Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Rotavirus Vaccine Coverage and Associated Factors Among a Rural Population: Findings from a Primary Health-Care Project in Two Northwest Ethiopia Districts
Authors Derso T, Kebede A, Wolde HF ![]() , Atnafu A
, Atnafu A ![]() , Dellie E
, Dellie E ![]()
Received 7 August 2020
Accepted for publication 25 September 2020
Published 8 October 2020 Volume 2020:11 Pages 429—435
DOI https://doi.org/10.2147/PHMT.S276037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Terefe Derso,1 Adane Kebede,2 Haileab Fekadu Wolde,3 Asmamaw Atnafu,2,4 Endalkachew Dellie2
1Department of Human Nutrition, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Dabat Research Centre Health and Demographic Surveillance System, Institute of Public Health College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Endalkachew Dellie Department of Health Systems and Policy
Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, PO. Box: 196, Gondar, Ethiopia
Email [email protected]
Objective: Rotavirus vaccines reduced severe rotavirus disease by more than 60% during the first year of life. In Ethiopia, however, about 28% and 6% of diarrheal disease hospitalizations and deaths among under-five children are associated with rotavirus, respectively. Therefore, this study aimed to investigate rotavirus coverage and associated factors in a rural population of the northwest, Ethiopia.
Methods: A community-based cross-sectional study was conducted from May to June 2019, in Dabat and Gondar Zuria districts, northwest Ethiopia. Data from 603 mothers paired with children aged 12– 36 months were collected through house-to-house visits. Variables having a p-value < 0.05 were considered to have a significant association with the outcome. Odds ratio (OR) with its 95% confidence interval (CI) was used as a measure of association.
Results: The prevalence of rotavirus vaccine coverage among children was 76.60% (95% CI; 69.98, 83.22). The dropout rate for rotavirus vaccine dose 2 out of rotavirus vaccine dose 1 was 1.99%. Mothers with formal education [AOR = 3.04; 95% CI: 1.63, 5.67] and received postnatal care [AOR = 4.37; 95% CI: 2.62, 7.27] had higher odds of rotavirus vaccine completion versus those without formal education and had not received postnatal care, respectively. Similarly, mothers who took < 1 hour to reach the vaccination center ([AOR = 2.38; 95% CI: 1.34, 4.2]) were positive predictors of rotavirus vaccine completion.
Conclusion: Rotavirus vaccine coverage in our study area was lower than the expected WHO target. Formal education, postnatal care, and time taken to reach vaccination centers were predictors to achieving full rotavirus vaccine coverage of children. Health-care services utilization after delivery should be intensified to improved child rotavirus vaccine completion in the districts. The long travel time should be dealt with by strengthening outreach services and increasing the number of new vaccination centers in the districts.
Keywords: rotavirus vaccine, child immunization, coverage, Ethiopia
Introduction
Rotaviruses are very contagious via the fecal-oral route and cause gastrointestinal infections in under-five children worldwide.1,2 Untreated diarrhea from rotaviruses can lead to severe dehydration and other complications such as seizures and encephalitis.3,4 Globally, one-fourth to one-third of all child deaths from diarrhea are associated with rotavirus infection.5 The Vast majority (95%) rotavirus deaths and hospitalizations in young children are found in low-income countries of Africa and Asia, especially the Sub-Saharan region.6,7
Reducing childhood undernutrition, poor access to clean water and unsafe sanitation are significantly important to avoid deaths from diarrheal disease in children. However, this is not sufficient to prevent all infections and an effective Rotavirus Vaccine (RVV) against the virus should be needed.8 The world health organization (WHO) introduced efficacy two doses of rotavirus vaccine (does 1 and 2) against rotavirus infections.9–11 Particularly, in low-income countries with poor access to clean water and unsafe sanitation, more than 60% of severe rotavirus disease is reduced by rotavirus vaccines during the first year of life.12 Scientific literature revealed that full rotavirus vaccine coverage can avoid 53% of all deaths13 and 40% diarrhea-related hospital admissions among under-five children from rotavirus.14 Generally, rotavirus vaccines have led to great reductions in child morbidity, mortality and health-care costs worldwide.15 However, child rotavirus vaccine coverage and uptake are still far from universal, especially in sub-Saharan countries, leading to preventable deaths among infants and children.6,16,17
Factors influencing immunization status of children vary among different sociodemographic, political, ethnic and cultural groups. Few previous studies revealed that maternal age above 25 years, higher maternal education, frequent number of primary care visits and high continuity of care18–20 were associated with higher odds of rotavirus vaccine completion. Likewise, children of mothers with adequate knowledge of rotavirus had increased completion of rotavirus vaccine series.19 Geographical accessibility of health-care services including immunization is another key determinant in the promotion of child health and reduction of child mortality.21 However, long-distance travel to vaccine providers in health facilities appeared to be a barrier to the delivery of infant vaccines in a remote community.22,23
Improving access to childhood vaccines in low-income countries has been a major goal of public health services.24 However, Ethiopia is one of five countries with the greatest rotavirus disease burden worldwide.25,26 Moreover, about 28% and 6% of diarrheal disease hospitalizations and deaths among under-five children in Ethiopia were caused by rotavirus, respectively.26,27 A monovalent rotavirus vaccine was introduced in the Ethiopian Expanded Program on Immunization in 2012.28 The Ethiopian Demographic and Health Survey (EDHS) documented that diarrheal morbidity in under-five children has dropped from 18% in 2005 to 13% in 2016. Despite these efforts, nearly half (44%) of children do not receive the rotavirus vaccine in Ethiopia, 2016.16 These children are at a high risk of diarrheal diseases due to rotavirus. The performance of immunization programmes is commonly measured by coverage and uptake of vaccines. Thus, ensuring that every child is immunized at the earliest or appropriate age is an important public health goal and the most cost-effective public health interventions.29 In resource-limited settings like Ethiopia, there is inadequate data on the coverage of the rotavirus vaccine since its introduction. Assessing rotavirus vaccine coverage is a critical component of public health. Therefore, this paper aimed to investigate rotavirus coverage and associated factors in the rural population of the northwest, Ethiopia.
Methods
Study Design and Setting
A community-based cross-sectional study was conducted from May to June 2019 in the two (Dabat and Gondar Zuria district) northwest Ethiopian Districts. Dabat and Gondar Zuria districts are the two neighboring districts among 23 districts in the north Gondar Zone of the Amhara region, consisting of 30 and 38 kebeles (smallest administrative unit in Ethiopia), respectively. The two districts are found in different ecological zones (high land, middle land, and low land), and have 145,509 inhabitants (Dabat district) and 231,324 inhabitants (Gondar district). For their livelihood, the residents largely depend on agriculture.
Population, Sample Size Determination, and Sampling Procedure
All children aged 12–36 months who lived in the study area for at least 6 months were included in the study. Of the total kebeles, eight kebeles in the Dabat district and ten kebeles in Gondar Zuria district were selected using the lottery method. A systematic sampling technique was used to select study participants. For households with multiple children fulfilling the inclusion criteria, a child was selected using lottery method. The sample size was calculated using Epi-info version 3.7 by considering the following assumptions: 50% as the prevalence of rotavirus vaccine coverage among children, 95% level of confidence and 5% margin of error. A design effect of 1.5 and 10% non-response rate were also anticipated which gives a final sample size of 633.
Data Collection Tools and Procedure
Data from the mothers or caregivers of the children were collected through home to home visits using a structured interviewer-administered questionnaire. The questionnaire was designed to capture socio-demographic characteristics; health service utilization; physical access to maternal health services, family planning and immunization status. The questionnaire was prepared in English, translated to Amharic (the local language), and retranslated back to English to maintain consistency. The questionnaire was administered in Amharic. Two days of training regarding data collection and sampling techniques were given to data collectors and supervisors. During pre-testing, the acceptability and the logical structure of the questionnaire were checked. Fifteen diploma nurses and three BSc nurses were recruited for data collectors and field supervisors, respectively. The data collection assesses for the presence of a child’s immunization card. Data on child vaccination (rotavirus vaccine dose 1 and 2) were collected from vaccination cards and, if unavailable, by parents’ interview only, as suggested. Data were checked for completeness and its quality daily by the field supervisors and investigators.
Measurements of Variables
RVV is administered orally with an interval of at least four weeks between the two doses. The recommended vaccination is a two-dose schedule, administered at 6 weeks (first dose, rotavirus dose 1) and 14 weeks (second dose, rotavirus dose 2) of age along with other EPI vaccines.28 The outcome variable was rotavirus vaccine (RVV) coverage, with receipt of 2-dose monovalent RVV series classified as complete. RVV coverage was calculated as; a 12–36 months old child who received the two doses of rotavirus vaccine divided by the total children included in this study. A partial series (1 dose of RVV) was categorized as an incomplete RVV series. Children who did not receive any rotavirus vaccine before this study was considered to be not immunized.10,16 The dropout rate was calculated by subtracting the number of children receiving the last dose of the RVV from the number of children receiving the first dose of the vaccine and dividing the difference by the number of children receiving the first dose of the vaccine.30 This proportion was then multiplied by 100 to obtain the dropout percentage.
In this study, Health Extension Workers (HEWs) frequency of home visits was assessed by the number of HEW visits made in a month. Accordingly, we categorized it into weekly visits if there were at least four visits per month, sometimes if there were less than four visits per month, and no visits if there was no visit at all in a month.
Data Processing and Analysis
Epi-data version 3.1 was used for data entry and data were exported to SPSS version 21 for analysis. Descriptive statistics were presented using texts and tables. Binary Logistic regression model was used to assess the relationship between the dependent (rotavirus vaccine coverage) and independent variables. Those variables which were significant in the bivariable analysis (p-value < 0.2) were entered into the multivariable analysis. In the final model, a significant association was declared at a p-value less than 0.05 with an adjusted odds ratio (AOR) and the corresponding 95% confidence interval.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the University of Gondar (Ref. No. IPH/180/06/2011). Informed consent was also obtained from children’s parents or guardians. Confidentiality of information was guaranteed by using code numbers and data was locked in a safety cabinet. Participants could opt out of the study at any time if they felt uncomfortable. Finally, the study was carried out in accordance with the Helsinki Declaration.
Results
Socio-Demographic and Health-Related Characteristics of Study Participants
In this study, 603 eligible children aged 12–36 months were included with a response rate of 95.26%. Most of the study participants (92.7% and 99.0 %, respectively) were married and lived in a rural area. The great majority of study participants were housewives (94.7%) and had no formal education (77.9%) (Table 1).
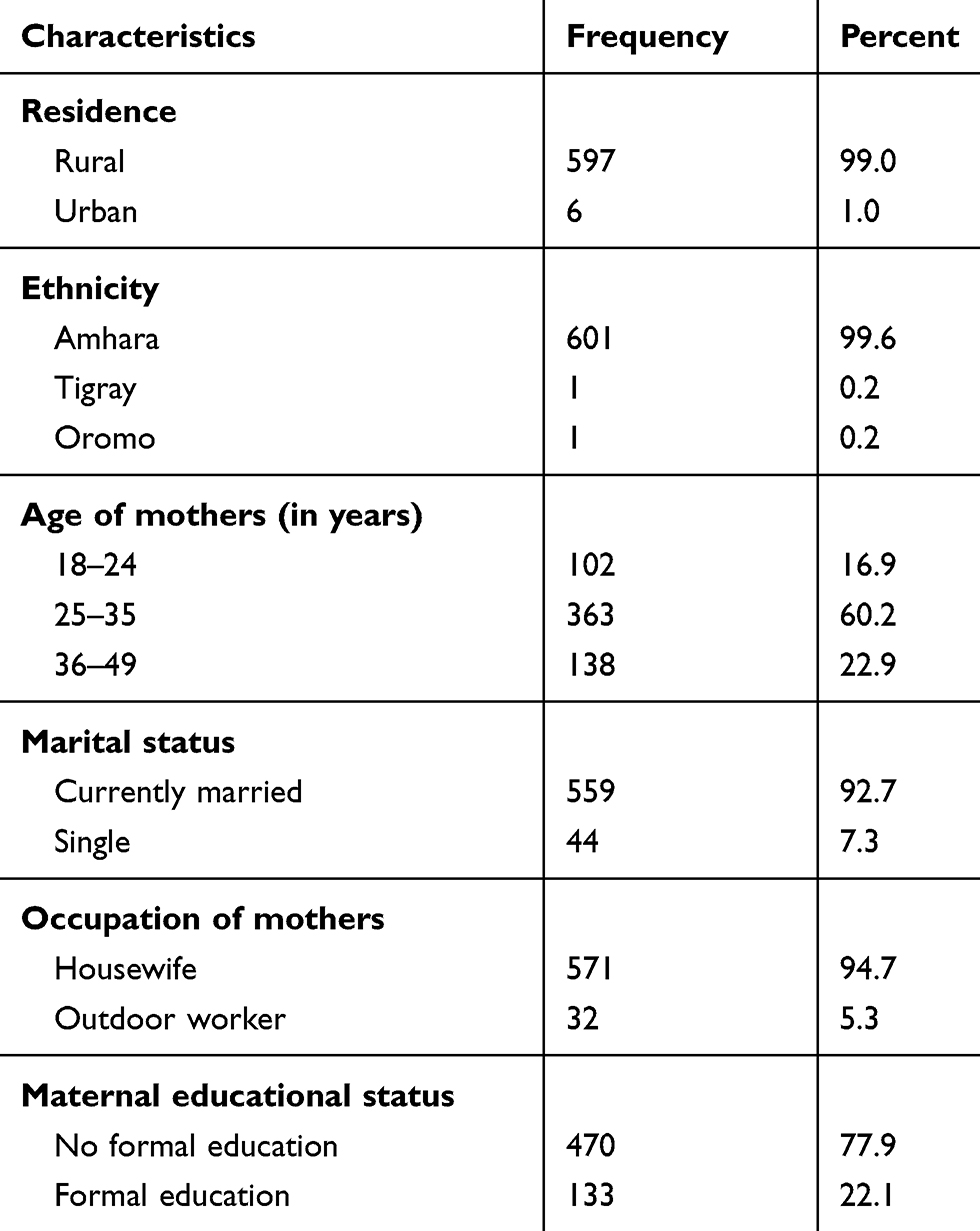 |
Table 1 Sociodemographic Characteristics of Study Participants in the Rural Population of Northwest Ethiopia, 2019 (N= 603) |
Health-Related Characteristics of Study Participants
Nearly one-fourth (23.2%) of the study participants traveled for more than one hour to reach the nearest vaccination facility or center. However, the majority (70.0%) of mothers gave birth in health institutions, 65.8% had a history of postnatal care and 63.2% had a child vaccination card at the time of the interview. (Table 2).
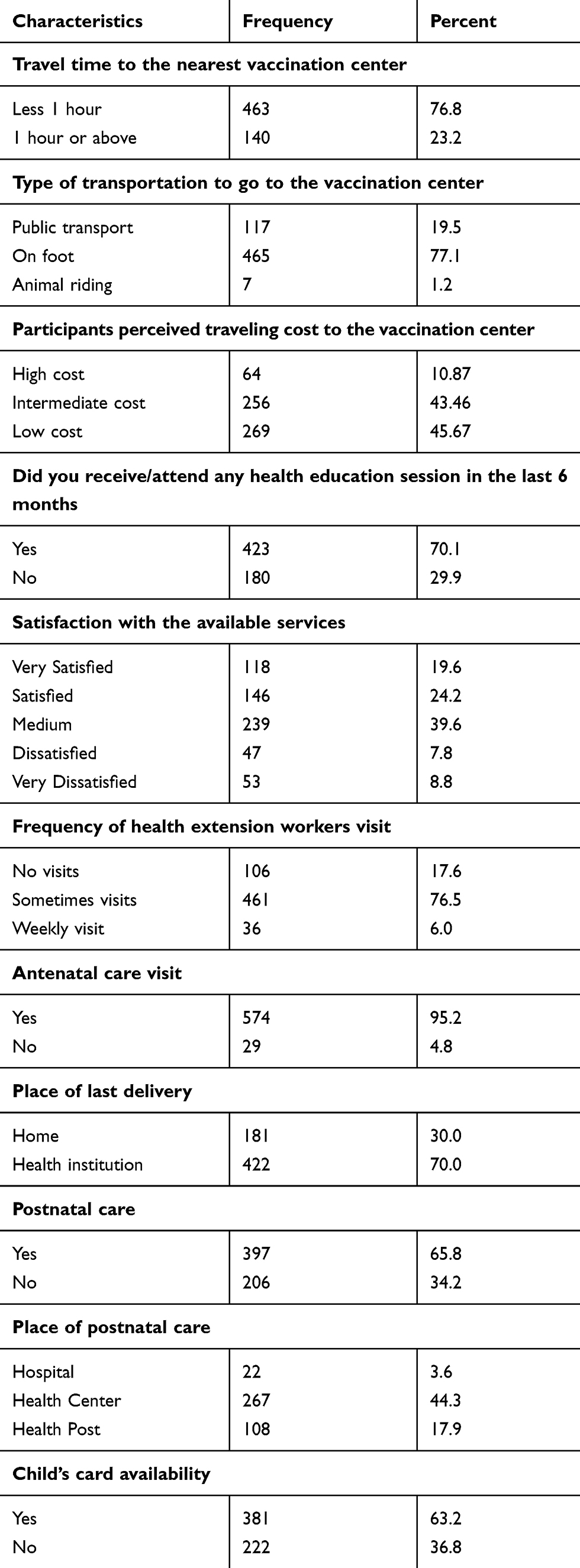 |
Table 2 Health-Related Characteristics of Study Participants in the Rural Population of Northwest Ethiopia, 2019 (N= 603) |
Prevalence of Rotavirus Vaccine Coverage
The overall prevalence of rotavirus vaccine coverage among children was 76.60% (95% CI; 69.98, 83.22). Of the 603 children, 474 (78.60%) had received only a single dose of the rotavirus vaccine. The study also indicated that the rotavirus vaccine dropout rate was 1.99%.
Factors Associated with Rotavirus Vaccine Coverage
In the bivariable analysis, age of the mother, source of health information from radio, maternal education, travel time to the nearest vaccination center, travel cost to the nearest vaccination center, antenatal care, postnatal care and place of delivery were factors associated with rotavirus vaccine coverage at a p-value of less than 0.2. The multivariable analysis revealed that maternal education, travel time to the nearest vaccination centers and postnatal care visits were significantly associated with rotavirus vaccine completion. Multivariable logistic regression revealed that mothers with formal education [AOR = 3.04; 95% CI: 1.63, 5.67] and received postnatal care [AOR = 4.37; 95% CI: 2.62, 7.27] had higher odds of rotavirus vaccine completion versus those without formal education and had not received postnatal care, respectively. Similarly, this study showed that mothers who took <1 hour to reach the vaccination center ([AOR = 2.38; 95% CI: 1.34, 4.2]) was another positive predictor of rotavirus vaccine completion (Table 3).
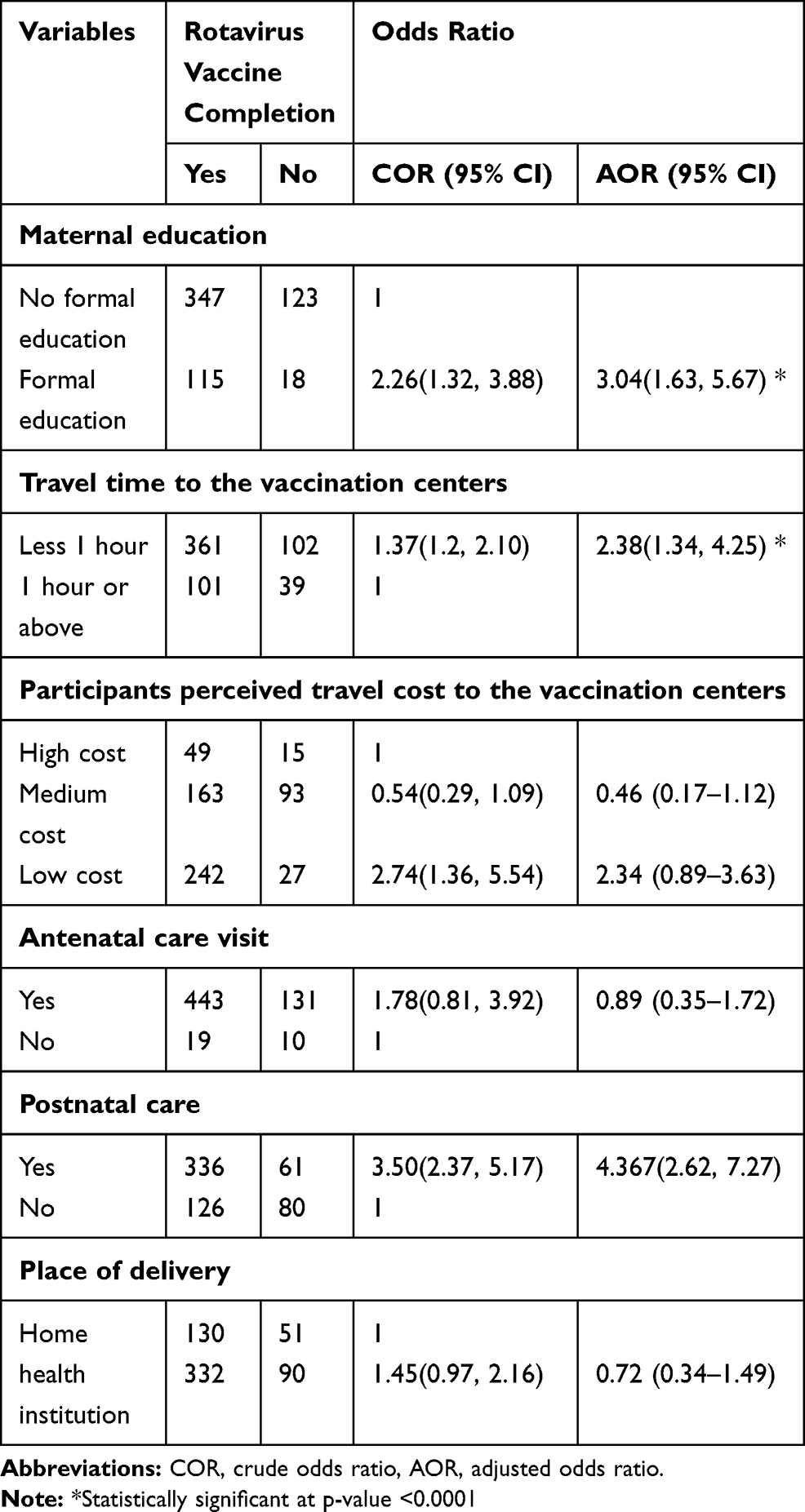 |
Table 3 Factors Associated with Rotavirus Vaccine Coverage in the Rural Population of Northwest, Ethiopia, 2019 (N= 603) |
Discussion
In this study, the prevalence of rotavirus vaccine coverage among children was 76.60%. Formal education, postnatal care and time taken to reach the nearest vaccination centers were predictors of rotavirus vaccine completion of children.
In this finding, the prevalence of rotavirus vaccine coverage was similar to a local study reported from Sekota Zuria district, Ethiopia (80%).31 However, the current finding was lower than reported from local studies Minjar-Shenkora district (89.2%)32 and Debre Markos Town (93.4%).33 The difference might be due to the study setting, the rural residence of all mothers with children in the current study compared to the former study settings.
The geographical inaccessibility of health facilities in rural residences has been found to hinder immunization uptake and difficulties encountered to reach healthcare facilities are major barriers to child immunization completion.34 Mothers living in rural areas were more likely to be affected by the long walking time needed to reach the health-care facilities from the house and had lower access to education and counseling on immunization.35 However, RVV coverage in the study area was higher than the national coverage of the 2016 EDHS report (56%).34 The low proportion of rotavirus coverage in the EDHS report compared to these districts might be due to EDHS data being a national-level data and thus a high variability of immunization services. Also, higher rotavirus vaccine coverage is documented in Kenya (86.3%)19 compared to the current finding. This might be explained by the higher educational status of mothers in Kenya (about 98% of study participants had primary and above educational status) could increase the use of available health services, as educated women would have a better awareness of the benefits of rotavirus vaccination.
Children from mothers with formal education had higher odds of completing the RVV schedule than those without formal education. Similar findings were reported in studies from Kenya19 and Canada.18 Educated mothers are generally more aware of the importance of available health and immunization services, have better communication skills, and tend to better utilize available health services.
The multivariable analysis showed that the likelihoods of rotavirus vaccine completion among children were higher among mothers who had a history of postnatal care follow-up compared with those who did not. Likewise, a greater number of primary care visits and high continuity of care have higher odds of rotavirus vaccine completion in Canada.18 This implies that mothers are getting adequate information about the child vaccination schedule during their postnatal care visits. The WHO guidelines for mothers and infants postnatal care include guidance on preventive measures like that of immunization.36
In this study, traveling time from home to the vaccination center was another predictive factor for rotavirus vaccine completion. Mothers who took <1 hour to reach the vaccination center was significantly associated with rotavirus vaccine completion. Similarly, a local study from Sekota Zuria district, mothers/caregivers who traveled for less than one hour to the vaccination center was associated with a child being fully immunized.31 This could be explained by the fact that as mothers often deal with different household responsibilities, a short travel time to reach the vaccination center would reduce an opportunity cost. In fact, the universal accessibility of health-care services like immunization is one of the key factors in promoting child health and reducing child mortality.21 However, long travel time to the vaccination center is a barrier to infant vaccines in the remote Ethiopian community.23
Limitations of the Study
Recall bias was a limitation of this study. There is a chance of children’s parents or caregivers that might prone to over or under-reporting of some variables. But strong efforts were made to minimize the over or under-reporting of some variables, mainly through recruiting experienced data collectors and supervisors and also assessed the presence of a children’s immunization card.
Conclusion and Recommendations
In the region, rotavirus vaccine coverage was still lower than expected WHO targets of at least 90% by 2015. Formal education, postnatal care, and time taken to reach vaccination centers were predictors to achieving full rotavirus vaccine coverage of children. Health-care services utilization after delivery should be intensified to improved child rotavirus vaccine completion in the districts. The long travel time should be addressed by strengthening outreach services and increasing the number of new vaccination centers/clusters in the districts.
Acknowledgments
The authors would like to thank data collectors, supervisors and all respondents for their willingness to participate in the study. Our appreciation will also go to the University of Gondar for their financial and material support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors declared that they have no competing interest in this work.
References
1. Giaquinto C, Van Damme P, Group RS. Age distribution of paediatric rotavirus gastroenteritis cases in Europe: the REVEAL† study. Scand J Infect Dis. 2010;42(2):142–147. doi:10.3109/00365540903380495
2. Grimwood K, Lambert SB, Milne RJ. Rotavirus infections and vaccines. Pediatric Drugs. 2010;12(4):235–256. doi:10.2165/11537200-000000000-00000
3. Ansari SA, Springthorpe VS, Sattar SA. Survival and vehicular spread of human rotaviruses: possible relation to seasonality of outbreaks. Rev Infect Dis. 1991;13(3):448–461. doi:10.1093/clinids/13.3.448
4. Greenberg HB, Estes MK. Rotaviruses: from pathogenesis to vaccination. Gastroenterology. 2009;136(6):1939–1951. doi:10.1053/j.gastro.2009.02.076
5. Clark A, Black R, Tate J, et al. Estimating global, regional and national rotavirus deaths in children aged< 5 years: current approaches, new analyses and proposed improvements. PLoS One. 2017;12(9):e0183392.
6. Seheri LM, Page NA, Mawela MPB, et al. Rotavirus vaccination within the South African expanded programme on immunisation. Vaccine. 2012;30:C14–C20. doi:10.1016/j.vaccine.2012.04.018
7. Troeger C, Blacker BF, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1211–1228. doi:10.1016/S1473-3099(18)30362-1
8. Yamashiro R, Sakudo A, Nagatsu M. Efficient recovery and enrichment of infectious rotavirus using separation with antibody-integrated graphite-encapsulated magnetic nanobeads produced by argon/ammonia gas plasma technology. Int J Nanomedicine. 2019;14:1865. doi:10.2147/IJN.S191784
9. Ruiz-Palacios GM, Pérez-Schael I, Velázquez FR, et al. Safety and efficacy of an attenuated vaccine against severe rotavirus gastroenteritis. N Engl J Med. 2006;354(1):11–22. doi:10.1056/NEJMoa052434
10. Vesikari T, Matson DO, Dennehy P, et al. Safety and efficacy of a pentavalent human–bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354(1):23–33. doi:10.1056/NEJMoa052664
11. Organization WH. Rotavirus vaccines: WHO position paper—January 2013. Weekly Epidemiol Rec/Relevé épidémiologique hebdomadaire. 2013;88(05):49–64.
12. Armah GE, Sow SO, Breiman RF, et al. Efficacy of pentavalent rotavirus vaccine against severe rotavirus gastroenteritis in infants in developing countries in sub-Saharan Africa: a randomised, double-blind, placebo-controlled trial. The Lancet. 2010;376(9741):606–614. doi:10.1016/S0140-6736(10)60889-6
13. Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr. 2018;172(10):958–965. doi:10.1001/jamapediatrics.2018.1960
14. Aliabadi N, Antoni S, Mwenda JM, et al. Global impact of rotavirus vaccine introduction on rotavirus hospitalisations among children under 5 years of age, 2008–16: findings from the Global Rotavirus Surveillance Network. Lancet Global Health. 2019;7(7):e893–e903. doi:10.1016/S2214-109X(19)30207-4
15. Soares‐Weiser K, Bergman H, Henschke N, et al. Vaccines for preventing rotavirus diarrhoea: vaccines in use. Cochrane Database Syst Rev. 2019;10.
16. Doherty T, Rohde S, Besada D, et al. Reduction in child mortality in Ethiopia: analysis of data from demographic and health surveys. J Glob Health. 2016;6:2. doi:10.7189/jogh.06.020401
17. Wandera EA, Mohammad S, Ouko JO, et al. Variation in rotavirus vaccine coverage by sub-counties in Kenya. Trop Med Health. 2017;45(1):9. doi:10.1186/s41182-017-0051-z
18. Wilson SE, Chung H, Schwartz KL, et al. Rotavirus vaccine coverage and factors associated with uptake using linked data: ontario, Canada. PLoS One. 2018;13(2):e0192809. doi:10.1371/journal.pone.0192809
19. Lucy W, Kanja AMP, Kirika L. Behavioral factors associated with the completion of rotavirus vaccine series in children attending pediatric asualty in a Public Hospital, Nairobi County, Kenya. Arch Commun Fam Med. 2018;1(1):24–32.
20. Aliabadi N, Wikswo ME, Tate JE, et al. Factors associated with rotavirus vaccine coverage. Pediatrics. 2019;143:2. doi:10.1542/peds.2018-1824
21. Kiwanuka S, Ekirapa E, Peterson S, et al. Access to and utilisation of health services for the poor in Uganda: a systematic review of available evidence. Trans R Soc Trop Med Hyg. 2008;102(11):1067–1074. doi:10.1016/j.trstmh.2008.04.023
22. Kiros G-E, White MJ. Migration, community context, and child immunization in Ethiopia. Soc Sci Med. 2004;59(12):2603–2616. doi:10.1016/j.socscimed.2004.04.009
23. Okwaraji YB, Mulholland K, Schellenberg J, et al. The association between travel time to health facilities and childhood vaccine coverage in rural Ethiopia. A community based cross sectional study. BMC Public Health. 2012;12(1):476. doi:10.1186/1471-2458-12-476
24. Jones G, Steketee RW, Black RE, et al. How many child deaths can we prevent this year? The Lancet. 2003;362(9377):65–71. doi:10.1016/S0140-6736(03)13811-1
25. Tate JE, Burton AH, Boschi-Pinto C, et al. 2008 estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programmes: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(2):136–141. doi:10.1016/S1473-3099(11)70253-5
26. Tate JE, Burton AH, Boschi-Pinto C, et al. World Health Organization Coordinated Global Rotavirus Surveillance Network. Global, regional, and national estimates of rotavirus mortality in children< 5 years of age, 2000–2013. Clin Infect Dis. 2016;62(Suppl 2):S96–S105.
27. Organization WH. Global Rotavirus Information and Surveillance Bulletin. Geneva: WHO; 2013.
28. Health FMo. Ethiopia National Expanded Programme on Immunization: Addis Ababa: BMJ Publishing Group FMOE; 2015.
29. Olusanya BO. Pattern and determinants of BCG immunisation delays in a sub-Saharan African community. Health Res Policy Syst. 2010;8(1):1. doi:10.1186/1478-4505-8-1
30. Federal Ministry of Health E. Ethiopian National Expanded Program on Immunization Comprehensive Multi-Year Plan 2016–2020. Addis Ababa: FMOH; 2015. Available from:: https://extranet.who.int/countryplanningcycles/sites/default/files/country_docs/Ethiopia/ethiop_cmyp_latest_revised_may_12_2015.pdf.
31. Girmay A, Dadi AF. Full immunization coverage and associated factors among children aged 12-23 months in a hard-to-reach areas of Ethiopia. Int J Pediatr. 2019;2019.
32. Mekonnen AG, Bayleyegn AD, Ayele ET. Immunization coverage of 12–23 months old children and its associated factors in Minjar-Shenkora district, Ethiopia: a community-based study. BMC Pediatr. 2019;19(1):1–8. doi:10.1186/s12887-019-1575-7
33. Gualu T, Dilie A. Vaccination coverage and associated factors among children aged 12–23 months in debre markos town, Amhara regional state, Ethiopia. Advan Public Health. 2017;2017.
34. Agency CS, ICF. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
35. Adedokun ST, Uthman OA, Adekanmbi VT, et al. Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors. BMC Public Health. 2017;17(1):236. doi:10.1186/s12889-017-4137-7
36. Organization WH. WHO Recommendations on Postnatal Care of the Mother and Newborn: World Health Organization; 2014.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.