Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Rumination, posttraumatic stress disorder, and mood symptoms in borderline personality disorder
Authors Dell'Osso L, Cremone IM, Carpita B, Dell'Oste V ![]() , Muti D
, Muti D ![]() , Massimetti G
, Massimetti G ![]() , Barlati S, Vita A, Fagiolini A
, Barlati S, Vita A, Fagiolini A ![]() , Carmassi C
, Carmassi C ![]() , Gesi C
, Gesi C
Received 18 December 2018
Accepted for publication 7 March 2019
Published 13 May 2019 Volume 2019:15 Pages 1231—1238
DOI https://doi.org/10.2147/NDT.S198616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Liliana Dell’Osso,1 Ivan M Cremone,1 Barbara Carpita,1 Valerio Dell’Oste,1 Dario Muti,1 Gabriele Massimetti,1 Stefano Barlati,2 Antonio Vita,2 Andrea Fagiolini,3,4 Claudia Carmassi,1 Camilla Gesi1
1Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy; 2Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy; 3Department of Mental Health, University of Siena, Siena, Italy; 4Department of Molecular Medicine, University of Siena, Siena, Italy
Background: The interrelationship between mood disorders and borderline personality disorder (BPD) has been long debated in the literature. Increasing attention has also been paid to the relationship between posttraumatic stress disorder (PTSD) and BPD, as well as to the role of rumination in the development and severity of BPD. This study aims to evaluate the association of rumination, PTSD, and mood spectrum among patients with BPD with or without comorbid mood disorders.
Methods: Fifty patients with BPD and 69 healthy controls were assessed with the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders 5, MoodSpectrum Self-Report (MOODS-SR), and Ruminative Response Scale (RRS).
Results: The BPD group was split into subjects with BPD+ mood disorder (MD) or BPD only) . PTSD-criteria fulfillment, MOODS, and RRS scores were significantly higher in both BPD subgroups than in controls, while BPD+MD patients scored significantly higher than the BPD-only group. RRS scores and PTSD-criteria fulfillment were significantly related to the presence of both BPD and BPD+MD, with no effect of MOODS-SR scores.
Conclusion: Our findings confirm the presence of a relationship between BPD and the PTSD spectrum, highlighting also a possible role of rumination in BPD psychopathology. Rumination and PTSD symptoms seem to prevail in the effect of mood spectrum in predicting BPD.
Keywords: ruminative thinking, borderline personality disorder, post-traumatic stress disorder, mood disorders
Introduction
Borderline Personality Disorder (BPD) is a serious mental illness characterized by unstable interpersonal relationships with sudden attachment, anxious dependence, and fear of being abandoned, together with affective instability, pervasive impulsiveness, recurrent self-injurious and suicidal behaviors, and threats.1 Emotional dysregulation is often indicated as the core feature of BPD, arising from a biological vulnerability interacting with an invalidating childhood environment and stress or trauma.2–4 The relevance of trauma to BPD psychopathogenesis is suggested by a large body of studies stressing that a significant percentage of BPD subjects report a history of childhood trauma,5–11 generally being at high risk of traumatic exposure during their entire life span.12–15 Besides providing further insight into the borderline construct, the association with trauma has also propelled interest in exploring the relationship between posttraumatic stress symptoms and BPD, with some authors arguing whether the borderline constellation of symptoms could pertain to a peculiar form of posttraumatic stress disorder (PTSD) called complex PTSD.16,17 Interestingly, as growing attention was devoted to this topic, some authors pointed out how partial and subthreshold PTSD as well should deserve attention, since these may relate to levels of distress, impairment, and comorbidity in a dose-dependent manner, showing an association in particular with mood symptoms.18–22
Recent parallel research has also shone light on the potential role of rumination in BPD.23–25 Rumination is a cognitive symptom related to negative emotional conditions, and is generally manifested as going over a problem or one’s distress and possible causes and consequences, as opposed to its solutions.26 Besides enhancing negative thinking, rumination has been shown to maintain, exacerbate, and predict depressive symptoms.27–29 Moreover, in response to negative life events, rumination seems to increase the risk of experiencing depressive episodes and is positively related to the length and severity of a depressive episode.27,30,31 Despite rumination usually being associated with depressive states, research on this topic has recently come across a variety of clinical conditions, including BPD, with most of the extant literature focusing so far on the relationship among rumination, BPD, and mood symptoms. Abela et al,32 for example, found that BPD patients with comorbid major depressive disorder (MDD) have higher levels of depressive rumination than those with MDD only. Conversely, Watkins33 reported a significant association between BPD features and rumination in patients with unipolar depressive disorders. Intriguingly, a growing literature is showing the importance of rumination in the development of psychopathological symptoms after exposure to trauma, raising the matter of the complex relationship among mood spectrum, rumination, and posttraumatic symptoms in patients suffering from BPD.
Based on this background, the aim of the present study was to evaluate the presence of PTSD symptoms, ruminative thinking and mood spectrum symptoms in a sample of BPD patients with or without comorbid mood disorder, as well as in a control (Ctl) group, with a specific focus on determining which of these dimensions is more associated with a diagnosis of BPD and on eventual differences between BPD patients with and without mood disorder.
Methods
Study sample
The sample included 50 patients with a clinical diagnosis of BPD, consecutively enrolled at three Italian university departments of psychiatry (Pisa, Brescia, and Siena) between May 2015 and April 2016. Exclusion criteria were age <18 years, language or intellectual impairment affecting the possibility to fulfill the assessments, and comorbidity with schizophrenia. A Ctl group of 69 healthy subjects with no current or lifetime mental disorders was also recruited at the same sites.
All subjects were assessed by means of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (DSM) 5,34 in order to assess comorbid mental disorders or to confirm healthy Ctl status. Moreover, all participants were asked to fill in two self-report instruments: the Mood Spectrum Self-Report (MOODS-SR)35–37 and the Ruminative Response Scale (RRS).38 All assessments were conducted by psychiatrists trained in the use of the study instruments at the University of Pisa. The study was conducted in accordance with the Declaration of Helsinki. The ethics committee of Azienda Ospedaliero–Universitaria di Pisa approved all recruitment and assessment procedures. Eligible subjects provided written informed consent after receiving a complete description of the study and having the opportunity to ask questions.
Assessment instruments
Mood Spectrum Self-Report
The MOODS-SR is an instrument derived from the Structured Clinical Interview for MOODS, developed by the Psychiatric Clinic of Pisa University in collaboration with the University of Pittsburgh. It is aimed at providing a thorough dimensional assessment of the psychopathological continuum that includes and gives importance to all the features of mood disorders, including prodromal, typical, atypical, residual, and trait-like symptoms.36,39 The questionnaire includes 161 dichotomous items (yes/no response), defined as present or absent for at least 3–5 days in the subject’s life span. Items are grouped in three manic/hypomanic and three depressive domains (exploring for each pole the areas of mood, energy, and cognition). A further domain explores disturbances in rhythmicity (eg, changes in mood, energy, and physical well-being according to weather, season, and phase of menstrual cycle) and vegetative functions (including sleep, appetite, and sexual behavior).
Ruminative Response Scale
The RRS is a self-report instrument evaluating rumination.38 It comprises 22 items rated on a 4-point scale measuring three different aspects of rumination. Eleven items are included in the Brooding domain, addressing a tendency to dwell on one’s negative mood and on the consequences of that mood (eg, thinking “What am I doing to deserve this?”). Five further items are included in the Reflection domain, addressing more active efforts to understand the reasons for one’s mood (eg, analyzing recent events to try to understand why you are depressed). The remaining six items are meant to explore the Depression domain, focusing on depressive rumination.
Statistical analyses
Means ± SD of scale scores were compared between groups using ANOVA. Post hoc pairwise comparisons were performed using Tukey’s test. Logistic regression analyses were used to evaluate potential predictors of a diagnosis of BPD. A first logistic regression was carried out using BPD diagnosis as the dependent variable and number of Diagnostic and Statistical Manual of Mental Disorders 5 PTSD criteria fulfilled and RRS-domain scores as independent variables. A second logistic regression analysis was conducted adding MOODS-SR depressive and manic component scores to the list of independent variables. Lastly, a third logistic regression was carried out using the number of PTSD criteria fulfilled, RRS-domain scores, and MOODS-SR depressive and manic component scores as independent variables and diagnosis of BPD with comorbid mood disorder (BPD+MD) as the dependent variable. Results were considered statistically significant at P=P=0.05. All data analysis was conducted using SPSS version 22.
Results
Sociodemographic and clinical characteristics of the study sample, including rates of comorbid disorders evaluated by means of the Structured Clinical Interview for theDiagnostic and Statistical Manual of Mental Disorders 5 have been reorted elsewhere.40 Overall, 27 (54%) subjects in the BPD group had a comorbid mood disorder (BPD+MD), while the remaining 23 (46%) did not (BPD only). BPD+MD group included subjects with a diagnosis of bipolar disorder I (n=10) and II (n=6), MDD (n=9), and persistent depressive disorder (n=4). Two subjects received a diagnosis of both MDD and persistent depressive disorder. Comparisons among groups on RRS and MOODS-SR scores and number of PTSD criteria endorsed are shown in Table 1. All MOODS-SR and RRS scores were significantly greater in BPD+MD patients than in the Ctl group. BPD+MD patients also scored significantly higher than BPD-only patients on MOODS-SR and RRS total scales, on all MOODS-SR scores but depressive mood, and on all RRS scores but Brooding. The BPD-only group scored significantly higher than the Ctl groupon both MOODS-SR and RRS total, on Depressive energy and Depressive cognition domain scores of MOODS-SR, and Depression-subscale score of the RRS. Both BPD+MD and BPD-only subjects reported a significantly greater number of PTSD criteria satisfied than Ctl subjects, with the BPD+MD group showing a significantly greater number of criteria compared to BPD-only group.
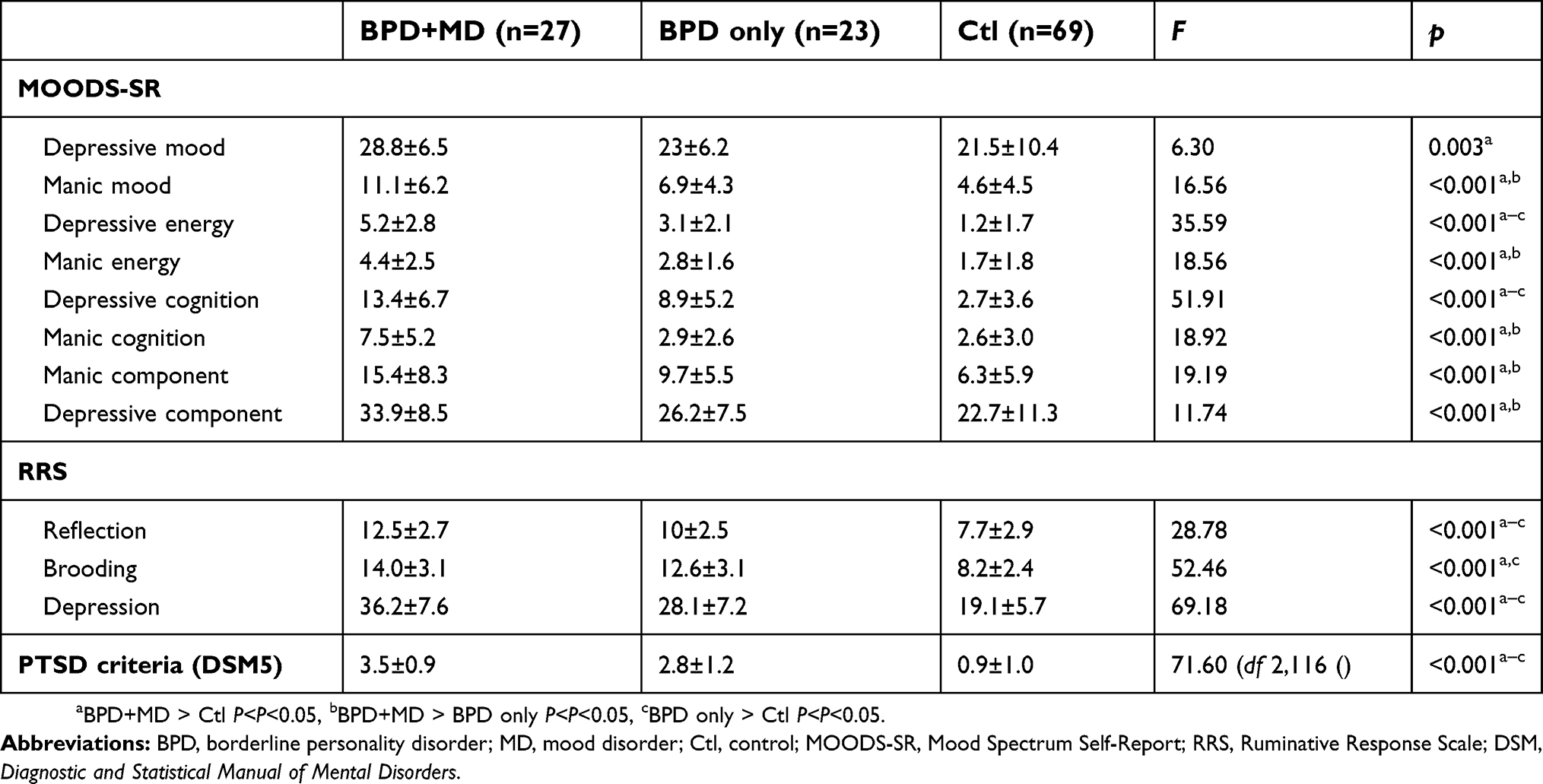 | Table 1 Characteristics of the study sample |
The results of the logistic regression conducted using BPD diagnosis as dependent variable and RRS-domain scores and number of PTSD criteria fulfilled as independent variables showed that RRS Depression and Brooding domain scores and the number of PTSD criteria endorsed were positively and significantly related to the diagnosis of BPD (Depression, β=0.38; OR 1.47; P=0.019; Brooding, β=0.19; OR =1.21; P=0.017; PTSD criteria: β=1.06; OR 2.87, P<0.001; Cox R2=0.566, Nagelkerke R2 =0.762; correct classification total percentage 87.1%). Reflection-domain scores of the RRS resulted in being a negative predictor of BPD status (β=−0.36, OR 0,70; P=0.047). After the addition of MOODS-SR manic and depressive scores to the independent-variable list, the RRS Brooding domain score and number of PTSD criteria fulfilled were still significantly related to BPD diagnosis, while RRS Depression and Reflection domain scores and MOODS-SR domain scores did not predict BPD status (Table 2).
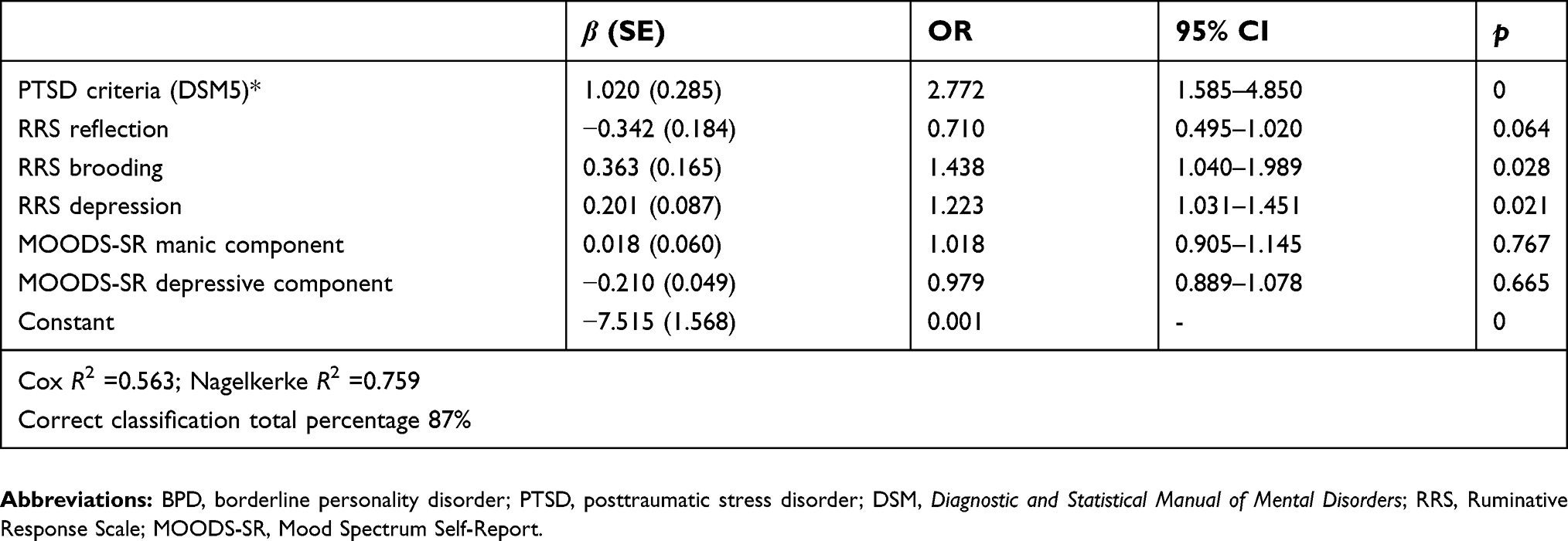 | Table 2 Logistic regression for predictors of BPD diagnosis (dependent variable) |
Table 3 displays the results of logistic regression carried out using diagnosis of BPD+MD as dependent variable and RRS-domain scores, MOODS-SR manic and depressive component scores, and the number of PTSD criteria fulfilled as independent variables. The number of PTSD criteria and the RRS Depression score positively and significantly predicted BPD+MD diagnosis.
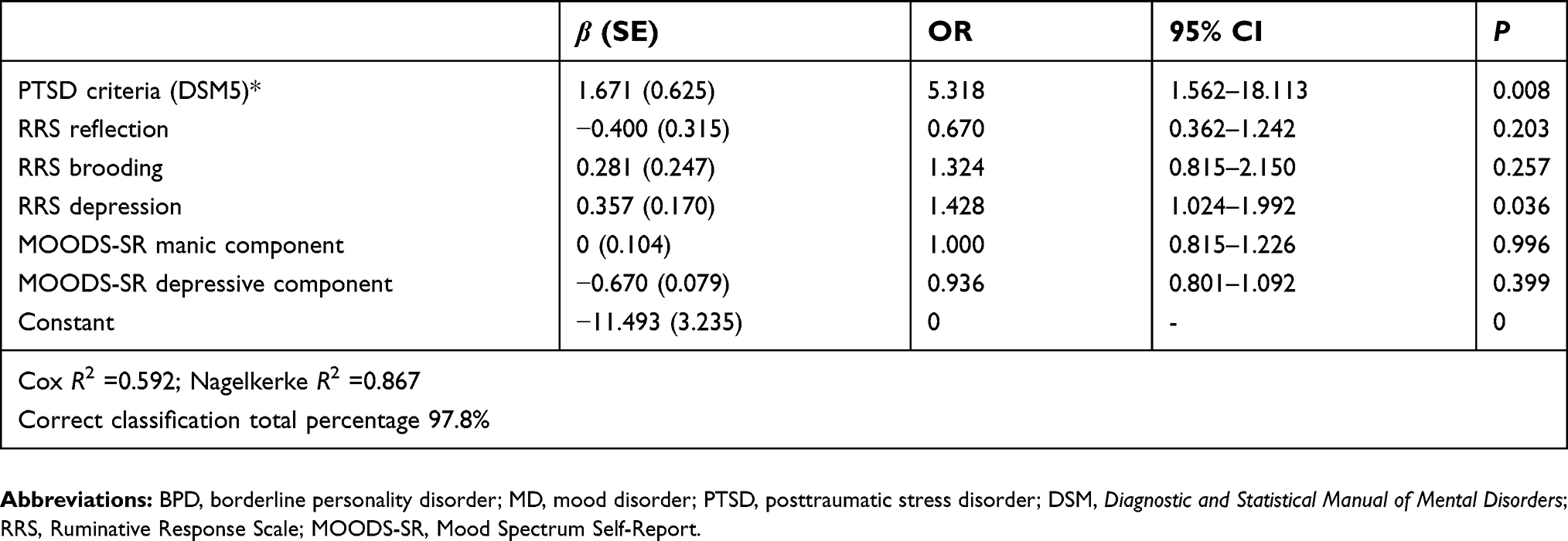 | Table 3 Logistic regression for predictors of BPD+MD (dependent variable) |
Discussion
The aim of the present study was to compare levels of rumination, mood-spectrum symptoms and PTSD symptoms among subjects with BPD with or without concurrent MD and healthy subjects, and to evaluate the extent to which these dimensions are associated with the diagnosis of BPD. Results showed that BPD patients had overall higher levels of rumination than subjects, with BPD+MD showing higher levels compared to BPD only. Similarly, BPD patients showed higher levels of mood spectrum symptoms than Ctl subjects on the MOODS-SR, with BPD+MD also exceeding BPD only on the total MOODS-SR scale, as well as on several domain scores. As expected, BPD patients, both with and without comorbid MD, showed a greater number of PTSD symptoms than healthy Ctl subjects. Interestingly, multivariate analyses showed that only PTSD symptoms and rumination significantly predicted BPD diagnosis, with a probability of being diagnosed with BPD increasing by 187% for every criterion of PTSD fulfilled and 47% for every additional point scored on the Brooding domain of the RRS, while no associations were found with MOODS-SR domain scores.
On one hand, our findings suggest the putative role of rumination in BPD psychopathology, while on the other they confirm and strengthen the relationship between trauma-related symptoms and BPD over and above the effect of mood-spectrum symptoms. While not included among the defining features of BPD, traumatic experiences, especially prolonged and occurring early in life, such as child abuse and neglect, are thought to play a significant role in the development of the borderline personality.5,6,41 Intriguingly, in the last decade it has even been debated whether BPD should be added to the spectrum of trauma-related disorders, as the emerging clinical entity named complex PTSD closely resembles a borderline clinical picture, besides sharing a few neurobiological correlates with BPD.16 Complex PTSD is indeed characterized by most of the core symptoms of PTSD, along with some BPD-like symptoms, such as affective dysregulation, disrupted beliefs about oneself as being diminished and worthless, difficulties in developing relationships, and feelings of guilt, shame, or failure,16,42,43 somehow prompting the hypothesis that BPD might actually arise from a posttraumatic process developed upon a temperamental vulnerability, at least in those cases who report a history of traumatic exposure and suffering from posttraumatic symptoms.44 In keeping with previous data,45 our results seem to corroborate the potential role of posttraumatic symptoms in BPD, not only when full comorbidity with PTSD is diagnosed but also when only some PTSD-symptom criteria are fulfilled.
Our findings on rumination suggest that BPD diagnosis is significantly linked to brooding, which represents the more maladaptive aspect of rumination, oriented to self-criticism and reflecting a passive comparison of one’s current situation with some unachieved standards.46 Interestingly, a large body og literature indicates that emotional dysfunction in BPD patients may depend on a broad array of maladaptive cognitive processes, including rumination. The emotional cascade model of BPD, for example, proposes that negative affect in BPD patients is a trigger of rumination, which in turn intensifies the affect, inducing a vicious cycle and ultimately leading to dysregulated behavior that represents an attempt to distract attention from the negative affect.47 Consistently with our findings, Selby et al48 found in a large study sample a significant association between the severity of BPD symptoms and a composite rumination variable that included depressive brooding, anger rumination, and catastrophizing. Moreover, the rumination variable mediated the relationship between BPD symptoms and dysregulated behaviors, such as self-harm and binge eating. Our results are somewhat in line also with recent data from Peters et al,49 who reported an association of BPD with specific styles and content of rumination. According to that study, rumination associated with BPD features seemed to be negative in valence and prolonged in time, with a focus on interpersonal themes, and including depressive brooding, anger, and stress-related ruminative thinking.49 Moreover, it is noteworthy that as reported elsewhere,40 a high rate (68%) of subjects in our sample had experienced physical or sexual abuse during their lifetime. According to previous literature, sexual abuse seems to show a particularly high correlation with rumination, while rumination seems to mediate the relationship between negative affect and the development of PTSD after interpersonal trauma, as well as social anxiety.7,33,50,51 Intriguingly, another study stressed the link between rumination and alexithymia, with difficulties in identifying emotions, in mediating the relationship between negative affect and BPD symptoms, further highlighting the dimension of social impairment in these patients.52 The present findings also add to previous findings, including one study from the same study sample showing higher levels of autism-spectrum symptoms in BPD patients compared to Ctl subjects, thus suggesting that rumination may be related to a subthreshold autism-spectrum sympthomatology.40,53–56
While the core emotional dysregulation of BPD patients has sometimes been considered part of the MD spectrum,57–59 mood symptoms did not predict BPD diagnosis in our sample, at least when rumination and PTSD symptoms were also taken into account. Given the high percentage of (MDs) in our sample (54%), we performed a logistic regression to explore predictive variables of the BPD+MD. Surprisingly, also in this case, mood-spectrum symptoms did not seem to be significantly predictive of PTSD criteria or RRS domains. This finding further confirms that rumination and PTSD symptoms might play a role on BPD psychopathology over and above the contribution of mood-spectrum symptoms and independently of comorbidity with MDs.
Our results must be considered in light of obvious limitations. First of all, the sample was small, and further studies with larger samples are needed to confirm our findings. Second, the cross-sectional design of the study and the lifetime assessment prevented us from elucidating the type of andf temporal sequence of the occurrence of trauma, posttraumatic symptoms, borderline symptoms, or rumination, such that any inference of causal relationships was not allowed. In particular, the lifetime assessment of posttraumatic symptoms did not allow evaluation of the differential impact of traumatic experiences occurring early in life or during adulthood. Third, the lack of a quantitative measure of BPD symptoms prevented us from evaluating the relationship between BPD-symptom severity and rumination or posttraumatic symptoms. Further, this was an exploratory study conducted with a small sample, and we did not differentiate in our analyses between subjects with or without current mood episodes, neither between subjects nor unipolar versus bipolar mood disorders. This may have greatly affected our results, considering also that the literature is currently stressing possible differences between bipolar disorders and MDD in respect to their relationship with PTSD, eventually depending also on current mood state. Further studies in larger samples and with longitudinal design are warranted to clarify relationships among MD, PTSD, rumination, and BPD.60
In the context of these limitations, our study highlights the potential role of trauma-related symptoms and rumination in BPD, suggesting the importance of carefully investigating both dimensions. A better understanding of the link between trauma and BPD, as well as recognizing the key role of ruminative thinking in these patients, may shed new light on the current understanding of both trauma- and stress-related disorders and personality disorders, adding new insights to the relationship between environmental stress and biological vulnerability in promoting psychopathology. From a clinical point of view, our results may also contribute to reconsideration and eventual improvement fo the targets for interventions in this patient population, which is often poorly responsive to available treatments.
Disclosure
AF reports grants, personal fees, and nonfinancial support from Allergan, Angelini, Apsen, Boheringer Ingelheim, Doc Generici, FB Health, Italfarmaco, Janssen, Lundbeck, Mylan, Otsuka, Pfizer, Recordati, Sanofi Aventis, Sunovion, and Vifor outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gunderson JG, Lyons-Ruth K. BPD‘s interpersonal hypersensitivity phenotype: a gene-environment-developmental model. J Pers Disord. 2008;22(1):22–41. doi:10.1521/pedi.2008.22.1.22
2. Linehan MM. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York, NY: Guilford Press; 1993.
3. Beauchaine TP, Klein DN, Crowell SE, Derbidge C, Gatzke-Kopp L. Multifinality in the development of personality disorders: a biology x sex x environment interaction model of antisocial and borderline traits. Dev Psychopathol. 2009;21(3):735–770. doi:10.1017/S0954579409000418
4. Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. 2009;10(6):434–445. doi:10.1038/nrn2639
5. Zanarini MC, Gunderson JG, Marino MF, Schwartz EO, Frankenburg FR. Childhood experiences of borderline patients. Compr Psychiatry. 1989;30(1):18–25. doi:10.1016/0010-440X(89)90114-4
6. Zanarini MC, Williams AA, Lewis RE, et al. Reported pathological childhood experiences associated with the development of borderline personality disorder. Am J Psychiatry. 1997;154(8):1101–1106. doi:10.1176/ajp.154.8.1101
7. Johnson JG, Cohen P, Brown J, Smailes EM, Bernstein DP. Childhood maltreatment increases risk for personality disorders during early adulthood. Arch Gen Psychiatry. 1999;56(7):600–606. doi:10.1001/archpsyc.56.7.600
8. Johnson JG, Cohen P, Smailes EM, Skodol AE, Brown J, Oldham JM. Childhood verbal abuse and risk for personality disorders during adolescence and early adulthood. Compr Psychiatry. 2001;42(1):16–23. doi:10.1053/comp.2001.19755
9. Spataro J, Mullen PE, Burgess PM, Wells DL, Moss SA. Impact of child sexual abuse on mental health: prospective study in males and females. Br J Psychiatry. 2004;184:416–421. doi:10.1192/bjp.184.5.416
10. Widom CS, Czaja SJ, Paris J. A prospective investigation of borderline personality disorder in abused and neglected children followed up into adulthood. J Pers Disord. 2009;23(5):433–446. doi:10.1521/pedi.2009.23.5.433
11. de Aquino Ferreira LF, Queiroz Pereira FH, Neri Benevides AML, Aguiar Melo MC. Borderline personality disorder and sexual abuse: a systematic review. Psychiatry Res. 2018;262:70–77. doi:10.1016/j.psychres.2018.01.043
12. Zanarini MC, Frankenburg FR, Reich DB, Marino MF, Haynes MC, Gunderson JG. Violence in the lives of adult borderline patients. J Nerv Ment Dis. 1999;187(2):65–71. doi:10.1097/00005053-199902000-00001
13. Zanarini MC, Frankenburg FR, Reich DB, Hennen J, Silk KR. Adult experiences of abuse reported by borderline patients and Axis II comparison subjects over six years of prospective follow-up. J Nerv Ment Dis. 2005;193(6):412–416. doi:10.1097/01.nmd.0000165295.65844.52
14. McGowan A, King H, Frankenburg FF, Fitzmaurice G, Zanarini MC. The course of adult experiences of abuse in patients with borderline personality disorder and Axis II comparison subjects: a 10-year follow-up study. J Pers Disord. 2012;26(2):192–202. doi:10.1521/pedi.2012.26.2.192
15. Zanarini MC, Temes CM, Ivey AM, et al. The 10-year course of adult aggression toward others in patients with borderline personality disorder and axis II comparison subjects. Psychiatry Res. 2017;252:134–138. doi:10.1016/j.psychres.2017.02.054
16. Cloitre M, Garvert DW, Weiss B, Carlson EB, Bryant RA. Distinguishing PTSD, complex PTSD, and borderline personality disorder: a latent class analysis. Eur J Psychotraumatol. 2014;5. 10.3402/ejpt.v5.25097. doi:10.3402/ejpt.v5.25097
17. Ford JD, Courtois CA, Complex PTSD. affect dysregulation, and borderline personality disorder. Borderline Personal Disord Emot Dysregul. 2014;1:9. doi:10.1186/2051-6673-1-9
18. Stein MB, Walker JR, Hazen AL, Forde DR. Full and partial posttraumatic stress disorder: findings from a community survey. Am J Psychiatry. 1997;154(8):1114–1119. doi:10.1176/ajp.154.8.1114
19. Zlotnick C, Franklin CL, Zimmerman M. Does “subthreshold” posttraumatic stress disorder have any clinical relevance? Compr Psychiatry. 2002;43(6):413–419. doi:10.1053/comp.2002.35900
20. Breslau N, Lucia VC, Davis GC. Partial PTSD versus full PTSD: an empirical examination of associated impairment. Psychol Med. 2004;34(7):1205–1214. doi:10.1017/S0033291704002594
21. Carmassi C, Akiskal HS, Bessonov D, et al. Gender differences in DSM-5 versus DSM-IV-TR PTSD prevalence and criteria comparison among 512 survivors to the L‘Aquila earthquake. J Affect Disord. 2014;160:55–61. doi:10.1016/j.jad.2014.02.028
22. Carmassi C, Corsi M, Bertelloni CA, et al. Mothers and fathers of children with epilepsy: gender differences in post-traumatic stress symptoms and correlations with mood spectrum symptoms. Neuropsychiatr Dis Treat. 2018;14:1371–1379. doi:10.2147/NDT.S158249
23. Baer RA, Peters JR, Eisenlohr-Moul TA, Geiger PJ, Sauer SE. Emotion-related cognitive processes in borderline personality disorder: a review of the empirical literature. Clin Psychol Rev. 2012;32(5):359–369. doi:10.1016/j.cpr.2012.03.002
24. Sauer-Zavala SE, Geiger PJ, Baer RA. The effect of anger rumination in the relationship between borderline personality disorder symptoms and precursors. J Pers Disord. 2013;27(4):465–472. doi:10.1521/pedi_2013_27_098
25. Meaney R, Hasking P, Reupert A. Prevalence of borderline personality disorder in university samples: systematic review, meta-analysis and meta-regression. PLoS One. 2016;11(5):e0155439. doi:10.1371/journal.pone.0155439
26. Nolan SA, Roberts JE, Gotlib IH. Neuroticism and ruminative response style as predictors of change in depressive symptomatology. Cognit Ther Res. 1998;22(5):445–455. doi:10.1023/A:1018769531641
27. Just N, Alloy LB. The response styles theory of depression: tests and an extension of the theory. J Abnorm Psychol. 1997;106(2):221–229. doi:10.1037/0021-843X.106.2.221
28. Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking Rumination. Perspect Psychol Sci. 2008;3(5):400–424. doi:10.1111/j.1745-6924.2008.00088.x
29. Brinker JK, Dozois DJ. Ruminative thought style and depressed mood. J Clin Psychol. 2009;65(1):1–19. doi:10.1002/jclp.20542
30. Nolen-Hoeksema S, Morrow J, Fredrickson BL. Response styles and the duration of episodes of depressed mood. J Abnorm Psychol. 1993;102(1):20–28. doi:10.1037/0021-843X.102.1.20
31. Nolen-Hoeksema S, Parker LE, Larson J. Ruminative coping with depressed mood following loss. J Pers Soc Psychol. 1994;67(1):92–104. doi:10.1037/0022-3514.67.1.92
32. Abela JR, Payne AV, Moussaly N. Cognitive vulnerability to depression in individuals with borderline personality disorder. J Pers Disord. 2003;17(4):319–329. doi:10.1521/pedi.17.4.319.23968
33. Watkins ER. Depressive rumination and co-morbidity: evidence for brooding as a transdiagnostic process. J Ration Emot Cogn Behav Ther. 2009;27(3):160–175. doi:10.1007/s10942-009-0098-9
34. First MB, Williams JB, Karg RS, Spitzer RL. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders, Clinician Version. Arlington, VA: American Psychiatric Association; 2015.
35. Fagiolini A, Dell’Osso L, Pini S, et al. Validity and reliability of a new instrument for assessing mood symptomatology: the Structured Clinical Interview for Mood Spectrum (SCI MOODS). Int J Meth Psych Res. 1999;8(2):71–81. doi:10.1002/mpr.58
36. Dell‘Osso L, Armani A, Rucci P, et al. Measuring mood spectrum: comparison of interview (SCI-MOODS) and self-report (MOODS-SR) instruments. Compr. Psychiatry. 2002;43(1):69–73. doi:10.1053/comp.2002.29852
37. Cassano GB, Benvenuti A, Miniati M, et al. The factor structure of lifetime depressive spectrum in patients with unipolar depression. J Affect Disord. 2009;115(1–2):87–99. doi:10.1016/j.jad.2008.09.006
38. Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: the 1989 Loma Prieta Earthquake. J Pers Soc Psychol. 1991;61(1):115–121. doi:10.1037/0022-3514.61.1.115
39. Frank E, Cassano GB, Shear MK, et al. The Spectrum model: a more coherent approach to the complexity of psychiatric symptomatology. CNS Spectr. 1998;3:23–34. doi:10.1017/S1092852900005836
40. Dell‘Osso L, Cremone IM, Carpita B, et al. Correlates of autistic traits among patients with borderline personality disorder. Compr Psychiatry. 2018;83:7–11. doi:10.1016/j.comppsych.2018.01.002
41. Leichsenring F, Leibing E, Kruse J, New AS, Leweke F. Borderline personality disorder. Lancet. 2011;377(9759):74–84. doi:10.1016/S0140-6736(10)61422-5
42. Cloitre M, Garvert DW, Brewin CR, Bryant RA, Maercker A. Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis. Eur J Psychotraumatol. 2013;4. 10.3402/ejpt.v4i0.20706. doi:10.3402/ejpt.v4i0.20706
43. Brewin CR, Cloitre M, Hyland P, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clin Psychol Rev. 2017;58:1–15. doi:10.1016/j.cpr.2017.09.001
44. Martín-Blanco A, Soler J, Villalta L, et al. Exploring the interaction between childhood maltreatment and temperamental traits on the severity of borderline personality disorder. Compr Psychiatry. 2014;55(2):311–318. doi:10.1016/j.comppsych.2013.08.026
45. Frías Á, Baltasar I, Birmaher B. Comorbidity between bipolar disorder and borderline personality disorder: prevalence, explanatory theories, and clinical impact. J Affect Disord. 2016;202:210–219. doi:10.1016/j.jad.2016.05.048
46. Treynor W, Gonzalez R, Holen-Hoeksema S. Rumination reconsidered: a psychometric analysis. Cognit Ther Res. 2003;27(3):247–259. doi:10.1023/A:1023910315561
47. Selby EA, Anestis MD, Joiner TE
48. Selby EA, Anestis MD, Bender TW, Joiner TE
49. Peters JR, Eisenlohr-Moul TA, Upton BT, Talavera NA, Folsom JJ, Baer RA. Characteristics of repetitive thought associated with borderline personality features: a multimodal investigation of ruminative content and style. J Psychopathol Behav Assess. 2017;39(3):456–466. doi:10.1007/s10862-017-9594-x
50. Marazziti D, Abelli M, Baroni S, Carpita B, Piccinni A, Dell‘Osso L. Recent findings on the pathophysiology of social anxiety disorder. Clin Neuropsychiatr. 2014;11(2):91–100.
51. Brown WJ, Hetzel-Riggin MD, Mitchell MA, Bruce SE. Rumination mediates the relationship between negative affect and posttraumatic stress disorder symptoms in female interpersonal trauma survivors. J Interpers Violence. 2018;17:886260518818434. doi:10.1177/0886260518818434
52. Meaney R, Hasking P, Reupert A. Borderline personality disorder symptoms in college students: the complex interplay between alexithymia, emotional dysregulation and rumination. PLoS One. 2016;11(6):e0157294. doi:10.1177/0886260518818434
53. Dell‘Osso L, Dalle Luche R, Gesi C, Moroni I, Carmassi C, Maj M. From asperger‘s autistischen psychopathen to DSM-5 autism spectrum disorder and beyond: a subthreshold autism spectrum model. Clin Pract Epidemiol Ment Health. 2016;12:120–131. doi:10.2174/1745017901612010120
54. Dell‘Osso L, Muti D, Carpita B, et al. The Adult Autism Subthreshold Spectrum (AdAS) model: A neurodevelopmental approach to mental disorders. J Psychopathol. 2018;24(3):118–124.
55. Dell‘Osso L, Carpita B, Cremone IM, et al. The mediating effect of trauma and stressor related symptoms and ruminations on the relationship between autistic traits and mood spectrum. Psychiatry Res. 2018;S0165–1781(18):30826. doi:10.1016/j.psychres.2018.10.040
56. Dell‘Osso L, Carpita B, Gesi C, et al. Subthreshold autism spectrum disorder in patients with eating disorders. Compr Psychiatry. 2018;81:66–72. doi:10.1016/j.comppsych.2017.11.007
57. Marwaha S. Borderline personality disorder and mood. Br J Psychiatry. 2014;205(2):161. doi:10.1192/bjp.205.2.161
58. Parker G. Is borderline personality disorder a mood disorder? Br J Psychiatry. 2014;204:252–253. doi:10.1192/bjp.bp.113.136580
59. Tyrer P. Borderline personality disorder and mood. Br J Psychiatry. 2014;205(2):161–162. doi:10.1192/bjp.205.2.161a
60. McCraw S, Parker G. The prevalence and outcomes of exposure to potentially traumatic stressful life events compared across patients with bipolar disorder and unipolar depression. Psychiatry Res. 2017;255:399–404. doi:10.1016/j.psychres.2017.06.070
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.