")
Back to Journals » Clinical Ophthalmology » Volume 18
Role of Intravitreal Dexamethasone Implant in the Management of Treatment-Naive Diabetic Macular Edema: A Pre-Cataract Surgical Approach for Patients with Systemic Contraindications to Anti-VEGF Therapy
Authors Chakraborty S , Ganguly S, Sheth JU
Received 10 November 2023
Accepted for publication 17 January 2024
Published 23 January 2024 Volume 2024:18 Pages 227—233
DOI https://doi.org/10.2147/OPTH.S449250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Somnath Chakraborty,1 Santanu Ganguly,2 Jay Umed Sheth3
1Department of Vitreoretinal Services, Retina Institute of Bengal, Siliguri, India; 2Department of Anterior Segment Services, Retina Institute of Bengal, Siliguri, India; 3Department of Vitreoretinal Services, Shantilal Shanghvi Eye Institute, Mumbai, MH, India
Correspondence: Somnath Chakraborty, Department of Vitreoretinal Services, Retina Institute of Bengal, Siliguri, India, Email [email protected]
Purpose: Diabetic macular edema (DME) is a significant cause of vision impairment, posing challenges in its management due to variable responses and patient diversity. While anti-vascular endothelial growth factor (anti-VEGF) agents have revolutionized DME treatment, some patients are not suitable candidates for this therapy. Intravitreal corticosteroid therapy, such as the dexamethasone implant (DEX), has emerged as an alternative. This study aimed to comprehensively investigate the role of intravitreal DEX in treatment-naive DME patients with systemic contraindications to anti-VEGF therapy, administered one month before cataract surgery.
Patients and Methods: A single-center retrospective study included 20 eyes with controlled diabetes, visually significant cataracts, untreated DME, and systemic contraindications for anti-VEGF therapy. Patients underwent DEX treatment followed by cataract surgery after one month. Best-corrected visual acuity (BCVA), central macular thickness (CMT), and intraocular pressure (IOP) were assessed at multiple time points.
Results: BCVA significantly improved on days 30, 90, and 180 post-DEX (P< 0.00001). CMT showed a significant decrease at day 30 (P< 0.00001), which was sustained through days 90 and 180 (P< 0.00001). Recurrent DME was observed in 25% of eyes on day 90. IOP increased significantly at days 30 (P< 0.00001) and 90 (P=0.0006), returning to baseline by day 180. However, only two eyes needed topical anti-glaucoma treatment. No other ocular or systemic adverse events were noted.
Conclusion: Intravitreal DEX administered one month before cataract surgery offers a promising treatment strategy for treatment-naive DME patients with systemic contraindications to anti-VEGF therapy. The study’s findings provide insights into improving visual acuity and reducing macular thickness, along with manageable IOP changes. This personalized approach is a valuable addition to DME management, especially for complex medical cases, warranting further research and consideration for clinical practice.
Keywords: diabetic macular edema, dexamethasone implant, Ozurdex
Introduction
Diabetic macular edema (DME) is a leading cause of vision impairment and blindness in individuals with diabetes, affecting their quality of life and imposing a significant economic burden on healthcare systems.1,2 Despite significant advancements in ophthalmology, it continues to pose a substantial clinical challenge due to its variable response to treatment and the diverse clinical profiles of patients affected by this condition. Historically, laser photocoagulation was the primary treatment for DME, but advancements in pharmacological therapies have since transformed its management.2 Chief among these innovations is the introduction of anti-vascular endothelial growth factor (anti-VEGF) agents, which have revolutionized DME treatment.3 However, not all patients are suitable candidates for or experience favorable responses to anti-VEGF therapy. Systemic contraindications, safety concerns, and individual patient variations contribute to the complexity of DME management.3–5 In such cases, alternative therapeutic strategies are warranted to address the unmet needs of these patients.
Intravitreal corticosteroid therapy, such as the dexamethasone implant, has emerged as a promising alternative for the management of DME, particularly in cases where anti-VEGF therapy is contraindicated or has proven to be ineffective.3 OZURDEX® (Allergan, Inc., Irvine, CA, USA) is a biodegradable dexamethasone implant, inserted into the vitreous cavity using a customized single-use applicator system. It gradually releases the 0.7 mg dexamethasone dose over 6 months.6–8 It is approved by the US Food and Drug Administration (US-FDA) for the treatment of uveitis, macular edema in retinal vein occlusion, and diabetic macular edema.9 These DEX implants offer the advantages of a sustained-release profile, allowing for less frequent intravitreal injections and potentially improving patient compliance.6,7,9
Patients with DME often experience concomitant cataract formation, necessitating cataract surgery.10 This dual challenge of cataract and macular edema presents a unique opportunity for optimizing patient care. At present, there is no established therapeutic protocol that is universally accepted that can improve the results of cataract removal in individuals with diabetes who also have DME. Combined cataract surgery with intravitreal anti-VEGF/steroid therapy has been suggested in some research, but others have recommended intravitreal therapy prior to cataract surgery.10–12 Kabanarou et al10 treated 17 patients of recalcitrant DME with the DEX implant who subsequently underwent cataract surgery after one month. The authors demonstrated improvement in vision and macular thickness lasting three months post-cataract surgery.10
The purpose of this study was to comprehensively investigate the role of intravitreal DEX as a therapeutic strategy for treatment-naive DME patients with systemic contraindications to anti-VEGF therapy when administered one month prior to cataract surgery. The focus on this specific patient population is driven by the recognition that these individuals often represent a medically complex and underserved group, with limited therapeutic options. By studying the outcomes, safety profile, and effectiveness of DEX in this context, we aim to contribute to the evolving understanding of DME management. Administering the DEX before surgery for cataracts is a strategy to optimize DME management by possibly lowering the inflammation response after surgery while concurrently addressing the macular edema.
Materials and Methods
This was a single-center, retrospective study performed at a tertiary eye care center in India between December 2021 to April 2023. The study was undertaken in accordance with the tenets established in the Declaration of Helsinki, and it was approved for conduct by the Institutional Review Board of the Retina Institute of Bengal in Siliguri, India. Informed written consent for the intravitreal therapy and the cataract surgery was obtained from all the patients.
Design
The inclusion criteria for the study were: controlled diabetics with age ≥ 18 years, glycated hemoglobin ≤ 8%, presence of clinically significant cataract along with untreated diabetic macular edema, and a systemic contraindication for intravitreal anti-VEGF therapy. The exclusion criteria were: history of ocular hypertension/glaucoma, any prior ocular surgery/ intravitreal therapy/ laser photocoagulation, or any other retinal pathology other than diabetic retinopathy (DR).
At baseline, all patients underwent intravitreal DEX under topical anesthesia in the operating room, under strict aseptic precautions. One month later, all of them underwent uncomplicated phacoemulsification cataract surgery with a posterior chamber intraocular lens (PCIOL) by a single experienced surgeon (SG). The patients were reviewed on days 1, 7, 30, 90, and 180 post-DEX. The following practices were performed at all visits: best-corrected visual acuity (BCVA) assessment using Snellen’s visual acuity chart, intraocular pressure (IOP) measurement using a Goldmann applanation tonometer, detailed anterior and dilated posterior segment evaluation, and spectral-domain optical coherence tomography (SD-OCT). Repeat DEX injection/laser photocoagulation was provided at the discretion of the physician on a pro-re-nata basis.
Outcome Measures
The primary outcome measure of the study was the change in BCVA and central macular thickness (CMT) on days 30, 90, and 180 from the baseline. Increases in intraocular pressure (IOP) and the occurrence of any other adverse events were recorded as safety outcomes.
Statistical Analysis
The statistical analysis was performed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). Data were presented as mean and mean ± Standard deviation (SD) for continuous variables. The Paired t-test was used to assess the changes in the BCVA, CMT, and IOP from the baseline. P values < 0.05 indicated statistical significance.
Results
Twenty eyes of 20 patients were included in the study. The average age of the participants in the study was 57.2 (± 5.47) years. A majority of the participants were male (75%). Based on the early treatment of diabetic retinopathy study (ETDRS) criteria, 75% of the eyes had moderate non-proliferative DR (NPDR), 15% had severe NPDR, and 10% had proliferative diabetic retinopathy (PDR).
Among 20 study patients with a systemic limitation to anti-VEGF therapy, a marginally higher proportion had a history of myocardial infarction (MI; 55%), while the remainder had a history of stroke (45%) within the previous three months. Table 1 provides the demographic details of the study population.
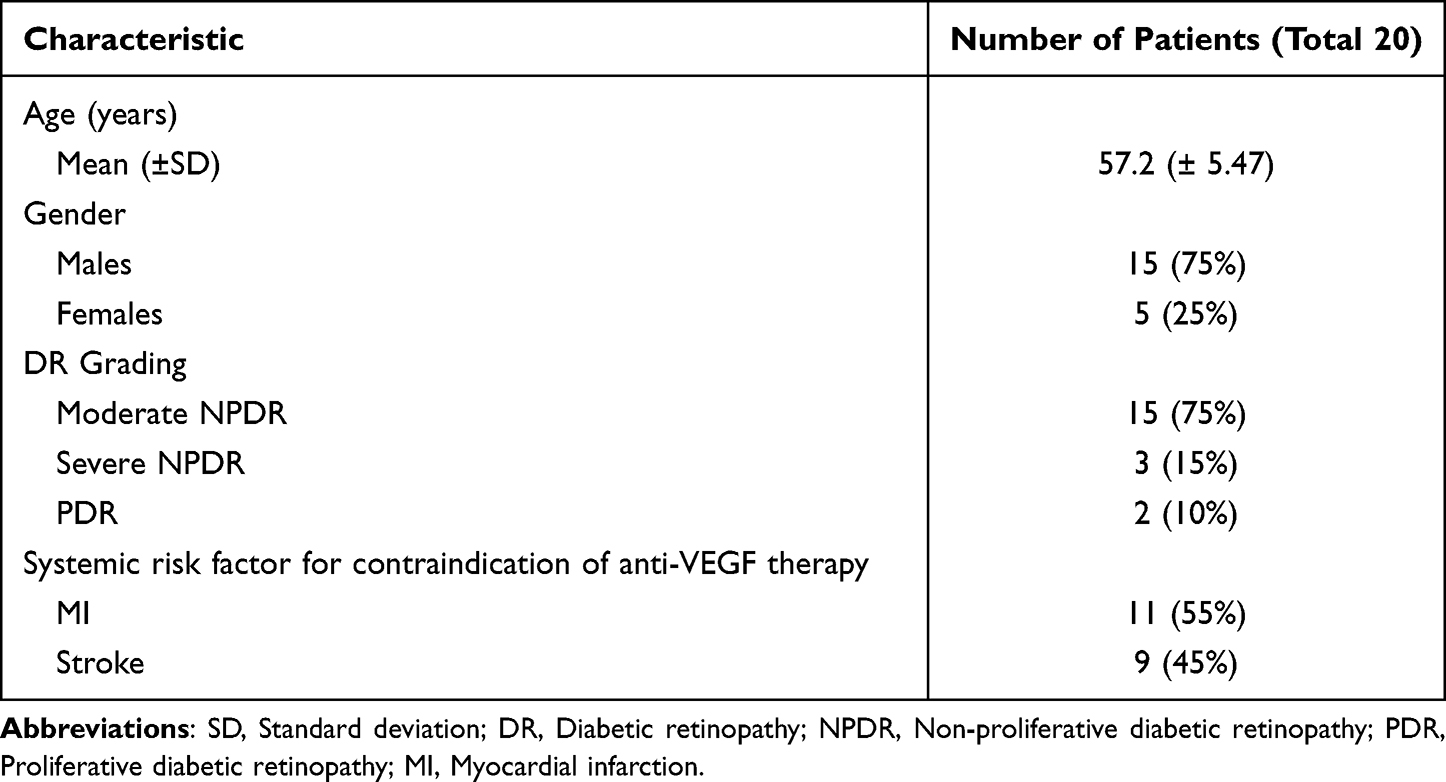 |
Table 1 Demographic Characteristics of the Study Population |
Best-Corrected Visual Acuity Outcomes
At baseline, the mean BCVA was 0.74 (± 0.26) logMAR. Following administration of DEX treatment, there was a significant improvement in visual acuity observed at days 30 (mean logMAR BCVA: 0.33 [± 0.2]; P<0.00001), 90 (mean logMAR BCVA: 0.3 [± 0.23]; P<0.00001), and 180 (mean logMAR BCVA: 0.19 [± 0.18]; P<0.00001), respectively (Figure 1).
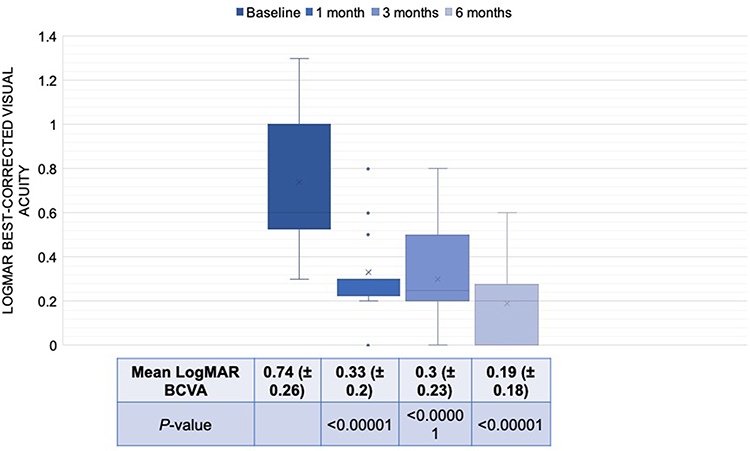 |
Figure 1 Box plots representing the changes in the best-corrected visual acuity (BCVA) after intravitreal Ozurdex therapy over 180 days. |
Central Macular Thickness Outcomes
The mean CMT of the study eyes at baseline was 422 (± 50.68) µm. A significant decrease in retinal thickness was detected at day 30 (mean CMT: 288.7 [(± 30.93] µm; P<0.00001), and this reduction persisted at day 90 (mean CMT: 301.55 [(± 56.52] µm; P<0.00001) and day 180 (mean CMT: 271.3 [(± 16.17] µm; P<0.00001) respectively (Figure 2).
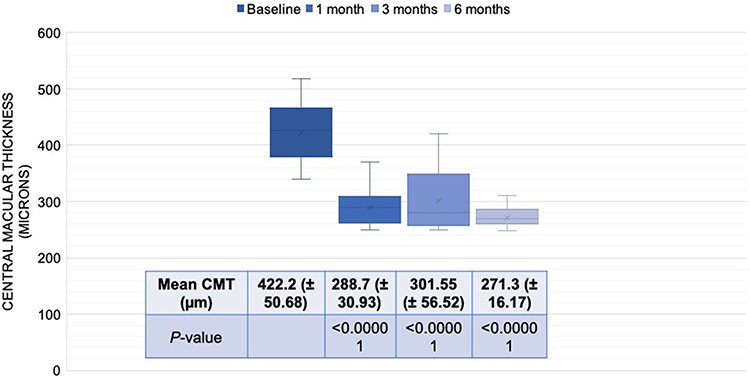 |
Figure 2 Box plots representing the changes in the central macular thickness (CMT) after intravitreal Ozurdex therapy over 180 days. |
Additional Treatment
Three eyes (15%) underwent pan-retinal photocoagulation (PRP) on day 60. Of these three eyes, two had PDR at baseline, and the third went on to develop PDR from severe NPDR at baseline. A total of five eyes (25%) developed a recurrence of DME at the 90-day mark and subsequently received a second administration of DEX implant.
Safety Analysis
The mean IOP at baseline was 17.1 (± 2.69) mmHg. After the DEX therapy, the mean IOP increased significantly to 20.3 (± 2.68) mmHg on day 30 (P<0.00001) (Figure 3). Of the 20 eyes, nine (45%) had an IOP of more than 21 mmHg, however, none was higher than 30 mmHg. Only two eyes (10%) needed treatment with a topical anti-glaucoma drug (AGM). On day 60, the mean IOP continued to be significantly elevated (19.3 [± 2.92] mmHg; P=0.0006) (Figure 3), with four eyes having IOP > 21 mmHg and none reporting IOP > 30 mmHg. The mean IOP reverted to baseline levels on day 180 (17.95 [± 3.02] mmHg; P=0.12), with no significant difference (Figure 3). At the end of the 180-day study period, none of the participant’s eyes required an AGM or surgery for elevated IOP. No additional ocular or systemic adverse events were reported during the duration of the study.
 |
Figure 3 Box plots representing the changes in the intraocular pressure (IOP) after intravitreal Ozurdex therapy over 180 days. |
Discussion
In the current study, the authors aimed to evaluate the use of intravitreal DEX implant as a therapeutic strategy for patients with treatment-naive DME who have systemic contraindications to anti-VEGF medication. The findings of the study demonstrate notable improvement in both visual acuity and macular thickness up to the 180th day. In the safety analysis, only a temporary increase in IOP was observed on day 30, which recovered to normal by day 180, with only two eyes requiring topical anti-glaucoma drugs.
Improvements in BCVA represent a critical outcome, as they signify a positive impact on patient’s vision, which is a primary concern for patients with DME. The improvements observed at day 30 persisted throughout the study. It is noteworthy that despite the presence of cataract on the 30th day, the patients demonstrated a significant improvement in visual acuity. The findings are unanticipated, although they demonstrate a high level of efficacy attributed to DEX in individuals with visually severe cataracts. In a comparable study conducted by Kabanarou et al,10 the researchers failed to observe any significant visual benefit one month after the administration of DEX. Nevertheless, there was significant improvement in vision following the cataract operation. A possible rationale for this occurrence may be attributed to the varying patient characteristics between both studies. Particularly, prior research exclusively examined those with recalcitrant DME, whereas those who participated in the current study were previously untreated. Additionally, the sustained improvement in BCVA noted in our study is particularly significant because it indicates the potential for prolonged therapeutic benefits, reducing the need for frequent interventions and improving patient quality of life.
The improvement in macular thickness is equally significant, and the persistence of these gains up to day 180 is particularly noteworthy. The reduction in CMT observed at day 30, and maintained through days 90 and 180, is a key indicator of improved anatomical outcomes. DME is characterized by the accumulation of fluid in the macular region, leading to structural changes in the retina.2 The observed reduction in CMT suggests that the DEX implant is effective in reducing this fluid accumulation, restoring retinal morphology, and contributing to visual improvement. These findings are consistent with previous studies highlighting the efficacy of corticosteroid therapy, and particularly the DEX implant, in reducing macular edema and improving vision in patients with DME.6,10,12–14 Moreover, the prolonged efficacy is essential in the management of chronic conditions like DME, as it reduces the need for frequent interventions and minimizes the potential burden on patients and healthcare systems. However, it is important to consider that DME is a complex and variable disease, and a longer-term follow-up would be beneficial to assess the durability of these improvements.
Recurrence of ocular edema was observed in 25% of the eyes in the current investigation on day 90. In a comparable study, the investigators found that 35% of the eyes developed a recurrence of edema.10 The higher frequency of recurrent edema observed in this study may be attributed to the inclusion of treatment-resistant cases, in contrast to our analysis which exclusively focused on treatment-naive eyes.
The study also evaluated the safety of DEX implant treatment, particularly with regard to the elevation of IOP, a common concern associated with corticosteroid therapy. The results showed a significant increase in mean IOP at day 30 following DEX implant administration. However, this IOP elevation was transient, as it returned to baseline levels by day 180. Importantly, only two eyes required topical AGM, indicating that the IOP increase was manageable and did not lead to significant complications. The transient nature of the IOP elevation is reassuring and suggests that DEX may have a favorable safety profile, especially when compared to other corticosteroid treatments. This is attributed to the sustained-release nature of the DEX implant, which gradually releases dexamethasone over several months, reducing the need for frequent injections and minimizing the risk of IOP-related side effects. The low requirement for AGM is a further testament to the manageable nature of the IOP increase. Comparing the safety profile of DEX with other corticosteroid treatments, such as intravitreal triamcinolone acetonide (IVTA), reveals that DEX is associated with a lower risk of elevated IOP.15,16 IVTA has been linked to a higher risk of IOP elevation and glaucoma, which has limited its long-term use.15,16 The findings of the current study, with only two eyes requiring topical AGM, support the notion that DEX may be a safer choice in terms of IOP management.
The outcomes of the study carry significant implications for the field of clinical practice. Firstly, they support the use of intravitreal DEX as an effective treatment strategy for treatment-naive DME patients who have systemic contraindications to anti-VEGF therapy. The substantial and sustained improvements in BCVA and CMT suggest that DEX is a valuable option for these patients, particularly in cases where anti-VEGF therapy is not feasible. Secondly, the use of DEX as a pre-cataract surgical approach in this study has significant implications. Administering the DEX implant one month prior to cataract surgery not only addresses macular edema but may also reduce inflammation and complications associated with cataract surgery. This dual approach has the potential to enhance patient care, streamline management, and improve outcomes. Moreover, the personalized approach emphasized in this study underscores the importance of considering patient-specific factors in the management of DME. Each patient’s medical history, systemic contraindications, and comorbidities should be taken into account when developing a tailored treatment plan. This approach aligns with the principles of precision medicine and individualized care. Finally, while the existing literature provides valuable evidence on the efficacy and safety of DEX in DME, the current study adds to this body of knowledge by focusing on a specific subset of patients—those with systemic contraindications to anti-VEGF therapy. This patient group is often underserved, and the study demonstrates that DEX is a viable and safe alternative for their management.
While the study provides valuable insights, it has certain limitations that should be acknowledged. It is a single-center, retrospective study with a relatively small sample size, which may limit the generalizability of the results. Larger, multicenter studies with more extensive cohorts are necessary to provide more robust evidence and validate these findings in a broader patient population. Additionally, the 180-day follow-up duration may not capture the long-term outcomes and potential recurrences of DME. Extended follow-up studies are essential to assess the durability of the DEX implant’s effects and monitor for any late complications. Future research should also delve into the patient-specific factors that influence the response to DEX implant therapy. Identifying patient subgroups that benefit the most from this treatment will help guide clinical decision-making.
Conclusion
To conclude, the current study provides compelling evidence for the use of intravitreal DEX implant as an effective therapeutic strategy for treatment-naive DME patients with systemic contraindications to anti-VEGF therapy. The improvements in BCVA and CMT, along with the manageable IOP increase and the low requirement for AGM, make this approach a promising option for DME patients, especially those with complex medical profiles. The study’s results have implications for clinical practice, including the potential for a pre-cataract surgical approach and the importance of patient-specific treatment plans. While further research is needed to confirm the long-term safety and efficacy of this approach, the findings offer hope for DME patients who face challenges in receiving optimal care. The DEX implant may provide a valuable addition to the array of treatments for DME, particularly in cases with systemic contraindications to anti-VEGF therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta N, Mansoor S, Sharma A, et al. Diabetic retinopathy and VEGF. Open Ophthalmol J. 2013;7(1):4–10. doi:10.2174/1874364101307010004
2. Bandello F, Battaglia Parodi M, Lanzetta P, et al. Diabetic macular edema. Dev Ophthalmol. 2017;58:102–138.
3. Chauhan MZ, Rather PA, Samarah SM, Elhusseiny AM, Sallam AB. Current and novel therapeutic approaches for treatment of diabetic macular edema. Cells. 2022;11(12):1950. doi:10.3390/cells11121950
4. Chakraborty S, Sheth JU. Contralateral effect following intravitreal brolucizumab injection in diabetic macular edema. Case Rep Ophthalmol Med. 2022;2022:3755249.
5. Chakraborty D, Sheth JU, Boral S, Sinha TK. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: a real-world case series. Am J Ophthalmol Case Rep. 2021;24:101197. doi:10.1016/j.ajoc.2021.101197
6. Fraser-Bell S, Kang HK, Mitchell P, Arnold JJ, Tainton J, Simonyi S. Dexamethasone intravitreal implant in treatment-naïve diabetic macular oedema: findings from the prospective, multicentre, AUSSIEDEX study. Br J Ophthalmol. 2023;107(1):72–78. doi:10.1136/bjophthalmol-2021-319070
7. Sharma A, Sheth J. Intravitreal dexamethasone implant for macular edema following uncomplicated phacoemulsification. Eur J Ophthalmol. 2015;25(3):e5. doi:10.5301/ejo.5000559
8. Sharma A, Sheth J, Madhusudan RJ, Sundaramoorthy SK. Effect of intravitreal dexamethasone implant on the contralateral eye: a case report. Retin Cases Brief Rep. 2013;7(3):217–219. doi:10.1097/ICB.0b013e31828993a1
9. He Y, Ren XJ, Hu BJ, Lam WC, Li XR. A meta-analysis of the effect of a dexamethasone intravitreal implant versus intravitreal anti-vascular endothelial growth factor treatment for diabetic macular edema. BMC Ophthalmol. 2018;18(1):121. doi:10.1186/s12886-018-0779-1
10. Kabanarou SA, Xirou T, Boutouri E, et al. Pre-operative intravitreal dexamethasone implant in patients with refractory diabetic macular edema undergoing cataract surgery. Sci Rep. 2020;10(1):5534. doi:10.1038/s41598-020-62561-3
11. Rauen PI, Ribeiro JA, Almeida FP, Scott IU, Messias A, Jorge R. Intravitreal injection of ranibizumab during cataract surgery in patients with diabetic macular edema. Retina. 2012;32(9):1799–1803. doi:10.1097/IAE.0b013e31824bebb8
12. Furino C, Boscia F, Niro A, et al. Combined phacoemulsification and intravitreal dexamethasone implant (Ozurdex®) in diabetic patients with coexisting cataract and diabetic macular edema. J Ophthalmol. 2017;2017:4896036. doi:10.1155/2017/4896036
13. Boyer DS, Yoon YH, Belfort R, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914.
14. Pareja-Ríos A, Ruiz-de la Fuente-Rodríguez P, Bonaque-González S, López-Gálvez M, Lozano-López V, Romero-Aroca P. Intravitreal dexamethasone implants for diabetic macular edema. Int J Ophthalmol. 2018;11(1):77–82. doi:10.18240/ijo.2018.01.14
15. Mishra SK, Gupta A, Patyal S, et al. Intravitreal dexamethasone implant versus triamcinolone acetonide for macular oedema of central retinal vein occlusion: quantifying efficacy and safety. Int J Retina Vitreous. 2018;4:13.
16. Badrinarayanan L, Rishi P, George R, Isaac N, Rishi E; Sankara Nethralaya Vitreo-Retinal group (SNVR). Incidence, risk factors, treatment, and outcome of ocular hypertension following intravitreal steroid injections: a comparative study. Ophthalmologica. 2022;245(5):431–438. doi:10.1159/000522504
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.