.
Clinical Examination
Detailed ocular and medical history were obtained from all patients at baseline. Clinical examination of the eye was performed at baseline and all follow-up visits. All subjects had a minimum of nine scheduled study visits: preoperative examination of both eyes and post- operative visit at 1-day, 1-week, and 1-, 3-, 6-, 9- and 12-months. Data from the first 6 months of this study are presented in this manuscript. The following clinical parameters were assessed: UDVA, CDVA, manifest refraction, intraocular pressure, biomicroscopic slit-lamp findings and dilated fundus examination, non-directed ocular/visual symptoms, adverse events, medical findings, and surgical complications. Investigations included corneal topography (Pentacam, Oculus Optikgerate GmbH, Germany) and pachymetry (Pentacam). Visual acuity was recorded using an Early Treatment Diabetic Retinopathy Study (ETDRS) computerized vision chart at 4.0 meters (13 feet) under photopic conditions (background luminance 85 cd/m2 (range 80–110 cd/m2). Intraoperative docking attempts, suction losses, and surgeon ease of lenticule dissection were also recorded. The intraoperative ease of lenticule removal was graded on a scale of 0–4 by the surgeons (where 0 = no dissection needed, and 4 = unable to dissect; Table 1) for each eye.
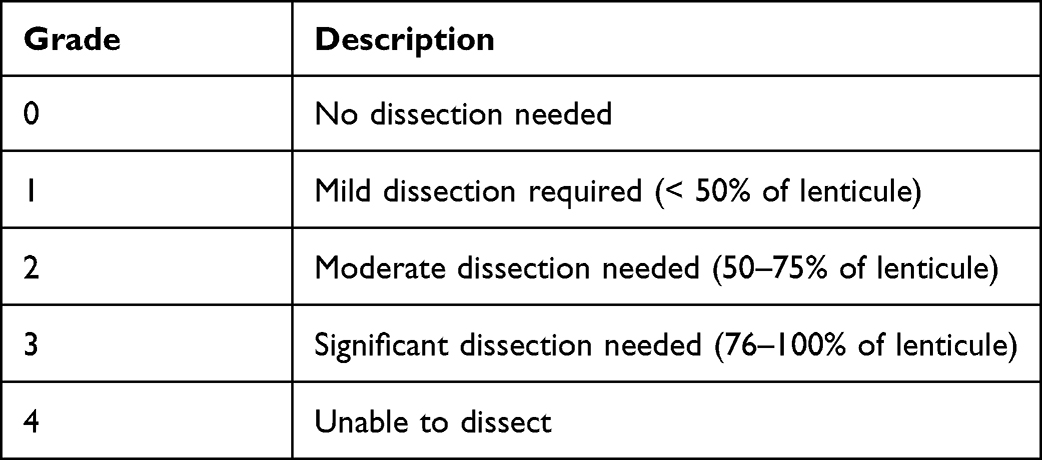 |
Table 1 Ease of Lenticule Removal Rating Scale |
Surgical Technique
All surgeries were performed by two surgeons (MSS and RS) who are experienced in lenticule extraction surgery for refractive correction. Surgeons followed the standardized treatment instructions provided with the ELITA system installed with precommercial software. Data entry for refractive error and keratometry readings were done on the ELITA treatment planning system software. A standard optical zone of 6.0 mm, central anterior depth of 110 μm, and entry cut arc length of 3 mm were used in all cases. The ELITA femtosecond laser was then used in conjunction with a sterile, single-use disposable patient interface (PI), consisting of a pre-sterilized suction ring and an application cone assembly, to facilitate accurate corneal laser incisions. During docking, the PI cone was attached to the PI mount of the ELITA system and the PI suction ring was attached to the surgery eye via a vacuum pump. The PI cone was then mated into the PI suction ring under surgeon guidance. The surgeon centered the lenticule treatment to the central corneal mark, which was placed either on the pupil center or visual axis using the corneal Purkinje image while subjects fixated on the coaxial fixation light (based on surgeon preference). The surgeon adjusted the cylinder axis to the toric alignment marks, which were placed on the periphery of the cornea. Following laser treatment, the lenticule was removed through a 3 mm incision in the cornea.
All eyes were targeted for emmetropia. A standard operating room environment protocol of relative humidity of 40–70% and temperature of 16–26°C (60.8–78.8°F) was followed for all cases. Surgeons used the Zeiss OPMI LUMERA 700 (Carl Zeiss Meditec AG Germany) ophthalmic microscope and AKRUS LS Comfort (AKRUS GmbH & Co, Germany) surgical bed with the ELITA laser system. Following treatment, postoperative pain control and use of bandage contact lenses were at the discretion of the surgeon. A postoperative regimen of topical antibiotics, corticosteroids, and preservative-free lubricating eye drops guidance was followed.
Outcome Measures
The primary effectiveness endpoint for the study was monocular UDVA, with 85% of eyes treated with the ELITA system expected to have UDVA of 20/40 or better from 1-month postoperatively. The primary safety endpoint was defined as maintenance of monocular CDVA, with less than 5% of all treated eyes expected to show a loss of >2 lines of CDVA from 1 week following surgery. Other endpoints included ease of lenticule removal, manifest refraction spherical equivalent (MRSE) and manifest refraction cylinder (MRC) predictability, refractive stability, induced refractive astigmatism (absolute change in MRC compared to pre-operative), and rate of adverse events.
Statistical Analysis
Statistical analyses were conducted to evaluate the visual outcomes with the ELITA laser system 6 months following surgery using SAS version 9.4 (SAS Institute, Cary, NC). Each treated eye was analyzed separately for all endpoints and missing data were not imputed. For surgeon operative day ratings, the frequency and proportion of eyes with each ease of lenticule removal rating score and the number of suction losses and docking attempts were calculated. The frequency and proportion of eyes with each acuity line of monocular UDVA (primary effectiveness endpoint) were summarized for each study visit. For maintenance of CDVA (primary safety endpoint), the proportion of eyes with CDVA line changes relative to the preoperative visit was calculated for each visit. The safety index (CDVA postoperative/CDVA preoperative) and the efficacy index (UDVA postoperative/CDVA preoperative) of the procedure were calculated following the methods described by Gomel et al.18 Cut-offs for success were defined as 0.85 for the safety index and 0.80 for the efficacy index, respectively.18 With a sample size of 130 eyes, the two-sided 95% confidence interval (CI) around the proportion of eyes with UDVA of 20/40 or better at 1 month post-operatively was 79% to 91%, ie, the precision (half width of the CI) of the estimate was 6%, assuming the point estimate of the proportion to be 85% based on the normal approximation to the binomial distribution.
Summary statistics (mean, standard deviation, minimum, and maximum) were calculated for logMAR UDVA and CDVA, MRSE, manifest refraction sphere (MRS), and MRC. The frequency and proportion of eyes with MRSE, under- or over-corrected by more than 1.00 D or 2.00 D were also summarized over time. Intended versus achieved MRSE regression analysis was performed and the accuracy of MRC was also summarized over time, including the frequency and proportion of eyes with MRC within ± 0.50 D and ± 1.00 D. Vector analyses following the methods recommended by the Astigmatism Project Group of the American National Standards Institute (ANSI) were conducted to evaluate the accuracy of astigmatic treatments.19 The intended refractive correction (IRC), surgically induced refractive correction (SIRC), error vector (EV), correction ratio (CR), error ratio (ER), error of magnitude (EM), and error of angle (EA) were all calculated at 6 months.
Refractive stability was evaluated for eyes with data at all follow-up visits (consistent cohort – eyes with data at 1, 3, and 6 months). Stability was considered achieved if the following criteria were met: at least 95% of the treated eyes had a change ≤1.00 D of MRSE between the two successive visits; the mean rate of change was ≤0.04 D/month over the same time period; and the 95% confidence intervals of the mean rate of change in MRSE between successive visits included zero. Stability should be confirmed at least 3 months after the stability time point. The frequency and proportion of eyes with medical/surgical findings or adverse events was also calculated.
Results
Eighty-five subjects (170 eyes) were enrolled in the current study across the two clinical sites (Table 2). The mean age of subjects was 25.8 ± 6.1 years (range 18–56 years); 54% were female, 46% were male, and 100% were Indian. The preoperative mean MRSE was −4.14 diopters (D) ± 1.32 D (range −1.38 D to −8.88 D); preoperative mean MRS was −3.75 D ± 1.27 D (range −1.25 D to −8.00 D) and mean MRC was −0.77 D ± 0.62 D (range 0.00 D to −3.00 D). All subjects had bilateral surgery, resulting in a total of 170 eyes being treated during the study. At the time of the interim analysis, data from 158, 130, 138 and 124 eyes were available from the 1-week, 1-, 3- and 6-month visits, respectively. There were no subjects discontinued or lost to follow-up.
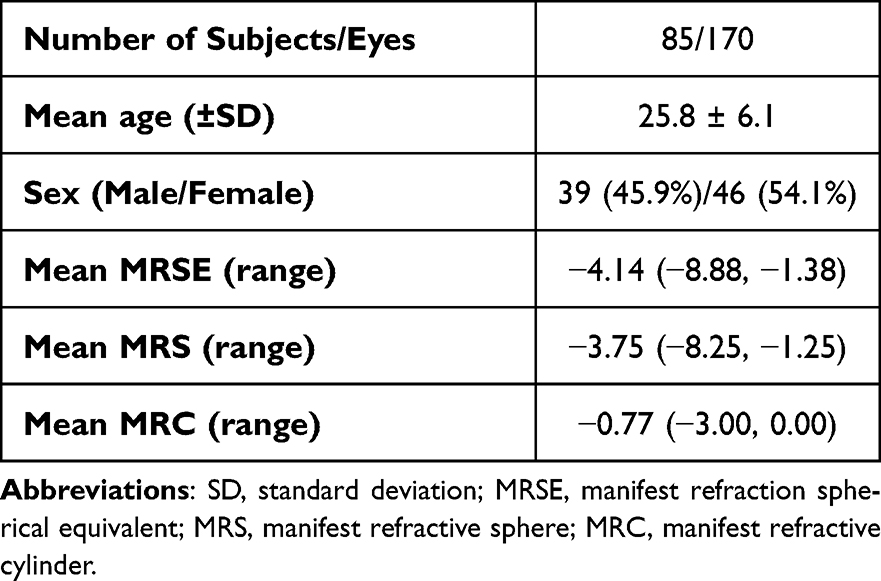 |
Table 2 Baseline Characteristics |
Visual Acuity
Mean logMAR UDVA was 1.02 ± 0.11 at the preoperative visit and significantly improved to −0.07 ± 0.07 at the 6-month postoperative visit (p < 0.0001). Monocular UDVA was 20/40 or better in 100% of eyes at the 1-week, 1-, 3- and 6-month study visits, exceeding the primary effectiveness endpoint target of 85% at 1 month. Similar results were observed for binocular UDVA over time, with 100% of eyes achieving 20/40 or better from the 1-week postoperative visit onwards. At the 1-day visit, 65.9% of eyes achieved 20/20 or better monocular UDVA, which increased to 85.4% at 1 week, 91.5% at 1 month, and 96% at 3 and 6 months (Figure 1).
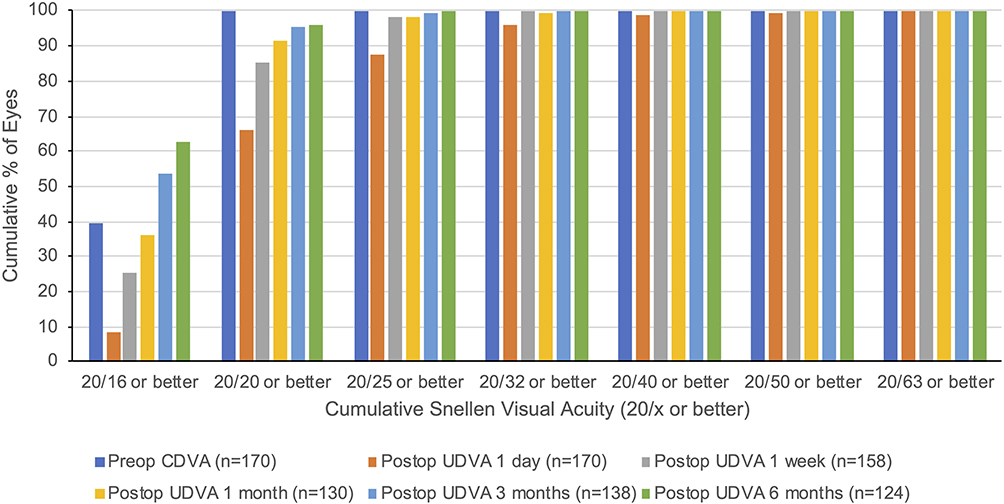 |
Figure 1 Cumulative Snellen visual acuity (20/× or better) comparing postoperative (postop) uncorrected distance visual acuity (UDVA) with preoperative (preop) corrected distance visual acuity (CDVA) at each time point. |
Mean logMAR CDVA was −0.04 ± 0.04 at the preoperative visit, and significantly improved to −0.11 ± 0.05 at the 6-month postoperative visit (p < 0.0001). All eyes achieved 20/20 or better monocular CDVA at 3 and 6 months. CDVA was maintained over time, with no eyes (0%) showing any loss of lines compared to preoperative CDVA at 6 months (Figure 2). The primary safety endpoint of <5% eyes showing >2 lines of CDVA loss at each time point was met. Further, gains of 1 and 2 lines of CDVA were achieved in 48.4% and 11.3% of eyes, respectively, at 6 months (Figure 2). The safety index of the treatment was 1.05 ± 0.14, 1.14 ± 0.17, and 1.18 ± 0.17 at the 1-week, 3-month, and 6-month visits, respectively. The efficacy Index was 0.95 ± 0.14, 1.06 ± 0.18, and 1.08 ± 0.18 at the 1-week, 3-month, and 6-month visits, respectively.
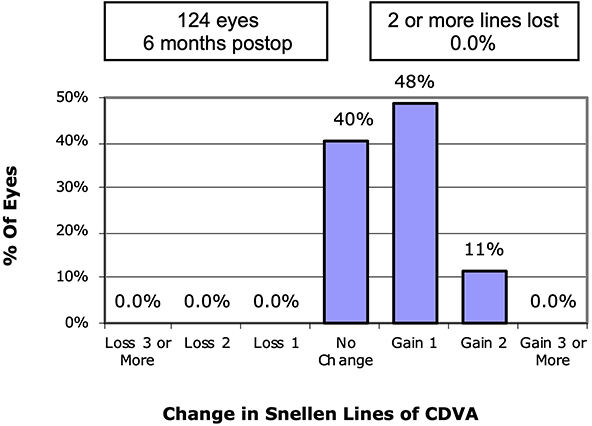 |
Figure 2 Change in corrected distance visual acuity (CDVA) at 6 months compared to preoperative. |
Refractive Outcomes
Regression analysis of attempted versus achieved MRSE at 3 (Figure 3A) and 6 (Figure 3B) months showed an R2 = 0.97 at both time points, with a tendency towards slight under-correction especially for higher myopes. Two eyes (of one subject) were under-corrected by greater than 1.00 D but less than 2.00 D. Preoperative MRSE for this subject was OD −6.50 D, OS −6.13 D. Accuracy of MRSE relative to the target of emmetropia is summarized in Table 3. The predictability of this procedure for ± 0.50 D of post-operative refractive error was 93.5% (129/138) at 3 months and 91.1% (113/124) at 6 months. The predictability of this procedure for ± 1.00 D was 98.6% (136/138) at 3 months and 98.4% (122/124) at 6 months (Figure 4). Accuracy of MRC relative to zero cylinder target is summarized in Table 4. At 6 months, 92% of the eyes had MRC within ± 0.50 D and 100% of eyes within ± 1.00 D.
 |
Table 3 Accuracy of Manifest Refraction Spherical Equivalent (MRSE) Relative to Emmetropia Target |
 |
Table 4 Accuracy of Manifest Refractive Cylinder (MRC) Relative to Zero Cylinder Target |
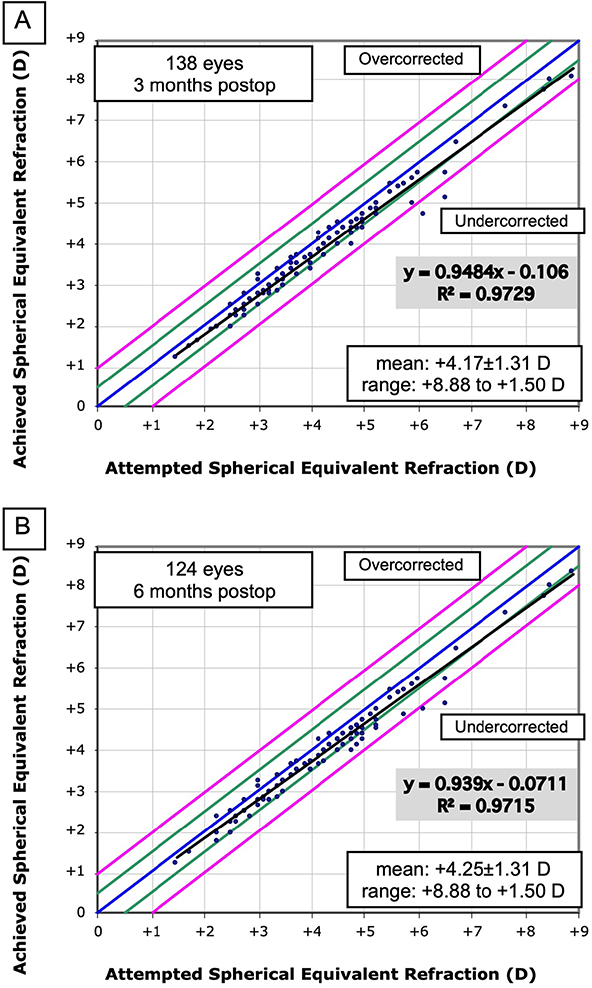 |
Figure 3 Attempted versus achieved spherical equivalent refraction at (A) 3 and (B) 6 months. The blue line indicates a perfect result, and the green and pink lines depict over- and under-correction of 0.50 D and 1.00 D, respectively. |
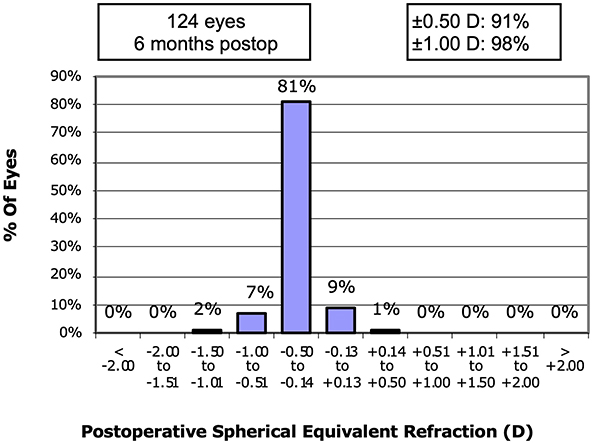 |
Figure 4 Spherical equivalent refractive accuracy at 6 months. |
The distribution of refractive astigmatism at 6 months compared to baseline is shown in Figure 5. Results of the vector analyses are summarized in Supplementary Tables S1–S3. The mean absolute EV was 0.19 D ± 0.27 D, the mean CR was 0.90 ± 0.28, and the mean ER was 0.22 ± 0.37. The mean EM was 0.04 D ± 0.27 D. Additionally, 95% (118/124) of eyes had an absolute EM within 0.50 D. The mean EA was 2.27 ± 17.88 degrees and 84% (104/124) of eyes had an absolute EA ≤15 degrees at 6 months.
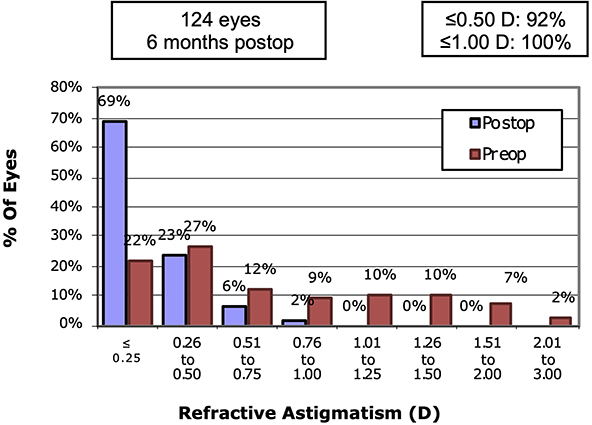 |
Figure 5 Distribution of refractive astigmatism at 6 months (Postop) compared to preoperative (Preop). |
Mean postoperative MRSE was stable over time, ranging from −0.34 D ± 0.24 D at 1 month to −0.33 D ± 0.23 at 6 months (Figure 6). Only two eyes (1.6%) showed a change in MRSE by >0.5 D between the 3- and 6-month visits. In the consistent cohort, refractive stability was achieved by 3 months with 100% (114/114) of eyes having a change in MRSE within ± 0.50 D between 1 and 3 months. Mean change in MRSE per month was 0.01 D (Table 5). The 95% confidence interval of mean change in MRSE included zero (−0.001, 0.061), confirming refractive stability at 6 months.
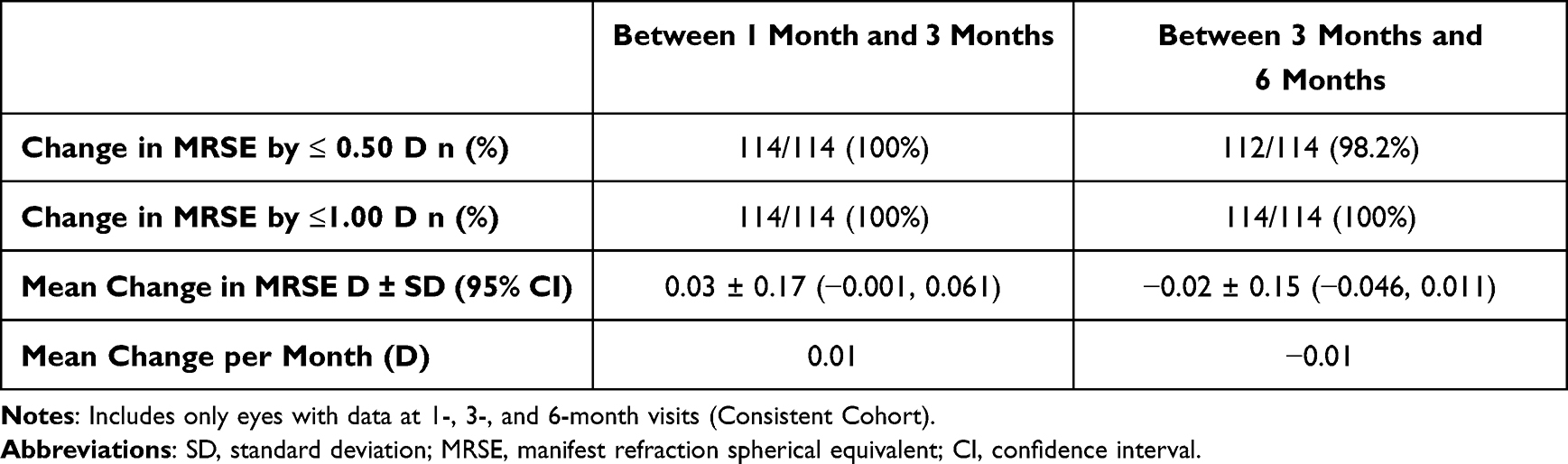 |
Table 5 Refractive Stability Between 1 and 3 Months, and 3 and 6 Months |
 |
Figure 6 Stability of spherical equivalent refraction over 6 months. |
Medical Findings, Surgical Complications, and Adverse Events
No (0%) serious adverse events were noted during the study. Subconjunctival hemorrhages were observed intraoperatively in 2 eyes of 1 subject, which resolved at 1 week. Trace corneal edema was noted in 6 eyes (3.5%) at the 1-day visit, which resolved by the 1-week visit. Mild corneal haze was observed in 1 eye (0.6%) at the 1-day visit, which also fully resolved by the 1-week visit. Corneal scarring, rated as barely visible on slit-lamp examination, was observed at the edge of the entry cut in 14 eyes (8.2%) at the 1-day visit, which increased to 60 eyes at the 3-month visit (43.5%) but then decreased to 30 eyes (24.2%) at the 6-month visit. Debris were noted in the corneal interface in one eye (0.6%) at the 1-day and 1-week visits. In two eyes (1.2%), the entry cut was inadvertently extended. One case was due to subject movement during lenticule removal. At 3 months, the subject’s UDVA and CDVA were 20/20 and 20/17, respectively. In the second case, there was a small uncut area in the periphery at the 4–5 o’clock position that required significant dissection. Intraoperative OCT showed a small uncut lenticular remnant, which was removed with further dissection, which was confirmed with OCT. The tissue manipulation resulted in the extension of the entry cut. This subject’s UDVA and CDVA at 3 months postoperatively were 20/23 and 20/18, respectively. None of these cases were clinically significant. Very few non-directed ocular symptoms were reported by the subjects; at 3 months, ocular irritation was reported in one eye (0.7%) and at 6 months, blurred intermediate vision was reported in 2 eyes (1.6%) and foreign body sensation in 2 eyes (1.6%).
Surgical Experience
Surgeon ratings of ease of lenticule removal are summarized in Figure 7. There was no/minimal (grade 0 or 1) difficulty in lenticule dissection in 85.3% of the eyes. Only 3/169 eyes (1.8%) were rated as grade 3 requiring significant dissection, and no eyes were rated as grade 4 (unable to dissect). No suction losses occurred during laser treatment and only one docking attempt was required for 93.3% of eyes.
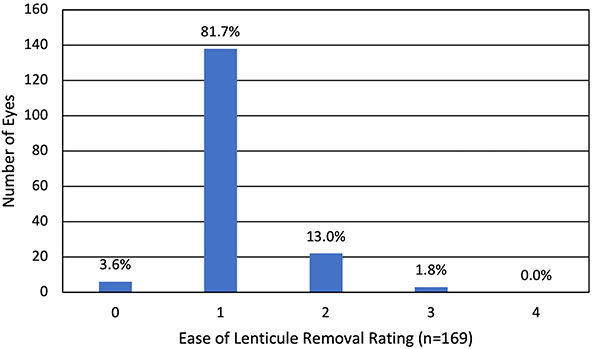 |
Figure 7 Ease of lenticule removal surgeon ratings (n=169), where 0 = no dissection needed and 4 = unable to dissect. Notes: See Table 1 for additional rating scale details. Data missing for 1 eye. |
Discussion
In a scanning electron microscopy study of human corneal lenticules after VisuMax (Carl Zeiss Meditec) femtosecond laser surgery, Kunert et al found that tissue bridges, cavitation bubbles and scratches caused surface irregularities.15 Surface regularity increased as pulse energy decreased, suggesting optimizing spot separation and pulse energy could lead to better corneal outcomes.15 High pulse energy, as used in first generation femtosecond lasers, was also implicated in the development of complications such as transient light sensitivity syndrome20 and corneal haze, due to activation of corneal keratocytes.15,21
The ELITA laser system was designed to deliver lower energy per pulse (40–90 nJ) compared to other laser systems on the market, such as the Carl Zeiss Meditec VisuMax (100–180 nJ)11,12 and Schwind ATOS (100–120 nJ),5,22 to produce continuous tissue-bridge-free corneal lenticules that are easy to remove to enable faster visual recovery. Another unique feature of the ELITA system is the biconvex lenticule shape that creates identical surfaces and tissue matching following lenticule removal. The biconvex shape is expected to cut less collagen fibers in the peripheral cornea by cutting deeper into the stroma, thereby potentially producing less opaque-bubble-layer and better preserving corneal biomechanical strength.23 Additionally, the biconvex lenticule shape is expected to better preserve corneal nerves.24,25 It is worthwhile noting that both the plano-convex lenticule shape, as used in conventional LALEX procedures, and the biconvex lenticule shape are calculated based on the same optical principle,3 and the volumes of the two lenticule shapes for a given refractive correction are the same. The steep learning curve of LALEX procedures, with lenticule dissection and extraction being the most difficult steps,13 has been shown to be a main barrier to adoption for many surgeons. In this study, ease of lenticule removal in the SILK procedure was rated favorably by the surgeons, with 85.3% of eyes requiring no or only mild dissection of the lenticule. In addition, immune responses to the laser treatment were minimal, with only one eye (0.6%) developing corneal haze at the 1-day visit, which was mild in nature and fully resolved by the 1-week visit. These results compared favorably to a 3-month clinical cohort study of 1574 eyes undergoing bilateral SMILE, where corneal haze (grade 0.5 to 1) was observed in 8% of eyes postoperatively.26
The ELITA Femtosecond Laser System with the SILK procedure produced excellent visual outcomes in this 6-month study. Fast visual recovery was observed, with 65.9% of eyes achieving UDVA of 20/20 at 1 day postoperatively, which improved to 85.4% at 1 week, 91.5% at 1 month and then 96% at 3 and 6 months. In comparison, visual recovery was slower following SmartSight lenticule extraction with only 37% and 71% of eyes achieving UDVA of 20/20 at postoperative 1 day and 1 week, respectively.22 When compared to SMILE, visual recovery was also faster at 1 day in this study, with only 55% of eyes undergoing SMILE achieving UDVA of 20/20 or better compared to 65.9%.27 However, by one week, the results were similar between the SILK and SMILE procedures, with 89% of SMILE treated eyes achieving UDVA of 20/20 or better.27
Monocular UDVA was 20/40 or better in 100% of eyes from the 1-week visit onwards in this study, exceeding the primary effectiveness endpoint target of 85%. The primary safety endpoint of <5% eyes showing >2 lines of CDVA loss at each time point was also met, with no eyes showing losses of >2 lines of CDVA. At 6 months, no losses of any lines of CDVA were recorded while improvements in CDVA were observed, with 48% of eyes gaining 1 line and 11% of eyes gaining 2 lines of CDVA compared to preoperative. In comparison, in a 6-month study of 113 eyes following SMILE surgery, 4% of eyes lost 1 line and 2% of eyes lost 2 lines of CDVA.27 In a 12-month study of 221 treated with SmartSight lenticule extraction, 1% of eyes lost 1 line of CDVA.5
For safety index, a value below 0.85 indicates that 2 or more lines of CDVA were lost. For efficacy index, a value below 0.8 indicates a loss of more than 2 lines of UDVA.18 Safety and efficacy indices exceeded these cut-offs at all follow-up visits, deeming the SILK procedure successful. The SILK safety and efficacy indices were comparable to those reported for the SMILE procedure;28–30 however, the safety index was better than that reported following the CLEAR procedure (0.98 at 10 months with CLEAR4 compared to 1.18 at 6 months achieved in this study).
Accuracy and stability of correction were also demonstrated, with 91.1% and 91.9% of eyes within ±0.50 D of target for MRSE and MRC, respectively, at 6 months. Refractive stability was achieved by 3 months following surgery and was maintained through 6 months. There was a tendency toward slight under-correction of MRSE by approximately one-third of a diopter, which may explain why 65.9% of eyes achieved UDVA of 20/20 or better at 1 day compared to 87.6% of eyes achieving 20/25 or better at the same visit. This under-correction could be addressed with nomogram modifications to potentially improve visual outcomes further. Only two eyes were under-corrected by more than 1 D, and those were two eyes of one subject, suggesting a possible difference in corneal structure and/or healing response.
The cylinder power and axis of astigmatism are most effectively represented and described mathematically by a vector. This allows the combination of magnitude and direction to be specified using a single mathematical expression.19 Using ANSI recommended vector analyses,19 the mean absolute EV was less than a quarter of a diopter. The mean CR of 0.9 was close to the ideal of 1.0, implying a slight under-correction of the cylinder, which could also be addressed with nomogram adjustments. The EM is the difference of the magnitude between the SIRC and the IRC (ideally 0 D); the mean EM was very small at only 0.04 D, further demonstrating the accuracy of the SILK procedure. When compared to SMILE after 12 months, the EM in this study was similar to the SMILE EM of −0.05 D reported by Zhang et al,31 but more favorable than the EM of −0.26 D reported by Jabbarvand et al in a similar population of subjects with low astigmatism (≤3.0 D cylinder).32 When assessing whether the treatment was applied at the correct axis, the mean EA in this study (2.27 ± 17.88 degrees) was also similar as that reported for SMILE at 12 months (−3.04 ± 11.57 degrees)31 but varied in direction from the IRC between the two procedures.31
The purpose of this clinical trial was to evaluate the visual outcomes of the ELITA Femtosecond Laser System. The primary safety and efficacy endpoints were clearly defined based on regulatory guidance, and standardized graphs for reporting of refractive surgery outcomes were utilized to enable comparison with other published outcomes. A limitation of this study is that it was conducted at two sites in one country. Future studies could include additional sites, more diverse patient population, and comparative study designs to other corneal refractive procedures.
No safety concerns were identified during this 6-month study, although follow-up was limited to only 6 months. Medical findings and surgical complications were minimal, consistent with other studies of LALEX procedures,10 and no serious adverse events occurred, supporting the safety of the SILK procedure using the ELITA system. Longer term follow-up of subjects up to 12 months is ongoing and will provide additional safety data and insights into the longer term visual performance achieved.
Conclusion
The ELITA Femtosecond Laser System delivered a consistent, safe, and effective treatment of myopic refractive errors with and without astigmatism over 6 months. Easy lenticule removal and fast visual recovery were demonstrated and supported the primary clinical hypothesis, with 85.4% of eyes achieving 20/20 or better and 100% of eyes achieving 20/40 or better UDVA 1 week after surgery; refractive stability was achieved as early as 3 months. Medical findings and surgical complications were minimal, and no serious adverse events occurred. Longer term follow-up of subjects up to 12 months is ongoing and will be reported in a future publication.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data. A summarized report with endpoints data tables based on statistical plan and analysis may be requested directly from the corresponding author for consideration. Access to anonymized data may be granted following review. Content with granted access will be available through email or other appropriate formats and for 3 months, upon review and consideration.
Acknowledgments
Manuscript preparation and editorial support were provided by Dr Carol Lakkis, iBiomedical Consulting (Melbourne, VIC, Australia) and funded by Johnson & Johnson Surgical Vision, Inc. Dr Ritika Sachdev (Centre for Sight, New Delhi, India), Dr Sriharsha Nagaraj (Narayana Nethralaya Eye Hospital, Bangalore, India), Akshay Shah (Actalent Services, Chicago, IL, USA), and Carmen Jones (Johnson & Johnson Surgical Vision, Inc., Milpitas, CA, USA) facilitated the conduct of this clinical study. Jesse Nelson (Johnson & Johnson Surgical Vision, Inc., Milpitas, CA, USA) was the lead clinical training expert for this study. Irene Yau (Johnson & Johnson Surgical Vision, Inc., Irvine, CA, USA) coordinated, facilitated, and enabled the preparation of this manuscript.
Funding
This study was supported by Johnson & Johnson Surgical Vision, Inc., which participated in the design and conduct of the study.
Disclosure
The authors have made the following disclosures:
M.S.S.: Consultant to Johnson & Johnson Surgical Vision, Inc. R.S., P.K., and R.M perform research supported by Johnson & Johnson Surgical Vision, Inc. B.L.S., Y.W., H.F., A.P.V., and M.L: Employees of Johnson & Johnson Surgical Vision, Inc. The authors report no other conflicts of interest in this work.
References
1. Aristeidou A, Taniguchi EV, Tsatsos M, et al. The evolution of corneal and refractive surgery with the femtosecond laser. Eye Vis. 2015;2:12. doi:10.1186/s40662-015-0022-6
2. Fuest M, Mehta JS. Advances in refractive corneal lenticule extraction. Taiwan J Ophthalmol. 2021;11(2):113–121. doi:10.4103/tjo.tjo_12_21
3. Munnerlyn CR, Koons SJ, Marshall J. Photorefractive keratectomy: a technique for laser refractive surgery. J Cataract Refract Surg. 1988;14:46–52. doi:10.1016/S0886-3350(88)80063-4
4. Leccisotti A, Fields SV, De Bartolo G. Refractive corneal lenticule extraction with the CLEAR femtosecond laser application. Cornea. 2023;42(10):1247–1256.
5. Pradhan KR, Arba Mosquera S. Twelve-month outcomes of a new refractive lenticular extraction procedure. J Optom. 2023;16(1):30–41. doi:10.1016/j.optom.2021.11.001
6. Janiszewska-Bil D, Czarnota-Nowakowska B, Grabarek BO, Dobrowolski D, Wylegala E, Lyssek-Boron A. Comparison of vision correction and corneal thickness at 180-day follow-up after Femtosecond Laser-Assisted In-Situ Keratomileusis (FS-LASIK), Photorefractive Keratectomy (PRK), and Small Incision Lenticule Extraction (SMILE): a study from a single center in Poland of 120 patients with myopia. Med Sci Monit. 2023;29:e939099. doi:10.12659/MSM.939099
7. Wei S, Wang Y, Wu D, Zu P, Zhang H, Su X. Ultrastructural changes and corneal wound healing after SMILE and PRK procedures. Curr Eye Res. 2016;41(10):1316–1325. doi:10.3109/02713683.2015.1114653
8. Kobashi H, Kamiya K, Shimizu K. Dry eye after small incision lenticule extraction and femtosecond laser-assisted LASIK: meta-analysis. Cornea. 2017;36(1):85–91. doi:10.1097/ICO.0000000000000999
9. Song YW, Cui MF, Feng Y, Qu M, Gao Y, He R. Comparative study of functional optical zone: small incision lenticule extraction versus femtosecond laser assisted excimer laser keratomileusis. Int J Ophthalmol. 2023;16(2):238–244. doi:10.18240/ijo.2023.02.10
10. Moshirfar M, Santos JM, Wang Q, et al. A literature review of the incidence, management, and prognosis of corneal epithelial-related complications after Laser-Assisted In Situ Keratomileusis (LASIK), Photorefractive Keratectomy (PRK), and Small Incision Lenticule Extraction (SMILE). Cureus. 2023;15(8):e43926.
11. Ji YW, Kim M, Kang DSY, et al. Lower laser energy levels lead to better visual recovery after small-incision lenticule extraction: prospective randomized clinical trial. Am J Ophthalmol. 2017;179:159–170. doi:10.1016/j.ajo.2017.05.005
12. Shah R, Shah S. Effect of scanning patterns on the results of femtosecond laser lenticule extraction refractive surgery. J Cataract Refract Surg. 2011;37(9):1636–1647. doi:10.1016/j.jcrs.2011.03.056
13. Titiyal JS, Kaur M, Rathi A, Falera R, Chaniyara M, Sharma N. Learning curve of small incision lenticule extraction: challenges and complications. Cornea. 2017;36(11):1377–1382. doi:10.1097/ICO.0000000000001323
14. Chansue E. Current Technique and Instrumentation for SMILE. In: Sekundo W, editor. Small Incision Lenticule Extraction (SMILE). Principles, Techniques, Complication Management, and Future Concepts. Switzerland: Springer International Publishing; 2015:56–65.
15. Kunert KS, Blum M, Duncker GI, Sietmann R, Heichel J. Surface quality of human corneal lenticules after femtosecond laser surgery for myopia comparing different laser parameters. Graefes Arch Clin Exp Ophthalmol. 2011;249(9):1417–1424. doi:10.1007/s00417-010-1578-4
16. Johnson & Johnson Vision. Johnson & Johnson Vision Receives CE mark approval for new corneal refractive technology, the ELITA femtosecond laser system; 2023. Available from: https://www.jjvision.com/press-release/johnson-johnson-vision-receives-ce-mark-approval-new-corneal-refractive-technology.
17. Chan C, Lawless M, Sutton G, Versace P, Hodge C. Small incision lenticule extraction (SMILE) in 2015. Clin Exp Optom. 2016;99(3):204–212. doi:10.1111/cxo.12380
18. Gomel N, Negari S, Frucht-Pery J, Wajnsztajn D, Strassman E, Solomon A. Predictive factors for efficacy and safety in refractive surgery for myopia. PLoS One. 2018;13(12):e0208608. doi:10.1371/journal.pone.0208608
19. Eydelman MB, Drum B, Holladay J, et al. Standardized analyses of correction of astigmatism by laser systems that reshape the cornea. J Refract Surg. 2006;22(1):81–95. doi:10.3928/1081-597X-20060101-16
20. Netto MV, Mohan RR, Medeiros FW, et al. Femtosecond laser and microkeratome corneal flaps: comparison of stromal wound healing and inflammation. J Refract Surg. 2007;23(7):667–676. doi:10.3928/1081-597X-20070901-05
21. McCulley JP, Petroll WM. Quantitative assessment of corneal wound healing following IntraLASIK using in vivo confocal microscopy. Trans Am Ophthalmol Soc. 2008;106:84–90; discussion 90–82.
22. Pradhan KR, Mosquera SA. Initial experience with the SCHWIND ATOS and SmartSight lenticule extraction. J Clin Res Med. 2020;3(4):1–5.
23. Randleman JB, Dawson DG, Grossniklaus HE, McCarey BE, Edelhauser HF. Depth-dependent cohesive tensile strength in human donor corneas: implications for refractive surgery. J Refract Surg. 2008;24(1):S85–S89. doi:10.3928/1081597X-20080101-15
24. Wong AHY, Cheung RKY, Kua WN, Shih KC, Chan TCY, Wan KH. Dry eyes after SMILE. Asia Pac J Ophthalmol. 2019;8(5):397–405. doi:10.1097/01.APO.0000580136.80338.d0
25. Marfurt CF, Cox J, Deek S, Dvorscak L. Anatomy of the human corneal innervation. Exp Eye Res. 2010;90(4):478–492. doi:10.1016/j.exer.2009.12.010
26. Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121(4):822–828. doi:10.1016/j.ophtha.2013.11.006
27. Liu M, Chen Y, Wang D, et al. Clinical outcomes after SMILE and femtosecond laser-assisted LASIK for myopia and myopic astigmatism: a prospective randomized comparative study. Cornea. 2016;35(2):210–216. doi:10.1097/ICO.0000000000000707
28. Ang M, Farook M, Htoon HM, Mehta JS. Randomized clinical trial comparing femtosecond LASIK and small-incision lenticule extraction. Ophthalmology. 2020;127(6):724–730. doi:10.1016/j.ophtha.2019.09.006
29. Cao K, Zhang J, Wang J, et al. Implantable collamer lens versus small incision lenticule extraction for high myopia correction: a systematic review and meta-analysis. BMC Ophthalmol. 2021;21(1):450. doi:10.1186/s12886-021-02206-9
30. Wei R, Li M, Zhang H, et al. Comparison of objective and subjective visual quality early after implantable collamer lens V4c (ICL V4c) and small incision lenticule extraction (SMILE) for high myopia correction. Acta Ophthalmol. 2020;98(8):e943–e950. doi:10.1111/aos.14459
31. Zhang J, Wang Y, Wu W, Xu L, Li X, Dou R. Vector analysis of low to moderate astigmatism with small incision lenticule extraction (SMILE): results of a 1-year follow-up. BMC Ophthalmol. 2015;15:8. doi:10.1186/1471-2415-15-8
32. Jabbarvand M, Khodaparast M, Moravvej Z, et al. Vector analysis of moderate to high myopic astigmatism after small-incision lenticule extraction (SMILE): 12-month follow-up. Eur J Ophthalmol. 2022;32(6):3312–3320. doi:10.1177/11206721221080821
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.