")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Ruxolitinib Treatment During Myelofibrosis Leads to Cutaneous Mycobacterium marinum Infection: A Case Report
Authors Chen X, Zhang D , Wang T , Ma W
Received 22 March 2023
Accepted for publication 27 May 2023
Published 13 June 2023 Volume 2023:16 Pages 1499—1503
DOI https://doi.org/10.2147/CCID.S413592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Xiaonan Chen,1 Dong Zhang,2 Teng Wang,3 Weiyuan Ma2
1Department of Hematology, Affiliated Hospital of Weifang Medical University, Weifang, People’s Republic of China; 2Department of Dermatology, Affiliated Hospital of Weifang Medical University, Weifang, People’s Republic of China; 3Department of Orthopedics, Qilu Hospital of Shandong University, Jinan, People’s Republic of China
Correspondence: Teng Wang, Qilu Hospital of Shandong University, Jinan, People’s Republic of China, Tel +86-531-82169361, Email [email protected] Weiyuan Ma, Department of Dermatology, Affiliated Hospital of Weifang Medical University, Weifang, People’s Republic of China, Tel +86-536-3081272, Email [email protected]
Abstract: Mycobacterium marinum is an atypical bacterium, and skin infections caused by it are relatively rare, usually occurring in workers engaged in seafood processing and housewives who clean and prepare fish for consumption. The infection often occurs after the skin is punctured by fish scales, spines, etc. The JAK/STAT signaling pathway is closely related to the human immune response to infections. Therefore, JAK inhibitors may induce and exacerbate various infections in clinical practice. This article reports a case of mycobacterium marinum skin infection in the left upper limb of a female patient with chronic idiopathic myelofibrosis during treatment with ruxolitinib. The patient denied being punctured or scratched by fish scales or spines. Clinical manifestations included multiple infiltrative erythemas and subcutaneous nodules in the thumb and forearm. Histopathological examination showed infiltration of mixed acute and chronic inflammatory cells in the subcutaneous tissue. The diagnosis was ultimately confirmed by NGS sequencing. The patient was cured after taking moxifloxacin and clarithromycin for 10 months. Infection is a common adverse reaction of JAK inhibitors, but no literature has reported on mycobacterium marinum skin infections occurring during JAK inhibitor treatment, which is relatively rare. As the clinical application of JAK inhibitors becomes more widespread, the skin infections they cause may present in various forms and require the attention of clinicians.
Keywords: ruxolitinib, JAK inhibitors, Mycobacterium marinum, skin, infection
Introduction
JAK inhibitors have been approved by the US Food and Drug Administration (FDA) for the treatment of various diseases such as myelofibrosis, rheumatoid arthritis, and atopic dermatitis. However, they may lead to serious adverse reactions such as thrombosis, infection, and tumors, and thus have been given a black box warning by the FDA.1–3 Among the skin infections that occur during JAK inhibitor treatment, herpes zoster is the most common, and there have been few reports of atypical mycobacterial skin infections.4–6 Skin infections caused by atypical mycobacteria are a relatively rare type of infectious skin disease, often caused by Mycobacterium marinum, Mycobacterium chelonae, and other infections. Patients often work in aquaculture and processing, or are housewives, chefs, etc. Clinically, it manifests as infiltrative plaques and nodules in the traumatized areas, skin, and subcutaneous tissues, which can be distributed along the lymphatic vessels in a band-like pattern.7 This article reports a female patient with myelofibrosis who developed a Mycobacterium marinum infection in the skin of the left upper limb during treatment with the JAK inhibitor ruxolitinib. The clinical presentation was infiltrative erythema and subcutaneous nodules on the left thumb and forearm, and the histopathology showed mixed infiltration of acute and chronic inflammatory cells in the subcutaneous tissue. NGS sequencing confirmed the infection was caused by Mycobacterium marinum. This case illustrates the diversity of skin infections that may occur during treatment with JAK inhibitors, and the need for clinical attention to atypical mycobacterial skin infections cannot be ignored.
Case Presentation
The patient is a 56-year-old female who came to seek medical attention due to the appearance of patches and nodules on her left thumb and forearm for the past 1.5 months. There was no obvious trigger before the onset. A red nodule about the size of a soybean appeared on the left thumb, and treatment with compound polymyxin B ointment (containing polymyxin B and lidocaine, etc.) was initiated for 2 weeks, but the skin lesion increased in size. Two red, infiltrative patches appeared on the skin of the left forearm 1 month prior. The patient denied any history of being stabbed or scratched by fish bones or scales, cleaning fish, or cleaning fish tanks before the onset. The patient was diagnosed with myelofibrosis 6 years ago and is currently on treatment with ruxolitinib (15mg per dose, twice a day), which has effectively controlled the disease. Physical examination revealed no obvious abnormalities. Dermatological examination showed a red nodule approximately 1.0 cm in diameter on the back of the distal phalanx of the left thumb, with a small amount of scales on the surface, hard and tough to the touch, and normal skin temperature. Two dark red infiltrative patches with clear boundaries and crusting and desquamation on the surface were seen on the left forearm (Figure 1). Skin scrapings were taken and examined under a microscope after being stained with 10% KOH, but no fungal hyphae or spores were found. Tissue blocks were taken for fungal culture, but no colonies grew. Total DNA was extracted from the tissue block and subjected to NGS sequencing, which revealed Mycobacterium marinum. Histological examination of the tissue showed irregular epidermal hyperplasia and downward extension of the epidermal papillae. Inflammatory cells such as lymphocytes, neutrophils, eosinophils, histiocytes, and multinucleated giant cells were diffusely infiltrated in the dermis (Figure 2). Staining with PAS, silver nitrate, and acid-fast staining were negative. Based on the clinical presentation and laboratory findings, a final diagnosis of cutaneous Mycobacterium marinum infection was made. Treatment with clarithromycin 250mg per dose, twice a day and moxifloxacin 400mg per dose, once a day was initiated. Meanwhile, administration of ruxolitinib was stopped and lenalidomide was used to control myelofibrosis. Regular liver function, renal function, and electrocardiogram monitoring was performed before and during treatment, and no abnormal changes were observed. After 1 month of treatment, the skin lesions began to shrink, and no new skin lesions appeared. After 10 months of treatment, the patient was followed up by phone, and the skin lesions had completely disappeared, and treatment was discontinued.
 |
Figure 1 Skin manifestations of Mycobacterium marinum infection. Multiple red nodules and plaques on the left thumb and forearm. |
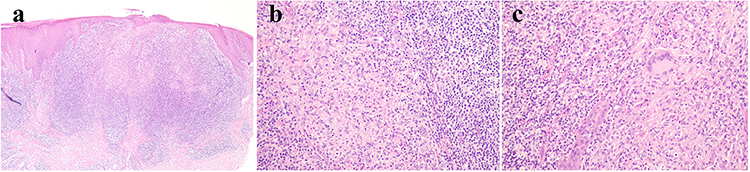 |
Figure 2 Histopathological examination. (a) Under low-power microscopy, there is diffuse inflammatory cell infiltration throughout the entire dermis (HE, ×40). (b) Under high-power microscopy, there is diffuse infiltration of inflammatory cells predominantly composed of lymphocytes, histiocytes, and neutrophils (HE, ×200). (c) There are granulomatous inflammatory changes with the presence of multinucleated giant cells (HE, ×200). |
Discussion
JAK (Janus kinase) is a family of non-receptor tyrosine kinases consisting of four members, Jak1, Jak2, Jak3, and Tyk2. The N-terminal domain of JAK binds to receptors, while the C-terminal domain contains the kinase domain. The substrate of JAK is STAT (signal transducer and activator of transcription), which has an N-terminal SH2 domain and a nuclear localization signal (NLS), a DNA binding domain in the middle, and a conserved tyrosine residue that is essential for its activation at the C-terminal end. Currently, seven members of the STAT family have been identified. After phosphorylation by JAK, STAT undergoes dimerization and translocates into the nucleus to regulate the expression of target genes. This signaling pathway is known as the JAK-STAT pathway. Research has found that JAK pairs form different signaling pathways for various cytokines downstream of STAT. For example, JAK1 and JAK3 regulate lymphocytes for IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21, JAK1 and JAK2 regulate IFN-γ, a pair of JAK2 regulates EPO, TPO, GM-CSF, IL-3, and IL-5, and IFN-α and IFN-β are regulated by JAK1 and TYK2.8 When the signal molecule (such as cytokines) binds to the receptor on the cell surface, JAK (Janus kinase) is activated and phosphorylates the receptor on the cell membrane, forming a dimer, which then activates STAT (signal transducer and activator of transcription) by phosphorylation. The phosphorylated STAT dimer translocates into the nucleus, binds to specific DNA, and regulates gene transcription, thereby affecting biological processes such as cell growth, differentiation, and apoptosis. Aberrant activation of the JAK/STAT signaling pathway is associated with various diseases, such as inflammation, immune disorders, and cancer. Therefore, JAK inhibitors are a new type of therapeutic drug that can intervene in this pathway by inhibiting JAK activation and treat related diseases.9,10
Myelofibrosis is a type of bone marrow disorder characterized by abnormal proliferation, and approximately 50% of patients with myelofibrosis have been found to have the JAK2 V617F mutation. This mutation occurs in the pseudokinase domain of JAK2, causing a conformational change that results in sustained activation of the JH1 kinase domain independent of extracellular cytokine signaling, leading to cell proliferation and tumorigenesis. Ruxolitinib, initially developed by Incyte, is a small-molecule inhibitor of JAK1/JAK2 kinases, and due to its inhibitory effect on JAK2, it was approved by the FDA in November 2011 for the treatment of intermediate-2 or high-risk myelofibrosis (MF).11 In 2014, it was further approved for polycythemia vera. Recently, it has also been used to treat acute graft-versus-host disease after organ transplantation.12,13 Ruxolitinib may produce anti-inflammatory effects by inhibiting JAK, so that cytokine production will also be reduced. However, for macrophages exposed to agonists such as Toll-like receptor 4 (TLR4), JAK inhibition may increase the inflammatory potential of macrophages. TLR4 is a receptor that recognizes bacterial components and triggers an immune response. TLR4 is associated with Mycobacterium marinum, including Mycobacterium atipic, and these bacteria can trigger the production of pro-inflammatory cytokines by macrophages through activation of TLR4. Therefore, JAK inhibition may interfere with the normal immune response to these bacteria and increase the risk of inflammation.14,15
Ruxolitinib can cause various infections such as urinary tract infections, respiratory tract infections, and herpes zoster,16 but there are few literature reports of atypical mycobacterial infections of the skin. Skin infections with Mycobacterium marinum, also known as swimming pool granuloma, are caused by M. marinum, a slow-growing, acid-fast, and non-tuberculous mycobacterium that is mainly distributed in natural water environments and aquariums. It can not only cause fish infections but also cause skin infections in humans through trauma. To establish infection, Mycobacterium marinum has the ability to enter and survive within host macrophages. The ability of Mycobacterium marinum to access the cytosol of macrophages and use host actin for motility is a unique characteristic of its pathogenesis. It is worth noting that the patient in this case denied a history of fish bone or scale injuries, cleaning fish, or cleaning fish tanks before the onset of the disease. Skin lesions in M. marinum infections are often solitary nodules on the upper limbs, followed by a sporotrichoid pattern when the pathogen spreads along lymphatic vessels. In some immunocompromised patients (such as those with AIDS, those receiving TNF-α inhibitors, organ transplants, etc.), the disease progresses faster, the skin lesions are more widespread, and even deep-seated infections in visceral organs can occur. In this case, the patient developed skin lesions while receiving ruxolitinib treatment for myelofibrosis and denied a history of trauma, and there have been no literature reports of such cases, suggesting that the infection may be related to the immunosuppression caused by ruxolitinib.17
When skin lesions are observed to be distributed along lymphatic vessels, lymphatic sporotrichosis and epithelioid sarcoma, among other diseases, should be differentiated. Fungal cultures, histopathological examinations, PAS staining, NGS sequencing, and other methods are important for definitive diagnosis. Sporotrichosis often has a history of exposure to wood, soil, plants, etc., and is sensitive to antifungal treatment. Epithelioid sarcoma shows atypical cells in histopathology. In this case, we used tissue NGS sequencing to determine that the pathogen was M. marinum. Treatment often involves using macrolides or tetracyclines for several weeks or even months, and surgical debridement is also an option in some cases.18,19
Conclusion
Infection, tumors, and thrombosis are common serious adverse reactions to JAK inhibitors. In addition to herpes zoster, there is also a possibility of atypical mycobacterial infection of the skin during JAK inhibitor therapy. Atypical mycobacterial skin infections, which often occur after trauma, manifest as local nodules or plaques that can spread along lymphatic vessels in a band-like distribution. Clinically, they need to be differentiated from fungal infections such as sporotrichosis and tumors such as squamous cell carcinoma. In clinical practice, healthcare providers should be aware of the possibility of various infections, including skin infections, in patients using JAK inhibitors. In addition to common viral infections such as herpes zoster, atypical mycobacterial infections should also be considered. NGS sequencing has great value in identifying the causative pathogen of the infection. Discontinuing JAK inhibitors and undergoing long-term, standardized antibiotic treatment can lead to recovery.
Consent
The patient had given written informed consent for the publication of her clinical details. Institutional approval is not required for this case study.
Funding
Research reported in this publication was supported by Traditional Chinese Medicine Science and Technology Project of Shandong Province (No. 2021Q093) and Doctoral Startup Fund of Affiliated Hospital of Weifang Medical University (No. 2021BKQ02).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Kotyla PJ, Engelmann M, Giemza-Stoklosa J, et al. Thromboembolic adverse drug reactions in janus kinase (jak) inhibitors: does the inhibitor specificity play a role? Int J Mol Sci. 2021;22(5):2449. doi:10.3390/ijms22052449
2. Clarke B, Yates M, Adas M, et al. The safety of jak-1 inhibitors. Rheumatology. 2021;60(Suppl 2):ii24–ii30. doi:10.1093/rheumatology/keaa895
3. Winthrop KL. The emerging safety profile of jak inhibitors in rheumatic disease. Nat Rev Rheumatol. 2017;13(4):234–243. doi:10.1038/nrrheum.2017.23
4. Kompa KG, Trottier CA, Hyman CL, Kohli R. Disseminated Mycobacterium avium complex myositis in a patient with graft-versus-host disease. Open Forum Infect Dis. 2022;9(8):ofac385. doi:10.1093/ofid/ofac385
5. Sayabovorn N, Chongtrakool P, Chayakulkeeree M. Cryptococcal fungemia and Mycobacterium haemophilum cellulitis in a patient receiving ruxolitinib: a case report and literature review. BMC Infect Dis. 2021;21(1):27. doi:10.1186/s12879-020-05703-2
6. Anand K, Burns EA, Ensor J, Rice L, Pingali SR. Mycobacterial infections with ruxolitinib: a retrospective pharmacovigilance review. Clin Lymphoma Myeloma Leuk. 2020;20(1):18–23. doi:10.1016/j.clml.2019.08.008
7. Johnson MG, Stout JE. Twenty-eight cases of mycobacterium marinum infection: retrospective case series and literature review. Infection. 2015;43(6):655–662. doi:10.1007/s15010-015-0776-8
8. Agashe RP, Lippman SM, Kurzrock R. Jak: not just another kinase. Mol Cancer Ther. 2022;21(12):1757–1764. doi:10.1158/1535-7163.MCT-22-0323
9. Roskoski R. Janus kinase (jak) inhibitors in the treatment of neoplastic and inflammatory disorders. Pharmacol Res. 2022;183:106362. doi:10.1016/j.phrs.2022.106362
10. Clark JD, Flanagan ME, Telliez JB. Discovery and development of janus kinase (jak) inhibitors for inflammatory diseases. J Med Chem. 2014;57(12):5023–5038. doi:10.1021/jm401490p
11. Harrison C, Kiladjian JJ, Al-Ali HK, et al. Jak inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366(9):787–798. doi:10.1056/NEJMoa1110556
12. Vannucchi AM, Kiladjian JJ, Griesshammer M, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015;372(5):426–435. doi:10.1056/NEJMoa1409002
13. Sailliet N, Brosseau C, Robert JM, et al. Role of jak inhibitors and immune cells in transplantation. Cytokine Growth Factor Rev. 2019;47:62–73. doi:10.1016/j.cytogfr.2019.05.002
14. Wang FY, Wang XM, Wang C, et al. Suppression of Mcl-1 induces apoptosis in mouse peritoneal macrophages infected with Mycobacterium tuberculosis. Microbiol Immunol. 2016;60(4):215–227. doi:10.1111/1348-0421.12368
15. Daza-Cajigal V, Albuquerque AS, Young DF, et al. Partial human Janus kinase 1 deficiency predominantly impairs responses to interferon gamma and intracellular control of mycobacteria. Front Immunol. 2022;13:888427. doi:10.3389/fimmu.2022.888427
16. Barraco F, Greil R, Herbrecht R, et al. Real-world non-interventional long-term post-authorisation safety study of ruxolitinib in myelofibrosis. Br J Haematol. 2020;191(5):764–774. doi:10.1111/bjh.16729
17. Lussana F, Cattaneo M, Rambaldi A, et al. Ruxolitinib-associated infections: a systematic review and meta-analysis. Am J Hematol. 2018;93(3):339–347. doi:10.1002/ajh.24976
18. Petrini B. Mycobacterium marinum: ubiquitous agent of waterborne granulomatous skin infections. Eur J Clin Microbiol Infect Dis. 2006;25(10):609–613. doi:10.1007/s10096-006-0201-4
19. Hashish E, Merwad A, Elgaml S, et al. Mycobacterium marinum infection in fish and man: epidemiology, pathophysiology and management; a review. Vet Q. 2018;38(1):35–46. doi:10.1080/01652176.2018.1447171
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.