")
Back to Journals » Clinical Interventions in Aging » Volume 18
Role of Measurable Residual Disease in Older Adult Acute Myeloid Leukemia
Received 19 February 2023
Accepted for publication 25 May 2023
Published 7 June 2023 Volume 2023:18 Pages 921—931
DOI https://doi.org/10.2147/CIA.S409308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Xueyao Li, Xiuzhen Tong
Department of Hematology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
Correspondence: Xiuzhen Tong, Department of Hematology, The First Affiliated Hospital, Sun Yat-sen University, 58 Second Zhongshan Road, Guangzhou, CPZN 510080, People’s Republic of China, Email [email protected]
Abstract: There is overwhelming evidence indicating that the use of measurable residual disease (MRD) as a biomarker provides critical prognostic information and that MRD may have a role in directing postremission decisions. There are a variety of assays for MRD assessment, such as multiparameter flow cytometry and molecular assessment of MRD, which present different characteristics in patients older than 60 years of age. Due to multiple reasons related to age, the progress of older adult AML patients is rarely investigated, especially with respect to MRD. In this review, we will clarify the characteristics of different assays for assessing MRD, focusing on its role as a risk-stratification biomarker to predict prognostic information and its role in optimal postremission therapy among older adult AML patients. These characteristics also provide guidance regarding the potential to apply personalized medicine in older adult AML patients.
Keywords: detection method, risk-stratification marker, postremission decisions, personalized medicine
Introduction
Acute myeloid leukemia (AML) can be diagnosed at any age but mainly presents in older adult patients, with a median age at diagnosis of 68 years.1 Although the prognosis of younger AML patients has improved over the past few years, the treatment of older adult patients remains challenging.2 The 5-year survival rate is 35%~40% for patients who are younger than 60 years and 5%~15% for patients who are older than 60 years; this difference is attributed to the higher incidence of unfavorable cytogenetics, higher expression of multidrug resistance, higher relapse rate, and lower ability to tolerate intensive chemotherapy, even in those who achieved complete remission (CR) in older adult patients.3,4 Even the tiniest remnants in older adult AML patients may lead to relapse, and each relapse may be associated with a decreased probability of long-term survival. Accordingly, eradication of even the posttreatment remnants of disease may be necessary to evaluate the long-term survival rate or even cure AML in older adult patients.
Herein, we focus on measurable residual disease (MRD) in older adult patients over 60 years of age. Currently, the most commonly used therapeutic assessment is CR, which is based on morphological assessment and was established decades ago. Due to its limited sensitivity and interobserver variability, bone marrow morphological assessment alone insufficient for discriminating the relapse rate.5 Therefore, the role of MRD in the AML landscape is gradually being taken seriously, as it can act as a powerful risk-stratification marker to assess the quality of response and to optimize postremission decisions.6
However, the role of MRD in older adults is rarely investigated because they are not being referred for intensive therapy and are excluded from clinical trials because of comorbidities, frailty, or other reasons. Thanks to hypomethylating agents (HAMs), low-intensity therapy (eg, low-dose cytarabine or HMAs plus BCL-2 inhibitors) has attracted attention, which has increased the possibility of achieving an MRD-negative CR for older adult patients and access to disease-specific therapy.6–10 This type of therapy also provides an opportunity to systematically measure patient-specific factors, particularly low-intensity therapy and MRD status posttherapy, thus facilitating the discrimination of favorable, intermediate and adverse patients for proper port-remission therapy.
The proper detection method for older adult AML patients still needs to be explored. Currently, several techniques are commonly used to assess MRD, such as multiparameter flow cytometry (MFC), real-time quantitative polymerase chain reaction (RT‒qPCR), droplet digital polymerase chain reaction (ddPCR), and next-generation sequencing (NGS). Each of these technologies differs in AML among older adults, and these methods vary in their sensitivity and applicability.11 There is an urgent need for a more objective, sensitive, and specific assessment of MRD to develop more individualized treatment.
In this review, we aimed to evaluate the applicability of MRD assessment in AML patients aged over 60 years, investigate the value of MRD in risk stratification and optimize postremission therapy.
MRD Detection in Older Adult AML Patients
Assessment of MRD allows for the detection and quantification of lower levels of residual leukemia cells, which can be detected by immunophenotype/molecular assessment and provide a relapse risk assessment for individual patients independently from other risk factors.11–14 The two most widely used techniques for MRD assessment are MFC and RT‒qPCR; newer technologies, such as ddPCR and NGS, vary in their sensitivity and applicability.15 Nevertheless, aging denotes different immunophenotypes and changing genetic markers, and their prognostic association also differs compared to younger AML patients (Table 1). Therefore, whether MRD assessment has a comparable effect in younger and older adult patients remains to be explored.
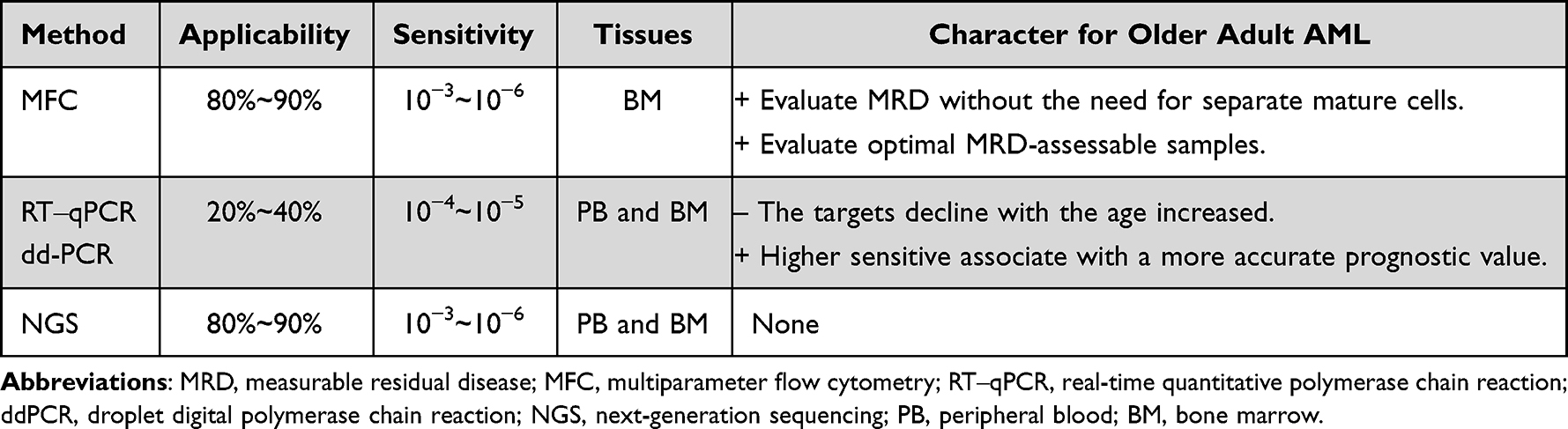 |
Table 1 Different Characteristics of MRD Techniques |
Multiparameter Flow Cytometry for MRD
Multiparameter flow cytometry (MFC) is currently the most commonly used assay to assess MRD in the majority of patients after a chemotherapy-induced morphologic CR, even for patients older than 60 years.16 MFC includes the methods of tracking leukemia-associated immunophenotypes (LAIP) and the “difference from normal” (DfN) analysis,17 and it is also available by integrating these methods, which is suggested by the European LeukemiaNet (ELN) MRD working party.11
In older adult AML patients, flow cytometric MRD detection has some particular advantages. First, aging is associated with the accumulation of mutations in mature cells. During targeted therapy-induced maturation, the presence of mature cells may be a particular issue for genetic MRD monitoring during targeted therapy performed on whole bone marrow (BM).18–20 Unlike molecular assays of MRD detection, immunophenotyping by flow cytometry permits MRD evaluation in the BM/peripheral blood for predicting relapse without the need for separate mature cells. Second, older patients are more likely to have samples that cannot be assessed for MRD; in such cases, flow cytometry could provide an estimate of BM hemodilution to evaluate which samples are suboptimal.6
Although some studies have shown that this technique is limited in BM with age-related increases, MFC-based MRD detection is still applicable for older adults with AML. Freeman et al first investigated the clinical significance of MFC-MRD in older adults with AML with nonacute promyelocytic leukemia. Their findings indicated that older adult AML patients in CR (morphology blasts<5%) but with immunophenotypic blasts (≥5%) observed by MFC after one or two courses had a poor overall survival (OS), which was not significantly different from older AML patients who were refractory according to morphology after one course (P=0.16). In contrast, patients with more than 5% blasts by morphology but MRD negativity after one course of remission had a much better 3-year OS than patients who were MRD positive with/without morphological refractoriness. The study provided evidence that MFC-based MRD detection is also useful in older adult AML patients.16
Molecular Techniques for MRD
Molecular techniques for MRD assessment rely on the detection of abnormal leukemia-related genes in nucleic acids, which can provide higher sensitivity and specificity than MFC. We applied molecular MRD with two objectives. First, the achievement of complete molecular remission at the end of therapy has begun to act as a therapeutic objective and prerequisite for a cure, indicating that it will likely inform therapeutic decisions.11,21 Second, due to high sensitivity, molecular progression and molecular relapse could be detected in advance of morphological relapse, thus permitting preemptive therapeutic intervention and improving the long-term outcome.11 (Table 2).
 |
Table 2 Biomarkers for MRD Assessment |
As a tool for molecular assessment, RT‒qPCR can be used to monitor genomic alterations by amplifying complementary DNA (cDNA), which is reverse transcribed by RNA from patient samples, through quantitative PCR. However, appropriate and validated targets, such as PML-RARA in acute promyelocytic leukemia (APL), CBF-AMMHC and RUNX1-RUNX1T1 in core-binding factor (CBF) AML, and recurrent mutations in NPM1, are present in less than 50% of AML patients, and with increasing age at diagnosis, these AML subtypes decline substantially.29–31 To overcome this limitation, markers that are highly expressed in leukemic blasts have been used to track MRD, such as WT1 and EVI1 mRNA transcripts. Several studies have used these transcripts as MRD markers and evaluated them over the course of treatment.32–34
NGS technology, which has a similar principle to PCR, can target multiple genes or the entire genome at once. Depending on the platform to detect MRD and the amount of input DNA, the sensitivity of NGC can reach 10−6, which makes it an attractive choice for every sensitive MRD detection. In a study of 201 patients (ages ranging from 18~63 years) treated with conventional therapy in morphological CR, NGS-based MRD detection identified over 80% of cases identified by MFC at the end of induction, whereas MFC identified 43.9% of cases that were identified by NGS, which demonstrated that NGS-based MRD detection is clinically informative and synergistic when combined with MFC.35 Compared to younger patients, older patients are likely to carry specific mutation genes, including TET2, RUNX1, ASXL1 and SRSF2,22,36–39 and have a trend of a higher trend of sAML with adverse genetic mutations.
In the context of MRD assessment, error-corrected NGS (EC-NGS) was newly developed for highly sensitive point mutation detection and can analyze multiple mutations in a single patient sample.11 However, the measurement of NGS is under development and not ready for routine application in the clinic.40–42
However, these molecular techniques to detect MRD in older adult AML patients present a problem: in a majority of older adult AML patients, there are no validated molecular markers of MRD,43 and the majority of studies on the prognostic value of molecular MRD status generally examine younger adults. Therefore, it is hard to apply the prognostic value to older patients. For instance, older adult AML patients with t(9;11) have worse disease-free survival, whereas younger patients with t(9;11) have a longer disease-free survival (DFS).44 Additionally, DNMT3A mutations coexisting with the combined NPM1/FLT3-ITD genotype in younger patients were associated with significantly shorter OS but not among older/intermediate cytogenetic risk patients.45 Similarly, the prognostic value of RUNX1 mutations also depends on age, which is associated with longer OS in younger patients but not in older patients.45 In light of this, more attention should be focused on these questions in the field of molecular MRD in older adult AML patients, and based on these particular mutations, individual therapy of these populations will hopefully be raised by researchers.
The Role of MRD in Older Adult AML Patients
Patients who are eligible for intensive chemotherapy only have a median OS of 5 years, and patients treated with nonintensive chemotherapy only have a median OS of 7–13 months.46–48 Therefore, the “one size fits all” therapy regimen cannot reflect the high immunology and molecular type of older adult AML, and there is an urgent need for well-tolerated and individualized therapy for older patients. Applicant MRD after different therapy cycles may reflect the resistance factors of all diagnosis and postdiagnosis previously, and its assessments could be helpful for guiding treatment in theory and recognizing which patients are candidates for hematopoietic stem cell transplantation (HSCT).31 Because of the heterogeneity of AML and the complexity of MRD assessment, the clinical application for AML is still doubtful. If MRD can be applied in the clinic, it can be used to redefine risk groups and guide treatment strategies.27 (Figure 1, Table 3).
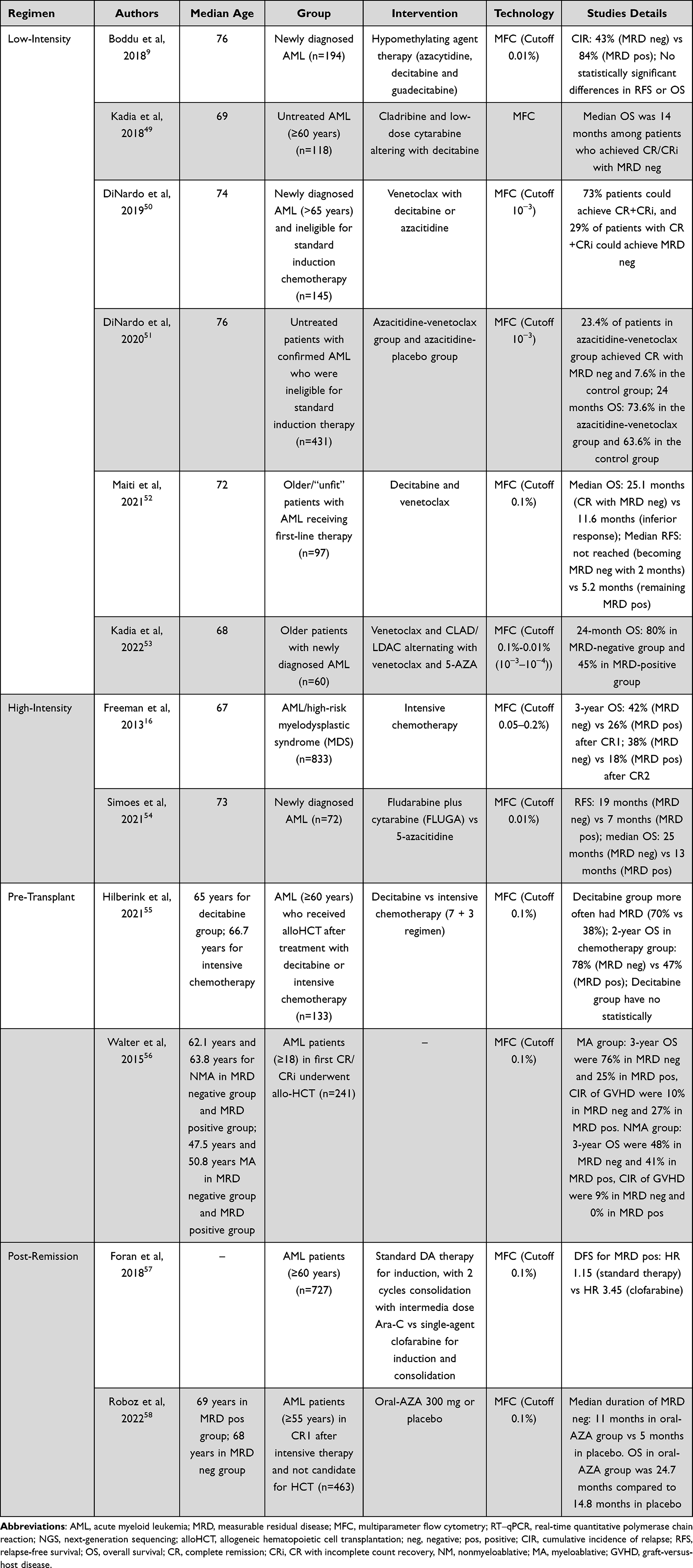 |
Table 3 Previous Studies of MRD in Older Adult AML |
 |
Figure 1 Summary of MRD in older adult AML patients. Characteristics of MRD in different treatment phases, and the most frequent uses of MRD are risk stratification prior to consolidation therapy and optimization of postremission therapy (consolidation chemotherapy). |
MRD in Low Intensity
Compared with younger AML patients (<60 years), older AML patients have distinct clinical characteristics: they more commonly exhibit the expression of unfavorable cytogenetics and multidrug resistance, they have a more frequent incidence of secondary AML (MDS-related AML or therapy for other malignancies), and they have greater treatment-related toxicity.2,3,59 For these reasons, low-intensity therapy (low-dose cytarabine or HMAs plus BCL-2 inhibitors) in older adult AML patients has gained attention, which may help to achieve a CR with MRD negativity. DiNardo et al investigated the efficiency of venetoclax combined with decitabine or azacitidine in older adult AML patients.50 The results showed that this low-intensity regimen in older adult AML patients could achieve high CR+CR with an incomplete count recovery (CRi) rate of 73%, and 29% of patients with CR+CRi could achieve MRD-negative status at least once during research. At a median follow-up of 15.1 months, the median duration of response and OS were not reached. This study demonstrated a promising result and a tolerable safety profile.
In subsequent research, DiNardo et al compared the efficacy of the azacitidine-venetoclax group and the azacitidine-placebo group in patients who were ineligible for standard therapy.51 The research found that proportion of patients with MRD-negative status who achieved CR was 23.4% in the azacitidine-venetoclax group and in 7.6% in the control group, and the OS rate at 24 months was 73.6% and 63.6% in the azacitidine-venetoclax group and control group, respectively. The results showed that MRD-negative status could be helpful to show the efficiency of azacitidine plus venetoclax. This evidence suggests that this therapy regimen would obtain higher MRD-negative status and increase survival, which may be a promising key in the future in this challenging population.
To further improve the outcomes of older adult AML and evaluate the efficiency of MRD-negative status. Kadia et al conducted a clinical trial of cladribine and low-dose cytarabine altered with decitabine for older adult AML.49 Among the 118 patients, 52 patients achieved CR/CRi after cycle 1, and 27 (52%) of these patients achieved MRD-negative status. Twenty-six patients achieved CR/CRi after cycle 2, and 13 (50%) of these patients were MRD-negative. In brief, 68% of patients achieved CR/CRi, and over half of these patients achieved MRD-negative status, with a median OS of 14 months, which proved that this regimen can be viewed as an available therapy for older or unfit AML patients.
Based on the above research, Kadia et al investigated the combination of venetoclax to cladribine +low-dose cytarabine alternating with 5-azacitidine in patients older than 60 years with newly diagnosed AML.53 The results showed that the CR+CRi rate was 93%, and 84% of patients could achieve MRD-negative status. The 24-month OS was 80% in the MRD-negative group and 45% in the MRD-positive group. The median DFS in the MRD-negative group was not reached (with a median follow-up of 22.1 months), while it was only 5.9 months in MRD-positive patients. This result could also provide warranted evidence for low-intensity therapy as the front-line therapy for older adult AML patients.
Similarly, a recent study conducted by Maiti et al also analyzed the prognostic value of MRD evaluated by MFC in older adult AML patients receiving 10-day decitabine and venetoclax.52 The median time to MRD-negative status was 2 months. Compared with patients who remained MRD positive, those who became MRD-negative within 2 months had a longer event-free survival (EFS) and OS; the median EFS was not reached vs 5.8 months, and the median OS was 25.1 vs 7.1 months. Furthermore, patients who became MRD-negative within 1 month had an 85% reduction in the risk of death (median OS, 25.1 vs 3.4 months). After achieving a response, 16 patients underwent SCT, and relapse occurred in 1 out of 10 patients who were MRD negative before SCT vs 2 out of 5 patients who were MRD positive (1 patient was not valuable for MRD negative). The result also indicates that MRD status with outcomes in older adult AML appears to be a useful prognostic tool.
MRD in High Intensity
Older adult AML patients are always thought to be unfit for intensive therapy because of fatal comorbidities, frailty, or other reasons. However, some studies have investigated intensive therapy for older adults and evaluated MRD.
Freeman et al evaluated whether MFC-based MRD detection could provide prognostic value in patients older than 60 years old who received intensive chemotherapy (daunorubicin with Ara-C or daunorubicin with clofarabine).16 The results showed that MRD-negative status was achieved in 51% of patients after CR1 and 64% of patients after CR2. Compared to MRD-positive status, MRD-negative status in CR1/CR2 conferred a significantly better 3-year survival (CR1: 42% vs 26%; CR2: 38% vs 18%; P<0.001) and reduced relapse rate (CR1: 71% vs 83%; CR2: 79% vs 91%; P<0.01). Furthermore, the median time to relapse was 17.1 months in the MRD-negative group and 8.5 months in the MRD-positive group. This result provides evidence that MRD could be a powerful prognostic predictor in older adult AML, which could lead to refinement of MRD-based risk stratification and provide information in this challenging group.
However, unlike intensive therapy and low-intensity therapy, the value of MRD has rarely been investigated in semi-intensive therapy. In the PETHEMA-FLUGAZA Phase 3 clinical trial, Simoes et al investigated the role of MRD in older adult AML patients treated with fludarabine plus cytarabine (FLUGA) vs AZA.54 Compared to patients with persistent MRD after induction, MRD-negative patients had significantly longer OS (median OS, 25 months vs 13 months, P=0.03) and relapse-free survival (RFS) (median RFS, 19 months vs 7 months, P=0.005). The research also showed that the CR/CRi rate was 33% in the FLUGA group vs 23% in the HMA group, but the quality of CR/CRi measured by MRD was similar (MRD-negative status was 14% in the HMA group vs 23% in the FLUGA group, P=0.54). Among patients with persistent MRD, relapse-free survival (RFS) was significantly longer in the AZA group (median RFS, 6 months vs 3 months, P=0.003). This study proved that CR with MRD-negative status could supersede morphological CR and act as an independent prognostic factor in older adult AML patients who received semi-intensive chemotherapy or AZA.
MRD Pretransplant
For multiple reasons, older adult patients are always excluded from the landscape of AML, and MRD-tailored HSCT has rarely been investigated. Walter et al showed the significance of MRD status at all ages (median age 43.1 years) before myeloablative allogeneic HSCT (allo-HSCT) for AML in CR1 and CR2. The 3-year OS was 73% for pretransplant MRD-negative patients in CR1, 32% for pretransplant MRD-positive patients in CR1, 73% for pretransplant MRD-negative patients in CR2 and 44% for pretransplant MRD-positive patients in CR2. Similarly, the relapse rate was 21% for pretransplant MRD-negative patients in CR1, 58% for pretransplant MRD-positive patients in CR1, 19% for pretransplant MRD-negative patients in CR2 and 68% for pretransplant MRD-positive patients in CR2. Interestingly, among the pretransplant MRD-negative patients, there was no statistical evidence that the increasing level of MRD was associated with an increased risk of OS, DFS, relapse or nonrelapse mortality. Based on the available data above, it is conceivable that MRD status – rather than the number of remissions – is the primary pre-HCT factor associated with relapse risk and outcome post-HCT.60
A retrospective study investigated the efficiency of decitabine versus conventional chemotherapy (7+3 regimen) in older adult AML patients who received allo-HSCT.55 Hilberink et al found that the pretransplantation MRD status in patients who received decitabine does not have similar prognostic value in older adult patients who received allo-HSCT. Although patients in the decitabine group had a more frequent MRD-positive status than those in the conventional chemotherapy group (70% vs 38%), there was no significant association between the MRD status and relapse (sHR 0.85; P=0.83) or death (HR 0.72; P=0.60) rate in the decitabine group, but the MRD-positive status in the chemotherapy group was still related to a higher relapse (sHR 4.81; P=0.0031) or death rate (HR 2.8; P=0.02). Because of different mechanisms of action, as well as dynamics of response between HMAs and conventional chemotherapy,61 the evaluation of survival benefit of HMAs is not limited to morphologic CR.9 From the above experiment, we conclude that it remains unclear whether MRD status could measure the survival benefits and predict prognosis in older adult AML patients treated with HAMs.
MRD as Post Remission Therapy Including Post Transplant
Foran et al evaluated the MRD status at the time of CR and investigated the impact on postremission treatment strategies.57 Patients were randomized to receive standard DA therapy for induction, with 2 cycles consolidation with intermediate-dose Ara-C, or single-agent clofarabine for induction and 2 cycles consolidation. The results indicate that MRD-negative patients had superior results regardless of the postremission therapy used. However, MRD-positive patients in CR/CRi who received clofarabine consolidation had inferior results compared to those who received standard chemotherapy. This discovery suggests that intermediate Ara-C may eliminate the adverse effects of MRD in older adult patients with CR/CRi and indicates that MRD status at the time of remission could be used to guide optimal postremission strategies in older adult AML.
Roboz et al conducted a randomized, phase 3 QUAZAR AML-001 trial (NCT01757535) evaluating oral azacitidine (Oral-AZA) in patients older than 55 years old with AML in first CR/CRi after intensive chemotherapy (induction with/without consolidation) who were not candidates for HSCT. The median time from randomization to first achievement of MRD negativity approximately corresponded to 56 days within baseline and day 1 of cycle 3 (28 d/cycle), and the median total duration of MRD negativity status was 11 months in the oral-AZA group and 5 months in the placebo group. Patients who were MRD negative at baseline had a longer duration of MRD negative status in the oral-AZA group (median 26.4 months vs 10.4 in placebo).
Compared to placebo, regardless of whether patients had postintensive chemotherapy MRD at study entry, both OS and RFS were significantly improved in the Oral-AZA group (OS, 24.7 months vs 14.8 months; RFS, 10.2 months vs 4.8 months).58,62 Furthermore, oral-AZA could also prolong the duration of MRD negative status by 6 months and contributed to a higher rate conversion of MRD+ to MRD- during the treatment (37% vs 19% in placebo).58 Overall, the data in QUAZRA AML-001 showed that MFC-based MRD analyses could provide powerful prognostic values and help physicians determine the postremission status.
For older adult AML patients undergoing HSCT, MRD could also provide powerful prognostic value. Walter et al used MRD to compare the outcomes of patients in first CR undergoing myeloablative or nonmyeloablative HSCT.56 MRD-negative patients in both groups had a longer 3-year OS and DFS. Among myeloablative HCT patients, the 3-year OS was 76% in the MRD-negative group and 25% in the MRD-positive group, and the DFS rates were 71% and 13%, respectively. Among nonmyeloablative HCT patients, the 3-year OS rates were 48% and 41%, respectively, and the DFS rates were 42% and 33%, respectively.
For acute and chronic graft-versus-host disease (GVHD), there was a considerable difference in the 100-day cumulative incidence of relapse (CIR) of GVHD. For myeloablative HCT patients, the CIRs of GVHD were 10% and 27% for the MRD-negative and MRD-positive groups, respectively, and 9% and 0% for the MRD-negative and MRD-positive groups in nonmyeloablative HSCT patients, respectively. The authors provide powerful evidence that the presence of MRD at the time of HSCT is associated with worse post-HSCT results and show the prognostic value of MRD posttransplantation.
Therefore, MRD assessment should be given more attention in the progress of therapy in older adult AML in future research, where MRD response could serve as a powerful risk-stratification marker and direct the following therapeutic regimen.
However, MRD negativity in older adult patients might indicate different therapeutic strategies than in younger patients.63 In younger patients, an MRD-positive status is the main criterion for accepting HSCT,14,64 while an MRD-negative status indicates that HSCT could be postponed to avoid possible transplant-related toxicity in the population that is likely to be cured.65 In older adult patients, an MRD-negative status might represent a “green light” of an aggressive or continuing treatment, such as immune therapy, clinical trials of maintenance or reduced intensity conditioning ASCT.66 Whether achieving an MRD-negative status in older adult patients might help physicians direct treatment remains unclear.
Conclusion
In summary, MRD detected by MFC or molecular techniques (PCR or NGS) is a powerful risk-stratification biomarker that is able to distinguish patients into subgroups with dramatically differing prognoses and for sequential monitoring and optimization of postremission decisions. The development of molecular MRD may prompt physicians to design personalized therapy aimed at achieving and maintaining an MRD-negative CR while minimizing treatment toxicity.6 However, it remains unclear how to optimally develop novel therapies for various older adult AML patients, which can act for a fixed duration and eradicate MRD, and how to improve the long-term survival of older adults. The outcomes of older adult patients treated with conventional strategies have not improved significantly in the last few years, but the application of MRD in older adult AML patients is promising to improve outcomes and quality of life.
Acknowledgments
This work was supported by Guangdong Basic and Applied Basic Research Foundation (NO.2019A1515010294) to TX.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jemal A, Tiwari R, Murray T, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004;54(1):8–29. doi:10.3322/canjclin.54.1.8
2. Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia. Blood. 2006;107(9):3481–3485. doi:10.1182/blood-2005-09-3724
3. Dohner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453–474. doi:10.1182/blood-2009-07-235358
4. Kantarjian H, Ravandi F, O’Brien S, et al. Intensive chemotherapy does not benefit most older patients (age 70 years or older) with acute myeloid leukemia. Blood. 2010;116(22):4422–4429. doi:10.1182/blood-2010-03-276485
5. Short N, Ravandi F. How close are we to incorporating measurable residual disease into clinical practice for acute myeloid leukemia? Haematologica. 2019;104(8):1532–1541. doi:10.3324/haematol.2018.208454
6. Buccisano F, Dillon R, Freeman SD, Venditti A. Role of minimal (measurable) residual disease assessment in older patients with acute myeloid leukemia. Cancers. 2018;10(7):215. doi:10.3390/cancers10070215
7. Gale RP, Hochhaus A. Therapy of older persons with acute myeloid leukemia. Leukemia. 2015;29(4):759. doi:10.1038/leu.2014.337
8. McClune BL, Weisdorf DJ, Pedersen TL, et al. Effect of age on outcome of reduced-intensity hematopoietic cell transplantation for older patients with acute myeloid leukemia in first complete remission or with myelodysplastic syndrome. J Clin Oncol. 2010;28(11):1878–1887. doi:10.1200/JCO.2009.25.4821
9. Boddu P, Jorgensen J, Kantarjian H, et al. Achievement of a negative minimal residual disease state after hypomethylating agent therapy in older patients with AML reduces the risk of relapse. Leukemia. 2018;32(1):241–244. doi:10.1038/leu.2017.285
10. Foran J. Frontline therapy of AML: should the older patient be treated differently?. Curr Hematol Malig Rep. 2014;9(2):100–108. doi:10.1007/s11899-014-0211-8
11. Schuurhuis GJ, Heuser M, Freeman S, et al. Minimal/measurable residual disease in AML: a consensus document from the European LeukemiaNet MRD working party. Blood. 2018;131(12):1275–1291. doi:10.1182/blood-2017-09-801498
12. Hourigan C, Karp J. Minimal residual disease in acute myeloid leukaemia. Nat Rev Clin Oncol. 2013;10(8):460–471. doi:10.1038/nrclinonc.2013.100
13. Hokland P, Ommen H. Towards individualized follow-up in adult acute myeloid leukemia in remission. Blood. 2011;117(9):2577–2584. doi:10.1182/blood-2010-09-303685
14. Buccisano F, Maurillo L, Del Principe M, et al. Prognostic and therapeutic implications of minimal residual disease detection in acute myeloid leukemia. Blood. 2012;119(2):332–341. doi:10.1182/blood-2011-08-363291
15. Fuda F, Chen W. Minimal/measurable residual disease detection in acute leukemias by multiparameter flow cytometry. Curr Hematol Malig Rep. 2018;13(6):455–466. doi:10.1007/s11899-018-0479-1
16. Freeman S, Virgo P, Couzens S, et al. Prognostic relevance of treatment response measured by flow cytometric residual disease detection in older patients with acute myeloid leukemia. J Clin Oncol. 2013;31(32):4123–4131. doi:10.1200/jco.2013.49.1753
17. Ravandi F, Walter R, Freeman S. Evaluating measurable residual disease in acute myeloid leukemia. Blood Adv. 2018;2(11):1356–1366. doi:10.1182/bloodadvances.2018016378
18. Zink F, Stacey SN, Norddahl GL, et al. Clonal hematopoiesis, with and without candidate driver mutations, is common in the elderly. Blood. 2017;130(6):742–752. doi:10.1182/blood-2017-02-769869
19. Corces-Zimmerman MR, Majeti R. Pre-leukemic evolution of hematopoietic stem cells: the importance of early mutations in leukemogenesis. Leukemia. 2014;28(12):2276–2282. doi:10.1038/leu.2014.211
20. Amatangelo MD, Quek L, Shih A, et al. Enasidenib induces acute myeloid leukemia cell differentiation to promote clinical response. Blood. 2017;130(6):732–741. doi:10.1182/blood-2017-04-779447
21. Dohner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
22. Genovese G, Kahler AK, Handsaker RE, et al. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. New Engl J Med. 2014;371(26):2477–2487. doi:10.1056/NEJMoa1409405
23. Schnittger S, Kern W, Tschulik C, et al. Minimal residual disease levels assessed by NPM1 mutation-specific RQ-PCR provide important prognostic information in AML. Blood. 2009;114(11):2220–2231. doi:10.1182/blood-2009-03-213389
24. Pratcorona M, Brunet S, Nomdedeu J, et al. Favorable outcome of patients with acute myeloid leukemia harboring a low-allelic burden FLT3-ITD mutation and concomitant NPM1 mutation: relevance to post-remission therapy. Blood. 2013;121(14):2734–2738. doi:10.1182/blood-2012-06-431122
25. Ostronoff F, Othus M, Lazenby M, Estey E, Appelbaum FR. Prognostic significance of NPM1 mutations in the absence of FLT3-internal tandem duplication in older patients with acute myeloid leukemia: a SWOG and UK national cancer research institute/medical research council report. J Clin Oncol. 2015;33(15):1715. doi:10.1200/Jco.2015.62.4288
26. Prebet T, Boissel N, Reutenauer S, et al. Acute myeloid leukemia with translocation (8;21) or inversion (16) in elderly patients treated with conventional chemotherapy: a collaborative study of the French CBF-AML intergroup. J Clin Oncol. 2009;27(28):4747–4753. doi:10.1200/JCO.2008.21.0674
27. Ossenkoppele G, Schuurhuis G. MRD in AML: does it already guide therapy decision-making? Hematology Am Soc Hematol Educ Program. 2016;2016(1):356–365. doi:10.1182/asheducation-2016.1.356
28. Nomdedéu J, Hoyos M, Carricondo M, et al. Bone marrow WT1 levels at diagnosis, post-induction and post-intensification in adult de novo AML. Leukemia. 2013;27(11):2157–2164. doi:10.1038/leu.2013.111
29. Short N, Rytting M, Cortes J. Acute myeloid leukaemia. Lancet. 2018;392(10147):593–606. doi:10.1016/s0140-6736(18)31041-9
30. Prassek VV, Rothenberg-Thurley M, Sauerland MC, et al. Genetics of acute myeloid leukemia in the elderly: mutation spectrum and clinical impact in intensively treated patients aged 75 years or older. Haematologica. 2018;103(11):1853–1861. doi:10.3324/haematol.2018.191536
31. Aitken M, Ravandi F, Patel K, Short N. Prognostic and therapeutic implications of measurable residual disease in acute myeloid leukemia. J Hematol Oncol. 2021;14(1):137. doi:10.1186/s13045-021-01148-5
32. Smol T, Nibourel O, Marceau-Renaut A, et al. Quantification of EVI1 transcript levels in acute myeloid leukemia by RT-qPCR analysis: a study by the ALFA Group. Leuk Res. 2015;39(12):1443–1447. doi:10.1016/j.leukres.2015.09.021
33. Cilloni D, Renneville A, Hermitte F, et al. Real-time quantitative polymerase chain reaction detection of minimal residual disease by standardized WT1 assay to enhance risk stratification in acute myeloid leukemia: a European LeukemiaNet study. J Clin Oncol. 2009;27(31):5195–5201. doi:10.1200/Jco.2009.22.4865
34. Gianfaldoni G, Mannelli F, Ponziani V, et al. Early reduction of WT1 transcripts during induction chemotherapy predicts for longer disease free and overall survival in acute myeloid leukemia. Haematol Hematol J. 2010;95(5):833–836. doi:10.3324/haematol.2009.011908
35. Patkar N, Kakirde C, Shaikh AF, et al. Clinical impact of panel-based error-corrected next generation sequencing versus flow cytometry to detect measurable residual disease (MRD) in acute myeloid leukemia (AML). Leukemia. 2021;35(5):1392–1404. doi:10.1038/s41375-021-01131-6
36. Metzeler KH, Becker H, Maharry K, et al. ASXL1 mutations identify a high-risk subgroup of older patients with primary cytogenetically normal AML within the ELN favorable genetic category. Blood. 2011;118(26):6920–6929. doi:10.1182/blood-2011-08-368225
37. Mendler JH, Maharry K, Radmacher MD, et al. RUNX1 mutations are associated with poor outcome in younger and older patients with cytogenetically normal acute myeloid leukemia and with distinct gene and MicroRNA expression signatures. J Clin Oncol. 2012;30(25):3109–3118. doi:10.1200/JCO.2011.40.6652
38. Gaidzik VI, Paschka P, Spath D, et al. TET2 mutations in acute myeloid leukemia (AML): results from a comprehensive genetic and clinical analysis of the AML study group. J Clin Oncol. 2012;30(12):1350–1357. doi:10.1200/JCO.2011.39.2886
39. Rucker FG, Schlenk RF, Bullinger L, et al. TP53 alterations in acute myeloid leukemia with complex karyotype correlate with specific copy number alterations, monosomal karyotype, and dismal outcome. Blood. 2012;119(9):2114–2121. doi:10.1182/blood-2011-08-375758
40. Young AL, Wong TN, Hughes AE, et al. Quantifying ultra-rare pre-leukemic clones via targeted error-corrected sequencing. Leukemia. 2015;29(7):1608–1611. doi:10.1038/leu.2015.17
41. Hiatt JB, Pritchard CC, Salipante SJ, O’Roak BJ, Shendure J. Single molecule molecular inversion probes for targeted, high-accuracy detection of low-frequency variation. Genome Res. 2013;23(5):843–854. doi:10.1101/gr.147686.112
42. Schmitt MW, Kennedy SR, Salk JJ, Fox EJ, Hiatt JB, Loeb LA. Detection of ultra-rare mutations by next-generation sequencing. Proc Natl Acad Sci U S A. 2012;109(36):14508–14513. doi:10.1073/pnas.1208715109
43. Grimwade D, Freeman SD. Defining minimal residual disease in acute myeloid leukemia: which platforms are ready for “prime time”? Blood. 2014;124(23):3345–3355. doi:10.1182/blood-2014-05-577593
44. Mrozek K, Marcucci G, Nicolet D, et al. Prognostic significance of the European LeukemiaNet standardized system for reporting cytogenetic and molecular alterations in adults with acute myeloid leukemia. J Clin Oncol. 2012;30(36):4515–4523. doi:10.1200/Jco.2012.43.4738
45. Metzeler KH, Herold T, Rothenberg-Thurley M, et al. Spectrum and prognostic relevance of driver gene mutations in acute myeloid leukemia. Blood. 2016;128(5):686–698. doi:10.1182/blood-2016-01-693879
46. Dombret H, Seymour JF, Butrym A, et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291–299. doi:10.1182/blood-2015-01-621664
47. Kantarjian HM, Thomas XG, Dmoszynska A, et al. Multicenter, randomized, open-label, phase III trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J Clin Oncol. 2012;30(21):2670–2677. doi:10.1200/jco.2011.38.9429
48. Schuh AC, Dohner H, Pleyer L, Seymour JF, Fenaux P, Dombret H. Azacitidine in adult patients with acute myeloid leukemia. Crit Rev Oncol Hematol. 2017;116:159–177. doi:10.1016/j.critrevonc.2017.05.010
49. Kadia TM, Cortes J, Ravandi F, et al. Cladribine and low-dose cytarabine alternating with decitabine as front-line therapy for elderly patients with acute myeloid leukaemia: a Phase 2 single-arm trial. Lancet Haematol. 2018;5(9):e411–e421. doi:10.1016/S2352-3026(18)30132-7
50. DiNardo CD, Pratz K, Pullarkat V, et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 2019;133(1):7–17. doi:10.1182/blood-2018-08-868752
51. DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. New Engl J Med. 2020;383(7):617–629. doi:10.1056/NEJMoa2012971
52. Maiti A, DiNardo C, Wang S, et al. Prognostic value of measurable residual disease after venetoclax and decitabine in acute myeloid leukemia. Blood Adv. 2021;5(7):1876–1883. doi:10.1182/bloodadvances.2020003717
53. Kadia TM, Reville PK, Wang X, et al. Phase II study of venetoclax added to cladribine plus low-dose cytarabine alternating with 5-azacitidine in older patients with newly diagnosed acute myeloid leukemia. J Clin Oncol. 2022;40(33):3848–3857. doi:10.1200/JCO.21.02823
54. Simoes C, Paiva B, Martinez-Cuadron D, et al. Measurable residual disease in elderly acute myeloid leukemia: results from the PETHEMA-FLUGAZA phase 3 clinical trial. Blood Adv. 2021;5(3):760–770. doi:10.1182/bloodadvances.2020003195
55. Hilberink JR, Morsink LM, van der Velden W, et al. Pretransplantation MRD in older patients with AML after treatment with decitabine or conventional chemotherapy. Transplant Cell Ther. 2021;27(3):246–252. doi:10.1016/j.jtct.2020.12.014
56. Walter RB, Gyurkocza B, Storer BE, et al. Comparison of minimal residual disease as outcome predictor for AML patients in first complete remission undergoing myeloablative or nonmyeloablative allogeneic hematopoietic cell transplantation. Leukemia. 2015;29(1):137–144. doi:10.1038/leu.2014.173
57. Foran JM, Sun ZX, Paietta E, et al. Minimal Residual Disease (MRD) at time of complete remission is commonly detected in Acute Myeloid Leukemia (AML) patients age ≥ 60 years and significantly impacts outcome based on post-remission treatment strategies: prospective analysis of ECOG-ACRIN (E-A) E2906 phase III trial. Blood. 2018;132. doi:10.1182/blood-2018-99-113950
58. Roboz GJ, Ravandi F, Wei AH, et al. Oral azacitidine prolongs survival of patients with AML in remission independently of measurable residual disease status. Blood. 2022;139(14):2145–2155. doi:10.1182/blood.2021013404
59. Oliai C, Schiller G. How to address second and therapy-related acute myelogenous leukaemia. Br J Haematol. 2020;188(1):116–128. doi:10.1111/bjh.16354
60. Walter R, Buckley S, Pagel J, et al. Significance of minimal residual disease before myeloablative allogeneic hematopoietic cell transplantation for AML in first and second complete remission. Blood. 2013;122(10):1813–1821. doi:10.1182/blood-2013-06-506725
61. Kharfan-Dabaja M. Guadecitabine for AML and MDS: hype or hope? Lancet Oncol. 2015;16(9):1009–1011. doi:10.1016/s1470-2045(15)00095-9
62. Wei A, Döhner H, Pocock C, et al. Oral azacitidine maintenance therapy for acute myeloid leukemia in first remission. N Engl J Med. 2020;383(26):2526–2537. doi:10.1056/NEJMoa2004444
63. Buccisano F, Maurillo L, Piciocchi A, et al. Minimal residual disease negativity in elderly patients with acute myeloid leukemia may indicate different postremission strategies than in younger patients. Ann Hematol. 2015;94(8):1319–1326. doi:10.1007/s00277-015-2364-5
64. Cornelissen J, Gratwohl A, Schlenk R, et al. The European LeukemiaNet AML working party consensus statement on allogeneic HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol. 2012;9(10):579–590. doi:10.1038/nrclinonc.2012.150
65. Appelbaum FR. Incorporating hematopoietic cell transplantation (HCT) into the management of adults aged under 60 years with acute myeloid leukemia (AML). Best Pract Res Clin Haematol. 2008;21(1):85–92. doi:10.1016/j.beha.2007.11.013
66. Ustun C, Lazarus H, Weisdorf D. To transplant or not: a dilemma for treatment of elderly AML patients in the twenty-first century. Bone Marrow Transplant. 2013;48(12):1497–1505. doi:10.1038/bmt.2013.67
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.