Back to Journals » Clinical Ophthalmology » Volume 20
Rotational Stability of the Clareon PanOptix Toric (CNWTTx) Hydrophobic Multifocal IOL: Real-World Clinical Outcomes
Authors Agarwal S ![]() , Chang LYL, Thornell E
, Chang LYL, Thornell E ![]()
Received 15 April 2026
Accepted for publication 9 June 2026
Published 18 June 2026 Volume 2026:20 615101
DOI https://doi.org/10.2147/OPTH.S615101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Smita Agarwal,1– 3 Lily Yu-Li Chang,1 Erin Thornell1
1Wollongong Eye Specialists, Wollongong, NSW, Australia; 2Graduate School of Medicine, University of Wollongong, Wollongong, NSW, Australia; 3Central Clinical School, Sydney University, Sydney, NSW, Australia
Correspondence: Smita Agarwal, Wollongong Eye Specialists, Level 2A, 2 Victoria St, Wollongong, NSW, Australia, Tel +61 2 4227 6388, Email [email protected]
Purpose: To assess and validate rotational stability and visual outcomes data of the CNWTTx (Clareon® PanOptix®) Toric multifocal intraocular lens (IOLs) in routine clinical practice.
Methods: In this prospective, single-centre, real-world, confirmatory study, CNWTTx was implanted in 40 eyes from 22 patients that underwent bilateral routine phacoemulsification. Manifest refraction, uncorrected vision at distance (UDVA), intermediate (UIVA) and near at 40 cm (N-40) and 33 cm (N-33) were measured at 4– 6 weeks and 12-weeks postoperatively. Quality of vision was assessed using the Near Acuity Visual Questionnaire (NAVQ), stereoacuity and contrast sensitivity (CS). Toric alignment was primarily measured using slit lamp examination at 1 hour, 1 week, 4– 6 weeks and 12 weeks postoperatively. Rotational stability was assessed by measuring change in toric alignment from target axis at each time point. iTrace was used as an exploratory method of assessing IOL rotation.
Results: Mean absolute and actual rotation at 12 weeks was 3.4° and − 1.3°, respectively, with 85% of eyes achieving ≤ 5° of rotation. Monocular uncorrected visual acuity was 0.06 ± 0.09, 0.1 ± 0.14, 0.13 ± 0.11 and 0.14 ± 0.11 LogMAR at 6 m, 60 cm, 40 cm and 33 cm, respectively. Postoperative spherical equivalent at 12 weeks was − 0.15 ± 0.28 D. NAVQ score increased significantly following surgery, and contrast sensitivity and stereoacuity were well maintained compared to age-normal values.
Conclusion: Accurate visual and refractive outcomes were achieved with CNWTTx in this cohort, and the lens remained stable from 1 week following implantation. This was consistent with the high patient-reported satisfaction despite visual phenomena inherent to diffractive IOLs. However, the percentage of eyes achieving ≤ 5° of rotation within this cohort was 5% lower than the ANSI Z80.30 standard, which was likely due to the small sample size of this study. Future studies with larger sample size are warranted to fully ascertain the lens’ performance against the ANSI Z80.30 benchmark.
Plain Language Summary: While offering patients a greater degree of spectacle independence following surgery, multifocal intraocular lenses (IOLs) require precise placement in the eye and to remain stable for optimal outcomes. The CNWTTx IOL is composed of a newer material than that of its predecessor, the TFNT00 toric IOL. It is unclear how this new material affects its stability within the eye.
We followed 40 eyes from 22 patients who had received the CNWTTx IOL and measured its position within the eye at 1 hour, 1 week, 4– 6 weeks and 3 months. We found that the majority of eyes rotated ≤ 5°, largely within 1 week of surgery. Additionally, patients achieved good and predictable visual and refractive outcomes.
These findings suggest that the stability of the CNWTTx IOL does not appear to be impacted by the new material and is an effective option for patients wanting spectacle independence.
Keywords: multifocal IOL, rotational stability, toric alignment, cataract surgery, real-world outcomes
Introduction
Toric IOLs were first introduced in the early 1990s to concurrently correct regular astigmatism and spherical refractive error during cataract surgery,1 but optimal efficacy depends on precise axis alignment. A 3° alignment error results in a 10% undercorrection of astigmatism, and a ≥30° alignment error can neutralise astigmatic correction altogether.2 To provide an internationally recognised and consistent guidance on lens alignment, the ANSI Z80.30 standard3 defines the IOL stability threshold as a change in rotation of 5° or less, a benchmark that must be achieved by at least 90% of eyes between consecutive postoperative visits spaced at least 3 months apart. As the majority of IOL rotation typically occurs during the first postoperative week before capsular bag contraction stabilises the lens,4 managing patient-specific anatomical risk factors (eg. a long axial length (AL), a large capsular bag and with-the-rule or oblique astigmatism) and considering physical IOL characteristics that increase risk of rotation (eg. a small overall diameter, rigid polymethyl methacrylate (PMMA) material, or traditional C-loop haptic designs) remain critical priorities.5 Consequently, manufacturers continuously optimise biomaterials and haptic geometries to attain more predictable IOL orientation and visual outcomes.6–9
This demand for precise orientation is further amplified when astigmatism correction is combined with presbyopia-correcting optics. While multifocal IOLs offer a higher degree of spectacle independence compared to standard monofocal IOLs, they can compromise visual quality by reducing contrast sensitivity and introducing photic phenomena such as glare and halos.10 Furthermore, multifocal toric IOLs are typically more sensitive to postoperative axis misalignment; a rotation greater than 5° or a residual refractive error exceeding 0.5 D can severely degrade optical image quality,11 making rigorous clinical evaluation of the rotational stability and refractive accuracy of newly introduced toric platforms essential. Such evaluations are particularly vital in ophthalmic markets characterised by high astigmatism-correction rates. For instance, Australia exhibits some of the highest global uptake rates for toric IOLs, which account for approximately 30% of all cataract implantations.12 Given this substantial surgical utility, investigating how new toric IOLs perform outside of tightly controlled clinical trials carries significant domestic relevance. Moreover, generating real-world evidence from such high-volume environments provides critical, translatable benchmarks for international regions with established or growing utilisation of toric IOL technology.
A prominent example of recent innovation in this area is the PanOptix® family of IOLs (Alcon Laboratories, Inc., Fort Worth, TX, USA), which utilises a non-apodized, aspheric, quadrifocal diffractive design featuring a 4.5 mm diffractive zone with 15 concentric rings. The established TFNT00 model (AcrySof® PanOptix®; Alcon Labs, Ft Worth, TX, USA) is composed of an acrylate/methacrylate copolymer, and incorporates STABLEFORCE™ modified C-loop haptics – a design well-documented for its excellent rotational stability, predictable distance, intermediate (60 cm) and near (40 cm) visual acuity, and high levels of spectacle independence.13–15 Building on this optical platform, the newer CNWTTx model (Clareon® PanOptix®; Alcon Labs, Ft Worth, TX, USA) shares the identical optic profile and haptic geometry, but introduces an updated cross-linked acrylic biomaterial initially introduced as the CNA0T0 monofocal IOL. This advanced polymer combines a hydrophilic component (2-hydroxyethyl-methacrylate) with a hydrophobic component (phenylethyl acrylate), yielding a higher water content (1.5% compared to the 0.5% found in TFNT00) that is distributed uniformly across the optic, designed to minimise glistening and surface haze.16 However, while the mechanical stability of the original TFNT00 platform17,18 and the CNA0T019,20 IOL in situ have been clinically validated in separate studies, it remains crucial to determine how the CNWTTx, a product of the TFNT00 trifocal optics and the CNA0T0 material combined, performs in rotational stability. Although its total water content remains low compared to hydrophilic IOLs, the increased IOL hydration could theoretically modify early capsular adhesion or fibronectin binding, potentially elevating the risk of early postoperative IOL rotation.
Recently, Garzón et al21 provided foundational data on this new platform, demonstrating excellent visual outcomes, rotational stability, centration, and patient satisfaction of CNWTTx. However, as real-world clinical environments present diverse patient demographics and clinical variations, further investigation of these initial findings in routine clinical practice is necessary. The present study provides a confirmatory evaluation of the findings reported by Garzón et al21 by assessing the rotational stability, visual acuity, and patient-reported outcomes of the CNWTTx IOL within a real-world, clinical setting.
Methods
Patient Demographics
The CNWTTx IOL was implanted in 40 eyes from 22 patients (age 63.1 ± 16.6 years; 36.4% male) who underwent routine phacoemulsification and implantation of CNWTTx (toric or non-toric) for the treatment of age-related cataract. CNWTTx were implanted bilaterally for 18 patients, while 4 patients received CNWTT0 non-toric IOLs in the fellow eye. Patients with previous keratorefractive surgery, ocular co-morbidity, preoperative chord mu > 0.5,22 and a non-emmetropic refractive target were excluded. This study received ethics approval from the University of Wollongong Health and Medical Human Research Ethics Committee (2023/352) and followed the Tenets of the Declaration of Helsinki. Informed consent was obtained for each participant prior to commencing the study.
Surgical Procedure
All surgeries were performed by the same surgeon (SA) at a single site. Biometry was performed preoperatively (IOLMaster 700; Zeiss; Germany), and lens power was calculated using the Barrett TK Universal II formula with a postoperative spherical equivalent target of ±0.25 D. Briefly, a 2.3 mm corneal incision was made temporally, followed by two 1 mm side ports positioned at 180°. Following the creation of a capsulorrhexis, phacoemulsification was performed and a CNWTTx Toric IOL was implanted. Target axis was selected using preoperative biometry and verified with autorefraction, and the IOLs were aligned intraoperatively using Callisto image-guidance technology following thorough removal of all viscoelastic from behind the IOL. The Callisto image-guidance software (Zeiss; Germany) uses preoperative scleral images and anatomical markers (ie blood vessels) to form a horizontal reference line that is projected through the microscope eyepiece along with a separate reference line indicating the nominated implantation axis (Supplementary Figure 1A). This allows for precise alignment of the IOL while accommodating for cyclorotation. Postoperatively, patients were advised to use ofloxacin (Ocuflox; Alcon; Fort Worth, TX) and prednisolone acetate (Prednefrin Forte; Abbvie; North Chicago, IL) eye drops, 1 drop 2 hourly on the day of surgery. From day 1 postop, patients were advised to use ofloxacin and prednisolone acetate four times a day for 2 and 4 weeks respectively, and to commence ketorolac tromethamine (Acular; Allergan; Irvine CA) drops one week after surgery, continuing four times a day for a week.
Postoperative Vision Assessment
Postoperative assessment was performed at 1 hour following surgery and repeated at 1 week, 4–6 weeks and 12 weeks. Uncorrected monocular and binocular distance visual acuity (UDVA) and monocular corrected distance visual acuity (BCVA) were measured at equivalent of 6 meters using Snellen chart (DMD-FVD-24 DMD Vista Vision Wide VA Tester, DMD Computers, Turin, Italy) under photopic conditions. Uncorrected (UIVA) and distance-corrected intermediate vision (DCIVA) were measured at 60 cm monocularly and binocularly using a reading chart (EDTRS 2000 Series; Precision Vision, Woodstock, Illinois, USA), and uncorrected and distance-corrected near vision was measured at 40 cm (UNVA-40 and DCNVA-40) and 33 cm (UNVA-33 and DCNVA-33) using a reading chart (EDTRS 2000 Series) under photopic conditions. Manifest refraction was conducted using a phoropter and Snellen chart placed at 6 meters.
Assessment of IOL Rotation and Stability
Intraoperative snapshots of the image-guidance system were used to verify that IOLs were successfully implanted at the target axis (Supplemental Figure 1A). Postoperatively, measurement of toric alignment was performed at 1 hour, 1 week, 4–6 weeks and 12 weeks following IOL implantation as described below. Following instillation of 1% tropicamide (Alcon; Geneva, Switzerland) and 2.5% phenylephrine (Bausch and Lomb; Laval, Canada), each eye was examined using retro-illumination on a slit lamp such that the toric markings were visible. A thin slit beam was then rotated till it overlapped with the toric markings, and the alignment was read directly from the protractor dial of the slit lamp. Patients were also assessed using automated aberrometry. Corneal topography and wavefront aberrometry scans were taken postoperatively using the iTrace (iTrace; Tracey technologies, Houston, TX, USA). Patients were instructed to maintain their head in an upright position throughout. The “Patient Education” display on the iTrace user interface shows a retro-illuminated image of the eye with toric markings clearly visible when sufficiently dilated. By clicking one of the toric markings, an axis is provided for that location, providing an objective and precise recording of the alignment of the IOL in situ (Supplemental Figure 1B). Toric rotation was recorded as the direction and change in degrees of alignment at each time point compared to the target axis. The iTrace Toric Check (Tracey Technologies, Houston, TX, USA) combines corneal topography and the total wavefront aberrometry of the eye to deduce alignment of the IOL in situ. This can deviate by up to 5° from the alignment of the actual toric markings due to variation in the manufacturing process of the IOL. For this reason, the iTrace Toric Check was not considered a viable way to accurately record change in alignment given that intraoperative placement of toric markings would be the starting point used to calculate rotation. Biometry (IOLMaster 700; Zeiss; Germany) was performed to assess anterior chamber depth (ACD), AL, and to visualize any significant IOL decentration, tilt and axial displacement.
Quality of Vision Assessment
Quality of vision was assessed at 12 weeks following IOL implantation of the second eye. Stereoacuity was assessed using Stereo Fly Test (Stereo Optical, Essilor International, France). Contrast sensitivity (CS) was measured monocularly and binocularly under mesopic conditions using Pelli Robson chart. The validated Near Activity Visual Questionnaire (NAVQ) was used to assess patient-reported outcomes and impacts on daily visual function. It is specially designed to assess near function in individuals with presbyopia and includes 10 questions that relate to everyday near vision tasks where patients are asked to self-report the level of difficulty they experience with each task. Upon completion, the NAVQ provides a Rasch score (0 to 100 with 100 being the best outcome), with overall satisfaction on a scale of 0 (completely satisfied) to 4 (completely unsatisfied) recorded as a separate score.
Statistical Analysis
Given the observational and confirmatory design of this real-world study, no formal sample size calculation or power analysis was conducted. The cohort size was determined by enrolling consecutive eligible cases who met the inclusion criteria and underwent routine cataract surgery with CNWTTx implantation during the designated study period. As this study was designed to confirm similar clinical endpoints previously reported in early published literature, a descriptive and pragmatic sample size of 40 eyes was deemed appropriate. This approach was also consistent with similar real-world, single-center clinical evaluations of new IOL platforms in routine practice.23–25
Pre- and postoperative visual and refractive parameters are presented as mean ± SD and were compared using paired two-tailed students T tests (Microsoft Excel V2601; Microsoft Corporation; Redmond, WA, USA). Correlation between change in axis and AL, ACD or amount of preoperative and residual cylinder was performed using the Pearson correlation test (Microsoft Excel V2601). Any relationship between patient satisfaction or near visual function scores as measured by NAVQ and visual outcomes were assessed using the Pearson correlation test (Microsoft Excel V2601). A P value ≤0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 40 eyes from 22 patients were included for analysis; 18 patients received CNWTTx Toric IOLs bilaterally, while 4 patients received CNWTTx Toric IOLs in the eye included for analysis; 45% (18 eyes) received T2, 40% (16 eyes) received T3, 5% (2 eyes) received T4 and 10% (4 eyes) received T5 IOLs.
Rotational Stability
Actual rotation (mean ± SD) was −2.8 ± 5.6° at 1 hour, −1.1 ± 4.3° at 1 week, −1.3 ± 4.7° at 4–6 weeks and −1.3 ± 4.2° at 3 months (Figure 1A). The majority of the rotation was recorded within the first week after which it remained stable (Figure 1). Clockwise rotation was recorded in 60% of eyes, with 35% and 5% exhibiting anticlockwise rotation and no rotation, respectively. Rotation was ≤5° for 85% of eyes. There was no correlation between amount of IOL rotation and preoperative ACD (P = 0.92), AL (P = 0.58) or corneal cylinder (P = 0.73), or residual cylinder (P = 0.45).
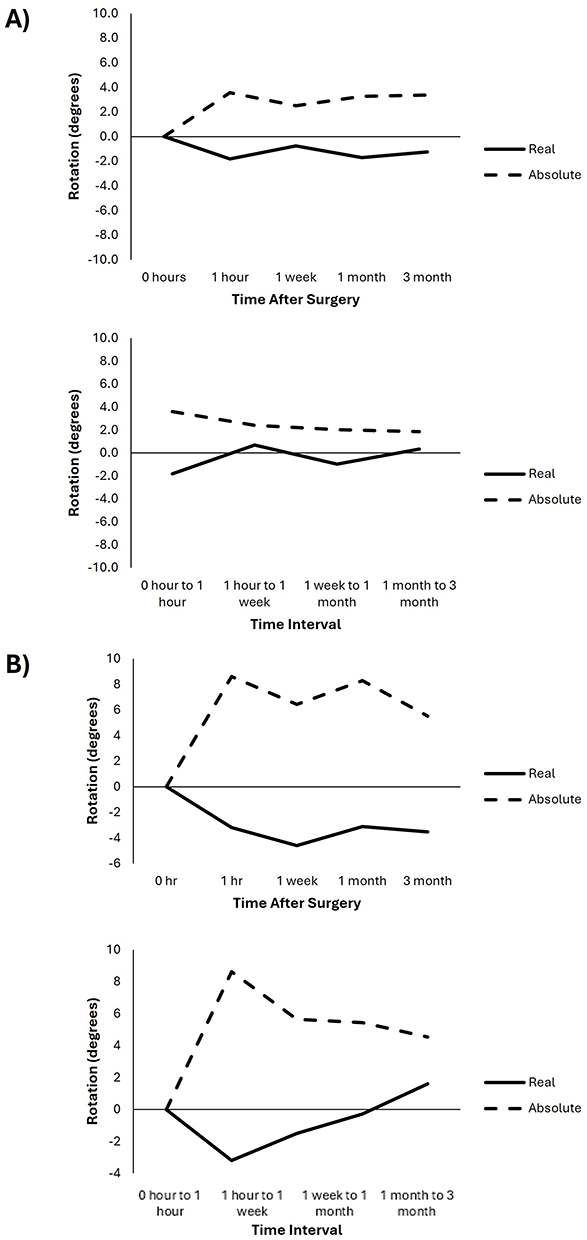 |
Figure 1 Refractive stability of the CNWTTx IOL as measured by real and absolute rotation from target axis at each time point and during each time interval measured using dilated slit-lamp examination (A) and ray tracing aberrometry (B). Abbreviation: IOL, intraocular lens. |
IOL rotation based on iTrace was −3.2 ± 12.1° at 1 hour (N = 21eyes), −4.6 ± 6.7° at 1 week (N = 23eyes), −3.1 ± 10.2° at 4–6 weeks (N = 24 eyes) and −3.5 ± 6.3° at 3 months (N = 21eyes) (Figure 1B). At 3 months, the difference between slit-lamp measurements versus iTrace was −2.0 ± 5.7°, with the data obtained by iTrace showing systematically greater rotation. Within the subset of 21 eyes, 62% of the eyes had IOL rotation within ±5° and 90.5% of the eyes within ±10° of that measured using slit-lamp examination.
Refraction and Visual Acuity
Mean MRSE was −0.15 ± 0.28 D at 3 months postoperative, with 92% of eyes achieving within ±0.5 of emmetropia (Figure 2A). Refractive astigmatism was −0.33 ± 0.25 D at 3 months postoperative, with 83% achieving −0.5 D or less, respectively (Figure 2B).
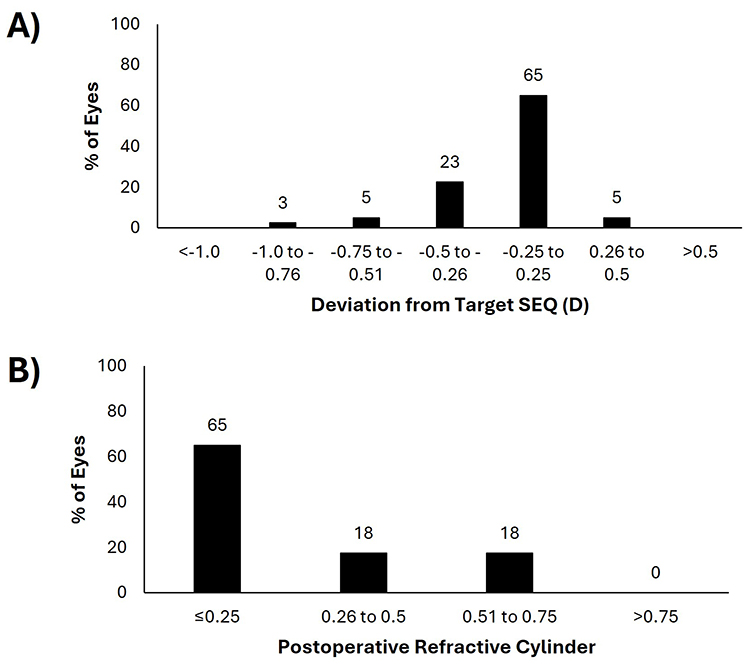 |
Figure 2 (A) Deviation from target SEQ and (B) postoperative refractive cylinder 3-months following implantation of the CNWTTx IOL. Abbreviations: D, dioptres; IOL, intraocular lens; SEQ, spherical equivalent. |
Postoperative monocular UDVA and BCVA at 3 months was LogMAR 0.06 ± 0.09 and LogMAR 0.00 ± 0.04 respectively (Table 1), with 85% and 100% achieving LogMAR 0.1 or better (Figure 3A). Monocular UIVA at 3 months was LogMAR 0.1 ± 0.14 with 73% of eyes achieving LogMAR 0.1 or better (Figure 3B). Intermediate vision did not change significantly with distance correction (P = 0.31). Monocular UNVA-40 and UNVA-33 at 3 months were LogMAR 0.13 ± 0.11 and 0.14 ± 0.11 respectively (Table 1), with 58% and 50% achieving LogMAR 0.1 or better (Figure 3C and D). UNVA-40 (P = 0.04) and UNVA-33 (P = 0.004) were both reduced with distance correction (Table 1).
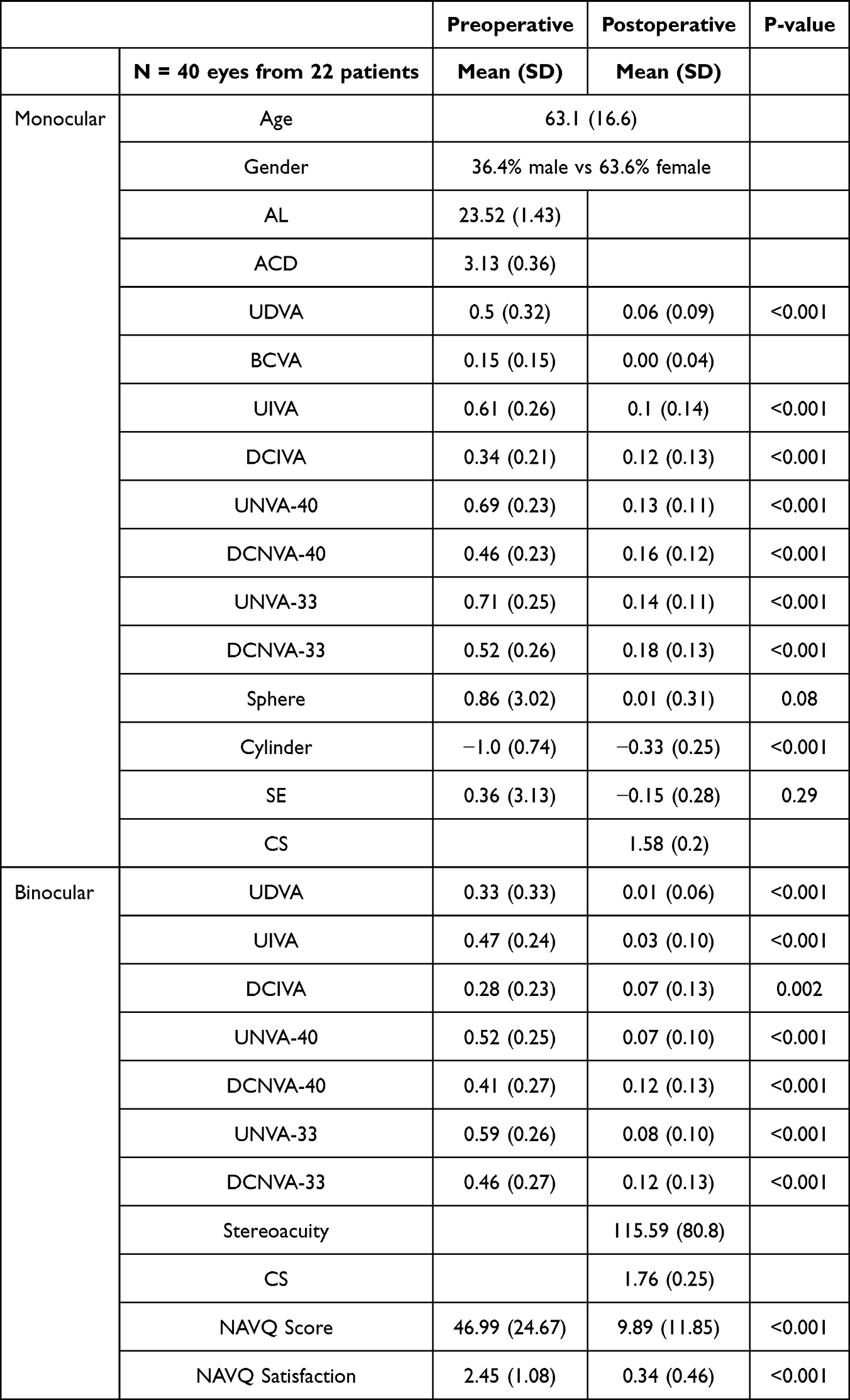 |
Table 1 Preoperative Demographics, and Pre- and Postoperative Visual and Refractive Outcomes at 3-Months Following Implantation of CNWTTx IOLs. IOL = Intraocular Lens |
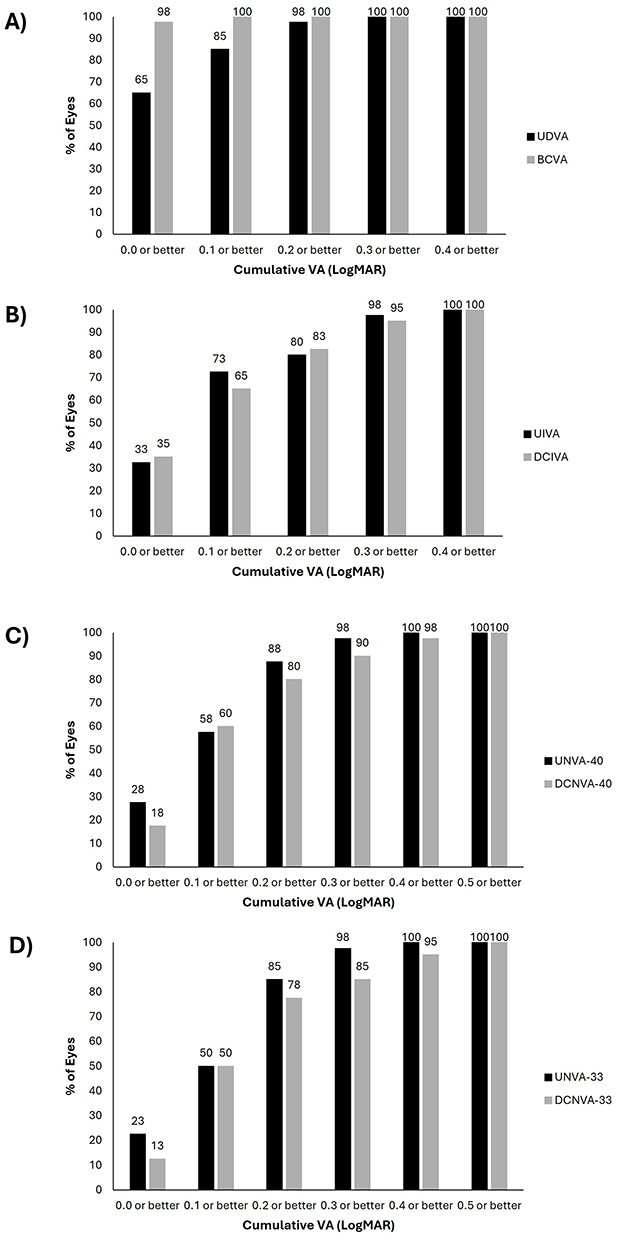 |
Figure 3 Cumulative uncorrected and distance-corrected visual acuity measured (A) monocularly at 6 meters, and binocularly at (B) 60 cm, (C) 40 cm and (D) 33 cm 3-months following implantation of the CNWTTx IOL. Abbreviations: BCVA, best-corrected distance visual acuity; DCIVA, distance-corrected intermediate visual acuity; DCNVA-40, distance-corrected near visual acuity measured at 40 cm; DCNVA-33, distance-corrected near visual acuity measured at 33 cm; IOL, intraocular lens; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA-40, uncorrected near visual acuity measured at 40 cm; UNVA-30, uncorrected near visual acuity measured at 33 cm; VA, visual acuity. |
Quality of Vision and Patient Reported Outcomes
At 3 months, stereoacuity was 115.59 ± 80.8 seconds of arc, and contrast sensitivity was 1.58 ± 0.2 and 1.76 ± 0.25, respectively, when measured monocularly and binocularly.
Both NAVQ score and satisfaction improved significantly following surgery (P < 0.001, Table 1). Overall, all patients reported to be either completely satisfied (best possible score of 0 on a scale of 0–4), or very satisfied (score of 1) with their vision following surgery. There was no significant correlation between NAVQ and visual outcomes (Supplementary Table 1). Patient-reported responses to individual NAVQ questions are described in Table 2; the highest level of difficulty was reported for “reading labels/instructions/ingredients/prices such as on: medicine bottles, food packaging”, and “seeing objects close to you in poor or dim light”. A total of 12 patients (ie. 55%) reported bothersome visual phenomena, and while degree of bothersomeness was not specifically assessed, no patients required IOL exchange.
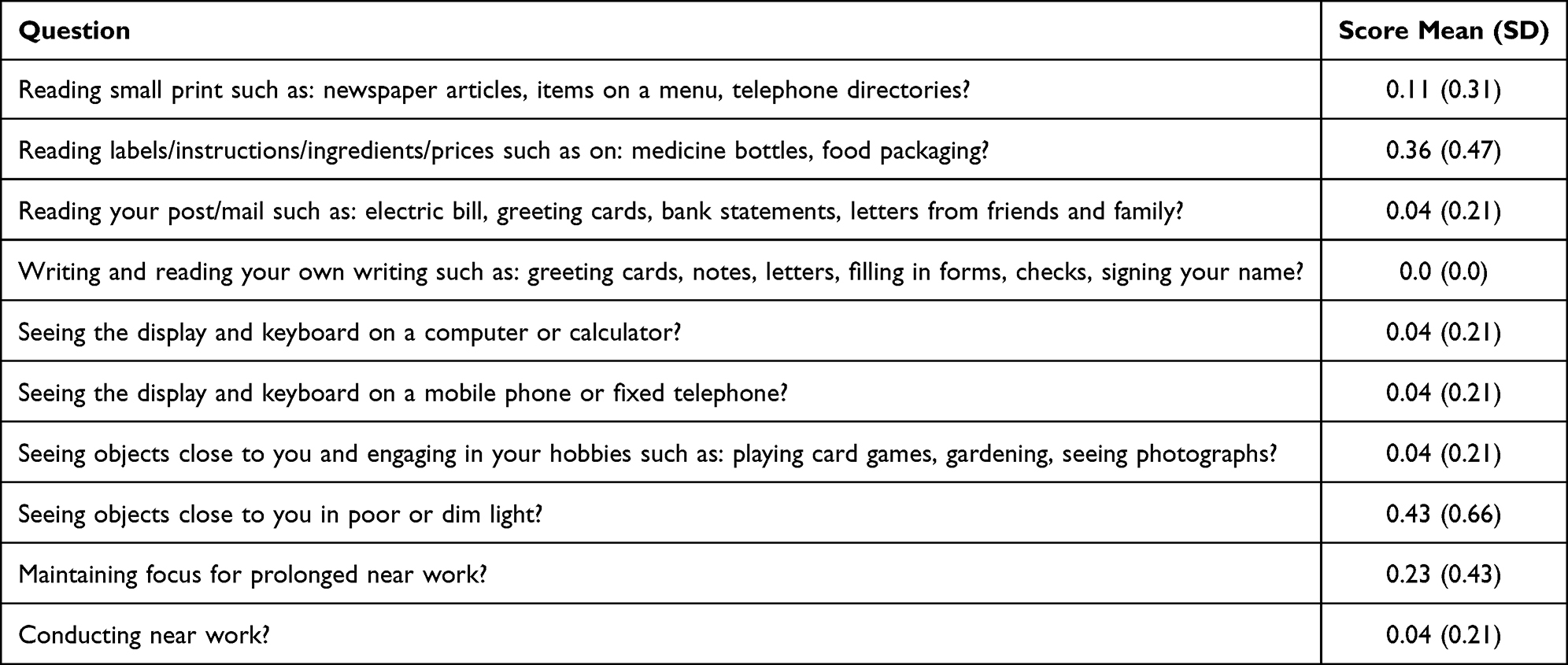 |
Table 2 Patient Reported Responses to NAVQ Questions Recorded at 3 Months Postoperative Following Implantation of CNWTTx IOLs. IOL = Intraocular Lens; NAVQ = Near Acuity Visual Questionnaire |
Discussion
This prospective, single-centre, non-comparative, real-world confirmatory study demonstrated clinical outcomes that are consistent with the existing evidence reported by Garzón et al (2025).21 The CNWTTx platform combines an updated cross-linked biomaterial with the proven optics, haptics, and geometry of the older TFNT00 model, which is widely recognised for its rotational stability.17,18 Although the CNA0T0 monofocal platform sharing this biomaterial has shown good stability with a mean absolute rotation of approximately 1°,19 data on the multifocal toric version (CNWTTx) has been limited to one single publication to date.21 As IOL materials can potentially alter early capsular adhesion and rotational dynamics, further evaluation of this updated platform in routine clinical practice was essential. Our findings demonstrated that this material update did not appear to compromise rotational stability and refractive reliability in a real-world clinical setting. However, it is important to note that this study did not include TFNT00 as a direct comparator, so there was no formal statistical analysis to establish superiority or non-inferiority. The clinical outcomes of this current study are therefore evaluated against previously published literature and the ANSI Z80.30 standard.3
Rotational stability of toric multifocal IOLs is particularly relevant, as visual outcomes have been shown to be more sensitive to rotation in situ compared to toric monofocal models.11,26 This current study found that CNWTTx Toric IOLs remained stable in situ over three months (actual rotation −1.3 ± 4.2°), with 85% rotating ≤5°, the threshold for what is believed to be clinically significant.3 While this is slightly below the 90% benchmark required by the ANSI Z80.30 standard, the 5% discrepancy is likely due to our small sample size. As our cohort was limited to 40 eyes, the difference between 85% and the 90% benchmark was attributed to IOL rotation >5° in two eyes. In a real-world clinical setting with diverse patient characteristics, this still represented an acceptable level of stability. Clinically, a 5° rotation results in a 16.7% loss of astigmatism correction, which leaves a small residual cylinder (typically 0.25 D or less) that may or may not impact visual quality. As a trifocal platform like the CNWTTx is typically more sensitive to uncorrected astigmatism than a monofocal platform, the potential impact of IOL rotation was further considered against the MRSE and patient satisfaction reported in our study. Since 92% of eyes were within ±0.5 D of target emmetropia and 100% of the patients reported to be completely or very satisfied with their vision, the fact that our cohort achieved 5% less eyes with ≤5° rotation vs. the ANSI Z80.30 standard was likely due to statistical reasons, rather than a true clinical deficiency of the CNWTTx IOL. Furthermore, for the 15% of eyes (6/40) that rotated more than 5°, no patients required surgical repositioning or an IOL exchange. In terms of the magnitude of IOL rotation, our results also compared favourably to what has been reported for other multifocal IOL models. A mean rotation of 3.53–4.02° at 3 months was reported for AT LISA toric 909M,27,28 and 1.59° was reported for CNWTT0 non-toric IOLs.9 To the author’s knowledge, only one paper has reported on the rotational stability of the CNWTTx Toric IOL to date which signifies the important gap this paper contributes to. Garzon et al21 reported a mean actual rotation of 1.08° and absolute rotation of 1.04° at 3 months following implantation of CNWTTx Toric IOLs, while the current data reports actual and absolute rotation of −1.3° and 3.4°, respectively. Interestingly, Garzon reported a mean actual rotation in an anticlockwise direction,21 while the majority of eyes in the current data rotated in a clockwise direction consistent with C-loop haptics. Variation in measured rotation may be due to differences in methodology. Garzon et al21 utilised image processing and the Position IntraOcular Lens Tracker (POILET) software to measure rotation while the current study utilized manual measurement of toric marking following dilated slit lamp examination and iTrace. These methods are more aligned with real-world data collection in the clinic, as both equipment are widely available and do not require purpose-built image-analysis software. However, a key limitation is the variability introduced due to patient positioning and cyclotorsion. For instance, high variation was seen with measurements taken at 1 hour and this may be attributed to the nerve block anesthetic used during surgery for some patients. IOL rotation data by iTrace was available for a subset of eyes only due to difficulty in identifying the toric markings on the IOL in situ, due to corneal reflection, poor patient fixation and tear film instability. Nevertheless, even after taking potential measurement variations from the slit lamp and incomplete iTrace dataset into consideration, it appears that the CNWTTx Toric IOL’s rotation in situ was not clinically significant and hence did not negatively impact visual outcomes.
This current study also found no relationship between amount of rotation and patient factors (ie. ACD and preoperative cylinder). Although this may be due to a relatively small sample size, it could also suggest that CNWTTx performs well for the standard general population. For future research, it may be beneficial to investigate the rotational stability of CNWTTx versus other available full range of focus toric IOLs in patients that may be more prone to IOL rotation eg. those with AL ≥26 mm and ACD >3.31 mm.
As for visual outcomes with the TFNT00 optical design, there is already abundant evidence in the literature that it achieves 20/25 or better in both corrected and uncorrected conditions across near, intermediate, and distance.13,17,29–33 More recently, specific data following CNWTT0 implantation has been reported by multiple research groups.34,35 The visual outcomes reported by Mendicute et al34 (ie. 0.07 LogMAR at 6 m, 0.01 LogMAR at 60 cm and 0.13 LogMAR at 40 cm) are similar to the current study, which also assessed visual outcomes at 33 cm, representing more visually demanding near tasks. It is interesting to note that uncorrected near visual acuity was maintained between this near range and achieved 0.13 LogMAR at 40 cm and 0.14 LogMAR at 33 cm. These visual acuity results are similar to what was reported by Garzon et al21 who included eyes with preoperative corneal astigmatism ranging from −1.5 to −4.19D. While UIVA and UNVA were not specifically reported, DCIVA (0.10 LogMAR) and DCNVA at 40 cm (0.13 LogMAR) were similar to what is reported in this current study (DCIVA LogMAR 0.12 and DCNVA LogMAR 0.16 at 40 cm). These good visual outcomes are consistent with accurate correction of both sphere and cylinder, (reported here as 92% and 83% achieving <0.5 D of SE and cylindrical error respectively) for this patient group (preoperative cylinder 0.25DC to 3.25DC). Mean postoperative SE was −0.15 D, consistent with the surgeon’s preference of the first minus SE target, which appears to be well tolerated as good UDVA was obtained. Notably, this study excluded eyes with a large CW chord mu (>0.5), minimising the risk of IOL decentration. While the current data suggests that the CNWTTx Toric IOL provides accurate visual and refractive outcomes in a real-world clinical cohort, further research including a larger and more diverse population may be beneficial to assess the IOL’s tolerance to decentration.
Quality of vision and patient reported outcomes in this study also reflected the aforementioned rotational stability and good visual acuity outcomes. All patients reported to be either “completely satisfied” or “very satisfied” postoperatively, with good near visual function based on NAVQ. Of those patients that reported to be very satisfied and who also recorded a NAVQ score >20 (ie. 5 patients), most experienced <5° of rotation and there was no apparent correlation with postoperative refractive error or visual acuity at any distance. Quality of vision was generally well maintained, with all but one patient achieving monocular CS ≥1.5 and stereoacuity better than or equal to 100 seconds of arc. Mean binocular mesopic CS (1.76 ± 0.25), was similar to the normative values for CS measured with Pelli-Robson for the healthy 60-year old population (1.68).36 While this current study did not utilise a validated questionnaire to assess visual disturbances, standardised interview questions with each participant were conducted to minimise participant burden. Of the 5 patients previously mentioned to have reported being “very satisfied”, 4 patients reported visual phenomena including ghosting, night-time glare and halos. This was a higher percentage when compared to patients who reported to be “completely satisfied” (80% versus 47%). Previous studies that have utilised validated questionnaires reported that patients struggled the most with night driving, computer tasks, reading the newspaper and performing handicrafts.21,35 Similarly, in the current study, patients reported having the most difficulty when reading small print on labels and reading under low light conditions. Diffractive multifocal optics are known to reduce the amount of usable light available to the retina, and therefore patient-reported difficulty in more visually demanding conditions is not unexpected and may be mitigated by preoperative counselling. There was no correlation between reports of difficulty with the overall NAVQ and satisfaction scores.
As this current study adopted methodologies more accessible in a clinical setting, limitations and variability do exist. Notably, toric IOL alignment was primarily measured using dilated slit lamp examination, and although this was exclusively done by a single experienced clinician, and consistent techniques and equipment, patient factors may have introduced variability during data collection. For example, the 1-hour measurements appeared to be impacted by the lingering effects of nerve block anaesthesia and cyclorotation. Furthermore, while patients were recruited bilaterally, inter-eye correlation was not accounted for due to the non-comparative, descriptive nature of the study. Further prospective cohort studies would benefit from adjusting for this potential source of error, or inclusion of monocular data only. The iTrace dataset also had its limitations due to incomplete data and scan quality issues, which the manufacturer recommends to mitigate by optimising the ocular surface, readjusting patient positioning, fixation, and ambient light.37 As this meant that iTrace data was only available for a subset of patients, in depth interpretation is limited and it may not reflect a larger sample group. For future investigations, it will be of value to understand how the semi-automated iTrace methodology compares with slit lamp examination and the image-based methods such as PIOLET.21 In order to comprehensively understand the accuracy and clinical usability of each method, one should ensure complete datasets are obtained, which will allow analysis of potential bias, level of agreement between methods, and their associated clinical significance.
In conclusion, this study contributes valuable real-world evidence to the currently limited literature on the CNWTTx platform, building upon the single prior clinical evaluation by Garzón et al (2025). Our findings confirm that the updated biomaterial provides rotational stability and predictable clinical outcomes in a real-world clinical setting. For eyes that lie at the outer limits of population norms, such as long AL (≥26 mm), deep ACD (>3.3 mm), or large chord mu (≥0.5 mm), further investigation is required to elucidate the IOL’s tolerance to rotation and decentration.
Data Sharing Statement
The authors do not wish to share the data included in this study due to patient privacy and confidentiality.
Ethics Approval
This study received ethics approval from the University of Wollongong Human Research Ethics Committee (2023/352) and was conducted according to the Tenets of the Declaration of Helsinki. Informed written consent was acquired from all participants prior to inclusion in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by an investigator-initiated grant from Alcon Laboratories (Australia) Pty Ltd. The funder had no involvement in the study design, analysis, interpretation of data, or the decision to submit the manuscript for publication.
Disclosure
This study recieved financial and material support from Alcon as an investigator initiated trial (#89159339). Dr Smita Agarwal reports receiving consulting fees as a member of the advisory committee at Alcon and honoraria for lectures and presentations given on behalf of Alcon and Zeiss. The authors report no other conflicts of interest in this work.
References
1. Shimizu KS, Misawa A, Suzuki Y. Toric intraocular lenses: correcting astigmatism while controlling axis shift. J Cataract Refract Surg. 1994;20:523–13. doi:10.1016/S0886-3350(13)80232-5
2. Felipe A, Artigas JM, Diez-Ajenjo A, Garcia-Domene C, Alcocer P. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg. 2011;37:1895–1901. doi:10.1016/j.jcrs.2011.04.036
3. American National Standards Institute. Ophthalmics - Toric Intraocular Lenses ANSI Z80.30-2010. New York, NY: ANSI; 2010.
4. Stanwood Till J, Yoder PR, Wilcox TK, Spielman JL. Toric intraocular lens implantation: 100 consecutive cases. J Cataract Refract Surg. 2002;28:295–301. doi:10.1016/S0886-3350(01)01035-5
5. Lin X, Ma D, Yang J. Insights into the rotational stability of toric intraocular lens implantation: diagnostic approaches, influencing factors and intervention strategies. Front Med. 2024;13:1349496. doi:10.3389/fmed.2024.1349496
6. Takaku R, Nakano S, Iida M, Oshika T. Influence of frosted haptics on rotational stability of toric intraocular lenses. Scientific Rep. 2021;11:15099. doi:10.1038/s41598-021-94293-3
7. Martin LR, Siedlecki D, Cabeza-Gil I, Calvo B. Influence of material and haptic design on the mechanical stability of intraoclar lenses by means of finite-element modeling. J Biomed Opt. 2018;23:035003.
8. Zheng Y, Chen Y, Gu X, et al. Evaluating the rotational stability of toric intraocular lenses with different haptic designs using finite element analysis. Exp Eye Res. 2026;264:110854. doi:10.1016/j.exer.2026.110854
9. Ribeiro F, Ferreira T. Comparison of visual and refractive outcomes of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2020;46:694–699. doi:10.1097/j.jcrs.0000000000000118
10. Nida Sen H, Sarikkola A, Uusitalo RJ, Laatikainen L. Quality of vision after AMO Array multifocal intraocular lens implantation. J Cataract Refract Surg. 2004;30:2483–2493. doi:10.1016/j.jcrs.2004.04.049
11. Ruiz-Alocer J, Martinez-Alberquilla I, Lorente-Velazques A, Alfonso JF, Madrid-Costa D. Effect of defocus combined with rotation on the optical performance of trifocal toric IOLs. Eur J Ophthalmol. 2022;32:249–254. doi:10.1177/11206721211002121
12. Goggin M. Toric intraocular lenses: evidence-based use. Clin Exp Ophthalmol. 2022;50:481–489. doi:10.1111/ceo.14106
13. Garcia-Perez JL, Gros-Otero J, Sanchez-Ramos C, Blazquez V, Contreras I. Short term visual outcomes of a new trifocal intraocular lens. BMC Ophthalmol. 2017;17:72. doi:10.1186/s12886-017-0462-y
14. Monaco G, Gari M, Di Censo F, Poscia A, Ruggi G, Scialdone A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43:737–747. doi:10.1016/j.jcrs.2017.03.037
15. Nicula CA, Popescu R, Rednik AM, Nicula D, Bulboaca AE, Stanescu I. Refractive lens exchange in hyperopic presbyopes with the AcrySof IQ PanOptix intraocular lens: one-year results and analysis of the literature. Ther Clin Risk Manag. 2020;16:1125–1137. doi:10.2147/TCRM.S279065
16. Maxwell A, Suryakumar R. Long-term effectiveness and safety of a three-piece acrylic hydrophobic intraocular lens modified with hydoxyethyl-methacrylate: an open-label, 3-year follow-up study. Clin Ophthalmol. 2018;12:2031. doi:10.2147/OPTH.S175060
17. Kohnen T, Marcini G, Alfonso JF, et al. Innovative trifocal (quadrifocal) presbyopia-correcting IOLs: 1-year outcomes from an international multicenter study. J Cataract Refract Surg. 2020;46:1142–1148. doi:10.1097/j.jcrs.0000000000000232
18. Mohaseb K, Tischler A, Hall B, et al. Refractive outcomes following bilateral implantation of a diffractive toric intraocular lens in a multisurgeon hospital setting. Can J Ophthalmol. 2024;59:e1–e6. doi:10.1016/j.jcjo.2022.11.001
19. LaHood B, Peterson RC. Real-world visual outcomes and rotational stability of a monofocal toric intraocular lens. Clin Ophthalmol. 2025;19:2945–2953. doi:10.2147/OPTH.S532933
20. Kramer BA, Hardten DR, Berdhal JP. Rotation characteristics of three toric monofocal intraocular lenses. Clin Ophthalmol. 2020;14:4379–4384. doi:10.2147/OPTH.S285818
21. Garzon N, Garcia-Bella J, Arriola-Villalobos P, Martinez-de-la-casa JM, Villanueva C, Garcia-Feijoo J. Rotational stability, centration and patient satisfaction outcomes with a trifocal toric intraocular lens. J Cataract Refract Surg. 2025;51:762–768. doi:10.1097/j.jcrs.0000000000001687
22. Montrimas A, Zemaitiene R, Yao K, Grzybowski A. Chord mu and chord alpha as postoperative predictors in multifocal intraocular lens implantation. Graefe’s Arch Clin Exp Ophthalmol. 2023;262:367–380. doi:10.1007/s00417-023-06098-x
23. Vale C, Menezes C, Firmino-Machado J, et al. Astigmatism management in cataract surgery with Precizon toric intraocular lens: a prospective study. Clin Ophthalmol. 2016;10:151–159. doi:10.2147/OPTH.S91298
24. Epitropoulos AT. Visual and refractive outcomes of a toric presbyopia-correcting intraocular lens. J Ophthalmol. 2016;2016:7458210. doi:10.1155/2016/7458210
25. Gundersen KG. Rotational stability and visual performance 3 months after bilateral implantation of a new toric extended range of vision intraocular lens. Clin Ophthalmol. 2018;12:1269–1278. doi:10.2147/OPTH.S173120
26. Garzon N, Poyales F, De Zarate BO, Ruiz-Garcia JL, Quiroga JA. Evaluation of rotation and visual outcomes after implantation of monofocal and multifocal toric intraocular lenses. J Refract Surg. 2015;31:90–97. doi:10.3928/1081597X-20150122-03
27. Shi R, Ma D, Zeng Q, et al. Rotational stability of monofocal and diffractive multifocal toric intraocular lens with identical design and material: a propensity score based prospective comparative study. BMC Ophthalmol. 2024;24:72. doi:10.1186/s12886-024-03281-4
28. Bai H, Sun J, Shi X, Li H, Wu X. Visual performance and rotational stability of a multifocal toric intraocular lens in myopic eyes. Graefe’s Arch Clin Exp Ophthalmol. 2023;261:2557–2565. doi:10.1007/s00417-023-06046-9
29. Alfonso JF, Fernandez-Vega-Cueto L, Fernandez-Vega L, Montes-Mico R. Visual function after implantation of a presbyopia-correcting trifocal intraocular lens. Ophthalmic Res. 2020;63:152–164. doi:10.1159/000500834
30. Alfonso JF, Fernandez-Vega-Cueto L, Alfonso-Bartolozzi B, Rodriguez-Una I, Montes-Mico R. Visual and refractive outcomes in hyperopic pseudophakic patients implanted with a trifocal intraocular lens. Clin Ophthalmol. 2019;13:2261–2268. doi:10.2147/OPTH.S229228
31. Alio JL, Plaza-Puche AB, Alio Del Barrio J, et al. Clinical outcomes with a diffractive trifocal intraocular lens. Eur J Ophthalmol. 2018;28:419–424. doi:10.1177/1120672118762231
32. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64:140–149. doi:10.1007/s10384-019-00712-4
33. Kim T, Chung T, Kim MJ, Lee K, Hyon JY. Visual outcomes and safety after bilateral implantation of a trifocal presbyopia correcting intraocular lens in a Korean population: a prospective single-arm study. BMC Ophthalmol. 2020;20:288. doi:10.1186/s12886-020-01549-z
34. Mendicute J, Lauzirika G, Illarramendi I, Martine-Soroa I. Visual, refractive, functional and patient satisfaction outcomes after implantation of a new trifocal diffractive intraocular lens. Clin Ophthalmol. 2024;18:27785. doi:10.2147/OPTH.S480311
35. Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. 2015;41:2330–2332. doi:10.1016/j.jcrs.2015.11.012
36. Mantyjarvi M, Laitinen T. Normal values for Pelli-Robson cs sensitivity test. J Cataract Refract Surg. 2001;27:261–266. doi:10.1016/S0886-3350(00)00562-9
37. Technologies T. Toric check. 2024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.