Back to Journals » International Journal of General Medicine » Volume 18
Routine Nasobiliary Cholangiography After ERCP for Choledocholithiasis May Be Unnecessary: A Single-Center Retrospective Cohort Study
Authors Yan Z, Ning Y, An Z, Zhao Q ![]() , Fang J
, Fang J
Received 26 June 2025
Accepted for publication 19 November 2025
Published 15 December 2025 Volume 2025:18 Pages 7521—7530
DOI https://doi.org/10.2147/IJGM.S549724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Gopal Krishna Dhali
Zi Yan,1– 3,* Yumei Ning,1– 3,* Zhi An,1– 3 Qiu Zhao,1– 3 Jun Fang2– 4
1Department of Gastroenterology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 2Hubei Provincial Clinical Research Center for Intestinal and Colorectal Diseases, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 3Hubei Key Laboratory of Intestinal and Colorectal Diseases, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 4Department of General Medicine, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiu Zhao, Department of Gastroenterology, Zhongnan Hospital of Wuhan University; Hubei Clinical Research Center and Key Laboratory of Intestinal and Colorectal Diseases, Wuhan, Hubei, People’s Republic of China, Email [email protected] Jun Fang, Department of General Medicine, Zhongnan Hospital of Wuhan University; Hubei Clinical Research Center and Key Laboratory of Intestinal and Colorectal Diseases, Wuhan, Hubei, People’s Republic of China, Email [email protected]
Objective: To evaluate the necessity of routine nasobiliary cholangiography (NBC) after Endoscopic retrograde cholangiopancreatography (ERCP) for common bile duct stones (CBDS) by comparing outcomes between patients with and without post-ERCP NBC.
Methods: Consecutive patients who underwent ERCP with CBDS extraction between January 2021 and June 2024. We compared the outcomes of patients who underwent NBC versus those who did not receive NBC after ERCP for CBDS extraction. The primary outcome was the incidence rate of residual stones (detected within≤ 6 months). Secondary outcomes included recurrence of CBDS (more than 6 months), hospitalization duration, antibiotic use duration, and overall cost. Multivariate logistic regression was used to identify independent predictors, reported with odds ratios (ORs) and 95% confidence intervals (CIs).
Results: The overall residual stone rate was 5.2% (16/308). The residual stone rate was 7.1% (10/141) in the NBC group, compared to 3.6% (6/167) in the no-NBC group, with no statistically significant difference between the groups (p=0.168). Post-ERCP NBC significantly increased costs (p< 0.01). Large stone diameter (OR=5.48, 95% CI: 1.16– 25.87) was an independent predictor for residual stones.
Conclusion: Routine NBC after ERCP for CBDS may not be necessary as it did not reduce residual stone rates but increased costs. NBC should be considered selectively for patients with large stone diameter (> 11.06 mm) or multiple stones.
Keywords: common bile duct stones, cost-benefit analysis, postoperative imaging, residual stones, stone recurrence
Introduction
Common bile duct stones (CBDS) represent a prevalent clinical challenge in gastroenterology practice worldwide.1–3 Endoscopic retrograde cholangiopancreatography (ERCP) and laparoscopic common bile duct exploration (LCBDE) have proven to be safe and effective ways of managing CBDS.4,5 Nowadays, ERCP has established itself as the gold standard for management due to its minimally invasive profile and high technical success.6–8 Despite technical advancements, complete stone clearance is not always achieved, with reported rates of residual stones ranging from 4% to 25%.9 These residual fragments can lead to significant complications, including recurrent cholangitis, pancreatitis,10 and the need for intervention, underscoring the critical importance of reliable post-procedural verification of biliary clearance.
Even if the extraction appears to be complete, residual stones may remain. Accordingly, in addition to balloon-occluded cholangiography, some endoscopists insert a nasobiliary drainage tube and later evaluate residual stones using cholangiography or other techniques.11 Balloon occlusion cholangiography is widely used owing to its simplicity and real-time capability but may miss small or radiolucent stones. Intraductal ultrasound (IDUS) offers high sensitivity without the need for contrast but requires specialized equipment and expertise, limiting its routine use.12 Cholangioscopy allows for direct visual inspection and targeted therapy but is costly, time-consuming, and not universally available.13,14 In this context, nasobiliary cholangiography (NBC) serves as a practical alternative, providing dynamic, high-resolution imaging of the biliary tree through an indwelling catheter.
Despite the advantages of NBC, there remains ongoing debate about its routine use after ERCP. While NBC is more sensitive than standard occlusion cholangiography and more accessible than IDUS or cholangioscopy, it entails additional procedure time, patient discomfort and costs. Previous prospective studies have questioned the necessity of routine nasobiliary drainage following ERCP, demonstrating that it may prolong hospitalization, increase patient discomfort, and extend radiation exposure without clear clinical benefit. Furthermore, no major guidelines currently provide definitive indications for nasobiliary tube placement after stone extraction, highlighting the ongoing uncertainty in clinical practice.15 Existing studies suggest that omitting endoscopic nasobiliary drainage (ENBD) after elective common bile duct stone clearance appears to be safe in selected patients.16 This supports a shift toward more selective use of ENBD rather than routine placement. In contrast to the relatively well-studied role of ENBD as a drainage tool, evidence regarding the specific use of nasobiliary tubes for postoperative cholangiography remains limited. No robust studies have systematically evaluated the clinical value or optimal application protocol of NBC as a dedicated imaging modality for detecting residual stones after ERCP. Consequently, there is a need to clarify the role of NBC in routine post-ERCP management and assess the potential risks and benefits.
Current societal guidelines reflect the ongoing uncertainty regarding the optimal verification strategy. The American Society for Gastrointestinal Endoscopy (ASGE) guidelines suggest that routine postoperative imaging may be considered but do not strongly endorse it for all cases, it can be performed during laparoscopic cholecystectomy.17 Similarly, the European Society of Gastrointestinal Endoscopy (ESGE) guidelines conditionally recommend confirmatory imaging primarily in high-risk scenarios, such as suspected incomplete clearance or complex anatomy.1 Current research on the necessity of routine nasobiliary drainage exists, but there is a lack of clinical studies and practical guidelines regarding post-ERCP NBC.15
This study addresses pressing clinical questions faced by endoscopists: Is routine NBC necessary for all patients after ERCP? Which patients truly benefit from this additional procedure? We employed a pragmatic study design comparing outcomes between routine versus selective NBC use, focusing on endpoints that matter most to clinicians: residual stone rates, hospitalization duration, and overall costs.
Methods
Study Design and Participants
This retrospective single-center cohort study consecutively enrolled patients undergoing ERCP for common bile duct stones (CBDS) at the Endoscopy Center of Zhongnan Hospital of Wuhan University from January 2021 and to June 2024. Prior to endoscopic retrograde cholangiopancreatography (ERCP), CBDS were confirmed using various diagnostic methods, including transabdominal ultrasonography (US), computed tomography (CT), and magnetic resonance cholangiopancreatography (MRCP). Patients who were scheduled to undergo ERCP with stones extraction were enrolled consecutively into our study.
Data were collected from the electronic medical record system, graphic endoscopy system and X-ray imaging system, including patient demographics (gender, age, BMI), preoperative laboratory examination, comorbidity conditions, the diameter of CBDS, the CBDS and gallstones, and other relevant clinical information. All eligible patients, or their legal representatives, provided informed consent before undergoing the procedure. The study protocol was approved by the Ethics Committee of Zhongnan Hospital of Wuhan University (2025080K).
Procedure
All endoscopic procedures were performed by two experienced endoscopists, each having performed over 1000 ERCPs.18–20 Patients received standardized intravenous sedation with morphine and diazepam and were positioned in the left lateral decubitus position. Routine antibiotic prophylaxis with a broad-spectrum antibiotic was administered prior to ERCP to reduce infectious complications.
Selective cannulation of the common bile duct was achieved using either a guidewire-assisted technique or contrast injection under fluoroscopic guidance. Endoscopic sphincterotomy (EST) was performed in cases involving large (>8 mm) stones or difficult stones.21,22 Stone extraction was accomplished using a basket and/or a retrieval balloon, with or without mechanical lithotripsy (Trapezoid RX Wire guided Retrieval Basket; Boston Scientific Corporation), as determined by the operator. Difficult stones, defined as those not amenable to standard extraction techniques, were managed with additional intervention techniques according to predefined criteria including large-balloon dilation, mechanical lithotripsy, cholangioscopy-assisted electrohydraulic/laser lithotripsy, or extracorporeal shock wave lithotripsy (ESWL).1,23
After successful stone extraction, complete clearance was verified through standardized occlusion cholangiography performed by injecting contrast (using a 5-mL syringe) via a balloon catheter with systematic fluoroscopic evaluation of the biliary tree. Nasobiliary catheter (Gauge: 8.5 Fr; Anrei Medical Device Corporation) placement was selectively performed based on predefined clinical indications including complex biliary anatomy and concomitant acute cholangitis. The catheter was inserted over a guidewire under fluoroscopic guidance and removed 3–5 days postoperatively if the patient’s recovery was uneventful and follow-up NBC confirmed the absence of residual stones. The NBC procedure was typically completed within 2–3 minutes.
Patient assignment to the NBC versus no-NBC groups was based on intraoperative clinical judgment, considering factors such as symptom severity, adequacy of clearance on occlusion cholangiography, and bleeding risk. Based on these criteria, 141 patients underwent post-ERCP NBC, while 167 patients without these indications were discharged without NBC. The average duration of nasobiliary tube presence in the NBC group was 3 days.
Follow-Up
Patients were enrolled in a structured follow-up protocol with scheduled outpatient evaluations at 0, 1, 3, and 6 months post-ERCP. Each visit included laboratory tests: complete blood count, liver function tests, amylase, lipase as well as abdominal ultrasonography. Additional imaging with CT or MRCP was initiated in cases of abnormal biochemical results, sonographic evidence of biliary dilation, or new-onset biliary symptoms. Endpoint definitions were predefined: residual stones were defined as those detected within six months of the initial procedure, whereas recurrent stones were those newly identified beyond six months.
Definitions and Outcomes
The primary outcome was the residual stone rate. Residual common bile duct stones were defined as the rediscovery of CBDS less than 6 months after the initial procedure or the identification of CBDS during the post-ERCP nasobiliary duct cholangiography.24 Secondary outcomes include post-ERCP choledocholithiasis recurrence, length of hospital stay, hospitalization cost, and antibiotic treatment duration. Recurrent choledocholithiasis was defined as the occurrence of choledocholithiasis more than 6 months after removal of stones.25 Length of stay was defined as the number of days from the date of admission to the date of discharge. We excluded patients with severe complications. Severe complications refer to patients experiencing procedure-related complications including severe pancreatitis (according to revised Atlanta criteria),26 perforation, severe bleeding requiring transfusion, or cholangitis with hemodynamic instability.
Statistical Analysis
Continuous variables are presented as the mean±standard deviation or median and interquartile range, as appropriate. Categorical variables are expressed as numbers or percentages (%). Continuous variables with a normal distribution were analyzed by independent samples t-test or Mann–Whitney U-test. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. Multivariate logistic regression was used to predict risk factors for residual CBDS, and the results werepresented as odds ratios (ORs) with 95% confidence intervals (CIs). The analyses were conducted with SPSS software version 27.0. A two-sided P value of less than 0.05 was considered statistically significant.
Results
Participants Characteristics
A total of 435 participants underwent ERCP for common bile duct stones during the study period. After applying the exclusion criteria detailed in Figure 1, 308 patients met the inclusion criteria and were included in the final analysis. Among them, 141 patients underwent post-ERCP nasobiliary duct cholangiography, while 167 patients were discharged from the hospital directly. The baseline characteristics of the two groups are summarized in Table 1. There were no significant differences between the groups in terms of gender, age distribution, comorbidities or pre-ERCP laboratory tests. However, a higher proportion of patients in the NBC group had undergone prior cholecystectomy compared to the no-NBC group (31.2% vs 21.0%, p<0.05).
 |
Table 1 Baseline Characteristics |
 |
Figure 1 Flow chart of the study. |
ERCP Procedure Characteristics
For patients with single or pigment stones, most of them were discharged from the hospital after observation for a period of time. For patients with multiple stones, post-ERCP NBC is more likely to be preferred (54.6% vs 69.5%; 45.4% vs 30.5%, p<0.001). The stone diameter in the NBC group was significantly larger than that in the no-NBC group (9.20 mm [6–12 mm] vs 6.68 mm [3–10 mm], p<0.001) (Table 2). There was no statistically significant difference in the CBD diameter and mechanical lithotripsy between the two groups (CBD diameter: 11.26 mm [9–13 mm] vs 10.66 mm [7–13 mm], P>0.05; mechanical lithotripsy: 8.5% vs 4.2%, P>0.05). In the NBC group, most patients underwent endoscopic papillary balloon dilation (EPBD) combined with endoscopic sphincterotomy (EST), while in the no-NBC group, patients often received pure EST alone (Pure EST: 31.2% vs 47.9%, P<0.05; EST+EPBD: 45.4% vs 26.9%, P<0.001). In the NBC group, the fluoroscopy time was longer than that of the no-NBC group (30.01 min [18–37 min] vs 26.17 min [16–32 min], P<0.05).
 |
Table 2 ERCP Procedure Characteristics |
Primary Outcome
The incidence rate of residual CBDS after ERCP was 7.1% (10 of 141 patients) in the NBC group and 3.6% (6 of 167 patients) in the no-NBC group (P=0.168) (Table 3).
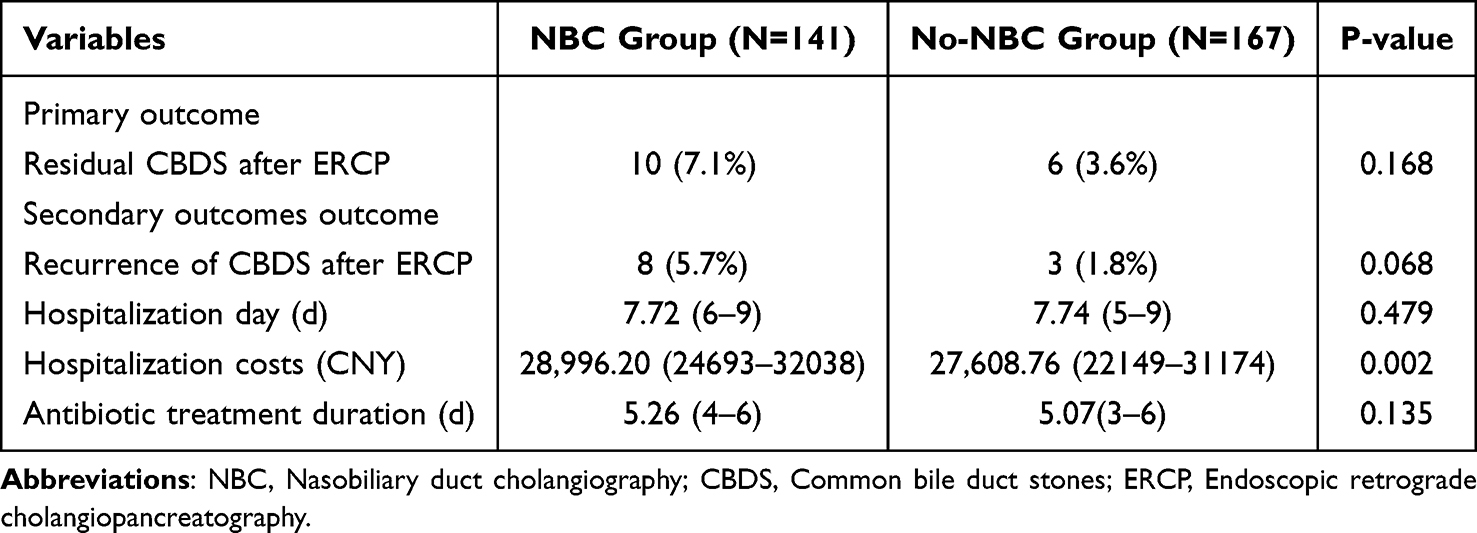 |
Table 3 Comparison of the Primary and Secondary Outcomes Between the Post-ERCP NBC and Without Post-ERCP NBC Groups |
Secondary Outcomes
There was no significant difference in the recurrence of CBDS after ERCP, hospitalization days and antibiotic treatment duration between the two groups (Table 3). But we found that post-ERCP NBC increased hospitalization costs (28,996.20 CNY[24,693–32,038 CNY] vs 27,608.76CNY [22,149–31,174 CNY], p=0.002)(Table 3).
Risk Factor Analyses
Based on the presence or absence of postoperative residual stones, we found that the diameter of CBDS significantly affected the postoperative residual stone rate (7.65 mm [4–10 mm] vs 11.06 mm [6–13 mm], P=0.015) (Table 4). In the multivariate analysis, we also found stone diameter was an important risk factor (odds ratio 5.48; 95% CI, 1.16 to 25.87; P=0.0320) (Table 5).
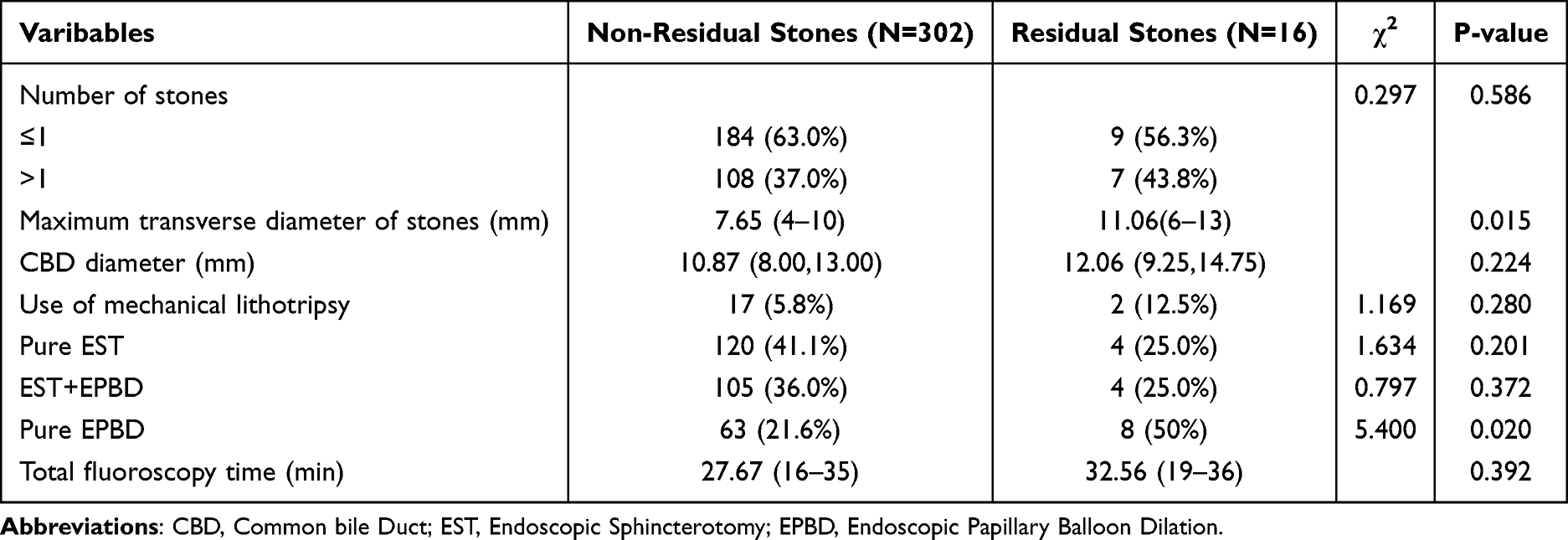 |
Table 4 Risk Factors for Residual Stones |
 |
Table 5 Multivariate Logistic Regression Analysis for Residual Common Bile Duct Stone |
Discussion
ERCP is a minimally invasive treatment for CBDS, offering several advantages, including minimal trauma, short operation time, low complication rates and favorable prognosis.27 Despite these benefits, several studies have reported a high rate of residual stones after ERCP, which remains a significant concern for clinicians.25,28–31 Recurrent cholangitis is a common complication in clinical practice, with residual stones being detected in 4–24% of patients after successful stone retrieval.3 Therefore, post-ERCP NBC to assess the presence of residual stones is crucial. Some endoscopists advocated for the use of cholangiography through an endoscopic nasobiliary drainage (ENBD) tube to confirm the absence of retained stones and prevent complications.32–34 However, the routine use of NBC remains inconsistent, and its optimal application after ERCP is unclear. Herein, our study investigated the value and necessity of the NBC after ERCP, providing new insights for clinical practice.
In this retrospective study, the incidence rate of residual CBDS was 5.2% (n=16). Comparing the NBC group with the no-NBC group, the pooled data revealed that post-ERCP NBC was associated with a higher rate of residual stones (7.1% vs 3.6%, P=0.168). Although comparisons about residual stones between the two groups showed without significant difference, repeat cholangiography could early identify residual stones and allow timely intervention, which potentially reduced the risk of severe complications.35,36 However, the added costs of hospitalization due to routine NBC and the prolonged retention time of the ENBD tube raise concerns about its universal application.16,34 Our results showed that post-ERCP NBC increased hospitalization fees (28,996.20 CNY[24,693–32,038 CNY] vs 27,608.76 CNY [22,149–31,174 CNY], p=0.002).
In this study, we found that clinicians were more likely to administer NBC after ERCP in patients with multiple (>1) stones or large (>11.06mm) stones. Cheon et al14 reported that the diameter of CBDS was an independent risk factor for incomplete clearance and a higher rate of residual stones, which was consistent with our current findings. Mechanical lithotripsy was often used to remove large stones.37,38 However, this method may lead to the generation of numerous stone fragments within the CBD, which were challenging to detect nidus using balloon occlusion cholangiography.11–13 Moreover, the presence of large stones often complicates the procedure by extending the procedure time. This can lead to significant gastrointestinal tract distention, multiple contrast injections, and the intrusion of intestinal air into the biliary system.36,39 These factors could all interfere with the accuracy of angiographic results, making it more difficult to assess the complete clearance of the bile duct. In light of these challenges, careful consideration must be given to the choice of imaging and intervention strategies during ERCP. In general, if stones were considered easy to remove during the initial ERCP, operators typically did not perform repeat cholangiography after the procedure. When patients’ condition was stable, they were discharged from the hospital as soon as possible. According to the data analysis, for patients who did not undergo post-ERCP NBC after stone removal, it was crucial for operators to carefully evaluate the bile duct during the procedure to ensure complete stone removal. For patients with difficult or numerous stones, we tend to perform post-ERCP NBC to check for residual stones. Therefore, selective post-ERCP cholangiography is more beneficial, as it not only reduces the hospitalization burden but also helps avoid further complications. Additionally, we noticed that the fluoroscopy time was longer and more patients had undergone cholecystectomy in the NBC group, probably owing to the more complex conditions of these patients and operators intended to put an ENBD tube for drainage.36 Accordingly, operators should be mindful of the potential complications associated with prolonged procedures, including the increased risk of bile duct injury, infection, or perforation.40 Moreover, a previous study indicated that symptomatic choledocholithiasis recurrence may be associated with the retention time of ENBD after ERCP, particularly for the duration of ENBD for more than 4.01 days.34 These risks emphasize the importance of a well-balanced approach to treatment, where the benefits of mechanical lithotripsy and post-ERCP imaging are weighed against the risks of extended procedure time and additional costs.
Previous studies have identified multiple factors contributing to residual stones, such as periampullary diverticula (PAD), CBD dilation, and intraoperative mechanical lithotripsy.11,41,42 However, our study found that stone diameter was the only significant factor associated with residual stones. This could be related to the sample size and procedure records, as only 17 (5.5%) patients with mechanical lithotripsy were included in our study. Additionally, we observed that patients in the NBC group were more likely to undergo combined endoscopic papillary balloon dilation (EPBD) and endoscopic sphincterotomy (EST) during the procedure, whereas the no-NBC group predominantly received EST alone. This finding aligns with previous studies, which suggest that the use of EPBD alone may decrease the likelihood of residual stones.43–45 Our results support this, showing that patients without residual stones were more likely to undergo EPBD (non-residual stones group: 63 of 302 (21.6%) vs residual stones group: 8 of 16 (50%), p<0.05). Therefore, in the residual stone group, a combination approach may be a better choice rather than EPBD alone.
Antonia Rizzuto et al reported that 13 patients (11%) had residual common biliary duct stones diagnosed by intraoperative cholangiography.46 Lee et al used direct peroral cholangioscopy (DPOC) and balloon cholangiography to evaluate residual bile duct stones and found that 28.3% (13/46) of the patients had residual bile duct stones, which were missed by balloon cholangiography.25,29 Shin Tsuchiya et al stated that in 14 of 59 patients (23.7%), IDUS detected small residual stones not seen on cholangiography.31 In this study, post-ERCP NBC was applied non-selectively, and therefore, the positive rate is expected to be lower than when used selectively for high-risk patients.6 Small stone fragments or bile sludge may not be identifiable through cholangiography. NBC is a post-ERCP remedial measure, and the operator may subjectively be more inclined to perform the imaging more thoroughly and carefully during ERCP, as they do not anticipate finding residual stones after the procedure to avoid repeat stone removal. However, in our study, the fluoroscopy time in the NBC group was longer than that of no-NBC group (30.01 min [18–37 min] vs 26.17 min [16–32 min], P<0.05), which avoided operator subject bias.
There are several limitations in the present study. First, this was a single-center, retrospective study instead of a randomized controlled trial. Second, there was a risk of ethnical bias or operator bias. Third, we failed to investigate other risk factors about residual CBDS except for stone diameter. This was probably due to the limited sample size. Accordingly, future multicenter and large sample studies are needed to conduct further confirm our results. Furthermore, using propensity-weighted analyses with longer follow-up (≥12 months) would strengthen the validity of the conclusions.
In conclusion, it is not necessary to perform NBC routinely for the patients with CBDS after ERCP. The decision to perform NBC should be individualized based on patient risk factors, clinical presentation, and resource availability. Post-ERCP NBC is recommended to conduct for patients with multiple (>1) or large (>11.06 mm) stones.
Abbreviations
ERCP, Endoscopic Retrograde Cholangiopancreatography; LCBDE, Laparoscopic Common Bile Duct Exploration; CBDS, Common Bile Duct Stones; ENBD, Endoscopic Nasobiliary Drainage; NBC, Nasobiliary Duct Cholangiography; PAD, Periampullary Diverticulum; EPBD, Endoscopic Papillary Balloon Dilation; EST, Endoscopic Sphincterotomy; PTCD, Percutaneous Transhepatic Cholangiographic Drainage; ESWL, Extracorporeal Shock Wave Lithotripsy, MRCP, Magnetic Resonance Cholangiopancreatography; US, Ultrasonography; CT, Computed Tomograpy.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The experimental protocol was established according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Zhongnan Hospital of Wuhan University (Clinical Trial Number: 2025080K). Informed consent was obtained by the attending physicians during the initial hospitalization prior to ERCP procedures. The consent process included explanation of the procedure, potential risks and benefits, and agreement to use anonymized data for research purposes, as approved by the Institutional Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Hubei Province(2023AFB792).
Disclosure
The authors declare no competing interests in this work.
References
1. Manes G, Paspatis G, Aabakken L, et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019;51:472–491. doi:10.1055/a-0862-0346
2. Williams E, Beckingham I, El Sayed G, et al. Updated guideline on the management of common bile duct stones (CBDS). Gut. 2017;66:765–782. doi:10.1136/gutjnl-2016-312317
3. Akbar UA, Vorla M, Chaudhary AJ, et al. Preventive saline irrigation of the bile duct to reduce the rate of residual common bile duct stones without intraductal ultrasonography: a systematic review and meta-analysis. Cureus. 2023;15:e46720. doi:10.7759/cureus.46720
4. Ricci C, Pagano N, Taffurelli G, et al. Comparison of efficacy and safety of 4 combinations of laparoscopic and intraoperative techniques for management of gallstone disease with biliary duct calculi: a systematic review and network meta-analysis. JAMA Surg. 2018;153:e181167. doi:10.1001/jamasurg.2018.1167
5. Varban O, Assimos D, Passman C, Westcott C. Video. Laparoscopic common bile duct exploration and holmium laser lithotripsy: a novel approach to the management of common bile duct stones. Surg Endosc. 2010;24:1759–1764. doi:10.1007/s00464-009-0837-0
6. Baiu I, Visser B. Endoscopic retrograde cholangiopancreatography. JAMA. 2018;320:2050. doi:10.1001/jama.2018.14481
7. Deng F, Zhou M, Liu PP, et al. Causes associated with recurrent choledocholithiasis following therapeutic endoscopic retrograde cholangiopancreatography: a large sample sized retrospective study. World J Clin Cases. 2019;7:1028–1037. doi:10.12998/wjcc.v7.i9.1028
8. Maple JT, Ikenberry SO, Anderson MA, et al. The role of endoscopy in the management of choledocholithiasis. Gastrointest Endosc. 2011;74:731–744. doi:10.1016/j.gie.2011.04.012
9. Nzenza TC, Al-Habbal Y, Guerra GR, Manolas S, Yong T, McQuillan T. Recurrent common bile duct stones as a late complication of endoscopic sphincterotomy. BMC Gastroenterol. 2018;18:39. doi:10.1186/s12876-018-0765-3
10. Podboy A, Gaddam S, Park K, Gupta K, Liu Q, Lo SK. Management of difficult choledocholithiasis. Dig Dis Sci. 2022;67:1613–1623. doi:10.1007/s10620-022-07424-9
11. Itoi T, Sofuni A, Itokawa F, Shinohara Y, Moriyasu F, Tsuchida A. Evaluation of residual bile duct stones by peroral cholangioscopy in comparison with balloon-cholangiography. Dig Endosc. 2010;22(Suppl 1):S85–89. doi:10.1111/j.1443-1661.2010.00954.x
12. Ohashi A, Ueno N, Tamada K, et al. Assessment of residual bile duct stones with use of intraductal US during endoscopic balloon sphincteroplasty: comparison with balloon cholangiography. Gastrointest Endosc. 1999;49:328–333. doi:10.1016/S0016-5107(99)70009-X
13. Huang SW, Lin CH, Lee MS, Tsou YK, Sung KF. Residual common bile duct stones on direct peroral cholangioscopy using ultraslim endoscope. World J Gastroenterol. 2013;19:4966–4972. doi:10.3748/wjg.v19.i30.4966
14. Yang JJ, Liu XC, Chen XQ, Zhang QY, Liu TR. Clinical value of DPOC for detecting and removing residual common bile duct stones (video). BMC Gastroenterol. 2019;19:135. doi:10.1186/s12876-019-1045-6
15. Lee JK, Lee SH, Kang BK, et al. Is it necessary to insert a nasobiliary drainage tube routinely after endoscopic clearance of the common bile duct in patients with choledocholithiasis-induced cholangitis? A prospective, randomized trial. Gastrointest Endosc. 2010;71:105–110. doi:10.1016/j.gie.2009.08.009
16. Yin J, Wang D, He Y, Sha H, Zhang W, Huang W. The safety of not implementing endoscopic nasobiliary drainage after elective clearance of choledocholithiasis: a systematic review and meta-analysis. BMC Surg. 2024;24:239. doi:10.1186/s12893-024-02535-8
17. Buxbaum JL, Abbas Fehmi SM, Sultan S, et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019;89:1075–1105.e1015. doi:10.1016/j.gie.2018.10.001
18. Scaffidi MA, Grover SC, Carnahan H, et al. Impact of experience on self-assessment accuracy of clinical colonoscopy competence. Gastrointest Endosc. 2018;87:827–836.e822. doi:10.1016/j.gie.2017.10.040
19. Parihar V, Moran C, Maheshwari P, et al. Measuring the value of endoscopic retrograde cholangiopancreatography activity: an opportunity to stratify endoscopists on the basis of their value. Eur J Gastroenterol Hepatol. 2018;30:718–721. doi:10.1097/MEG.0000000000001129
20. Ding B, Wang J, Wei X, et al. Efficacy and safety of ERCP in patients with situs inversus totalis: multicenter case series and literature review. BMC Gastroenterol. 2022;22:497. doi:10.1186/s12876-022-02593-3
21. Kim JH, Yang MJ, Hwang JC, Yoo BM. Endoscopic papillary large balloon dilation for the removal of bile duct stones. World J Gastroenterol. 2013;19:8580–8594. doi:10.3748/wjg.v19.i46.8580
22. Testoni PA, Mariani A, Aabakken L, et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016;48:657–683. doi:10.1055/s-0042-108641
23. Anderloni A. Difficult common bile duct stones: still “difficult” or just. “different”? Endoscopy. 2020;52:429–430. doi:10.1055/a-1151-8793
24. Wu Y, Xu CJ, Xu SF. Advances in risk factors for recurrence of common bile duct stones. Int J Med Sci. 2021;18:1067–1074. doi:10.7150/ijms.52974
25. Lin Y, Yang M, Cao J, et al. Saline irrigation for reducing the recurrence of common bile duct stones after lithotripsy: a randomized controlled trial. EClinicalMedicine. 2023;59:101978. doi:10.1016/j.eclinm.2023.101978
26. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. doi:10.1136/gutjnl-2012-302779
27. Zhang J, Ling X. Risk factors and management of primary choledocholithiasis: a systematic review. ANZ J Surg. 2021;91:530–536. doi:10.1111/ans.16211
28. Pierce RA, Jonnalagadda S, Spitler JA, et al. Incidence of residual choledocholithiasis detected by intraoperative cholangiography at the time of laparoscopic cholecystectomy in patients having undergone preoperative ERCP. Surg Endosc. 2008;22:2365–2372. doi:10.1007/s00464-008-9785-3
29. Lee YN, Moon JH, Choi HJ, et al. Direct peroral cholangioscopy using an ultraslim upper endoscope for management of residual stones after mechanical lithotripsy for retained common bile duct stones. Endoscopy. 2012;44:819–824. doi:10.1055/s-0032-1309880
30. Wu X, Wu S, Tang S. Endoscopic nasobiliary drainage-based saline-injection ultrasound: an imaging technique for remnant stone detection after retrograde cholangiopancreatography. BMC Gastroenterol. 2022;22:318. doi:10.1186/s12876-022-02394-8
31. Tsuchiya S, Tsuyuguchi T, Sakai Y, et al. Clinical utility of intraductal US to decrease early recurrence rate of common bile duct stones after endoscopic papillotomy. J Gastroenterol Hepatol. 2008;23:1590–1595. doi:10.1111/j.1440-1746.2008.05458.x
32. Mutignani M, Shah SK, Foschia F, Pandolfi M, Perri V, Costamagna G. Transnasal extraction of residual biliary stones by Seldinger technique and nasobiliary drain. Gastrointest Endosc. 2002;56:233–238. doi:10.1016/S0016-5107(02)70183-1
33. Wang Y, Yang Y, Wang K, Tang S. The value of contrast-enhanced ultrasound-guided contrast injection via the endoscopic nasobiliary drainage duct in diagnosing residual common bile duct stones. Biomed Res Int. 2020;2020:3281241. doi:10.1155/2020/3281241
34. Wu J, Wang G. Retention Time of Endoscopic Nasobiliary Drainage and Symptomatic Choledocholithiasis Recurrence After Endoscopic Retrograde Cholangiopancreatography: a Single-center, Retrospective Study in Fuyang, China. Surg Laparosc Endosc Percutan Tech. 2022;32:481–487. doi:10.1097/SLE.0000000000001059
35. Noji T, Nakamura F, Nakamura T, et al. ENBD tube placement prior to laparoscopic cholecystectomy may reduce the rate of complications in cases with predictably complicating biliary anomalies. J Gastroenterol. 2011;46:73–77. doi:10.1007/s00535-010-0281-x
36. Ricci E, Conigliaro R, Bertoni G, Mortilla MG, Bedogni G, Contini S. Nasobiliary drainage following endoscopic sphincterotomy. A useful method of preventing and treating early complications. Surg Endosc. 1987;1:147–150. doi:10.1007/BF00590920
37. Leung JW, Tu R. Mechanical lithotripsy for large bile duct stones. Gastrointest Endosc. 2004;59:688–690. doi:10.1016/S0016-5107(04)00174-9
38. Facciorusso A, Gkolfakis P, Ramai D, et al. Endoscopic treatment of large bile duct stones: a systematic review and network meta-analysis. Clin Gastroenterol Hepatol. 2023;21:33–44.e39. doi:10.1016/j.cgh.2021.10.013
39. Dapeng B, Jinpei D, Haixia N, Yinmo Y, Qiushi F. Value of nasobiliary cholangiography in the diagnosis of residual common bile duct stones after endoscopic retrograde cholangiopancreatography and related factors of residual common bile duct stones. J Clin Hepatol. 2021;37:868–871.
40. Bishay K, Meng ZW, Khan R, et al. Adverse events associated with endoscopic retrograde cholangiopancreatography: systematic review and meta-analysis. Gastroenterology. 2024;168:568–586. doi:10.1053/j.gastro.2024.10.033
41. Li S, Su B, Chen P, Hao J. Risk factors for recurrence of common bile duct stones after endoscopic biliary sphincterotomy. J Int Med Res. 2018;46:2595–2605. doi:10.1177/0300060518765605
42. Lin YY, Wang YD, Yue P, et al. Could saline irrigation clear all residual common bile duct stones after lithotripsy? A self-controlled prospective cohort study. World J Gastroenterol. 2021;27:358–370. doi:10.3748/wjg.v27.i4.358
43. Tsai TJ, Lai KH, Lin CK, et al. Role of endoscopic papillary balloon dilation in patients with recurrent bile duct stones after endoscopic sphincterotomy. J Chin Med Assoc. 2015;78:56–61. doi:10.1016/j.jcma.2014.08.004
44. Omar MA, Abdelshafy M, Ahmed MY, Rezk AG, Taha AM, Hussein HM. Endoscopic papillary large balloon dilation versus endoscopic sphincterotomy for retrieval of large choledocholithiasis: a prospective randomized trial. J Laparoendosc Adv Surg Tech A. 2017;27:704–709. doi:10.1089/lap.2016.0601
45. Feng Y, Zhu H, Chen X, et al. Comparison of endoscopic papillary large balloon dilation and endoscopic sphincterotomy for retrieval of choledocholithiasis: a meta-analysis of randomized controlled trials. J Gastroenterol. 2012;47:655–663. doi:10.1007/s00535-012-0528-9
46. Rizzuto A, Fabozzi M, Settembre A, et al. Intraoperative cholangiography during cholecystectomy in sequential treatment of cholecystocholedocholithiasis: to be, or not to be, that is the question A cohort study. Int J Surg. 2018;53:53–58. doi:10.1016/j.ijsu.2018.03.023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.