")
Back to Journals » Patient Preference and Adherence » Volume 17
Rural, Regional, Racial Disparities in Telemedicine Use During the COVID-19 Pandemic Among US Adults: 2021 National Health Interview Survey (NHIS)
Authors Park JH , Lee MJ, Tsai MH, Shih HJ , Chang J
Received 9 September 2023
Accepted for publication 18 December 2023
Published 20 December 2023 Volume 2023:17 Pages 3477—3487
DOI https://doi.org/10.2147/PPA.S439437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jeong-Hui Park,1,* Min Jee Lee,2,* Meng-Han Tsai,3,4 Huan-Ju Shih,5 Jongwha Chang6
1Department of Health Behavior, School of Public Health, Texas A&M University, College Station, TX, USA; 2Population Science and Policy, School of Medicine, Southern Illinois University, Springfield, IL, USA; 3Georgia Prevention Institute, Augusta University, Augusta, GA, USA; 4Cancer Prevention, Control, & Population Health Program, Georgia Cancer Center, Augusta University, Augusta, GA, USA; 5Department of Health Administration and Policy, School of Public Health, George Mason University, Fairfax, VA, USA; 6Department of Pharmaceutical Sciences, Irma Lerma Rangel School of Pharmacy, Texas A&M University, College Station, TX, USA
*These authors contributed equally to this work
Correspondence: Jongwha Chang, Email [email protected]
Objective: The primary objective of this study is to conduct a comparative analysis of telemedicine utilization patterns among adult populations residing in both rural and urban areas and evaluate the probability of telemedicine adoption among adults dwelling in both rural and urban areas amid the backdrop of the COVID-19 pandemic.
Methods: Our study has attained sample populations (n = 279,260, National Weighted Estimates = 2,391,188,373) through the secondary analysis of the National Health Interview Survey (NHIS) for the year 2021. We examined the relationship between the rural, regional, and racial variables using chi-square tests and binary logistic regression associated with telemedicine use in our multivariable analysis.
Results: Telemedicine use by population decreased with decreasing urbanization level, from 40.2% among adults living in large central metropolitan to 29.7% among adults living in rural area (p< 0.0001). Regarding household income, adults with 400% or more of the federal poverty level (FPL) were significantly more likely to use telemedicine than adults with less than 100% of the FPL. Females were more likely than males to utilize telemedicine. In terms of region, adults living in the West were 1.25 times more likely to use telemedicine than adults living in the Northeast, and minority race/ethnicity groups (eg, Non-Hispanic Black, Hispanic, and other) are less likely to use the telemedicine rather than Non-Hispanic White.
Conclusion: Health equity is attained when all demographic groups enjoy uniform access to healthcare services, but disparities emerge when there are discernible variations in access to treatment. Considering this study’s findings, it becomes evident that the distinctions in poverty rates, median income levels, and healthcare utilization patterns across racial and regional lines may serve as indicators of potential health equity concerns.
Keywords: telemedicine, COVID-19, NHIS sample, healthcare utilization
A Letter to the Editor has been published for this article.
Background
Telehealth has assumed a pivotal role within the contemporary landscape characterized by transformative shifts in mobility dynamics facilitated by technological advancements driven by the ubiquity of smartphones, tablets, computers, and a plethora of digital devices.1 The evolution of virtual services, epitomized by telehealth, which in select instances, obviates the necessity for physical travel and offers a comprehensive spectrum of healthcare services, ranging from preventive measures to therapeutic interventions, care provisions, and support mechanisms.2 The emergence of the COVID-19 pandemic in the early months of 2020 further accentuated the significance of telehealth in the United States (U.S.). This period witnessed a marked concentration of telehealth utilization among adults aged 18–49 years, experiencing an incremental rise from 66% in 2019 to 69% in 2020, and the proportion of telehealth visits attributed to individuals aged 18–49 years exhibited a noticeable increase, elevating from 68% during the inaugural week of January 2020 to 73% by the closing week of March.3 Furthermore, 69% of patients engaged in telehealth encounters during the initial stages of the pandemic in 2020 were managed within the confines of their homes.3
A strategy aimed at mitigating healthcare disparities involves improving the accessibility of healthcare services, with a specific focus on marginalized and underrepresented segments of society, including ethnic minorities and individuals residing in geographically remote or underserved areas.4 Therefore, the central objective of both telemedicine and telehealth pertains to the amelioration of health disparities, achieved by bridging the healthcare accessibility gap that disproportionately affects individuals residing in rural regions, where access to healthcare providers is diminished.5,6 Nonetheless, the effective implementation of telehealth faces barriers and considerations, such as provider barriers including lack of training, uncertainty about the value or ability to provide appropriate care, and the cost of equipment.7 Salient is the digital divide, an obstacle to the widespread utilization of telehealth services. Specifically, 97% of Americans can access high-speed fixed service, but these figures dwindle to 65% and 60% in rural and tribal lands, respectively,8 and eHealth utilization is influenced by demographic factors such as age, gender, and socioeconomic status.9,10
Acknowledging the significance of prioritizing essential medical services, healthcare providers were compelled to make strategic adjustments, resulting in the reduction of non-essential medical appointments.11 While this prioritization strategy was intended to safeguard vital healthcare resources and personnel,12 it concurrently impeded routine access to medical care that individuals had come to rely upon. Moreover, the pandemic ushered in a host of stringent measures, including restrictions on visitors to healthcare facilities.13 While these measures were instituted with the noble intention of curbing the transmission of the virus within healthcare settings, they inadvertently engendered barriers for those seeking medical attention. The resultant reduced access to vital medical care not only posed immediate challenges but also cast a spotlight on the broader systemic vulnerabilities within healthcare infrastructure.14,15
Given the paramount concern surrounding COVID-19, two antecedent studies posit that medical centers should proactively address the pandemic by swiftly incorporating digital tools and technologies, notably telemedicine and virtual care,16 and assert that these technological solutions possess the capacity to reduce emergency room visits, preserve healthcare resources, and mitigate the transmission of COVID-19 by enabling the remote treatment of patients both during and after the pandemic.17 However, undoubtedly, the delicate equilibrium that underpins telemedicine accessibility was severely disrupted by the advent of the COVID-19 pandemic.18,19 In a study focused on pediatric dermatology patients under the age of 18 during the pandemic, the results illuminated factors contributing to disparities in telemedicine utilization, notably, the study highlighted that certain factors, such as being of Hispanic/Latino ethnicity and possessing public insurance, may be linked to discrepancies in access to technology.20 Singh et al conducted a study involving veterans with rheumatoid disease during the COVID-19 pandemic, wherein video-based telemedicine was employed, and reported an increased comfort level among rheumatoid patients with telemedicine.21 However, it is crucial to acknowledge a significant limitation in the study design, as data from participants unable to utilize telemedicine were excluded due to the survey format and this omission represents a notable constraint, preventing the comprehensive reporting of treatment experiences among rheumatoid patients who faced challenges in accessing telemedicine during the COVID-19 era.21
Notwithstanding certain legal and ethical concerns,22 the consensus among the majority of medical professionals is that telemedicine presents a viable avenue for healthcare delivery during global epidemics.23 Therefore, in order to facilitate the successful implementation of telemedicine, the primary objective of this study is to examine the adoption patterns of telemedicine among adults in the United States, considering both rural and urban residency, with a specific focus on the influence of the COVID-19 pandemic, and investigate the association between rates of telemedicine utilization and the variations observed between rural and urban settings. As a secondary objective, the investigation seeks to evaluate the probability of telemedicine usage among US adults, considering socio-demographic characteristics, factors that facilitate or hinder access to health services, and health-related aspects such as perceived or actual health status that necessitate care. This secondary objective is particularly relevant in the context of the ongoing COVID-19 pandemic.
Methods
Data Source
This study constitutes a secondary analysis of the National Health Interview Survey (NHIS) for the year 2021. The NHIS population consisted of civilians aged 18 and older who were not institutionalized in the US NHIS utilized a clustered, stratified, multistage probability sample design. National estimates were generated using sampling weights provided by the NHIS, which accounted for stratification, clustering, and oversampling procedures. We downloaded NHIS datasets available to the public from the NHIS/CDC website. Using subject and family IDs, we utilized personal and individual datasets. The NHIS methods and sample selection are described elsewhere.24 A total of 294,820 individuals aged ≥ 18 years responded to the 2021 NHIS. After excluding all the cases with at least one missing relevant data and cases with refusal or do not know answer (n=15,560), we included 279,260 respondents as the study final sample. This study was approved for waiver from the Institutional Review Board of Texas A&M University (IRB2023-0268).
Variables
The primary outcome of this study was to adults who were said “yes” responses to the question, “In the past 12 months, have you had an appointment with a doctor, nurse, or other health professional by video or by phone?”.25 Demographic variables (age and gender), race/ethnicity, educational attainment, region, rurality, and telemedicine were all measured at the individual level as study variables. Age was a measure of categorization. 1) −44, 2) 45–64, and 3) 65+. Sex was a categorical variable (male 0 female 1). Blacks versus Whites were the self-identified races. Hispanics versus non-Hispanics were the self-identified ethnicities. Educational attainment consisted of the following components: 1) High school dropout, 2) High school graduate, 3) Some college, and 4) Bachelor’s degree or higher. Region was a four-level categorical variable that was encoded as follows: 1) Northeast, 2) the Midwest, 3) the South, and 4) the West. The categories of rurality included the following: 1) Large central metropolitan ̶ counties that encompass the entire population of the largest principal city within the metropolitan statistical areas (MSA) and/or entirely contained within the boundaries of the largest principal city within the MSA and/or house a minimum of 250,000 residents from any principal city within the MSA, 2) Large fringe metropolitan ̶ counties (or their equivalents) are situated in MSAs with a population of 1 million or more but do not meet the criteria to be classified as large central, 3) Medium and small metropolitan ̶ counties (or their equivalents) are found within MSAs with populations ranging from 250,000 to 999,999 or within MSAs with populations below 250,000, 4) Rural ̶ counties (or their equivalents) are located in micropolitan statistical areas and non-core counties.
Statistical Analysis
All statistical analyses for NHIS 2021 utilized sampling weights to accurately represent the entire population. Initially, the characteristics of the final dataset sample were examined. The characteristics of the population were displayed as weighted frequency (percentage) or means (SD). Then, chi-square tests were used to examine the relationship between study variables. In our multivariable analysis, we used binary logistic regression associated with telemedicine use. SAS statistical software was used for all analyses (version 9.4; SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided, and a p-value of 0.05 was used to determine statistical significance.
Results
Patient Characteristics
Table 1 presents the characteristics of the study participants. The 2021 NHIS data identified a total of 279,260 populations (weighted n = 2,391,183,396). Among the sample population, 37% of adults reported using telemedicine within the past 12 months. 13.4% of the sample population resided in rural areas. Further details on population characteristics can be found in Table 1.
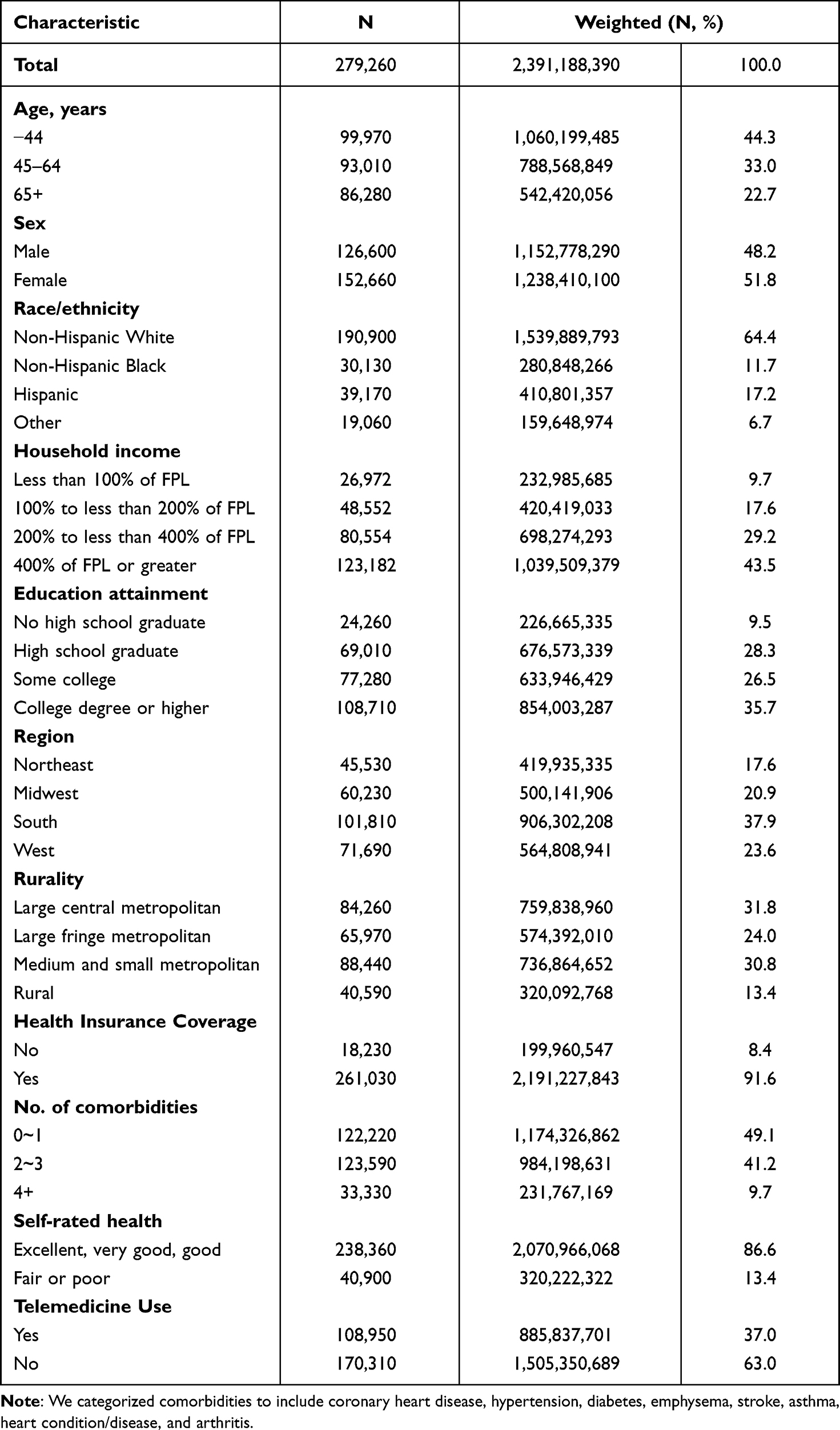 |
Table 1 Characteristics of Study Participants: National Health Interview Survey, 2021 |
Telemedicine Use During COVID-19 Pandemic by Rurality
Table 2 shows the utilization of telemedicine during the COVID-19 pandemic by rurality. The use of telemedicine declined with decreasing levels of urbanization, ranging from 40.2% among adults residing in large central metropolitan areas to 29.7% among those in rural areas (p<0.0001).
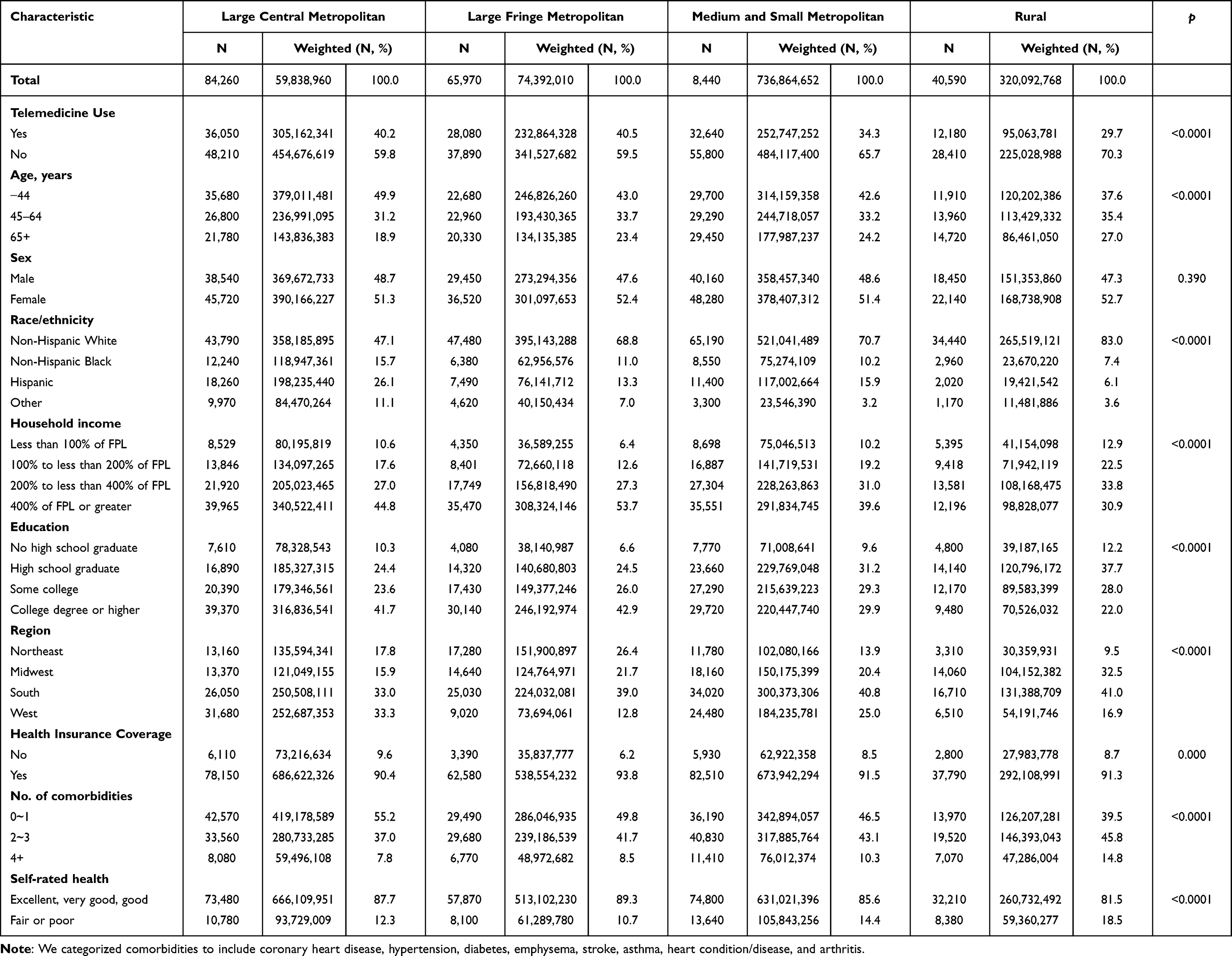 |
Table 2 Telemedicine Use During COVID-19 Pandemic by Rurality: National Health Interview Survey, 2021 |
Association Between Rural-Urban Status and Telemedicine Use
Table 3 displays the association between rural-urban status and telemedicine utilization among US adults. Statistically significant differences were observed in telemedicine use between rural and urban adult populations. Adults in rural areas were 42% less likely to utilize telemedicine than their counterparts in large central metropolitan areas (adjusted odds ratio [AOR] = 0.58, p<0.0001). In addition, adults residing in medium and small metropolitan areas were 27% less likely to utilize telemedicine than those in large central metropolitan areas (odds ratio [OR]= 0.73, p<0.0001).
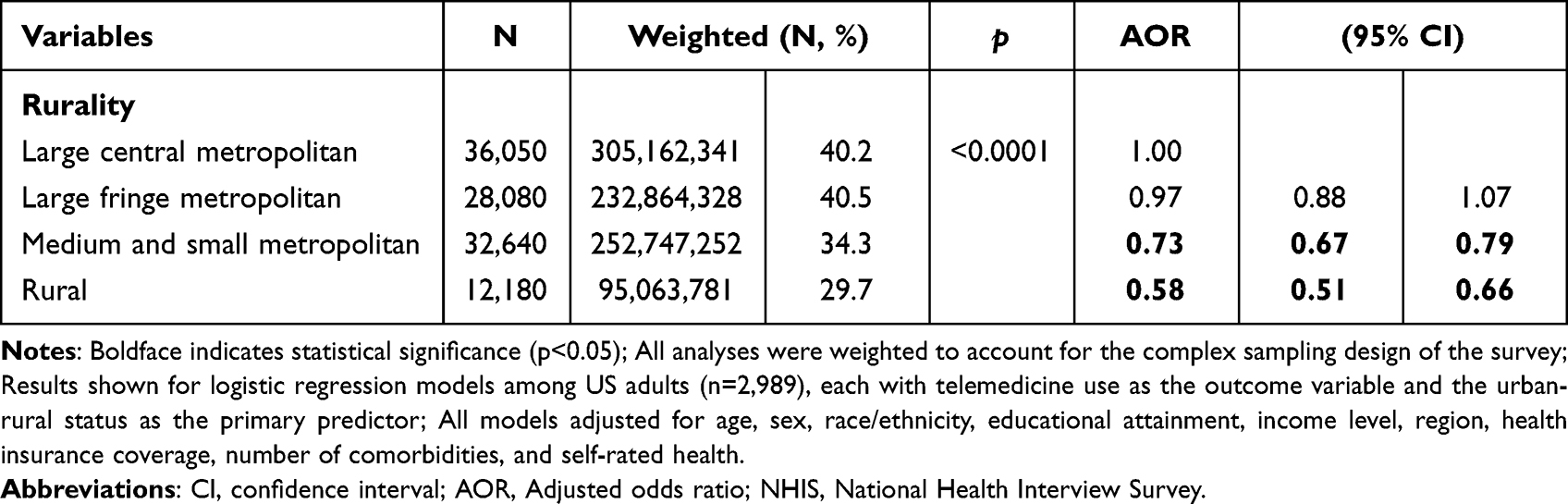 |
Table 3 Association Between Rural-Urban Status and Telemedicine Use Among US Adults: NHIS, 2021 |
Odds of a Telemedicine Use During the COVID-19 Pandemic
Table 4 shows the results of the logistic analysis examining the use of telemedicine by US adults during the COVID-19 pandemic. Adults living in rural areas had a significantly lower likelihood of using telemedicine than adults living in large central metropolitan areas (OR = 0.58 for rural adults). Regarding household income, adults with incomes at or above 400% of the federal poverty level (FPL) were significantly more likely to use telemedicine than adults with less than 100% of the FPL (OR = 1.16 for adults with incomes at or above 400% of the FPL). Gender differences were observed, with females were more likely than males to utilize telemedicine (OR for females = 1.58). Additionally, adults living in the West region were 1.25 times more likely to use telemedicine than those in the Northeast region, and minority race/ethnicity groups (eg, Non-Hispanic Black, Hispanic, and other) are less likely to use the telemedicine rather than Non-Hispanic White (OR for Non-Hispanic Black = 0.77, OR for Hispanic = 0.91, and OR for other = 0.69).
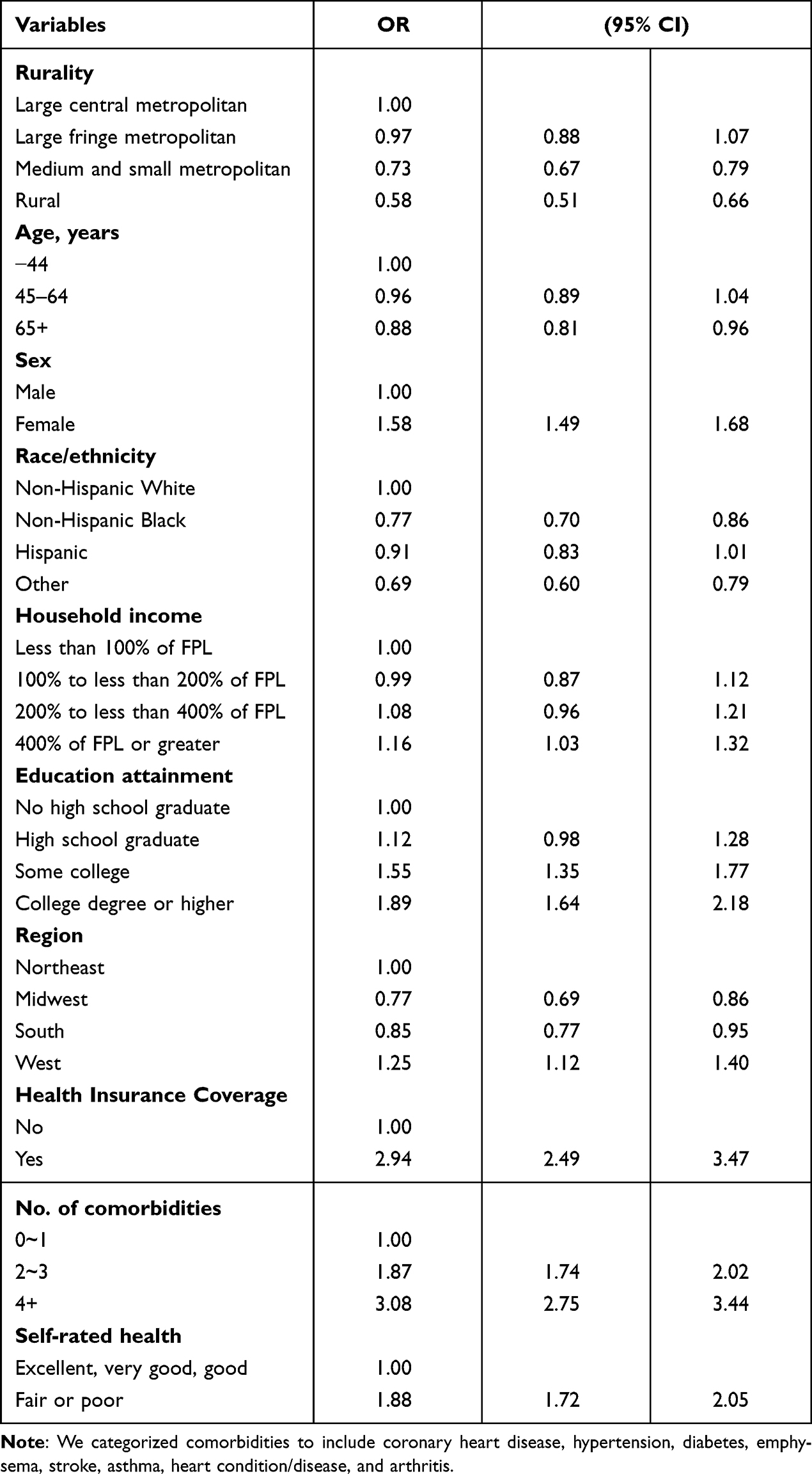 |
Table 4 Odds of a Telemedicine Use During the COVID-19 Pandemic Among US Adults: National Health Interview Survey, 2021 |
Discussion
The study aimed to compare telemedicine utilization patterns among adult populations living in rural and urban areas during the COVID-19 pandemic and explore the association between the regional environment, race/ethnicity, and telemedicine utilization. Our results indicated that adults living in large central metropolitan areas utilized telemedicine approximately twice as often as adults living in rural areas, and telemedicine utilization has decreased significantly as urbanization levels have decreased. In addition, we found that adults living in Midwest and South were significantly less likely to use telemedicine than adults living in Northeast and West, and that low household income and non-white populations were associated with low telemedicine utilization rates.
Our investigation revealed a noteworthy trend wherein the utilization of telemedicine services in rural regions during the COVID-19 pandemic exhibited a proportional decrease as the degree of urbanization diminished (in order of metropolitan central cities, large fringe metropolitan cities, medium and small metropolitan cities, and rural areas). Multiple scholarly inquiries have been dedicated to scrutinizing the disparities in telehealth utilization that manifested during the initial phases of the COVID-19 pandemic,26,27 and these results are consistent with our outcomes. The findings from prior studies consistently highlighted a discernible pattern: older individuals, non-white populations, and those covered by Medicaid or lacking insurance coverage in rural populations demonstrated a reduced likelihood of engaging in telehealth consultations, in contrast to their counterparts who were white, English-speaking, and possessed commercial insurance.28,29 While the COVID-19 pandemic catalyzed a rapid and widespread transition to synchronous, real-time audio and/or video-based telemedicine modalities,30 our research outcomes underscore the persistence of healthcare inequities within rural areas, even in the presence of readily accessible telemedicine services in the home environment during the pandemic. These issues may be attributed to impediments encountered when attempting to access healthcare services, particularly those contingent upon technology-driven modalities of care. Technological barriers encompass deficiencies in possessing suitable technological equipment, inadequate digital proficiency, and unreliable internet connectivity.31,32 Therefore, these challenges can obstruct healthcare access and utilization for rural patients, underscoring the necessity for heightened endeavors to enhance healthcare access equitably within rural populations.
An additional noteworthy observation concerning the utilization of telemedicine during the COVID-19 pandemic pertains to the influence of different regional factors, namely the Northeast, Midwest, South, and West. Specifically, our findings elucidated that adult residing in the Midwest and South regions of the US showed diminished telemedicine utilization in comparison to their counterparts inhabiting the Northeast and West regions. These results are also consistent with the results of a previous study that examined telemedicine utilization rates by race, age, and region in breast cancer patients during the COVID-19 pandemic.33 One plausible explanation for these findings could be the dearth of telemedicine infrastructure and supportive systems within Midwest and South communities. This assumption will be able to be drawn from insights gleaned from a previous investigation that employed the Census Household Pulse survey, revealing that residents residing in the southern and mid-western states exhibit lower rates of telemedicine utilization.34 While telemedicine has frequently been cited as a means to enhance healthcare access for underserved populations,35,36 the absence of requisite infrastructure investments in these regions poses a risk of telemedicine perpetuating disparities among non-metropolitan residents, particularly those dwelling in the central regions of the country.
From a racial and ethnic perspective, our study unearthed noteworthy disparities in telemedicine utilization between non-Hispanic whites and other racial/ethnic groups, encompassing non-Hispanic Blacks, Hispanics, and other minority categories. However, it’s worth noting that these findings stand in contrast to earlier investigations conducted in the initial phases of the COVID-19 pandemic. One such study, which collected data between April and May 2020, revealed an uptick in telemedicine use rates among non-white individuals, including Black/African American and Asian populations, as well as Hispanic/Latino communities during the early stages of the pandemic.37 Additionally, a study employing 2020 NHIS data, collected from March to June 2020, reported no significant discrepancies in telemedicine utilization based on race or ethnicity.38 Importantly, it’s crucial to underscore that our current study is based on an analysis of 2021 NHIS data, and this dataset includes measures of COVID-19 status spanning from January to December 2021. Our findings, derived from this extended temporal window, unequivocally indicate that as COVID-19 becomes more pervasive within our society, there is a discernible gap in telemedicine utilization that corresponds with race/ethnicity. Our study indicated that the progress in telemedicine does not uniformly benefit all segments of the American population. Consequently, it is imperative for future research endeavors to delve into the underlying factors, such as structural racism, that persistently contribute to adverse health outcomes. Furthermore, telemedicine was initially championed as a means to mitigate healthcare disparities along racial and ethnic lines even prior to the pandemic, however, our understanding of ethnic disparities related to telemedicine utilization, particularly regarding whether these disparities have widened or diminished during the course of the COVID-19 pandemic, remains an intricate challenge that necessitates continued exploration and examination.
Our investigation uncovered compelling associations between socioeconomic factors, specifically education level and household income, and the utilization of telemedicine services. Adults with higher education levels were approximately 1.89 times more likely to engage in telemedicine utilization compared to their counterparts with lower educational attainment. Similarly, individuals with elevated household income exhibited a 1.1 times greater likelihood of telemedicine utilization when compared to those with lower incomes. These findings resonate with previous research indicating that individuals with lower educational levels tend to access telehealth services less frequently due to heightened concerns regarding privacy, confidentiality, and the absence of a physical healthcare provider during telehealth visits, in contrast to individuals with higher educational backgrounds.39,40 Additionally, our study underscored disparities in telemedicine access based on income, with low-income adults facing more pronounced barriers compared to their higher-income counterparts. Reports from the US Federal Communications Commission affirmed significant disparities in household income between those with and without access to broadband internet.41 Furthermore, a prior research has elucidated that economic disparities and poverty rates are pivotal factors contributing to healthcare disparities in the US, underscoring how financial disparities can detrimentally impact healthcare access.42 Consequently, our study posits that social determinants, such as education level and household income, serve as indicators of disparities in telemedicine utilization. Therefore, establishing equitable digital access and availability, with consideration of these social determinants, is imperative to fortify the nexus between technology and healthcare. While we acknowledge the inherent challenges in ensuring universal internet access, we contend that as telemedicine assumes a transformative role in the healthcare landscape, it is incumbent upon us to champion digital equity. It is essential to proactively anticipate and address disparities, promoting health equity as telemedicine continues to evolve and shape the clinical landscape.
Limitation
This study still has a few limitations. Firstly, it relied upon cross-sectional data extracted from the 2021 NHIS to investigate the association between telemedicine utilization and rural disparities. Secondly, since the questionnaire for telemedicine use did not investigate the specific types and proportions associated with the modality, the associations found may vary depending on the modality type. Furthermore, it’s important to acknowledge that all data pertaining to telemedicine utilization were obtained through self-reported responses within questionnaires. There exists the potential for responses to be participants to both under- and over-estimation, and it’s crucial to note that these findings have not undergone validation by medical institutions, introducing an element of response bias. Finally, it’s essential to recognize that this study spanned a year characterized by the persistent presence of the COVID-19 pandemic. During this ongoing healthcare crisis, access to conventional face-to-face healthcare services remained limited. Given this evolving healthcare landscape, individuals who initially reported no involvement with telemedicine may have subsequently turned to telehealth services following their initial survey response. Consequently, our estimations regarding the actual extent of telemedicine utilization in 2021 may be conservative, reflecting a healthcare environment in flux during the study period.
Policy Implication
The study provides valuable insights into patient utilization of telehealth and healthcare access. As awareness of telehealth usage grows, strategies to enhance its benefits are needed. The Centers for Medicare and Medicaid implemented temporary payment policies during the pandemic, suggesting policymakers should consider permanent policies. The research shows that patients in urban areas are more likely to use telehealth services than those in rural areas. This suggests that infrastructure policies should focus on affordable internet services in regions with limited internet access. Future research should explore the challenges and benefits of telehealth implementation, and policymakers should use this information to promote adoption.
Conclusion
The observed disparities in telemedicine utilization, specifically in rural areas, emphasize the intricate nature of its utilization in these regions. This accentuates the imperative for tailored healthcare strategies and interventions that are attuned to the unique characteristics of rural areas. Health equity is attained when all demographic groups enjoy uniform access to healthcare services, but disparities emerge when there are discernible variations in access to treatment.43,44 Considering this study’s findings, it becomes evident that the distinctions in poverty rates, median income levels, and healthcare utilization patterns in rural areas may serve as indicators of potential health equity concerns.
Data Privacy and Sharing Statements
The data accessed compiled with relevant data protection and privacy regulations. The dataset used during the current study are available from the corresponding author on reasonable request.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Lewis R, Steckler R. Lewis2020emerging. Emerging technologies and cities: assessing the impacts of new mobility on cities; 2020.
2. Oluyede L, Cochran AL, Wolfe M, Prunkl L, McDonald N. Addressing transportation barriers to health care during the COVID-19 pandemic: perspectives of care coordinators. Transp Res A Policy Pract. 2022;159:157–168. doi:10.1016/j.tra.2022.03.010
3. Koonin LM, Hoots B, Tsang CA, et al. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. MMWR. 2020;69(43):1595. doi:10.15585/mmwr.mm6943a3
4. López CM, Qanungo S, Jenkins CM, Acierno R. Technology as a means to address disparities in mental health research: a guide to “tele-tailoring” your research methods. Prof Psychol. 2018;49(1):57. doi:10.1037/pro0000176
5. Gilmore AK, Ward-Ciesielski EF. Perceived risks and use of psychotherapy via telemedicine for patients at risk for suicide. J Telemed Telecare. 2019;25(1):59–63. doi:10.1177/1357633X17735559
6. Stavroulaki T. Mind the gap: antitrust, health disparities and telemedicine. Am J L Med. 2019;45(2–3):171–187. doi:10.1177/0098858819860607
7. Klink K, Coffman M, Moore M, Jetty A, Petterson S, Bazemore A. Family Physicians and Telehealth: Findings from a National Survey Project Report. Washington, DC, USA: Robert Graham Center; 2015.
8. Tipre M, Scarinci IC, Pandya VN, et al. Attitudes toward telemedicine among urban and rural residents. J Telemed Telecare. 2022; 1357633X221094215. doi:10.1177/1357633X221094215
9. Scott Kruse C, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M. Evaluating barriers to adopting telemedicine worldwide: a systematic review. J Telemed Telecare. 2018;24(1):4–12. doi:10.1177/1357633X16674087
10. Walker D, Fareed N, Hefner J, Huerta T, McAlearney A. Age and Race Disparities in Use of an Inpatient Portal: Exploring the Digital Divide. Academy health; 2019.
11. Jain A, Bk DT, Myers C. Covid-19 created an elective surgery backlog: how can hospitals get back on track. Harvard Business Review. 2020;10:1.
12. Andrist E, Clarke RG, Harding M. Paved with good intentions: hospital visitation restrictions in the age of coronavirus disease 2019. Pediatr Crit Care Med. 2020;21(10):e924. doi:10.1097/PCC.0000000000002506
13. Vance AJ, Duy J, Laventhal N, Iwashyna TJ, Costa DK. Visitor guidelines in US children’s hospitals during COVID-19. Hosp Pediatr. 2021;11(6):e83–e89. doi:10.1542/hpeds.2020-005772
14. McBride DL. The impact of visiting restrictions during the COVID-19 pandemic on pediatric patients. J Pediatric Nurs. 2021;61:436–438. doi:10.1016/j.pedn.2021.09.004
15. Silvera GA, PhD JA W, Stanowski A, Studer Q. The influence of COVID-19 visitation restrictions on patient experience and safety outcomes: a critical role for subjective advocates. Patient Exp J. 2021;8(1):30–39. doi:10.35680/2372-0247.1596
16. Jnr BA. Use of telemedicine and virtual care for remote treatment in response to COVID-19 pandemic. J Med Syst. 2020;44(7):132. doi:10.1007/s10916-020-01596-5
17. Bokolo AJ. Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic. Ir J Med Sci. 2021;190(1):1–10. doi:10.1007/s11845-020-02299-z
18. Organization WH. Coronavirus disease (COVID-19): weekly epidemiological update, 31 august 2020; 2020.
19. Walker PG, Whittaker C, Watson OJ, et al. The impact of COVID-19 and strategies for mitigation and suppression in low-and middle-income countries. Science. 2020;369(6502):413–422. doi:10.1126/science.abc0035
20. Duan GY, De Luzuriaga AM R, Schroedl LM, Rosenblatt AE. Disparities in telemedicine use during the COVID‐19 pandemic among pediatric dermatology patients. Pediatr Dermatol. 2022;39(4):520–527. doi:10.1111/pde.14982
21. Singh JA, Richards JS, Chang E, Joseph AM, Ng B. Telemedicine use during the covid-19 pandemic by resilient rheumatology providers: a national veterans affairs follow-up survey. J Rheumatol. 2022;49(4):424–431. doi:10.3899/jrheum.210967
22. Nittari G, Khuman R, Baldoni S, et al. Telemedicine practice: review of the current ethical and legal challenges. Telemed E-Health. 2020;26(12):1427–1437. doi:10.1089/tmj.2019.0158
23. Battineni G, Pallotta G, Nittari G, Amenta F. Telemedicine framework to mitigate the impact of the COVID-19 pandemic. J Taibah Univ Sci. 2021;16(2):300. doi:10.1016/j.jtumed.2020.12.010
24. Parsons VL, Moriarity C, Jonas K, Moore TF, Davis KE, Tompkins L. Design and estimation for the national health interview survey, 2006-2015. Vital Health Stat. 2014;2(165):1–53.
25. Lucas JW, Villarroel MA. Telemedicine Use Among Adults: United States, 2021. US Department of Health and Human Services, Centers for Disease Control and …; 2022.
26. Chang M-H, Moonesinghe R, Truman BI. Telehealth availability and usage among medicare beneficiaries during the COVID-19 pandemic, October and November 2020. J Public Health Manage Pract. 2022;28(1):77–85. doi:10.1097/PHH.0000000000001448
27. Datta P, Eiland L, Samson K, Donovan A, Anzalone AJ, McAdam-Marx C. Telemedicine and health access inequalities during the COVID-19 pandemic. J Glob Health. 2022;12:1
28. Hsiao V, Chandereng T, Lankton RL, et al. Disparities in telemedicine access: a cross-sectional study of a newly established infrastructure during the COVID-19 pandemic. Appl Clin Inform. 2021;12(03):445–458. doi:10.1055/s-0041-1730026
29. Eberly LA, Kallan MJ, Julien HM, et al. Patient characteristics associated with telemedicine access for primary and specialty ambulatory care during the COVID-19 pandemic. JAMA network open. 2020;3(12):e2031640. doi:10.1001/jamanetworkopen.2020.31640
30. Patel SY, Mehrotra A, Huskamp HA, Uscher-Pines L, Ganguli I, Barnett ML. Trends in outpatient care delivery and telemedicine during the COVID-19 pandemic in the US. JAMA Intern Med. 2021;181(3):388–391. doi:10.1001/jamainternmed.2020.5928
31. Quinton JK, Ong MK, Vangala S, et al. The association of broadband internet access and telemedicine utilization in rural western Tennessee: an observational study. BMC Health Serv Res. 2021;21(1):765. doi:10.1186/s12913-021-06746-0
32. Roberts ET, Mehrotra A. Assessment of disparities in digital access among medicare beneficiaries and implications for telemedicine. JAMA Intern Med. 2020;180(10):1386–1389. doi:10.1001/jamainternmed.2020.2666
33. Calip GS, Cohen A, Rohrer R, et al. Telemedicine use among patients with metastatic breast cancer during the COVID‐19 pandemic: differences by race, age, and region. Pharmacoepidemiol Drug Saf. 2023;32(1):66–72. doi:10.1002/pds.5541
34. Karimi M, Lee EC, Couture SJ, et al. National survey trends in telehealth use in 2021: disparities in utilization and audio vs. video services. US Dep Health & Hum Serv. 2022;2022:1.
35. Marcin JP, Shaikh U, Steinhorn RH. Addressing health disparities in rural communities using telehealth. Pediatr Res. 2016;79(1):169–176. doi:10.1038/pr.2015.192
36. Batsis JA, Pletcher SN, Stahl JE. Telemedicine and primary care obesity management in rural areas–innovative approach for older adults? BMC Geriatr. 2017;17(1):1–9. doi:10.1186/s12877-016-0396-x
37. Pagán VM, McClung KS, Peden CJ. An observational study of disparities in telemedicine utilization in primary care patients before and during the COVID-19 pandemic. Telemed E-Health. 2022;28(8):1117–1125. doi:10.1089/tmj.2021.0412
38. Narcisse M-R, Andersen JA, Felix HC, Hayes CJ, Eswaran H, McElfish PA. Factors associated with telehealth use among adults in the United States: findings from the 2020 national health interview survey. J Telemed Telecare. 2022;1357633X221113192. doi:10.1177/1357633X221113192
39. Jennett P, Jackson A, Healy T, et al. A study of a rural community’s readiness for telehealth. J Telemed Telecare. 2003;9(5):259–263. doi:10.1258/135763303769211265
40. Zhang D, Shi L, Han X, et al. Disparities in telehealth utilization during the COVID-19 pandemic: findings from a nationally representative survey in the United States. J Telemed Telecare. 2021; 1357633X211051677. doi:10.1177/1357633X211051677
41. Federal Communications Commission2020. Broadband deployment report 2020.
42. Chang J, Medina M, Shin DY, Kim SJ. Racial disparity and regional variance in healthcare utilization among patients with lung cancer in US hospitals during 2016–2019. Arch Public Health. 2023;81(1):1–9. doi:10.1186/s13690-023-01166-4
43. Johnson C, Rastetter M, Olayiwola JN. Pathways to equity: a pilot study implementing a health equity leadership curriculum in residency education as an antidote to systemic racism. J Natl Med Assoc. 2022;114(2):141–146. doi:10.1016/j.jnma.2021.12.015
44. Farrer L, Marinetti C, Yk C, Costongs C. Advocacy for health equity: a synthesis review. Milbank Q. 2015;93(2):392–437. doi:10.1111/1468-0009.12112
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.